
Seizures Following Carotid Endarterectomy: A Comprehensive Meta-Analysis of 69,479 Patients and Evidence-Based Recommendations for Perioperative Care



Abstract
1. Background
Objectives
- (1)
- Investigate the pooled prevalence of seizures following CEA.
- (2)
- Analyze the potential progression of postoperative seizures to epilepsy.
2. Materials and Methods
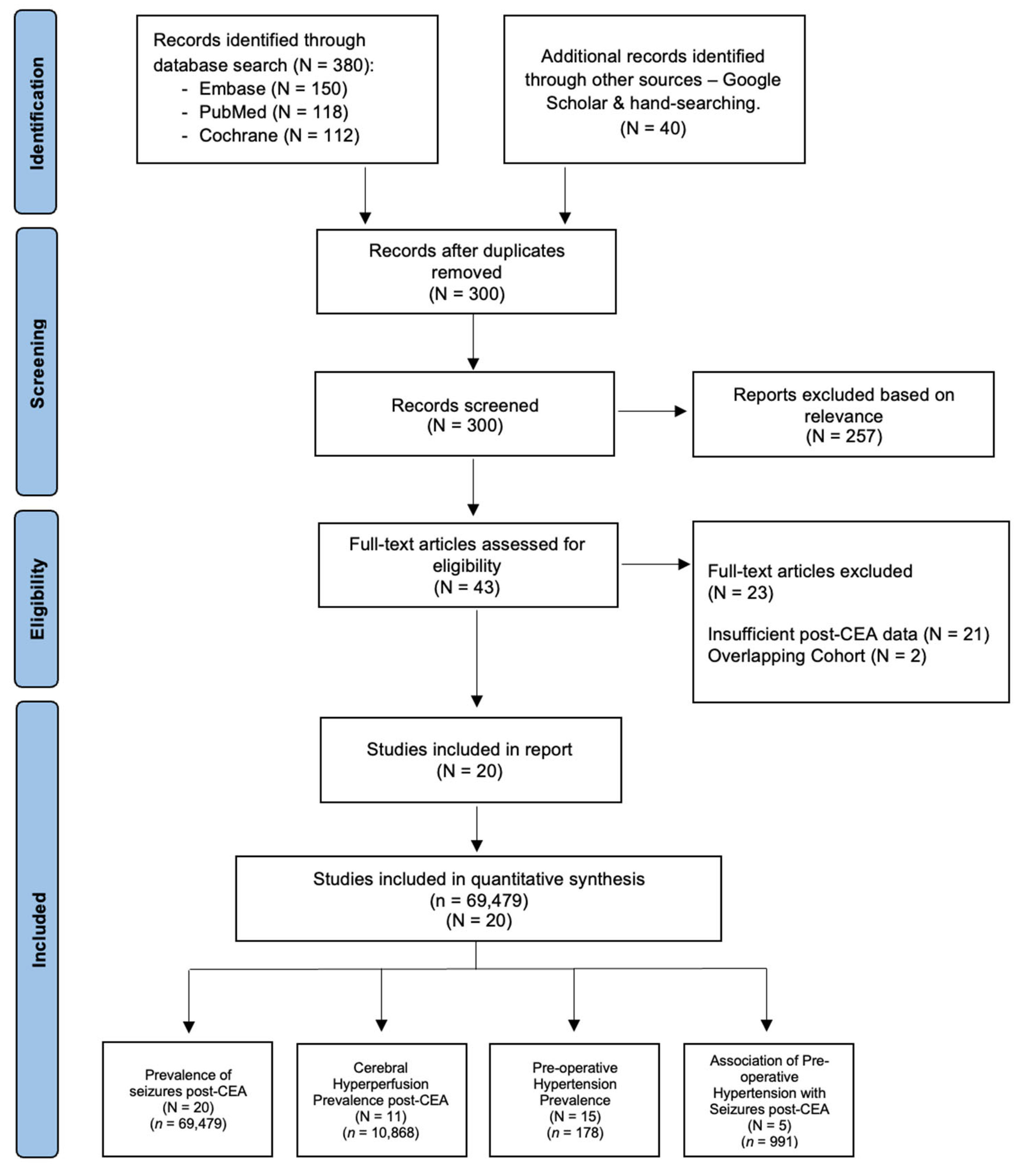
2.1. Literature Search and Study Selection
2.2. Inclusion and Exclusion Criteria
2.3. Data Extraction and Methodological Quality Assessment
2.4. Statistical Methodology
3. Results
3.1. Description of Included Studies
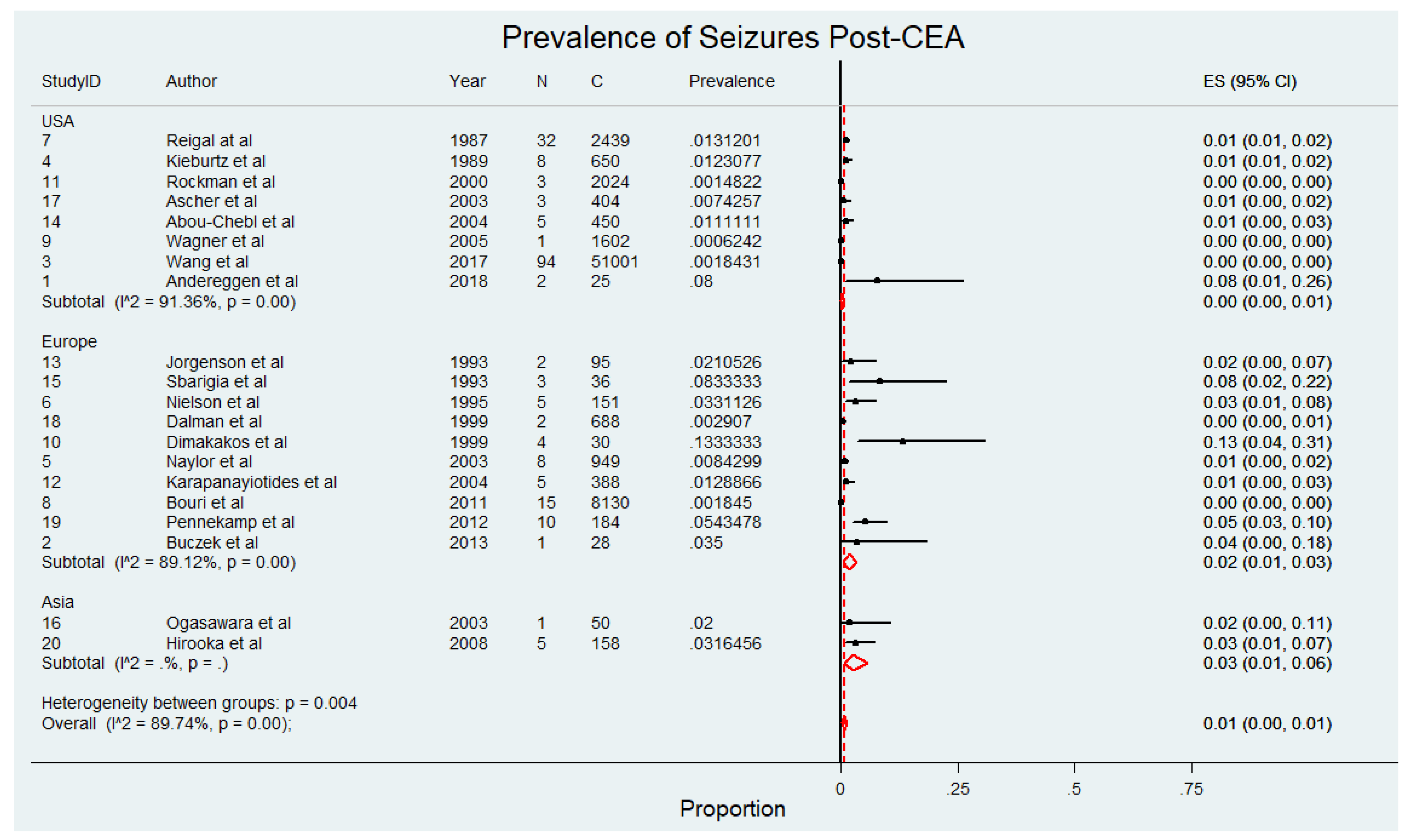
3.2. Overall Prevalence of Seizures in Patients Undergoing CEA

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study ID | Author | Year | Region | Study Type | Sample Size (n) | Seizure Prevalence (n, %) | Follow-Up Duration (Days) | Age (Years ± SD) | Male (n, %) * | AF (n, %) | HL (n, %) | HTN (n, %) | CAD (n, %) | Previous stroke/TIA (n, %) | Smoking (n, %) | Diabetes (n, %) |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | Andereggen et al. [11] | 2018 | USA | Prospective | 25 | 2 (8.0) | 1–5 | 71.0 ± 8.7 | 18 (72.0) | - | 20 (80.0) | 20 (80.0) | 9 (36.0) | 17 (68.0) | 17 (68.0) | 8 (32.0) |
| 2 | Buczek et al. [5] | 2013 | Europe | Prospective | 28 | 1 (3.6) | 2–5 | 70.2 ± 9.4 | 23 (82.1) | - | - | 22 (78.6) | - | 11 (39.3) | - | 8 (28.6) |
| 3 | Wang et al. [9] | 2017 | USA | Retrospective | 51,001 | 94 (0.2) | 3–6 | 70.2 ± 9.4 | 30,804 (60.4) | - | - | 45,238 (88.7) | 14,586 (28.6) | 15,096 (29.6) | 24,276 (47.6) | 17,697 (34.7) |
| 4 | Kieburtz et al. [8] | 1989 | USA | Retrospective | 650 | 8 (1.2) | 7 | 69.5 ± 10.0 | - | - | - | 488 (75.1) | - | 81 (12.5) | 569 (87.5) | 81 (12.5) |
| 5 | Naylor et al. [6] | 2003 | Europe | Prospective | 949 | 8 (0.8) | 2–8 | 65.8 ± 10.4 | 4 (0.4) œ | - | - | - | - | - | - | - |
| 6 | Nielson et al. [4] | 1995 | Europe | Prospective | 151 | 5 (3.3) | 5–7 | 62.0 | 97 (64.2) | - | - | - | 40 (26.0) | 59 (39.0) | - | 17 (11.0) |
| 7 | Reigal et al. [10] | 1987 | USA | Retrospective | 2439 | 32 (1.3) | 1–7 | - | - | - | - | - | - | - | - | - |
| 8 | Bouri et al. [30] | 2011 | Europe | Retrospective | 8130 | 15 (0.2) | 3–6 | 66.0 ± 9.5 | - | - | - | 1545 (19.0) | - | - | - | - |
| 9 | Wagner et al. [20] | 2005 | USA | Retrospective | 1602 | 1 (0.1) | 1–7 | - | - | - | - | - | 224 (14.0) | |||
| 10 | Dimakakos et al. [28] | 1999 | Europe | Prospective | 30 | 4 (13.3) | 1–7 | 66.6 ± 15.0 | 22 (73.0) | - | 18 (60.0) | 17 (57.0) | 17 (57.0) | 15 (50.0) | 5 (17.0) | |
| 11 | Rockman et al. [22] | 2000 | USA | Retrospective | 2024 | 3 (0.1) | 1–7 | 68.7 ± 9.4 | 1295 (64.0) | - | - | 1416 (70.0) | 951 (47.0) | 850 (42.0) | 971 (48.0) | 506 (25.0) |
| 12 | Karapanayiotides et al. [25] | 2004 | Europe | Prospective | 388 | 5 (1.3) | 2–7 | 70.4 ± 6.2 | 77 (20.0) | - | - | 230 (59.0) | - | |||
| 13 | Jorgenson et al. [26] | 1993 | Europe | Prospective | 95 | 2 (2.1) | 1–14 | 59.0 ±12.0 | 62 (65.0) | - | - | 44 (46.0) | - | 48 (51.0) | ||
| 14 | Abou-Chebl et al. [32] | 2004 | USA | Retrospective | 450 | 5 (1.1) | 1–4 | 72.7 ± 10.9 | - | - | 197 (44.0) | 339 (75.0) | 255 (57.0) | 225 (50.0) | 176 (39.0) | |
| 15 | Sbarigia et al. [21] | 1993 | Europe | Prospective | 36 | 3 (8.3) | 1–2 | 67.0 ± 6.0 | 32 (89.0) | - | - | 27 (75.0) | - | |||
| 16 | Ogasawara et al. [24] | 2003 | Asia | Prospective | 50 | 1 (2.0) | 1–6 | 68.6 ± 5.8 | 44 (88.0) | - | - | - | - | |||
| 17 | Ascher et al. [31] | 2003 | USA | Prospective | 404 | 3 (0.7) | 1–8 | 69.0 ± 8.0 | 221 (55.0) | - | - | 275 (68.0) | 98 (24.0) | 129 (32.0) | 176 (44.0) | 122 (30.0) |
| 18 | Dalman et al. [29] | 1999 | Europe | Prospective | 688 | 2 (0.3) | 1–7 | 69.0 ± 10.3 | 447 (65.0) | - | - | - | - | |||
