
Effect of Vitamin K on Bone Mineral Density and Fracture Risk in Adults: Systematic Review and Meta-Analysis

 , , ,
, , ,
Abstract
:1. Introduction
2. Methodology
2.1. Search Strategy
2.2. Study Selection
2.3. Data Extraction
2.4. Statistical Analysis
3. Results
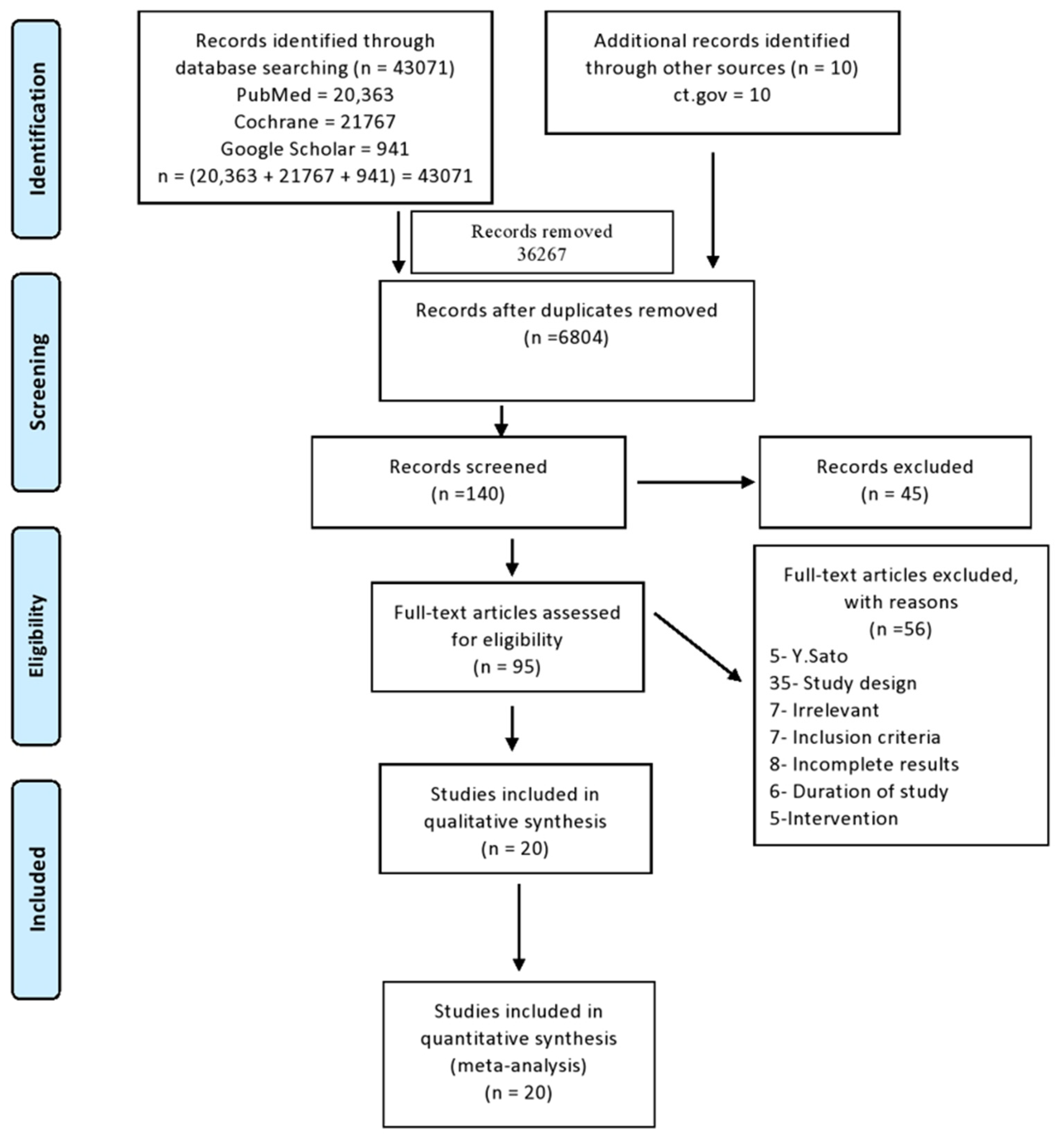
3.1. Study Selection
3.2. Study Characteristics
3.3. Meta-Analysis
3.3.1. Fractures
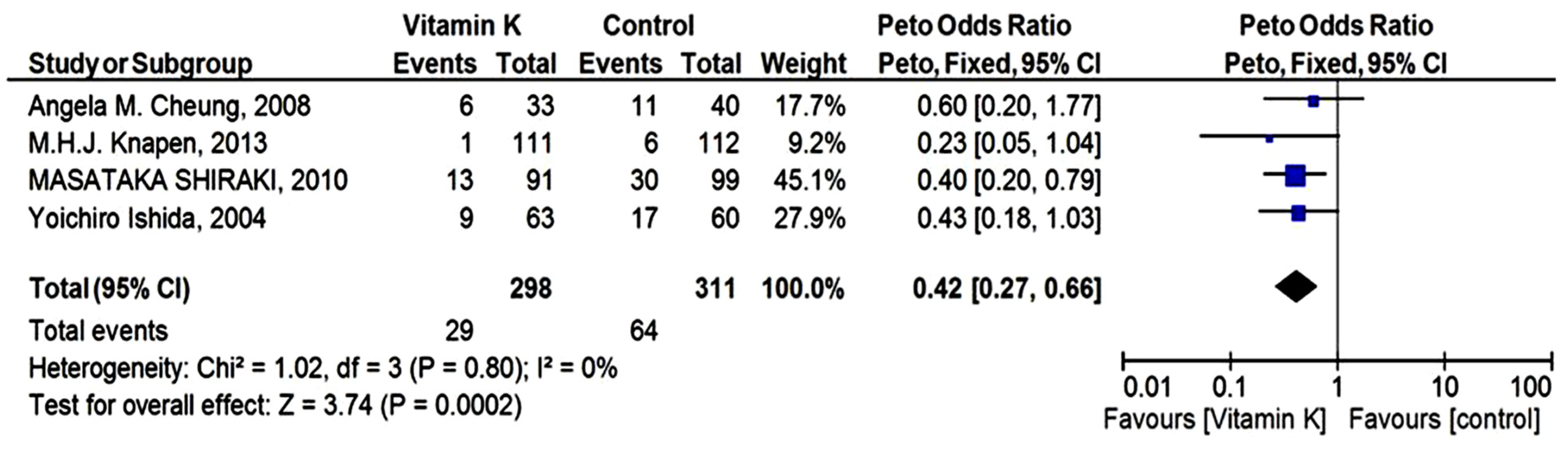
3.3.2. Vertebral Fractures
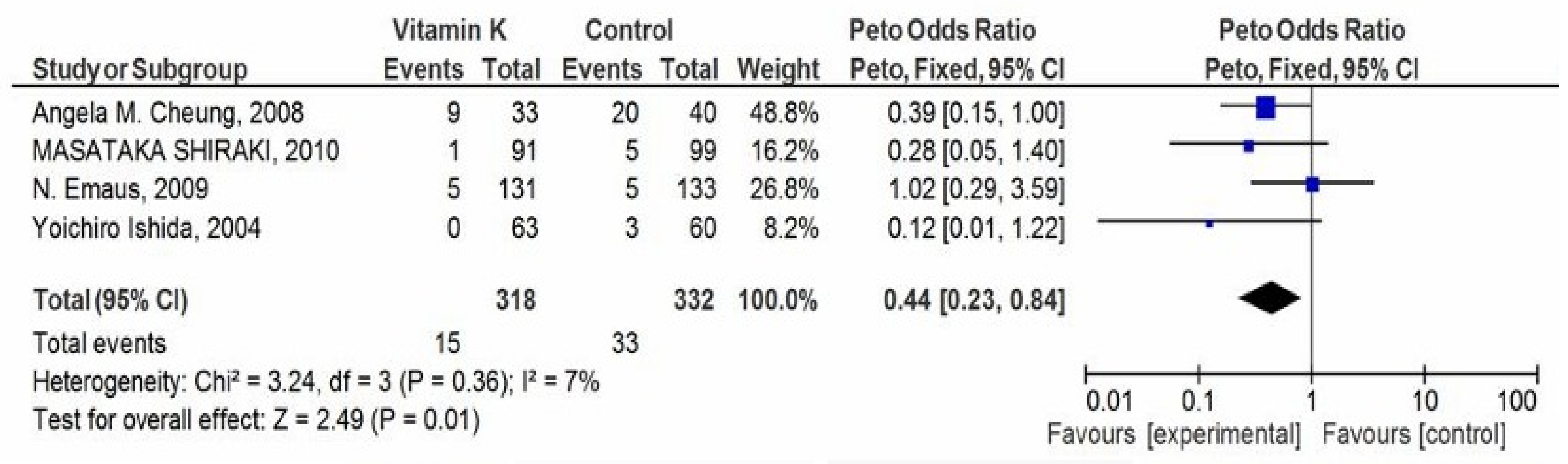
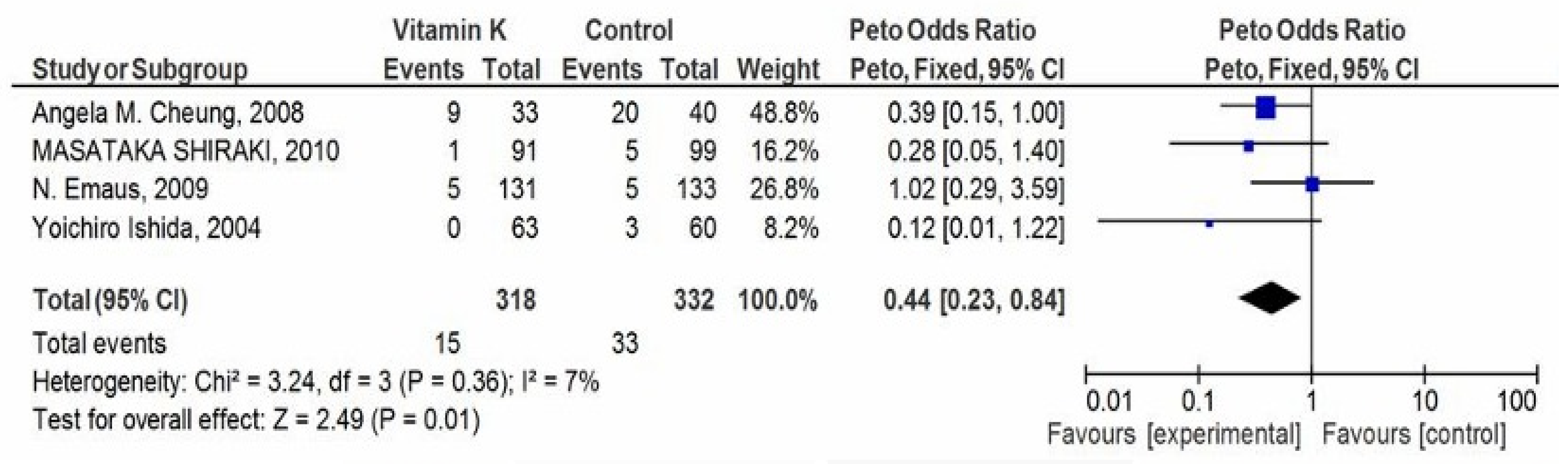
3.3.3. Clinical Fractures
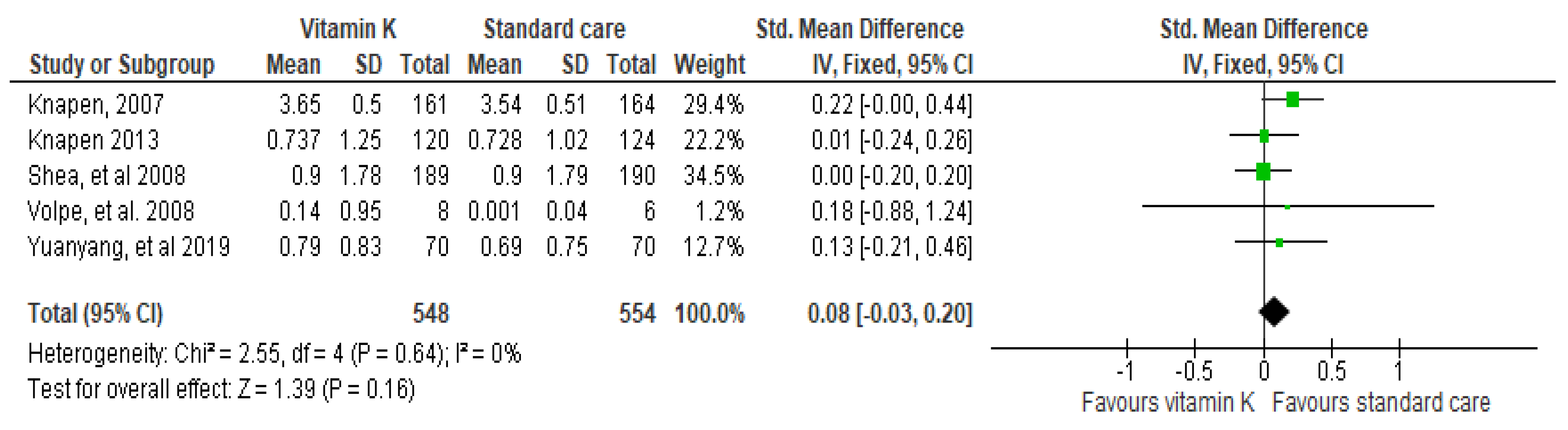
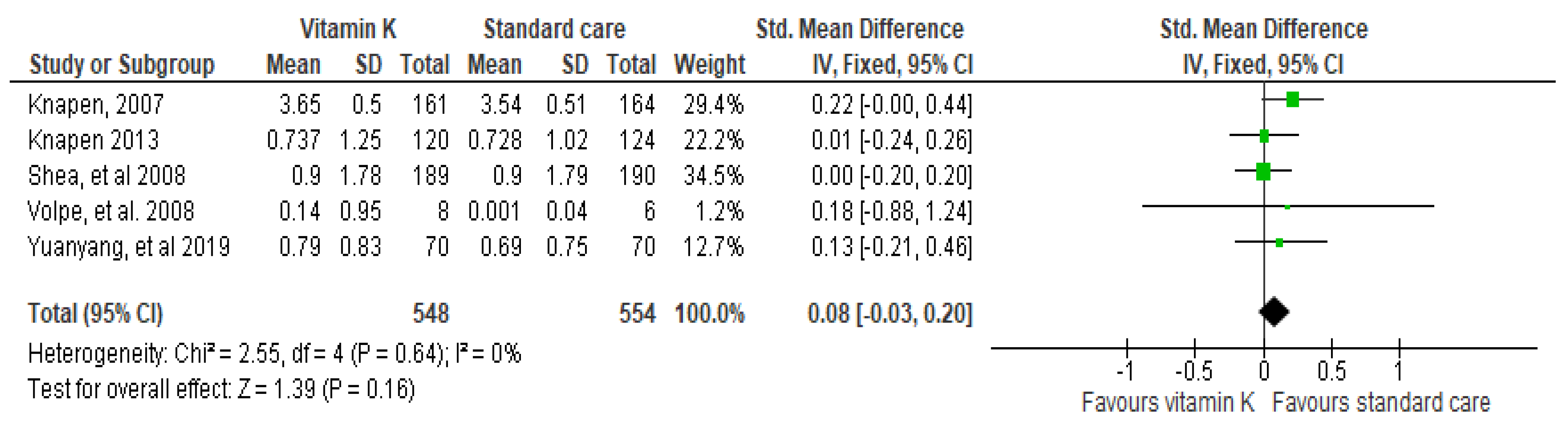
3.3.4. BMD as Outcome
4. Discussion
5. Limitations
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Akbari, S.; Rasouli-Ghahroudi, A.A. Vitamin K and Bone Metabolism: A Review of the Latest Evidence in Preclinical Studies. BioMed Res. Int. 2018, 2018, 1–8. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ahmadieh, H.; Arabi, A. Vitamins and bone health: Beyond calcium and vitamin D. Nutr. Rev. 2011, 69, 584–598. [Google Scholar] [CrossRef] [PubMed]
- Binkley, N.; Harke, J.; Krueger, D.; Engelke, J.; Vallarta-Ast, N.; Gemar, D.; Checovich, M.; Chappell, R.; Suttie, J. Vitamin K Treatment Reduces Undercarboxylated Osteocalcin but Does Not Alter Bone Turnover, Density, or Geometry in Healthy Postmenopausal North American Women. J. Bone Miner. Res. 2009, 24, 983–991. [Google Scholar] [CrossRef] [PubMed]
- Bolton-Smith, C.; McMurdo, M.E.T.; Paterson, C.R.; Mole, P.A.; Harvey, J.M.; Fenton, S.T.; Prynne, C.J.; Mishra, G.D.; Shearer, M.J. Two-Year Randomized Controlled Trial of Vitamin K1 (Phylloquinone) and Vitamin D3 Plus Calcium on the Bone Health of Older Women. J. Bone Miner. Res. 2007, 22, 509–519. [Google Scholar] [CrossRef]
- Sozen, T.; Ozışık, L.; Başaran, N.Ç. An overview and management of osteoporosis. Eur. J. Rheumatol. 2017, 4, 46. [Google Scholar] [CrossRef]
- Center, J.R.; Nguyen, T.V.; Schneider, D.; Sambrook, P.N.; Eisman, J.A. Mortality after all major types of osteoporotic fracture in men and women: An observational study. Lancet 1999, 353, 878–882. [Google Scholar] [CrossRef]
