
Cardiac Reverse Remodelling by 2D and 3D Echocardiography in Heart Failure Patients Treated with Sacubitril/Valsartan

 ,
,  , ,
, , 
Abstract
:1. Introduction
2. Materials and Methods
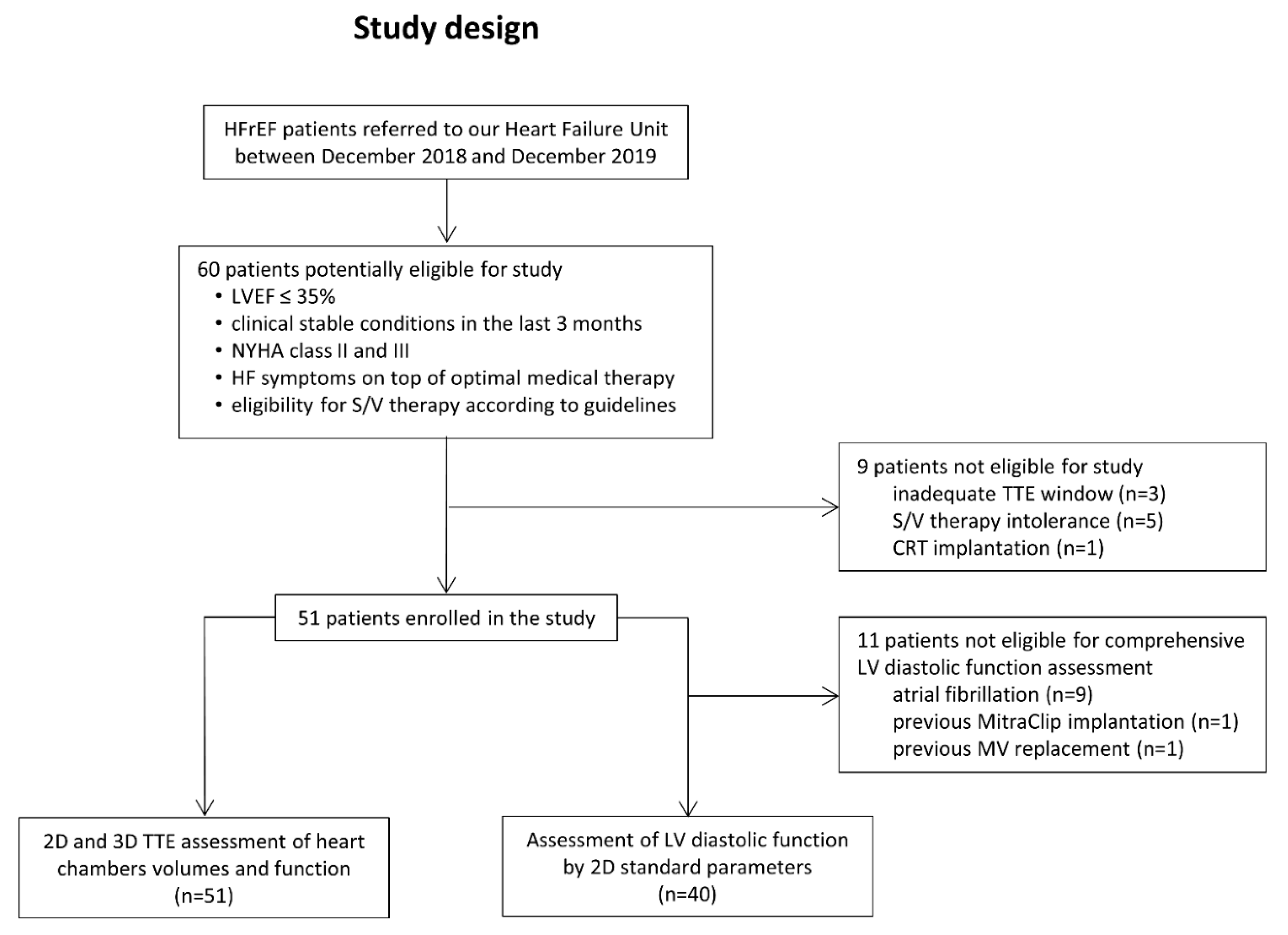
2.1. Patient Population and Study Design
2.2. Echocardiographic Examination
2.3. Statistical Analysis
3. Results
3.1. Baseline Characteristics of Study Population
3.2. Clinical and Echocardiographic Data
3.3. Follow-Up
4. Discussion
5. Conclusions
Study Limitations
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Januzzi, J.L.; Butler, J.; Fombu, E.; Maisel, A.; McCague, K.; Pina, I.L.; Prescott, M.F.; Riebman, J.B.; Solomon, S. Rationale and methods of the Prospective Study of Biomarkers, Symptom Improvement, and Ventricular Remodeling During Sacubitril/Valsartan Therapy for Heart Failure (PROVE-HF). Am. Heart J. 2018, 199, 130–136. [Google Scholar] [CrossRef]
- McMurray, J.J.; Packer, M.; Desai, A.S.; Gong, J.; Lefkowitz, M.P.; Rizkala, A.R.; Rouleau, J.; Shi, V.C.; Solomon, S.D.; Swedberg, K.; et al. Dual angiotensin receptor and neprilysin inhibition as an alternative to angiotensin-converting enzyme inhibition in patients with chronic systolic heart failure: Rationale for and design of the Prospective comparison of ARNI with ACEI to Determine Impact on Global Mortality and morbidity in Heart Failure trial (PARADIGM-HF). Eur. J. Heart Fail. 2013, 15, 1062–1073. [Google Scholar] [CrossRef] [Green Version]
- Januzzi, J.L., Jr.; Prescott, M.F.; Butler, J.; Felker, G.M.; Maisel, A.S.; McCague, K.; Camacho, A.; Pina, I.L.; Rocha, R.A.; Shah, A.M.; et al. Association of Change in N-Terminal Pro-B-Type Natriuretic Peptide Following Initiation of Sacubitril-Valsartan Treatment with Cardiac Structure and Function in Patients with Heart Failure with Reduced Ejection Fraction. JAMA 2019, 322, 1085–1095. [Google Scholar] [CrossRef]
- Wang, Y.; Zhou, R.; Lu, C.; Chen, Q.; Xu, T.; Li, D. Effects of the Angiotensin-Receptor Neprilysin Inhibitor on Cardiac Reverse Remodeling: Meta-Analysis. J. Am. Heart Assoc. 2019, 8, e012272. [Google Scholar] [CrossRef] [Green Version]
- Castrichini, M.; Manca, P.; Nuzzi, V.; Barbati, G.; De Luca, A.; Korcova, R.; Stolfo, D.; Lenarda, A.D.; Merlo, M.; Sinagra, G. Sacubitril/Valsartan Induces Global Cardiac Reverse Remodeling in Long-Lasting Heart Failure with Reduced Ejection Fraction: Standard and Advanced Echocardiographic Evidences. J. Clin. Med. 2020, 9, 906. [Google Scholar] [CrossRef] [Green Version]
