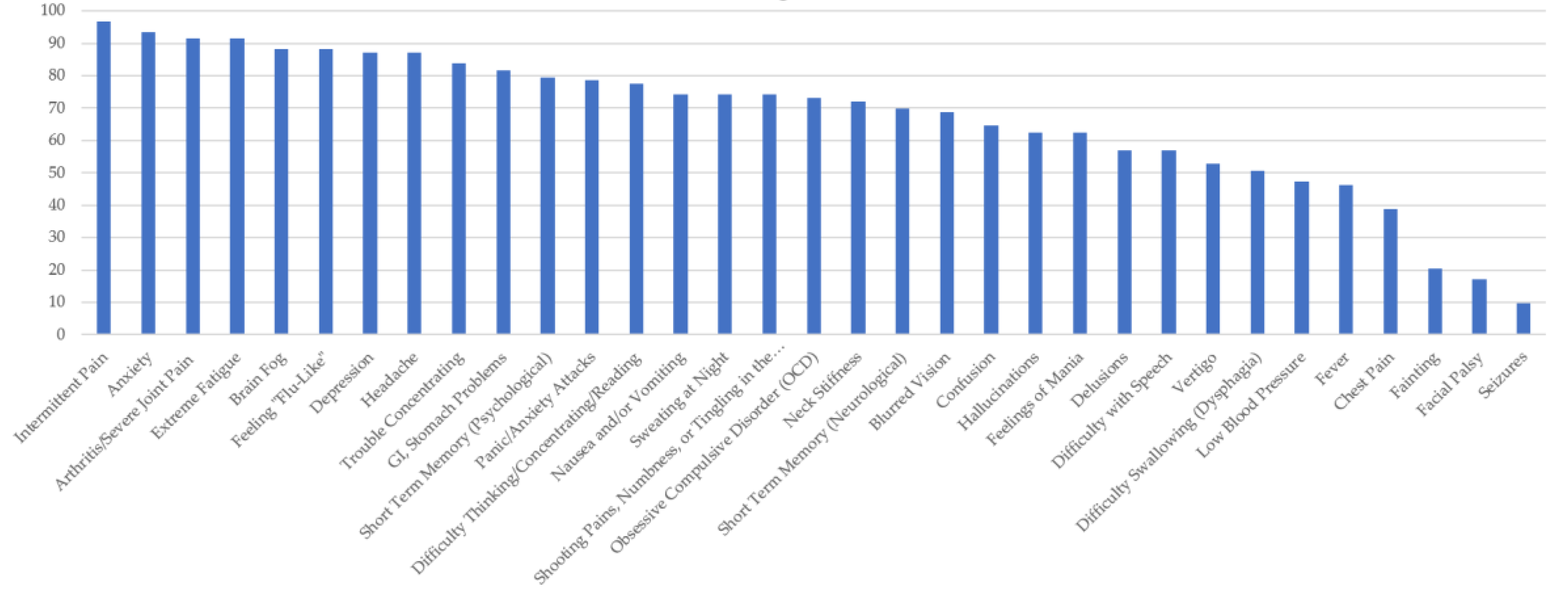
Figure 1.
Percentage of Respondents with Ehrlichiosis Reporting Specific Symptoms.
Figure 1.
Percentage of Respondents with Ehrlichiosis Reporting Specific Symptoms.
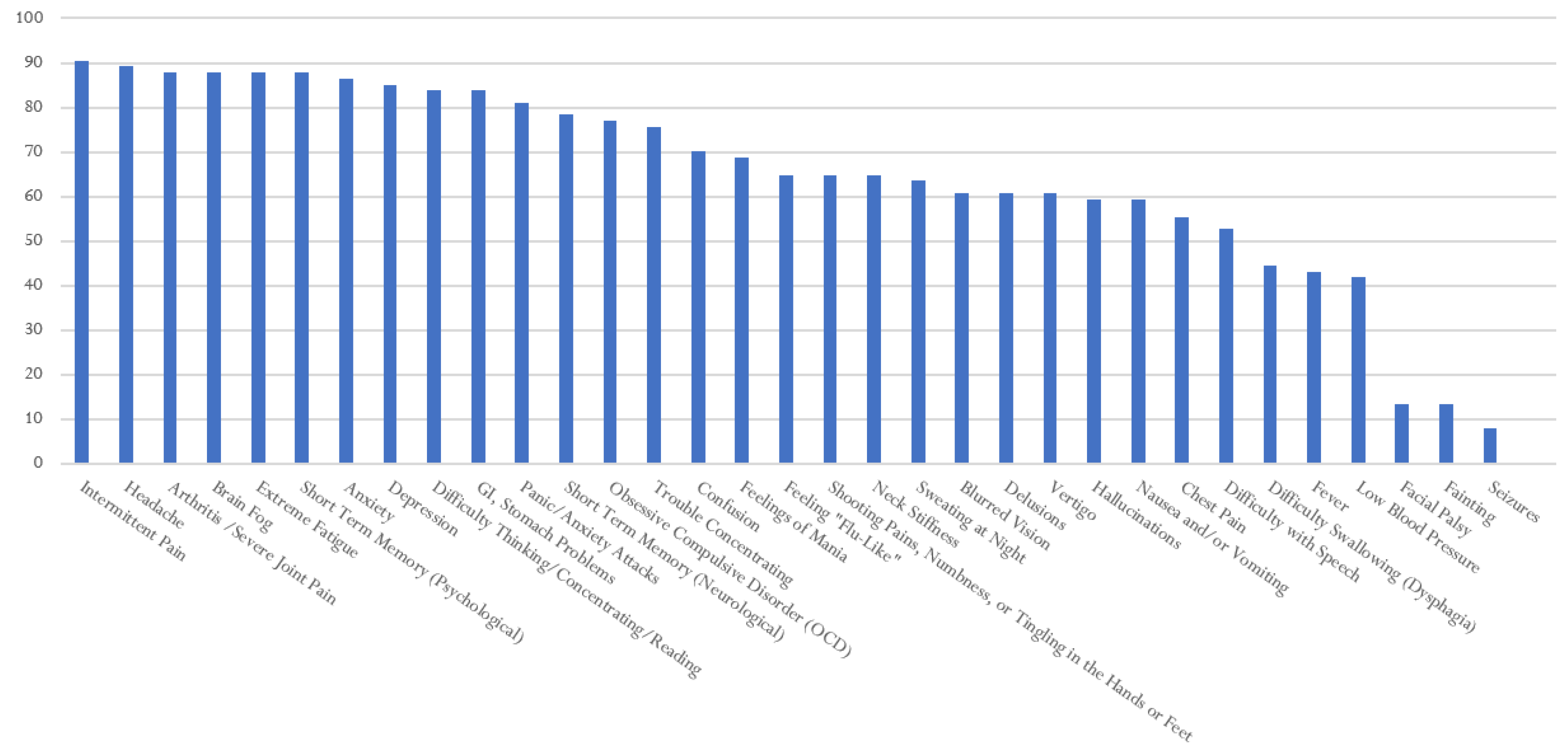
Figure 2.