- Chalmers, G.L. Disorders of bone. Practitioner 1978, 220, 711–721. [Google Scholar] [CrossRef]
- Cheung, A.M.; Tile, L.; Lee, Y.; Tomlinson, G.; Hawker, G.; Scher, J.; Hu, H.; Vieth, R.; Thompson, L.; Jamal, S.; et al. Vitamin K Supplementation in Postmenopausal Women with Osteopenia (ECKO Trial): A Randomized Controlled Trial. PLoS Med. 2008, 5, e196. [Google Scholar] [CrossRef]
- Emaus, N.; Gjesdal, C.G.; Almas, B.; Christensen, M.; Grimsgaard, A.S.; Berntsen, G.K.R.; Salomonsen, L.; Fønnebø, V. Vitamin K2 supplementation does not influence bone loss in early menopausal women: A randomised double-blind placebo-controlled trial. Osteoporos. Int. 2009, 21, 1731–1740. [Google Scholar] [CrossRef]
- Braam, L.A.J.L.M.; Knapen, M.H.J.; Geusens, P.; Brouns, F.; Gerichhausen, M.J.W.; Vermeer, C. Vitamin K1 Supplementation Retards Bone Loss in Postmenopausal Women Between 50 and 60 Years of Age. Calcif. Tissue Res. 2003, 73, 21–26. [Google Scholar] [CrossRef]
- Hao, G.; Zhang, B.; Gu, M.; Chen, C.; Zhang, Q.; Zhang, G.; Cao, X. Vitamin K intake and the risk of fractures. Medicine 2017, 96, e6725. [Google Scholar] [CrossRef] [PubMed]
- Hirao, M.; Hashimoto, J.; Ando, W.; Ono, T.; Yoshikawa, H. Response of serum carboxylated and undercarboxylated osteocalcin to alendronate monotherapy and combined therapy with vitamin K2 in postmenopausal women. J. Bone Miner. Metab. 2008, 26, 260–264. [Google Scholar] [CrossRef] [PubMed]
- Ishida, Y.; Kawai, S. RETRACTED: Comparative efficacy of hormone replacement therapy, etidronate, calcitonin, alfacalcidol, and vitamin K in postmenopausal women with osteoporosis: The Yamaguchi Osteoporosis Prevention Study. Am. J. Med. 2004, 117, 549–555. [Google Scholar] [CrossRef] [PubMed]
- Je, S.H.; Joo, N.-S.; Choi, B.-H.; Kim, K.-M.; Kim, B.-T.; Park, S.-B.; Cho, D.-Y.; Kim, K.-N.; Lee, D.-J. Vitamin K Supplement Along with Vitamin D and Calcium Reduced Serum Concentration of Undercarboxylated Osteocalcin While Increasing Bone Mineral Density in Korean Postmenopausal Women over Sixty-Years-Old. J. Korean Med. Sci. 2011, 26, 1093–1098. [Google Scholar] [CrossRef]
