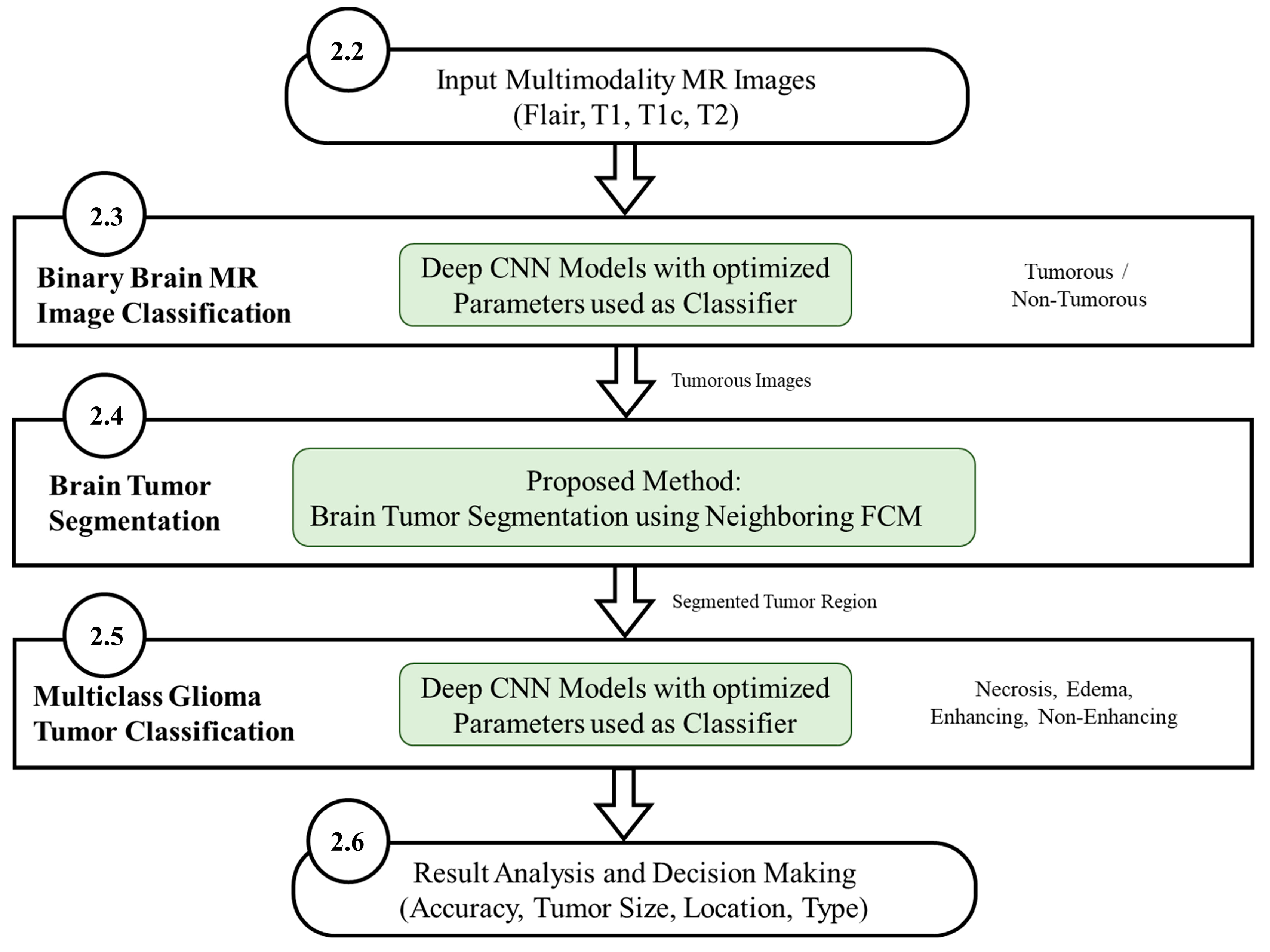
The final output of the proposed system should be able to specify whether an image contains a tumor or not. For images that contain a tumor, the system further segments the tumorous region and classifies the tumor into one of four classes; Necrosis, Edema, Enhancing and non-enhancing. The system further specifies based on analysis the location and size of the tumor. The information retrieved from the system outperforms previous methods mentioned in the literature in terms of accuracy, precision, recall and F measure which helps to determine a proper diagnosis and proper treatment.
