
Efficacy of Invasive and Non-Invasive Methods in Orthodontic Tooth Movement Acceleration: A Systematic Review

 , , and
, , and
Abstract
1. Introduction
1.1. Orthodontic Tooth Movement Description
1.2. Invasive Methods
1.3. Non-Invasive Methods
2. Materials and Methods
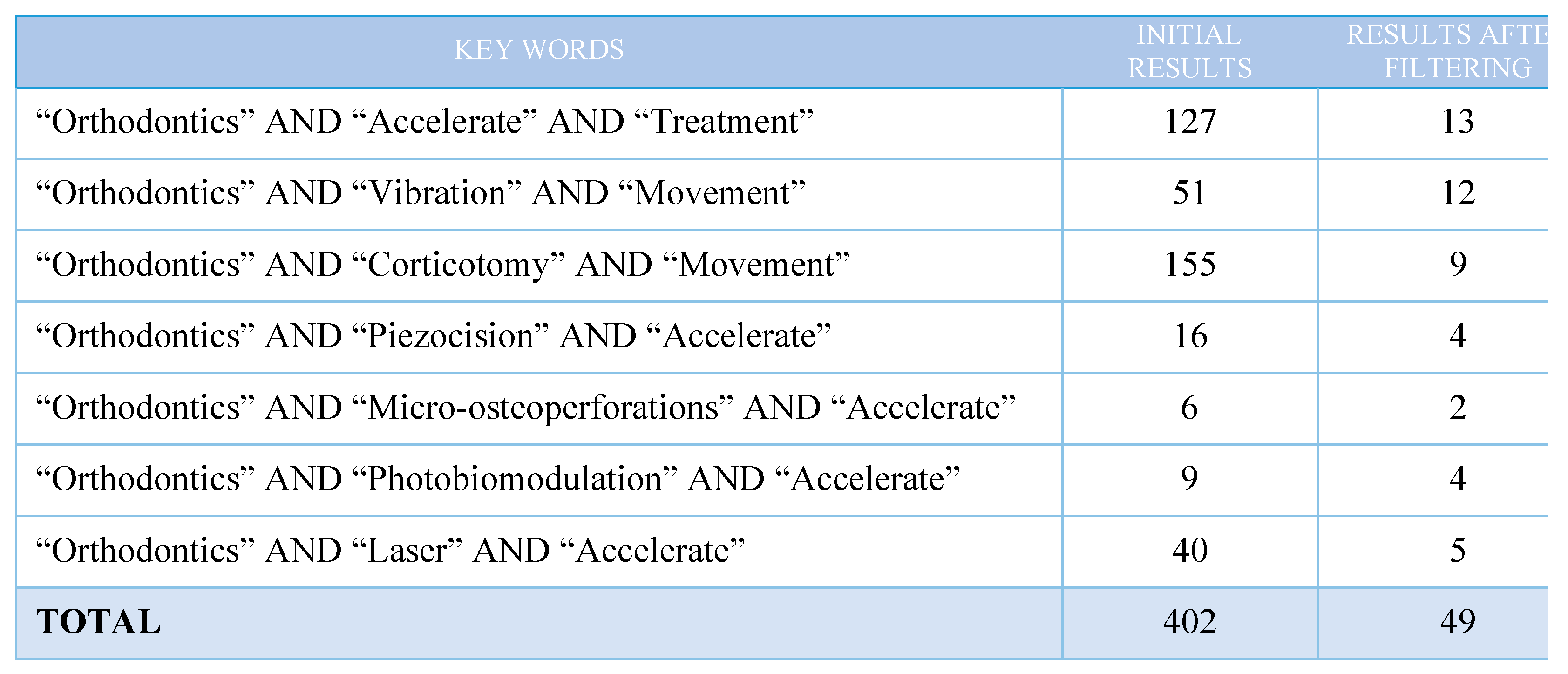
2.1. Search Strategy
2.2. Eligibility Criteria
2.2.1. Inclusion Criteria
- Population: adolescent and adult patients with Class II malocclusion requiring or not requiring the extraction of the maxillary first premolars, biprotrusive patients requiring the extraction of the four first premolars and patients with anterior lower crowding with or without requiring the extraction of the lower first premolars.
- Intervention: various surgical and non-surgical techniques used to accelerate the orthodontic tooth movement.
- Comparison: the control group is made of patients undergoing conventional orthodontic treatment (conventional brackets, self-ligating brackets or aligners) without auxiliary techniques.
- Results: rate of tooth movement in canine/incisor retraction or reduction in anterior upper and/or anterior lower crowding.
- Study Design: randomized controlled trials (RCTs).
2.2.2. Exclusion Criteria
- Studies that were conducted on animals.
- Studies that were conducted more than ten years ago.
- Studies with less than 6 participants.
- Studies other than randomized controlled trials: journal articles, systematic reviews, case reports…
- Studies referring to the acceleration of tooth movement as a result of orthognathic surgery, distraction osteogenesis procedures, electrical currents, pulsed electromagnetic fields and pharmacological approaches.