- Kasukawa, Y.; Miyakoshi, N.; Ebina, T.; Aizawa, T.; Hongo, M.; Nozaka, K.; Ishikawa, Y.; Saito, H.; Chida, S.; Shimada, Y. Effects of risedronate alone or combined with vitamin K2 on serum undercarboxylated osteocalcin and osteocalcin levels in postmenopausal osteoporosis. J. Bone Miner. Metab. 2013, 32, 290–297. [Google Scholar] [CrossRef]
- Morishita, M.; Nagashima, M.; Wauke, K.; Takahashi, H.; Takenouchi, K. Osteoclast inhibitory effects of vitamin K2 alone or in combination with etidronate or risedronate in patients with rheumatoid arthritis: 2-year results. J. Rheumatol. 2008, 35, 407–413. [Google Scholar]
- Purwosunu, Y.; Rachman, I.A.; Reksoprodjo, S.; Sekizawa, A. Muharram Vitamin K2 treatment for postmenopausal osteoporosis in Indonesia. J. Obstet. Gynaecol. Res. 2006, 32, 230–234. [Google Scholar] [CrossRef]
- Somekawa, Y.; Chigughi, M.; Harada, M. Use of Vitamin K2 (Menatetrenone) and 1,25-dihydroxyvitamin D 3 in the Prevention of Bone Loss Induced by Leuprolide. J. Clin. Endocrinol. Metab. 1999, 84, 2700–2704. [Google Scholar] [CrossRef]
- Shea, M.K.; Dallal, G.E.; Dawson-Hughes, B.; Ordovas, J.M.; O’Donnell, C.J.; Gundberg, C.M.; Peterson, J.W.; Booth, S.L. Vitamin K, circulating cytokines, and bone mineral density in older men and women23. Am. J. Clin. Nutr. 2008, 88, 356–363. [Google Scholar] [CrossRef] [Green Version]
- Shiraki, M.; Shiraki, Y.; Aoki, C.; Miura, M. Vitamin K2 (Menatetrenone) Effectively Prevents Fractures and Sustains Lumbar Bone Mineral Density in Osteoporosis. J. Bone Miner. Res. 2010, 15, 515–521. [Google Scholar] [CrossRef]
- Mott, A.; Bradley, T.; Wright, K.; Cockayne, E.S.; Shearer, M.J.; Adamson, J.; Lanham-New, S.A.; Torgerson, D.J. Correction to Effect of vitamin K on bone mineral density and fractures in adults: An updated systematic review and meta-analysis of randomised controlled trials. Osteoporos. Int. 2019, 30, 1543–1559. [Google Scholar] [CrossRef] [PubMed]
- Volpe, S.L.; Leung, M.M.; Giordano, H. Vitamin K supplementation does not significantly impact bone mineral density and biochemical markers of bone in pre- and perimenopausal women. Nutr. Res. 2008, 28, 577–582. [Google Scholar] [CrossRef] [PubMed]
