
PVR (CD155) Expression as a Potential Prognostic Marker in Multiple Myeloma

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients
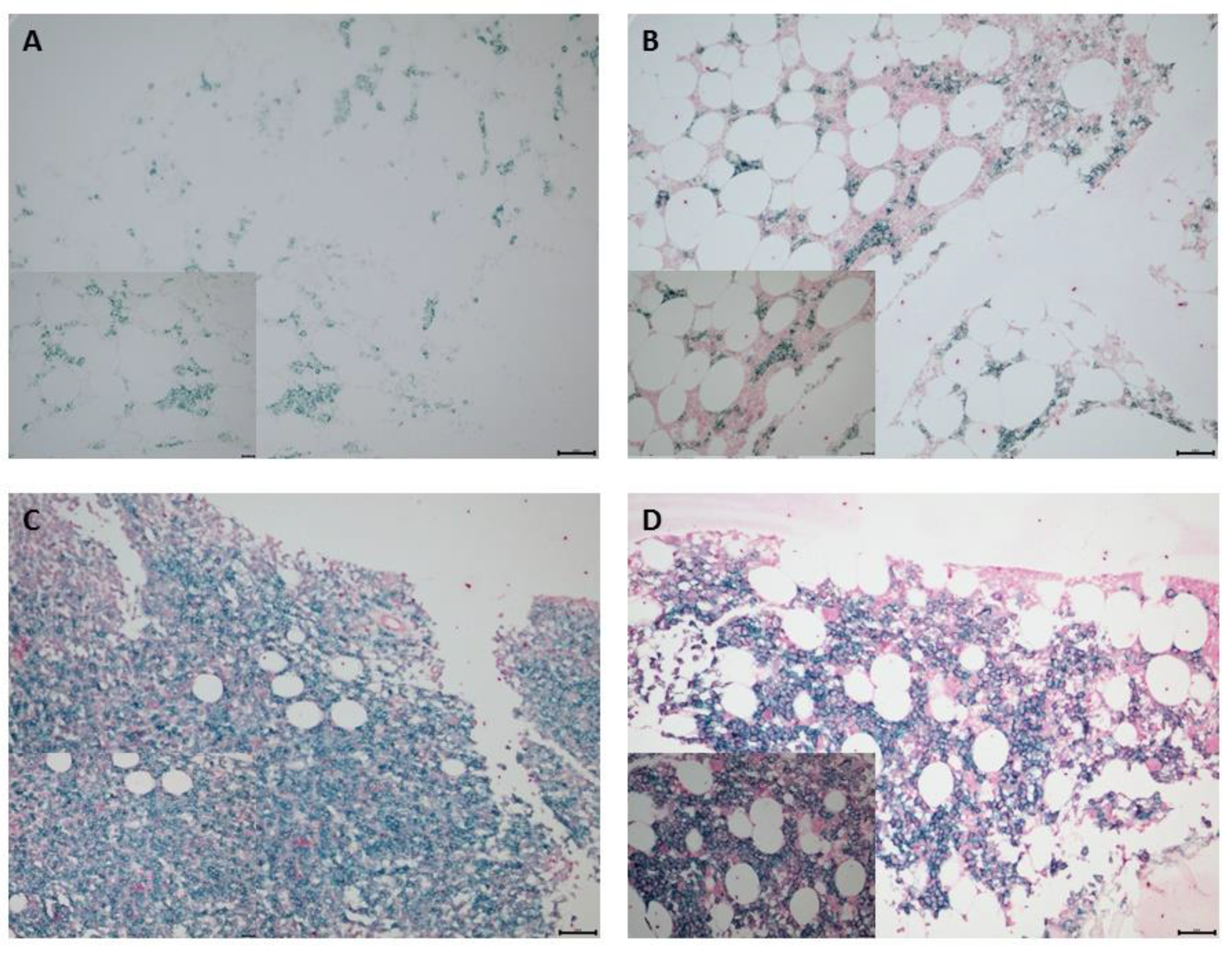
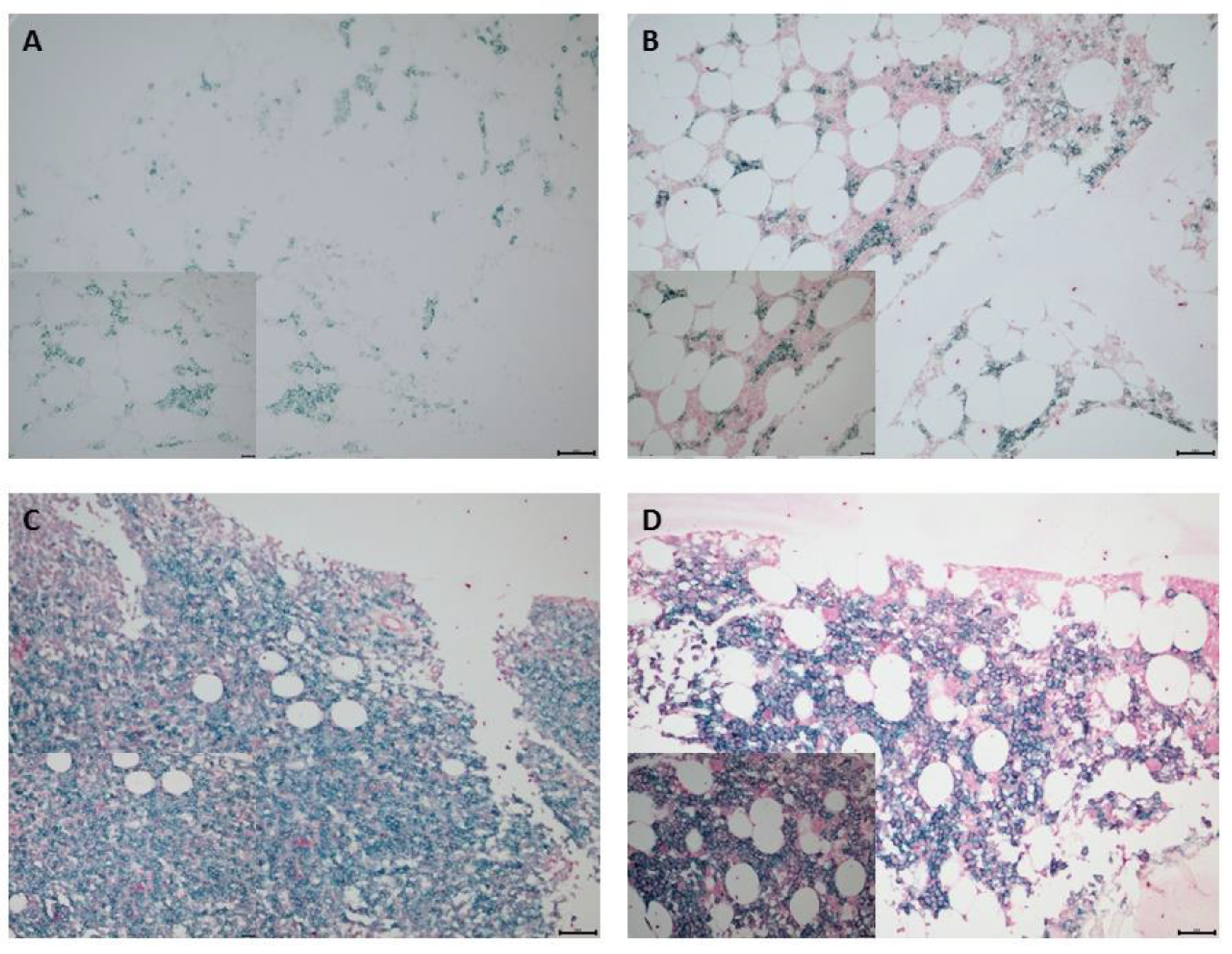
2.2. Immunohistochemistry (IHC) Staining and Analysis
2.3. Gene-Expression Analysis
2.4. Enzyme-Linked Immunosorbent Assay (ELISA)
2.5. Flow Cytometry
2.6. Statistical Analysis
3. Results
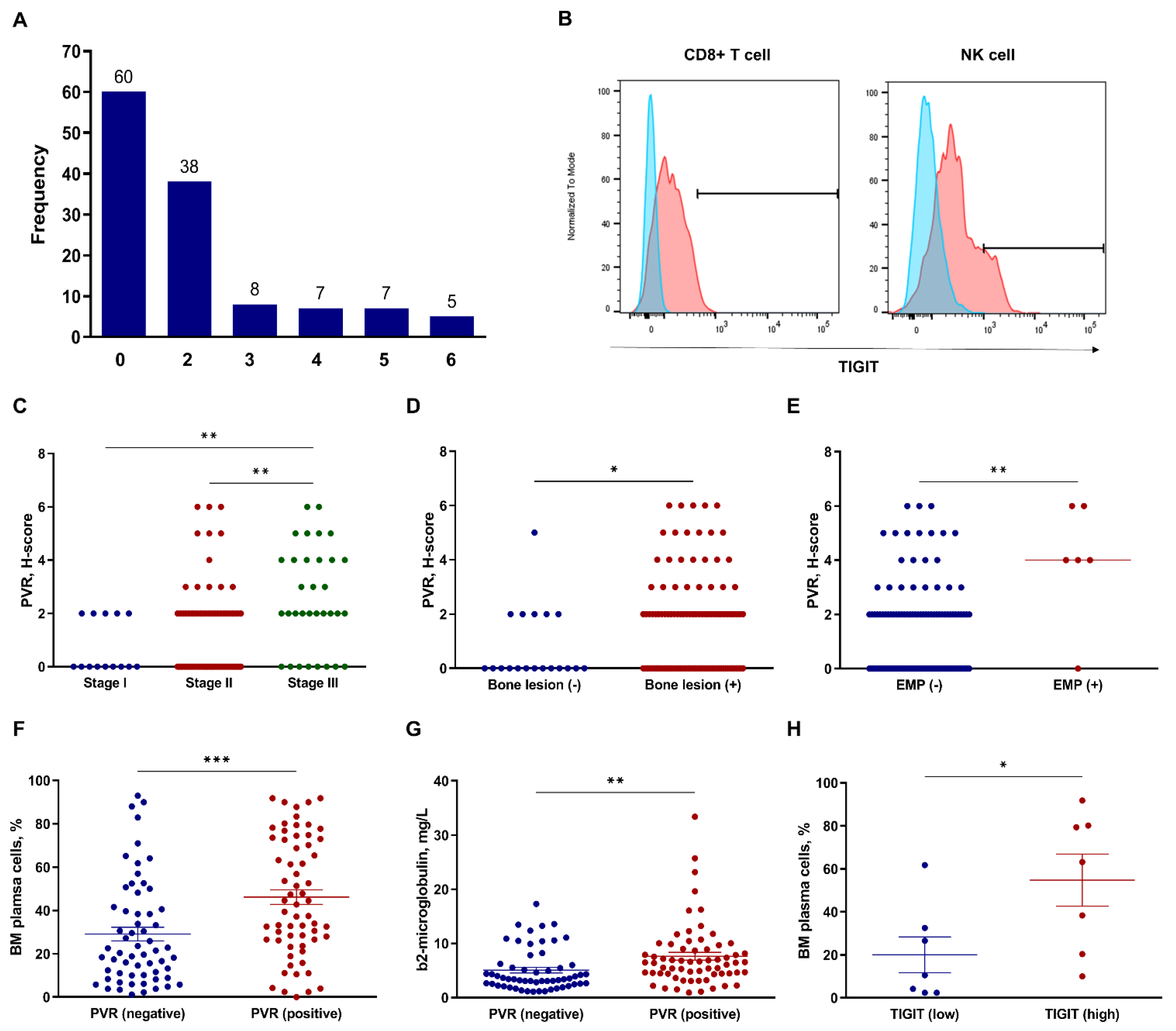
3.1. PVR and TIGIT Expression Relative to Clinical Factors
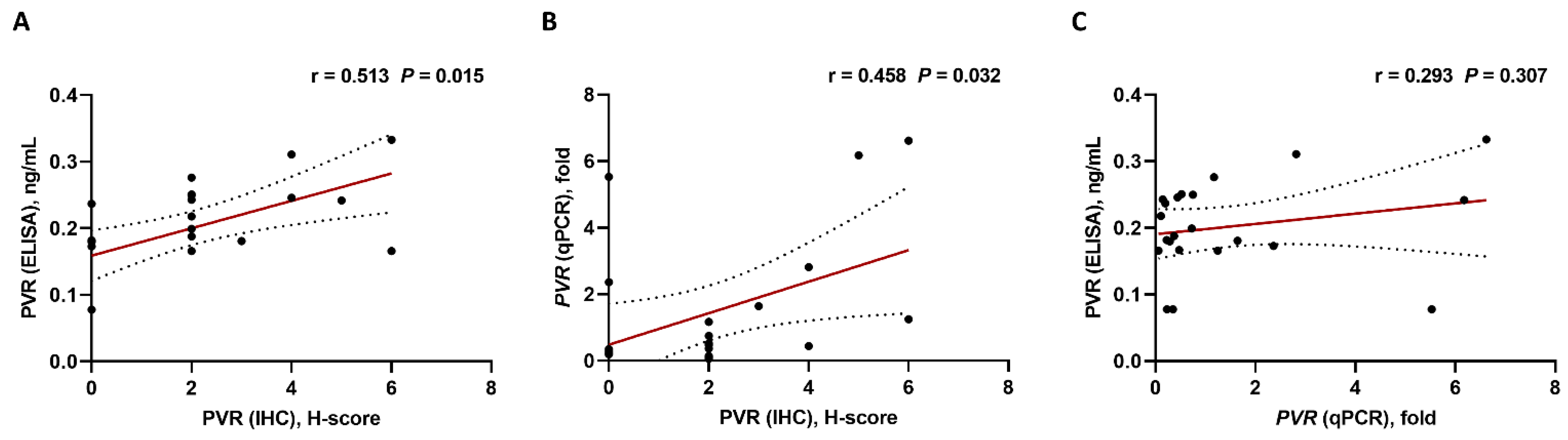
3.2. Analysis of PVR Expression Using Different Detection Methods
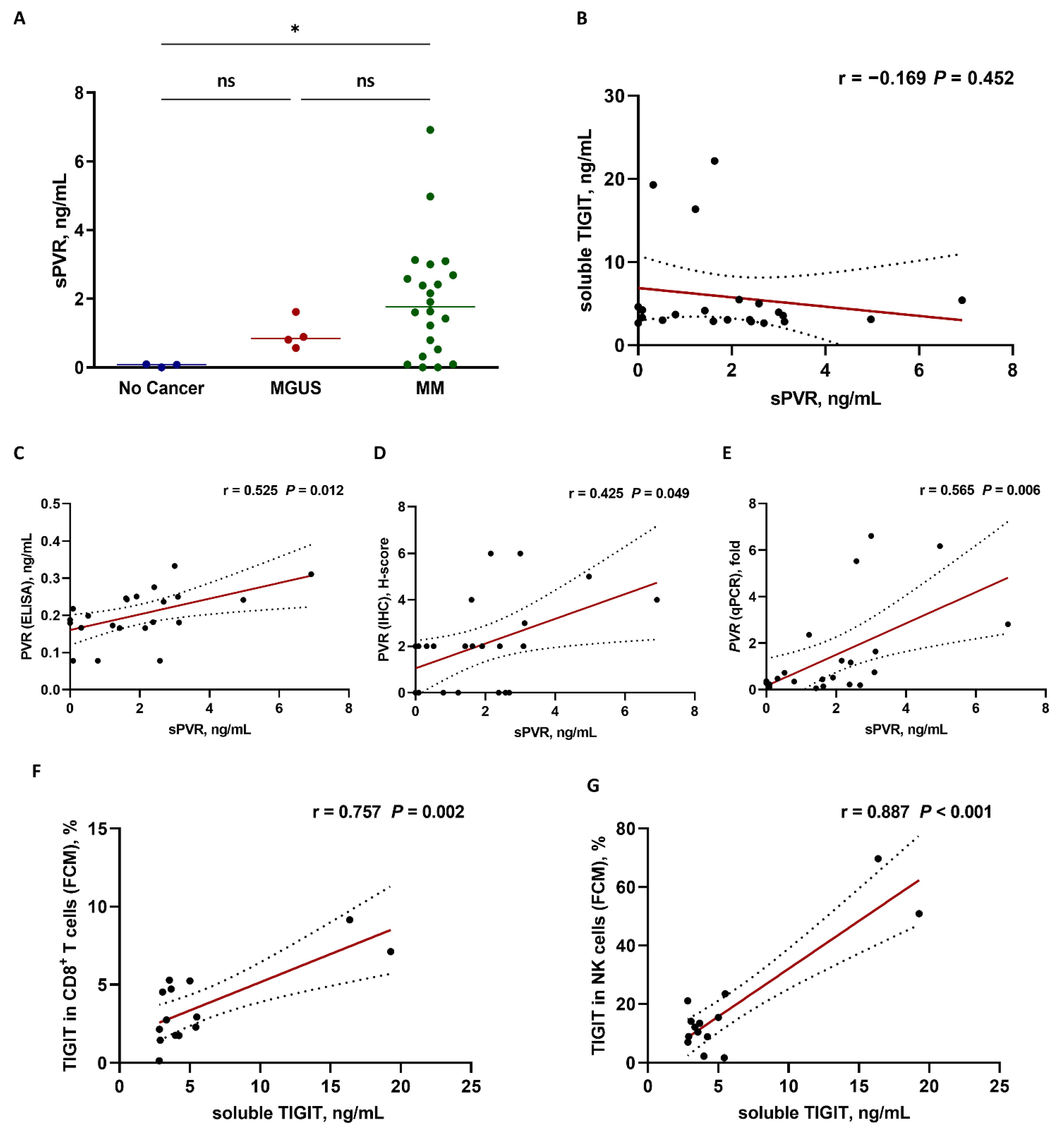
3.3. Analysis of Soluble PVR and TIGIT Levels
3.4. Patient Characteristics According to PVR-Expression Status
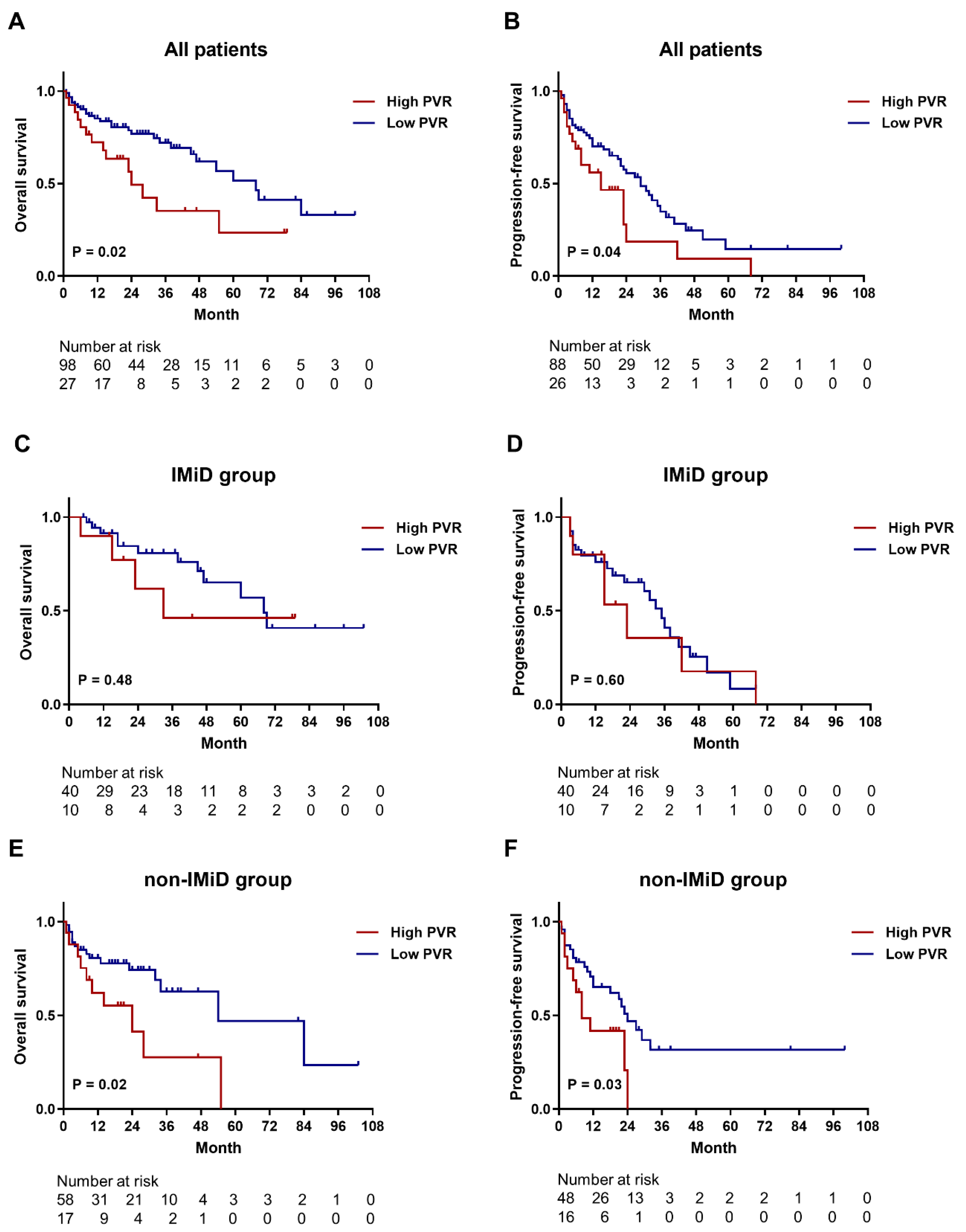
3.5. Survival Analysis
3.6. Prognostic Implication of PVR Expression
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Kučan Brlić, P.; Lenac Roviš, T.; Cinamon, G.; Tsukerman, P.; Mandelboim, O.; Jonjić, S. Targeting PVR (CD155) and its receptors in anti-tumor therapy. Cell. Mol. Immunol. 2019, 16, 40–52. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liu, L.; You, X.; Han, S.; Sun, Y.; Zhang, J.; Zhang, Y. CD155/TIGIT, a novel immune checkpoint in human cancers (review). Oncol. Rep. 2021, 45, 835–845. [Google Scholar] [CrossRef] [PubMed]
- Bronte, V. The expanding constellation of immune checkpoints: A DNAMic control by CD155. J. Clin. Investig. 2018, 128, 2199–2201. [Google Scholar] [CrossRef] [PubMed]
- Takai, Y.; Miyoshi, J.; Ikeda, W.; Ogita, H. Nectins and nectin-like molecules: Roles in contact inhibition of cell movement and proliferation. Nat. Rev. Mol. Cell Biol. 2008, 9, 603–615. [Google Scholar] [CrossRef] [PubMed]
- Smazynski, J.; Hamilton, P.T.; Thornton, S.; Milne, K.; Wouters, M.C.A.; Webb, J.R.; Nelson, B.H. The immune suppressive factors CD155 and PD-L1 show contrasting expression patterns and immune correlates in ovarian and other cancers. Gynecol. Oncol. 2020, 158, 167–177. [Google Scholar] [CrossRef] [PubMed]
