Iridoschisis—A Systematic Review

 , ,
, ,
Abstract
1. Introduction
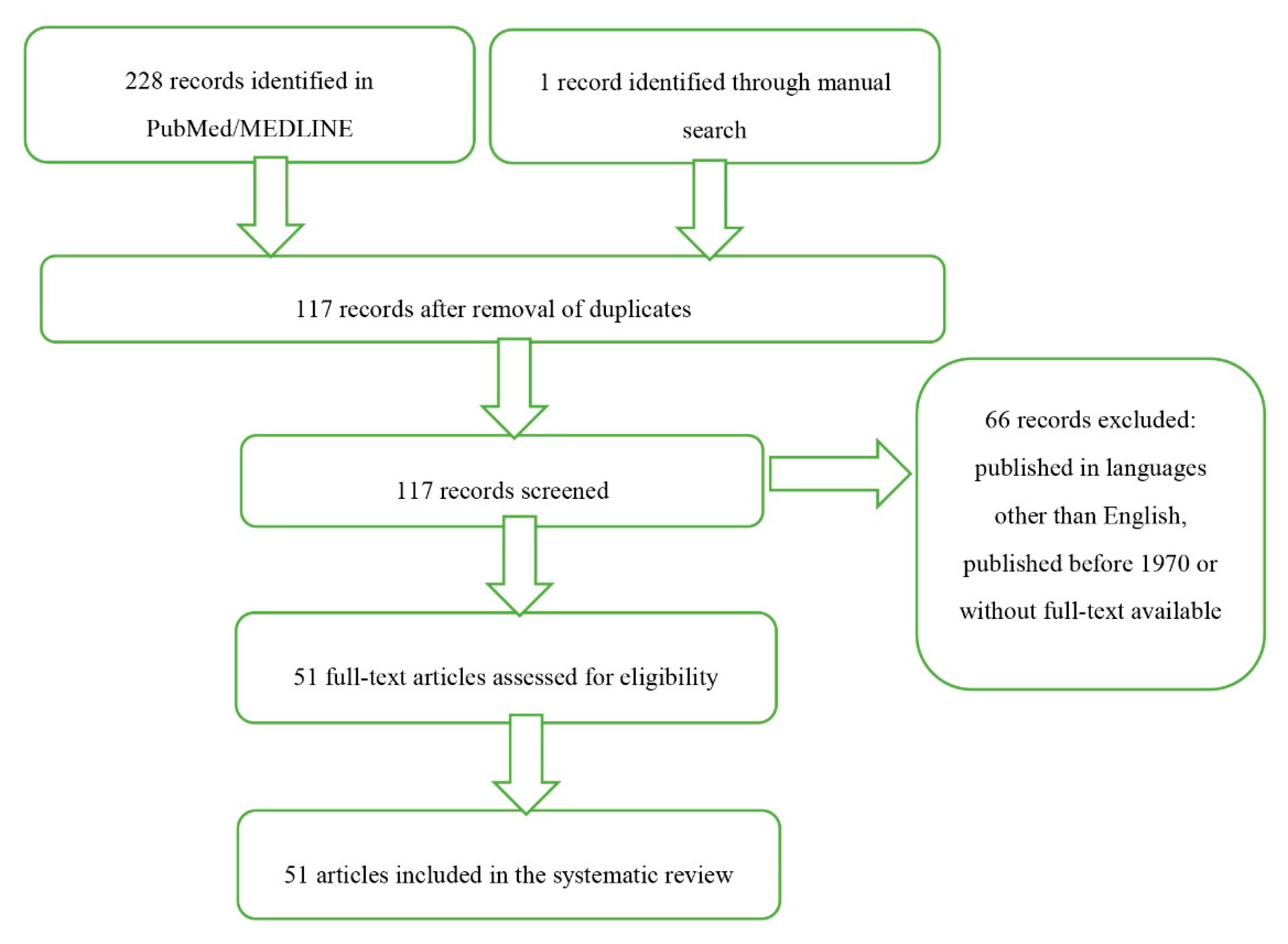
2. Method of Literature Search
3. Definition
4. Epidemiology and Inheritance
5. Pathophysiology
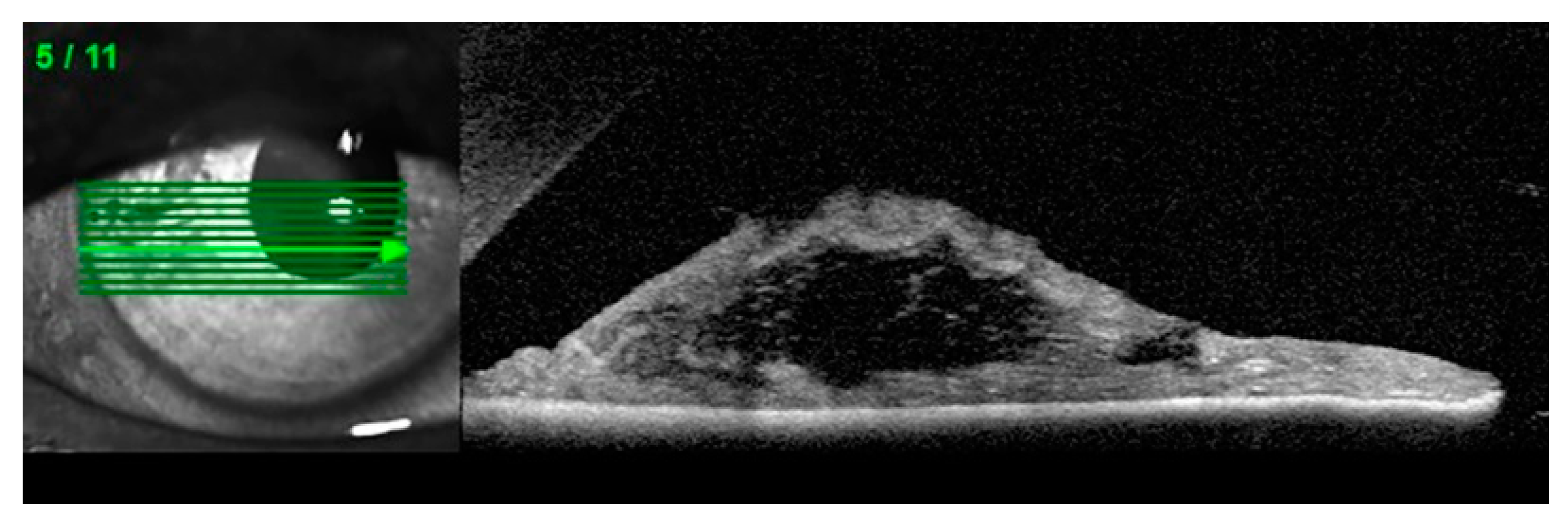
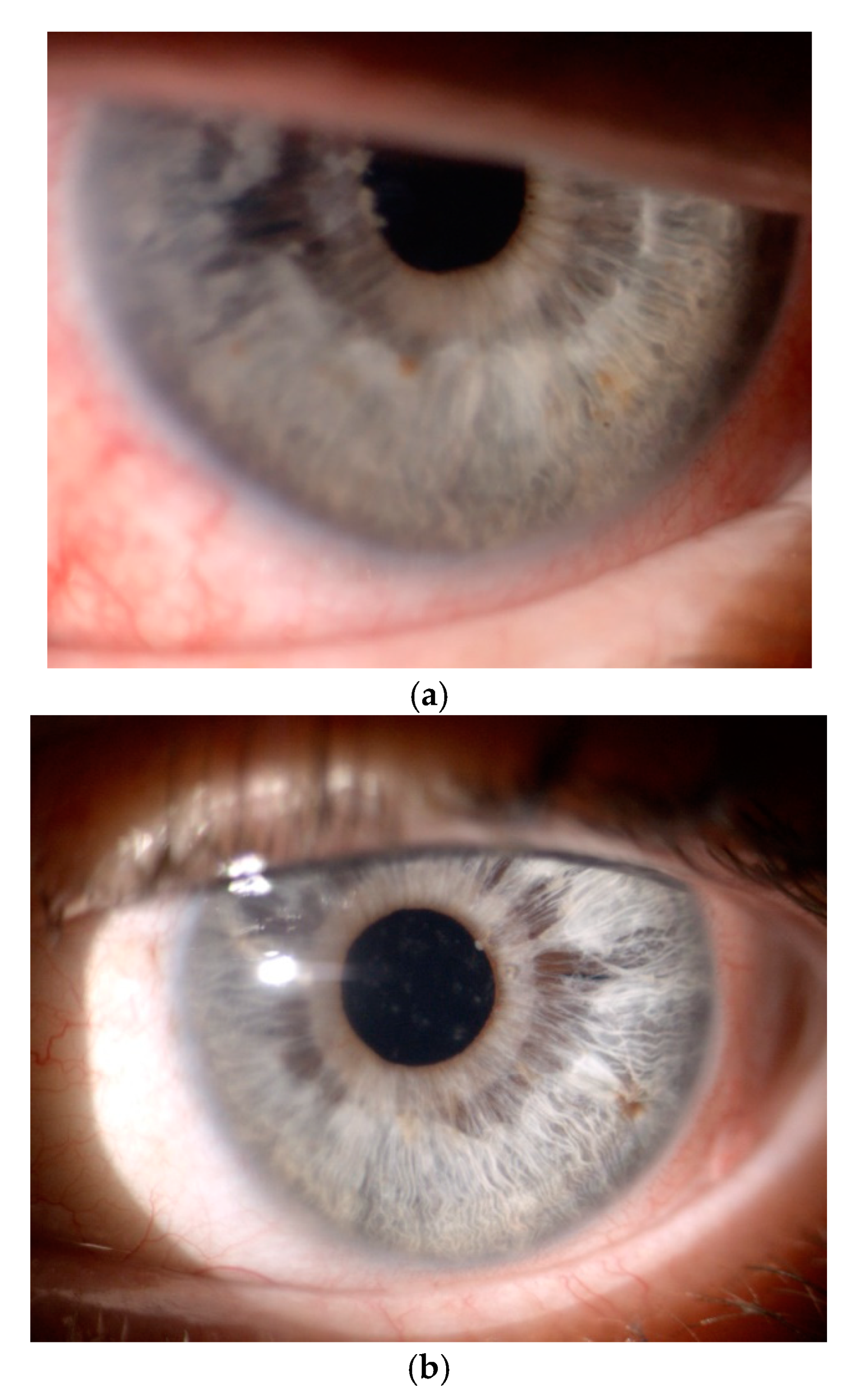
6. Clinical Characteristics and Diagnostic Imaging
7. Glaucoma and Other Associated Ocular Pathologies
8. Differential Diagnoses
9. Glaucoma Characteristics and Treatment in Patients with Iridoschisis
10. Phacoemulsification in Patients with Iridoschisis
11. Corneal Decompensation Treatment in Patients with Iridoschisis
12. Discussion
13. Conclusions
Funding
Conflicts of Interest
References
- Gogaki, E.; Tsolaki, F.; Tiganita, S.; Skatharoudi, C.; Balatsoukas, D. Iridoschisis: Case report and review of the literature. Clin. Ophthalmol. 2011, 5, 381–384. [Google Scholar] [CrossRef][Green Version]
- Lowenstein, A.; Foster, J. Iridoschisis with multiple rupture of stromal threads. Br. J. Ophthalmol. 1945, 29, 277–282. [Google Scholar] [CrossRef]
- Schmitt, A. Detachment of the anterior half of the iris plane. Klin Monatsbl Angenheilkd. 1922, 68, 214–215. [Google Scholar]
- Mansour, A.M. A family with iridoschisis, narrow anterior chamber angle, and presenile cataract. Ophthalmic Paediatr. Genet. 1986, 7, 145–149. [Google Scholar] [CrossRef]
- Danias, J.; Aslanides, I.M.; Eichenbaum, J.W.; Silverman, R.H.; Reinstein, D.Z.; Coleman, D.J. Iridoschisis: High frequency ultrasound imaging. Evidence for a genetic defect? Br. J. Ophthalmol. 1996, 80, 1063–1067. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Loewenstein, A.; Foster, J.; Sledge, S.K. A further case of iridoschisis. Br. J. Ophthalmol. 1948, 32, 129–134. [Google Scholar] [CrossRef]
- Romano, A.; Treister, G.; Barishak, R.; Stein, R. Iridoschisis and angle-closure glaucoma. Ophthalmologica 1972, 164, 199–207. [Google Scholar] [CrossRef]
- Pérez-Carro, G.; Vilanova, M.; Antuña, M.G.; Cárcaba, V.; Junceda-Moreno, J. Iridoschisis associated to congenital syphilis: Serological confirmation at the 80’s. Arch. Soc. Esp. Oftalmol. 2009, 84, 353–358. [Google Scholar]
- Foss, A.J.; Hykin, P.G.; Benjamin, L. Interstitial keratitis and iridoschisis in congenital syphilis. J. Clin. Neuroophthalmol. 1992, 12, 167–170. [Google Scholar]
- Chen, Y.; Qian, Y.; Lu, P. Iridoschisis: A case report and literature review. BMC Ophthalmol. 2017, 17, 24. [Google Scholar] [CrossRef]
- Pesudovs, K.; Schoneveld, P.G. Iridoschisis. Clin. Exp. Optom. 1999, 82, 29–33. [Google Scholar]
- Aaberg, T.; Nelson, M. Iridoschisis and cataract in a juvenile patient with periocular eczema. JCRS Online Case Rep. 2017, 5, 54–57. [Google Scholar] [CrossRef]
- Albers, E.C.; Klein, B.A. Iridoschisis: A clinical and histopathologic study. Am. J. Ophthalmol. 1958, 46, 794–802. [Google Scholar] [CrossRef]
- Carnevalini, A.; Menchini, U.; Bandello, F.; Scialdone, A.; Brancarto, R. Aspects fluoroiridographiques de L ‘Iridoschisis. J. Fr. Ophthalmol. 1988, 11, 329–332. [Google Scholar]
- Bøjer, J. Iridoschisis: Essential iris atrophy. Acta Ophthalmol. 1953, 31, 253–264. [Google Scholar] [CrossRef]
- Payne, T.D.; Thomas, R.P. Iridoschisis: A case report. Am. J. Ophthalmol. 1966, 62, 966–967. [Google Scholar] [CrossRef]
- Agard, E.; Malcles, A.; El Chehab, H.; Ract-Madoux, G.; Swalduz, B.; Aptel, F.; Denis, P.; Dot, C. Iridoschisis, a special form of iris atrophy. J. Fr. Ophthalmol. 2013, 36, 368–371. [Google Scholar] [CrossRef] [PubMed]
- Lee, E.J.; Lee, J.; Hyon, J.; Kim, M.; Wee, W. A case of cataract surgery without pupillary device in the eye with iridoschisis. Korean J. Ophthalmol. 2008, 22, 58–62. [Google Scholar] [CrossRef]
- Salmon, J.F.; Murray, A.D. The association of iridoschisis and primary angle-closure glaucoma. Eye 1992, 6, 267–272. [Google Scholar] [CrossRef]
- Rodrigues, M.C.; Spaeth, G.L.; Krachmer, J.H.; Laibson, P.R. Iridoschisis associated with glaucoma and bullous keratopathy. Am. J. Ophthalmol. 1983, 95, 73–81. [Google Scholar] [CrossRef]
- Srinivasan, S.; Batterbury, M.; Hiscott, P. Bullous keratopathy and corneal decompensation secondary to iridoschisis: A clinicopathological report. Cornea 2005, 24, 867–869. [Google Scholar]
- Wang, H.B.; Hu, Y.X.; Feng, X. Corneal endothelial decompensation secondary to iridoschisis in degenerative myopic eyes: A case report. Int. J. Ophthalmol. 2012, 5, 116–118. [Google Scholar]
