
Perioperative Considerations for the Surgical Treatment of Crohn’s Disease with Discussion on Surgical Antibiotics Practices and Impact on the Gut Microbiome


{kind=link}
{kind=link}
{kind=link}
Abstract
1. Introduction: Incidence, Etiology, Overview of Surgical Management, and Aims of This Paper
2. Materials and Methods
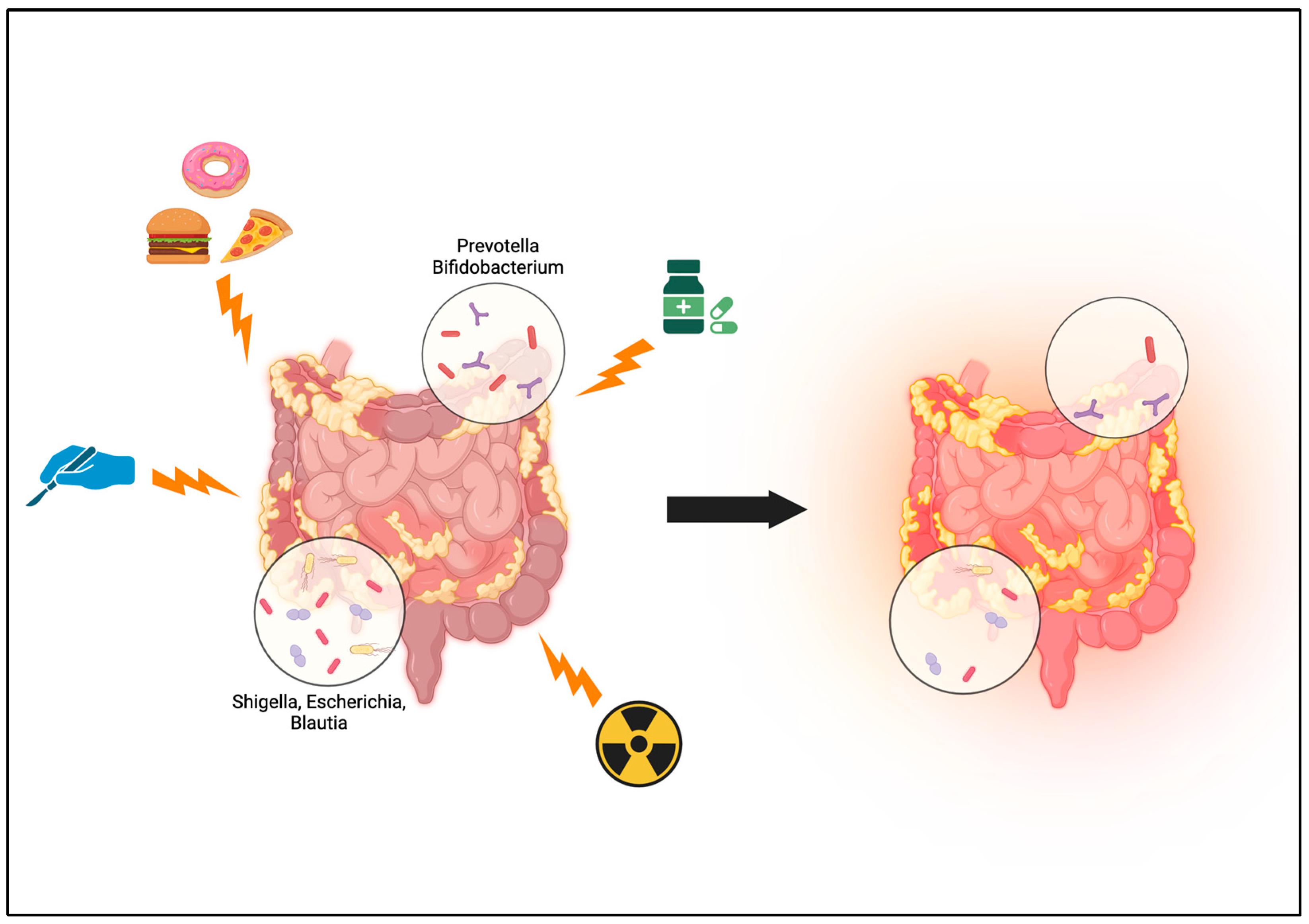
3. Overview of the Microbiome in Crohn’s Disease
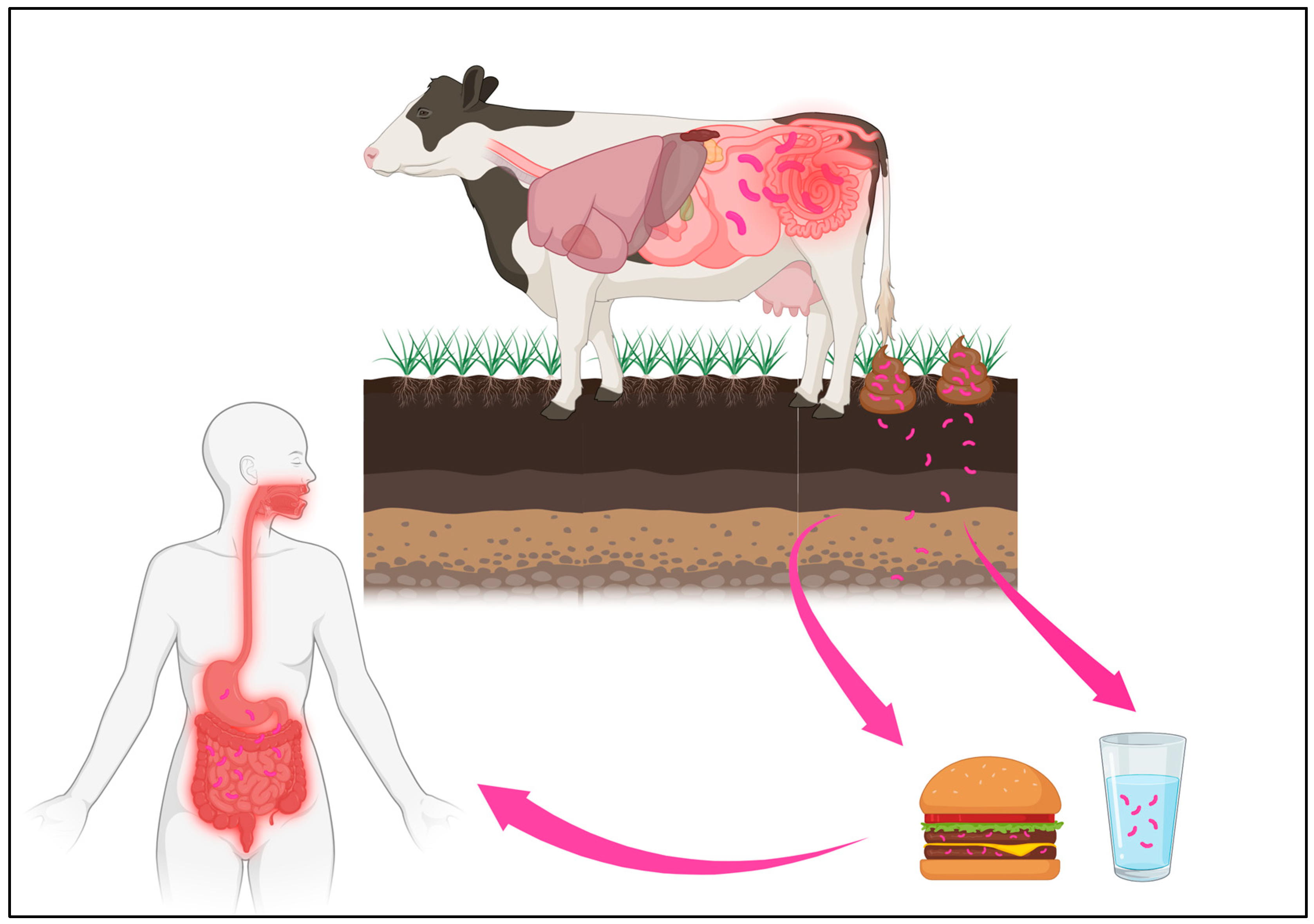
4. Mycobacterium avium paratuberculosis
5. Perioperative Optimization
5.1. Nutrition
5.2. Hydration
5.3. Smoking Cessation
5.4. Psychological Health and Stress
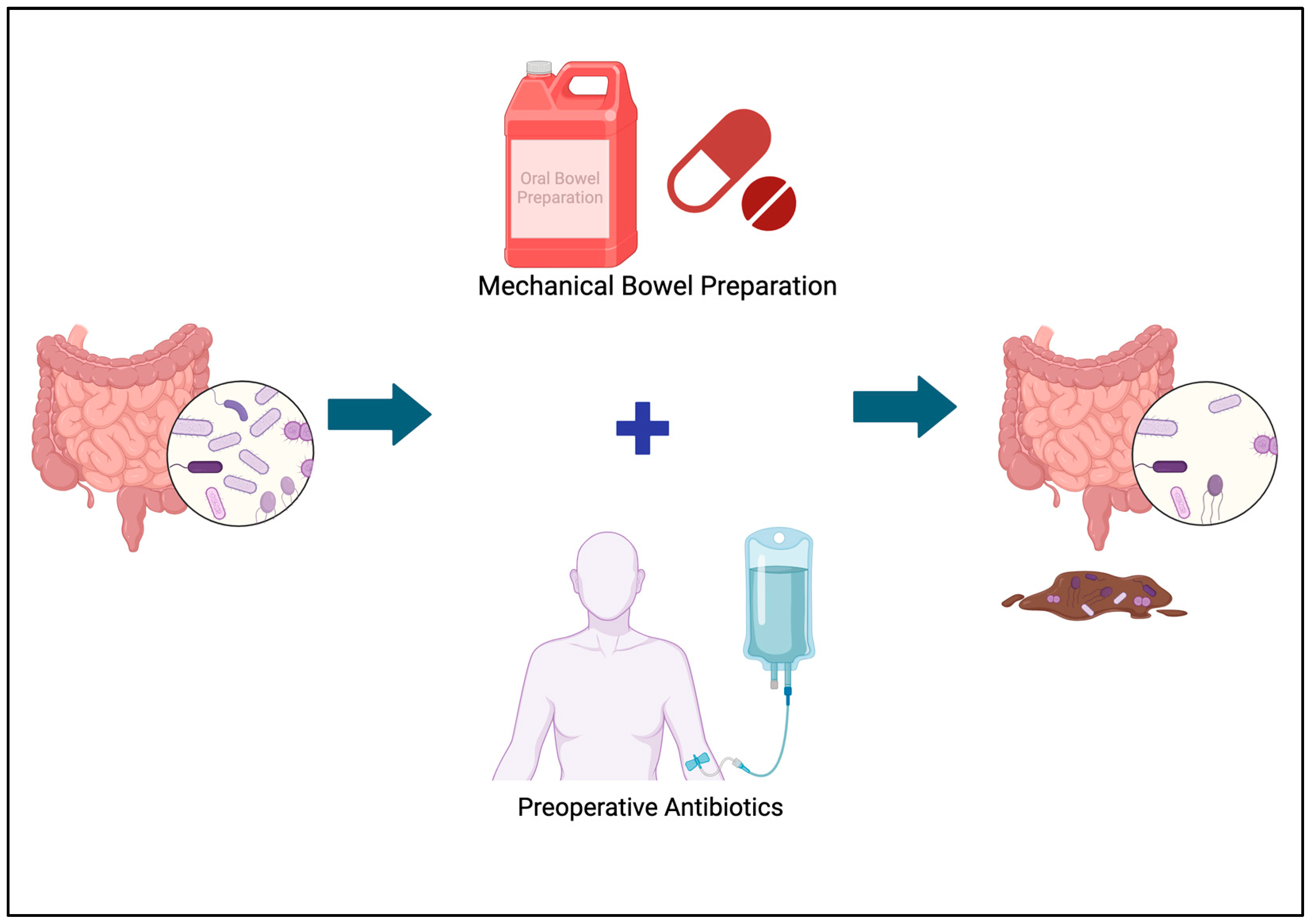
6. Preoperative Bowel Preparation
The Microbiome and Bowel Preparation
7. Perioperative Medication Considerations
7.1. Steroids
7.2. Biologics
7.3. Pain Management
7.4. Probiotics
8. Discussion and Future Directions
8.1. Fecal Microbiota Transplantation (FMT)
8.2. Surgical Innovations
9. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Borowitz, S.M. The Epidemiology of Inflammatory Bowel Disease: Clues to Pathogenesis? Front. Pediatr. 2023, 10, 1103713. [Google Scholar] [CrossRef] [PubMed]
- Kaplan, G.G.; Windsor, J.W. The Four Epidemiological Stages in the Global Evolution of Inflammatory Bowel Disease. Nat. Rev. Gastroenterol. Hepatol. 2021, 18, 56–66. [Google Scholar] [CrossRef] [PubMed]
- Meima-van Praag, E.M.; Buskens, C.J.; Hompes, R.; Bemelman, W.A. Surgical Management of Crohn’s Disease: A State of the Art Review. Int. J. Colorectal Dis. 2021, 36, 1133–1145. [Google Scholar] [CrossRef] [PubMed]
- Coward, S.; Clement, F.; Benchimol, E.I.; Bernstein, C.N.; Avina-Zubieta, J.A.; Bitton, A.; Carroll, M.W.; Hazlewood, G.; Jacobson, K.; Jelinski, S.; et al. Past and Future Burden of Inflammatory Bowel Diseases Based on Modeling of Population-Based Data. Gastroenterology 2019, 156, 1345–1353.e4. [Google Scholar] [CrossRef] [PubMed]
- Dahlhamer, J.M. Prevalence of Inflammatory Bowel Disease among Adults Aged ≥18 Years—United States, 2015. MMWR Morb. Mortal. Wkly. Rep. 2016, 65, 1166–1169. [Google Scholar] [CrossRef] [PubMed]
- Huang, H.; Fang, M.; Jostins, L.; Umićević Mirkov, M.; Boucher, G.; Anderson, C.A.; Andersen, V.; Cleynen, I.; Cortes, A.; Crins, F.; et al. Fine-Mapping Inflammatory Bowel Disease Loci to Single-Variant Resolution. Nature 2017, 547, 173–178. [Google Scholar] [CrossRef] [PubMed]
- Ek, W.E.; D’Amato, M.; Halfvarson, J. The History of Genetics in Inflammatory Bowel Disease. Ann. Gastroenterol. 2014, 27, 294–303. [Google Scholar] [PubMed]
- Sanmarco, L.M.; Chao, C.-C.; Wang, Y.-C.; Kenison, J.E.; Li, Z.; Rone, J.M.; Rejano-Gordillo, C.M.; Polonio, C.M.; Gutierrez-Vazquez, C.; Piester, G.; et al. Identification of Environmental Factors That Promote Intestinal Inflammation. Nature 2022, 611, 801–809. [Google Scholar] [CrossRef]
- Kaplan, G.G.; Ng, S.C. Understanding and Preventing the Global Increase of Inflammatory Bowel Disease. Gastroenterology 2017, 152, 313–321.e2. [Google Scholar] [CrossRef] [PubMed]