- Masson, D.; Jarry, A.; Baury, B.; Blanchardie, P.; Laboisse, C.; Lustenberger, P.; Denis, M.G. Overexpression of the CD155 gene in human colorectal carcinoma. Gut 2001, 49, 236–240. [Google Scholar] [CrossRef] [Green Version]
- Duan, X.; Liu, J.; Cui, J.; Ma, B.; Zhou, Q.; Yang, X.; Lu, Z.; Du, Y.; Su, C. Expression of TIGIT/CD155 and correlations with clinical pathological features in human hepatocellular carcinoma. Mol. Med. Rep. 2019, 20, 3773–3781. [Google Scholar] [CrossRef] [Green Version]
- Sun, Y.; Luo, J.; Chen, Y.; Cui, J.; Lei, Y.; Cui, Y.; Jiang, N.; Jiang, W.; Chen, L.; Chen, Y.; et al. Combined evaluation of the expression status of CD155 and TIGIT plays an important role in the prognosis of LUAD (lung adenocarcinoma). Int. Immunopharmacol. 2020, 80, 106198. [Google Scholar] [CrossRef]
- Zhao, K.; Ma, L.; Feng, L.; Huang, Z.; Meng, X.; Yu, J. CD155 overexpression correlates with poor prognosis in primary small cell carcinoma of the esophagus. Front. Mol. Biosci. 2020, 7, 608404. [Google Scholar] [CrossRef]
- Huang, D.W.; Huang, M.; Lin, X.S.; Huang, Q. CD155 expression and its correlation with clinicopathologic characteristics, angiogenesis, and prognosis in human cholangiocarcinoma. OncoTargets Ther. 2017, 10, 3817–3825. [Google Scholar] [CrossRef] [Green Version]
- Lozano, E.; Mena, M.P.; Díaz, T.; Martin-Antonio, B.; León, S.; Rodríguez-Lobato, L.G.; Oliver-Caldés, A.; Cibeira, M.T.; Bladé, J.; Prat, A.; et al. Nectin-2 expression on malignant plasma cells is associated with better response to TIGIT blockade in multiple myeloma. Clin. Cancer Res. 2020, 26, 4688–4698. [Google Scholar] [CrossRef] [PubMed]
- Stamm, H.; Oliveira-Ferrer, L.; Grossjohann, E.M.; Muschhammer, J.; Thaden, V.; Brauneck, F.; Kischel, R.; Müller, V.; Bokemeyer, C.; Fiedler, W.; et al. Targeting the TIGIT-PVR immune checkpoint axis as novel therapeutic option in breast cancer. Oncoimmunology 2019, 8, e1674605. [Google Scholar] [CrossRef] [PubMed]