- Minezaki, T.; Hattori, T.; Nakagawa, H.; Kumakura, S.; Goto, H. Non-Descemet’s stripping automated endothelial keratoplasty for bullous keratopathy secondary to iridoschisis. Clin. Ophthalmol. 2013, 7, 1353–1355. [Google Scholar]
- Crosby, N.J.; McDonnell, P.; Shah, P. Iridoschisis associated with nanophthalmos and bullous keratopathy. Int. Ophthalmol. 2013, 33, 83–85. [Google Scholar] [CrossRef]
- Greenwald, M.F.; Niles, P.I.; Johnson, A.T.; Vislisel, J.M.; Greiner, M.A. Descemet membrane endothelial keratoplasty for corneal decompensation due to iridoschisis. Am. J. Ophthalmol. Case Rep. 2018, 9, 34–37. [Google Scholar] [CrossRef]
- Torricelli, A.; Reis, A.S.C.; Abucham, J.Z.; Suzuki, R.; Malta, R.F.S.; Monteiro, M.L.R. Bilateral nonarteritic anterior ischemic neuropathy following acute angle-closure glaucoma in a patient with iridoschisis: Case report. Arq. Bras. Oftalmol. 2011, 74, 61–63. [Google Scholar] [CrossRef][Green Version]
- Paniagua, L.; Bande, M.F. Rodríguez-Ares MT, Piñeiro A. A presentation of iridoschisis with plateau iris: An imaging study. Clin. Exp. Optom. 2015, 98, 290–291. [Google Scholar] [CrossRef]
- Shima, C.; Otori, Y.; Miki, A.; Tano, J. A case of iridoschisis associated with plateau iris configuration. Jpn. J. Ophthalmol. 2007, 51, 390–391. [Google Scholar] [CrossRef]
- Nguyen, A.T.; Liu, T.; Liu, J. Applications of Scheimpflug Imaging in Glaucoma Management: Current and Potential Applications. J. Ophthalmol. 2016, 2016. [Google Scholar] [CrossRef] [PubMed]
- Salmon, J.F. The association of iridoschisis and angle-recession glaucoma. Am. J. Ophthalmol. 1992, 114, 766–767. [Google Scholar] [CrossRef]
- Auffarth, G.U.; Reuland, A.J.; Heger, T.; Völcker, H.E. Cataract surgery in eyes with iridoschisis using the Perfect Pupil iris extension system. J. Cataract. Refract. Surg. 2005, 31, 1877–1880. [Google Scholar] [CrossRef] [PubMed]
- Chen, H.S.; Kang, E.Y.; Wu, W.C. Capsular delamination of the crystalline lens and iridoschisis. Can. J. Ophthalmol. 2020, 55, 343–344. [Google Scholar] [CrossRef] [PubMed]
- Pieklarz, B.; Grochowski, E.; Dmuchowska, D.A.; Saeed, E.; Sidorczuk, P.; Mariak, Z. Iris-claw lens implantation in a patient with iridoschisis. Am. J. Case Rep. 2020, 21, e925234. [Google Scholar] [CrossRef] [PubMed]
- Krohn, D.L.; Garrett, E.E. Iridoschisis and keratoconus; report of case in a twenty-year-old man. Arch. Ophthalmol. 1954, 52, 426–432. [Google Scholar] [CrossRef]
- Porteous, A.; Low, S.; Younis, S.; Bloom, P. Lens extraction and intraocular lens implant to manage iridoschisis. Clin. Exp. Ophthalmol. 2014, 3, 82–83. [Google Scholar] [CrossRef]
- Agrawal, S.; Agrawal, J.; Agrawal, T.P. Iridoschisis associated with lens subluxation. J. Cataract. Refract. Surg. 2001, 27, 2044–2046. [Google Scholar] [CrossRef]
- Adler, R.A.; Weinberg, R.S. Iridoschisis and bilateral lens subluxation associated with periocular eczema. J. Cataract. Refract. Surg. 2004, 30, 234–236. [Google Scholar] [CrossRef]
- Mutoh, T.; Matsumoto, Y.; Chikuda, M. A case of iridoschisis associated with lens displacement into the vitreous cavity. Clin. Ophthalmol. 2010, 4, 487–491. [Google Scholar] [CrossRef][Green Version]
- Eiferman, R.A.; Law, M.; Lane, L. Iridoschisis and keratoconus. Cornea 1994, 13, 78–79. [Google Scholar] [CrossRef]
- Petrovic, A.; Kymionis, G. Massive iridoschisis after penetrating keratoplasty successfully managed with nd:Yag punctures: A case report. Eur. J. Ophthalmol. 2019. [Google Scholar] [CrossRef]
- Yusuf, I.H.; Salmon, J.F. Iridoschisis and keratoconus in a patient with severe allergic eye disease and compulsive eye rubbing: A case report. J. Med. Case Rep. 2016, 10, 134. [Google Scholar] [CrossRef] [PubMed]
- Weseley, A.C.; Freeman, W.R. Iridoschisis and the corneal endothelium. Ann. Ophthalmol. 1983, 5, 955–964. [Google Scholar]
- Chapman, K.O.; Demetriades, A.M. Juvenile iridoschisis and incomplete plateau iris configuration. J Glaucoma. 2011, 24, 142–144. [Google Scholar] [CrossRef]
- Swaminathan, S.S.; Cavuoto, K.M.; Chang, T.C. Iridoschisis in Angle-Closure Glaucoma Associated with Alkali Burn. JAMA Ophthalmol. 2017, 135, e172313. [Google Scholar] [CrossRef] [PubMed]
- Sacchetti, M.; Marenco, M.; Macchi, I.; Ambrosio, O.; Rama, P. Diagnosis and Management of Iridocorneal Endothelial Syndrome. BioMed Res. Int. 2015, 2015. [Google Scholar] [CrossRef]