- Landolfo, M.; Piani, F.; Esposti, D.D.; Cosentino, E.; Bacchelli, S.; Dormi, A.; Borghi, C. Effects of sacubitril valsartan on clinical and echocardiographic parameters of outpatients with heart failure and reduced ejection fraction. Int. J. Cardiol. Heart Vasc. 2020, 31, 100656. [Google Scholar] [CrossRef]
- Moon, M.G.; Hwang, I.C.; Choi, W.; Cho, G.Y.; Yoon, Y.E.; Park, J.B.; Lee, S.P.; Kim, H.K.; Kim, Y.J. Reverse remodelling by sacubitril/valsartan predicts the prognosis in heart failure with reduced ejection fraction. ESC Heart Fail. 2021, 8, 2058–2069. [Google Scholar] [CrossRef] [PubMed]
- Khan, Z.; Gholkar, G.; Tolia, S.; Kado, H.; Zughaib, M. Effect of sacubitril/valsartan on cardiac filling pressures in patients with left ventricular systolic dysfunction. Int. J. Cardiol. 2018, 271, 169–173. [Google Scholar] [CrossRef] [PubMed]
- Correale, M.; Mallardi, A.; Mazzeo, P.; Tricarico, L.; Diella, C.; Romano, V.; Ferraretti, A.; Leopizzi, A.; Merolla, G.; Di Biase, M.; et al. Sacubitril/valsartan improves right ventricular function in a real-life population of patients with chronic heart failure: The Daunia Heart Failure Registry. Int. J. Cardiol. Heart Vasc. 2020, 27, 100486. [Google Scholar] [CrossRef] [PubMed]
- McMurray, J.J.; Packer, M.; Desai, A.S.; Gong, J.; Lefkowitz, M.P.; Rizkala, A.R.; Rouleau, J.L.; Shi, V.C.; Solomon, S.D.; Swedberg, K.; et al. Angiotensin-neprilysin inhibition versus enalapril in heart failure. N. Engl. J. Med. 2014, 371, 993–1004. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mogensen, U.M.; Gong, J.; Jhund, P.S.; Shen, L.; Kober, L.; Desai, A.S.; Lefkowitz, M.P.; Packer, M.; Rouleau, J.L.; Solomon, S.D.; et al. Effect of sacubitril/valsartan on recurrent events in the Prospective comparison of ARNI with ACEI to Determine Impact on Global Mortality and morbidity in Heart Failure trial (PARADIGM-HF). Eur. J. Heart Fail. 2018, 20, 760–768. [Google Scholar] [CrossRef] [PubMed]
- Packer, M.; McMurray, J.J.; Desai, A.S.; Gong, J.; Lefkowitz, M.P.; Rizkala, A.R.; Rouleau, J.L.; Shi, V.C.; Solomon, S.D.; Swedberg, K.; et al. Angiotensin receptor neprilysin inhibition compared with enalapril on the risk of clinical progression in surviving patients with heart failure. Circulation 2015, 131, 54–61. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pina, I.L.; Camacho, A.; Ibrahim, N.E.; Felker, G.M.; Butler, J.; Maisel, A.S.; Prescott, M.F.; Williamson, K.M.; Claggett, B.L.; Desai, A.S.; et al. Improvement of Health Status Following Initiation of Sacubitril/Valsartan in Heart Failure and Reduced Ejection Fraction. JACC Heart Fail. 2021, 9, 42–51. [Google Scholar] [CrossRef] [PubMed]