Percentage of Respondents with Babesiosis Reporting Specific Symptoms.
Figure 2.
Percentage of Respondents with Babesiosis Reporting Specific Symptoms.
Figure 3.
Percentage of Respondents with Anaplasmosis Reporting Specific Symptoms.
Figure 3.
Percentage of Respondents with Anaplasmosis Reporting Specific Symptoms.
Figure 4.
Percentage of Respondents with Lyme disease Reporting Specific Symptoms.
Figure 4.
Percentage of Respondents with Lyme disease Reporting Specific Symptoms.
Figure 5.
Percentage of Respondents with RMSF Reporting Specific Symptoms.
Figure 5.
Percentage of Respondents with RMSF Reporting Specific Symptoms.
Figure 6.
Facial/Bell’s Palsy Symptom Frequency, by TBD.
Figure 6.
Facial/Bell’s Palsy Symptom Frequency, by TBD.
Table 1.
Headache is a common feature of many TBDs. It often presents with other neurological symptoms. Case reports and scholarly literature indicate headache occurs in LD, Borrelia miyamotoi disease (BMD), and Powasan Virus, among others.
Table 1.
Headache is a common feature of many TBDs. It often presents with other neurological symptoms. Case reports and scholarly literature indicate headache occurs in LD, Borrelia miyamotoi disease (BMD), and Powasan Virus, among others.
| Occurs in early stages of LD. Common with other symptoms, such as fever, myalgia (muscle pain), arthralgia (joint stiffness), fatigue, flu-like symptoms, cranial nerve palsies, neck-stiffness, and meningitis. A headache is one of the most common manifestations of LD. | [6,12,36,37] |
| RMSF can cause a severe headache that is typically accompanied by a host of symptoms, including, nausea, vomiting, extreme fatigue, fever, and pain. | [7] |
| Meningitis, and associated headaches, is a neurologic expression of early-disseminated LD. | [7,38,39] |
| A headache is a clinical presentation in the co-infection, babesiosis, which is a parasite transmitted by the same tick that transmits LD. Babesiosis causes a malaria-like illness. | [40] |
| Headaches are common among patients infected with Bartonella species, specifically B. henselae. Headaches are reported with additional neurological symptoms, including memory loss, numbness, or a loss of sensation and balance problems. | [41,42] |
| Borrelia miyamotoi disease (BMD) symptoms include the following: fever, chills, headache, myalgia, arthralgia, malaise, and fatigue. Presentation of BMD is similar to human anaplasmosis and a differential diagnosis is warranted. | [12,43] |
| In human ehrlichiosis, headaches presents with fever, malaise, myalgia, and numerous multisystem presentations. Meningoencephalitis occurs in 20% of patients. | [44,45] |
| A headache is a clinical feature of tularemia. | [46] |
| Eighty-two percent of patients with anaplasmosis reported a headache. | [47] |
| A case report of a man in his sixties with a headache and non-focal weakness showed Powassan virus disease (PVD) in a serum analysis. | [48] |
| Headaches are reported by the CDC in the following TBDs: Lyme disease, babesiosis, Borrelia miyamotoi disease (severe headache), Heartland virus, anaplasmosis, Bourbon virus disease, Rocky Mountain spotted fever (severe headache), PVD, rickettsiosis, Tick-borne relapsing fever, tularemia, Colorado tick fever, Rickettsia parkeri rickettsiosis, and ehrlichiosis. | [27] |
Table 2.
Confusion/Altered Mental Status. Altered mental status is found in patients with ehrlichiosis, LD, TBRF, and Powassan, and anaplasmosis, among others. Numerous clinical reports indicated confusion and altered mental status as symptoms of TBDs.
Table 2.
Confusion/Altered Mental Status. Altered mental status is found in patients with ehrlichiosis, LD, TBRF, and Powassan, and anaplasmosis, among others. Numerous clinical reports indicated confusion and altered mental status as symptoms of TBDs.
| Approximately 20% of patients with human monocytic ehrlichiosis (HME) present with neurological manifestations that include an altered mental status. Seizures may also be present. | [49] |
| Soldiers participating in summer exercises at Fort Chaffee, Arkansas, seroconverted to rickettsiae. Although some were asymptomatic, others presented with confusion, accompanied by dyspnea, myalgia, fever, and chills. | [44,50] |
| A case report found that an altered mental status was the sole manifestation of the central nervous system of early LD in an 84-year-old man. | [51] |
| Disorientation is a clinical manifestation of Lyme disease. | [52] |
| Confusion is a clinical feature of TBRF. | [46] |
| Confusion is a neurological symptom of anaplasmosis. | [7] |
| Confusion is noted in 20% of ehrlichiosis cases. “In a review of 21 patients,” (Ratnasamy, et al., 1996), “the most common clinical finding that predicted CSF abnormalities was a change in mental status. A total of 14 patients underwent computerized tomographic studies, and none of these studies showed abnormalities. Four (19%) of the 21 patients with CNS manifestations of ehrlichiosis and abnormal CSF findings died”. | [7,53,54] |
| An 87-year-old man, presenting with an altered mental status, tested positive for three tick-borne diseases, specifically, Powassan virus encephalitis, severe babesiosis, and Lyme disease (Lyme carditis). | [55] |
| A 74-year-old woman with an affinity for gardening “presented with one week of progressive dyspnea, cough with mucoid expectoration, and fatigue. On presentation, she was afebrile, hypotensive, and tachycardic. General examination was significant for altered mental status, dyspnea, pallor, and peripheral edema”. A peripheral blood smear revealed babesiosis. She also had titers for anaplasmosis. | [56] |
| The CDC lists confusion as an uncommon symptom of Borrelia miyamotoi disease. Altered mental status is a symptom of ehrlichiosis from all the following agents: Ehrlichia chaffeensis, Ehrlichia ewingii, and Ehrlichia muris eauclairensis; Powassan virus disease (PVD); RMSF (after five days); Tick-borne encephalitis (TBE); and babesiosis from both agents, babesiosis microti, and other babesiosis species. | [27] |
Table 3.