- Shields, M.B. Axenfeld-Rieger and Iridocorneal Endothelial syndromes: Two spectra of Disease with Striking Similarities and Differences. J. Glaucoma 2001, 10 (Suppl. S1), S36–S38. [Google Scholar] [CrossRef] [PubMed]
- You, Z.; Qin, Y.; Li, G.; Shi, K. Goniosynechialysis combined with cataract extraction for iridoschisis: A case report. Medicine 2017, 96, e8295. [Google Scholar] [CrossRef]
- Goyeneche, H.G.; Osorio, J.T.; Malo, L.M. Iridoschisis in Latin America: A case report and literature review. Pan-Am. J. Ophthalmol. 2018, 17, 84–88. [Google Scholar]
- Snyder, M.E.; Malyugin, B.; Marek, S.L. Novel approaches to phacoemulsification in iridoschisis. Can. J. Ophthalmol. 2019, 54, e221–e225. [Google Scholar] [CrossRef]
- Wilczynski, M.; Kucharczyk, M. Phacoemulsification with Malyugin ring in an eye with iridoschisis, narrow pupil, anterior and posterior synechiae: Case report. Eur. J. Ophthalmol. 2013, 23, 909–912. [Google Scholar] [CrossRef]
- Rozenberg, I.; Seabra, F.P. Avoiding iris trauma from phacoemulsification in eyes with iridoschisis. J. Cataract. Refract. Surg. 2004, 30, 741–745. [Google Scholar] [CrossRef] [PubMed]
- Castanera, A.P.A.; Jorge, M.D. Pupil Management during Phacoemulsification in Patients with Iridoschisis. J. Cataract. Refract. Surg. 2001, 26, 797–799. [Google Scholar] [CrossRef]
- Smith, G.T.; Liu, C.S.C. Flexible iris hooks for phacoemulsification in patients with iridoschisis. J. Cataract. Refract. Surg. 2000, 26, 1277–1280. [Google Scholar] [CrossRef]
- Ghanem, V.C.; Ghanem, E.A.; Ghanem, R.C. Iridectomy of the anterior iris stroma using the vitreocutter during phacoemulsification in patients with iridoschisis. J. Cataract. Refract. Surg. 2003, 29, 2057–2059. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Distinguishing Features | Iridoschisis | ICE | ARS | ||
|---|---|---|---|---|---|
| Chandler Syndrome | Cogan-Reese Syndrome | Essential Iris Atrophy | |||
| Age of Onset | 6th–7th decade | 3rd–4th decade | congenital, at birth | ||
| Gender Predisposition | slightly more often in women | mostly in women | no | ||
| Laterality | more often bilateral | mostly unilateral | bilateral | ||
| Congenital | no | no | yes | ||
| Iris | - stromal splitting with strands floating in the aqueous humor - sectoral, mainly inferior - without hole(s) | - minimal irideal alterations - areas of irideal atrophy should not progress to a full-thickness iris hole(s) | - different degrees of iris atrophy - multiple yellowish or brown irideal nodules | - irideal atrophy - stretched and full-thickness hole(s) | - iris may be normal except for the iridocorneal adhesions - mild stromal thinning - atrophy with full-thickness holes - stromal hypoplasia |
| Localization | mostly inferior, but also other parts of the iris may be affected | diffuse | diffuse | ||
| Cornea | rarely involved, but focal endothelial cell loss may occur, possibly with subsequent endothelial decompensation | - evident early corneal edema | - corneal edema may occur | - corneal edema may occur | - central cornea usually normal - endothelial changes due to PAS - edema - posterior embryotoxon |
| - endothelial dystrophy - specular microscopic evidence of ICE-cells, i.e., abnormal, rounded, large and pleomorphic cells with pathognomonic intracellular dark spots | |||||
| Pupils | round and reactive | corectopia | changes uncommon | polycoria | - corectopia - polycoria - ectropion uvae |
| Anterior Chamber Angle | PAS possible | gradually progressing PAS | PAS | ||
| Progression | yes | yes | often stationary or only a minor progression | ||
| Glaucoma | - various forms of glaucoma in 65% of the cases: - most often secondary ACG (Table 2) - sporadically open-angle glaucoma [9,14], angle recession glaucoma [30] | secondary ACG in 50% of the cases | secondary ACG in 50% of the cases | ||
| Other Ocular or Systemic Anomalies | a number of possible associated ocular conditions (uncertain relevance) | no non-ocular findings | - craniofacial dysmorphism-dental abnormalities-musculoskeletal malformations - possibility of other systemic abnormalities | ||
| Author, Publication Year, Reference | Type of Glaucoma | Age (Years), Sex | History of Ocular Trauma or Hereditary Ocular Disease | Clinical Characteristics and Imaging Results | Iridoschisis Laterality, Localization | Other Findings | Conservative Treatment | Surgery or Laser Treatment | Comments |
