A Systematic Review: Family Support Integrated with Diabetes Self-Management among Uncontrolled Type II Diabetes Mellitus Patients

Abstract
:1. Introduction
2. Objective
3. Methods
3.1. Eligibility Criteria
3.2. Search Strategy
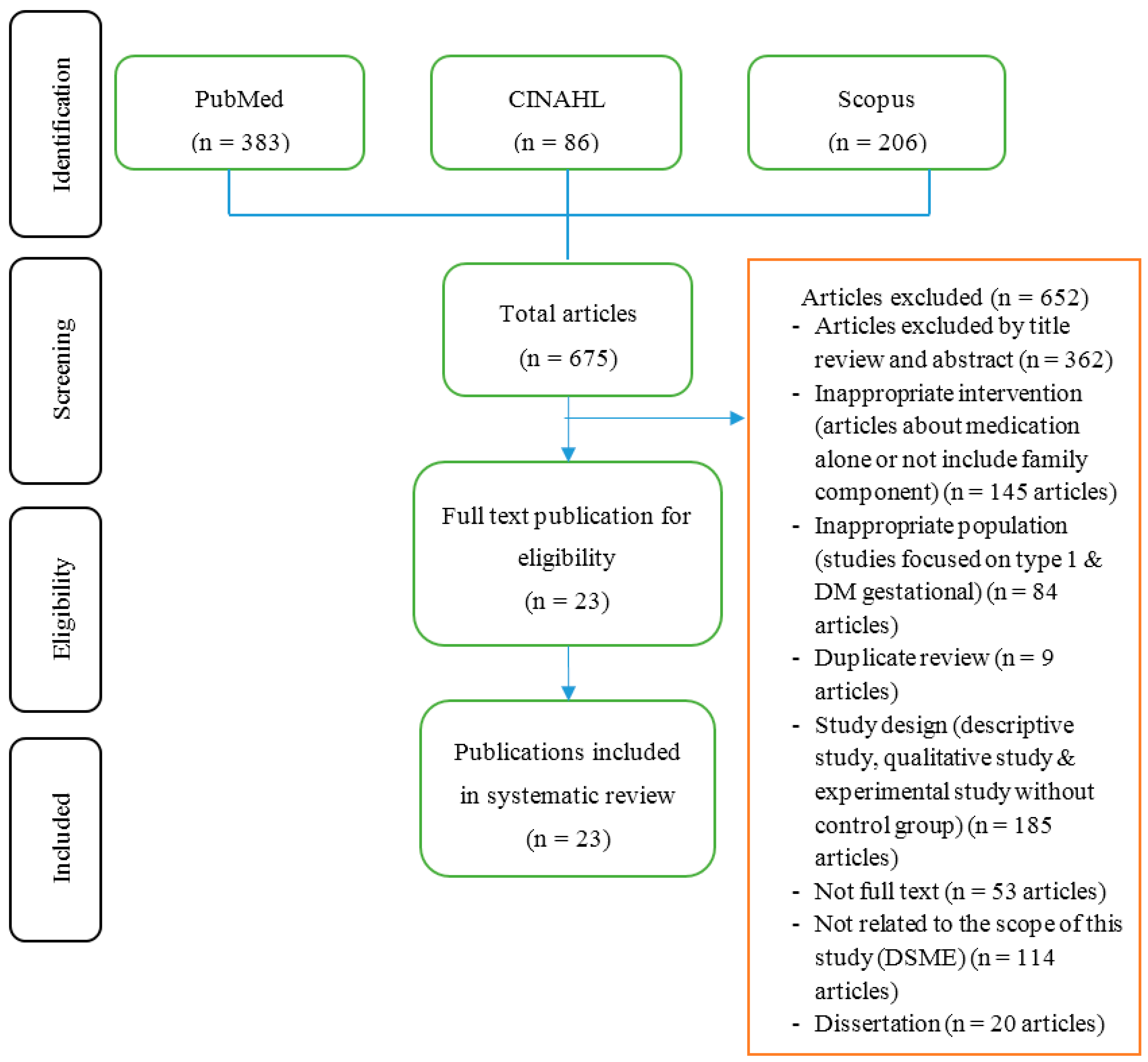
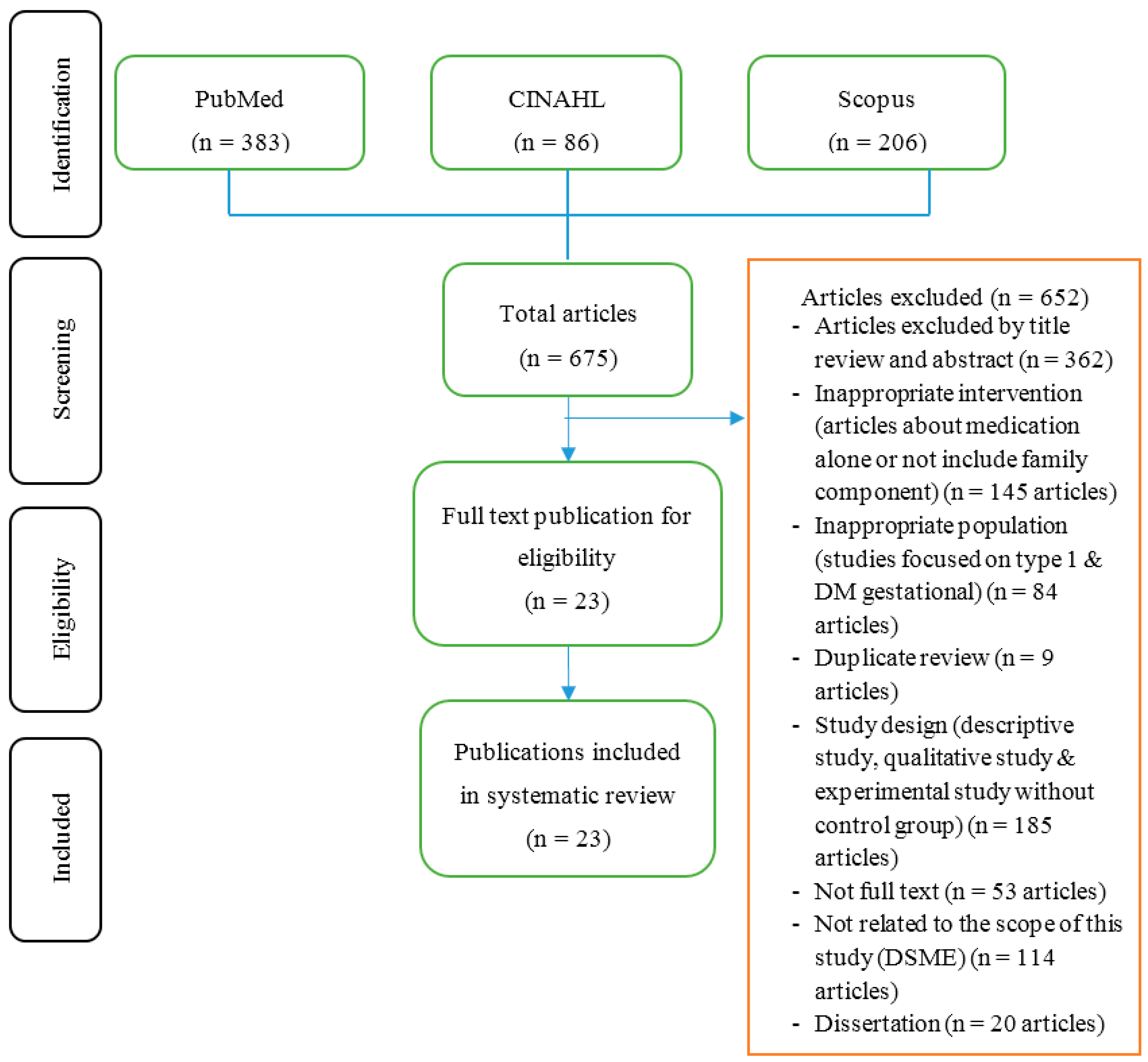
3.3. Study Selection
3.4. Synthesis of Results
4. Results
4.1. DM Self-Management Education (DSME)
4.1.1. Teaching Strategy
4.1.2. Educational Materials
4.1.3. Follow-Up
4.2. Integration of Family Support in the DSME Program
4.3. Effectiveness of Family Support Integration on Diabetes Outcomes
4.3.1. Self-Management Behavior Outcomes
4.3.2. Psychological Outcomes
4.3.3. Self-Efficacy
4.3.4. Social Support Perceived
4.3.5. Clinical Outcomes
5. Discussion
6. Strength & Limitations
7. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- American Diabetes Association. Foundations of care: Education, nutrition, physical activity, smoking cessation, psychosocial care, and immunization. Diabetes Care 2015, 38, S20–S30. [Google Scholar]
- Abdullah, N.; Attia, J.; Oldmeadow, C.; Scott, R.J.; Holliday, E.G. The architecture of risk for type 2 diabetes: Understanding Asia in the context of global findings. Int. J. Endocrinol. 2014, 1–21. [Google Scholar] [CrossRef] [PubMed]
- American Diabetes Association. Standards of medical care in diabetes—2014. Diabetes Care 2014, 37 (Suppl. 1), S14–S80. [Google Scholar]
- Radin, M.S. Pitfalls in hemoglobin A1c measurement: When results may be misleading. J. Gen. Int. Med. 2014, 29, 388–394. [Google Scholar] [CrossRef] [PubMed]
- American Diabetes Association. Standards of Medical Care in Diabetes. Diabetes Care 2013, 40 (Suppl. 1), S11–S66. [Google Scholar]
- Long, A.N.; Dagogo-Jack, S. Comorbidities of diabetes and hypertension: Mechanisms and approach to target organ protection. J. Clin. Hypertens. 2011, 13, 244–251. [Google Scholar] [CrossRef] [PubMed]
- Zulman, D.M.; Rosland, A.M.; Choi, H.; Langa, K.M.; Heisler, M. The influence of diabetes psychosocial attributes and self-management practices on change in diabetes status. Patient Educ. Couns. 2012, 87, 74–80. [Google Scholar] [CrossRef] [PubMed]
- Shrivastava, S.R.; Shrivastava, P.S.; Ramasamy, J. Role of self-care in management of diabetes mellitus. J. Diabetes Metab. Disord. 2013, 12, 14. [Google Scholar] [CrossRef] [PubMed]