Pain may present as rheumatological, muscle-skeletal, or neurological. The present study asked survey respondents about pain severity in general. Below, pain is covered with a focus on neurological and also in general, including arthritis, joint, and muscle pain, which tend to present as common symptoms with other frequently occurring symptoms, such as headache and fatigue.
Table 3.
Pain may present as rheumatological, muscle-skeletal, or neurological. The present study asked survey respondents about pain severity in general. Below, pain is covered with a focus on neurological and also in general, including arthritis, joint, and muscle pain, which tend to present as common symptoms with other frequently occurring symptoms, such as headache and fatigue.
| “Neurogenic pain with radiculitis is often the starting symptom in adult patients with tick-borne Lyme neuroborreliosis and in some cases the only clinical manifestation”. | [57] |
| In all of the 41 patients with neuroborreliosis that were examined, pain presented early and was a prominent symptom. | [58] |
| In a systematic review, the authors found that arthralgias (joint pain) is “the most common form of pain associated with Lyme arthritis”. Acute nervous system involvement also involves acute pain in Lyme disease. The pain is typically neuropathic, aching, radicular, and can be worse at night. | [57,59] |
| Lyme arthritis may produce knee pain in up to 60% of cases of Lyme borreliosis in North America. | [59,60] |
| One to three weeks after a tick bite in human granulocytic anaplasmosis (HGA), patients present with fever, chills, “faintness, or generalized musculoskeletal pain with headaches and myalgia”. | [61] |
| In a systemic review, and based on 21 studies, exposed patients with LD were more likely to have the following: neck pain, myalgia, and arthralgia. These symptoms overlapped with paresthesia, sleep disorder, poor appetite, and concentration difficulties. Neck pain, myalgia, and arthralgia were the three most common overlapping symptoms among exposed patients in North America and Europe. | [62] |
| In a case report of a 16-year-old boy in Missouri who presented with fever and myalgia, he was diagnosed with ehrlichiosis. | [63] |
| Myalgias is commonly reported in cases of tularemia, following an incubation period of 3–5 days, and is accompanied by fever, malaise, and headaches, among other symptoms. | [7] |
| Lyme radiculoneuritis presents with severe and deep muscle pain, which is often asymmetric and worse at night. | [7] |
| Myalgia is common in almost every tick-borne disease, including babesiosis, RMSF, tularemia, and ehrlichiosis, according to the American Family Physician. | [64] |
| Myalgia is a clinical feature associated with the following: Anaplasma phagocytophilum, Ehrlichia chaffeensis, Ehrlichia ewingii, Lyme disease (B. burgdorferi), B. miyamotoi, Powassan virus, and Heartland virus. | [16] |
| The CDC reports the following diseases associated with pain: Babesiosis–abdominal pain; Borrelia miyamotoi disease–abdominal pain; ehrlichiosis–muscle pain; Lyme disease–migratory pain in tendons, bursae, muscle, and bones; tularemia–abdominal pain, severe throat pain, and pleuritic chest pain. | [27] |
Table 4.
Scholarship related to LD or tick-borne disease and seizures appears in individual case reports more frequently than population studies. Official recognition by the CDC of seizures in tick-borne disease are noted only in Powassan virus disease and tick-borne encephalitis virus (TBE).
Table 4.
Scholarship related to LD or tick-borne disease and seizures appears in individual case reports more frequently than population studies. Official recognition by the CDC of seizures in tick-borne disease are noted only in Powassan virus disease and tick-borne encephalitis virus (TBE).
| Progressive inflammatory reactions are related to seizure activity. In LD, a psychoimmune process is associated with psychiatric symptoms in LD patients. “Borrelia burgdorferi infections have been associated with the proinflammatory cytokines IL-6, IL-8, IL-12, IL-18 and interferon g, the chemokines CXCL12 and CXCL13 and increased levels proinflammatory lipoproteins”. | [65] |
| There was a case report of a patient presenting with Lyme cerebral vasculitis and grand mal seizures. Stroke and stroke-like syndromes can also be associated with LD. | [66] |
| Comorbidities result from immune and metabolic effects as LD progresses, leading to the gradual development of a host of neuropsychiatric symptoms. These can include seizures, depersonalization, suicide, anxiety disorders, eating disorders, depression, autism spectrum disorders, and other neuropsychiatric sequelae. | [67] |
| A previously healthy 13-year-old boy presented with seizures. Through serological testing, the patient was diagnosed with neuroborreliosis and improved with three weeks of ceftriaxone. | [68] |
| In death certificates with LD as the underlying cause of death, there was one report of a seizure disorder being the terminal event. | [69] |
| A case report of an 18-year-old male presenting with seizures and a headache had a positive serum analysis for PVD. | [48] |
| The Centers for Disease Control and Prevention recognize seizures as a symptom in PVD and tick-borne encephalitis virus. | [27] |
Table 5.
Vertigo and/or dizziness may not be fully recognized as a TBD symptom. Medical literature and case reports demonstrate that vertigo is present in cases of LD and TBRF.
Table 5.
Vertigo and/or dizziness may not be fully recognized as a TBD symptom. Medical literature and case reports demonstrate that vertigo is present in cases of LD and TBRF.
| Can present as the sole symptom in later stage or chronic LD. | [70] |
| In a study of 38 patients with confirmed LD, vertigo was found to be a symptom of LD. LD can result in labyrinthitis and hearing-organ damage. | [71] |
| A study of 266 LD patients presented most commonly with headaches, a stiff neck, and dizziness. | [72] |
| In a study of 73 patients, “Borrelia infection is an etiological factor which should be considered in patients suffering from vertigo especially if positional nystagmus is present”. | [73] |
| As LD progresses to the second stage, the primary symptoms become malaise, fever and chills, headache, myalgias, arthralgias, and dizziness. | [74] |
| Dizziness, often accompanied by confusion, is a clinical manifestation of TBRF. | [46] |
| According to the CDC, vertigo is uncommon and only present with Borrelia miyamotoi. | [27] |
Table 6.
Tingling and numbness tend to occur in the extremities and are associated with LD in case reports.
Table 6.