- Weiner, R.B.; Baggish, A.L.; Chen-Tournoux, A.; Marshall, J.E.; Gaggin, H.K.; Bhardwaj, A.; Mohammed, A.A.; Rehman, S.U.; Barajas, L.; Barajas, J.; et al. Improvement in structural and functional echocardiographic parameters during chronic heart failure therapy guided by natriuretic peptides: Mechanistic insights from the ProBNP Outpatient Tailored Chronic Heart Failure (PROTECT) study. Eur. J. Heart Fail. 2013, 15, 342–351. [Google Scholar] [CrossRef] [PubMed]
- Ponikowski, P.; Voors, A.A.; Anker, S.D.; Bueno, H.; Cleland, J.G.F.; Coats, A.J.S.; Falk, V.; Gonzalez-Juanatey, J.R.; Harjola, V.P.; Jankowska, E.A.; et al. 2016 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure: The Task Force for the diagnosis and treatment of acute and chronic heart failure of the European Society of Cardiology (ESC)Developed with the special contribution of the Heart Failure Association (HFA) of the ESC. Eur. Heart J. 2016, 37, 2129–2200. [Google Scholar] [CrossRef] [PubMed]
- Lang, R.M.; Badano, L.P.; Mor-Avi, V.; Afilalo, J.; Armstrong, A.; Ernande, L.; Flachskampf, F.A.; Foster, E.; Goldstein, S.A.; Kuznetsova, T.; et al. Recommendations for cardiac chamber quantification by echocardiography in adults: An update from the American Society of Echocardiography and the European Association of Cardiovascular Imaging. J. Am. Soc. Echocardiogr. 2015, 28, 1–39 e14. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pepi, M.; Tamborini, G.; Galli, C.; Barbier, P.; Doria, E.; Berti, M.; Guazzi, M.; Fiorentini, C. A new formula for echo-Doppler estimation of right ventricular systolic pressure. J. Am. Soc. Echocardiogr. 1994, 7, 20–26. [Google Scholar] [CrossRef]
- Baumgartner, H.; Falk, V.; Bax, J.J.; De Bonis, M.; Hamm, C.; Holm, P.J.; Iung, B.; Lancellotti, P.; Lansac, E.; Rodriguez Munoz, D.; et al. 2017 ESC/EACTS Guidelines for the management of valvular heart disease. Eur. Heart J. 2017, 38, 2739–2791. [Google Scholar] [CrossRef] [PubMed]