- Tong, W.T.; Vethakkan, S.R.; Ng, C.J. Why do some people with type 2 diabetes who are using insulin have poor glycaemic control? A qualitative study. BMJ Open 2015, 5, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Miller, T.A.; Dimatteo, M.R. Importance of family/social support and impact on adherence to diabetic therapy. Diabetes Metab. Syndr. Obes. Targets Ther. 2013, 6, 421–426. [Google Scholar] [CrossRef] [PubMed]
- Wong-Rieger, D.; Rieger, F.P. Health coaching in diabetes: Empowering patients to self-manage. Can. J. Diabetes 2013, 37, 41–44. [Google Scholar] [CrossRef] [PubMed]
- Wagner, E.H.; Austin, B.T.; Davis, C.; Hindmarsh, M.; Schaefer, J.; Bonomi, A. Improving Chronic Illness Care: Translating Evidence into Action. Health Aff. 2001, 20, 64–78. [Google Scholar] [CrossRef]
- Baig, A.A.; Benitez, A.; Quinn, M.T.; Burnet, D.L. Family interventions to improve diabetes outcomes for adults. Ann. N. Y. Acad. Sci. 2015, 1353, 89–112. [Google Scholar] [CrossRef] [PubMed]
- Institute Joanna Briggs. Joanna Briggs Institute Reviewers’ Manual 2014 Edition; The Joanna Briggs Institute Publisher: Adelaide, Austrialia, 2014. [Google Scholar]
- Wild, S.H.; Hanley, J.; Lewis, S.C.; McKnight, J.A.; McCloughan, L.B.; Padfield, P.L.; Parker, R.A.; Paterson, M.; Pinnock, H.; Sheikh, A.; et al. Supported Telemonitoring and Glycemic Control in People with Type 2 Diabetes: The Telescot Diabetes Pragmatic Multicenter Randomized Controlled Trial. PLoS Med. 2016, 13, e1002098. [Google Scholar]
- Aikens, J.E.; Rosland, A.M.; Piette, J.D. Improvements in illness self-management and psychological distress associated with telemonitoring support for adults with diabetes. Prim. Care Diabetes 2015, 9, 127–134. [Google Scholar] [CrossRef] [PubMed]
- Hu, J.; Wallace, D.C.; McCoy, T.P.; Amirehsani, K.A. A family-based diabetes intervention for Hispanic adults and their family members. Diabetes Educ. 2014, 40, 48–59. [Google Scholar] [CrossRef] [PubMed]
- Hamidreza, K.T.; Farah, M.; Mohsen, K.N.; Mohsen, H.; Gholamhossein, M. Impact of family support improvement behaviors on anti diabetic medication adherence and cognition in type 2 diabetic patients. J. Diabetes Metab. Disord. 2014, 13, 6. [Google Scholar]
- Fall, E.; Roche, B.; Izaute, M.; Batisse, M.; Tauveron, I.; Chakroun, N. A brief psychological intervention to improve adherence in type 2 diabetes. Diabetes Metab. 2013, 39, 432–438. [Google Scholar] [CrossRef] [PubMed]