- Stamm, H.; Klingler, F.; Grossjohann, E.M.; Muschhammer, J.; Vettorazzi, E.; Heuser, M.; Mock, U.; Thol, F.; Vohwinkel, G.; Latuske, E.; et al. Immune checkpoints PVR and PVRL2 are prognostic markers in AML and their blockade represents a new therapeutic option. Oncogene 2018, 37, 5269–5280. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Harjunpää, H.; Guillerey, C. TIGIT as an emerging immune checkpoint. Clin. Exp. Immunol. 2020, 200, 108–119. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yeo, J.; Ko, M.; Lee, D.H.; Park, Y.; Jin, H.S. TIGIT/CD226 axis regulates anti-tumor immunity. Pharmaceuticals 2021, 14, 200. [Google Scholar] [CrossRef] [PubMed]
- Liang, R.; Zhu, X.; Lan, T.; Ding, D.; Zheng, Z.; Chen, T.; Huang, Y.; Liu, J.; Yang, X.; Shao, J.; et al. TIGIT promotes CD8+ T cells exhaustion and predicts poor prognosis of colorectal cancer. Cancer Immunol. Immunother. 2021, 70, 2781–2793. [Google Scholar] [CrossRef]
- Tang, W.; Pan, X.; Han, D.; Rong, D.; Zhang, M.; Yang, L.; Ying, J.; Guan, H.; Chen, Z.; Wang, X. Clinical significance of CD8+ T cell immunoreceptor with ig and ITIM domains+ in locally advanced gastric cancer treated with SOX regimen after D2 gastrectomy. Oncoimmunology 2019, 8, e1593807. [Google Scholar] [CrossRef] [Green Version]
- Liu, X.; Li, M.; Wang, X.; Dang, Z.; Jiang, Y.; Wang, X.; Kong, Y.; Yang, Z. PD-1+ TIGIT+ CD8+ T cells are associated with pathogenesis and progression of patients with hepatitis B virus-related hepatocellular carcinoma. Cancer Immunol. Immunother. 2019, 68, 2041–2054. [Google Scholar] [CrossRef]
- Xiao, K.; Xiao, K.; Li, K.; Xue, P.; Zhu, S. Prognostic role of TIGIT expression in patients with solid tumors: A meta-analysis. J. Immunol. Res. 2021, 2021, 5440572. [Google Scholar] [CrossRef]