3.1. Brain MR Image Classification Results
Several experiments with different parameter combinations of batch size (100, 200, and 500) and epochs (4, 8, 16, 32, and 64) were performed for the proposed CNN models. The batch size of 100 and epochs value of 8 was found to be achieving the best accuracy and thus chosen with results presented. As shown in
Table 7 and
Table 8, the accuracy, precision, recall, and F-measure for model 1 and model 2 are presented. The results are also compared with the existing well-known CNN models like LeNet [
27], AlexNet [
15,
16], and GoogleNet [
17,
28]. The AlexNet experiments show promising results with an accuracy of 96.95% and 96.53% for HGG and LGG, respectively as compared to LeNet and GoogleNet, but model 2 performance is far better than AlexNet, LeNet and GoogleNet. The famous CNN models (LeNet, AlexNet, GoogleNet) leads to overfitting and do not perform well for brain tumor classification because of complex architectures with high number of layers designed for very large number of output classes (1000 classes) with RGB input images. For example, AlexNet has 64 filters in the first convolutional layer which are mostly encoded with color information. Due to the small batch size for a large dataset of 169,880 MR images with enhanced CNN model 2, highest results are achieved with 8 epochs. It is also clear in the results that the number of Epochs is directly proportional to effectiveness. The effectiveness increases with the increase in the number of Epochs. The proposed models especially model 2 achieved the best accuracy for both LGG and HGG and for all modalities. For HGG, model 2 achieved the best classification accuracy for the flair modality of 98.74% with precision of 0.983, recall of 0.985, and F-measure of 0.984. For LGG, model 2 achieved the best accuracy for the flair modality of 97.33% with precision of 0.960, recall of 0.988, and F-measure of 0.974. Model 2 outperformed model 1 and outperform the well-known CNN models specified.
The proposed models are also tested on the AANLIB and PMIS datasets and results are compared with LeNet, AlexNet and GoogleNet CNN models as shown in
Table 9. The results are reaffirmed and validated showing that for both AANLIB and PMIS datasets, the proposed CNN models outperformed the well-known CNN models and that Model 2 in outperformed all other models by achieving 100% accuracy. This shows that the proposed models solve the problems of overfitting as well as problems of data availability.
Table 10 shows a summary of the results obtained in this work and a comparison with the latest literature. The proposed methods achieved an average accuracy ranging from 96.88% to a maximum of 98.74%, whereas, previously published results indicated relatively less accuracies as shown in
Table 10. The proposed CNN model 2 as classifier achieved 98.74% on a very large dataset (BraTS 2015). The accuracy obtained using the proposed approach in this work is very high even when using a big dataset (BraTS 2015), which shows the robustness of the approach.
3.2. Glioma Tumor Segmentation Results
Tumor regions were extracted from the tumorous images by ignoring the non-tumorous images using the proposed neighboring FCM based tumor segmentation method. The experimental results of brain tumor segmentation are evaluated based on visual comparison, accuracy, specificity, sensitivity, dice similarity coefficient (DSC) and mutual information (MI).
