
Pituitary Adenoma in the Philippines: A Scoping Review on the Treatment Gaps, Challenges, and Current State of Care

 ,
, 
Abstract

1. Introduction
2. Methods
2.1. Protocol
2.2. Eligibility Criteria
2.3. Information/Data Sources
2.4. Search and Selection of Sources
2.5. Charting of Data and Synthesis of Results
3. Results
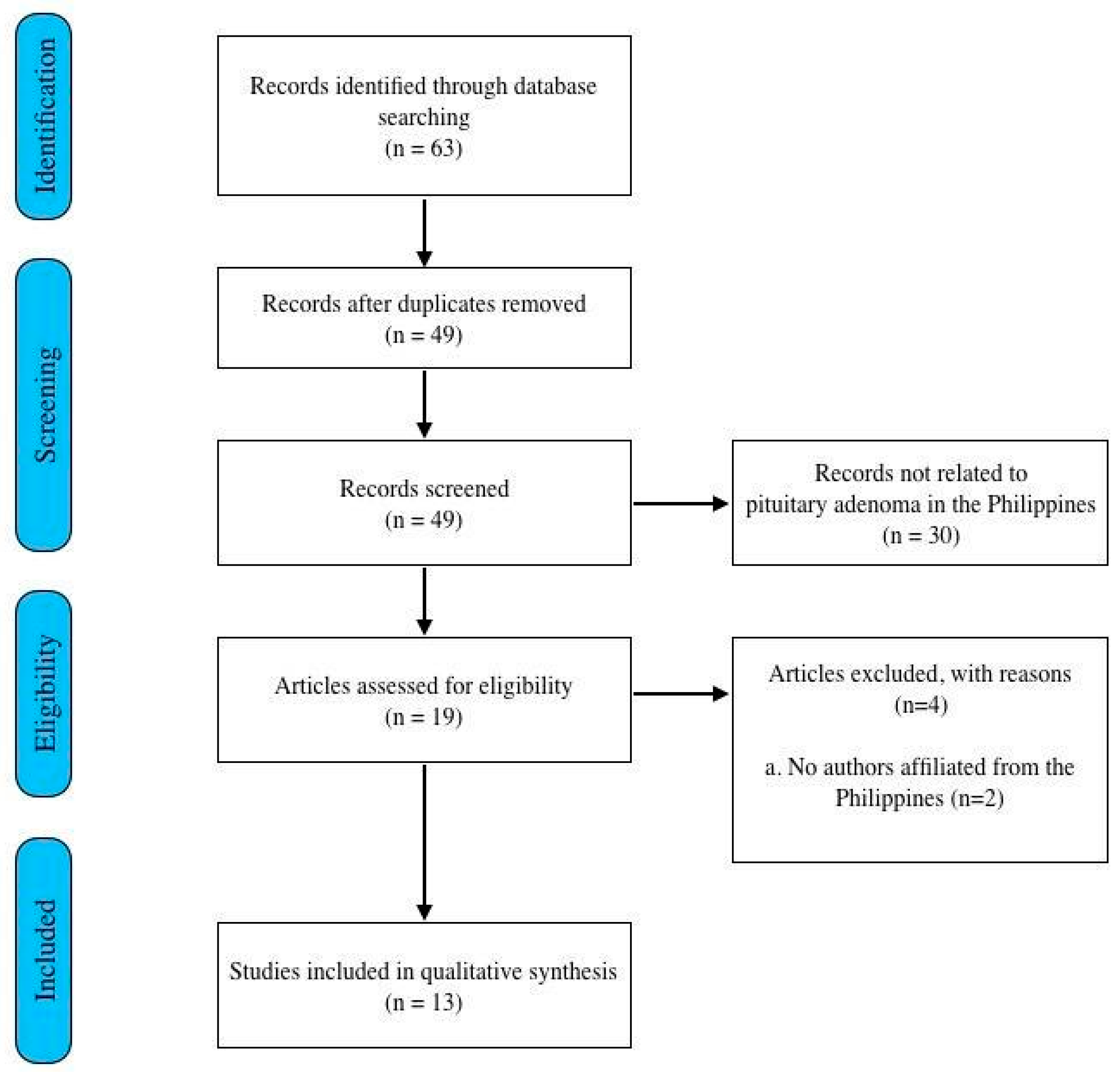
3.1. Search of Studies
3.2. Epidemiology of Pituitary Adenoma in the Philippines
3.3. Other Local Researches in Pituitary Adenoma
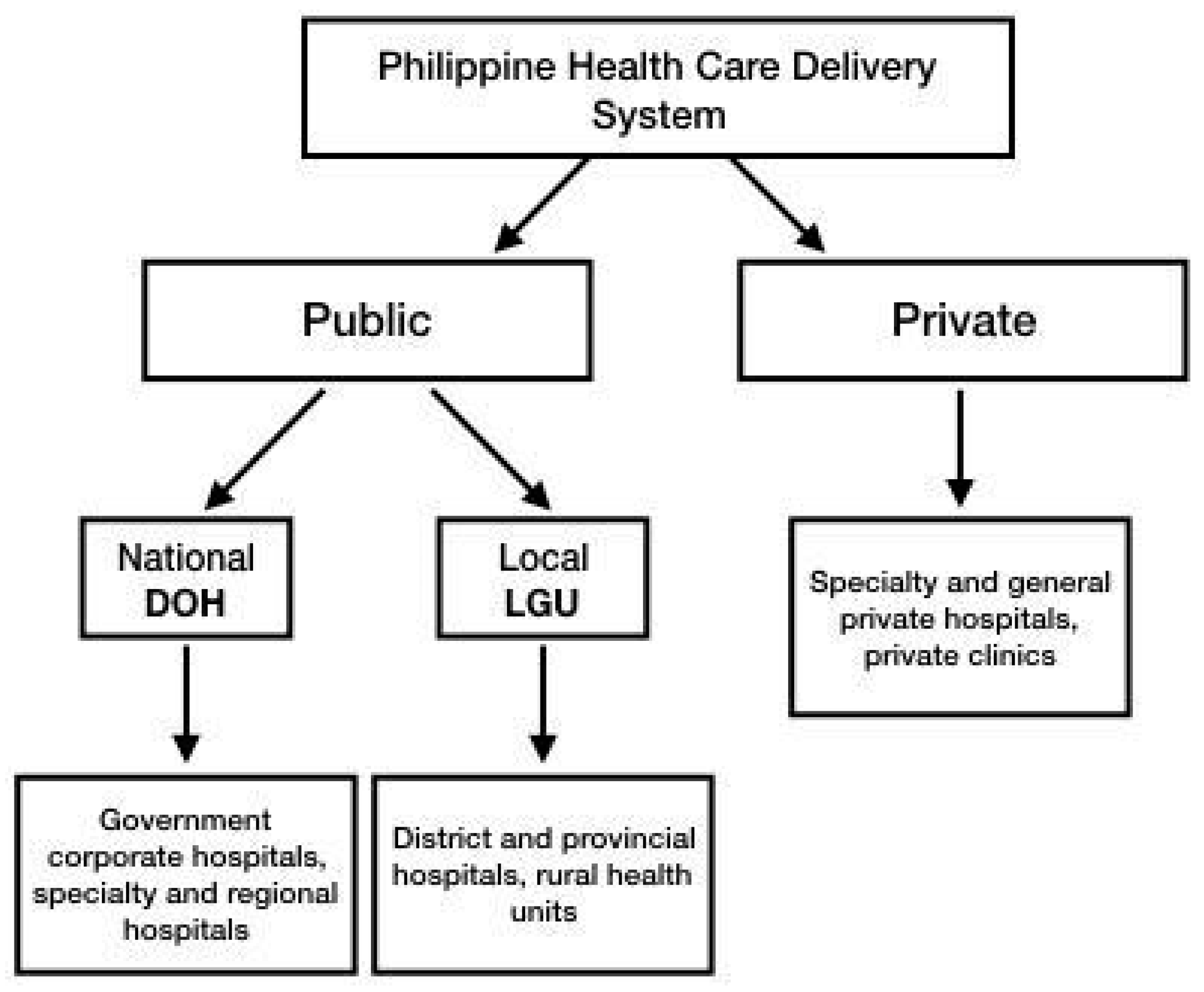
3.4. The Healthcare System of the Philippines
3.5. Healthcare Financing and Coverage in the Philippines
3.6. Specialist Training and Medical Education
3.7. Challenges on Diagnostics
3.8. Challenges on Treatment
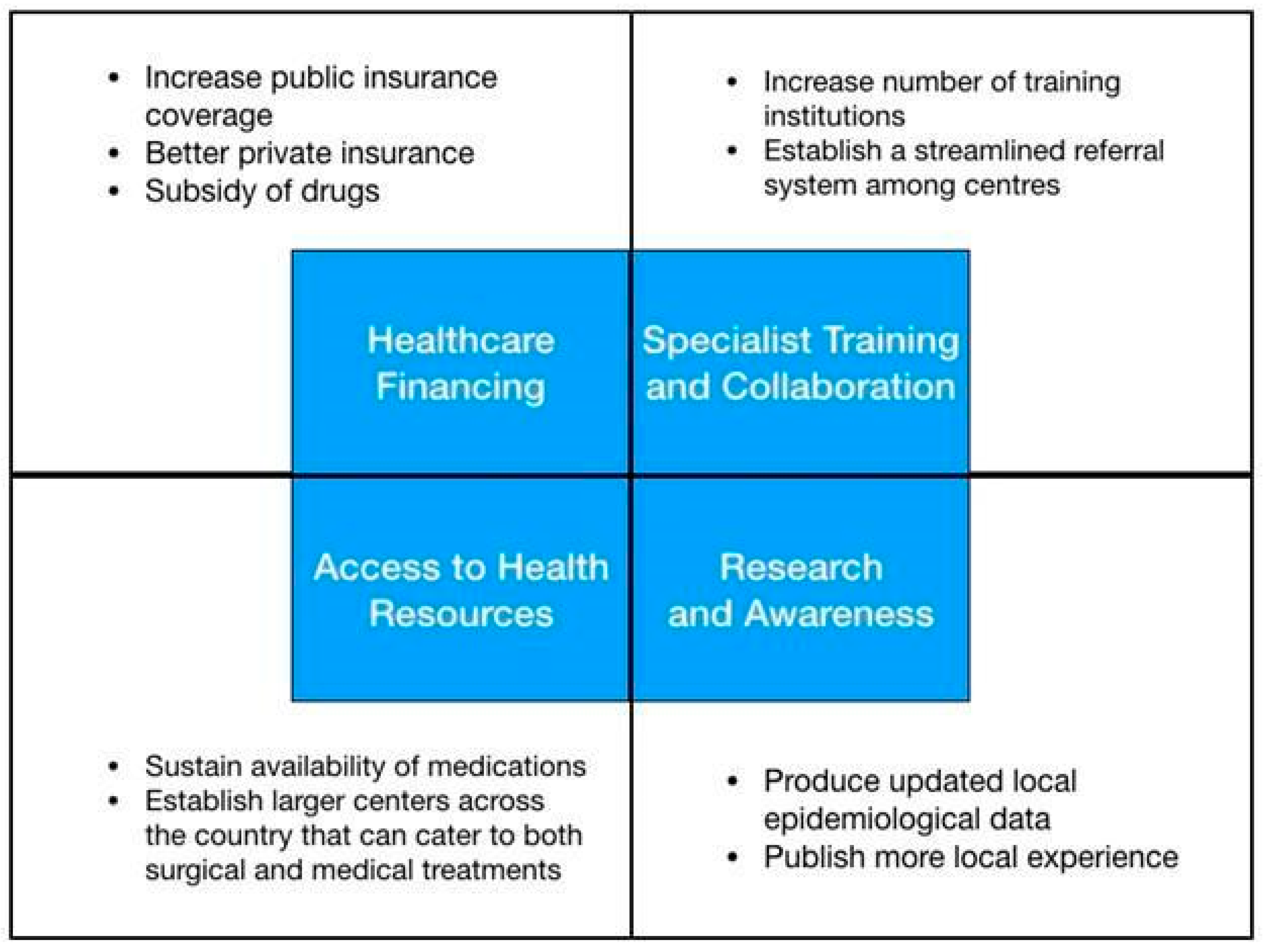
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Daly, A.F.; Beckers, A. The epidemiology of pituitary adenomas. Endocrinol Metab. Clin. N. Am. 2020, 49, 347–355. [Google Scholar] [CrossRef] [PubMed]