- Robling, M.; McNamara, R.; Bennert, K.; Butler, C.C.; Channon, S.; Cohen, D.; Crowne, E.; Hambly, H.; Hawthorne, K.; Hood, K.; et al. The effect of the Talking Diabetes consulting skills intervention on glycaemic control and quality of life in children with type 1 diabetes: Cluster randomised controlled trial (DEPICTED study). BMJ 2012, 344, e2359. [Google Scholar] [CrossRef] [PubMed]
- Sinclair, K.A.; Makahi, E.K.; Shea-Solatorio, C.; Yoshimura, S.R.; Townsend, C.K.; Kaholokula, J.K. Outcomes from a diabetes self-management intervention for Native Hawaiians and Pacific People: Partners in Care. Ann. Behav. Med. Publ. Soc. Behav. Med. 2013, 45, 24–32. [Google Scholar] [CrossRef] [PubMed]
- Keogh, K.M.; Smith, S.M.; White, P.; McGilloway, S.; Kelly, A.; Gibney, J.; O’Dowd, T. Psychological Family Intervention for Poorly Controlled Type 2 Diabetes. Am. J. Manag. Care 2011, 17, 105–113. [Google Scholar] [PubMed]
- Kang, C.M.; Chang, S.C.; Chen, P.L.; Liu, P.F.; Liu, W.C.; Chang, C.C.; Chang, W. Comparison of family partnership intervention care vs. conventional care in adult patients with poorly controlled type 2 diabetes in a community hospital: A randomized controlled trial. Int. J. Nurs. Stud. 2010, 47, 1363–1373. [Google Scholar] [CrossRef] [PubMed]
- Kluding, P.M.; Singh, R.; Goetz, J.; Rucker, J.; Bracciano, S.; Curry, N. Feasibility and effectiveness of a pilot health promotion program for adults with type 2 diabetes: Lessons learned. Diabetes Educ. 2010, 36, 595–602. [Google Scholar] [CrossRef] [PubMed]
- Garcia-Huidobro, D.; Bittner, M.; Brahm, P.; Puschel, K. Family intervention to control type 2 diabetes: A controlled clinical trial. Fam. Pract. 2011, 28, 4–11. [Google Scholar] [CrossRef] [PubMed]
- Vincent, D. Culturally tailored education to promote lifestyle change in Mexican Americans with type 2 diabetes. J. Am. Acad. Nurse Pract. 2009, 21, 520–527. [Google Scholar] [CrossRef] [PubMed]
- Rosal, M.C.; Ockene, I.S.; Restrepo, A.; White, M.J.; Borg, A.; Olendzki, B.; Scavron, J.; Candib, L.; Welch, G.; Reed, G. Randomized trial of a literacy-sensitive, culturally tailored diabetes self-management intervention for low-income latinos: Latinos en control. Diabetes Care 2011, 34, 838–844. [Google Scholar] [CrossRef] [PubMed]