- Nagueh, S.F.; Smiseth, O.A.; Appleton, C.P.; Byrd, B.F., 3rd; Dokainish, H.; Edvardsen, T.; Flachskampf, F.A.; Gillebert, T.C.; Klein, A.L.; Lancellotti, P.; et al. Recommendations for the Evaluation of Left Ventricular Diastolic Function by Echocardiography: An Update from the American Society of Echocardiography and the European Association of Cardiovascular Imaging. J. Am. Soc. Echocardiogr. 2016, 29, 277–314. [Google Scholar] [CrossRef] [Green Version]
- Narang, A.; Mor-Avi, V.; Prado, A.; Volpato, V.; Prater, D.; Tamborini, G.; Fusini, L.; Pepi, M.; Goyal, N.; Addetia, K.; et al. Machine learning based automated dynamic quantification of left heart chamber volumes. Eur. Heart J. Cardiovasc. Imaging 2019, 20, 541–549. [Google Scholar] [CrossRef]
- Volpato, V.; Mor-Avi, V.; Narang, A.; Prater, D.; Goncalves, A.; Tamborini, G.; Fusini, L.; Pepi, M.; Patel, A.R.; Lang, R.M. Automated, machine learning-based, 3D echocardiographic quantification of left ventricular mass. Echocardiography 2019, 36, 312–319. [Google Scholar] [CrossRef]
- Muraru, D.; Spadotto, V.; Cecchetto, A.; Romeo, G.; Aruta, P.; Ermacora, D.; Jenei, C.; Cucchini, U.; Iliceto, S.; Badano, L.P. New speckle-tracking algorithm for right ventricular volume analysis from three-dimensional echocardiographic data sets: Validation with cardiac magnetic resonance and comparison with the previous analysis tool. Eur. Heart J. Cardiovasc. Imaging 2016, 17, 1279–1289. [Google Scholar] [CrossRef]
- Martens, P.; Belien, H.; Dupont, M.; Vandervoort, P.; Mullens, W. The reverse remodeling response to sacubitril/valsartan therapy in heart failure with reduced ejection fraction. Cardiovasc. Ther. 2018, 36, e12435. [Google Scholar] [CrossRef] [Green Version]
- Tamborini, G.; Muratori, M.; Brusoni, D.; Celeste, F.; Maffessanti, F.; Caiani, E.G.; Alamanni, F.; Pepi, M. Is right ventricular systolic function reduced after cardiac surgery? A two- and three-dimensional echocardiographic study. Eur. J. Echocardiogr. 2009, 10, 630–634. [Google Scholar] [CrossRef] [Green Version]
- Von Lueder, T.G.; Wang, B.H.; Kompa, A.R.; Huang, L.; Webb, R.; Jordaan, P.; Atar, D.; Krum, H. Angiotensin receptor neprilysin inhibitor LCZ696 attenuates cardiac remodeling and dysfunction after myocardial infarction by reducing cardiac fibrosis and hypertrophy. Circ. Heart Fail. 2015, 8, 71–78. [Google Scholar] [CrossRef] [Green Version]
- McMurray, J.J. Neprilysin inhibition to treat heart failure: A tale of science, serendipity, and second chances. Eur. J. Heart Fail. 2015, 17, 242–247. [Google Scholar] [CrossRef] [PubMed]