- Alinsonorin, D.; Santos-Batongbacal, M.; Paz-Pacheco, E.; Trajano-Acampado, L. Pituitary adenoma: Clinical profile of 120 patients at the Philippine General Hospital. Philipp. J. Int. Med. 2003, 41, 323–329. [Google Scholar]
- Seng, K.S.; Malilay, O.R.M. Extracapsular resection of pituitary adenomas: A systematic review. Asian J. Neurosurg. 2023, 18, 5–11. [Google Scholar] [CrossRef] [PubMed]
- Bunoy, L.S.; Co, J.M.I.O. Inappropriate secretion of thyroid stimulating hormone in a Filipino patient with a pituitary macroadenoma. J. ASEAN Fed. Endocr. Soc. 2012, 27, 114–118. [Google Scholar] [CrossRef][Green Version]
- Chavez, S.; Tan, C. Pituitary macroadenoma presenting as a synchronous occurrence of acromegaly and Cushing’s disease. Rev. Argent. Endocrinol. Metab. 2021, 58, 226. [Google Scholar]
- Faltado, A.L.; Macalalad-Josue, A.A.; Li, R.J.S.; Quisumbing, J.P.M.; Yu, M.G.Y.; Jimeno, C.A. Factors associated with postoperative diabetes insipidus after pituitary surgery. Endocrinol. Metab. 2017, 32, 426. [Google Scholar] [CrossRef]
- Kim, E.H.; Kim, J.; Ku, C.R.; Lee, E.J.; Kim, S.H. Surgical treatment of prolactinomas: Potential role as a first-line treatment modality. Yonsei Med. J. 2023, 64, 489–496. [Google Scholar] [CrossRef]
- Biermasz, N.R. The burden of disease for pituitary patients. Best Pract. Res. Clin. Endocrinol. Metab. 2019, 33, 101309. [Google Scholar] [CrossRef]
- Tricco, A.C.; Lillie, E.; Zarin, W.; O’Brien, K.K.; Colquhoun, H.; Levac, D. PRISMA Extension for Scoping Reviews (PRISMA-ScR): Checklist and explanation. Ann. Intern. Med. 2018, 169, 467–473. [Google Scholar] [CrossRef]
- Villegas, M.; Quinto, G.; Quimpo, J. A review of patients with pituitary tumors at St. Luke’s Medical Center from January 1997 to September 2000. Philipp. J. Intern. Med. 2002, 40, 40–43. [Google Scholar]
- Lo, T.E.; Cabradilla, J.M.; Lim, S.A.; Jimeno, C.A. Endogenous Cushing’s syndrome: The Philippine General Hospital experience. J. Solid. Tumors 2013, 4, 1–10. [Google Scholar]
- Tating, D.L.R.P.; Montevirgen, N.D.S.; Cajucom, L. Cushing’s syndrome from pituitary microadenoma and pulmonary nodules. Oncol. Nurs. Forum. 2016, 43, 136–140. [Google Scholar] [CrossRef]
- Sandoval, M.A.S.; Bruno, R.G. Nail hyperpigmentation in ACTH-secreting pituitary adenoma (Cushing’s disease) and its resolution after successful trans-sphenoidal excision. BMJ Case Rep. 2020, 13, e234905. [Google Scholar] [CrossRef] [PubMed]
- Division for Human Health: DIRAC (Directory of Radiotherapy Centres). Available online: https://dirac.iaea.org/Query/Countries (accessed on 5 December 2023).
