
Assessing Accessibility and Social Equity of Tertiary Hospitals for Older Adults: A City-Wide Study of Tianjin, China




Abstract
:1. Introduction
2. Methods
2.1. Measuring Accessibility to Tertiary Hospitals
2.2. Assessing Disparities of Accessibility
2.3. Assessing Social Equity
3. Case Study
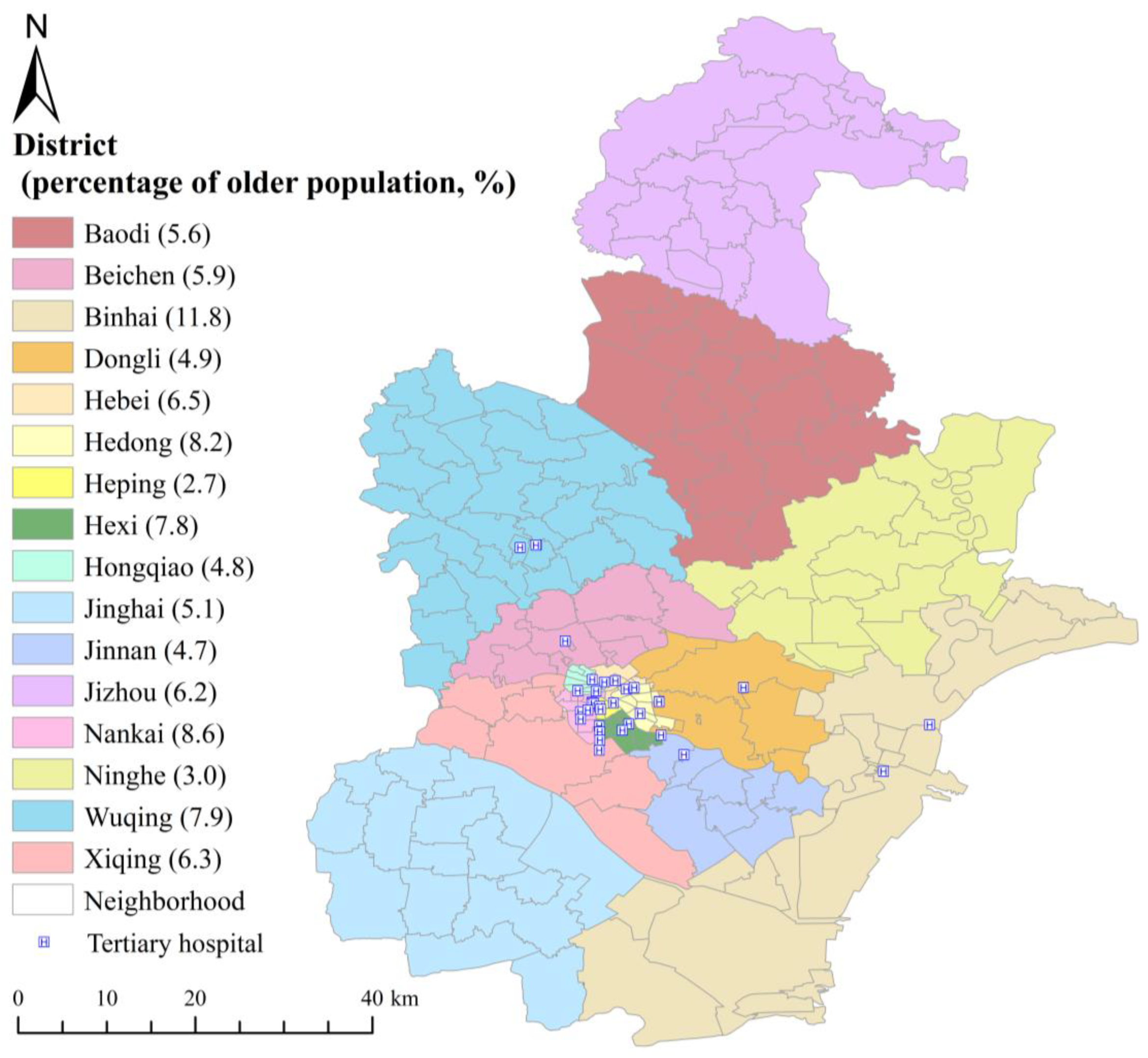