Tingling and numbness tend to occur in the extremities and are associated with LD in case reports.
| A 72-year-old man, with a history of a bite two weeks earlier, presented with numbness and tingling. He tested positive for Borrelia burgdorferi, via a western blot and enzyme-linked immunosorbent assay. The patient was diagnosed with transverse myelitis from Lyme disease and babesiosis. | [75] |
| As LD progresses, patients can present with a combination of neurological symptoms. These can include the following: memory loss; inability to concentrate; and muscle weakness, with tingling and numbness in the arms and legs. | [76] |
| Tingling, numbness, and pain, particularly on the extremities, are common features of LD, particularly in the second and third stages. | [77,78] |
| A case report of a 31-year-old man with a dual diagnosis of Lyme and Guillain–Barre syndrome (GBS), presented with progressive numbness in his hands and feet. The symptoms resolved with intravenous immunoglobulin and parenteral ceftriaxone. | [79] |
| The Centers for Disease Control and Prevention does not list tingling or numbness as symptoms of LD or any TBD in the annual report. | [27] |
Table 7.
Cognitive function (concentration, word finding, and memory difficulty)–limited literature is available regarding cognitive function among TBD patients in the United States. Concentration tends to be related to Tick-borne encephalitis, which is endemic in Europe and Asia. The following studies are reported from the US.
Table 7.
Cognitive function (concentration, word finding, and memory difficulty)–limited literature is available regarding cognitive function among TBD patients in the United States. Concentration tends to be related to Tick-borne encephalitis, which is endemic in Europe and Asia. The following studies are reported from the US.
| An inability to concentrate develops with Lyme disease’s progression and is accompanied by other neurological symptoms. | [76] |
| Short-term memory deficits progress with LD and are accompanied by other neurological symptoms, such as tingling and numbness. | [76] |
| In a systematic review of exposed patients in North America and Europe, the symptoms of those with North American strains of Lyme disease were more cognitive-related, with 10–20% of these patients experiencing cognitive symptoms and fatigue more than six months after antibiotic treatment. | [62] |
| “Up to 46% of patients [with TBD] are left with permanent sequelae at long-time follow-up, the most commonly reported residuals being various cognitive or neuropsychiatric complaints, balance disorders, headache, dysphasia, hearing defects, and spinal paralysis”. | [80] |
| The Centers for Disease Control does not list concentration or memory as symptoms of LD or any TBD. | [27] |
Table 8.
Paralysis: difficulty swallowing (dysphagia) and Bell’s palsy. This exploratory study was designed to capture different sources of information and assess the possible disconnect among them, with respect to patient symptoms. Dysphagia is one symptom with which medical providers may not be familiar, but self-reports or case reports in the medical literature might suggest that the symptom may require further exploration. Unlike dysphagia, Bell’s palsy is recognized by official public health sources and is suggested as a recognized symptom of LD in approximately eight percent of cases [
81].
Table 8.
Paralysis: difficulty swallowing (dysphagia) and Bell’s palsy. This exploratory study was designed to capture different sources of information and assess the possible disconnect among them, with respect to patient symptoms. Dysphagia is one symptom with which medical providers may not be familiar, but self-reports or case reports in the medical literature might suggest that the symptom may require further exploration. Unlike dysphagia, Bell’s palsy is recognized by official public health sources and is suggested as a recognized symptom of LD in approximately eight percent of cases [
81].
| In a case report of an 87-year-old hunter with Lyme neuroborreliosis (LNB), dysphagia occurred as a consequence of facial weakness. The patient’s dysphagia and other symptoms improved with intravenous ceftriaxone after two weeks. The patient was readmitted with a cough and dyspnea. This case suggests that acute respiratory failure can develop from diaphragmatic paralysis. | [33] |
| North American tick paralysis (TP) can present with cranial nerve, which may include drooling, dysphagia, and facial weakness. | [82] |
| Neuroborreliosis includes multiple neurological symptoms, including dysphagia. In a case report of a 76-year-old woman with LB, the woman received two weeks of IV Ceftriaxone. Her confusion improved rapidly, while her dysphagia gradually improved. | [83] |
| Five hundred and fifty-nine patients presented with facial palsy in a Netherlands hospital-based study and 4.7% (26) of them had LNB. Of these, over 70% of LBN patients with facial palsy did not report a tick bite or rash. LNB patients with facial palsy were more likely to occur in the summer months. LBN patients with facial palsy presented more often with headaches, than non-LBN-palsy patients. | [84] |
| Bell’s palsy can be bilateral and is the most common LD neurological symptom in children. Intermittent and continuing arthritis, and, less often, encephalopathy or neuropathy are also common. | [16] |
| Kim et al. (2012), reported a case of a “32-year-old man with rapidly progressive bilateral ptosis, dysphagia, spastic paraparesis, and voiding difficulty in whom Lyme disease was diagnosed through serologic tests for antibodies and Western blot testing”. | [85] |
| In LD, the peripheral nervous system is typically affected more than the CNS, this includes Bell’s palsy. | [7] |
| A patient presented with Bell’s palsy, in addition to numerous other symptoms, including altered mental status and multisystem organ involvement. The patient was found to have ehrlichiosis. | [86] |
| The CDC reports facial palsy in the following: TBRF, but notes it is very rare; and Bell’s palsy and other cranial neuropathy are noted as LD symptoms. The CDC does not report dysphagia as a symptom of any TBD. | [27] |
Table 9.
Difficulty with, or slurred speech (dysarthria). Dysarthria is a neurological manifestation of a number of tick-borne diseases. Numerous case reports link difficulty with speech or slurred speech to anaplasmosis, LD, and PVD. The CDC does not report dysarthria as a symptom of any TBD, indicating more research is needed with this neurological manifestation.
Table 9.
Difficulty with, or slurred speech (dysarthria). Dysarthria is a neurological manifestation of a number of tick-borne diseases. Numerous case reports link difficulty with speech or slurred speech to anaplasmosis, LD, and PVD. The CDC does not report dysarthria as a symptom of any TBD, indicating more research is needed with this neurological manifestation.