- Yang, Z.Z.; Kim, H.J.; Wu, H.; Jalali, S.; Tang, X.; Krull, J.E.; Ding, W.; Novak, A.J.; Ansell, S.M. TIGIT expression is associated with T-cell suppression and exhaustion and predicts clinical outcome and anti-PD-1 response in follicular lymphoma. Clin. Cancer Res. 2020, 26, 5217–5231. [Google Scholar] [CrossRef]
- Kong, Y.; Zhu, L.; Schell, T.D.; Zhang, J.; Claxton, D.F.; Ehmann, W.C.; Rybka, W.B.; George, M.R.; Zeng, H.; Zheng, H. T-cell immunoglobulin and ITIM domain (TIGIT) associates with CD8+ T-cell exhaustion and poor clinical outcome in AML patients. Clin. Cancer Res. 2016, 22, 3057–3066. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liu, G.; Zhang, Q.; Yang, J.; Li, X.; Xian, L.; Li, W.; Lin, T.; Cheng, J.; Lin, Q.; Xu, X.; et al. Increased TIGIT expressing NK cells with dysfunctional phenotype in AML patients correlated with poor prognosis. Cancer Immunol. Immunother. 2022, 71, 277–287. [Google Scholar] [CrossRef] [PubMed]
- Guillerey, C.; Harjunpää, H.; Carrié, N.; Kassem, S.; Teo, T.; Miles, K.; Krumeich, S.; Weulersse, M.; Cuisinier, M.; Stannard, K.; et al. TIGIT immune checkpoint blockade restores CD8+ T-cell immunity against multiple myeloma. Blood 2018, 132, 1689–1694. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rajkumar, S.V. Updated diagnostic criteria and staging system for multiple myeloma. Am. Soc. Clin. Oncol. Educ. Book 2016, 35, e418–e423. [Google Scholar] [CrossRef]
- Contal, C.; O’Quigley, J. An application of changepoint methods in studying the effect of age on survival in breast cancer. Comp. Stat. Data Anal. 1999, 30, 253–270. [Google Scholar] [CrossRef]
- D’Anastasi, M.; Notohamiprodjo, M.; Schmidt, G.P.; Dürr, H.R.; Reiser, M.F.; Baur-Melnyk, A. Tumor load in patients with multiple myeloma: Beta2-microglobulin levels versus whole-body MRI. AJR Am. J. Roentgenol. 2014, 203, 854–862. [Google Scholar] [CrossRef]