3.1. Study Area and Data Source
3.2. Results
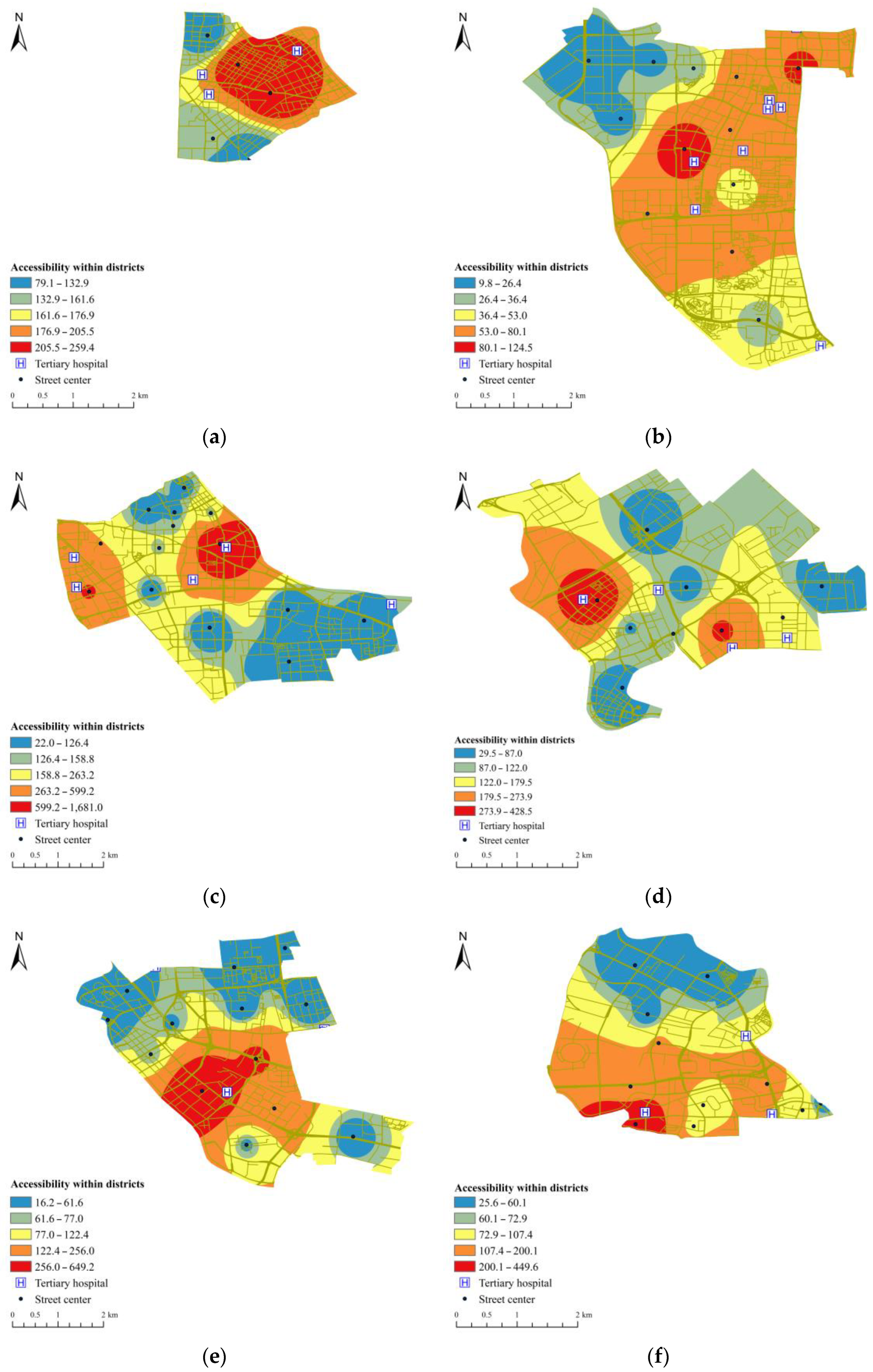
3.2.1. Accessibility to Tertiary Hospitals within Regions
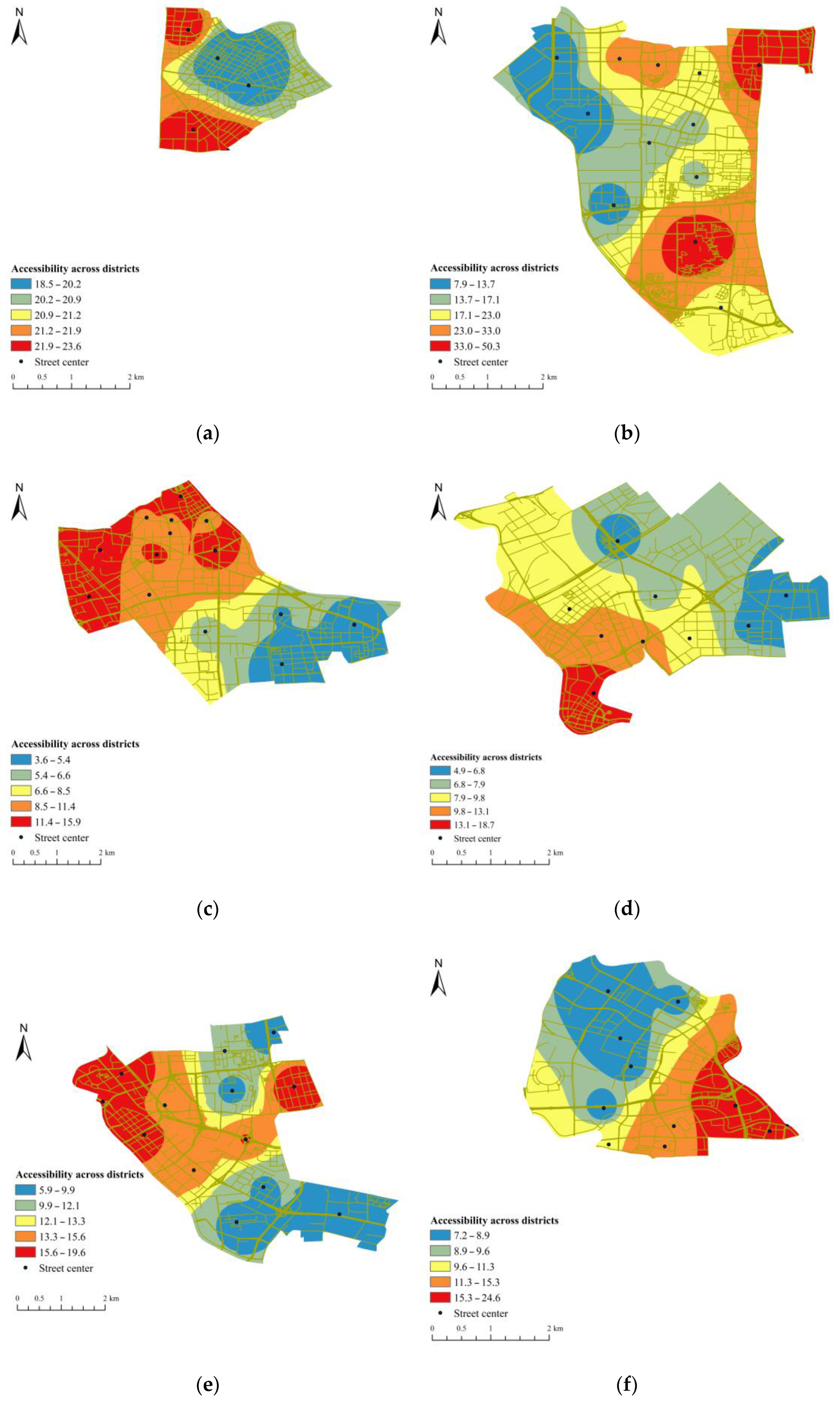
3.2.2. Accessibility to Tertiary Hospitals across Regions
3.2.3. Overall Accessibility to Tertiary Hospitals
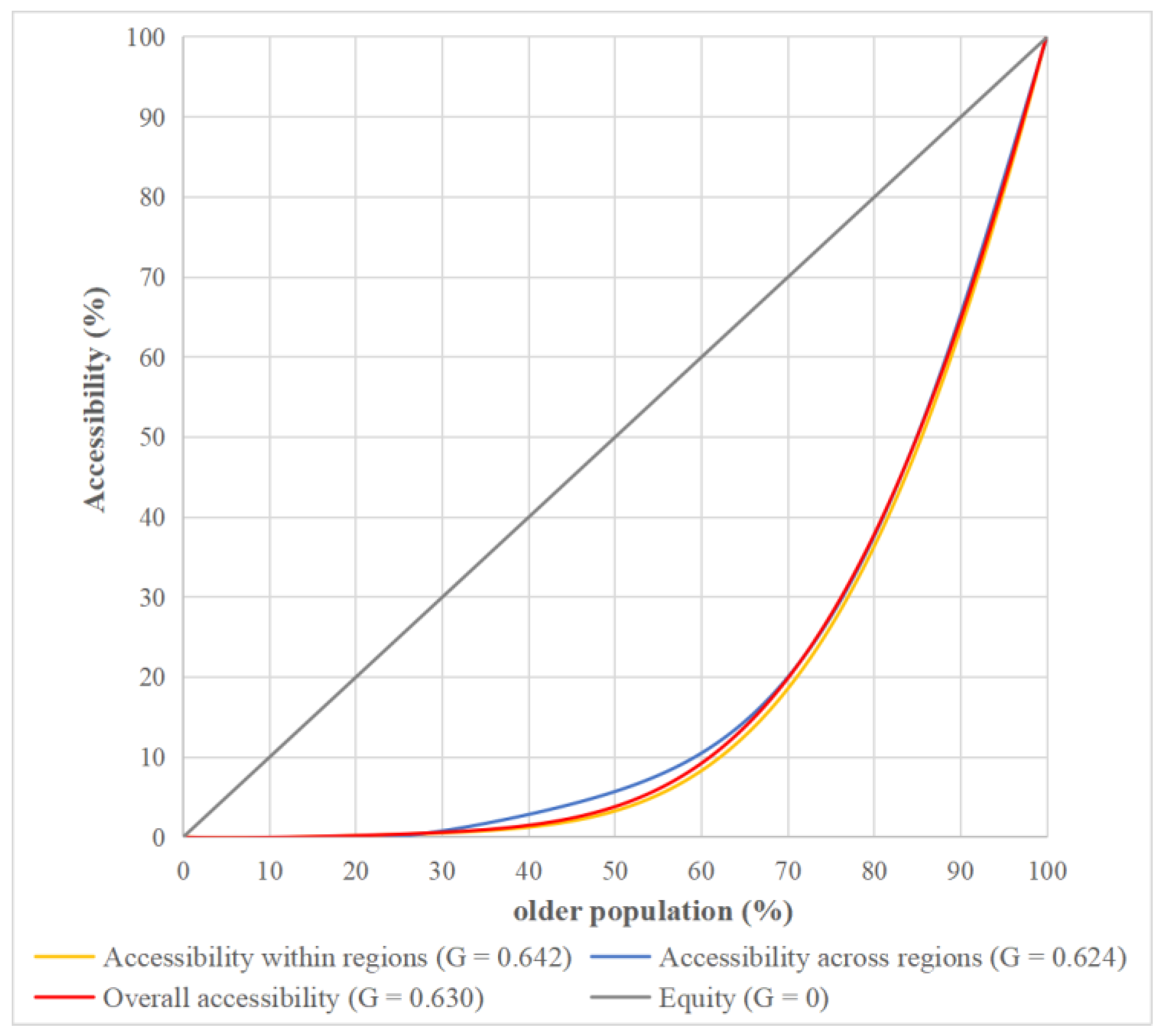