As shown in
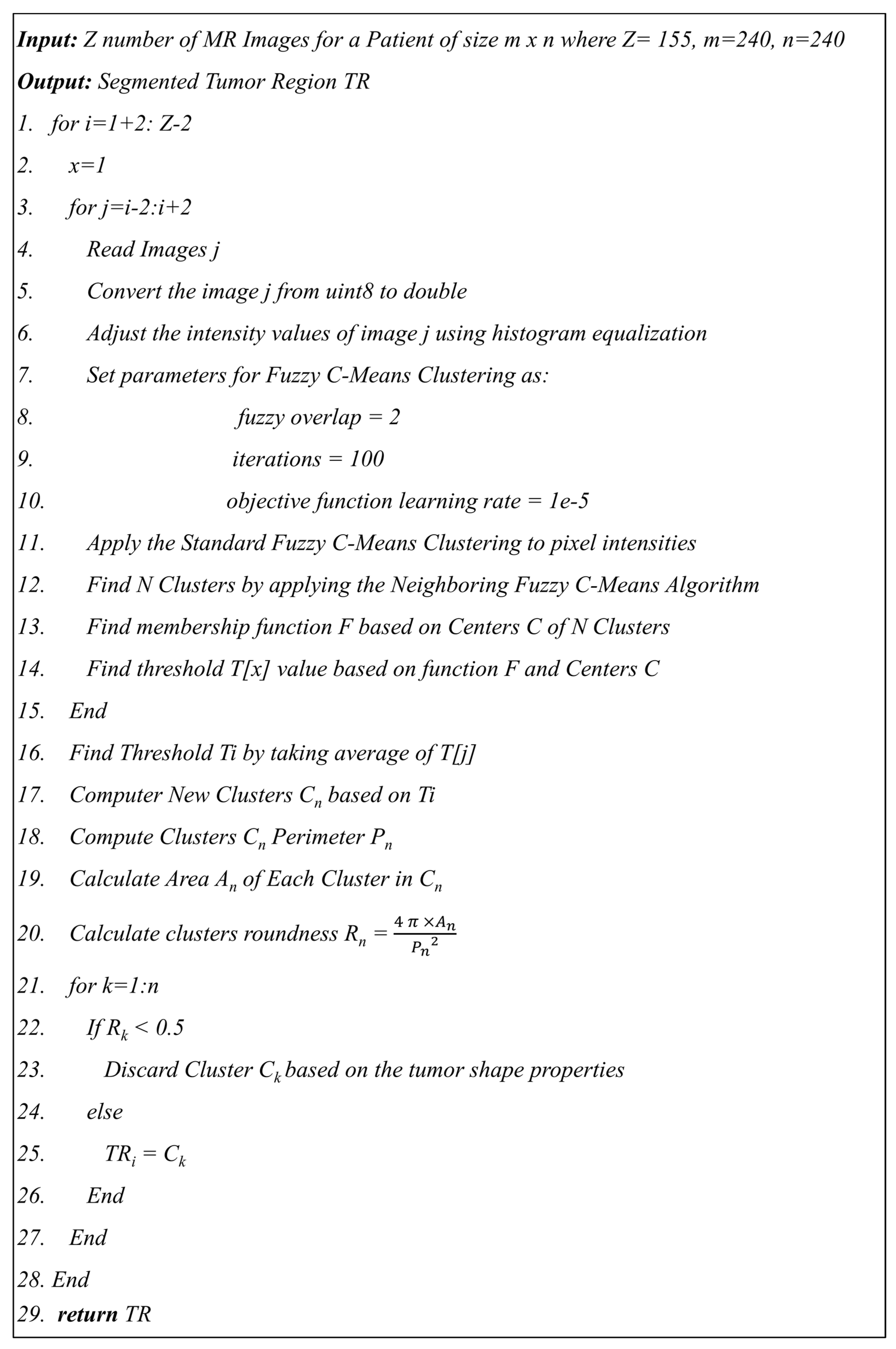
Figure 9 of the proposed algorithm, image intensity values were manipulated to enhance the segmentation by saturating the highest 1% and lowest 1% of all the pixel values in the MR image which enhances the contrast of the grayscale image. The enhancement method was applied to all the images before converting the image to black and white. The visual results are shown in
Figure 10 to compare the original brain MR sample image and the intensity manipulated image.
The previous two and following two images are used as a reference along with the actual image to calculate the threshold value for the segmentation.