- Molfetta, R.; Zitti, B.; Lecce, M.; Milito, N.D.; Stabile, H.; Fionda, C.; Cippitelli, M.; Gismondi, A.; Santoni, A.; Paolini, R. CD155: A multi-functional molecule in tumor progression. Int. J. Mol. Sci. 2020, 21, 922. [Google Scholar] [CrossRef] [Green Version]
- You, H.; Zhang, Y.Z.; Lai, H.L.; Li, D.; Liu, Y.Q.; Li, R.Z.; Khan, I.; Hsiao, W.W.; Duan, F.G.; Fan, X.X.; et al. Prognostic significance of tumor poliovirus receptor and CTLA4 expression in patients with surgically resected non-small-cell lung cancer. J. Cancer Res. Clin. Oncol. 2020, 146, 1441–1450. [Google Scholar] [CrossRef]
- Yong, H.; Cheng, R.; Li, X.; Gao, G.; Jiang, X.; Cheng, H.; Zhou, X.; Zhao, W. CD155 expression and its prognostic value in postoperative patients with breast cancer. Biomed. Pharmacother. 2019, 115, 108884. [Google Scholar] [CrossRef]
- Koike, S.; Horie, H.; Ise, I.; Okitsu, A.; Yoshida, M.; Iizuka, N.; Takeuchi, K.; Takegami, T.; Nomoto, A. The poliovirus receptor protein is produced both as membrane-bound and secreted forms. EMBO J. 1990, 9, 3217–3224. [Google Scholar] [CrossRef]
- Baury, B.; Masson, D.; McDermott, B.M.; Jarry, A.; Blottière, H.M.; Blanchardie, P.; Laboisse, C.L.; Lustenberger, P.; Racaniello, V.R.; Denis, M.G. Identification of secreted CD155 isoforms. Biochem. Biophys. Res. Commun. 2003, 309, 175–182. [Google Scholar] [CrossRef]
- Iguchi-Manaka, A.; Okumura, G.; Kojima, H.; Cho, Y.; Hirochika, R.; Bando, H.; Sato, T.; Yoshikawa, H.; Hara, H.; Shibuya, A.; et al. Increased soluble CD155 in the serum of cancer patients. PLoS ONE 2016, 11, e0152982. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jin, A.L.; Yang, Y.H.; Su, X.; Yang, W.J.; Liu, T.; Chen, W.; Li, T.; Ding, L.; Wang, H.; Wang, B.L.; et al. High serum soluble CD155 level predicts poor prognosis and correlates with an immunosuppressive tumor microenvironment in hepatocellular carcinoma. J. Clin. Lab. Anal. 2022, 36, e24259. [Google Scholar] [CrossRef] [PubMed]