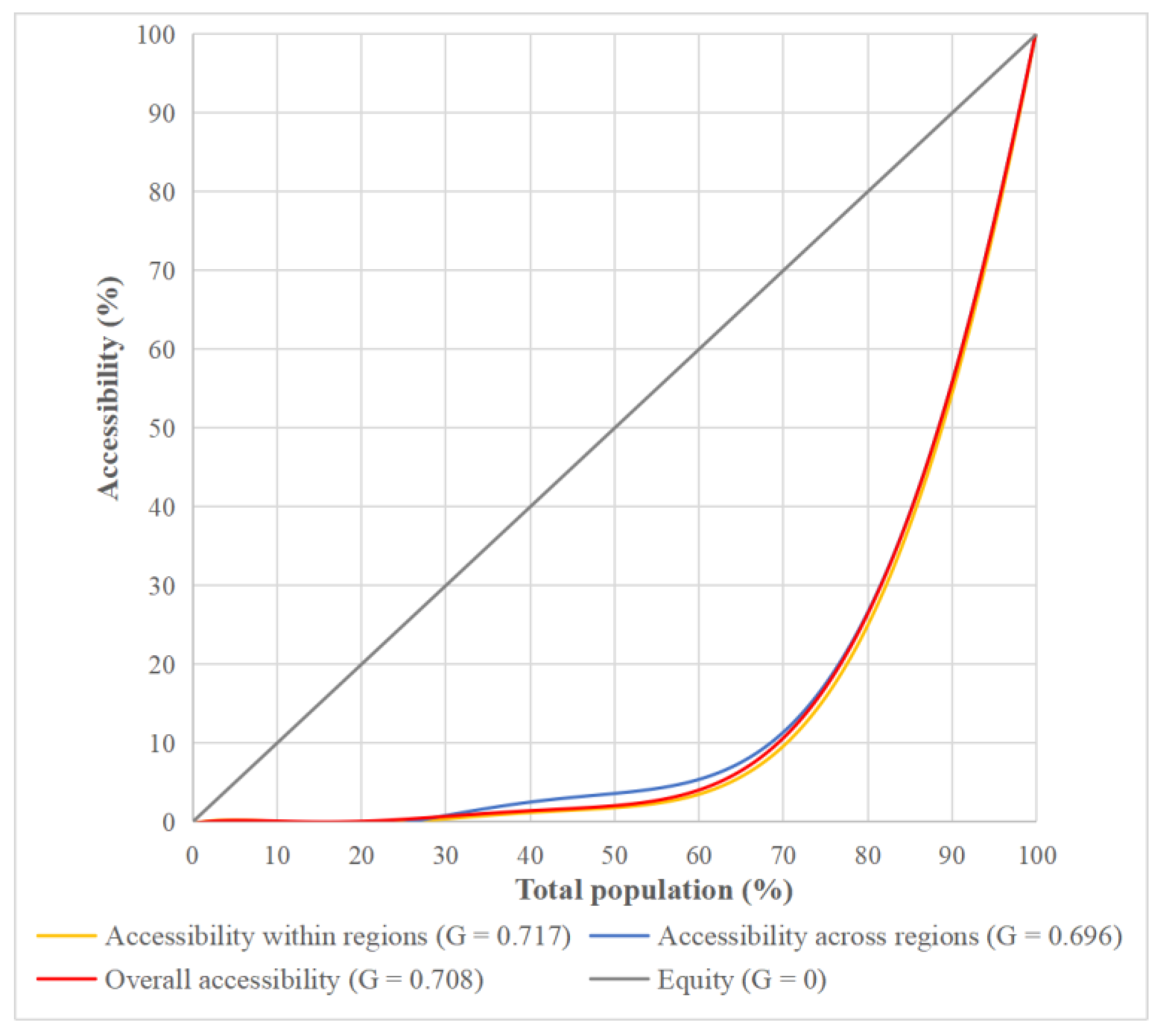
3.2.4. Social Equity of Tertiary Hospitals
4. Discussion
4.1. Regional Comparison
4.2. Social Equity Comparison
4.3. Policy Considerations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- United Nations. World Population Ageing 2019; United Nations: New York, NY, USA, 2019. [Google Scholar]
- Starfield, B.; Shi, L.; Macinko, J. Contribution of primary care to health systems and health. Milbank Q. 2015, 83, 457–502. [Google Scholar] [CrossRef] [PubMed]
- Yang, N.; Shen, L.; Shu, T.; Liao, S.; Peng, Y.; Wang, J. An integrative method for analyzing spatial accessibility in the hierarchical diagnosis and treatment system in China. Soc. Sci. Med. 2021, 270, 113656. [Google Scholar] [CrossRef]
- Chinese State Council. Guiding Opinions of the General Office of the State Council on Promoting the Construction of a Hierarchical Diagnosis and Treatment System. Available online: http://www.gov.cn/zhengce/content/2015-09/11/content_10158.htm (accessed on 19 September 2015).