- Hurych, J.; Mascellani Bergo, A.; Lerchova, T.; Hlinakova, L.; Kubat, M.; Malcova, H.; Cebecauerova, D.; Schwarz, J.; Karaskova, E.; Hecht, T.; et al. Faecal Bacteriome and Metabolome Profiles Associated with Decreased Mucosal Inflammatory Activity Upon Anti-TNF Therapy in Paediatric Crohn’s Disease. J. Crohns Colitis 2024, 18, 106–120. [Google Scholar] [CrossRef] [PubMed]
- Núñez-Sánchez, M.A.; Melgar, S.; O’Donoghue, K.; Martínez-Sánchez, M.A.; Fernández-Ruiz, V.E.; Ferrer-Gómez, M.; Ruiz-Alcaraz, A.J.; Ramos-Molina, B. Crohn’s Disease, Host–Microbiota Interactions, and Immunonutrition: Dietary Strategies Targeting Gut Microbiome as Novel Therapeutic Approaches. Int. J. Mol. Sci. 2022, 23, 8361. [Google Scholar] [CrossRef] [PubMed]
- Nalluri-Butz, H.; Bobel, M.C.; Nugent, J.; Boatman, S.; Emanuelson, R.; Melton-Meaux, G.; Madoff, R.D.; Jahansouz, C.; Staley, C.; Gaertner, W.B. A Pilot Study Demonstrating the Impact of Surgical Bowel Preparation on Intestinal Microbiota Composition Following Colon and Rectal Surgery. Sci. Rep. 2022, 12, 10559. [Google Scholar] [CrossRef] [PubMed]
- Bernell, O.; Lapidus, A.; Hellers, G. Risk Factors for Surgery and Postoperative Recurrence in Crohn’s Disease. Ann. Surg. 2000, 231, 38–45. [Google Scholar] [CrossRef] [PubMed]
- Lloyd-Price, J.; Mahurkar, A.; Rahnavard, G.; Crabtree, J.; Orvis, J.; Hall, A.B.; Brady, A.; Creasy, H.H.; McCracken, C.; Giglio, M.G.; et al. Strains, Functions and Dynamics in the Expanded Human Microbiome Project. Nature 2017, 550, 61–66. [Google Scholar] [CrossRef] [PubMed]
- Neish, A.S. Microbes in Gastrointestinal Health and Disease. Gastroenterology 2009, 136, 65–80. [Google Scholar] [CrossRef] [PubMed]
- Alam, A.; Neish, A. Role of Gut Microbiota in Intestinal Wound Healing and Barrier Function. Tissue Barriers 2018, 6, 1539595. [Google Scholar] [CrossRef] [PubMed]
- Boatman, S.; Seraphine, C.; Staley, C.; Jahansouz, C.; Kavalukas, S. Different Primary Locations of Crohn’s Disease Are Associated with Unique Microbiome Profiles. J. Gastrointest. Surg. 2023, 27, 1727–1729. [Google Scholar] [CrossRef] [PubMed]
- Kandpal, M.; Indari, O.; Baral, B.; Jakhmola, S.; Tiwari, D.; Bhandari, V.; Pandey, R.K.; Bala, K.; Sonawane, A.; Jha, H.C. Dysbiosis of Gut Microbiota from the Perspective of the Gut-Brain Axis: Role in the Provocation of Neurological Disorders. Metabolites 2022, 12, 1064. [Google Scholar] [CrossRef] [PubMed]
- Blakeley-Ruiz, J.A.; Erickson, A.R.; Cantarel, B.L.; Xiong, W.; Adams, R.; Jansson, J.K.; Fraser, C.M.; Hettich, R.L. Metaproteomics Reveals Persistent and Phylum-Redundant Metabolic Functional Stability in Adult Human Gut Microbiomes of Crohn’s Remission Patients despite Temporal Variations in Microbial Taxa, Genomes, and Proteomes. Microbiome 2019, 7, 18. [Google Scholar] [CrossRef] [PubMed]