- Jordan, C.; Carmen, C.C.; Esposo, E.; Rosales, R.; Maravilla, R.D. The sleeping giant: An atypical case of a giant pituitary adenoma presenting as acromegaly with minimal symptoms of mass effect. J. ASEAN Fed. Endoc. Soc. 2019, 34, 76. [Google Scholar]
- Cudal, B.; Montano, C.; Pontillas, A.; Baraoidan, R. Post-operative complications of trans-sphenoidal surgery in a local tertiary hospital during hospital stay. Philipp. J. Int. Med. 2018, 56, 15–18. [Google Scholar]
- Carampatana-Jandug, C.; Esguerra, J.M.; Panilagao, G.; Mejia, A.; Rama, J.; Bilocura, F.E. In-hospital postoperative complications in patients with pituitary adenoma who underwent pituitary surgery from January 2010 to December 2015: A multicenter study. J. Endocr. Metab. 2017, 7, 122–130. [Google Scholar] [CrossRef][Green Version]
- Fonte, J.; Matawaran, B.; Cunanan, E.; Mercado-Asis, L. Treatment outcomes of pituitary tumors at the University of Santo Tomas Hospital: 2004–2008. Philipp. J. Int. Med. 2009, 47, 121–128. [Google Scholar] [CrossRef]
- Dayrit, M.M.; Lagrada, L.P.; Picazo, O.F.; Pons, M.C.; Villaverde, M.C. The Philippines Health System Review; World Health Organization: New Delhi, India, 2018; Volume 8, pp. 1–12. [Google Scholar]
- Pagaling, G.T.; Turalde, C.W.R.; Jamora, R.D.G. Autoimmune encephalitis in the Philippines: A scoping review on the treatment gaps, challenges, and current state of care. Front. Neurol. 2022, 13, 788309. [Google Scholar] [CrossRef]
- Philippines: Philippine Institute for Developmental Studies. Health Expenses Remain a Big Burden for Pinoys Despite UHC. Available online: https://www.pids.gov.ph/details/news/in-the-news/health-expenses-remain-a-big-burden-for-pinoys-despite-uhc# (accessed on 12 August 2023).
- World Health Organization. Global Health Expenditure Database. Available online: https://apps.who.int/nha/database/country_profile/Index/en (accessed on 18 August 2023).
- Philippine Health Insurance Corporation List of Medical Case Rates. Available online: https://www.philhealth.gov.ph/circulars/2017/annexes/0019/AnnexA-MedicalCaseRates (accessed on 12 August 2023).
- Official Gazette of the Republic of the Philippines Republic Act No. 11463. Available online: https://www.officialgazette.gov.ph/2019/12/03/republic-act-no-11463/ (accessed on 12 August 2023).
- Let’s Save the Brain. Available online: https://letssavethebrain.org/about-us/ (accessed on 16 August 2023).
- Philippine Cancer Resources Cancer Index. Available online: http://www.cancerindex.org/Philippines (accessed on 15 December 2023).
- Sagip Buhay Medical Foundation, Inc. UP-PGH Department of Medicine. Available online: https://uppghmedicine.com.ph/services/sagip/ (accessed on 15 December 2023).
- Russ, S.; Shafiq, I. Pituitary Adenoma; StatPearls Publishing: Treasure Island, FL, USA, 2023. [Google Scholar]
- Tan, G.H. Diabetes care in the Philippines. Ann Glob Health 2016, 81, 863. [Google Scholar] [CrossRef]
- World Health Organization. The Global Health Observatory. Available online: https://www.who.int/data/gho/data/indicators/indicator-details/GHO/medical-doctors-(per-10-000-population) (accessed on 15 December 2023).