| A 63-year-old woman presented with the following: dysarthria (slurred speech), fever, confusion, and new-onset thrombocytopenia, two weeks after a tick bite. She was diagnosed with human granulocytic anaplasmosis (HGA). | [87] |
| A 63-year-old male presented with fever, dysarthria, and dysphagia after receiving multiple tick bites on a recent vacation. Symptoms were accompanied by the following: lymphopenia and thrombocytopenia. Laboratory findings concluded that the patient had human granulocytic anaplasmosis (HGA). | [88] |
| Dysarthria occurs in acute illness, among short- and long-term survivors, and among hospitalized patients with Powassan virus disease (PVD). The incubation period for PVD is 1–4 weeks. | [89,90] |
| Sequelae in PVD survivors occurs with mutism, and in the long-term, with anarthria (a severe form of dysarthria) and aphasia (loss of ability to understand or express speech). | [91,92,93] |
| Apnea and psychoses present with dysarthria, as short-term neurological sequelae with PVD. Seventy-five percent of PVD cases include significant neurological complications. | [89] |
| Dysarthria was the only consequence of neuroborreliosis in a case report of a 65-year-old man. | [94] |
| Case reports of dysarthria are found in rickettsial infections of granulocytes. Human granulocytic anaplasmosis (HGA) is caused by the intracellular bacterium, Anaplasma phagocytophilum. | [88,95] |
| A 46-year-old man was admitted to hospital with dizziness, fever, and trouble walking. The symptoms developed four months after visiting an endemic area. The patient was diagnosed with Lyme neuroborreliosis and, when examined, had dysarthria, ataxia (uncoordinated movements), and hemianopsia (blindness in half of his vision). | [96] |
| In a study of 30 LD patients with LD or “Lyme-like” disease in Brazil, dysarthria occurred in 6.7%. | [97] |
| A 66-year-old woman presented to the hospital with slurred speech, lethargy, and ataxia (loss of coordination). She was confirmed to have Ehrlichia chaffeensis. | [49] |
| The Mayo Clinic lists dysarthria as a symptom of LD, but not in relation to other TBDs. The National Organization for Rare Diseases (NORD) reports dysarthria in Rocky Mountain spotted fever (RMSF). | [98,99] |
| The CDC does not report difficulty with speech or slurred speech, or dysarthria as symptoms associated with Lyme disease or other TBDs. | [99] |
Table 10.
Low blood pressure (hypotension). Hypotension is associated with autonomic nervous system dysfunction and is demonstrated primarily with ehrlichiosis in the case reports. The National Organization for Rare Diseases (NORD) recognizes hypotension with ehrlichiosis and RMSF, but the CDC does not link this symptom to any TBD.
Table 10.
Low blood pressure (hypotension). Hypotension is associated with autonomic nervous system dysfunction and is demonstrated primarily with ehrlichiosis in the case reports. The National Organization for Rare Diseases (NORD) recognizes hypotension with ehrlichiosis and RMSF, but the CDC does not link this symptom to any TBD.
| A patient presented with life-threatening hypotension from babesiosis hemolysis. | [100] |
| Chronic babesiosis includes life-altering symptoms similar to malaria, including hypotension and headaches. | [101] |
| Profound hypotension is associated with human monocytotropic ehrlichiosis (HME), caused by the bacterium Ehrlichia chaffeensis. It is also associated with human granulocytotropic anaplasmosis (HGA), caused by A. phagocytophilum. | [102,103] |
| There was a case study of a 52-year-old man who had been hiking in Georgia and was bitten by a tick, who then presented to the ER with a fever and low blood pressure. He tested positive for HME. A similar case occurred with a man from Tennessee, who presented with a fever and low blood pressure. He also tested positive for HME. | [104] |
| TBRF can lead to hypotension. | [46] |
| Low blood pressure (hypotension) is reported with human monocytic ehrlichiosis (HME) and RMSF by NORD. | [99] |
| Low blood pressure is reported as a complication of babesiosis by the CDC. | [27] |
Table 11.
Fainting (syncope). Syncope has been reported with Lyme disease and other tick-borne diseases. Although syncope, generally, may be associated with neurological conditions, it may have cardiovascular etiologies. In the TBD case reports, fainting tended to be associated with Lyme carditis, rather than neurological origins.
Table 11.
Fainting (syncope). Syncope has been reported with Lyme disease and other tick-borne diseases. Although syncope, generally, may be associated with neurological conditions, it may have cardiovascular etiologies. In the TBD case reports, fainting tended to be associated with Lyme carditis, rather than neurological origins.
| There was a case report in which a 55-year-old man was admitted to the hospital with flu-like symptoms, shortness of breath, near syncope, and bradycardia of 20–30 beats per minute. He had exposure to tick bites and tested positive for LD. He was diagnosed with Lyme carditis. “Considering Lyme carditis as a differential diagnosis in patients with an AV block of an unknown etiology can result in a timely diagnosis and treatment of Lyme carditis”. | [105] |
| “Clinical manifestations include syncope, light-headedness, fainting, shortness of breath, palpitations, and/or chest pain. Atrioventricular (AV) electrical block of varying severity presents the most common conduction disorder in Lyme carditis”. | [106] |
| There was a case report of a 20-year-old male who presented to an outpatient physician’s office after a five-minute episode of syncope. The patient had a rash and was an avid outdoorsman. He was found to have persistent bradycardia, a complete heart block, and Lyme carditis. Lyme disease was confirmed via two-tier testing. | [107] |
| A 53-year-old man from Delaware suffered from recurrent syncope and fevers, and thrombocytopenia and macroscopic hematuria. He was diagnosed and treated for Babesiosis with antibiotics and atovaquone, with his symptoms resolving within 48 h. | [108] |
| Five women, aged 22–44, had a history of LD, but were successfully treated with antibiotics. They later “developed symptoms of fatigue, cognitive dysfunction, orthostatic palpitations and either near syncope or frank syncope”. All were diagnosed with postural orthostatic tachycardia syndrome (POTS). | [109] |
| Three patients with Lyme borreliosis, who were previously healthy, developed syncope abruptly. All three also had an atrioventricular (AV) heart block. | [110] |
| Syncope, chest pain, and dyspnea occur in LD patients within 2–4 weeks of infection, but symptoms can take up to seven months to appear. | [16] |
| Syncope is not reported by the CDC as a symptom of any TBD. | [27] |
Table 12.
Depression is found in many patients with LD and is noted by a state-level public health report as a clinical feature of babesiosis.
Table 12.
Depression is found in many patients with LD and is noted by a state-level public health report as a clinical feature of babesiosis.
| In a study of post-treatment LD syndrome patients (PTLD) compared to health controls, those with PTLD were significantly more likely to have depression, using the Beck Depression Inventory-II scale. | [113] |
| Seventy-seven percent of LD patients reported having depression. | [114] |
| Depression is the most common symptom in LD patients, with psychiatric sequelae ranging from 22% to 66%. | [115,116] |
| The Michigan and New York State governments list depression as a clinical feature of babesiosis in their reference literature on emerging infectious diseases for healthcare providers. | [117] |
| In a study of patients with late-stage Lyme borrelia, “a significantly higher percentage of depressive disorders was...noted in the group of males and females with neuroborreliosis [in comparison to those with Lyme arthritis]”. | [118] |
| In a study of the self-reported symptoms of those diagnosed with LD, the most frequently noted symptoms were as follows: depression, extreme fatigue, headaches, neck and back pain, brain fog, and anxiety. | [3] |
| The CDC lists depression as uncommon, but possible in babesiosis. The CDC does not include depression as a symptom linked to any other TBD. | [27] |
Table 13.