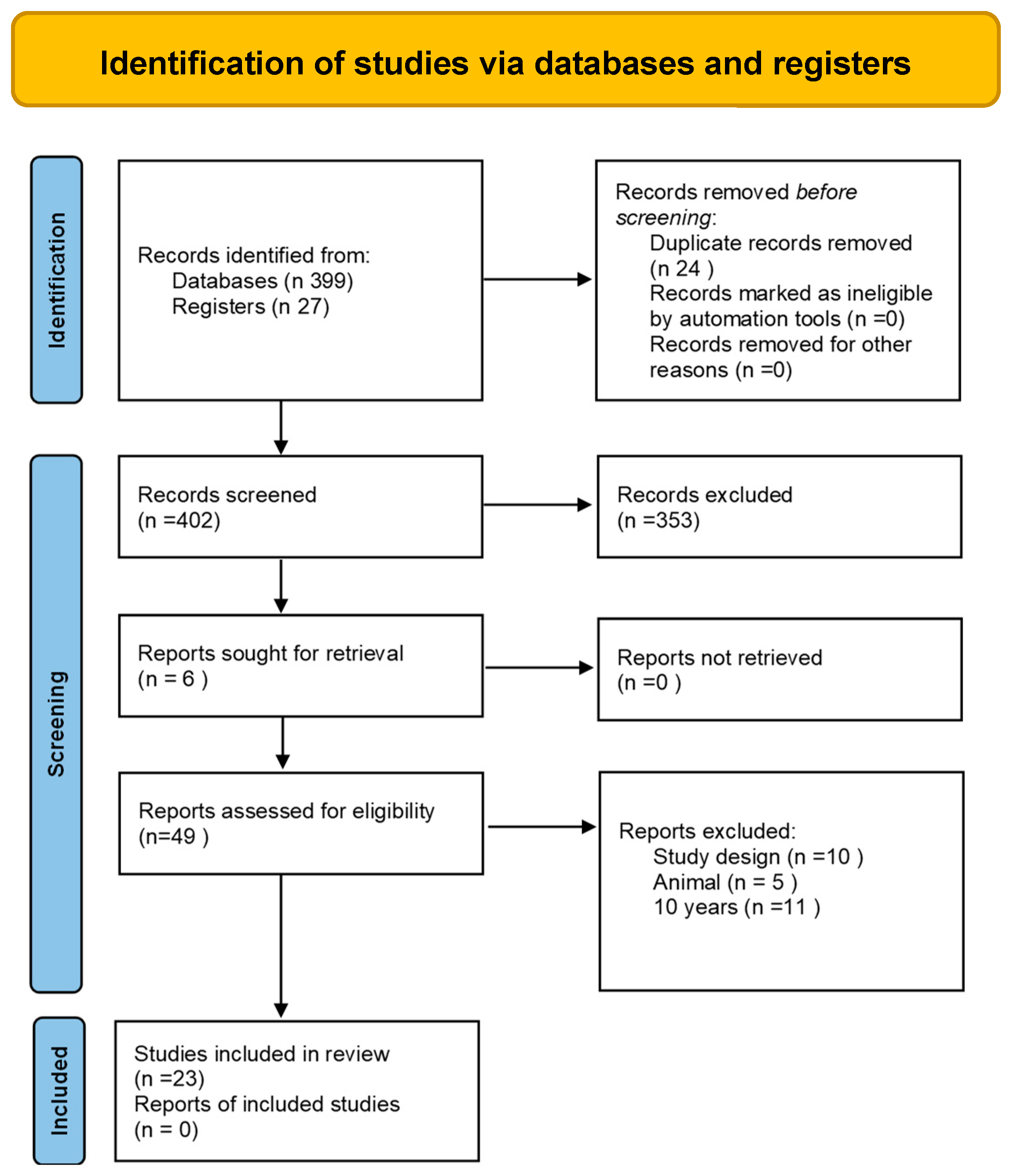
2.3. Study Selection
2.4. Risk of Bias in Individual Studies
3. Results
3.1. Data Extraction and Analysis
3.2. Risk of Bias Assessment
3.3. Description of Interventions
3.3.1. Corticotomies
3.3.2. Piezocision
3.3.3. Micro-Osteoperforations (MOP)
3.3.4. Photobiomodulation
3.3.5. Microvibration
3.4. Effects of Interventions
3.4.1. Corticotomies
3.4.2. Piezocision
3.4.3. Micro-Osteoperforations
3.4.4. Photobiomodulation
3.4.5. Microvibration
4. Discussion
5. Conclusions
- Although the contemporary literature describes numerous methods to accelerate orthodontic tooth movement, in most cases, there is no scientific evidence behind their efficacy, so their success cannot be guaranteed by applying such techniques in daily clinical practice.
- There is some evidence about surgical techniques and photobiomodulation (LLLT and LED laser) being effective in accelerating tooth movement, at least in the short-term. On the contrary, we have not found any evidence to support the effectiveness of the use of microvibration therapy during orthodontic treatment.
- The requirement for further research in the field of orthodontic tooth movement acceleration is evident, with well-designed studies paying attention to optimal application protocols, overall treatment time, potential side effects and cost–benefit analysis based on the specific characteristics of each technique.