- Knapen, M.H.J.; Schurgers, L.J.; Vermeer, C. Vitamin K2 supplementation improves hip bone geometry and bone strength indices in postmenopausal women. Osteoporos. Int. 2007, 18, 963–972. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vermeer, C.; Knapen, M. Vitamin K and Bone. Diet Nutr. Bone Health 2011, 14, 191–200. [Google Scholar] [CrossRef]
- Iwamoto, I.; Kosha, S.; Noguchi, S.-I.; Murakami, M.; Fujino, T.; Douchi, T.; Nagata, Y. A longitudinal study of the effect of vitamin K2 on bone mineral density in postmenopausal women a comparative study with vitamin D3 and estrogen–progestin therapy. Maturitas 1999, 31, 161–164. [Google Scholar] [CrossRef]
- Yuanyang, G.; Runlin, X.; Bo, X.; Donghua, F.; Jun, M. Effect of vitamin K2 on bone mineral density and serum cathepsin K in female osteoporosis patients. Trop. J. Pharm. Res. 2019, 18, 181. [Google Scholar] [CrossRef]
- Johnell, O.; Kanis, J.A. An estimate of the worldwide prevalence and disability associated with osteoporotic fractures. Osteoporos. Int. 2006, 17, 1726–1733. [Google Scholar] [CrossRef]
- Armour, K.E.; Armour, K.J.; Gallagher, M.E.; Gödecke, A.; Helfrich, M.H.; Reid, D.M.; Ralston, S.H. Defective Bone Formation and Anabolic Response to Exogenous Estrogen in Mice with Targeted Disruption of Endothelial Nitric Oxide Synthase. Endocrinology 2001, 142, 760–766. [Google Scholar] [CrossRef]
- Odén, A.; McCloskey, E.V.; Kanis, J.A.; Harvey, N.; Johansson, H. Burden of high fracture probability worldwide: Secular increases 2010–2040. Osteoporos. Int. 2015, 26, 2243–2248. [Google Scholar] [CrossRef]
- Palermo, A.; Tuccinardi, D.; D’Onofrio, L.; Watanabe, M.; Maggi, D.; Maurizi, A.R.; Greto, V.; Buzzetti, R.; Napoli, N.; Pozzilli, P.; et al. Vitamin K and osteoporosis: Myth or reality? Metabolism 2017, 70, 57–71. [Google Scholar] [CrossRef] [Green Version]
- Rachner, T.D.; Khosla, S.; Hofbauer, L.C. Osteoporosis: Now and the future. Lancet 2011, 377, 1276–1287. [Google Scholar] [CrossRef] [Green Version]
- Reginster, J.-Y.; Ferrari, S.; Hadji, P. Current challenges in the treatment of osteoporosis: An opportunity for bazedoxifene. Curr. Med. Res. Opin. 2014, 30, 1165–1176. [Google Scholar] [CrossRef] [PubMed]