- Iguchi-Manaka, A.; Okumura, G.; Ichioka, E.; Kiyomatsu, H.; Ikeda, T.; Bando, H.; Shibuya, A.; Shibuya, K. High expression of soluble CD155 in estrogen receptor-negative breast cancer. Breast Cancer 2020, 27, 92–99. [Google Scholar] [CrossRef] [Green Version]
- Azzazi, M.; Hegab, H.; Abdelallah, N.E.L.H.; Mohamed, H. AML-126: Prognostic value of serum CD 155 in adult acute myeloid leukemia patients: Relation to clinical outcome. Clin. Lymphoma Myeloma Leuk. 2020, 20, S182–S183. [Google Scholar] [CrossRef]
- Lozano, E.; Dominguez-Villar, M.; Kuchroo, V.; Hafler, D.A. The TIGIT/CD226 axis regulates human T cell function. J. Immunol. 2012, 188, 3869–3875. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Patient | IHC (H-Score) | ELISA (ng/mL) | qPCR (Fold, PVR/GAPDH) |
|---|---|---|---|
| #1 | 2 | 0.251 | 0.520 |
| #2 | 0 | 0.078 * | 0.348 |
| #3 | 4 | 0.311 | 2.815 |
| #4 | 3 | 0.181 | 1.643 |
| #5 | 0 | 0.173 | 2.362 |
| #6 | 0 | 0.078 * | 5.528 |
| #7 | 2 | 0.243 | 0.143 |
| #8 | 2 | 0.250 | 0.751 |
| #9 | 2 | 0.276 | 1.170 |
| #10 | 6 | 0.333 | 6.619 |
| #11 | 6 | 0.166 | 1.248 |
| #12 | 4 | 0.246 | 0.443 |
| #13 | 2 | 0.167 | 0.475 |
| #14 | 0 | 0.078 * | 0.227 |
| #15 | 2 | 0.218 | 0.109 |
| #16 | 2 | 0.188 | 0.373 |
| #17 | 2 | 0.199 | 0.729 |
| #18 | 0 | 0.182 | 0.223 |
| #19 | 0 | 0.237 | 0.199 |
| #20 | 0 | 0.180 | 0.285 |
| #21 | 2 | 0.166 | 0.061 |
| #22 | 5 | 0.242 | 6.176 |
| Total (n = 125) | Low (n = 98) | High (n = 27) | p | |
|---|---|---|---|---|
| Age, y | 66.0 (58.0–72.0) | 66.0 (58.0–72.3) | 66.0 (58.0–72.0) | 0.865 |
| Sex, female | 56 (44.8) | 46 (46.9) | 10 (37.0) | 0.360 |
| ECOG PS, ≥2 | 8 (6.4) | 6 (6.1) | 2 (7.4) | 0.682 |
| BM plasma cells, % | 32.6 (15.6–61.3) | 30.4 (12.8–51.9) | 46.5 (25.9–77.0) | 0.018 |
| Serum M-protein, g/dL | 2.20 (0.45–4.75) | 2.12 (0.39–4.63) | 3.30 (0.50–5.00) | 0.350 |
| Albumin, g/dL | 3.30 (2.75–3.90) | 3.40 (2.80–3.90) | 2.90 (2.50–3.70) | 0.088 |
| <3.5 g/dL | 71 (56.8) | 54 (55.1) | 17 (63.0) | 0.465 |