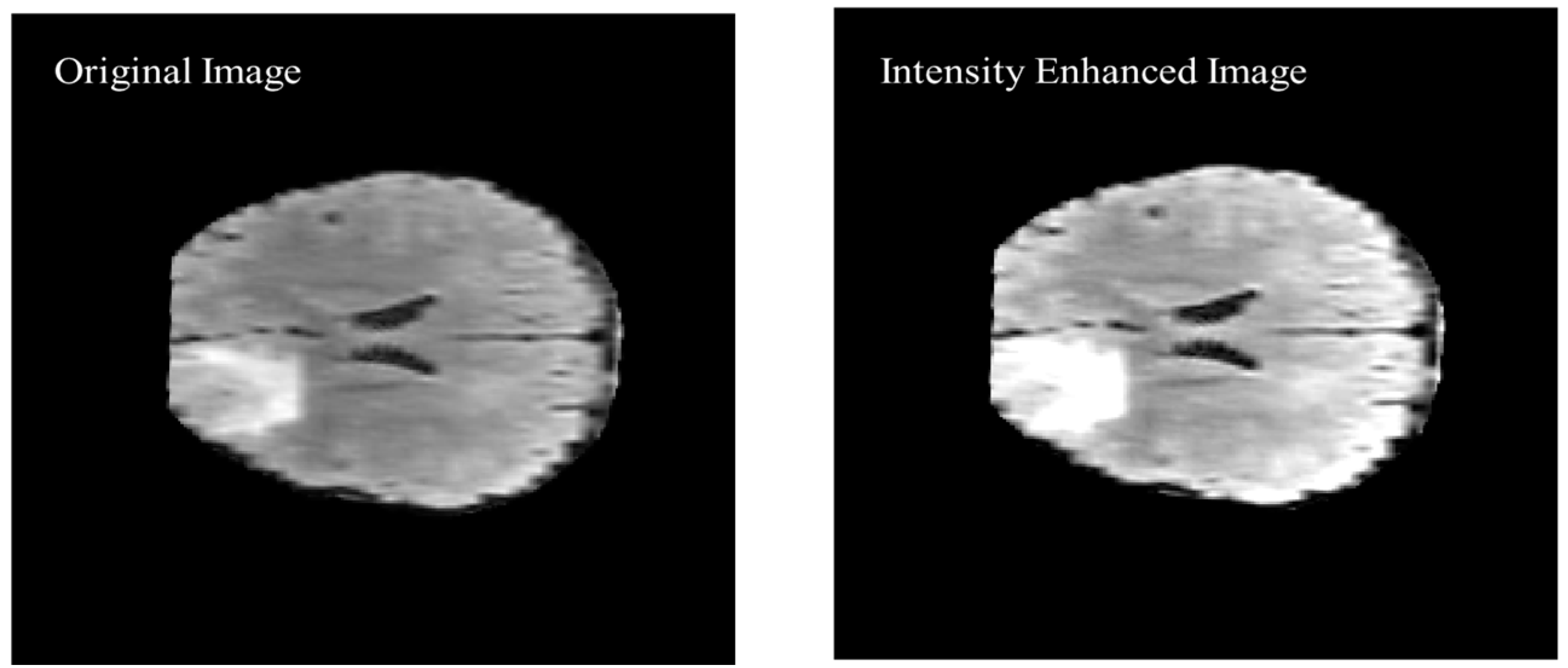
Figure 11 shows the black and white (BW) binary image generated based on the neighboring FCM threshold applied to intensity-enhanced MR image.