- Russo, E.; Cinci, L.; Di Gloria, L.; Baldi, S.; D’Ambrosio, M.; Nannini, G.; Bigagli, E.; Curini, L.; Pallecchi, M.; Andrea Arcese, D.; et al. Crohn’s Disease Recurrence Updates: First Surgery vs. Surgical Relapse Patients Display Different Profiles of Ileal Microbiota and Systemic Microbial-Associated Inflammatory Factors. Front. Immunol. 2022, 13, 886468. [Google Scholar] [CrossRef] [PubMed]
- Dalziel, T.K. Chronic Interstitial Enteritis. Br. Med. J. 1913, 2, 1068–1070. [Google Scholar]
- Honap, S.; Johnston, E.; Agrawal, G.; Al-Hakim, B.; Hermon-Taylor, J.; Sanderson, J. Anti-Mycobacterium Paratuberculosis (MAP) Therapy for Crohn’s Disease: An Overview and Update. Frontline Gastroenterol. 2020, 12, 397–403. [Google Scholar] [CrossRef] [PubMed]
- Behr, M.A.; Kapur, V. The Evidence for Mycobacterium Paratuberculosis in Crohn’s Disease. Curr. Opin. Gastroenterol. 2008, 24, 17–21. [Google Scholar] [CrossRef] [PubMed]
- Das, K.M.; Seril, D.N. Mycobacterium Avium Subspecies Paratuberculosis in Crohn’s Disease The Puzzle Continues. J. Clin. Gastroenterol. 2012, 46, 8. [Google Scholar] [CrossRef] [PubMed]
- Feller, M.; Huwiler, K.; Stephan, R.; Altpeter, E.; Shang, A.; Furrer, H.; Pfyffer, G.E.; Jemmi, T.; Baumgartner, A.; Egger, M. Mycobacterium Avium Subspecies Paratuberculosis and Crohn’s Disease: A Systematic Review and Meta-Analysis. Lancet Infect. Dis. 2007, 7, 607–613. [Google Scholar] [CrossRef] [PubMed]
- Selby, W.; Pavli, P.; Crotty, B.; Florin, T.; Radford-Smith, G.; Gibson, P.; Mitchell, B.; Connell, W.; Read, R.; Merrett, M.; et al. Two-Year Combination Antibiotic Therapy with Clarithromycin, Rifabutin, and Clofazimine for Crohn’s Disease. Gastroenterology 2007, 132, 2313–2319. [Google Scholar] [CrossRef]
- Behr, M.A.; Hanley, J. Antimycobacterial Therapy for Crohn’s Disease: A Reanalysis. Lancet Infect. Dis. 2008, 8, 344. [Google Scholar] [CrossRef] [PubMed]
- Greenstein, R.J.; Su, L.; Shahidi, A.; Brown, S.T. On the Action of 5-Amino-Salicylic Acid and Sulfapyridine on M. Avium Including Subspecies Paratuberculosis. PLoS ONE 2007, 2, e516. [Google Scholar] [CrossRef] [PubMed]
- Jernberg, C.; Löfmark, S.; Edlund, C.; Jansson, J.K. Long-Term Ecological Impacts of Antibiotic Administration on the Human Intestinal Microbiota. ISME J. 2007, 1, 56–66. [Google Scholar] [CrossRef] [PubMed]
- Carmichael, J.C.; Keller, D.S.; Baldini, G.; Bordeianou, L.; Weiss, E.; Lee, L.; Boutros, M.; McClane, J.; Steele, S.R.; Feldman, L.S. Clinical Practice Guideline for Enhanced Recovery after Colon and Rectal Surgery from the American Society of Colon and Rectal Surgeons (ASCRS) and Society of American Gastrointestinal and Endoscopic Surgeons (SAGES). Surg. Endosc. 2017, 31, 3412–3436. [Google Scholar] [CrossRef] [PubMed]
- Gustafsson, U.O.; Scott, M.J.; Hubner, M.; Nygren, J.; Demartines, N.; Francis, N.; Rockall, T.A.; Young-Fadok, T.M.; Hill, A.G.; Soop, M.; et al. Guidelines for Perioperative Care in Elective Colorectal Surgery: Enhanced Recovery after Surgery (ERAS®) Society Recommendations: 2018. World J. Surg. 2019, 43, 659–695. [Google Scholar] [CrossRef] [PubMed]