Anxiety is not well studied in the medical literature as a symptom of TBDs, but is shown to be present with LD. TBRF is also associated with anxiety.
Table 13.
Anxiety is not well studied in the medical literature as a symptom of TBDs, but is shown to be present with LD. TBRF is also associated with anxiety.
| Sixty-seven percent of LD patients report having anxiety. | [114] |
| Neurological psychiatric symptoms develop gradually in patients with Lyme borreliosis (LB) and include anxiety disorders, such as panic disorders, social anxiety, general anxiety, and other anxiety disorders. | [67,119] |
| Anxiety is a clinical feature of bartonella, which is often recognized as a co-infection of Lyme disease. | [120] |
| TBRF can produce psychiatric symptoms, including anxiety, and patients should be monitored for anxiety during treatment. | [46] |
| “A higher level of risk to self and others is associated with multiple symptoms developing after acquiring [Lyme and Associated Diseases] LAD, in particular, explosive anger, intrusive images, sudden mood swings, paranoia, dissociative episodes, hallucinations, disinhibition, panic disorder, rapid cycling bipolar, depersonalization, social anxiety disorder, substance abuse, hypervigilance, generalized anxiety disorder, genital-urinary symptoms, chronic pain, anhedonia, depression, low frustration tolerance, and posttraumatic stress disorder”. | [121] |
| The CDC does not recognize anxiety as a symptom of any tick-borne disease. | [27] |
Table 14.
Fatigue and malaise. Fatigue (i.e., extreme tiredness) or malaise (i.e., lack of wellbeing) are often reported in the literature as primarily clinical features of Lyme and other tick-borne diseases, particularly in cases of human monocytic ehrlichiosis (HME). Although ample evidence supports fatigue and malaise as symptoms of LD, scholarly literature is burdened with debates regarding chronic LD or post-treatment Lyme disease syndrome (PTLDS). The findings, below, focus on the earlier stages of LD and other tick-borne diseases.
Table 14.
Fatigue and malaise. Fatigue (i.e., extreme tiredness) or malaise (i.e., lack of wellbeing) are often reported in the literature as primarily clinical features of Lyme and other tick-borne diseases, particularly in cases of human monocytic ehrlichiosis (HME). Although ample evidence supports fatigue and malaise as symptoms of LD, scholarly literature is burdened with debates regarding chronic LD or post-treatment Lyme disease syndrome (PTLDS). The findings, below, focus on the earlier stages of LD and other tick-borne diseases.
| Fatigue is a clinical presentation of Lyme disease, Bourbon virus (BRB), and Heartland virus. | [16] |
| The majority of Lyme disease patients in the United States develop fatigue, which typically presents with headaches, an EM rash, a mildly stiff neck, and arthralgia or myalgia. | [122] |
| In a study of Pennsylvania’s health records, Lyme disease was found to be more prevalent than surveillance data, with “20.8% (n = 735) of cases with a diagnosis code and treatment had a diagnosis of malaise or fatigue, pain, or cognitive difficulties not present in the past 26 weeks”, specifically within 4–52 weeks following their Lyme disease diagnosis. There was “no prior evidence of chronic fatigue, fibromyalgia, or chronic pain based on diagnosis codes linked to encounters, medication orders, or problem lists”. | [123] |
| A 55-year-old man presented with AV block, fatigue, malaise, and flu-like symptoms. The case report concluded that “Lyme carditis [should be considered] as a differential diagnosis in patients with an AV block”. | [105] |
| An EM rash is often accompanied by the following clinical features: fever, malaise, headache, myalgia or arthralgia, regional lymphadenopathy, and a stiff neck. | [124] |
| In a prospective, double-blind study of 1156 males who had positive Borrelia antibodies, the authors found the following: “Seropositive subjects who had never suffered from clinically manifest Lyme borreliosis or neuroborreliosis showed significantly more often chronic fatigue (p = 0.02) and malaise (p = 0.01) than seronegative recruits”. They concluded as follows: “It is worth examining whether an antibiotic therapy should be considered in patients with chronic fatigue syndrome and positive Borrelia serology”. | [125] |
| Malaise is a common clinical presentation, typically with headaches, in ehrlichiosis. | [126] |
| In a population study of confirmed human granulocytic ehrlichiosis (HGE) cases, malaise, with fever, headaches, and myalgia, were the most common symptoms. | [127] |
| “The hallmarks of symptomatic human monocytic ehrlichiosis (HME) include fever, headache, myalgia, nausea, malaise, transaminitis, and blood cell abnormalities”. Two cases presented with the additional symptom of sudden sensorineural hearing loss. | [128] |
| Fatigue is a classic presentation in anaplasmosis, with other non-specific influenza-like symptoms, such as fever, fatigue, muscle aches, and headaches. | [129,130] |
| Babesiosis presents with typical clinical symptoms that include the following: fever, fatigue, malaise, weakness, chills, sweats, and headaches. | [131] |
| The CDC reports fatigue as present in the following TBDs: Borrelia miyamotoi, babesiosis, Colorado tick fever, Heartland virus disease, and tularemia. Malaise is reported in the following: RMSF, anaplasmosis, tularemia, babesiosis, ehrlichiosis, and Lyme disease, with malaise as “flu-like symptoms” accompanied by headaches, fever, myalgia, and arthralgia. | [27] |
Table 15.
Mania, panic attacks, delusions, or hallucinations. Tick-borne illnesses are noted by patients and advocacy organizations to cause psychiatric symptoms similar to bi-polar and schizophrenia, reportedly leading to unnecessary institutionalization and/or misdiagnosis. Official sources of information are lacking on these psychiatric manifestations, which may delay diagnosis, as medical providers are not informed via the public health system. Mania, panic attacks, hallucinations, and delusions have been combined in this section to cover the overlapping presence of the three clinical manifestations in the scholarly literature.
Table 15.