| 19 | Pennekamp et al. [23] | 2012 | Europe | Prospective | 184 | 10 (5.4) | 1–7 | 68.8 ± 10.9 | 141 (77.0) | - | 164 (89.0) | 135 (73.0) | 50 (27.0) | 61 (33.0) | 36 (20.0) | |
| 20 | Hirooka et al. [27] | 2008 | Asia | Prospective | 158 | 5 (3.2) | 1–7 | 67.2 ± 6.5 | 150 (95.0) | - | - | 128 (81.0) | - | 111 (70.0) | - | - |
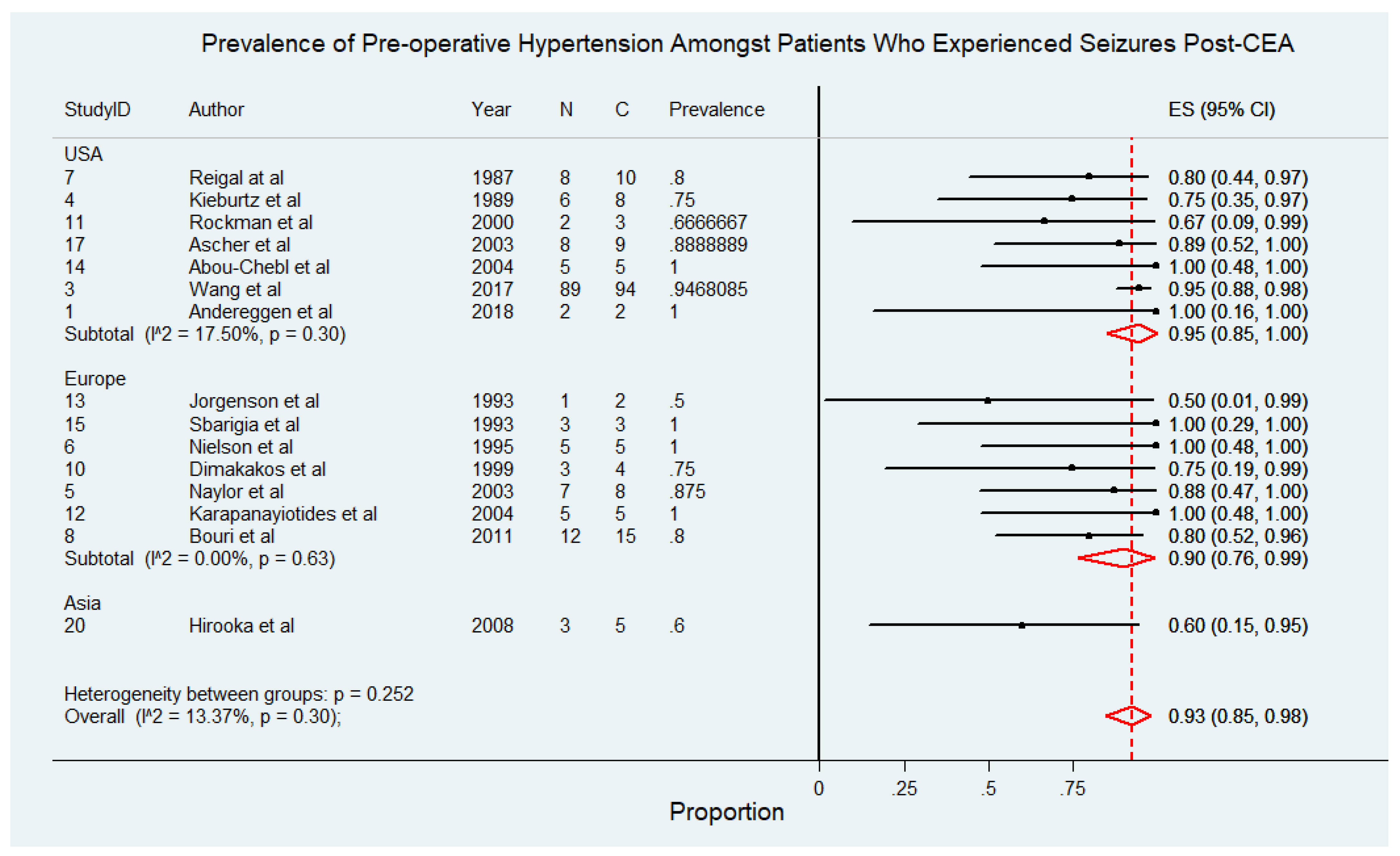
3.3. Prevalence of Pre-Operative Hypertension Among Patients Who Experienced Seizures Post-CEA
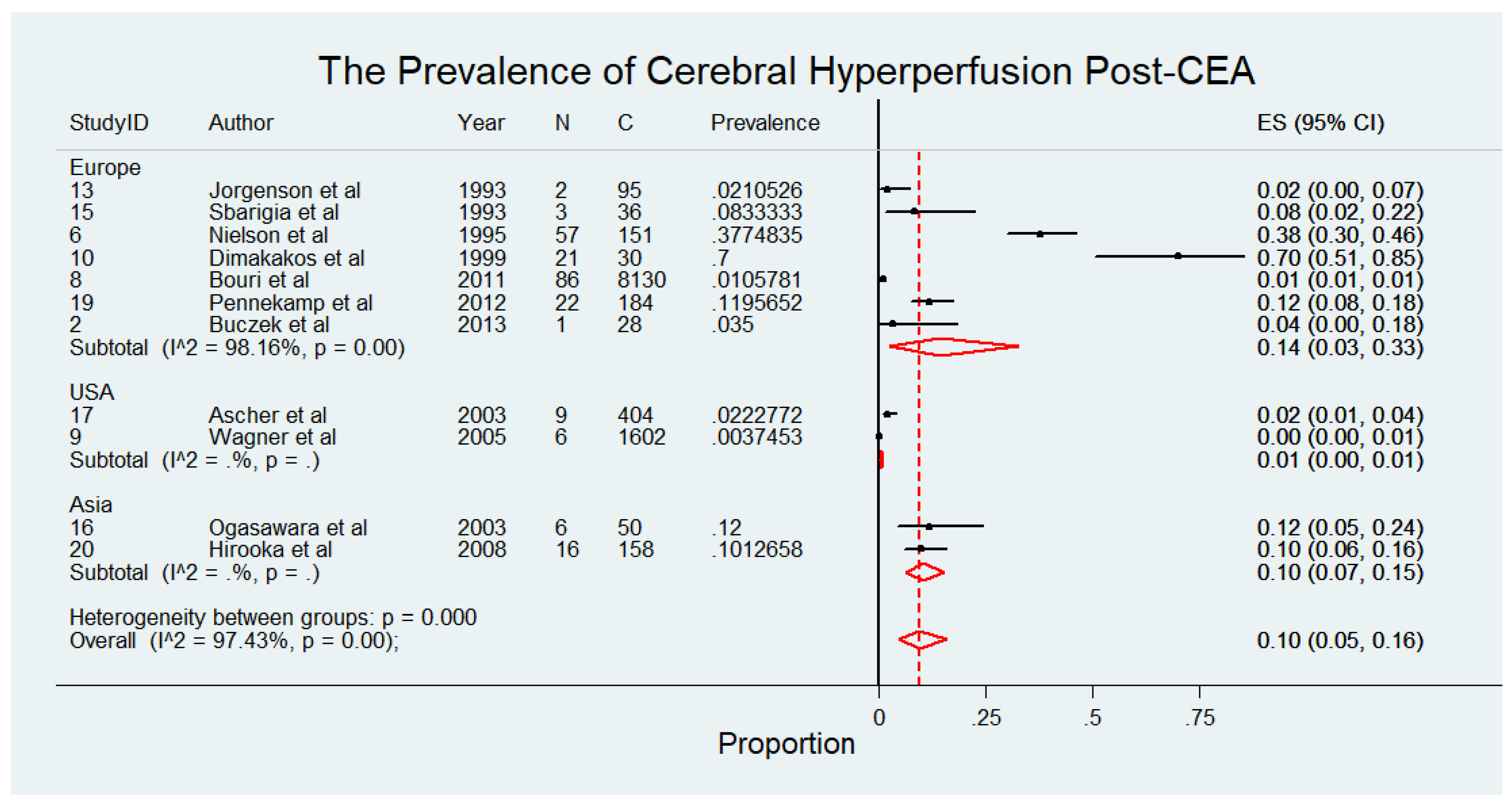
3.4. Prevalence of Cerebral Hyperperfusion Post-CEA
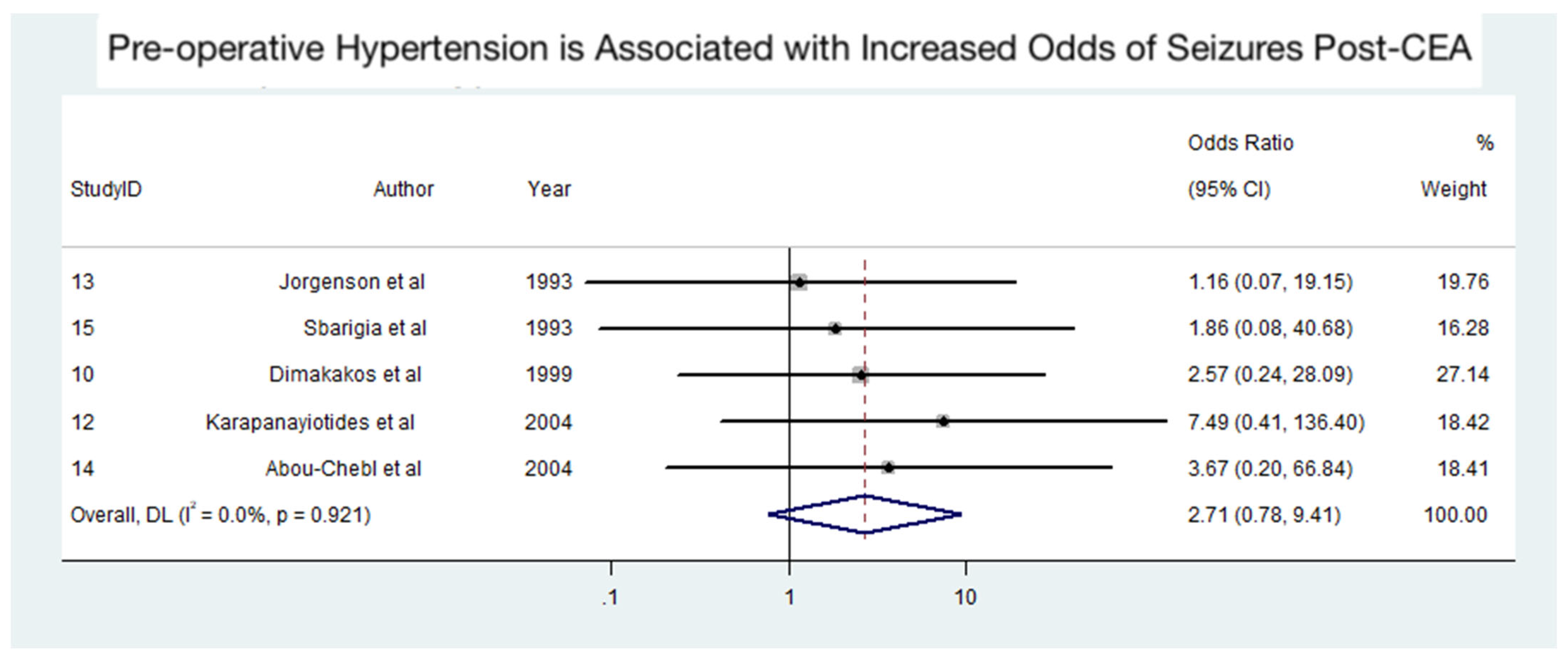
3.5. Association Between Pre-Operative Hypertension and Seizures Post-CEA
4. Discussion
4.1. Limitations
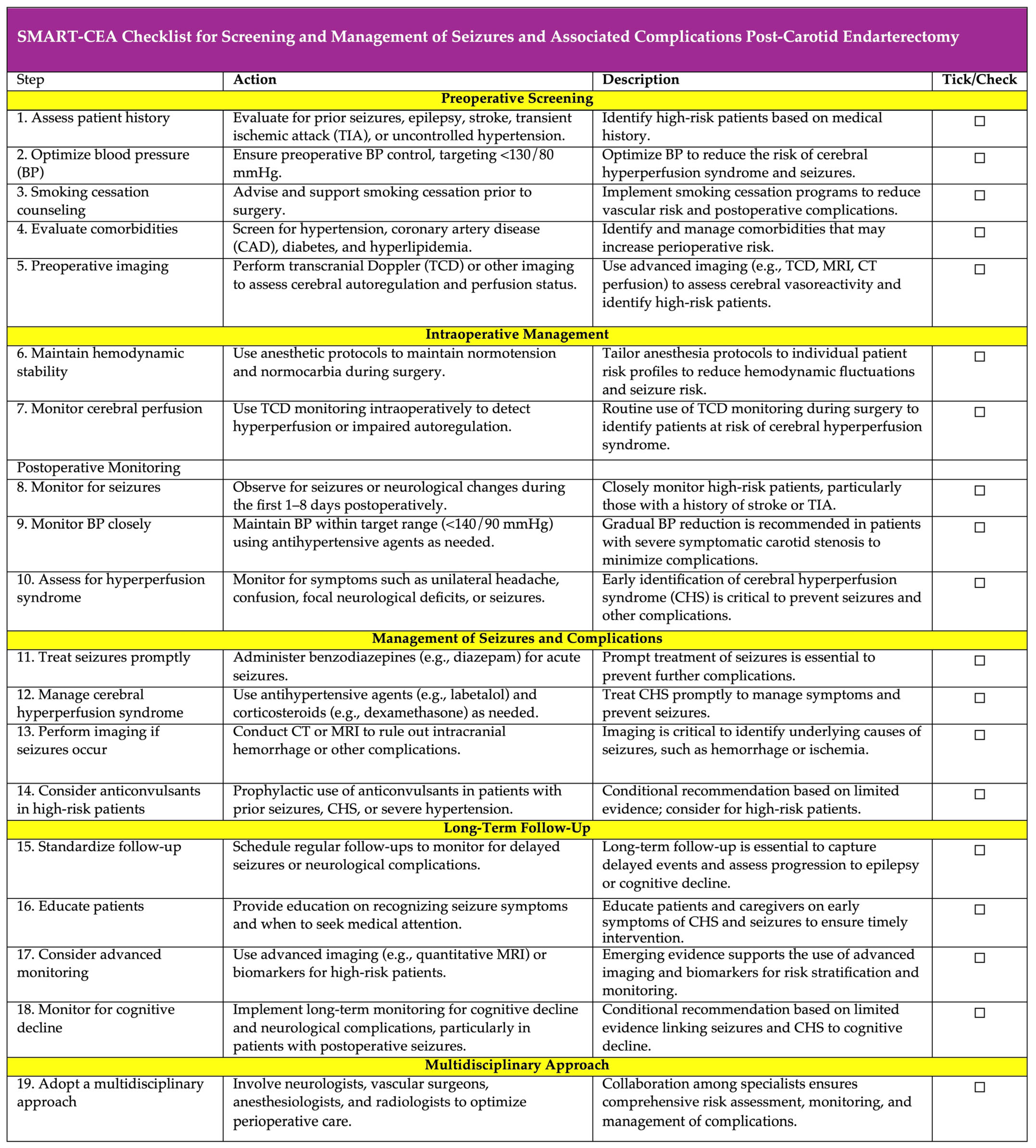
4.2. Recommendations
SMART-CEA Checklist: A Practical Framework for Preventing and Managing Postoperative Seizures Following Carotid Endarterectomy
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Rerkasem, A.; Orrapin, S.; Howard, D.P.; Rerkasem, K. Carotid endarterectomy for symptomatic carotid stenosis. Cochrane Database Syst. Rev. 2020, 9, CD001081. [Google Scholar] [CrossRef]
- Morris, D.R.; Ayabe, K.; Inoue, T.; Sakai, N.; Bulbulia, R.; Halliday, A.; Goto, S. Evidence-Based Carotid Interventions for Stroke Prevention: State-of-the-art Review. J. Atheroscler. Thromb. 2017, 24, 373–387. [Google Scholar] [CrossRef] [PubMed]
- Manole, A.M.; Sirbu, C.A.; Mititelu, M.R.; Vasiliu, O.; Lorusso, L.; Sirbu, O.M.; Ionita Radu, F. State of the Art and Challenges in Epilepsy-A Narrative Review. J. Pers. Med. 2023, 13, 623. [Google Scholar] [CrossRef]
- Nielsen, T.G.; Sillesen, H.; Schroeder, T.V. Seizures following carotid endarterectomy in patients with severely compromised cerebral circulation. Eur. J. Vasc. Endovasc. Surg. 1995, 9, 53–57. [Google Scholar] [CrossRef]
- Buczek, J.; Karlinski, M.; Kobayashi, A.; Bialek, P.; Czlonkowska, A. Hyperperfusion syndrome after carotid endarterectomy and carotid stenting. Cerebrovasc. Dis. 2013, 35, 531–537. [Google Scholar] [CrossRef]
- Naylor, A.R.; Evans, J.; Thompson, M.M.; London, N.J.; Abbott, R.J.; Cherryman, G.; Bell, P.R. Seizures after carotid endarterectomy: Hyperperfusion, dysautoregulation or hypertensive encephalopathy? Eur. J. Vasc. Endovasc. Surg. 2003, 26, 39–44. [Google Scholar] [CrossRef] [PubMed]
- Biller, J.; Feinberg, W.M.; Castaldo, J.E.; Whittemore, A.D.; Harbaugh, R.E.; Dempsey, R.J.; Caplan, L.R.; Kresowik, T.F.; Matchar, D.B.; Toole, J.; et al. Guidelines for carotid endarterectomy: A statement for healthcare professionals from a special writing group of the Stroke Council, American Heart Association. Stroke 1998, 29, 554–562. [Google Scholar] [CrossRef] [PubMed]
- Kieburtz, K.; Ricotta, J.J.; Moxley, R.T., 3rd. Seizures following carotid endarterectomy. Arch. Neurol. 1990, 47, 568–570. [Google Scholar] [CrossRef] [PubMed]
- Wang, G.J.; Beck, A.W.; DeMartino, R.R.; Goodney, P.P.; Rockman, C.B.; Fairman, R.M. Insight into the cerebral hyperperfusion syndrome following carotid endarterectomy from the national Vascular Quality Initiative. J. Vasc. Surg. 2017, 65, 381–389 e382. [Google Scholar] [CrossRef] [PubMed]
- Reigel, M.M.; Hollier, L.H.; Sundt, T.M., Jr.; Piepgras, D.G.; Sharbrough, F.W.; Cherry, K.J. Cerebral hyperperfusion syndrome: A cause of neurologic dysfunction after carotid endarterectomy. J. Vasc. Surg. 1987, 5, 628–634. [Google Scholar] [CrossRef] [PubMed]
- Andereggen, L.; Amin-Hanjani, S.; El-Koussy, M.; Verma, R.K.; Yuki, K.; Schoeni, D.; Hsieh, K.; Gralla, J.; Schroth, G.; Beck, J.; et al. Quantitative magnetic resonance angiography as a potential predictor for cerebral hyperperfusion syndrome: A preliminary study. J. Neurosurg. 2018, 128, 1006–1014. [Google Scholar] [CrossRef] [PubMed]