- Trépanier, M.; Minnella, E.M.; Paradis, T.; Awasthi, R.; Kaneva, P.; Schwartzman, K.; Carli, F.; Fried, G.M.; Feldman, L.S.; Lee, L. Improved Disease-Free Survival after Prehabilitation for Colorectal Cancer Surgery. Ann. Surg. 2019, 270, 493–501. [Google Scholar] [CrossRef]
- Gillis, C.; Fenton, T.R.; Sajobi, T.T.; Minnella, E.M.; Awasthi, R.; Loiselle, S.-È.; Liberman, A.S.; Stein, B.; Charlebois, P.; Carli, F. Trimodal Prehabilitation for Colorectal Surgery Attenuates Post-Surgical Losses in Lean Body Mass: A Pooled Analysis of Randomized Controlled Trials. Clin. Nutr. Edinb. Scotl. 2019, 38, 1053–1060. [Google Scholar] [CrossRef] [PubMed]
- Santa Mina, D.; van Rooijen, S.J.; Minnella, E.M.; Alibhai, S.M.H.; Brahmbhatt, P.; Dalton, S.O.; Gillis, C.; Grocott, M.P.W.; Howell, D.; Randall, I.M.; et al. Multiphasic Prehabilitation Across the Cancer Continuum: A Narrative Review and Conceptual Framework. Front. Oncol. 2021, 10, 598425. [Google Scholar] [CrossRef] [PubMed]
- Kitzman, D.W.; Whellan, D.J.; Duncan, P.; Pastva, A.M.; Mentz, R.J.; Reeves, G.R.; Nelson, M.B.; Chen, H.; Upadhya, B.; Reed, S.D.; et al. Physical Rehabilitation for Older Patients Hospitalized for Heart Failure. N. Engl. J. Med. 2021, 385, 203–216. [Google Scholar] [CrossRef] [PubMed]
- Montgomery, J.R.; Englesbe, M.J. Changes in Frailty Status: Some Better, Some Worse. Transplantation 2019, 103, 1540–1541. [Google Scholar] [CrossRef]
- Hall, D.E.; Youk, A.; Allsup, K.; Kennedy, K.; Byard, T.D.; Dhupar, R.; Chu, D.; Rahman, A.M.; Wilson, M.; Cahalin, L.P.; et al. Preoperative Rehabilitation Is Feasible in the Weeks Prior to Surgery and Significantly Improves Functional Performance. J. Frailty Aging 2022, 12, 267–276. [Google Scholar] [CrossRef] [PubMed]
- (Kristine) Koekkoek, W.; Panteleon, V.; van Zanten, A.R. Current Evidence on ω-3 Fatty Acids in Enteral Nutrition in the Critically Ill: A Systematic Review and Meta-Analysis. Nutrition 2019, 59, 56–68. [Google Scholar] [CrossRef] [PubMed]
- Chacko, J.; Pawar, S.; Seppelt, I.; Brar, G. Do Tradition-Borne Fasting Practices Apply to ICU Patients with a Protected Airway? In Controversies in Critical Care; Springer Nature Singapore: Singapore, 2023; pp. 347–352. ISBN 978-981-19993-9-0. [Google Scholar]
- American Society for Parenteral and Enteral Nutrition. Guidelines for the Use of Parenteral and Enteral Nutrition in Adult and Pediatric Patients. J. Parenter. Enter. Nutr. 2002, 26, 1SA–138SA. [Google Scholar] [CrossRef]
- Delaney, C.P.; Zutshi, M.; Senagore, A.J.; Remzi, F.H.; Hammel, J.; Fazio, V.W. Prospective, Randomized, Controlled Trial between a Pathway of Controlled Rehabilitation With Early Ambulation and Diet and Traditional Postoperative Care After Laparotomy and Intestinal Resection. Dis. Colon Rectum 2003, 46, 851–859. [Google Scholar] [CrossRef] [PubMed]
- Yoong, S.L.; Tursan d’Espaignet, E.; Wiggers, J.; St. Claire, S.; Mellin-Olsen, J.; Grady, A. Tobacco and Postsurgical Outcomes: WHO Tobacco Knowledge Summaries; World Health Organization: Geneva, Switzerland, 2020.