- Mor-Avi, V.; Lang, R.M. The use of real-time three-dimensional echocardiography for the quantification of left ventricular volumes and function. Curr. Opin. Cardiol. 2009, 24, 402–409. [Google Scholar] [CrossRef]
- Italiano, G.; Fusini, L.; Mantegazza, V.; Tamborini, G.; Muratori, M.; Ghulam Ali, S.; Penso, M.; Garlasche, A.; Gripari, P.; Pepi, M. Novelties in 3D Transthoracic Echocardiography. J. Clin. Med. 2021, 10, 408. [Google Scholar] [CrossRef]
- Almufleh, A.; Marbach, J.; Chih, S.; Stadnick, E.; Davies, R.; Liu, P.; Mielniczuk, L. Ejection fraction improvement and reverse remodeling achieved with Sacubitril/Valsartan in heart failure with reduced ejection fraction patients. Am. J. Cardiovasc. Dis. 2017, 7, 108–113. [Google Scholar] [PubMed]
- Guerra, F.; Ammendola, E.; Ziacchi, M.; Aspromonte, V.; Pellegrino, P.L.; Del Giorno, G.; Dell’Era, G.; Pimpini, L.; Santoro, F.; Floris, R.; et al. Effect of SAcubitril/Valsartan on left vEntricular ejection fraction and on the potential indication for Implantable Cardioverter Defibrillator in primary prevention: The SAVE-ICD study. Eur. J. Clin. Pharmacol. 2021, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Tamborini, G.; Marsan, N.A.; Gripari, P.; Maffessanti, F.; Brusoni, D.; Muratori, M.; Caiani, E.G.; Fiorentini, C.; Pepi, M. Reference values for right ventricular volumes and ejection fraction with real-time three-dimensional echocardiography: Evaluation in a large series of normal subjects. J. Am. Soc. Echocardiogr. 2010, 23, 109–115. [Google Scholar] [CrossRef] [PubMed]
- Cameli, M.; Loiacono, F.; Sparla, S.; Solari, M.; Iardino, E.; Mandoli, G.E.; Bernazzali, S.; Maccherini, M.; Mondillo, S. Systematic Left Ventricular Assist Device Implant Eligibility with Non-Invasive Assessment: The SIENA Protocol. J. Cardiovasc. Ultrasound 2017, 25, 39–46. [Google Scholar] [CrossRef] [PubMed]
- Amsallem, M.; Mercier, O.; Kobayashi, Y.; Moneghetti, K.; Haddad, F. Forgotten No More: A Focused Update on the Right Ventricle in Cardiovascular Disease. JACC Heart Fail. 2018, 6, 891–903. [Google Scholar] [CrossRef] [PubMed]
- Mottram, P.M.; Marwick, T.H. Assessment of diastolic function: What the general cardiologist needs to know. Heart 2005, 91, 681–695. [Google Scholar] [CrossRef] [Green Version]
- Solomon, S.D.; Zile, M.; Pieske, B.; Voors, A.; Shah, A.; Kraigher-Krainer, E.; Shi, V.; Bransford, T.; Takeuchi, M.; Gong, J.; et al. The angiotensin receptor neprilysin inhibitor LCZ696 in heart failure with preserved ejection fraction: A phase 2 double-blind randomised controlled trial. Lancet 2012, 380, 1387–1395. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