- Di Gennaro, G.; Casciato, S.; Quarato, P.P.; Mascia, A.; D’Aniello, A.; Grammaldo, L.G.; De Risi, M.; Meldolesi, G.N.; Romigi, A.; Esposito, V.; et al. Acute postoperative seizures and long-term seizure outcome after surgery for hippocampal sclerosis. Seizure 2015, 24, 59–62. [Google Scholar] [CrossRef] [PubMed]
- Fiest, K.M.; Sauro, K.M.; Wiebe, S.; Patten, S.B.; Kwon, C.S.; Dykeman, J.; Pringsheim, T.; Lorenzetti, D.L.; Jette, N. Prevalence and incidence of epilepsy: A systematic review and meta-analysis of international studies. Neurology 2017, 88, 296–303. [Google Scholar] [CrossRef]
- Stavem, K.; Bjornaes, H.; Langmoen, I.A. Long-term seizures and quality of life after epilepsy surgery compared with matched controls. Neurosurgery 2008, 62, 326–334; discussion 334-325. [Google Scholar] [CrossRef] [PubMed]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef] [PubMed]
- Stafstrom, C.E.; Carmant, L. Seizures and epilepsy: An overview for neuroscientists. Cold Spring Harb. Perspect. Med. 2015, 5. [Google Scholar] [CrossRef] [PubMed]
- Carey, R.M.; Whelton, P.K. Evidence for the Universal Blood Pressure Goal of <130/80 mm Hg Is Strong: Controversies in Hypertension—Pro Side of the Argument. Hypertension 2020, 76, 1384–1390. [Google Scholar] [CrossRef]
- Pennekamp, C.W.; Moll, F.L.; De Borst, G.J. Role of transcranial Doppler in cerebral hyperperfusion syndrome. J. Cardiovasc. Surg. 2012, 53, 765–771. [Google Scholar]
- Wan, X.; Wang, W.; Liu, J.; Tong, T. Estimating the sample mean and standard deviation from the sample size, median, range and/or interquartile range. BMC Med. Res. Methodol. 2014, 14, 135. [Google Scholar] [CrossRef] [PubMed]
- Wagner, W.H.; Cossman, D.V.; Farber, A.; Levin, P.M.; Cohen, J.L. Hyperperfusion syndrome after carotid endarterectomy. Ann. Vasc. Surg. 2005, 19, 479–486. [Google Scholar] [CrossRef] [PubMed]
- Sbarigia, E.; Speziale, F.; Giannoni, M.F.; Colonna, M.; Panico, M.A.; Fiorani, P. Post-carotid endarterectomy hyperperfusion syndrome: Preliminary observations for identifying at risk patients by transcranial Doppler sonography and the acetazolamide test. Eur. J. Vasc. Surg. 1993, 7, 252–256. [Google Scholar] [CrossRef] [PubMed]
- Rockman, C.B.; Jacobowitz, G.R.; Lamparello, P.J.; Adelman, M.A.; Woo, D.; Schanzer, A.; Gagne, P.J.; Landis, R.; Riles, T.S. Immediate reexploration for the perioperative neurologic event after carotid endarterectomy: Is it worthwhile? J. Vasc. Surg. 2000, 32, 1062–1070. [Google Scholar] [CrossRef]
- Pennekamp, C.W.; Tromp, S.C.; Ackerstaff, R.G.; Bots, M.L.; Immink, R.V.; Spiering, W.; de Vries, J.P.; Kappelle, L.J.; Moll, F.L.; Buhre, W.F.; et al. Prediction of cerebral hyperperfusion after carotid endarterectomy with transcranial Doppler. Eur. J. Vasc. Endovasc. Surg. 2012, 43, 371–376. [Google Scholar] [CrossRef] [PubMed]
- Ogasawara, K.; Konno, H.; Yukawa, H.; Endo, H.; Inoue, T.; Ogawa, A. Transcranial regional cerebral oxygen saturation monitoring during carotid endarterectomy as a predictor of postoperative hyperperfusion. Neurosurgery 2003, 53, 309–314; discussion 314-305. [Google Scholar] [CrossRef] [PubMed]
- Karapanayiotides, T.; Meuli, R.; Devuyst, G.; Piechowski-Jozwiak, B.; Dewarrat, A.; Ruchat, P.; Von Segesser, L.; Bogousslavsky, J. Postcarotid endarterectomy hyperperfusion or reperfusion syndrome. Stroke 2005, 36, 21–26. [Google Scholar] [CrossRef] [PubMed]
- Jorgensen, L.G.; Schroeder, T.V. Defective cerebrovascular autoregulation after carotid endarterectomy. Eur. J. Vasc. Surg. 1993, 7, 370–379. [Google Scholar] [CrossRef]
- Hirooka, R.; Ogasawara, K.; Sasaki, M.; Yamadate, K.; Kobayashi, M.; Suga, Y.; Yoshida, K.; Otawara, Y.; Inoue, T.; Ogawa, A. Magnetic resonance imaging in patients with cerebral hyperperfusion and cognitive impairment after carotid endarterectomy. J. Neurosurg. 2008, 108, 1178–1183. [Google Scholar] [CrossRef]