- Garcia, A.A.; Brown, S.A.; Horner, S.D.; Zuniga, J.; Arheart, K.L. Home-based diabetes symptom self-management education for Mexican Americans with type 2 diabetes. Health Educ. Res. 2015, 30, 484–496. [Google Scholar] [CrossRef] [PubMed]
- John, D.P.; Ananda, S.; James, E.A. Randomized Controlled Trial of mHealth Telemonitoring with Enhanced Caregiver Support for Diabetes Self-management. J. Clin. Trials 2014, 4, 194. [Google Scholar]
- Toobert, D.J.; Strycker, L.A.; Barrera, M., Jr.; Osuna, D.; King, D.K.; Glasgow, R.E. Outcomes from a multiple risk factor diabetes self-management trial for Latinas: Inverted exclamation markViva Bien! Ann. Behav. Med. 2011, 41, 310–323. [Google Scholar] [CrossRef] [PubMed]
- Toobert, D.J.; Strycker, L.A.; Glasgow, R.E.; Osuna, D.; Doty, A.T.; Barrera, M.; Geno, C.R.; Ritzwoller, D.P. ¡Viva Bien!: Overcoming Recruitment Challenges in a Multiple-Risk-Factor Diabetes Trial. Am. J. Health Behav. 2010, 34, 432–441. [Google Scholar] [CrossRef] [PubMed]
- Gary, T.L.; Batts-Turner, M.; Yeh, H.-C.; Hill-Briggs, F.; Bone, L.R.; Wang, N.-Y.; Levine, D.M.; Powe, N.R.; Saudek, C.D.; Hill, M.N.; et al. The Effects of a Nurse Case Manager and a Community Health Worker Team on Diabetic Control, Emergency Department Visits, and Hospitalizations Among Urban African Americans With Type 2 Diabetes Mellitus. Arch. Intern. Med. 2009, 169, 1788–1794. [Google Scholar] [CrossRef] [PubMed]
- Utz, S.W.; Williams, I.C.; Jones, R.; Hinton, I.; Alexander, G.; Yan, G.; Moore, C.; Blankenship, J.; Steeves, R.; Oliver, M.N. Culturally tailored intervention for rural African Americans with type 2 diabetes. Diabetes Educ. 2008, 34, 854–865. [Google Scholar] [CrossRef] [PubMed]
- Toobert, D.J.; Strycker, L.A.; King, D.; Barrera, M., Jr.; Osuna, D.; Glasgow, R. Long-term outcomes from a multiple-Risk-Factor Diabetes Trial for Latinas: ¡Viva Bien! Behav. Med. Pract Policy Res. 2011, 1, 416–426. [Google Scholar] [CrossRef] [PubMed]
- Tang, T.S.; Funnell, M.M.; Sinco, B.; Spencer, M.S.; Heisler, M. Peer-Led, Empowerment-Based Approach to Self-Management Efforts in Diabetes (PLEASED): A Randomized Controlled Trial in an African American Community. Ann. Fam. Med. 2015, 1, 27–35. [Google Scholar] [CrossRef] [PubMed]
- Tai, J.M.; Jerica, M.B.; Peter, H.; Betty, G.; Nan, L.-W.; Sheila, W.; Steve, B. The Family Education Diabetes Series (FEDS): Community-based participatory research with a midwestern American Indian community. Nurs. Inq. 2010, 17, 359–372. [Google Scholar]