|---|---|---|---|---|---|---|---|---|---|
| Gogaki et al., 2011 [1] | AAC (ACG possible) | 80, F | No | - VA: LE 6/200 - IOP: LE 54 mmHg - Biomicroscopy: typical findings in AC - Optic disc: evaluation impossible - Gonioscopy: closed angle (Shaffer grade 0-1) for 270° and scattered PAS in the superior quadrants of both eyes | Bilateral, inferiorly | Mature cataract | - Acute treatment: acetazolamide, dorzolamide/timolol, isoptocarpine, intravenous mannitol and oral analgesics - Chronic treatment: isoptocarpine | No | Good IOP control with topical treatment |
| Mansour, 1985 [4] | Case 1: likely ACG in LE | 54, F | No information | - BVCA: RE 6/60, LE 6/2000 - IOP: RE 10 mmHg, LE 12 mmHg - Optic disc: no data - Gonioscopy: RE open anterior chamber angle with normal angle structures for 360°, LE anterior chamber +1 centrally and peripherally with grade 1 to 2 angle - Provocative test: increase in IOP to 13 mmHg | Bilateral, inferiorly, more prominent in LE | - Pseudophakic RE (lens extraction 3 years earlier) - Dense nuclear cataract in LE | No | Uncomplicated intracapsular lens extraction and iridectomy in LE | Postoperative BVCA: LE 6/30 |
| Case 2: ACG | 57, F (sister of patient from Case 1) | No information | - VA: RE 6/600, LE hand motion - IOP: RE 14 mmHg, LE 4 mmHg - Optic disc: no data - Gonioscopy: RE narrow angle with no structures seen and PAS superiorly | Extensive, bilateral iridoschisis | - Cataract in RE - Iris incarceration, pupillary occlusion and phthisis bulbi with low intraocular pressure (post-operative complications) in LE | No | - Extracapsular lens extraction in RE - Complicated intracapsular lens extraction in LE four years earlier | - Postoperative BVCA: RE 6/21 | |
| Danias et al., 1966 [5] | ACG | 71, F | History of the excision of fibrous dysplasia from the left frontal bone and superior orbital decompression | - BVCA: RE 6/7.5, LE 6/12 - IOP: RE 23 mmHg, LE 26 mmHg - Optic disc: RE c/d = 0.5, LE c/d = 0.8 - Gonioscopy: narrow angles - Goldmann perimetry: full fields in both eyes although the Humphrey hemifield borderline glaucomatous in LE | Bilateral, all quadrants affected, more pronounced inferiorly and in LE | - Iridocorneal touch inferiorly in RE - Nanophthalmos - Hyaloid residues in LE | No information | Laser iridotomy in LE | IOP one month later: LE 23 mmHg with essentially unchanged gonioscopic findings |
| Romano et al., 1972 [7] | Case 1: ACG | 63, M | No information | - VA: RE 6/76, LE 6/76 - IOP: RE 14 mmHg, LE 13 mmHg - Optic discs: partial cupping - Gonioscopy: PAS in the lower in both eyes | Bilateral, symmetrical, between 4 and 7 o’clock position | Bilateral nuclear and slight posterior cortical cataract | Pilocarpine and acetazolamide | - Bilateral basal iridectomy 17 years earlier because of AAC - One year later uneventful intracapsular cryo-extraction of cataract in RE | - No obvious progression of iridoschisis during a three-year follow-up - Postoperative BCVA in RE: 6/24 |
| Case 2: ACG | 61, F | No information | - VA: RE 6/8, LE 6/10 - IOP: RE 14 mmHg, LE 40 mm Hg - Optic disc: RE “normal”, LE “almost completely excavated” - Gonioscopy: narrow angle in LE, closed in the lower quadrants - Provocative test with neosynephrine: IOP raised to 24 mm in RE | Unilateral in RE, between 4 and 7 o’clock position | Pilocarpine, eserine into LE, pilocarpine into RE, acetazolamide | - Peripheral iridencleisis in LE - Peripheral iridectomy in RE (AAC in the night after the LE surgery) | Minor progression of iridoschisis during a two-year follow-up | ||
| Case 3: ACG, AAC (3 weeks earlier) | 75, F | No information | - VA: “normal” in both eyes - IOP: RE >30 mmHg in spite of intensive treatment, LE 18 mmHg - Optic discs: no cupping - Gonioscopy: almost completely closed angle in RE, very narrow but still open angle in LE - Visual field: upper nasal defect in RE - Provocative test: no increase in IOP in LE | Bilateral, between 5 and 7 o’clock position | Iridocorneal touch | Pilocarpine in both eyes | - Iridencleisis in RE | ||
| Case 4: ACG in RE | 55, F | No information | - VA, IOP, optic disc: no data - Gonioscopy: closed angle except from the area of the coloboma - Patient under control for the last 15 years; lost vision in LE | Between 4 and 8 o’clock position | Nuclear posterior cortical cataract in RE (developed later) | No information | - Total iridectomy in RE (development of a spontaneous filtrating bleb with further loss of activity) - Cyclodialysis in RE two years later (tension could not be controlled) - Cataract; extraction of the lens in RE | ||