Mania, panic attacks, delusions, or hallucinations. Tick-borne illnesses are noted by patients and advocacy organizations to cause psychiatric symptoms similar to bi-polar and schizophrenia, reportedly leading to unnecessary institutionalization and/or misdiagnosis. Official sources of information are lacking on these psychiatric manifestations, which may delay diagnosis, as medical providers are not informed via the public health system. Mania, panic attacks, hallucinations, and delusions have been combined in this section to cover the overlapping presence of the three clinical manifestations in the scholarly literature.
| In a case report of a previously healthy 35-year-old woman, with no prior history of psychiatric disorders and no family history of mania, months of psychiatric symptoms developed after she refused continued treatment for LD. The woman had a presumed EM rash and lived in a Lyme-endemic area. Additional symptoms included severe fatigue, headaches, and an irritable mood. Her mania overlapped with auditory hallucinations and paranoid delusions. Episodes continued until she ultimately agreed to treatment with IV antibiotics, which resulted in an improvement in all the symptoms. | [132] |
| A 64-year-old woman was admitted to a psychiatric hospital with visual hallucinations. She also developed neurological symptoms and had an abnormal EEG. A lumbar puncture showed LB. She had a history of tick bites, and her husband had experienced similar symptoms. Medications for psychosis failed to help her improve. | [133] |
| A seven-year-old boy presented with Alice in Wonderland syndrome, with distorted perceptions of shapes and sizes, and he also had auditory hallucinations. His Lyme serology was positive in both the serum and cerebrospinal fluid. His symptoms dissipated after three weeks of intravenous ceftriaxone. | [134] |
| Musical hallucinations occurred in two female patients with neurologic Lyme disease. The case reports suggest the following: “Patients with musical hallucinations of unknown cause should be tested for infection with the Lyme disease spirochete”. | [135] |
| A patient presented with “no neurological signs but marked psychiatric symptoms induced by borrelia burgdorferi, whose clinical picture was indistinguishable from an endogenous schizophrenia…The case demonstrated the aetiologic nonspecificity of paranoid symptoms and hallucinations and emphasizes that in psychotic patients without psychiatric history additional diagnostic measures should be performed”. | [136] |
| Three patients with panic-like episodes were also described and were found to have tick-borne diseases. “Each woman experienced symptoms that are not usual in panic disorder but are typical of neurological Lyme disease, including exquisite sensitivity to light, touch, and sounds, joint pain often in combination with cognitive changes including mental fogginess and loss of recent memory, and some degree of bizarre, shifting, and often excruciating neurological pain”. | [137] |
| The CDC does not report mania, panic attacks, delusions, or hallucinations as symptoms or sequalae of any TBD. | [27] |
Table 16.
CDC Tickborne Diseases of the United States: A Reference Manual for Healthcare Providers (2018). Summary of all TBD Symptoms.
Table 16.
CDC Tickborne Diseases of the United States: A Reference Manual for Healthcare Providers (2018). Summary of all TBD Symptoms.
| Symptom | LD | Ehrlichiosis | Babesiosis | Anaplasmosis | CTF | RMSF | BMD | HVD | PVD | R Parkeri | TBRF | Tularemia |
|---|
| Rash | • | in children | | uncommon | • | • | uncommon | | | • | | |
| Fever/Chills | • | • | • | • | • | high | • | • | • | • | • | • |
| Fatigue | • | • | • | • | • | | • | • | • | | | • |
| Malaise | • | • | • | • | | • | | | | | | • |
| Headache | • | • | • | severe | • | severe | severe | • | • | • | • | • |
| Myalgia | • | • | • | • | • | • | • | • | | • | • | • |
| Nausea/Vomiting | | • | • | • | | • | uncommon | • | • | | • | • |
| Shakes/Rigors | | | | • | | | | | | | | |
| Diarrhea | | • | | • | | | uncommon | • | | | | • |
| Anorexia | • | • | • | | • | uncommon | | | | | • | |
| Arthralgia | • | | • | | | | • | • | | | • | • |
| Dark urine | | | • | | | | • | | | | | |
| Confusion | | | | | | | • | | | | | |
| Vertigo/Dizziness | | | | | | | uncommon | | | | | |
| Dyspnea | | | | | | | uncommon | | | | | |
| Pharyngeal erythema | • | | | | • | | | | | | | |
| Lymphadenopathy | • | | | | • | | | | | | | • |
| Altered mental status | | • | • | | • | • | | | • | | | |
| Decreased appetite | | | | | | | | •• | | | | |
| Baker’s cyst | • | | | | | | | | | | | |
| Conduction abnormalities | • | | | | | | | | | | | |
| Myocarditis/Pericarditis | • | | | | | | | | | | | |
| Bell’s palsy or other cranial neuropathy | • | • | • | | • | | | | • | | • | |
| Meningitis | • | | | | | | | | • | | | |
Motor and sensory radiculoneuropathy, and
mononeuritis multiplex | • | | | | | | | | | | | |
| Subtle cognitive difficulties | • | | | | | | | | | | | |
| Encephalitis, encephalomyelitis, subtle | • | | | | | | | | • | | | |
| encephalopathy, and pseudotumor cerebri (all rare) | • | | | | | | | | | | | |
| Paresis | | | | | | | | | • | | | |
| Seizures | | | | | | | | | • | | | |
| Aphasia (loss of speech) | | | | | | | | | | | | |
| Multi-organ system damage | | | | | | • | | | | | | |
Table 17.
Symptom comparison from medical literature and the public health reference manual for common TBDs.
Table 17.
Symptom comparison from medical literature and the public health reference manual for common TBDs.