- Williams, I.C.; Utz, S.W.; Hinton, I.; Yan, G.; Jones, R.; Reid, K. Enhancing diabetes self-care among rural African Americans with diabetes: Results of a two-year culturally tailored intervention. Diabetes Educ. 2014, 40, 231–239. [Google Scholar] [CrossRef] [PubMed]
- Aikens, J.E.; Zivin, K.; Trivedi, R.; Piette, J.D. Diabetes self-management support using mHealth and enhanced informal caregiving. J. Diabetes Complicat. 2014, 28, 171–176. [Google Scholar] [CrossRef] [PubMed]
- Sassmann, H.; de Hair, M.; Danne, T.; Lange, K. Reducing stress and supporting positive relations in families of young children with type 1 diabetes: A randomized controlled study for evaluating the effects of the DELFIN parenting program. BMC Pediatr. 2012, 12, 152. [Google Scholar] [CrossRef] [PubMed]
- Rosland, A.M.; Piette, J.D. Emerging models for mobilizing family support for chronic disease management: A structured review. Chronic Illn. 2010, 6, 7–21. [Google Scholar] [CrossRef] [PubMed]
- Islam, N.S.; Tandon, D.; Mukherji, R.; Tanner, M.; Ghosh, K.; Alam, G.; Haq, M.; Rey, M.J.; Trinh-Shevrin, C. Understanding barriers to and facilitators of diabetes control and prevention in the New York City Bangladeshi community: A mixed-methods approach. Am. J. Public Health. 2012, 102, 486–490. [Google Scholar] [CrossRef] [PubMed]
- Trief, P.; Sandberg, J.G.; Ploutz-Snyder, R.; Brittain, R.; Cibula, D.; Scales, K.; Weinstock, R.S. Promoting couples collaboration in type 2 diabetes: The diabetes support project pilot data. Fam. Syst. Health 2011, 29, 253–261. [Google Scholar] [CrossRef] [PubMed]
- Chomsky, N. What is Special About Language? University of Arizona: Tucson, AZ, USA, 2012. [Google Scholar]

{kind=link}
| References | Design | Component of DSME | Integration of Family Support in DSME | Follow-Up | Education Materials | Outcomes |
|---|---|---|---|---|---|---|
| Wild (2016) [15] | Randomized control trial (RCT) |
|
|
|
|
|
| Garcia (2015) [28] | Randomized control trial (RCT) |
|
|
|
|
|
| Aikens (2015) [16] | Randomized control trial (RCT) |
|
|
|
|
|
| Tang (2015) [35] | Randomized control trial (RCT) |
|
|
| Not mentioned |
|
| Hu (2014) [17] | Quasi-experimental |
|
|
|
|
|
| John et al., (2014) [29] | Randomized control trial (RCT) |
|
|
|
|
|