- Greenstein, R.J.; Su, L.; Brown, S.T. Growth of M. Avium Subspecies Paratuberculosis in Culture Is Enhanced by Nicotinic Acid, Nicotinamide, and α and β Nicotinamide Adenine Dinucleotide. Dig. Dis. Sci. 2011, 56, 368–375. [Google Scholar] [CrossRef] [PubMed]
- Thomsen, T.; Villebro, N.; Møller, A.M. Interventions for Preoperative Smoking Cessation. Cochrane Database Syst. Rev. 2014, 2014, CD002294. [Google Scholar] [CrossRef] [PubMed]
- Schonborn, J.L.; Anderson, H. Perioperative Medicine: A Changing Model of Care. BJA Educ. 2019, 19, 27–33. [Google Scholar] [CrossRef] [PubMed]
- Bonaz, B.L.; Bernstein, C.N. Brain-Gut Interactions in Inflammatory Bowel Disease. Gastroenterology 2013, 144, 36–49. [Google Scholar] [CrossRef] [PubMed]
- Bailey, M.T.; Dowd, S.E.; Galley, J.D.; Hufnagle, A.R.; Allen, R.G.; Lyte, M. Exposure to a Social Stressor Alters the Structure of the Intestinal Microbiota: Implications for Stressor-Induced Immunomodulation. Brain. Behav. Immun. 2011, 25, 397–407. [Google Scholar] [CrossRef] [PubMed]
- Goehler, L.E.; Gaykema, R.P.A.; Opitz, N.; Reddaway, R.; Badr, N.; Lyte, M. Activation in Vagal Afferents and Central Autonomic Pathways: Early Responses to Intestinal Infection with Campylobacter Jejuni. Brain. Behav. Immun. 2005, 19, 334–344. [Google Scholar] [CrossRef] [PubMed]
- Sudo, N.; Chida, Y.; Aiba, Y.; Sonoda, J.; Oyama, N.; Yu, X.; Kubo, C.; Koga, Y. Postnatal Microbial Colonization Programs the Hypothalamic–Pituitary–Adrenal System for Stress Response in Mice. J. Physiol. 2004, 558, 263–275. [Google Scholar] [CrossRef] [PubMed]
- Poggio, J. Perioperative Strategies to Prevent Surgical-Site Infection. Clin. Colon Rectal Surg. 2013, 26, 168–173. [Google Scholar] [CrossRef] [PubMed]
- Baum, M.L.; Anish, D.S.; Chalmers, T.C.; Sacks, H.S.; Smith, H.; Fagerstrom, R.M. A Survey of Clinical Trials of Antibiotic Prophylaxis in Colon Surgery: Evidence against Further Use of No-Treatment Controls. N. Engl. J. Med. 1981, 305, 795–799. [Google Scholar] [CrossRef] [PubMed]
- Nelson, R.L.; Gladman, E.; Barbateskovic, M. Antimicrobial Prophylaxis for Colorectal Surgery. Cochrane Database Syst. Rev. 2014, 2015, CD001181. [Google Scholar] [CrossRef] [PubMed]
- Scarborough, J.E.; Mantyh, C.R.; Sun, Z.; Migaly, J. Combined Mechanical and Oral Antibiotic Bowel Preparation Reduces Incisional Surgical Site Infection and Anastomotic Leak Rates after Elective Colorectal Resection: An Analysis of Colectomy-Targeted ACS NSQIP. Ann. Surg. 2015, 262, 331–337. [Google Scholar] [CrossRef] [PubMed]
- Pineda, C.E.; Shelton, A.A.; Hernandez-Boussard, T.; Morton, J.M.; Welton, M.L. Mechanical Bowel Preparation in Intestinal Surgery: A Meta-Analysis and Review of the Literature. J. Gastrointest. Surg. 2008, 12, 2037–2044. [Google Scholar] [CrossRef] [PubMed]
- Dahabreh, I.J.; Steele, D.W.; Shah, N.; Trikalinos, T.A. Oral Mechanical Bowel Preparation for Colorectal Surgery: Systematic Review and Meta-Analysis. Dis. Colon Rectum 2015, 58, 698–707. [Google Scholar] [CrossRef] [PubMed]
- Nalluri, H.; Kizy, S.; Ewing, K.; Luthra, G.; Leslie, D.B.; Bernlohr, D.A.; Sadowsky, M.J.; Ikramuddin, S.; Khoruts, A.; Staley, C.; et al. Peri-Operative Antibiotics Acutely and Significantly Impact Intestinal Microbiota Following Bariatric Surgery. Sci. Rep. 2020, 10, 20340. [Google Scholar] [CrossRef] [PubMed]
- Nagata, N.; Tohya, M.; Fukuda, S.; Suda, W.; Nishijima, S.; Takeuchi, F.; Ohsugi, M.; Tsujimoto, T.; Nakamura, T.; Shimomura, A.; et al. Effects of Bowel Preparation on the Human Gut Microbiome and Metabolome. Sci. Rep. 2019, 9, 4042. [Google Scholar] [CrossRef] [PubMed]
- Gorkiewicz, G.; Thallinger, G.G.; Trajanoski, S.; Lackner, S.; Stocker, G.; Hinterleitner, T.; Gülly, C.; Högenauer, C. Alterations in the Colonic Microbiota in Response to Osmotic Diarrhea. PLoS ONE 2013, 8, e55817. [Google Scholar] [CrossRef]
- Powles, S.T.R.; Gallagher, K.I.; Chong, L.W.L.; Alexander, J.L.; Mullish, B.H.; Hicks, L.C.; McDonald, J.A.K.; Marchesi, J.R.; Williams, H.R.T.; Orchard, T.R. Effects of Bowel Preparation on Intestinal Bacterial Associated Urine and Faecal Metabolites and the Associated Faecal Microbiome. BMC Gastroenterol. 2022, 22, 240. [Google Scholar] [CrossRef] [PubMed]
- Drago, L.; Toscano, M.; De Grandi, R.; Casini, V.; Pace, F. Persisting Changes of Intestinal Microbiota after Bowel Lavage and Colonoscopy. Eur. J. Gastroenterol. Hepatol. 2016, 28, 532–537. [Google Scholar] [CrossRef] [PubMed]