- Lu, C.; Zhang, Z.; Lan, X. Impact of China’s referral reform on the equity and spatial accessibility of healthcare resources: A case study of Beijing. Soc. Sci. Med. 2019, 235, 112386. [Google Scholar] [CrossRef] [PubMed]
- National Development and Reform Commission. Implementation Plan for Establishing the Efficient and High-Quality Medical and Health Service System during the 14th Five-Year Plan. 2021. Available online: https://www.ndrc.gov.cn/xxgk/zcfb/tz/202107/t20210701_1285212.html?code=&state=123 (accessed on 25 May 2022).
- Li, Z.; Gao, Y.; Yu, L.; Choguill, C.L.; Cui, W. Analysis of the elderly’s preferences for choosing medical service facilities from the perspective of accessibility: A case study of tertiary general hospitals in Hefei, China. Int. J. Environ. Res. Public Health 2021, 19, 9432. [Google Scholar] [CrossRef]
- Koenig, J.G. Indicators of urban accessibility: Theory and application. Transportation 1980, 9, 145–172. [Google Scholar] [CrossRef]
- Van Herzele, A.; Wiedemann, T. A monitoring tool for the provision of accessible and attractive urban green spaces. Landsc. Urban Plan. 2003, 63, 109–126. [Google Scholar] [CrossRef]
- Nykiforuk, C.I.J.; Glenn, N.M.; Hosler, I.; Craig, H.; Reynard, D.; Molner, B.; Candlish, J.; Lowe, S. Understanding urban accessibility: A community-engaged pilot study of entrance features. Soc. Sci. Med. 2021, 273, 113775. [Google Scholar] [CrossRef]
- Cheng, L.; Yang, M.; De Vos, J.; Witlox, F. Examining geographical accessibility to multi-tier hospital care services for the elderly: A focus on spatial equity. J. Transp. Health 2020, 19, 100926. [Google Scholar] [CrossRef]
- Zhang, F.; Li, D.; Ahrentzen, S.; Zhang, J. Assessing spatial disparities of accessibility to community-based service resources for Chinese older adults based on travel behavior: A city-wide study of Nanjing, China. Habitat Int. 2019, 88, 101984. [Google Scholar] [CrossRef]
- Chen, Y.; Bouferguene, A.; Li, H.X.; Liu, H.; Shen, Y.; Al-Hussein, M. Spatial gaps in urban public transport supply and demand from the perspective of sustainability. J. Clean. Prod. 2018, 195, 1237–1248. [Google Scholar] [CrossRef]
- Li, S.; Duan, H.; Smith, T.E.; Hu, H. Time-varying accessibility to senior centers by public transit in Philadelphia. Transp. Res. Part A Policy Pract. 2021, 151, 245–258. [Google Scholar] [CrossRef]
- Guo, S.; Song, C.; Pei, T.; Liu, Y.; Ma, T.; Du, Y.; Chen, J.; Fan, Z.; Tang, X.; Peng, Y.; et al. Accessibility to urban parks for elderly residents: Perspectives from mobile phone data. Landsc. Urban Plan. 2019, 191, 103642. [Google Scholar] [CrossRef]
- Pettersson, C.; Slaug, B.; Granbom, M.; Kylberg, M.; Iwarsson, S. Housing accessibility for senior citizens in Sweden: Estimation of the effects of targeted elimination of environmental barriers. Scand. J. Occup. Ther. 2018, 25, 407–418. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, X.; Yang, H.; Duan, Z.; Pan, J. Spatial accessibility of primary health care in China: A case study in Sichuan Province. Soc. Sci. Med. 2018, 209, 14–24. [Google Scholar] [CrossRef] [PubMed]
- Tao, Z.; Cheng, Y.; Du, S.; Feng, L.; Wang, S. Accessibility to delivery care in Hubei Province, China. Soc. Sci. Med. 2020, 260, 113186. [Google Scholar] [CrossRef]