- Dimakakos, P.B.; Tsiligiris, V.; Gouliamos, A.; Kotsis, T.E.; Katsaros, G. Postcarotid endarterectomy symptoms. Pre- and postoperative clinical and MRI findings. Int. Angiol. 1999, 18, 277–286. [Google Scholar]
- Dalman, J.E.; Beenakkers, I.C.; Moll, F.L.; Leusink, J.A.; Ackerstaff, R.G. Transcranial Doppler monitoring during carotid endarterectomy helps to identify patients at risk of postoperative hyperperfusion. Eur. J. Vasc. Endovasc. Surg. 1999, 18, 222–227. [Google Scholar] [CrossRef] [PubMed]
- Bouri, S.; Thapar, A.; Shalhoub, J.; Jayasooriya, G.; Fernando, A.; Franklin, I.J.; Davies, A.H. Hypertension and the post-carotid endarterectomy cerebral hyperperfusion syndrome. Eur. J. Vasc. Endovasc. Surg. 2011, 41, 229–237. [Google Scholar] [CrossRef]
- Ascher, E.; Markevich, N.; Schutzer, R.W.; Kallakuri, S.; Jacob, T.; Hingorani, A.P. Cerebral hyperperfusion syndrome after carotid endarterectomy: Predictive factors and hemodynamic changes. J. Vasc. Surg. 2003, 37, 769–777. [Google Scholar] [CrossRef] [PubMed]
- Abou-Chebl, A.; Yadav, J.S.; Reginelli, J.P.; Bajzer, C.; Bhatt, D.; Krieger, D.W. Intracranial hemorrhage and hyperperfusion syndrome following carotid artery stenting: Risk factors, prevention, and treatment. J. Am. Coll. Cardiol. 2004, 43, 1596–1601. [Google Scholar] [CrossRef] [PubMed]
- van Mook, W.N.; Rennenberg, R.J.; Schurink, G.W.; van Oostenbrugge, R.J.; Mess, W.H.; Hofman, P.A.; de Leeuw, P.W. Cerebral hyperperfusion syndrome. Lancet Neurol. 2005, 4, 877–888. [Google Scholar] [CrossRef]
- Edwards, A.M.; Birchler, C.R.; Park, S.; Baker, J.M.; Molnar, R.G. Cerebral Hyperperfusion Syndrome Presenting As Status Epilepticus Following Carotid Endarterectomy. Cureus 2021, 13, e20551. [Google Scholar] [CrossRef]
- Sharifian, M. Hypertensive encephalopathy. Iran. J. Child. Neurol. 2012, 6, 1–7. [Google Scholar] [PubMed]
- Aceto, P.; Lai, C.; De Crescenzo, F.; Crea, M.A.; Di Franco, V.; Pellicano, G.R.; Perilli, V.; Lai, S.; Papanice, D.; Sollazzi, L. Cognitive decline after carotid endarterectomy: Systematic review and meta-analysis. Eur. J. Anaesthesiol. 2020, 37, 1066–1074. [Google Scholar] [CrossRef]
- Galyfos, G.; Sianou, A.; Filis, K. Cerebral hyperperfusion syndrome and intracranial hemorrhage after carotid endarterectomy or carotid stenting: A meta-analysis. J. Neurol. Sci. 2017, 381, 74–82. [Google Scholar] [CrossRef] [PubMed]
- Huibers, A.E.; Westerink, J.; de Vries, E.E.; Hoskam, A.; den Ruijter, H.M.; Moll, F.L.; de Borst, G.J. Editor’s Choice—Cerebral Hyperperfusion Syndrome After Carotid Artery Stenting: A Systematic Review and Meta-analysis. Eur. J. Vasc. Endovasc. Surg. 2018, 56, 322–333. [Google Scholar] [CrossRef] [PubMed]
- Goldstein, L.B.; Hasselblad, V.; Matchar, D.B.; McCrory, D.C. Comparison and meta-analysis of randomized trials of endarterectomy for symptomatic carotid artery stenosis. Neurology 1995, 45, 1965–1970. [Google Scholar] [CrossRef]
- Magee, T.R.; Davies, A.H.; Horrocks, M. Transcranial Doppler evaluation of cerebral hyperperfusion syndrome after carotid endarterectomy. Eur. J. Vasc. Surg. 1994, 8, 104–106. [Google Scholar] [CrossRef]
- Katyal, A.; Bhaskar, S.M.M. Value of pre-intervention CT perfusion imaging in acute ischemic stroke prognosis. Diagn. Interv. Radiol. 2021, 27, 774–785. [Google Scholar] [CrossRef] [PubMed]
- Bagley, J.H.; Priest, R. Carotid Revascularization: Current Practice and Future Directions. Semin. Intervent Radiol. 2020, 37, 132–139. [Google Scholar] [CrossRef] [PubMed]
- Gurm, H.S.; Yadav, J.S.; Fayad, P.; Katzen, B.T.; Mishkel, G.J.; Bajwa, T.K.; Ansel, G.; Strickman, N.E.; Wang, H.; Cohen, S.A.; et al. Long-term results of carotid stenting versus endarterectomy in high-risk patients. N. Engl. J. Med. 2008, 358, 1572–1579. [Google Scholar] [CrossRef] [PubMed]