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
References
- Tsichlaki, A.; Chin, S.Y.; Pandis, N.; Fleming, P.S. How long does treatment with fixed orthodontic appliances last? A systematic review. Am. J. Orthod. Dentofac. Orthop. 2016, 149, 308–318. [Google Scholar] [CrossRef] [PubMed]
- Mavreas, D.; Athanasiou, A.E. Factors affecting the duration of orthodontic treatment: A systematic review. Eur. J. Orthod. 2008, 30, 386–395. [Google Scholar] [CrossRef] [PubMed]
- Bishara, S.E.; Ostby, A.W. White spot lesions: Formation, prevention, and treatment. Semin. Orthod. 2008, 14, 174–182. [Google Scholar] [CrossRef]
- Segal, G.R.; Schiffman, P.H.; Tuncay, O.C. Meta analysis of the treatment-related factors of external apical root resorption. Orthod. Craniofac Res. 2004, 7, 71–78. [Google Scholar] [CrossRef]
- Royko, A.; Denes, Z.; Razouk, G. The relationship between the length of orthodontic treatment and patient compliance. Fogorvosi Szle. 1999, 92, 79–86. [Google Scholar]
- Gkantidis, N.; Mistakidis, I.; Kouskoura, T.; Pandis, N. Effectiveness of non-conventional methods for accelerated orthodontic tooth movement: A systematic review and meta-analysis. J. Dent. 2014, 42, 1300–1319. [Google Scholar] [CrossRef]
- Huang, H.; Williams, R.C.; Kyrkanides, S. Accelerated orthodontic tooth movement: Molecular mechanisms. Am. J. Orthod. Dentofac. Orthop. 2014, 146, 620–632. [Google Scholar] [CrossRef]
- Krishnan, V.; Davidovitch, Z. On a path to unfolding the biological mechanisms of orthodontic tooth movement. J. Dent. Res. 2009, 88, 597–608. [Google Scholar] [CrossRef]
- Doshi-Mehta, G.; Bhad-Patil, W.A. Efficacy of low-intensity laser therapy in reducing treatment time and orthodontic pain: A clinical investigation. Am. J. Orthod. Dentofac. Orthop. 2012, 141, 289–297. [Google Scholar] [CrossRef]
- Woodhouse, N.R.; DiBiase, A.T.; Johnson, N.; Slipper, C.; Grant, J.; Alsaleh, M.; Donaldson, A.N.A.; Cobourne, M.T. Supplemental vibrational force during orthodontic alignment: A randomized trial. J. Dent. Res. 2015, 94, 682–689. [Google Scholar] [CrossRef]
- Showkatbakhsh, R.; Jamilian, A.; Showkatbakhsh, M. The effect of pulsed electromagnetic fields on the acceleration of tooth movement. World J. Orthod. 2010, 11, 52–56. [Google Scholar]
- Kim, D.H.; Park, Y.G.; Kang, S.G. The effects of electrical current from a microelectrical device on tooth movement. Korean J. Orthod. 2008, 38, 337–345. [Google Scholar] [CrossRef]
- Bartzela, T.; Türp, J.C.; Motschall, E.; Maltha, J.C. Medication effects on the rate of orthodontic tooth movement: A systematic literature review. Am. J. Orthod. Dentofac. Orthop. 2009, 135, 16–26. [Google Scholar] [CrossRef] [PubMed]
- Higgins, J.; Altman, D.; Gøtzsche, P.; Jüni, P.; Moher, D.; Oxman, A.D.; Savovic, J.; Schulz, K.F.; Weeks, L.; Sterne, J.A.C.; et al. The Cochrane collaboration’s tool for assessing risk of bias in randomised trials. Br. Med. J. 2011, 343, 5928. [Google Scholar] [CrossRef] [PubMed]
- Abd ElMotaleb, M.A.; El-Beialy, A.R.; El-Sharaby, F.A.; ElDakroury, A.E.; Eid, A.A. Effectiveness of low frequency vibration on the rate of canine retraction: A randomized controlled clinical trial. Sci. Rep. 2024, 14, 7952. [Google Scholar] [CrossRef]
- Alkebsi, A.; Al-Maaitah, E.; Al-Shorman, H.; Alhaija, E.A. Three-dimensional assessment of the effect of micro-osteoperforations on the rate of tooth movement during canine retraction in adults with class II malocclusion: A randomized controlled clinical trial. Am. J. Orthod. Dentofac. Orthop. 2018, 153, 771–785. [Google Scholar] [CrossRef]
- Alfawal, A.M.H.; Hajeer, M.Y.; Ajaj, M.A.; Hamadah, O.; Brad, B. Evaluation of piezocision and laser-assisted flapless corticotomy in the acceleration of canine retraction: A randomized controlled trial. Head. Face Med. 2018, 14, 4. [Google Scholar] [CrossRef]
- Al-Okla, N.; Bader, D.M.; Makki, L. Effect of photobiomodulation on maxillary decrowding and root resorption: A randomized clinical trial. APOS Trends Orthod. 2019, 8, 200–203. [Google Scholar]
- AlSayed Hasan, M.M.A.; Sultan, K.; Hamadah, O. Low-level laser therapy effectiveness in accelerating orthodontic tooth movement: A randomized controlled clinical trial. Angle Orthod. 2017, 87, 499–504. [Google Scholar] [CrossRef]
- Aboalnaga, A.A.; Salah Fayed, M.M.; El-Ashmawi, N.A.; Soliman, S.A. Effect of micro-osteoperforation on the rate of canine retraction: A split-mouth randomized controlled trial. Prog. Orthod. 2019, 20, 21. [Google Scholar] [CrossRef]
- Babanouri, N.; Ajami, S.; Saleh, P. Effect of mini-screw-facilitated micro-osteoperforation on the rate of orthodontic tooth movement: A single-center, split-mouth, randomized, controlled trial. Prog. Orthod. 2020, 21, 7. [Google Scholar] [CrossRef] [PubMed]