| Foss et al., 1992 [9] | Case 1 and 3: no evidence of glaucoma | ||||||||
| Case 2: 10-year history of bilateral chronic open angle glaucoma | 70, F | No information | - VA: RE 6/24, LE 6/20 - IOP: 18 mmHg in both eyes - Optic disc: glaucomatous damage in both eyes - Gonioscopy: a limited view of the open angle with moderate pigment deposition, without PAS - Visual fields: constrictions in both eyes | Bilateral | Bilateral interstitial keratitis | Topical antiglaucoma treatment | No | No progression on topical antiglaucoma treatment | |
| Case 4: 24-year history of bilateral chronic open angle glaucoma | 75, F | No information | - VA: RE hand movements, LE 6/60 - IOP: RE 16 mmHg, LE 5 mmHg - Optic disc: c/d = 0.5 in both eyes - Gonioscopy: open anterior chamber angles with mild pigment deposition | Unilateral, inferiorly | - Interstitial keratitis and old keratic precipitates in LE - Bilateral inferonasal chorioretinal scarring - Moderate nuclear cataract in RE | Topical antiglaucoma medication for 10 years, followed by IOP increase to 50 mmHg (despite topical and oral acetazolamide) | - Uncomplicated trabeculectomies in both eyes (no additional medication needed for 14 years after the surgery) - Extracapsular cataract extraction and penetrating keratoplasty in RE 10 years after the first surgery | ||
| Chen et al., 2017 [10] | Case 1 and 2: no evidence of glaucoma | ||||||||
| Case 3: ACG | 66, M | No | - Preoperative BCVA: RE 6/38, LE 6/15 - IOP: RE 22 mmHg, LE 35 mmHg - Optic disc: no data - Gonioscopy: Discontinuous PAS and pigment deposition superiorly - Scheimpflug images: peripheral AC partially shallowed, but the iridocorneal angle still open in both eyes | Bilateral, temporally | Cortical cataract and dust turbidity of the vitreous body | - Travoprost, brinzolamide, carteolol, brimonidine - On topical medication–IOP: RE 18 mmHg, LE 32 mmHg | Glaucoma surgery recommended as a necessary treatment option in the future | Significant fluctuations of IOP with pharmacotherapy | |
| Carnevalini et al., 1988 [14] | Case 1: no evidence of glaucoma | ||||||||
| Case 2: open angle glaucoma | 66, M | No | - VA/Optic disc: no data - IOP: 12 mmHg in both eyes | Unilateral, inferiorly in RE | No data | Pilocarpine | Trabeculectomy five years earlier | ||
| Case 3: glaucoma in RE (diagnosed after head trauma) | 55, F | Head trauma 20 years earlier | - VA: RE 6/600 - IOP: RE 14 mmHg, LE 10 mmHg - Optic disc: post-traumatic atrophy in LE | No data | Post-traumatic optic nerve atrophy in LE | Miotics in RE | |||
| Case 4: no data (abstract only) | |||||||||
| Payne and Thomas, 1966 [16] | 79, M | No information | - VA: RE 6/30, LE hand movements - IOP: RE 20 mmHg, LE 35 mmHg (before treatment), later 20 mmHg in both eyes - Optic disc: severe cupping and atrophy in both eyes - Gonioscopy: chamber angles open albeit narrow - Visual fields: 5 to 10 degrees in both eyes | - Bilateral, inferiorly - Iridoschisis following miotic therapy, | Bilateral subcapsular cataract | Pilocarpine and, eventually, epinephrine bitartrate | No | Glaucoma readily controlled with epinephrine bitartrate (as stated by the authors) | |
| Salmon and Murray, 1992 [19] | 12 patients (summary) AAC or ACG | 3 M, aged 54-72 9 F, aged 39-76 | No | - IOP: mean 53 mmHg (range 12-65 mmHg) - In 10 patients with a history of headaches or ocular pain: a. optic discs: evidence of glaucomatous disc damage with a corresponding field defect in 14 eyes from seven patients; no damage to the optic nerve in five eyes from three patients b. gonioscopy: evidence of angle closure, in particular involving the superior angle in all ten patients - In two patients without headaches or ocular pain: a. AAC after pupillary dilation in one case b. closed superior angle with normal optic disc in another case | - Bilateral in 7 patients - Unilateral in 5 patients - Inferiorly in 17 eyes - Superiorly and inferiorly in 2 eyes | - Limited corneal touch in 12 eyes: localized corneal opacity in one eye, decompensated, edematous cornea in one eye, interstitial keratitis in one patient - Clear lenses in two eyes - Lens subluxation in one patient - Nuclear or cortical cataract