- Trystula, M.; Musialek, P. Transient flow reversal combined with sustained embolic prevention in transcervical revascularization of symptomatic and highly-emboligenic carotid stenoses for optimized endovascular lumen reconstruction and improved peri- and post-procedural outcomes. Postep. Kardiol. Interwencyjnej 2020, 16, 495–506. [Google Scholar] [CrossRef]
- Zhang, G.Q.; Bose, S.; Stonko, D.P.; Abularrage, C.J.; Zarkowsky, D.S.; Hicks, C.W. Transcarotid artery revascularization is associated with similar outcomes to carotid endarterectomy regardless of patient risk status. J. Vasc. Surg. 2022, 76, 474–481 e473. [Google Scholar] [CrossRef]
- Ezzeldin, M.; Hassan, A.E.; Kerro, A.; Martucci, M.; Hussain, M.S.; Mir, O.; Sheriff, F.G.; Kan, P.; Ezepue, C.; Janjua, N.A.; et al. Carotid Artery Stenting Outcomes by Neurointerventional Surgeons (CASONI). Stroke Vasc. Interv. Neurol. 2024, 0, e001459. [Google Scholar] [CrossRef]
- Farooq, M.U.; Goshgarian, C.; Min, J.; Gorelick, P.B. Pathophysiology and management of reperfusion injury and hyperperfusion syndrome after carotid endarterectomy and carotid artery stenting. Exp. Transl. Stroke Med. 2016, 8, 7. [Google Scholar] [CrossRef] [PubMed]
- McCleary, A.J.; Maritati, G.; Gough, M.J. Carotid endarterectomy; local or general anaesthesia? Eur. J. Vasc. Endovasc. Surg. 2001, 22, 1–12. [Google Scholar] [CrossRef]
- Stoneham, M.D.; Stamou, D.; Mason, J. Regional anaesthesia for carotid endarterectomy. Br. J. Anaesth. 2015, 114, 372–383. [Google Scholar] [CrossRef]
- Sultan, S.; Acharya, Y.; Dulai, M.; Tawfick, W.; Hynes, N.; Wijns, W.; Soliman, O. Redefining postoperative hypertension management in carotid surgery: A comprehensive analysis of blood pressure homeostasis and hyperperfusion syndrome in unilateral vs. bilateral carotid surgeries and implications for clinical practice. Front. Surg. 2024, 11, 1361963. [Google Scholar] [CrossRef]
- Kim, K.H.; Lee, C.H.; Son, Y.J.; Yang, H.J.; Chung, Y.S.; Lee, S.H. Post-carotid endarterectomy cerebral hyperperfusion syndrome: Is it preventable by strict blood pressure control? J. Korean Neurosurg. Soc. 2013, 54, 159–163. [Google Scholar] [CrossRef] [PubMed]
- Hoel, A.W.; Nolan, B.W.; Goodney, P.P.; Zhao, Y.; Schanzer, A.; Stanley, A.C.; Eldrup-Jorgensen, J.; Cronenwett, J.L.; Vascular Study Group of New, E. Variation in smoking cessation after vascular operations. J. Vasc. Surg. 2013, 57, 1338–1344.e1. [Google Scholar] [CrossRef] [PubMed]
- Kim, T.I.; Zhang, Y.; Amin, H.P.; Ochoa Chaar, C.I. Presentation and outcomes of carotid endarterectomy in active smokers. J. Vasc. Surg. 2020, 72, 1720–1727.e1. [Google Scholar] [CrossRef] [PubMed]
- Straus, S.; Vootukuru, N.; Willie-Permor, D.; Elsayed, N.; Ross, E.; Malas, M. The Effect of Preoperative Smoking Status on Carotid Endarterectomy Outcomes in Asymptomatic Patients. J. Vasc. Surg. 2024. [Google Scholar] [CrossRef] [PubMed]
- Chamseddine, H.; Shepard, A.; Constantinou, C.; Nypaver, T.; Weaver, M.; Boules, T.; Kavousi, Y.; Onofrey, K.; Peshkepija, A.; Halabi, M.; et al. Pre-operative Smoking Cessation Improves Carotid Endarterectomy Outcomes in Asymptomatic Carotid Stenosis Patients. J. Vasc. Surg. 2024. [Google Scholar] [CrossRef]
- Eckstein, H.H. European Society for Vascular Surgery Guidelines on the Management of Atherosclerotic Carotid and Vertebral Artery Disease. Eur. J. Vasc. Endovasc. Surg. 2018, 55, 1–2. [Google Scholar] [CrossRef]
- Fassaert, L.M.M.; Immink, R.V.; van Vriesland, D.J.; de Vries, J.P.M.; Toorop, R.J.; Kappelle, L.J.; Westerink, J.; Tromp, S.C.; de Borst, G.J. Transcranial Doppler 24 Hours after Carotid Endarterectomy Accurately Identifies Patients Not at Risk of Cerebral Hyperperfusion Syndrome. Eur. J. Vasc. Endovasc. Surg. 2019, 58, 320–327. [Google Scholar] [CrossRef] [PubMed]