| β2-microglobulin, mg/L | 4.87 (3.07–8.35) | 4.44 (2.66–7.87) | 6.63 (5.39–10.5) | 0.004 |
| ≥5.5 mg/L | 53 (42.4) | 35 (35.7) | 18 (66.7) | 0.004 |
| LDH, IU/L | 390 (303–480) | 363 (297–463) | 434 (391–570) | 0.070 |
| >ULN | 53 (42.4) | 37 (37.8) | 16 (59.3) | 0.045 |
| Calcium, mg/dL | 9.10 (8.35–9.75) | 9.20 (8.48–9.70) | 8.50 (7.80–10.5) | 0.886 |
| >11 mg/dL | 12 (9.6) | 4 (6.7) | 8 (12.3) | 0.285 |
| Creatinine, mg/dL | 1.07 (0.81–1.84) | 1.03 (0.80–1.53) | 1.20 (1.01–2.21) | 0.123 |
| >2 mg/dL | 24 (19.2) | 10 (16.7) | 14 (21.5) | 0.490 |
| Hb, g/dL | 9.50 (8.30–11.3) | 9.65 (8.70–11.4) | 8.30 (7.40–9.30) | 0.002 |
| <10 g/dL | 75 (60.0) | 28 (46.7) | 47 (72.3) | 0.003 |
| Cytogenetic abnormalities | ||||
| High risk * | 41 (32.8) | 28 (28.6) | 13 (48.1) | 0.055 |
| ISS | ||||
| Stage I | 26 (20.8) | 25 (25.5) | 1 (3.7) | 0.006 |
| Stage II | 46 (36.8) | 38 (38.8) | 8 (29.6) | |
| Stage III | 53 (42.4) | 35 (35.7) | 18 (66.7) | |
| R-ISS | ||||
| Stage I | 14 (11.2) | 14 (14.3) | 0 (0.0) | <0.001 |
| Stage II | 78 (62.4) | 66 (67.3) | 12 (44.4) | |
| Stage III | 33 (26.4) | 18 (18.4) | 15 (55.6) | |
| CTx regimen, 1st | ||||
| VTD | 26 (20.8) | 22 (22.4) | 4 (14.8) | 0.381 |
| TD or RD | 24 (19.2) | 17 (17.3) | 7 (25.9) | |
| VMP | 57 (45.6) | 45 (45.9) | 12 (44.4) | |
| Others | 7 (5.6) | 4 (4.1) | 3 (11.1) | |
| Supportive only | 11 (8.8) | 10 (10.2) | 1 (3.7) | |
| CTx regimen, 2nd (n = 62) | 0.864 † | |||
| KRD or IRD | 22 (35.5) | 20 (43.5) | 2 (12.5) | |
| TD or RD | 15 (24.2) | 8 (17.4) | 7 (43.8) | |
| VD | 21 (33.9) | 16 (34.8) | 5 (31.2) | |
| Others | 4 (6.5) | 2 (4.3) | 2 (12.5) | |
| CTx regimen, 3rd (n = 32) | 0.296 † | |||
| KRD or IRD | 7 (21.9) | 4 (16.7) | 3 (37.5) | |
| RD or PD | 19 (59.4) | 14 (58.3) | 5 (62.5) | |
| VD | 4 (12.5) | 4 (16.7) | 0 | |
| Others | 2 (6.2) | 2 (8.3) | 0 | |
| Transplantation | ||||
| Auto-SCT | 30 (24.0) | 22 (22.4) | 8 (29.6) | 0.439 |