- Mondia, M.W.L.; Espiritu, A.I.; Batara, J.M.F.; Jamora, R.D.G. Neuro-oncology in the Philippines: A scoping review on the state of medical practice, deterrents to care and therapeutic gaps. Ecancermedicalscience 2021, 15, 1238. [Google Scholar] [CrossRef]
- Ignacio, K.H.D.; Espiritu, A.I.; Jamora, R.D.G. The current status and challenges in multiple sclerosis management in the Philippines. Mult. Scler. Relat. Dis. 2020, 46, 102510. [Google Scholar] [CrossRef] [PubMed]
- PNA Fellows Philippine Neurological Association. Available online: https://www.philippineneurologicalassociation.com/pna-fellows (accessed on 15 December 2023).
- Academy of Filipino Neurosurgeons, Inc. Members. Available online: https://www.afninc.org/members-2/ (accessed on 26 October 2023).
- Training Institutions Philippine College of Endocrinology Diabetes and Metabolism. Available online: https://endo-society.org.ph/training-institutions/ (accessed on 5 December 2023).
- Facilities of Philippine Radiation Oncology Society. Available online: https://pros.org.ph/facilities/ (accessed on 5 December 2023).
- Philippine Society of Pathologists, Inc. History. Available online: https://psp.com.ph/accreditation (accessed on 25 February 2024).
- Philippine College of Radiology. Available online: https://philippinecollegeofradiology.org.ph/about-us (accessed on 25 February 2024).
- Mendoza, E.; Malong, C.L.; Tanchee-Ngo, M.J.; Mercado-Asis, L. Acromegaly with cardiomyopathy, cardiac thrombus and hemorrhagic cerebral infarct: A case report of therapeutic dilemma with review of literature. Int. J. Endocrinol. Metab. 2015, 13, e18841. [Google Scholar] [CrossRef] [PubMed]
- Varrassi, M.; Cobianchi, F.; Bruno, F. High-resolution magnetic resonance imaging at 3T of pituitary gland: Advantages and pitfalls. Gland Surg. 2019, 13, S208–S215. [Google Scholar] [CrossRef]
- Zampetti, B.; Grossrubatscher, E.; Dalino, P.; Boccardi, E.; Loli, P. Bilateral inferior petrosal sinus sampling. Endocr. Connect. 2016, 5, R12–R25. [Google Scholar] [CrossRef] [PubMed]
- Laboratory Test Prices. Available online: https://www.nwdi.com.ph/prices (accessed on 5 August 2023).
- St. Luke’s News and Events. Available online: https://www.stlukes.com.ph/news-and-events/news-and-press-release/st-lukes-medical-center-quezon-city-introduces-countrys-first-30t-signatm-pioneer-wide-bore-mri (accessed on 25 February 2024).
- Te, J.; Pacia, E. Neuronavigation vs traditional C-arm fluoroscopy in transsphenoidal surgery for the excision of pituitary macroadenomas: A comparative study from the University of Santo Tomas Hospital, Philippines. J. Am. Coll. Surg. 2018, 227, 1–2. [Google Scholar] [CrossRef]
- De Roxas, R.C.; Pedro, K.M.; Rivera, J.P.; Batara, J.M.F. Current treatment status of adult brain tumors in the Philippine General Hospital. J. Neurol. Neurorehab. Res. 2017, 2, 3–4. [Google Scholar] [CrossRef]
- Jane, J.A., Jr.; Catalino, M.P.; Laws, E.R., Jr. Surgical Treatment of Pituitary Adenomas; Endotext: South Dartmouth, MA, USA, 2000. [Google Scholar]
- Loyo-Varela, M.; Herrada-Pineda, T.; Revilla-Pacheco, F.; Manrique-Guzman, S. Pituitary tumor surgery: Review of 3004 cases. World Neurosurg. 2013, 79, 331–336. [Google Scholar] [CrossRef]
- Drug Price Reference Index Department of Health Philippines. Available online: https://dpri.doh.gov.ph/home/drug_2020_index/659 (accessed on 5 September 2023).