- Harrell, L.; Wang, Y.; Antonopoulos, D.; Young, V.; Lichtenstein, L.; Huang, Y.; Hanauer, S.; Chang, E. Standard Colonic Lavage Alters the Natural State of Mucosal-Associated Microbiota in the Human Colon. PLoS ONE 2012, 7, e32545. [Google Scholar] [CrossRef] [PubMed]
- Shobar, R.M.; Velineni, S.; Keshavarzian, A.; Swanson, G.; DeMeo, M.T.; Melson, J.E.; Losurdo, J.; Engen, P.A.; Sun, Y.; Koenig, L.; et al. The Effects of Bowel Preparation on Microbiota-Related Metrics Differ in Health and in Inflammatory Bowel Disease and for the Mucosal and Luminal Microbiota Compartments. Clin. Transl. Gastroenterol. 2016, 7, e143. [Google Scholar] [CrossRef] [PubMed]
- Boatman, S.; Kohn, J.; Jahansouz, C. The Influence of the Microbiome on Anastomotic Leak. Clin. Colon Rectal Surg. 2023, 36, 127–132. [Google Scholar] [CrossRef]
- Palmisano, S.; Campisciano, G.; Iacuzzo, C.; Bonadio, L.; Zucca, A.; Cosola, D.; Comar, M.; De Manzini, N. Role of Preoperative Gut Microbiota on Colorectal Anastomotic Leakage: Preliminary Results. Updat. Surg. 2020, 72, 1013–1022. [Google Scholar] [CrossRef] [PubMed]
- Menees, S.; Higgins, P.; Korsnes, S.; Elta, G. Does Colonoscopy Cause Increased Ulcerative Colitis Symptoms? Inflamm. Bowel Dis. 2007, 13, 12–18. [Google Scholar] [CrossRef]
- Shogan, B.D.; Belogortseva, N.; Luong, P.M.; Zaborin, A.; Lax, S.; Bethel, C.; Ward, M.; Muldoon, J.P.; Singer, M.; An, G.; et al. Collagen Degradation and MMP9 Activation by Enterococcus faecalis Contribute to Intestinal Anastomotic Leak. Sci. Transl. Med. 2015, 7, 286ra68. [Google Scholar] [CrossRef] [PubMed]
- Shakhsheer, B.A.; Versten, L.A.; Luo, J.N.; Defazio, J.R.; Klabbers, R.; Christley, S.; Zaborin, A.; Guyton, K.L.; Krezalek, M.; Smith, D.P.; et al. Morphine Promotes Colonization of Anastomotic Tissues with Collagenase—Producing Enterococcus Faecalis and Causes Leak. J. Gastrointest. Surg. 2016, 20, 1744–1751. [Google Scholar] [CrossRef] [PubMed]
- Taur, Y.; Xavier, J.B.; Lipuma, L.; Ubeda, C.; Goldberg, J.; Gobourne, A.; Lee, Y.J.; Dubin, K.A.; Socci, N.D.; Viale, A.; et al. Intestinal Domination and the Risk of Bacteremia in Patients Undergoing Allogeneic Hematopoietic Stem Cell Transplantation. Clin. Infect. Dis. 2012, 55, 905–914. [Google Scholar] [CrossRef] [PubMed]
- Taur, Y.; Jenq, R.R.; Perales, M.-A.; Littmann, E.R.; Morjaria, S.; Ling, L.; No, D.; Gobourne, A.; Viale, A.; Dahi, P.B.; et al. The Effects of Intestinal Tract Bacterial Diversity on Mortality Following Allogeneic Hematopoietic Stem Cell Transplantation. Blood 2014, 124, 1174–1182. [Google Scholar] [CrossRef] [PubMed]
- Alverdy, J.C.; Hyman, N. Bowel Preparation under Siege. Br. J. Surg. 2020, 107, 167–170. [Google Scholar] [CrossRef] [PubMed]
- Appau, K.A.; Fazio, V.W.; Shen, B.; Church, J.M.; Lashner, B.; Remzi, F.; Brzezinski, A.; Strong, S.A.; Hammel, J.; Kiran, R.P. Use of Infliximab within 3 Months of Ileocolonic Resection Is Associated with Adverse Postoperative Outcomes in Crohn’s Patients. J. Gastrointest. Surg. Off. J. Soc. Surg. Aliment. Tract 2008, 12, 1738–1744. [Google Scholar] [CrossRef] [PubMed]
- Lightner, A.L.; McKenna, N.P.; Tse, C.S.; Raffals, L.E.; Loftus, E.V.; Mathis, K.L. Postoperative Outcomes in Vedolizumab-Treated Crohn’s Disease Patients Undergoing Major Abdominal Operations. Aliment. Pharmacol. Ther. 2018, 47, 573–580. [Google Scholar] [CrossRef] [PubMed]
- Magro, F.; Gionchetti, P.; Eliakim, R.; Ardizzone, S.; Armuzzi, A.; Barreiro-de Acosta, M.; Burisch, J.; Gecse, K.B.; Hart, A.L.; Hindryckx, P.; et al. Third European Evidence-Based Consensus on Diagnosis and Management of Ulcerative Colitis. Part 1: Definitions, Diagnosis, Extra-Intestinal Manifestations, Pregnancy, Cancer Surveillance, Surgery, and Ileo-Anal Pouch Disorders. J. Crohns Colitis 2017, 11, 649–670. [Google Scholar] [CrossRef] [PubMed]
- Law, C.C.; Bell, C.; Koh, D.; Bao, Y.; Jairath, V.; Narula, N. Risk of Postoperative Infectious Complications from Medical Therapies in Inflammatory Bowel Disease. Cochrane Database Syst. Rev. 2020, 10, CD013256. [Google Scholar] [CrossRef] [PubMed]
- Peyrin-Biroulet, L.; Oussalah, A.; Williet, N.; Pillot, C.; Bresler, L.; Bigard, M.-A. Impact of Azathioprine and Tumour Necrosis Factor Antagonists on the Need for Surgery in Newly Diagnosed Crohn’s Disease. Gut 2011, 60, 930–936. [Google Scholar] [CrossRef] [PubMed]