| Allo-SCT | 0 | 0 | 0 | |
| None | 95 (76.0) | 76 (77.6) | 19 (70.4) |
| Prognostic Factors | Univariate | Multivariate | ||||
|---|---|---|---|---|---|---|
| HR | 95% CI | p | HR | 95% CI | p | |
| Age, y | 1.032 | 1.000, 1.065 | 0.052 | 1.032 | 0.997, 1.068 | 0.075 |
| ECOG PS, ≥2 | 3.142 | 1.097, 8.994 | 0.033 | 3.768 | 1.185, 11.983 | 0.025 |
| BM plasma cells, % | 1.004 | 0.992, 1.016 | 0.525 | |||
| Serum M-protein, mg/dL | 0.950 | 0.835, 1.080 | 0.434 | 0.887 | 0.765, 1.028 | 0.111 |
| Albumin, g/dL | 0.900 | 0.595, 1.359 | 0.615 | |||
| β2-microglobulin, mg/L | 1.041 | 0.987, 1.099 | 0.139 | |||
| LDH, >ULN | 2.912 | 1.545, 5.488 | 0.001 | 2.069 | 1.040, 4.113 | 0.038 |
| Cytogenetics, high-risk * | 2.072 | 1.086, 3.956 | 0.027 | 2.373 | 1.165, 4.834 | 0.017 |
| Achievement of CR | 0.323 | 0.127, 0.823 | 0.018 | |||
| PVR expression, high | 2.127 | 1.114, 4.065 | 0.022 | 2.029 | 1.003, 4.103 | 0.048 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lee, B.-H.; Kim, J.-H.; Kang, K.-W.; Lee, S.-R.; Park, Y.; Sung, H.-J.; Kim, B.-S. PVR (CD155) Expression as a Potential Prognostic Marker in Multiple Myeloma. Biomedicines 2022, 10, 1099. https://doi.org/10.3390/biomedicines10051099
Lee B-H, Kim J-H, Kang K-W, Lee S-R, Park Y, Sung H-J, Kim B-S. PVR (CD155) Expression as a Potential Prognostic Marker in Multiple Myeloma. Biomedicines. 2022; 10(5):1099. https://doi.org/10.3390/biomedicines10051099
Chicago/Turabian StyleLee, Byung-Hyun, Ji-Hea Kim, Ka-Won Kang, Se-Ryeon Lee, Yong Park, Hwa-Jung Sung, and Byung-Soo Kim. 2022. "PVR (CD155) Expression as a Potential Prognostic Marker in Multiple Myeloma" Biomedicines 10, no. 5: 1099. https://doi.org/10.3390/biomedicines10051099
APA StyleLee, B.-H., Kim, J.-H., Kang, K.-W., Lee, S.-R., Park, Y., Sung, H.-J., & Kim, B.-S. (2022). PVR (CD155) Expression as a Potential Prognostic Marker in Multiple Myeloma. Biomedicines, 10(5), 1099. https://doi.org/10.3390/biomedicines10051099