- Rizzoli, R.; Body, J.J.; De Censi, A.; Reginster, J.Y.; Piscitelli, P.; Brandi, M.L. Guidance for the prevention of bone loss and fractures in postmenopausal women treated with aromatase inhibitors for breast cancer: An ESCEO position paper. Osteoporos. Int. 2012, 23, 2567–2576. [Google Scholar] [CrossRef] [PubMed]
- Rodríguez, C.R.-O.; Curiel, M.D. Vitamin K and Bone Health: A Review on the Effects of Vitamin K Deficiency and Supplementation and the Effect of Non-Vitamin K Antagonist Oral Anticoagulants on Different Bone Parameters. J. Osteoporos. 2019, 2019, 2069176. [Google Scholar] [CrossRef]
- Salari, N.; Ghasemi, H.; Mohammadi, L.; Behzadi, M.H.; Rabieenia, E.; Shohaimi, S.; Mohammadi, M. The global prevalence of osteoporosis in the world: A comprehensive systematic review and meta-analysis. J. Orthop. Surg. Res. 2021, 16, 1–20. [Google Scholar] [CrossRef]
- Zhao, B.; Zhao, W.; Wang, Y.; Zhao, Z.; Zhao, C.; Wang, S.; Gao, C. Prior administration of vitamin K2 improves the therapeutic effects of zoledronic acid in ovariectomized rats by antagonizing zoledronic acid-induced inhibition of osteoblasts proliferation and mineralization. PLoS ONE 2018, 13, e0202269. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Author | Ethical Approval | Selection Bias | Performance Bias (Blinding) | Attrition Bias Incomplete Outcome | Selective Reporting | |
|---|---|---|---|---|---|---|
| Randomization | Allocation | |||||
| [10] | University Hospital medical ethics committee | Low | Low | Low | Low | Low |
| [8] | (#NCT00150969 (#ISRCTN61708241) | Low | Low | Low | Low | Low |
| [9] | NCT00290212 | Low | Low | Low | Low | Low |
| [12] | Low | Low | Unclear | Low | Low | |
| [13] | Ethics committee of the Tsushimi Hospital | Low | Low | Unclear | Low | Low |
| [14] | IRB of Cha Hospital (EKI-GLA-06-32). | Low | Low | Unclear | Low | Low |
| [15] | Ethical Committee of Kakunodate General Hospital | Low | Low | Unclear | Low | Low |
| [16] | Low | Low | Low | Low | Low | |
| [17] | Ethics Committee of Indonesia University | Low | Low | Low | Low | Low |
| [18] | Local ethics committees | Low | Low | Unclear | Low | Low |
| [19] | IRB at Tufts University-New England Medical Center NCT00183001 | Low | Low | Low | Low | Low |
| [20] | Low | Low | Unclear | Low | Low | |