- DiBiase, A.T.; Woodhouse, N.R.; Papageorgiou, S.N.; Johnson, N.; Slipper, C.; Grant, J.; Alsaleh, M.; Khaja, Y.; Cobourne, M.T. Effects of supplemental vibrational force on space closure, treatment duration, and occlusal outcome: A multicenter randomized clinical trial. Am. J. Orthod. Dentofac. Orthop. 2018, 153, 469–480. [Google Scholar] [CrossRef] [PubMed]
- da Matta Cid Pinto Fernandes, L.S.; Figueiredo, D.S.F.; Oliveira, D.D.; Houara, R.G.; Rody, W.J., Jr.; Gribel, B.F.; Soares, R.V. The effects of corticotomy and piezocision in orthodontic canine retraction: A randomized controlled clinical trial. Prog. Orthod. 2021, 22, 37. [Google Scholar] [CrossRef] [PubMed]
- Ghaffar, Y.K.A.; El Sharaby, F.A.; Negm, I.M. Effect of low-level laser therapy on the time needed for leveling and alignment of mandibular anterior crowding. Angle Orthod. 2022, 92, 478–486. [Google Scholar] [CrossRef] [PubMed]
- Gibreal, O.; Hajeer, M.Y.; Brad, B. Efficacy of piezocision-based flapless corticotomy in the orthodontic correction of severely crowded lower anterior teeth: A randomized controlled trial. Eur. J. Orthod. 2018, 41, 188–195. [Google Scholar] [CrossRef]
- Jaber, S.T.; Al-Sabbagh, R.; Hajeer, M.Y. Evaluation of the efficacy of laser-assisted fapless corticotomy in accelerating canine retraction: A split-mouth randomized controlled clinical trial. J. Oral. Maxillofac. Surg. 2022, 26, 81–89. [Google Scholar] [CrossRef]
- Katchooi, M.; Tai, S.; Cohanim, B.; Spiekerman, C.; Huang, G.; Bayirli, B. Effect of supplemental vibration on orthodontic treatment with aligners: A randomized trial. Am. J. Orthod. Dentofac. Orthop. 2018, 153, 336–346. [Google Scholar] [CrossRef]
- Kumar, P.; Rampurawala, A.H.; Patil, A.S. Effect of micro-osteoperforations (MOPs) on the rate of en masse orthodontic tooth retraction. J. Orofac. Orthop. 2024, 85, 189–198. [Google Scholar] [CrossRef]
- Lalnunpuii, H.; Batra, P.; Sharma, K.; Srivastava, A.; Raghavan, S. Comparison of rate of orthodontic tooth movement in adolescent patients undergoing treatment by first bicuspid extraction and en-mass retraction, associated with low level laser therapy in passive self-ligating and conventional brackets: A randomized controlled trial. Int. Orthod. 2020, 18, 412–423. [Google Scholar]
- Miles, P.; Fisher, E. Assessment of the changes in arch perimeter and irregularity in the mandibular arch during initial alignment with the AcceleDent Aura appliance vs. no appliance in adolescents: A single-blind randomized clinical trial. Am. J. Orthod. Dentofac. Orthop. 2016, 150, 928–936. [Google Scholar] [CrossRef]
- Moradinejad, M.; Chaharmahali, R.; Shamohammadi, M.; Mir, M.; Rakhshan, V. Low-level laser therapy, piezocision, or their combination vs. conventional treatment for orthodontic tooth movement: A hierarchical 6-arm split-mouth randomized clinical trial. J. Orofac. Orthop. 2024, 85, 110–122. [Google Scholar] [CrossRef] [PubMed]
- Mordente, C.M.; Oliveira, D.D.; Palomo, J.M.; Cardoso, P.A.; Assis, M.A.L.; Zenóbio, E.G.; Souki, B.Q.; Soares, R.V. The effect of micro-osteoperforations on the rate of maxillary incisors’ retraction in orthodontic space closure: A randomized controlled clinical trial. Prog. Orthod. 2024, 25, 6. [Google Scholar] [CrossRef] [PubMed]
- Qamruddin, I.; Husein, A.; Alam, M.K.; Mahroof, V.; Fida, M.; Khamis, M.F. Effects of lowlevel laser irradiation on the rate of orthodontic tooth movement and associated pain with self-ligating brackets. Am. J. Orthod. Dentofac. Orthop. 2017, 152, 622–630. [Google Scholar] [CrossRef] [PubMed]
- Raghav, P.; Khera, A.K.; Preeti, P.; Jain, S.; Mohan, S.; Tiwari, A. Effect of micro-osteoperforations on the rate of orthodontic tooth movement and expression of biomarkers: A randomized controlled clinical trial. Dent. Press. J. Orthod. 2022, 27, e2219403. [Google Scholar] [CrossRef]
- Sivarajan, S.; Doss, J.G.; Papageorgiou, S.N.; Cobourne, M.T.; Wey, M.C. Mini-implant supported canine retraction with micro-osteoperforation: A split-mouth randomized clinical trial. Angle Orthod. 2019, 89, 183–189. [Google Scholar] [CrossRef]
- Uribe, F.; Davoody, L.; Mehr, R. Efficiency of piezotome-corticision assisted orthodontics in alleviating mandibular anterior crowding-a randomized clinical trial. Eur. J. Orthod. 2017, 39, 595–600. [Google Scholar] [CrossRef]
- Venkatachalapathy, S.; Natarajan, R.; Maheswari, R.U.; Rajakumar, P.; Rangarajan, S.; Patil, D.; Manickavasagam, V. Effect of Frequency of Micro-osteoperforation on Miniscrewsupported Canine Retraction: A Single-centered, Split-mouth Randomized Controlled Trial. J. Contemp. Dent. Pract. 2022, 23, 781–787. [Google Scholar] [CrossRef]