- Huotari, T.; Antikainen, H.; Keistinen, T.; Rusanen, J. Accessibility of tertiary hospitals in Finland: A comparison of administrative and normative catchment areas. Soc. Sci. Med. 2017, 182, 60–67. [Google Scholar] [CrossRef] [Green Version]
- Cheng, G.; Zeng, X.; Duan, L.; Lu, X.; Sun, H.; Jiang, T.; Li, Y. Spatial difference analysis for accessibility to high level hospitals based on travel time in Shenzhen, China. Habitat Int. 2016, 53, 485–494. [Google Scholar] [CrossRef] [Green Version]
- Kim, K.; Ghorbanzadeh, M.; Horner, M.W.; Ozguven, E.E. Identifying areas of potential critical healthcare shortages: A case study of spatial accessibility to ICU beds during the COVID-19 pandemic in Florida. Transp. Policy 2021, 110, 478–486. [Google Scholar] [CrossRef]
- Zhang, T.; Xu, Y.; Ren, J.; Sun, L.; Liu, C. Inequality in the distribution of health resources and health services in China: Hospitals versus primary care institutions. Int. J. Equity Health 2017, 16, 42. [Google Scholar] [CrossRef] [Green Version]
- Lorenz, M.O. Methods of measuring the concentration of wealth. Publ. Am. Stat. Assoc. 1905, 9, 209–219. [Google Scholar] [CrossRef]
- Huang, Y.; Todd, D. The energy implications of Chinese regional disparities. Energy Policy 2010, 38, 7531–7538. [Google Scholar] [CrossRef]
- Liu, B.; Shen, Y.; Chen, Y.; Chen, X.; Wang, Y. A two-layer weight determination method for complex multi-attribute large-group decision-making experts in a linguistic environment. Inf. Fusion 2015, 23, 156–165. [Google Scholar] [CrossRef]
- Delbosc, A.; Gurrie, G. Using Lorenz curves to assess public transport equity. J. Transp. Geogr. 2011, 19, 1252–1259. [Google Scholar] [CrossRef]
- Chen, Y.; Bouferguene, A.; Shen, Y.; Al-Hussein, M. Assessing accessibility-based service effectiveness (ABSEV) and social equity for urban bus transit: A sustainability perspective. Sustain. Cities Soc. 2019, 44, 499–510. [Google Scholar] [CrossRef]
- Ricciardi, A.M.; Xia, J.C.; Currie, G. Exploring public transport equity between separate disadvantaged cohorts: A case study in Perth, Australia. J. Transp. Geogr. 2015, 43, 111–122. [Google Scholar] [CrossRef]
- Tao, Y.; Henry, K.; Zou, Q.; Zhong, X. Methods for measuring horizontal equity in health resource allocation: A comparative study. Health Econ. Rev. 2014, 4, 10. [Google Scholar] [CrossRef] [Green Version]
- Ben-Akiva, M.; Lerman, S. Disaggregate travel and mobility choice models and measure of accessibility. In Behavioural Travel Modeling; Routledge: London, UK, 2021; pp. 654–679. [Google Scholar]
- Guagliardo, M.F. Spatial accessibility of primary care: Concepts, methods and challenges. Int. J. Health Geogr. 2004, 3, 3. [Google Scholar] [CrossRef] [Green Version]
- Boisjoly, G.; Deboosere, R.; Wasfi, R.; Orpana, H.; Manaugh, K.; Buliung, R.; El-Geneidy, A. Measuring accessibility to hospitals by public transport: An assessment of eight Canadian metropolitan regions. J. Transp. Health 2020, 18, 100916. [Google Scholar] [CrossRef]
- Peeters, D.; Thomas, I. Distance predicting functions and applied location-allocation models. J. Geogr. Syst. 2000, 2, 167–184. [Google Scholar] [CrossRef]
- Chen, Y.; Liu, B.; Shen, Y.; Wang, X. Spatial analysis of change trend and influencing factors of total factor productivity in China’s regional construction industry. Appl. Econ. 2018, 50, 2824–2843. [Google Scholar] [CrossRef]