in all remaining eyes; in some with anterior subcapsular lens opacities (suggestive of previous Glaukomflecken) | - Preoperative topical treatment in all patients (no more information) | - YAG laser peripheral iridotomy in fourteen eyes - Trabeculectomy in three patients after iridotomy - Uniocular implantation of a Molteno tube in one patient despite the treatment mentioned above (persistent increase in intraocular pressure) - Cataract extraction with intraocular lens implantation and iridectomy as primary surgical treatment in two patients (corneal graft simultaneously to cataract extraction in one eye) - Subsequent cataract surgery in further five patients during a five-year follow-up period - Enucleation in one eye (untreated AAC) | Long-term intraocular pressure control was achieved in all patients, although topical pilocarpine was required after peripheral iridotomy in four cases (as stated by the authors) |
| Rodrigues et al., 1983 [20] | Case 1: increased IOP in RE | 87, F | No information | - VA: RE 6/20, LE 6/60 - IOP: RE 24 mmHg, LE 14 mmHg - Optic disc: normal in both eyes - Gonioscopy: open angle (Schaffer grade 2-3 wherever the angle could be visualized | Bilateral, inferiorly | - Iridocorneal touch in both eyes - Bullous keratopathy in LE - Mild bilateral senile macular degeneration | No | Combined corneal transplant, cataract extraction and large sector iridectomy inferiorly in LE | |
| Case 3 | 63, F | No information | - VA: no data - IOP: 22 mmHg in both eyes - Optic disc: early glaucomatous damage in both eyes - Progressive visual field loss - Gonioscopy: narrow anterior chamber angles | Bilateral, inferiorly | Bilateral early cataract | - Pilocarpine and acetazolamide –> increase in IOP to >30 mmHg despite the addition of epinephrine (as stated by the authors) | - Trabeculectomy followed by cataract extraction in LE - Cataract extraction with a wide iridectomy in RE | - unsatisfactory visual result after cataract extraction in LE due to the presence of a friable material from the iris over the anterior vitreous face with occlusion of the pupillary aperture -> vitrectomy with removal of the iris material - Postoperative VA: RE 6/10, LE 6/15, postoperative IOP: RE 15 mmHg, LE 31 mmHg | |
| Case 4 | 51, F | No information | - VA: RE 6/60 -> then, light perception, LE light perception - IOP: RE 24 mmHg, LE 25 mmHg - Optic disc: advanced glaucomatous damage - Gonioscopy: no data | Probably bilateral | Cataract | Pilocarpine and acetazolamide | Filtration surgery | ||
| Case 5 | 72, F | - VA: RE 6/20, LE light perception with projection - IOP: RE 16 mmHg, LE 19 mmHg - Optic disc: RE normal, LE could not be visualized - Gonioscopy: AC angle in RE optically closed secondary to strings of iris stroma; angle slit-like albeit open between the 3 and 6 o’clock positions - AC angle narrow and optically closed superonasally, no definite PAS | Bilateral, inferonasally | Mature cataract in LE and mild cataract in RE | No | Cataract extraction and sector iridectomy in LE | |||
| Case 6 ACG | 65, M | No information | - VA: RE 6/12, LE 6/60 - IOP: RE 8 mm Hg, LE 17 mm Hg - Optic disc: RE c/d = 0.3, LE not visible because of the marked AC reaction - Gonioscopy: narrow AC angle in RE, optically closed AC angle in LE with PAS superiorly | - Bilateral, inferotemporally in RE - More marked in LE: inferiorly, in particular nasally | - Corneal edema and inflammatory reaction (including fibrin, 3+ cells and flare in LE) | - Pilocarpine postoperatively to LE | - Surgical peripheral iridectomy in RE - Laser iridectomy in LE | - Postoperative: IOP in RE 15 mmHg without topical treatment, laser iridectomy closure in LE -> IOP 19 mmHg -> pilocarpine -> peripheral iridectomy inferiorly in the area of the iridoschisis - Final postoperative VA 6/12 in both eyes, Final IOP: RE 16 mmHg, LE 19 mmHg without therapy | |
| Case 2: no evidence of glaucoma | |||||||||
| Minezaki, 2013 [23] | ACG | 79, F | No information | - BCVA: RE hand movements, LE 6/8 - IOP: RE not determined, LE 8 mmHg | - Bullous keratopathy - Virtually nonexistent anterior chamber in RE | - Cataract surgery with iridectomy succeeded to deepen the anterior chamber and to remove the floating iris leaf, although corneal edema remained - NDSAEK four days later resolved corneal edema and restored visual acuity | |||