- Li, Q.; Hua, Y.; Liu, J.; Zhou, F.; Du, L.; Li, J.; Li, Q.; Jiao, L. Intraoperative Transcranial Doppler Monitoring Predicts the Risk of Cerebral Hyperperfusion Syndrome After Carotid Endarterectomy. World Neurosurg. 2022, 165, e571–e580. [Google Scholar] [CrossRef] [PubMed]
- Mehdi, Z.; Birns, J.; Partridge, J.; Bhalla, A.; Dhesi, J. Perioperative management of adult patients with a history of stroke or transient ischaemic attack undergoing elective non-cardiac surgery. Clin. Med. 2016, 16, 535–540. [Google Scholar] [CrossRef]
- Yokoyama, T.; Sunaga, S.; Onuki, H.; Otsuka, K.; Jimbo, H. Nonconvulsive Status Epilepticus Associated with Cerebral Hyperperfusion Syndrome after Carotid Endarterectomy: A Case Report. NMC Case Rep. J. 2023, 10, 197–202. [Google Scholar] [CrossRef]
- Lin, Y.H.; Liu, H.M. Update on cerebral hyperperfusion syndrome. J. Neurointerv. Surg. 2020, 12, 788–793. [Google Scholar] [CrossRef]
- Bevilacqua, S.; Ticozzelli, G.; Orso, M.; Alba, G.; Capoccia, L.; Cappelli, A.; Cernetti, C.; Diomedi, M.; Dorigo, W.; Faggioli, G.; et al. Anesthetic management of carotid endarterectomy: An update from Italian guidelines. J. Anesth. Analg. Crit. Care 2022, 2, 24. [Google Scholar] [CrossRef]
- Chang, E.; Wu, L.; Li, X.; Zhou, J.; Zhi, H.; Sun, M.; Chen, G.; Bi, J.; Li, L.; Li, T.; et al. Dexmedetomidine decreases cerebral hyperperfusion incidence following carotid stenting: A double-blind, randomized controlled trial. Med. 2024. [Google Scholar] [CrossRef]
- Fan, X.; Lai, Z.; Lin, T.; You, H.; Wei, J.; Li, M.; Liu, C.; Feng, F. Pre-operative Cerebral Small Vessel Disease on MR Imaging Is Associated With Cerebral Hyperperfusion After Carotid Endarterectomy. Front. Cardiovasc. Med. 2021, 8, 734392. [Google Scholar] [CrossRef] [PubMed]
- Fujimoto, S.; Toyoda, K.; Inoue, T.; Hirai, Y.; Uwatoko, T.; Kishikawa, K.; Yasumori, K.; Ibayashi, S.; Iida, M.; Okada, Y. Diagnostic impact of transcranial color-coded real-time sonography with echo contrast agents for hyperperfusion syndrome after carotid endarterectomy. Stroke 2004, 35, 1852–1856. [Google Scholar] [CrossRef]
- Bender, M.; Malojčić, B. The utility of transcranial color Doppler in cerebral hyperperfusion syndrome. Front. Neurol. 2023, 14, 1223016. [Google Scholar] [CrossRef]
- Hu, M.; Zhang, C.; Xiao, X.; Guo, J.; Sun, H. Effect of intensive self-management education on seizure frequency and quality of life in epilepsy patients with prodromes or precipitating factors. Seizure—Eur. J. Epilepsy 2020, 78, 38–42. [Google Scholar] [CrossRef]
- Aliasgharpour, M.; Dehgahn Nayeri, N.; Yadegary, M.A.; Haghani, H. Effects of an educational program on self-management in patients with epilepsy. Seizure 2013, 22, 48–52. [Google Scholar] [CrossRef]
- Chang, C.H.; Chang, T.Y.; Chang, Y.J.; Huang, K.L.; Chin, S.C.; Ryu, S.J.; Yang, T.C.; Lee, T.H. The role of perfusion computed tomography in the prediction of cerebral hyperperfusion syndrome. PLoS ONE 2011, 6, e19886. [Google Scholar] [CrossRef]
- Araya, S.; Akamatsu, Y.; Ono, Y.; Yamazaki, R.; Fujiwara, S.; Chida, K.; Kobayashi, M.; Koji, T.; Ogasawara, K. Impact of postoperative cerebral hyperperfusion on 2-year cognitive outcomes of patients undergoing carotid endarterectomy. J. Neurosurg. 2024, 1–8. [Google Scholar] [CrossRef] [PubMed]
| Specific Recommendation | Explanation | Grading | Grading Justification |
|---|---|---|---|
| Optimize pre-operative blood pressure (BP) control | Pre-operative BP control should be optimized, particularly in patients with hypertension, to reduce the risk of cerebral hyperperfusion syndrome and seizures post-CEA. | 1b | Strong recommendation supported by good-quality evidence from observational studies and clinical guidelines showing hypertension as a significant risk factor for postoperative complications [38,56]. |