- Vercellotti, T.; Podesta, A. Orthodontic microsurgery: A new surgically guided technique for dental movement. Int. J. Periodontics Restor. Dent. 2007, 27, 324–331. [Google Scholar]
- Hoogeveen, E.J.; Jansma, J.; Ren, Y. Surgically facilitated orthodontic treatment: A systematic review. Am. J. Orthod. Dentofac. Orthop. 2014, 145, 51–64. [Google Scholar] [CrossRef]
- Carvalho-Lobato, P.; Garcia, V.J.; Tallón-Walton, V.; Ustrell-Torrent, J.M.; ManzanaresCéspedes, M.C.; Kasem, K. Tooth movement in orthodontic treatment with low-level laser therapy: A systematic review of human and animal studies. Photomed. Laser Surg. 2014, 32, 302–309. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
|
Author Origin Year Study Design | Technique Used | Primary Objective |
Participants—Total (M/F) Age Control Group Malocclusion | lntervention Protocol | Results and Adverse Effects |
|---|---|---|---|---|---|
| Abd ElMotaleb et al. [15] Egypt 2024 RTC | MV vs. CO | To investigate the effectiveness of AcceleDent Aura vibrating device on the rate of canine retraction. | 32 (0/32) 15/21 16 Patients requiring extraction of upper first premolars and canine retraction. | Intervention group subjects were given AcceleDent devices, which delivered gentle micropulses (0.25 N at 30 Hz). Retraction of the canine was performed using a NiTi coil spring delivering a force of 150 g per side. | No evidence that AcceleDent Aura appliance in conjunction with fixed orthodontic appliance had any effect on acceleration of the rate of canine retraction in the maxillary arch. Pain level could not be reduced by vibrational force with AcceleDent device during orthodontic treatment. Root length was not affected by vibrational forces. |
| Alkebsi et al. [16] Jordan 2018 RTC SM | MOP vs. CO | To investigate the effect of MOP on the rate of tooth movement on canine retraction after the extraction of the premolars. |
| 1.5 mm wide × 3.4 mm deep MOP made with a 1.5 mm diameter and 6 mm long micro-screw in three points distal to the canine. Canine traction with NiTi closed coil springs-150 g force-(begins 6 months after the extraction of the PMs). | No significant differences in the rate of tooth movement between MOP and CG. Sensation of swelling on the first day. |
| Alfawal et al. [17] Syria 2018 RTC SM | G l PZ vs. CO G2 LAFC vs. CO | To evaluate the effectiveness of piezocision and laser-assisted flapless corticotomies when accelerating canine retraction. |
| PZ: two incisions between canine and second PM, 3 mm deep × 10 mm long. LAFC: five perforations between canine and second PM, 3 mm deep, performed with a laser. Canine traction with NiTi closed coil-150 g force-(start of retraction with a 0.19 × 0.25 13-Ti archwire). | Piezocision and laser-assisted flapless corticotomies appear to be effective techniques for canine retraction (it was twice as fast as a conventional retraction in the first month and 1.5 times as fast in the second month). No effect on anchorage loss and canine rotation during retraction. |
| Al-Okla et al. [18] Dubai 2018 RTC | LEO vs. CO | Examine the effect of photobiomodulation on maxillary crowding. |
| Low-level laser with light-emitting diode (OrthoPulse®) of 850 nm wavelength and energy of 0.065 J/cm2. Applied five minutes per dental arch per day for 6 months. |
|
| AISayed et al. [19] Syria 2017 RTC | LLLT vs. ca | Evaluate the efficacy of LLLT in accelerating the movement in crowded maxillary incisors. |
| 830 nm wavelength Ga-Al-As semiconductor laser device with a 2.25- J/cm2 irradiation dose and with an energy of 2 J/point. The laser was applied at the root of each incisor at four points (1 min/tooth) on Days 3, 7 and 14 and then every 15 days until the end of the alignment and leveling stage. | LLLT reduced the time required for alignment and leveling by 26%, making it an effective method for accelerating aTM in cases of dental crowding. No adverse effects. |
| Aboalnaga et al. [20] Egypt 2019 RTC SM | MOP vs. CO | To evaluate the effect of MOP on the rate of orthodontic tooth movement (canine retraction). |
| Three MOP distal to the canine made with a 1.8 mm diameter and 8 mm long micro-screw just before beginning the canine retraction in the center of the extraction space. Canine traction with NiTi coil springs-150 g force-(begins 3 months after the extraction of the PMs). |
|
| Babanouri et al. [21] Iran 2020 RTC SM | Gl: MOP1 vs. CO G2: MOP2 vs. CO | To determine the influence of the number of MOP in the acceleration of orthodontic tooth movement in canine retraction. |