| Torricelli et al., 2011 [26] | ACG | 55, F | No information | - VA: RE hand movements, LE light perception - IOP: RE 42 mmHg, LE 44 mmHg - Optic disc: edema with no vascular tortuosity and no cup in both eyes - Gonioscopy: narrow angles (Shaffer grade 0) | Bilateral, inferiorly | NAION | Timolol, brimonidine, pilocarpine, prednisolone eye drops, mannitol and acetazolamide | YAG laser iridotomy provided satisfactory IOP control | - Two months later: BCVA RE 6/6, LE 6/60; IOP 11 mmHg in both eyes with no medication; optic disc edema followed by optic disc pallor in both eyes (as stated by the authors) |
| Paniagua et al., 2015 [27] | Iris plateau | 80, F | No | - VA: RE <6/60, LE 6/15 - IOP: 14 mmHg in both eyes - Optic disc: no data - Gonioscopy: slight angle closure (Shaffer grade 2 in both eyes), no PAS - Ultrasonic biomicroscopy: incomplete angle closure in both eyes in all four quadrants caused by the anterior displacement of the ciliary body (iris plateau) | Bilateral, inferonasal quadrants | - Iridocorneal contact - Cortical cataract | No information | No information | |
| Shima et al., 2007 [28] | ACG | 79, M | No information | - VA: RE 6/6, LE 6/5 - IOP: 24 mmHg in both eyes - Optic disc: glaucomatous damage, RE c/d = 0.7, LE c/d = 0.8 - Gonioscopy: narrow angles (Shaffer grade 2) for 270° and scattered PAS in the superior quadrants in both eyes - Goldmann perimetry: temporal arcuate scotoma in both eyes - UBM: typical features of plateau iris configuration | Bilateral, inferiorly | Iridocorneal contact in the inferior quadrants of both eyes | Neither medical treatment with latanoprost, carteolol or pilocarpine eye drops nor laser gonioplasty provided satisfactory IOP control | Combined trabeculotomy and phacoemulsification in both eyes | Postoperative IOP: RE 13 mmHg, LE 11 mmHg with timolol treatment (four months after the surgery) |
| Salmon, 1992 [30] | Case 1: ARG | 54, M | History of facial and ocular trauma at young age | - BCVA: RE 6/20, LE 6/30 - IOP: RE 57 mmHg, LE 58 mmHg - Optic disc: advanced glaucomatous damage in both eyes - Gonioscopy: angle recession 180° in RE and 90° in LE | Bilateral, superior-inferiorly | Corneal edema in RE | IOP was not controlled pharmacologically | - Trabeculectomy in both eyes - Molteno tube in LE, subsequently | Postoperative IOP controlled in both eyes with topical antiglaucoma treatment (four years later) |
| Case 2: ARG | 50, M | History of ocular trauma many years earlier | - VA: RE 6/12 - IOP: RE 40 mmHg - Optic disc: advanced glaucomatous damage in RE - Advanced visual field loss in RE - Gonioscopy: angle recession 110° in RE | Plausibly unilateral, superior-inferiorly | Phthisis in LE | IOP was not controlled pharmacologically | Trabeculectomy in RE | ||
| Pieklarz et al., 2020 [33] | ACG | 47, M with moderate intellectual disability, possible Marfan syndrome | No | - VA: hand motion in both eyes - IOP: RE 34 mmHg, LE 30 mmHg - Optic disc: RE c/d = 0.6, LE c/d = 0.9 (postoperatively) | Bilateral, superior-temporally | - Bilateral temporal lens subluxation - Bilateral mature cataract | Topical antiglaucoma treatment in both eyes | - Pars plana vitrectomy and lensectomy with iris-claw lens implantation in LE complicated by possible uveitis-glaucoma-hyphema syndrome - Uneventful pars plana vitrectomy with lensectomy and intrascleral sutureless intraocular lens fixation (Yamane technique) in RE | Postoperative VA: RE 6/60, LE 6/152; postoperative IOP: RE 17 mmHg, LE 29 mmHg |
| Porteous et al., 2014 [35] | Case 1: AAC in RE | 49, M | No information | - BVCA: RE 6/12, LE 5/6 - IOP: RE 42 mmHg, LE 20 mmHg - AS-OCT: secondary angle closure in both eyes | Bilateral, superiorly and inferiorly | Nuclear cataract in RE | Oral acetazolamide and maximal topical IOP lowering medication in RE reduced IOP to 18 mmHg within 2 h | Uncomplicated cataract extraction in RE | Postoperative BCVA: RE 6/6; postoperative IOP: RE 18 mmHg without medication |
| Case 2: AAC in LE | 62, M | No information | - VA: LE 6/36 - IOP: LE 50 mmHg - Optic disc: LE normal - UBM: crowding of the inferior angle from iris strands | Unilateral, inferiorly in LE | Cataract in LE | - Oral acetazolamide and maximal topical IOP lowering medication reduced IOP within 2 h in LE - Prostaglandin analogue before the surgery | Uncomplicated cataract extraction in LE | Postoperative BCVA: LE 6/12; postoperative IOP: LE 14 mmHg without medication | |