- Wong, D.J.; Roth, E.M.; Feuerstein, J.D.; Poylin, V.Y. Surgery in the Age of Biologics. Gastroenterol. Rep. 2019, 7, 77–90. [Google Scholar] [CrossRef] [PubMed]
- Gaines, S.; Hyoju, S.; Williamson, A.J.; Van Praagh, J.B.; Zaborina, O.; Rubin, D.T.; Alverdy, J.C.; Shogan, B.D.; Hyman, N. Infliximab Does Not Promote the Presence of Collagenolytic Bacteria in a Mouse Model of Colorectal Anastomosis. J. Gastrointest. Surg. 2020, 24, 2637–2642. [Google Scholar] [CrossRef] [PubMed]
- Ding, N.S.; McDonald, J.A.K.; Perdones-Montero, A.; Rees, D.N.; Adegbola, S.O.; Misra, R.; Hendy, P.; Penez, L.; Marchesi, J.R.; Holmes, E.; et al. Metabonomics and the Gut Microbiome Associated with Primary Response to Anti-TNF Therapy in Crohn’s Disease. J. Crohns Colitis 2020, 14, 1090–1102. [Google Scholar] [CrossRef] [PubMed]
- Alatawi, H.; Mosli, M.; Saadah, O.I.; Annese, V.; Al-Hindi, R.; Alatawy, M.; Al-Amrah, H.; Alshehri, D.; Bahieldin, A.; Edris, S. Attributes of Intestinal Microbiota Composition and Their Correlation with Clinical Primary Non-Response to Anti-TNF-α Agents in Inflammatory Bowel Disease Patients. Bosn. J. Basic Med. Sci. 2022, 22, 412–426. [Google Scholar] [CrossRef]
- Sharma, U.; Olson, R.K.; Erhart, F.N.; Zhang, L.; Meng, J.; Segura, B.; Banerjee, S.; Sharma, M.; Saluja, A.K.; Ramakrishnan, S.; et al. Prescription Opioids Induce Gut Dysbiosis and Exacerbate Colitis in a Murine Model of Inflammatory Bowel Disease. J. Crohns Colitis 2020, 14, 801–817. [Google Scholar] [CrossRef] [PubMed]
- Darnall, B.D.; Ziadni, M.S.; Krishnamurthy, P.; Flood, P.; Heathcote, L.C.; Mackey, I.G.; Taub, C.J.; Wheeler, A. “My Surgical Success”: Effect of a Digital Behavioral Pain Medicine Intervention on Time to Opioid Cessation After Breast Cancer Surgery—A Pilot Randomized Controlled Clinical Trial. Pain Med. 2019, 20, 2228–2237. [Google Scholar] [CrossRef]
- Lee, A.; Shelton, E.; Bidwell, S.; Shankar, K.; Ando, K.; Gaudilliere, B.; Shelton, A.; Kin, C. Association of Prehabilitation with Postoperative Opioid Use in Colorectal Surgery: An Observational Cohort Study. J. Surg. Res. 2022, 273, 226–232. [Google Scholar] [CrossRef] [PubMed]
- Gorissen, K.J.; Benning, D.; Berghmans, T.; Snoeijs, M.G.; Sosef, M.N.; Hulsewe, K.W.E.; Luyer, M.D.P. Risk of Anastomotic Leakage with Non-Steroidal Anti-Inflammatory Drugs in Colorectal Surgery. Br. J. Surg. 2012, 99, 721–727. [Google Scholar] [CrossRef] [PubMed]
- Klein, M.; Gögenur, I.; Rosenberg, J. Postoperative Use of Non-Steroidal Anti-Inflammatory Drugs in Patients with Anastomotic Leakage Requiring Reoperation after Colorectal Resection: Cohort Study Based on Prospective Data. BMJ 2012, 345, e6166. [Google Scholar] [CrossRef] [PubMed]
- Modasi, A.; Pace, D.; Godwin, M.; Smith, C.; Curtis, B. NSAID Administration Post Colorectal Surgery Increases Anastomotic Leak Rate: Systematic Review/Meta-Analysis. Surg. Endosc. 2019, 33, 879–885. [Google Scholar] [CrossRef] [PubMed]
- Holte, K.; Andersen, J.; Jakobsen, D.H.; Kehlet, H. Cyclo-Oxygenase 2 Inhibitors and the Risk of Anastomotic Leakage after Fast-Track Colonic Surgery. Br. J. Surg. 2009, 96, 650–654. [Google Scholar] [CrossRef] [PubMed]
- Yauw, S.T.K.; Arron, M.; Lomme, R.M.L.M.; van den Broek, P.; Greupink, R.; Bhatt, A.P.; Redinbo, M.R.; van Goor, H. Microbial Glucuronidase Inhibition Reduces Severity of Diclofenac-Induced Anastomotic Leak in Rats. Surg. Infect. 2018, 19, 417–423. [Google Scholar] [CrossRef] [PubMed]
- Bhangu, A.; Singh, P.; Fitzgerald, J.E.F.; Slesser, A.; Tekkis, P. Postoperative Nonsteroidal Anti-Inflammatory Drugs and Risk of Anastomotic Leak: Meta-Analysis of Clinical and Experimental Studies. World J. Surg. 2014, 38, 2247–2257. [Google Scholar] [CrossRef] [PubMed]
- Carlini, M.; Grieco, M.; Spoletini, D.; Menditto, R.; Napoleone, V.; Brachini, G.; Mingoli, A.; Marcellinaro, R. Implementation of the Gut Microbiota Prevents Anastomotic Leaks in Laparoscopic Colorectal Surgery for Cancer:The Results of the MIRACLe Study. Updat. Surg. 2022, 74, 1253–1262. [Google Scholar] [CrossRef] [PubMed]
- Dore, M.P.; Rocchi, C.; Longo, N.P.; Scanu, A.M.; Vidili, G.; Padedda, F.; Pes, G.M. Effect of Probiotic Use on Adverse Events in Adult Patients with Inflammatory Bowel Disease: A Retrospective Cohort Study. Probiotics Antimicrob. Proteins 2020, 12, 152–159. [Google Scholar] [CrossRef] [PubMed]