| Routine use of transcranial Doppler (TCD) monitoring | Routine use of TCD monitoring during and after CEA to identify patients at risk of cerebral hyperperfusion syndrome. | 2a | Moderate-quality evidence from observational studies and clinical practice guidelines demonstrating the utility of TCD in detecting hyperperfusion and preventing complications [29,57,58]. |
| Monitor patients with history of stroke or transient ischemic attack (TIA) postoperatively | Patients with a history of stroke or TIA should be closely monitored postoperatively for seizures, as they represent a high-risk subgroup. | 2b | Moderate-quality evidence from observational studies indicates that prior cerebrovascular events increase the risk of seizures post-CEA, though further research is needed to confirm causality [59]. |
| Implement smoking cessation programs pre-operatively | Smoking cessation programs should be implemented pre-operatively for patients undergoing CEA to reduce overall vascular risk and potential postoperative complications. | 2b | Weaker recommendation based on lower-quality evidence from observational studies linking smoking to worse vascular outcomes, though direct evidence for seizure prevention is limited [52,53,54,55]. |
| Standardize long-term follow-up for seizure development post-CEA | Long-term follow-up and monitoring for seizure development post-CEA should be standardized, extending beyond the immediate postoperative period to capture delayed events. | 2c | Conditional recommendation based on emerging evidence and expert consensus, as current studies lack consistent long-term follow-up data to assess seizure progression or epilepsy development [60]. |
| Use perioperative anesthetic protocols to maintain normotension and normocarbia | Use of perioperative anesthetic protocols that maintain normotension and normocarbia to minimize the risk of cerebral hyperperfusion syndrome and associated seizures. | 2a | Moderate-quality evidence from observational studies and clinical practice guidelines regarding perioperative management studies showing that maintaining stable hemodynamics reduces the risk of hyperperfusion and seizures [61,62]. |
| Treat cerebral hyperperfusion syndrome with antihypertensive agents and sedatives | Patients with cerebral hyperperfusion syndrome should be promptly treated with antihypertensive agents (e.g., labetalol) or sedatives (e.g., Dexmedetomidine) to manage symptoms and prevent seizures. | 2b | Moderate-quality evidence from observational studies and clinical practice guidelines supports the use of these interventions, though randomized controlled trials are lacking [47,63]. |
| Future studies should focus on identifying biomarkers or imaging predictors | Future studies should focus on identifying biomarkers or imaging predictors (e.g., quantitative MRI or TCD) for seizure risk stratification in patients undergoing CEA. | Not graded | No specific grade assigned due to the lack of direct evidence; this recommendation reflects the need for further research to improve risk prediction and patient outcomes [57,64,65]. |
| Early identification and management of cerebral hyperperfusion syndrome (CHS) | Implement early identification protocols for CHS using TCD or advanced imaging modalities (e.g., MRI, CT perfusion) to detect hyperperfusion and prevent complications such as seizures. | 2a | Moderate-quality evidence supports the use of TCD and imaging for identifying CHS, though further research is needed to standardize protocols and validate their effectiveness [29,58,66]. |