| Agrawal et al., 2001 [36] | ACG in LE; AAC in RE | 50, M | No trauma | - BVCA: RE 6/6, LE 6/12 - IOP: RE 16 mmHg, LE 30 mmHg (despite medication) - Optic disc: normal in LE - Gonioscopy: slit angles in RE, closed angles with multiple PAS in LE - Visual field: normal in RE, generalized depression in LE | Unilateral in LE, inferotemporally; | Inferotemporal lens subluxation in LE | Local and systemic antiglaucoma medication in LE; pilocarpine in RE | - Trabeculectomy in LE - Intracapsular cataract extraction in LE six years later (advanced cataract) | - The patient did not consent for laser iridotomy; IOP and visual fields remained stable thereafter - Three years later, the patient developed AAC in RE as he had discontinued the pilocarpine eyedrops; he resumed to use of the drops - During a follow-up, the iridoschisis, present only in LE, remained unchanged |
| Swaminathan et al., 2017 [44] | Iridoschisis and glaucoma possibly secondary to alkali burn | F, in her early 30′s | Progressive increase in IOP | Probably secondary to alkali burn | - Cataract - Corneal opacification unresponsive to pharmacotherapy | A glaucoma drainage implant in LE without complications, with resultant improvement of IOP control | |||
| You et al., 2017 [47] | Bilateral ACG | 67, F | No | - VA: RE 6/30, LE light perception - IOP: RE 58 mmHg, LE 22 mmHg - Optic disc: RE c/d = 0.8, LE ocular fundus fuzzy - Gonioscopy: AC angle N IV (Scheie classification); PAS detected in 3 out of 4 quadrants via dynamic gonioscopy in RE and in all quadrants in LE | Bilateral, inferiorly | - Cortical cataract in both eyes - Pterygium in LE | - For financial reasons, the patient elected to postpone surgical treatment of LE - four IOP-lowering drugs: pilocarpine, timolol, brinzolamide, and brimonidine in LE | -Goniosynechialysis and phacoemulsification with IOL implantation in RE - Laser peripheral iridotomy in LE | - Postoperative VA: RE 20/33; postoperative IOP RE 11 mmHg - The outcome in this case suggests that laser peripheral iridectomy may provide limited treatment in iridoschisis complicated by ACG triggered by PAS; goniosynechialysis combined with cataract removal seems a better treatment option (as stated by the authors) |
| Gomez Goyeneche et al., 2018 [48] | Case 1 | 70, M | No | - VA: 6/6 in both eyes - IOP: 28 mmHg in both eyes - Optic disc: normal in both eyes - Gonioscopy: closed angle (Shaffer grade 0–1) for 270° in both eyes - Visual field: normal in both eyes | Unilateral, inferior-nasally in RE | Bilateral mild cataract | - An ocular hypotensive agent was initiated | The patient was scheduled for bilateral peripheral laser iridotomy | A 6-month follow-up was scheduled for glaucoma review |
| Case 2: ACG | 72, M | No | - BCVA: RE 6/24, LE CF - IOP: 12 mmHg in both eyes - Optic disc: c/d = 0.9 in both eyes - Gonioscopy: permeable iridotomy and Shaffer grade 3 angles in both eyes | Unilateral, inferior-nasally in LE | - Mature cataract in LE - Pseudophakic RE | No | - The patient was scheduled for trabeculectomy combined with cataract extraction in LE - Past history of iridotomy in RE | ||
| Case 3 | 59, F | No | - BVCA: 6/7.5 in both eyes - IOP: RE 14 mmHg, LE 16 mmHg - Optic disc: normal in both eyes - Gonioscopy: Shaffer grade 2angles | Bilateral, inferior-nasally | - Hyphema in RE - Bilateral mild cataract | No | The patient was scheduled for bilateral peripheral laser iridotomy | A 6-month follow-up was scheduled for glaucoma review |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pieklarz, B.; Grochowski, E.T.; Saeed, E.; Sidorczuk, P.; Mariak, Z.; Dmuchowska, D.A. Iridoschisis—A Systematic Review. J. Clin. Med. 2020, 9, 3324. https://doi.org/10.3390/jcm9103324
Pieklarz B, Grochowski ET, Saeed E, Sidorczuk P, Mariak Z, Dmuchowska DA. Iridoschisis—A Systematic Review. Journal of Clinical Medicine. 2020; 9(10):3324. https://doi.org/10.3390/jcm9103324
Chicago/Turabian StylePieklarz, Barbara, Emil Tomasz Grochowski, Emil Saeed, Patryk Sidorczuk, Zofia Mariak, and Diana Anna Dmuchowska. 2020. "Iridoschisis—A Systematic Review" Journal of Clinical Medicine 9, no. 10: 3324. https://doi.org/10.3390/jcm9103324
APA StylePieklarz, B., Grochowski, E. T., Saeed, E., Sidorczuk, P., Mariak, Z., & Dmuchowska, D. A. (2020). Iridoschisis—A Systematic Review. Journal of Clinical Medicine, 9(10), 3324. https://doi.org/10.3390/jcm9103324