- Knox, N.C.; Forbes, J.D.; Van Domselaar, G.; Bernstein, C.N. The Gut Microbiome as a Target for IBD Treatment: Are We There Yet? Curr. Treat. Options Gastroenterol. 2019, 17, 115–126. [Google Scholar] [CrossRef] [PubMed]
- Forbes, A.; Escher, J.; Hébuterne, X.; Kłęk, S.; Krznaric, Z.; Schneider, S.; Shamir, R.; Stardelova, K.; Wierdsma, N.; Wiskin, A.E.; et al. ESPEN Guideline: Clinical Nutrition in Inflammatory Bowel Disease. Clin. Nutr. Edinb. Scotl. 2017, 36, 321–347. [Google Scholar] [CrossRef] [PubMed]
- Boicean, A.; Birlutiu, V.; Ichim, C.; Anderco, P.; Birsan, S. Fecal Microbiota Transplantation in Inflammatory Bowel Disease. Biomedicines 2023, 11, 1016. [Google Scholar] [CrossRef] [PubMed]
- Ianiro, G.; Bibbò, S.; Scaldaferri, F.; Gasbarrini, A.; Cammarota, G. Fecal Microbiota Transplantation in Inflammatory Bowel Disease: Beyond the Excitement. Medicine 2014, 93, e97. [Google Scholar] [CrossRef] [PubMed]
- Waller, K.M.J.; Leong, R.W.; Paramsothy, S. An Update on Fecal Microbiota Transplantation for the Treatment of Gastrointestinal Diseases. J. Gastroenterol. Hepatol. 2022, 37, 246–255. [Google Scholar] [CrossRef] [PubMed]
- Sokol, H.; Landman, C.; Seksik, P.; Berard, L.; Montil, M.; Nion-Larmurier, I.; Bourrier, A.; Le Gall, G.; Lalande, V.; De Rougemont, A.; et al. Fecal Microbiota Transplantation to Maintain Remission in Crohn’s Disease: A Pilot Randomized Controlled Study. Microbiome 2020, 8, 12. [Google Scholar] [CrossRef] [PubMed]
- Ali, S.; Navaneethan, U. Chapter 15—Endoscopic Stent Treatment for Crohn’s Disease. In Interventional Inflammatory Bowel Disease: Endoscopic Management and Treatment of Complications; Shen, B., Ed.; Academic Press: Cambridge, MA, USA, 2018; pp. 181–186. ISBN 978-0-12-811388-2. [Google Scholar]
- Scotti, G.B.; Lorenzetti, R.; Aratari, A.; Lamazza, A.; Fiori, E.; Papi, C.; Festa, S. Stricturing Crohn’s Disease: What Is the Role of Endoscopic Stenting? A Systematic Review. Clin. Endosc. 2023, 56, 726–734. [Google Scholar] [CrossRef] [PubMed]
- De Jonge, S.W.; Atema, J.J.; Solomkin, J.S.; Boermeester, M.A. Meta-Analysis and Trial Sequential Analysis of Triclosan-Coated Sutures for the Prevention of Surgical-Site Infection. Br. J. Surg. 2017, 104, e118–e133. [Google Scholar] [CrossRef] [PubMed]
- Edmiston, C.E.; Daoud, F.C.; Leaper, D. Is There an Evidence-Based Argument for Embracing an Antimicrobial (Triclosan)-Coated Suture Technology to Reduce the Risk for Surgical-Site Infections?: A Meta-Analysis. Surgery 2013, 154, 89–100. [Google Scholar] [CrossRef] [PubMed]
- Suh, I.; Long, S.A.; Coe, J.; Koehler, J.; Fry, D.; Welton, M.L. The Efficacy of a Novel Surgical Device in Preventing Intraoperative Wound Contamination in an In Vivo Porcine Model. J. Laparoendosc. Adv. Surg. Tech. A 2018, 28, 445–451. [Google Scholar] [CrossRef] [PubMed]
- Mao, L.; Zhou, S.; Liao, J.; Zhou, X.; Wang, J. Effect of Wound Protectors in Reducing the Incidence of Surgical Site Wound Infection in Lower Gastrointestinal Surgery: A Meta-analysis. Int. Wound J. 2022, 20, 813–821. [Google Scholar] [CrossRef] [PubMed]



Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Olson, S.; Welton, L.; Jahansouz, C. Perioperative Considerations for the Surgical Treatment of Crohn’s Disease with Discussion on Surgical Antibiotics Practices and Impact on the Gut Microbiome. Antibiotics 2024, 13, 317. https://doi.org/10.3390/antibiotics13040317
Olson S, Welton L, Jahansouz C. Perioperative Considerations for the Surgical Treatment of Crohn’s Disease with Discussion on Surgical Antibiotics Practices and Impact on the Gut Microbiome. Antibiotics. 2024; 13(4):317. https://doi.org/10.3390/antibiotics13040317
Chicago/Turabian StyleOlson, Shelbi, Lindsay Welton, and Cyrus Jahansouz. 2024. "Perioperative Considerations for the Surgical Treatment of Crohn’s Disease with Discussion on Surgical Antibiotics Practices and Impact on the Gut Microbiome" Antibiotics 13, no. 4: 317. https://doi.org/10.3390/antibiotics13040317
APA StyleOlson, S., Welton, L., & Jahansouz, C. (2024). Perioperative Considerations for the Surgical Treatment of Crohn’s Disease with Discussion on Surgical Antibiotics Practices and Impact on the Gut Microbiome. Antibiotics, 13(4), 317. https://doi.org/10.3390/antibiotics13040317