| Overall Population (n = 51) | IHD (n = 24) | Non-IHD (n = 27) | p Value | |
|---|---|---|---|---|
| Age (y) | 65 ± 10 | 66 ± 9 | 64 ± 10 | NS |
| Male (n, %) | 43 (84.3) | 21 (87.5) | 22 (81.5) | NS |
| BMI (kg/m2) | 26.2 ± 4.2 | 26.3 ± 3.7 | 26.0 ± 4.6 | NS |
| Hypertension (n, %) | 32 (62.7) | 13 (54.2) | 19 (70.4) | NS |
| Dyslipidaemia (n, %) | 32 (62.7) | 18 (75.0) | 14 (51.9) | NS |
| COPD (n, %) | 2 (3.9) | 1 (4.2) | 1 (3.7) | NS |
| Smoking history (n, %) | 35 (68.6) | 21 (87.5) | 14 (51.9) | 0.008 |
| CKD Stage (n, %) | NS | |||
| I | 14 (27.5) | 4 (16.6) | 10 (37.0) | |
| II | 16 (31.4) | 10 (41.7) | 6 (22.2) | |
| III | 21 (41.2) | 10 (41.7) | 11 (40.7) | |
| Hyperuricemia (n, %) | 10 (19.6) | 4 (16.6) | 6 (22.2) | NS |
| Diabetes mellitus (n, %) | 9 (17.6) | 5 (20.8) | 4 (14.8) | NS |
| Previous cardiac surgery (n, %) | 7 (13.7) | 6 (25.0) | 1 (3.7) | 0.042 |
| Previous PCI (n, %) | 22 (43.1) | 21 (87.5) | 1 (3.7) | <0.001 |
| Previous MitraClip procedure | 1 (2.0) | 1 (4.2) | 0 | NS |
| History of atrial fibrillation (n, %) | 14 (27.4) | 4 (16.6) | 10 (37.0) | NS |
| LBBB (n, %) | 14 (27.5) | 2 (8.3) | 12 (44.4) | 0.005 |
| Device therapy (n, %) | ||||
| ICD | 14 (27.5) | 11 (45.8) | 3 (11.1) | 0.011 |
| CRT-P | 1 (2.0) | 0 | 1 (3.7) | NS |
| CRT-D | 10 (19.6) | 4 (16.6) | 6 (22.2) | NS |
| CCB (n, %) | 1 (2.0) | 0 | 1 (3.7) | NS |
| α Blockers (n, %) | 1 (2.0) | 0 | 1 (3.7) | NS |
| Ivabradin (n, %) | 7 (13.7) | 4 (16.6) | 3 (11.1) | NS |
| Digoxin (n, %) | 6 (11.8) | 3 (12.5) | 3 (11.1) | NS |
| β Blockers (n, %) | 51 (100.0) | 24 (100.0) | 27 (100.0) | NA |
| ACEi (n, %) | 36 (70.6) | 16 (66.7) | 21 (77.8) | NS |
| ARB (n, %) | 13 (25.5) | 8 (33.3) | 6 (22.2) | NS |
| MRA (n, %) | 39 (76.5) | 17 (70.8) | 22 (81.5) | NS |
| Nitrates (n, %) | 1 (2.0) | 1 (4.2) | 0 | NS |
| Loop diuretic (n, %) | 42 (82.4) | 20 (83.3) | 22 (81.5) | NS |
| Thiazide (n, %) | 2 (3.9) | 1 (4.2) | 1 (3.7) | NS |
| Antiplatelet (n, %) | 36 (70.6) | 23 (95.8) | 13 (48.1) | <0.001 |
| OAC (n, %) | 19 (37.3) | 12 (50.0) | 7 (25.9) | NS |
| Baseline | 6MFU | |||||
|---|---|---|---|---|---|---|
| All (n = 51) | IHD (n = 24) | Non-IHD (n = 27) | All (n = 51) | IHD (n = 24) | Non-IHD (n = 27) | |
| Clinical Variables | ||||||