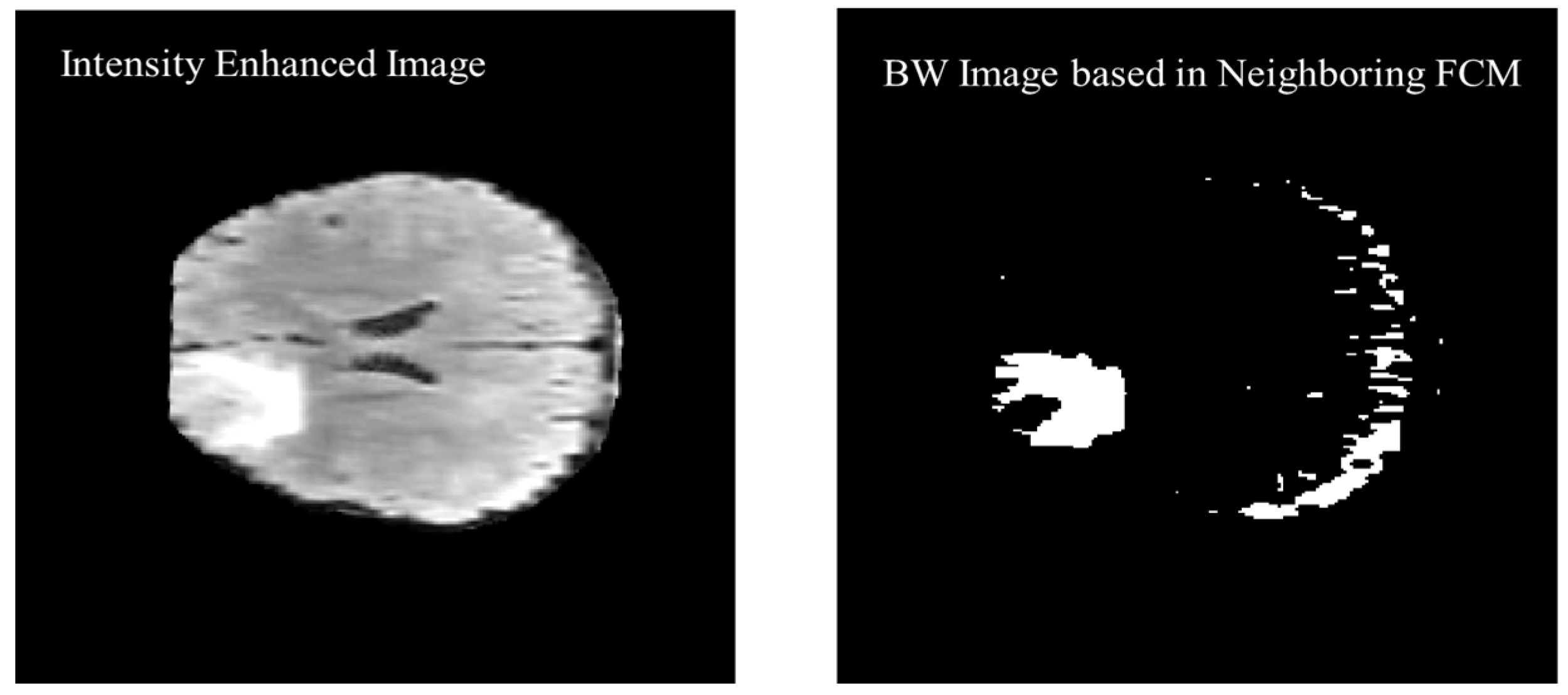
Morphological operations are applied for further enhancement of the tumor region in the binary image. Small regions in the binary are removed based on the connected pixel count values of less than 256 from the
MR image having total 57,600 pixels. Erosion and dilation morphological operations with a structure size of
pixels are applied to fill the small gaps in the binary image.
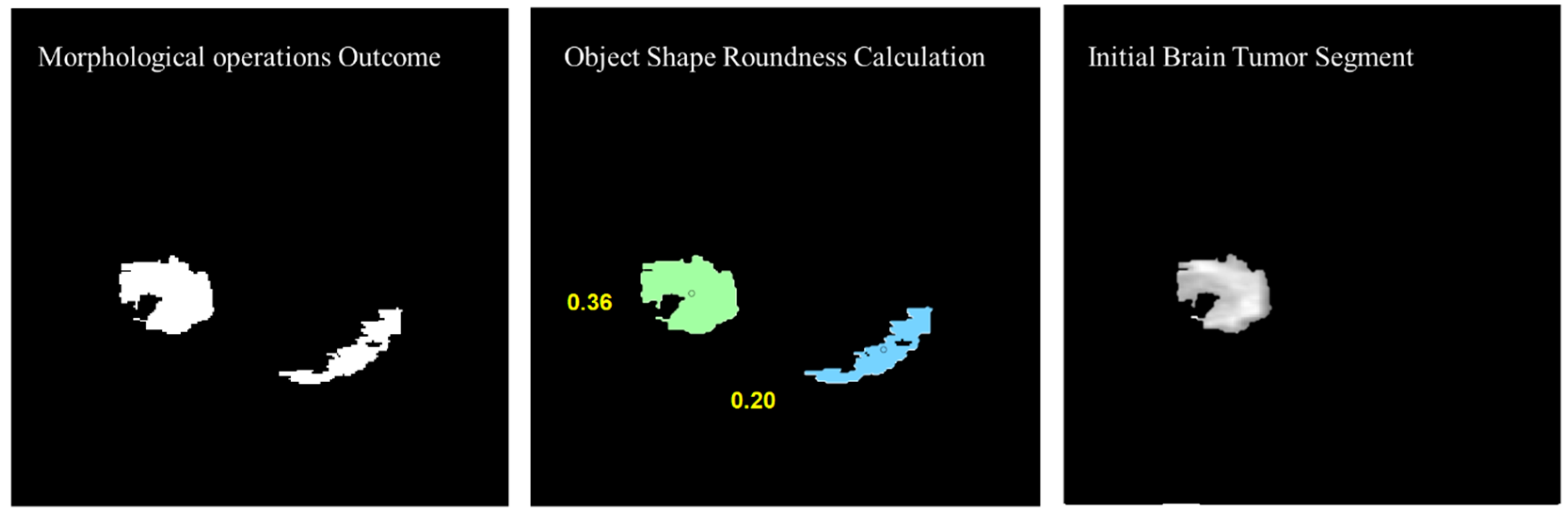
Figure 12 shows the visual results after removing the small regions from the binary image and applying the morphological operations (erosion and dilation).
To remove the non-tumor parts from the binary image, the number of objects was calculated in the binary image and the tumor region was selected based on the shape roundness properties of the objects. In