| Gradual blood pressure reduction in severe symptomatic carotid stenosis | Gradually reduce blood pressure in patients with severe symptomatic carotid stenosis to minimize the risk of stroke progression and hyperperfusion syndrome. | 2a | Observational studies and expert consensus suggest that gradual blood pressure management reduces complications, though high-quality RCTs are lacking [61]. |
| Use of anticonvulsants in high-risk patients | Consider prophylactic use of anticonvulsants in high-risk patients (e.g., those with prior seizures, CHS, or severe hypertension) undergoing CEA. | 2c | Conditional recommendation based on limited evidence and expert consensus, with a need for further research to establish efficacy and safety [61]. |
| Tailored perioperative anesthesia protocols | Tailor anesthesia protocols to individual patient risk profiles, including the use of regional anesthesia where appropriate, to reduce hemodynamic fluctuations and seizure risk. | 2b | Moderate-quality evidence supports the benefits of regional anesthesia, though its applicability may vary based on patient and procedural factors [6,48,49]. |
| Patient education on postoperative symptoms | Educate patients and caregivers on recognizing early symptoms of CHS and seizures (e.g., severe headache, confusion, focal neurological deficits) to ensure prompt medical attention. | 2c | Conditional recommendation based on expert consensus, as evidence on the impact of patient education on outcomes is limited [67,68]. |
| Standardized use of advanced imaging for risk stratification | Incorporate advanced imaging techniques (e.g., quantitative MRI, CT perfusion) preoperatively to assess cerebral vasoreactivity and identify patients at high risk for postoperative seizures. | 2c | Emerging evidence supports the utility of advanced imaging, but further studies are needed to validate its role in routine clinical practice [64,69]. |
| Multidisciplinary approach to perioperative care | Adopt a multidisciplinary approach involving neurologists, vascular surgeons, anesthesiologists, and radiologists to optimize perioperative care and reduce seizure risk. | Not graded | No specific evidence available to grade this recommendation, but it reflects expert consensus and best practices in perioperative care. |
| Long-term monitoring for cognitive decline | Implement long-term monitoring for cognitive decline and neurological complications in patients undergoing CEA, particularly those with postoperative seizures. | 2c | Conditional recommendation based on limited evidence linking seizures and CHS to cognitive decline, with a need for further research [70]. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rajesh, K.; Shen, H.; Bhaskar, S.M.M. Seizures Following Carotid Endarterectomy: A Comprehensive Meta-Analysis of 69,479 Patients and Evidence-Based Recommendations for Perioperative Care. Diagnostics 2025, 15, 6. https://doi.org/10.3390/diagnostics15010006
Rajesh K, Shen H, Bhaskar SMM. Seizures Following Carotid Endarterectomy: A Comprehensive Meta-Analysis of 69,479 Patients and Evidence-Based Recommendations for Perioperative Care. Diagnostics. 2025; 15(1):6. https://doi.org/10.3390/diagnostics15010006
Chicago/Turabian StyleRajesh, Kruthajn, Helen Shen, and Sonu M. M. Bhaskar. 2025. "Seizures Following Carotid Endarterectomy: A Comprehensive Meta-Analysis of 69,479 Patients and Evidence-Based Recommendations for Perioperative Care" Diagnostics 15, no. 1: 6. https://doi.org/10.3390/diagnostics15010006
APA StyleRajesh, K., Shen, H., & Bhaskar, S. M. M. (2025). Seizures Following Carotid Endarterectomy: A Comprehensive Meta-Analysis of 69,479 Patients and Evidence-Based Recommendations for Perioperative Care. Diagnostics, 15(1), 6. https://doi.org/10.3390/diagnostics15010006