| Hamidreza (2014) [18] | Randomized control trial (RCT) |
|
|
| Not mentioned |
|
| William et al., (2014) [37] | A quasi-experiment |
|
|
|
|
|
| Fall (2013) [19] | Randomized control trial (RCT) |
| Not mentioned | Not mentioned | Not mentioned |
|
| Robling et al., (2012) [20] | Cluster randomized controlled trial |
|
|
|
|
|
| Sinclair (2013) [21] | Randomized control trial (RCT) |
|
|
|
|
|
| Toobert (2010) [30] Tobert (2011a) [31] | Randomized control trial (RCT)Randomized control trial (RCT) |
|
|
| Not mentioned |
|
| Rosal (2011) [27] | Randomized control trial (RCT) |
|
|
|
|
|
| Keogh (2011) [22] | Randomized control trial (RCT) |
|
|
| Not mentioned |
|
| Kang (2010) [23] | Randomized control trial (RCT) |
|
|
|
|
|
| Tai (2010) [36] | Mix methods |
|
|
| Not mentioned |
|
| Kluding (2010) [24] | Pretest-posttest single group |
|
| Not mentioned |
|
|
| García-Huidobro (2011) [25] | Randomized control trial (RCT) |
|
|
|
|
|
| Gary (2009) [32] | Randomized control trial (RCT) |
|
|
| Not mentioned |
|
| Vincent (2008) [26] | Randomized control trial (RCT) |
|
|
| Not mentioned |
|
| Utz (2008) [33] | Randomized control trial (RCT) |
|
|
|
|
|
| Islam et al., (2012) [41] | Mix method |
|
|
| Not mentioned |
|
© 2017 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pamungkas, R.A.; Chamroonsawasdi, K.; Vatanasomboon, P. A Systematic Review: Family Support Integrated with Diabetes Self-Management among Uncontrolled Type II Diabetes Mellitus Patients. Behav. Sci. 2017, 7, 62. https://doi.org/10.3390/bs7030062
Pamungkas RA, Chamroonsawasdi K, Vatanasomboon P. A Systematic Review: Family Support Integrated with Diabetes Self-Management among Uncontrolled Type II Diabetes Mellitus Patients. Behavioral Sciences. 2017; 7(3):62. https://doi.org/10.3390/bs7030062
Chicago/Turabian StylePamungkas, Rian Adi, Kanittha Chamroonsawasdi, and Paranee Vatanasomboon. 2017. "A Systematic Review: Family Support Integrated with Diabetes Self-Management among Uncontrolled Type II Diabetes Mellitus Patients" Behavioral Sciences 7, no. 3: 62. https://doi.org/10.3390/bs7030062
APA StylePamungkas, R. A., Chamroonsawasdi, K., & Vatanasomboon, P. (2017). A Systematic Review: Family Support Integrated with Diabetes Self-Management among Uncontrolled Type II Diabetes Mellitus Patients. Behavioral Sciences, 7(3), 62. https://doi.org/10.3390/bs7030062