| Symptom | Reported in Scientific and Medical
Literature | Reported by the Centers for Disease
Control | Reported in the Scientific Literature, but Not
Recognized by the CDC |
|---|
| Headache | LD, BVD, babesiosis, ehrlichiosis, tularemia, anaplasmosis, RMSF, and PVD | LD, ehrlichiosis, babesiosis, anaplasmosis, RMSF BMD, PVD, and tularemia | None, headache is the most common presenting neurological symptom among all TBDs |
| Confusion/Altered Mental Status | LD, babesiosis, ehrlichiosis, anaplasmosis, and PVD | Confusion: BMD
Altered mental status: ehrlichiosis, babesiosis, RMSF, and PVD | LD
anaplasmosis |
| Pain | LD, babesiosis, ehrlichiosis, anaplasmosis, tularemia, RMSF, and PVD | LD, Babesiosis, ehrlichiosis, anaplasmosis, tularemia, RMSF, and PVD | PVD |
| Seizures | LD, RMSF | PVD | LD
RMSF |
| Vertigo/Dizziness | LD, RMSF | None | LD
RMSF |
| Tingling/Numbness | LD | None | LD |
| Cognitive Function (concentration, memory difficulty, and word recall) | LD | None | LD |
| Paralysis: difficulty swallowing (dysphagia) or Bell’s palsy | Bell’s palsy: LD, ehrlichiosis,
and dysphagia: LD | Bell’s Palsy: LD, ehrlichiosis, babesiosis,
and dysphagia: none | Dysphagia: LD |
| Difficulty with, or slurred speech (Dysarthria) | LD, anaplasmosis, ehrlichiosis, PVD, and RMSF | None | LD, anaplasmosis, ehrlichiosis, PVD, RMSF |
| Low Blood Pressure (hypotension) | babesiosis, ehrlichiosis, and anaplasmosis (also present in TBRF) | Babesiosis | Ehrlichiosis, anaplasmosis, and TBRF |
| Fainting (syncope) | LD, babesiosis | None | LD, babesiosis |
| Depression | LD, babesiosis | Babesiosis, but uncommon | LD |
| Anxiety | LD (also present in TBRF) | None | LD |
| Fatigue and malaise | LD, ehrlichiosis, anaplasmosis, and babesiosis | LD, Ehrlichiosis, anaplasmosis, babesiosis, and tularemia (and other TBDs) | None, fatigue and malaise are commonly agreed upon as classic symptoms of TBDs |
| Mania, panic attacks, delusions, or hallucinations | LD | None | LD |
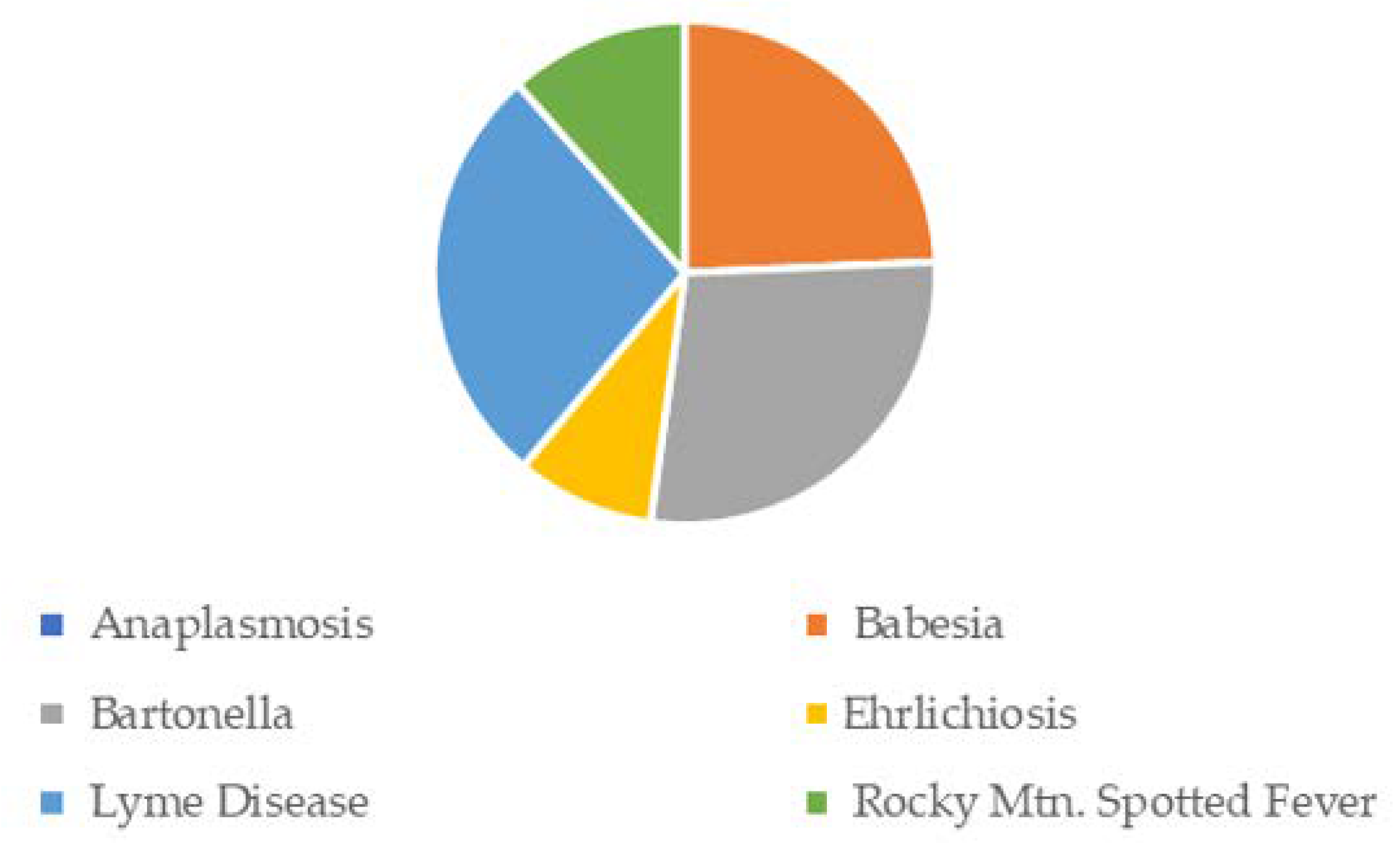
Table 18.
Respondent Characteristics by Diagnostic Category. Summary statistics for the number of respondents, and their age and sex, who reported a tick-borne disease are provided for each disease (i.e., by diagnostic category).
Table 18.
Respondent Characteristics by Diagnostic Category. Summary statistics for the number of respondents, and their age and sex, who reported a tick-borne disease are provided for each disease (i.e., by diagnostic category).
| Diagnostic Cohort | Has Diagnosis | Age | Female |
|---|
| Statistics Presented | n (% of Analytical Cohort) | Mean (Standard Deviation) | Median (Inter-Quartile Range) [Minimum–Maximum] | n (% of Diagnostic Cohort) (% of Analytical Cohort) |
|---|
| Anaplasmosis | 7 (4.73%) | 48.14 (13.85) | 44 (31) [34–68] | 5 (71.43%) [3.38%] |
| Babesiosis | 22 (14.86%) | 40.09 (16.27) | 44 (20) [9–67] | 17 (77.27%) [11.49%] |
| Bartonella | 23 (15.54%) | 42.17 (14.91) | 44 (22) [9–67] | 20 (86.96%) [13.51%] |
| Ehrlichiosis | 12 (8.11%) | 43.92 (18.70) | 48.5 (21.5) [9–69] | 9 (75%) [6.08%] |
| Lyme Disease | 43 (29.05%) | 45.58 (15.87) | 45 (25) [9–79] | 39 (90.7%) [26.35%] |
| Rocky Mountain Spotted Fever | 37 (25.00%) | 51.46 (12.84) | 54 (21) [25–73] | 31 (83.78%) [20.95%] |










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}