| [21] | ethics committee of Osaka City University medical school | Unclear | Unclear | Unclear | Unclear | Unclear |
| [22] | Human Subjects Committee at the University of Massachusetts Amherst | Low | Low | Low | Low | Low |
| [3] | University of Wisconsin Health Sciences Human Subjects Committee | Low | Low | No | Low | Low |
| [4] | The Tayside Committee on Medical Research Ethics | Low | Low | Low | Low | Low |
| [23] | University Hospital medical ethics committee | Low | Low | Low | Low | Low |
| [24] | CT00642551 | Low | Low | Low | Low | Low |
| [25] | According to institutional guidelines | Low | Low | Unclear | Low | Low |
| [26] | Approval no. 20180726 | Low | Low | Unclear | Low | Low |
| Author | Country | Population | Primary Outcome | Intervention Type (No. of Patients) | Dose of Vit K | Follow-Up Period | Age (yrs) |
|---|---|---|---|---|---|---|---|
| [16] | Japan | Patients with rheumatoid arthritis | BMD | Group (Vit K)- 21 | 45 mg | 24 M | 61.4 ± 9.6 62.3 ± 9.0 63.4 ± 7.2 |
| Group (K+ Risedronate)—29 | |||||||
| Group (K+ Etidronate)—29 | |||||||
| Total—79 | |||||||
| [13] | Japan | Postmenopausal female | BMD | Group (Alendronate + K2)—26 | 45 mg | 12 M | 69.8 (8.7) 67.0 (6.6) |
| Group(Vit K2)—22 | |||||||
| Total—48 | |||||||
| [25] | New York | Postmenopausal female | BMD & OC | Group (Placebo)—60 | 1 mg | 3 Y | 55.1 (2.9) 55.3 (2.8) |
| Group (Mineral+ Vit D)—46 | |||||||
| Group (Mineral+ Vit D + K1)—56 | |||||||
| Total—162 | |||||||
| [14] | New York | Postmenopausal female with osteopenia | BMD OC | Group (Vit K1)—217 | 5 mg | 2 Y | 59.2 58.9 |
| Group (Placebo)—223 | |||||||
| Total—440 | |||||||
| [27] | Japan | Postmenopausal female | BMD | Group (Control)—66 | 45 mg | 2 Y | 50-75 |
| Group (Hormone replacement therapy)—66 | |||||||
| Group (Etidronate)—66 | |||||||
| Group (Calcitonin)—66 | |||||||
| Group (Alfacalcidol)—66 | |||||||
| Group (Vit K)—66 | |||||||
| Total- 396 | |||||||
| [15] | Korea | Postmenopausal female | BMD | Group (Vit K2)—38 | 15 mg | 6 M | >60 |
| Group (Control)—40 | |||||||
| Total—78 | |||||||
| [28] | Japan | Postmenopausal, female osteoporosis | Serum Uncarboxylated OC, incidence of fracture | Group (Risedronate)—51 | 45 mg | 1 Y | 75 |