Figure 13, objects’ roundness properties are measured from the binary image and the roundness values for each object are displayed. The initial brain tumor segment is extracted based on the best roundness value.
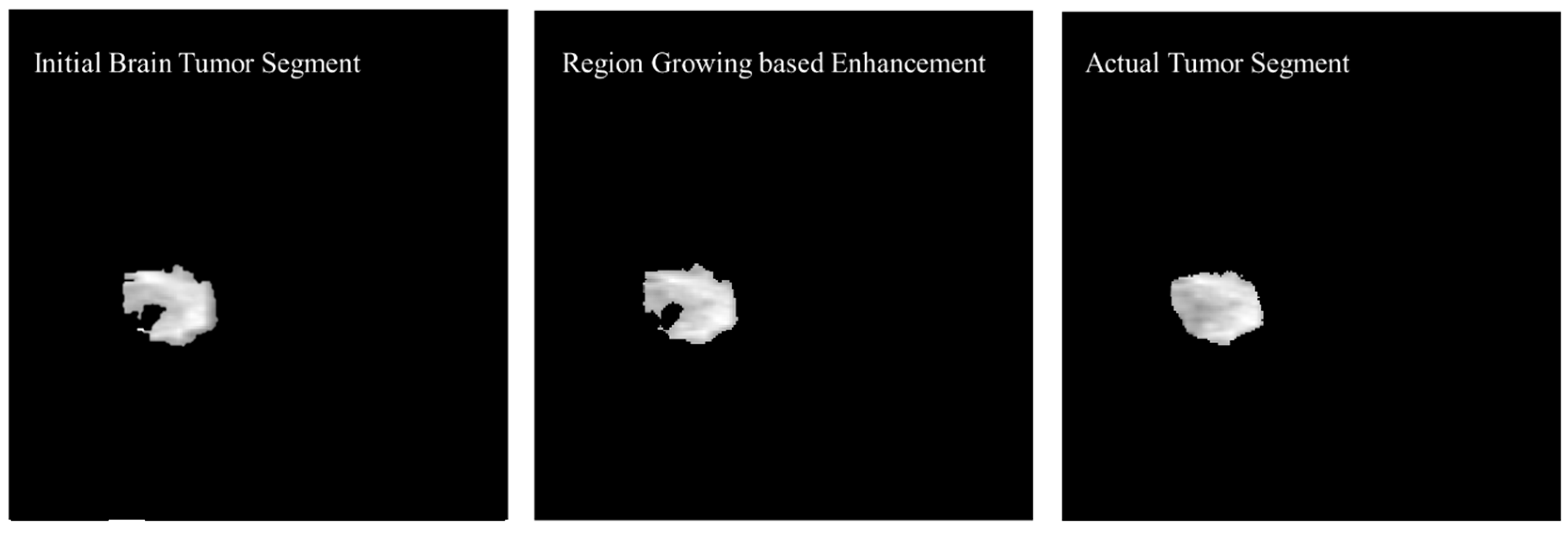
The initial tumor segment is enhanced using the region growing method. The first step in the process of edge segmentation based on the region-growing technique is to find the seed pixels which is selected based on the Neighboring FCM based initial segmentation. In the first step, a geometric structure from a gray level image was secured then centers of adjacent labeled edges were given as initial input to the algorithm.