28, which was reduced to 25 Class II division 1 or Class I with biprotrusion, slight or no crowding and requiring the extraction of the first PMs. | MOP 1: three MOP performed on the oral surface. MOP 2: three MOP on the oral surface and three on the palate. MOP are performed with a 1.2 mm diameter micro-screw between the canine distal and in the mesial of the second PM. Canine traction with a NiTi closed coil-150 g force-(start 4 months after the extraction of the PMs). | lncreased the rate of retraction in MOP 1 and MOP 2 with respect to the control sides, being greater in MOP 2. No adverse effects. |
| DiBiase et al. [22] United Kingdom 2017 RTC | MV vs. CO | Learn the effect of supplemental vibrational force on space closure in conventional orthodontic treatment. |
|
The canine retraction was performed with a NiTi coil, and it was started with a 0.19 × 0.25 13-Ti archwire. | There were no differences in the rate of space closure in the mandibular arch between the experimental group and the control group. No benefit from the use of a vibrating device in the rate of mandibular space closure, treatment time or treatment results. |
| Fernandes et al. [23] Brazil 2021 RTC SM | G l: AC vs. CO G2: PZ vs. CO G3: AC vs. PZ | To assess the efficacy of alveolar corticotomy and piezocision when accelerating maxillary canine retraction. |
| AC: vertical incisions in the canine mesial and distal and in the mesial of the second PM. Also, a horizontal corticotomy joining the vertical cuts and additional spherical bone injuries. PZ: three vertical incisions to the mesial and distal of the canine root and the mesial of the second PM (3 mm deep × 5 mm long). Canine retraction: NiTi coil (begins 3 months after the extraction of the PMs). | Alveolar corticotomy and piezocision are not effective at accelerating the maxillary canine retraction. NM |
| Ghaffar et al. [24] Egypt 2022 RTC | LLLT vs. CO | To assess the effect of low-level laser therapy (LLLT) on overall leveling and alignment time of mandibular anterior crowding and associated pain after initial archwire placement. | 32, reduced to 30 (0/30) 18/25 years 16, reduced to 15 Angle Class I malocclusion. Mandibular anterior irregularity index ranging from 4 to 10 mm. | Power Mode Continuous Wavelength 940 6 10 nm Energy density 25.7 J/cm2 per application Power output 2.5 W Application tool Tooth-whitening handpiece (35 mm 3 8 mm) ¼ (2.8 cm2) Application zones and time Labially at the vestibule for 30 s. Laser treatment intervals at d 0, 3, 7, 14 and 30 and then repeated every 2 wks. | LLLT has a potential for acceleration of anterior segment alignment as well as reduction in the pain associated with placement of initial archwires. The mean time for leveling and alignment was significantly lower in the laser group compared to the control group (68.2 6 28.7 and 109.5 6 34.7 days, respectively). |
| Gibreal et al. [25] Syria 2019 RTC | PZ vs. CO | To evaluate the effectiveness of piezocision-assisted flapless corticotomies when accelerating anterior lower alignment. |
|
| Significant increase in anterior lower alignment rate in the group undergoing the piezocision technique. A 59% reduction in time for alignment and leveling. |
| Jaber et al. [26] Syria 2021 RTC SM | LAFC vs. CO | To assess the efficacy of laser-assisted flapless corticotomy when accelerating canine retraction. |
|
| LAFC appears to be an effective method to accelerate canine retraction 1.6 times faster on the experimental side than on the control one (2.5 times faster from weeks 1 to 4, 1.8 times faster from 4 to 8 and no difference from 8 to 12). A mild degree of pain and discomfort. |
| Katchooi et al. [27] Canada 2018 RTC | MV vs. INV | To evaluate the effects of a supplemental vibrating device during treatment with clear aligners in adult patients. |
| 30 Hz and 0.25 N vibrating device (AcceleDent ®). Application for 20 min/day until completing six aligner changes (performed every 7 days). | There is no evidence that the use of a supplemental vibrating device accelerates orthodontic tooth movement. No differences between the experimental group and the control group. |
| Kumar et al. [28] India 2024 RTC | MOP vs. CO | To evaluate the effect of micro-osteoperforations on the rate of orthodontic tooth movement during masse anterior retraction. | 20 (7/13) 18–35 years 10 Skeletal class I bimaxillary dentoalveolar protrusion or class I malocclusion (with dental crowding), with bilateral extraction of maxillary and mandibular first premolars. | MOP were performed mesially and distally to all six anterior teeth in the interdental cortical region on the labial aspect of both arches. MOP were performed at the beginning of space closure (T0) and 1 month after beginning of space closure (T1). En masse retraction was performed with sliding mechanics with a coil spring. | The use of MOP is effective in increasing the rate of en masse tooth retraction in both the maxillary and the mandibular arch. The rate of tooth movement was greater, even in the post-MOP period, as compared to the control group. |