- Philippine Food and Drug Administration. Available online: https://verification.fda.gov.ph/drug_productsview.php?showdetail=®istration_number=DR-XY45172 (accessed on 18 December 2023).





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Author | Age/ Sex | Type of Adenoma | Clinical Presentation | Imaging Findings | Hormonal Rofile | Surgical Treatment | Medical Treatment | Outcome |
|---|---|---|---|---|---|---|---|---|
| Bunoy et al., 2012 [4] | 38/M | macro- adenoma | seizures, frontal headache, blurring of vision (bitemporal hemianopsia) | 4.0 × 5.0 × 4.5 cm sellar-suprasellar mass | low cortisol, high TSH, normal ACTH | cranioto- my with excision of the tumor | methima- zole, prednisone | Improved |
| Tating et al., 2016 [12] | 13/M | micro- adenoma | bilateral lower extremity weakness, hypertension | 0.8 × 0.9 × 0.8 cm anterior pituitary gland mass | high ACTH, high cortisol | transphenoidal adenomectomy was indicated but deferred because dexamethasone suppression test revealed high serum cortisol and 24-h free urine cortisol | none | Expired |
| Sandoval et al., 2020 [13] | 37/F | Macro- adenoma | amenorrhea, progressive weight gain, facial roundness, leg weakness, easy bruisability, blurring of vision (bitemporal hemianopsia), hyperpigmented fingernails | 4.6 × 4.1 × 7 cm lobulated, heterogeneously enhancing sellar-suprasellar mass with cystic and necrotic components | High ACTH | transphenoidal excision | none | Improved |
| Mendo-za et al., 2015 [14] | 46/F | macro- adenoma | amenorrhea, acromegaly | 2.1 × 3.3 × 2.4 cm sellar-suprasellar mass with foci of intratumoral hemorrhages suggestive of subclinical pituitary apoplexy | high GH, high prolactin | none | cabergo- line 0.5 mg tablet once a week | Improved |
| Jordan et al., 2022 [15] | 40/F | Giant adenoma | acromegaly, headache, blurring of vision (bitemporal hemianopsia) | 6.4 × 7.0 × 5.5 cm lobulated pituitary mass with cystic degeneration and necrosis | high GH, high IGF-1 | surgical resection via transcranial approach | bromocriptine, radiotherapy | Improved |
| Author | Title | Journal | Institution | Publication Year | Study Design |
|---|---|---|---|---|---|
| Alinsonorin, et al. [2] | Pituitary adenoma: clinical profile of 120 patients at the Philippine General Hospital | Philippine Journal of Internal Medicine | Philippine General Hospital | 2003 | Retrospective, descriptive |
| Seng, et al. [3] | Extracapsular resection of pituitary adenomas: a systemic review | Asian Journal of Neurosurgery | Philippine General Hospital | 2023 | Systematic review |
| Faltado, et al. [6] | Factors associated with postoperative diabetes insipidus after pituitary surgery | International Journal of Endocrinology and Metabolism | Philippine General Hospital | 2017 | Retrospective cohort |
| Villegas, et al. [10] | A review of patients with pituitary tumors at St. Luke’s Medical Center from January 1997 to September 2000 | Philippine Journal of Internal Medicine | St. Luke’s Medical Center | 2002 | Retrospective study |
| Lo, et al. [11] | Endogenous Cushing’s syndrome: the Philippine General Hospital experience | Journal of ASEAN Federation of Endocrine Societies | Philippine General Hospital | 2014 | Cross-sectional |