Figure 14 shows the enhancement in the initial brain tumor segment by applying region growing method and a visual comparison was made with the actual tumor segment.
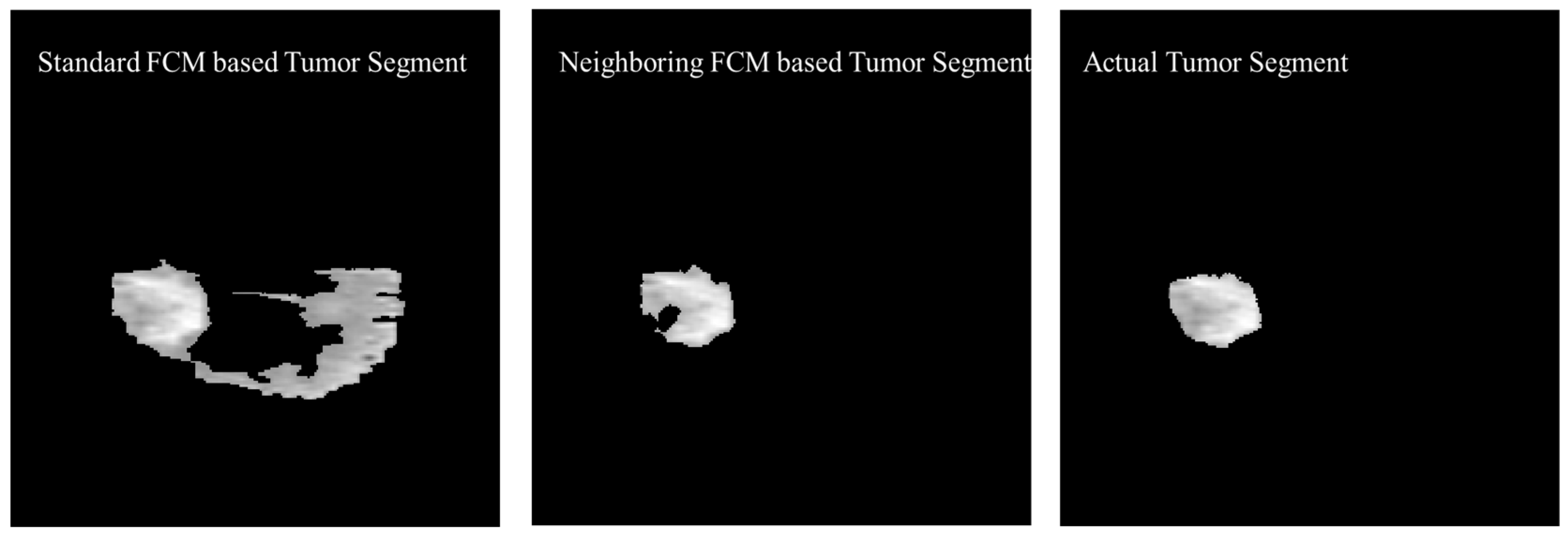
The experimental results were also generated based on the standard FCM to compare with the proposed neighboring FCM based tumor segmentation method.
Figure 15 shows the visual comparison of the standard FCM based tumor segment with the neighboring FCM based tumor segment and the actual tumor segment.