| Lalnunpuii et al. [29] India 2020 RTC | LLLT + CB vs. LLLT + SLB vs. CO | To learn about the efficacy of LLLT when increasing the rate of aTM. |
| 658 nm wavelength Ga-Al-As semiconductor laser device with a 2.29- J/cm2 irradiation dose and with an energy of 2.2 J/point. Applied in 10 points (10 sec/point) of the canine root (five in vestibular and five in palate) on days 0, 3, 7 and 14 and then every 15 days until canine retraction is complete. Canine traction with active laceback ligatures and 150 g force (start with a 0.19 × 0.25 -Ti archwire). | LLLT increases the rate of aTM in adolescent patients with four PM extractions and en masse retraction. There are no differences between the CB and SLB group. No adverse effects. |
| Miles and Fisher [30] Australia 2016 RTC | MV vs. CO | Evaluate the effects of a vibrating device on the anterior alignment of the mandibular arch and the degree of discomfort during it in an adolescent patient. |
| Supplemental vibrating device (AcceleDent ®), 30 Hz, 0.25 N.
| No statistically significant differences between the experimental group and the control group. There was also no difference in pain perception between the device group and the control group. |
| Moradinejad et al. [31] Iran 2024 RTC | G1: LLT vs. CO (n22) G2: LLT + PZ vs. Co (n22) G3: PZ vs. CO (n20) | To assess the effect of LLLT, PZ or a combination on accelerating canine retraction. | 64 NM 64 Class II requiring tooth extraction of first upper PMs. | LLLT (940 nm, 8 J, 0.5 W, 16 s, 12 sites), piezocision and LLLT + piezocision. | All three methods accelerated orthodontic tooth movements, with the combination of LLLT + piezocision producing the strongest and LLLT producing the weakest acceleration. |
| Mordente et al. [32] Brazil 2024 RTC SM | MOP vs. CO | To evaluate the impact of MOP on the retraction rate of the upper incisors and space closure rate over a 4-month period | 42, reduced to 37 (17/20) 24.3 ± 8.1 21 Class I or II (ANB < 7º) requiring extraction of first maxillary PMs. | All MOP were performed only once and on the same day that the maxillary incisors’ retraction was begun. Closed nickel-titanium (Ni–Ti) springs (Sentalloy 200 g, Dentsply/ GAC, York, PA, USA) with 200 g of force were connected from the hooks to the TADs bilaterally. | MOP did not accelerate the retraction of the maxillary incisors, nor were they associated with greater incisor inclination or root resorption. |
| Qamruddin et al. [33] Pakistan 2017 RTC SM | LLLT vs. CO | To evaluate the effect of LLLT applied at three-week intervals on aTM and associated pain using SLB. |
| 940 nm wavelength Ga-Al-As semiconductor laser device with an energy of 7.S J/cm2. Applied in 10 points (3 s/point) around the canine root (five in vestibular and five in palatal) every 3 weeks for three visits. Canine traction with coil 150 g force (start with a 0.19 × 0.25 -Ti archwire). | LLLT applied every 3 weeks accelerates aTM and reduces pain associated with it. Canine retraction was greater on the side undergoing the laser procedure (1.6 ± 0.38 mm) compared to the control side (0.79 ± 0.35 mm). |
| Raghav et al. [34] India 2020 | MOP vs. CO | To evaluate the effectiveness of micro-osteoperforations on the rate of canine retraction and expression of biomarkers in gingival crevicular fluid. |
| Three perforations distal to canine root, with a perforation width and depth of 2 and 5 mm, respectively, under copious saline irrigation. Canine retraction was performed on 0.019 × 0.025 in stainless-steel wire with a NiTi closed coil spring (GAC international), and a force of 150 g was used. | Micro-ostoperforation increased the rate of tooth movement only for the first 4 weeks; thereafter, no effect was observed on the rate of canine retraction during 8, 12 and 16 weeks. |