| Cudal, et al. [16] | Postoperative complications of trans-sphenoidal surgery in a local tertiary hospital during hospital stay | Philippine Journal of Internal Medicine | Makati Medical Center | 2018 | Retrospective cross- sectional |
| Carampatana-Jandug, et al. [17] | In-hospital postoperative complications in patients with pituitary adenoma who underwent pituitary surgery from January 2010 to December 2015: a multicenter study | International Journal of Endocrinology and Metabolism | Chong Hua Hospital | 2017 | Retrospective cohort |
| Fonte, et al. [18] | Treatment outcomes of pituitary tumors at the University of Santo Tomas Hospital: 2004–2008 | Philippine Journal of Internal Medicine | University of Santo Tomas Hospital | 2009 | Retrospective cohort |
| Specialist | Specialist to Filipino Ratio |
|---|---|
| Endocrinologist | 1:198,000 |
| Adult Neurologist | 1:140,000 |
| Neurosurgeon | 1:600,000 |
| Pediatric Neurologist | 1:315,000 |
| Radiologist | 1:51,555 |
| Radiation Oncologist | 1:900,000 |
| Neuropathologist | 1:34,800,000 |
| Laboratory Test/Imaging | Cost Government-Subsidized (USD) | Cost No Government No Subsidy (USD) | Cost Private (USD) |
|---|---|---|---|
| IGF-1 | NA | NA | 175.00 |
| ACTH | NA | NA | 136.90 |
| Cortisol | NA | NA | 52.80 |
| Prolactin | 5.80 | 8.50 | 9.10–31.20 |
| FSH | 6.10 | 9.70 | 11.50–24.20 |
| LH | 9.20 | 12.40 | 13.00–24.20 |
| Estradiol | 6.90 | 10.60 | 11.10–46.80 |
| Testosterone | 15.30 | 32.20 | 33.80–46.80 |
| TSH | 6.10 | 10.50 | 12.10–14.40 |
| FT3 | 8.30 | 12.90 | 13.60–49.90 |
| FT4 | 6.40 | 10.00 | 10.50–49.90 |
| Cranial MRI with contrast | 153.70 | 179.30 | 190.00–210.90 |
| Cranial MRI—plain | 75.60 | 91.30 | 96.60–107.30 |
| Cranial CT scan with contrast | 86.30 | 98.10 | 103.00–112.80 |
| Cranial CT scan—plain | 26.30 | 54.40 | 65.30–73.50 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tabuzo, M.M.B.; Hernandez, M.A.L.U.; Chua, A.E.; Maningat, P.D.; Chiu, H.H.C.; Jamora, R.D.G. Pituitary Adenoma in the Philippines: A Scoping Review on the Treatment Gaps, Challenges, and Current State of Care. Med. Sci. 2024, 12, 16. https://doi.org/10.3390/medsci12010016
Tabuzo MMB, Hernandez MALU, Chua AE, Maningat PD, Chiu HHC, Jamora RDG. Pituitary Adenoma in the Philippines: A Scoping Review on the Treatment Gaps, Challenges, and Current State of Care. Medical Sciences. 2024; 12(1):16. https://doi.org/10.3390/medsci12010016
Chicago/Turabian StyleTabuzo, Mykha Marie B., Mary Angeline Luz U. Hernandez, Annabell E. Chua, Patricia D. Maningat, Harold Henrison C. Chiu, and Roland Dominic G. Jamora. 2024. "Pituitary Adenoma in the Philippines: A Scoping Review on the Treatment Gaps, Challenges, and Current State of Care" Medical Sciences 12, no. 1: 16. https://doi.org/10.3390/medsci12010016
APA StyleTabuzo, M. M. B., Hernandez, M. A. L. U., Chua, A. E., Maningat, P. D., Chiu, H. H. C., & Jamora, R. D. G. (2024). Pituitary Adenoma in the Philippines: A Scoping Review on the Treatment Gaps, Challenges, and Current State of Care. Medical Sciences, 12(1), 16. https://doi.org/10.3390/medsci12010016