Better effectiveness of neighboring FCM can be observed through statistical analysis. Prominent improvement of 14.3% and 16.37% was secured with respect to Accuracy and DSC, respectively and other parameters as well. In the proposed neighboring FCM technique, the labeling of the images is going to be influenced by immediate neighbors only, so it gives better results as compared to standard FCM. The proposed method has outperformed in terms of average DSC, specificity, and sensitivity with values 90.87%, 99.86% and 95.52% as compared to the standard FCM average DSC, specificity, and sensitivity with values 66.86%, 87.22% and 81.29%, respectively.
Table 11 shows a comparison between the proposed segmentation technique with techniques proposed in recent literature. Dice Similarity Coefficient (DSC) is used for comparison purposes as it is the common metric adopted in recent literature. Results indicate that the proposed segmentation technique achieved an average DSC of 90.87% which outperforms all the methods listed in
Table 11.
The reason for this improvement was mainly because of extra neighboring information incorporated along with the original image and in the final stage region growing algorithm was used to secure a more accurate segmented image. FCM parameter selection is highly sensitive to noise and computational time will increase rapidly with non-homogeneous pixel intensities. The modification in original FCM function is made to tackle the non-homogeneous intensities of the pixels. In the proposed method, each image is influenced by immediate neighbors. This phenomenon creates a regularized effect and influence on labeling with respect to neighbors, which will secure a more homogeneous biased solution.
3.3. Glioma Tumor Classification Results
Although Model 2 was proposed for binary classification of MR image into tumorous and nontumorous it still performed better than LeNet, AlexNet and GoogleNet for multiclass Glioma tumor classification as shown in
Table 12 and
Table 13 but the Model 3 further improved the performance by reducing the convolutional filter size and number of parameters. The CNN architecture models were proposed namely; model 2 which is same model proposed and explained in
Section 3.3 (
Table 6) and model 3 which is optimized model architecture described in
Table 7. As shown in
Table 12 and
Table 13, model 2 achieved highest average accuracy 95.94% and 96.30% for HGG and LGG, respectively using Flair images. The combination of proposed enhanced model 3 and Batch size 200, epochs 8 reduced the overfitting and improved the classification accuracies as compared to other well-known CNN architectures; LeNet, AlexNet, and GoogleNet. It also outperformed model 2 proposed in this study.
In the proposed enhanced CNN model 3 was used as classifier and parameters such as batch size and epoch were further tuned based on accuracy results. The results of the proposed model 3 were compared with the existing CNN models (LeNet, AlexNet and GoogleNet) and model 2. For HGG Glioma, model 3 with batch size of 200 and 8 epoch achieved the highest average accuracy of 95.94% for enhanced model 3 with Flair MR images. The average accuracies showed improvement as shown in
Table 12 and
Table 13. For LGG Glioma classification, the batch size of 200 and 8 epoch secured the highest average accuracy for model 3 of 96.30% accuracy for Flair MR images.
The AlexNet experiments show promising results with an average accuracy of 92.31% and 93.14% for HGG and LGG, respectively as compared to LeNet and GoogleNet but still model 3 performance is far better than AlexNet, LeNet and GoogleNet. The famous CNN models (LeNet, AlexNet, and GoogleNet) do not perform well for brain tumor classification because of the complex architectures with high number of layers and parameters designed for very large number of output classes (1000 classes) with RGB input images. For example, AlexNet has 64 filters in the first convolutional layer which are mostly encoded with color information. In a deep learning model, if the number of parameters is higher than the training data set as observed for the case of LeNet, AlexNet and GoogleNet. In this case, regularization becomes a more critical step. The approximation of temporary functions of the input data in the design of CNN architecture plays an important role. This approximation is connected with the selection of parameters of the network like depth and width. In the process of regularization, overfitting of the algorithm is avoided especially when the complexity of the model increases. Hence, from the statistical analysis presented in
Table 12 and
Table 13, it can be concluded that if CNN model 3 is used as a classifier then the best classification accuracy is achieved for all the classes and Glioma types with a batch size of 200 and 8 epochs.
As shown in
Table 14, the proposed technique using CNN as a classifier achieved an accuracy of 96.30% for multiclass classification. When compared with other recent techniques from literature, it is evident that the proposed technique outperformed those listed in
Table 14. This also outperformed the other methods that were published recently using the same dataset.


















{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}