| Group (Risedronate + Vit K2)—50 | |||||||
| Total—101 | |||||||
| [2] | Japan | Postmenopausal, female | BMD OC Uncarboxylated OC | Group (Vit K2)—33 | 45 mg | 48 W | 60–75 |
| Group (Control)—30 | |||||||
| Total—63 | |||||||
| [23] | Washington | Free living male and postmenopausal female | BMD OC Uncarboxylated OC | Group (Vit K)—189 | 500 µg | 3 y | 68 ± 6 |
| Group (No treatment)—190 | |||||||
| Total—379 | |||||||
| [9] | Norway | Postmenopausal female | BMD OC | Group K2(MK-7))—167 | 360 µg | 1 Y | 60 |
| Group (Placebo)—167 | |||||||
| Total—334 | |||||||
| [21] | Japan | Cirrhosis + viral hepatitis, female | BMD | Group (Vit K2)—25 | 15 mg | 2 Y | 59 ± 9 61± 8 |
| Group (Control)—25 | |||||||
| Total—50 | |||||||
| [29] | Japan | Osteoporosis, female | LBMD CF | Group Control (Calcium)—121 | 45 mg | 24 M | - |
| Group (Vit K 2)—120 | |||||||
| Total- 241 | |||||||
| [30] | Japan | Female, uterine leiomyomas/endometriosis | BMD | Group(Leuprolide acetate)—28 | 45 mg | 6 M | 46.2 ± 0.5 |
| Group (Leuprolide acetate + vit K2)—28 | |||||||
| Group (Leuprolide acetate + Rocaltrol)—26 | |||||||
| Group (Leuprolide acetate + Vit K + Rocaltrol)—28 | |||||||
| Total—110 | |||||||
| [17] | America | Pre and perimenopausal female, cirrhosis | BMD | Group (Vit K) | 600 µg | 6 M | 25–50 Y |
| Group (Placebo) | |||||||
| Total—14 | |||||||
| [31] | America | Postmenopausal female | BMD | Group (Placebo)—129 | 1 mg 15 mg | 12 M | 62.4 (0.6) 62.7 (0.7) 62.4 (0.7) |
| Group (Vit K1)—126 | |||||||
| Group (MK- 4)—126 | |||||||
| Total—381 | |||||||
| [32] | Netherland | Postmenopausal female | BMD | Group (Placebo)—164 | 45 mg | 3 Y | 66.0 ± 0.5 65.9 ± 0.4 |
| Group (Vit K2)—161 | |||||||
| Total—325 | |||||||
| [33] | Netherland | Healthy, Postmenopausal female | BMD BMC | Group (Placebo)—124 | 180 µg | 3 Y | 55–65 Y |
| Group (MK—7)—120 | |||||||
| Total—240 | |||||||
| [34] | Japan | Postmenopausal female | BMD BMC VF | Group (Control)—19 | 45 mg | 1 Y | 53.690± 84 55.991± 55 52.691± 76 53.390 ±76 |
| Group (Vit K2)—17 | |||||||
| Group (Vit D2)—16 | |||||||
| Group (Hormone Replacement Therapy)—23 | |||||||
| Total—72 | |||||||