| Sivarajan et al. [35] Malasya 2019 | Group 1 (MOP 4-weekly maxilla/8-weekly mandible) Group 2 (MOP 8-weekly maxilla/12-weekly mandible) Group 3 (MOP 12-weekly maxilla/4-weekly mandible) vs. CO | To investigate the effect of micro-osteoperforation (MOP) on mini-implant-supported canine retraction using fixed appliances. | 30 (7/23) 22.2 ± 3.72 years 30 Class I or II/III incomplete and extraction of all four first premolar teeth as part of the orthodontic treatment. | Three separate MOP were made directly through the buccal mucosa adjacent to the extraction site in a vertical direction 2 mm apart and 3 mm in depth (measured using a rubber stopper) using an Orlus screw (Ortholution.com), width 1.6 mm and length 6 mm. | MOP was associated with statistically significantly increased overall canine retraction of 1.1 mm over a 16-week period of observation. There were only small differences in tooth movement when intervals of 4, 8 and 12 week MOP were used. Moderate pain was associated with MOP at 4-week intervals, while only mild pain was perceived for intervals of 8 and 12 weeks. |
| Uribe et al. [36] USA 2017 | PZ vs. CO | To evaluate the alignment rate of mandibular crowding with piezocision compared to CO. |
|
| There is no evidence that piezotome corticision is effective at relieving anterior mandibular crowding. There were no complications. |
| Venkatachalapathy et al. [37] India 2022 | MOP vs. CO | To evaluate the increase in the rate of tooth movement by increasing the number and frequency of micro-osteoperforations (MOP) | 20 (NM) 15/25 years 20 Class I molar canine relationship and bimaxillary protrusion that required the removal of both maxillary and mandibular first premolars. | Micro-osteoperforations were performed without any flap elevation. The MOP in the center of the socket were placed at a height of 5, 10 and 15 mm from the alveolar crest, respectively, and two MOP were placed at a height of 7 and 12 mm distal to the canine, whereas the control site did not receive any MOP. A NiTi closed coil spring was placed between the TAD and the serpentine hook. | MOP increased the rate of canine retraction by 2-fold when compared with the control group. |
| Random Sequence Generation (Selection Bias) | Allocation Concealment (Selection Bias) | Blinding of Participants and Personnel (Performance Bias) | Blinding of Outcome Assessment (Detection Bias) | Incomplete Outcome Data (Attrition Bias) | Selective Reporting (Reporting Bias) | Other Bias | |
|---|---|---|---|---|---|---|---|
| Abd ElMotaleb et al. [15] Egypt 2024 |  | |  | | | | |
|
Alkebsi et al. [16] Jordan 2018 | | |  | | | | |
|
Alfawal et al. [17] Syria 2018 | | | | | | | |
| Al-Okla et al. [18] Dubai 2018 | | | | | | | |
|
AISayed et al. [19] Syria 2017 | | | | | | | |
| Aboalnaga et al. [20] Egypt 2019 | | | | | | | |
| Babanouri et al. [21] lran 2020 | | | | | | | |
| DiBiase et al. [22] United Kingdom 2017 | | | | | | | |
|
Fernandes et al. [23] Brazil 2021 | | | | | | | |
| Ghaffar et al. [24] Egypt 2022 | | | | | | | |
|
Gibreal et al. [25] Syria 2019 | | | | | | | |
|
Jaber et al. [26] Syria 2021 | | | | | | | |
|
Katchooi et al. [27] Canada 2018 | | | | | | | |
| Kumar et al. [28] India 2024 | | | | | | | |
|
Lalnunpuii et al. [29] India 2020 | | | | | | | |
| Miles and Fisher [30] Australia 2016 | | | | | | | |
| Moradinejad et al [31] Iran 2024 | | | | | | | |
| Mordente et al. [32] Brazil 2024 | | | | | | | |
|
Qamruddin et al. [33] Pakistan 2017 | | | | | | | |
| Raghav et al. [34] India 2020 | | | | | | | |
| Sivarajan et al. [35] Malasya 2019 | | | | | | | |
|
Uribe et al. [36] USA 2017 | | | | | | | |
| Venkatachalapathy et al. [37] India 2022 | | | | | | | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Castillo-Montaño, L.; Colino-Gallardo, P.; Baptista-Sanchez, H.; Drewling, I.; Alvarado-Lorenzo, M.; Antonio-Zancajo, L.; Colino-Paniagua, C. Efficacy of Invasive and Non-Invasive Methods in Orthodontic Tooth Movement Acceleration: A Systematic Review. Appl. Sci. 2024, 14, 10700. https://doi.org/10.3390/app142210700
Castillo-Montaño L, Colino-Gallardo P, Baptista-Sanchez H, Drewling I, Alvarado-Lorenzo M, Antonio-Zancajo L, Colino-Paniagua C. Efficacy of Invasive and Non-Invasive Methods in Orthodontic Tooth Movement Acceleration: A Systematic Review. Applied Sciences. 2024; 14(22):10700. https://doi.org/10.3390/app142210700
Chicago/Turabian StyleCastillo-Montaño, Laura, Pedro Colino-Gallardo, Hugo Baptista-Sanchez, Isabel Drewling, Mario Alvarado-Lorenzo, Laura Antonio-Zancajo, and Carlos Colino-Paniagua. 2024. "Efficacy of Invasive and Non-Invasive Methods in Orthodontic Tooth Movement Acceleration: A Systematic Review" Applied Sciences 14, no. 22: 10700. https://doi.org/10.3390/app142210700
APA StyleCastillo-Montaño, L., Colino-Gallardo, P., Baptista-Sanchez, H., Drewling, I., Alvarado-Lorenzo, M., Antonio-Zancajo, L., & Colino-Paniagua, C. (2024). Efficacy of Invasive and Non-Invasive Methods in Orthodontic Tooth Movement Acceleration: A Systematic Review. Applied Sciences, 14(22), 10700. https://doi.org/10.3390/app142210700