- Rey, S.J.; Montouri, B.D. US regional income convergence: A spatial econometric perspective. Reg. Stud. 1999, 33, 143–156. [Google Scholar] [CrossRef]
- Moran, P.A.P. The interpretation of statistical maps. J. R. Stat. Soc. Ser. B 1948, 10, 243–251. [Google Scholar] [CrossRef]
- Dewan, A.; Abdullah, A.Y.M.; Shogib, M.R.I.; Karim, R.; Rahman, M.M. Exploring spatial and temporal patterns of visceral leishmaniasis in endemic areas of Bangladesh. Trop. Med. Health 2017, 45, 29. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Graham, J.E.; Fisher, S.R.; Bergés, I.M.; Kuo, Y.F.; Ostir, G.V. Walking speed threshold for classifying walking independence in hospitalized older adults. Phys. Ther. 2010, 90, 1591–1597. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jin, C.; Cheng, J.; Lu, Y.; Huang, Z.; Cao, F. Spatial inequity in access to healthcare facilities at a county level in a developing country: A case study of Deqing County, Zhejiang, China. Int. J. Equity Health 2015, 14, 67. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rosero-Bixby, L. Spatial access to health care in Costa Rica and its equity: A GIS-based study. Soc. Sci. Med. 2004, 58, 1271–1284. [Google Scholar] [CrossRef] [PubMed]
- Martin, D.J.; Jordan, H.; Roderick, P. Taking the bus: Incorporating public transport timetable data into health care accessibility modelling. Environ. Plan. A 2008, 40, 2510–2525. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| District | Rank | Rank | Rank | |||
|---|---|---|---|---|---|---|
| Hexi | 1 | 1 | 0.4410 | 5 | 1 | 1 |
| Heping | 0.6581 | 2 | 0.9710 | 2 | 0.7154 | 2 |
| Hebei | 0.5574 | 3 | 0.4165 | 6 | 0.5718 | 3 |
| Hongqiao | 0.4524 | 4 | 0.6235 | 3 | 0.4881 | 4 |
| Hedong | 0.4468 | 5 | 0.5836 | 4 | 0.4793 | 5 |
| Beichen | 0.4047 | 6 | 0.1289 | 7 | 0.4006 | 6 |
| Nankai | 0.2028 | 7 | 1 | 1 | 0.2795 | 7 |
| Wuqing | 0.1048 | 8 | 0.0185 | 11 | 0.1025 | 8 |
| Xiqing | 0.0274 | 9 | 0.1108 | 8 | 0.0357 | 9 |
| Jinnan | 0.0240 | 10 | 0.0613 | 10 | 0.0283 | 11 |
| Dongli | 0.0266 | 11 | 0.0963 | 9 | 0.0306 | 10 |
| Binhai | 0.0218 | 12 | 0.0111 | 13 | 0.0219 | 12 |
| Jinghai | 0 | 13 | 0.0148 | 12 | 0.0012 | 13 |
| Ninghe | 0 | 13 | 0.0106 | 14 | 0.0009 | 14 |
| Baodi | 0 | 13 | 0.0069 | 15 | 0.0006 | 15 |
| Jizhou | 0 | 13 | 0 | 16 | 0 | 16 |
| CV | Moran’s I | |
|---|---|---|
| Accessibility within regions | 1.206 | 0.314 *** |
| Accessibility across regions | 1.200 | 0.550 *** |
| Overall accessibility | 1.171 | 0.370 *** |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chen, Y.; Ding, Q.; Shen, Y. Assessing Accessibility and Social Equity of Tertiary Hospitals for Older Adults: A City-Wide Study of Tianjin, China. Buildings 2022, 12, 2107. https://doi.org/10.3390/buildings12122107
Chen Y, Ding Q, Shen Y. Assessing Accessibility and Social Equity of Tertiary Hospitals for Older Adults: A City-Wide Study of Tianjin, China. Buildings. 2022; 12(12):2107. https://doi.org/10.3390/buildings12122107
Chicago/Turabian StyleChen, Yuan, Qiushi Ding, and Yinghua Shen. 2022. "Assessing Accessibility and Social Equity of Tertiary Hospitals for Older Adults: A City-Wide Study of Tianjin, China" Buildings 12, no. 12: 2107. https://doi.org/10.3390/buildings12122107