| [35] | UK | Healthy, female | BMD | Group (Placebo)—61 | 200 µg | 2 Y | >60 |
| Group (Vit K1)—60 | |||||||
| Group (VitD3+ Ca)—62 | |||||||
| Group (VitK1+D3+ Ca)—61 | |||||||
| Total—244 | |||||||
| [3] | Nigeria | Osteoporotic female | BMD Serum OC | Group (Vit K 2)—70 | 15 mg | 6 M | 64.07 ± 9.63 |
| Group (Strontium renate)—70 | |||||||
| Group (Control)—70 | |||||||
| Total—210 |
| Outcomes | Absolute Effect | Relative Effect (95% CI) | Number of Studies | Certainty of the Evidence (GRADE) | |
|---|---|---|---|---|---|
| Without Vit K (CONTROL) | With Vit K (Vitamin K) | ||||
| BMD | 554 | 548 | RR [OR] (−0.03) to (0.2) | [5] | ⊕⊕⊕⊖ Moderate |
| Difference: 95% CI: [−0.03] to [0.2] | |||||
| Clinical Fracture | 33 Per 332 | 15 per 318 | RR [OR] (0.23) to (0.84) | [4] | ⊕⊕⊖⊖ Low |
| Difference: 95% CI: [0.23] to [0.84] | |||||
| Vertebral Fracture | 64 per 311 | 29 per 298 | RR [OR] (0.27) to (0.66) | [4] | ⊕⊕⊖⊖ Low |
| Difference: 95% CI: [0.27] to [0.66] | |||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Salma; Ahmad, S.S.; Karim, S.; Ibrahim, I.M.; Alkreathy, H.M.; Alsieni, M.; Khan, M.A. Effect of Vitamin K on Bone Mineral Density and Fracture Risk in Adults: Systematic Review and Meta-Analysis. Biomedicines 2022, 10, 1048. https://doi.org/10.3390/biomedicines10051048
Salma, Ahmad SS, Karim S, Ibrahim IM, Alkreathy HM, Alsieni M, Khan MA. Effect of Vitamin K on Bone Mineral Density and Fracture Risk in Adults: Systematic Review and Meta-Analysis. Biomedicines. 2022; 10(5):1048. https://doi.org/10.3390/biomedicines10051048
Chicago/Turabian StyleSalma, Syed Sufian Ahmad, Shahid Karim, Ibrahim M. Ibrahim, Huda M. Alkreathy, Mohammed Alsieni, and Mohammad Ahmed Khan. 2022. "Effect of Vitamin K on Bone Mineral Density and Fracture Risk in Adults: Systematic Review and Meta-Analysis" Biomedicines 10, no. 5: 1048. https://doi.org/10.3390/biomedicines10051048
APA StyleSalma, Ahmad, S. S., Karim, S., Ibrahim, I. M., Alkreathy, H. M., Alsieni, M., & Khan, M. A. (2022). Effect of Vitamin K on Bone Mineral Density and Fracture Risk in Adults: Systematic Review and Meta-Analysis. Biomedicines, 10(5), 1048. https://doi.org/10.3390/biomedicines10051048