| NTproBNP (pg/mL) | 1225 [661–2896] | 1111 [404–2239] | 1543 [761–4288] | 915 * [370–1812] | 869 * [377–1492] | 941 * [300–2845] |
| SBP (mmHg) | 119 ± 17 | 118 ± 21 | 120 ± 14 | 107 ± 14 * | 106 ± 13 * | 107 ± 14 * |
| HR (bpm) | 67 ± 10 | 63 ± 8 | 71 ± 10 † | 65 ± 10 | 63 ± 10 | 67 ± 10 |
| NYHA Class | ||||||
| II | 40 (78.4) | 19 (79.2) | 21 (77.8) | 47 (92.2) * | 22 (91.7) | 25 (92.6) * |
| III | 11 (21.6) | 5 (20.8) | 6 (22.2) | 4 (7.8) * | 2 (8.3) | 2 (7.4) * |
| 2DTTE Variables | ||||||
| LAVi (mL/m2) | 47.7 ± 14.6 | 46.9 ± 16.1 | 48.4 ± 13.3 | 44.4 ± 13.4 * | 44.2 ± 14.2 | 44.5 ± 12.9 * |
| LV EDVi (mL/m2) | 101.8 ± 28.6 | 102.6 ± 29.9 | 101.0 ± 28.0 | 92.1 ± 27.6 * | 97.9 ± 26.5 | 87.0 ± 28.0 * |
| LV ESVi (mL/m2) | 70.0 ± 23.0 | 71.1 ± 23.6 | 69.0 ± 22.9 | 59.5 ± 25.0 * | 66.0 ± 23.0 * | 53.8 ± 25.8 * |
| LV EF (%) | 31.9 ± 4.5 | 31.4 ± 5.1 | 32.3 ± 3.9 | 37.1 ± 8.9 * | 33.7 ± 7.2 | 40.1 ± 9.2 *,† |
| MR grade | ||||||
| <moderate | 40 (78.4) | 20 (83.3) | 20 (74.1) | 46 (90.2) * | 22 (91.7) | 24 (88.9) * |
| ≥moderate | 11 (21.6) | 4 (16.7) | 7 (25.9) | 5 (9.8) * | 2 (8.3) | 3 (11.1) * |
| TAPSE (mm) | 19.8 ± 4.2 | 18.5 ± 4.5 | 20.9 ± 3.7 † | 19.5 ± 4.6 | 18.0 ± 3.7 | 20.8 ± 5.0 † |
| RVD1 (mm) | 42.2 ± 7.8 | 41.2 ± 5.6 | 43.0 ± 9.3 | 40.4 ± 8.3 * | 39.8 ± 7.1 | 41 ± 9.4 |
| RVD2 (mm) | 30.9 ± 7.4 | 29.6 ± 5.6 | 32.1 ± 8.7 | 29.6 ± 6.7 | 28.1 ± 5.9 | 30.8 ± 7.7 |
| RVD3 (mm) | 78.5 ± 11.3 | 76.5 ± 12.5 | 80.3 ± 10.2 | 79.3 ± 9.2 | 77.5 ± 7.2 | 81.0 ± 10.6 |
| RV EDAi (cm2/m2) | 12.0 ± 3.8 | 11.3 ± 2.5 | 12.7 ± 4.6 | 11.7 ± 3.4 | 10.7 ± 2.2 | 12.5 ± 4.2 |
| RV ESAi (cm2/m2) | 7.4 ± 2.7 | 7.0 ± 2.5 | 7.8 ± 3.3 | 6.7 ± 2.6 * | 6.3 ± 1.9 * | 7.1 ± 3.0 |
| RV FAC (%) | 39.3 ± 9.5 | 38.9 ± 9.9 | 39.7 ± 9.3 | 43.0 ± 9.1 * | 42.2 ± 8.7 | 43.8 ± 9.5 * |
| TR grade | ||||||
| <moderate | 43 (84.3) | 23 (95.8) | 20 (74.1) | 46 (90.2) | 23 (95.8) | 23 (85.2) |
| ≥moderate | 8 (15.7) | 1 (4.2) | 7 (25.9) | 5 (9.8) | 1 (4.2) | 4 (14.8) |
| SPAP (mmHg) | 38.1 ± 12.4 | 39.9 ± 13.3 | 36.8 ± 11.9 | 34.6 ± 10.1 | 34.9 ± 10.3 | 34.4 ± 10.2 |
| 3DTTE Variables | ||||||
| LAVi max (mL/m2) | 43.9 ± 13.7 | 42.0 ± 12.4 | 45.5 ± 14.8 | 40.7 ± 15.7 * | 40.5 ± 14.5 | 40.8 ± 16.8 * |
| LV EDVi (mL/m2) | 122.8 ± 29.4 | 120.8 ± 27.3 | 124.5 ± 31.6 | 107.0 ± 29.4 * | 111.7 ± 29.3 * | 103.0 ± 29.5 * |
| LV ESVi (mL/m2) | 84.3 ± 24.9 | 82.4 ± 22.7 | 86.0 ± 27.0 | 68.2 ± 26.7 * | 73.9 ± 25.3 * | 63.3 ± 27.3 * |
| LV EF (%) | 32.0 ± 5.0 | 32.4 ± 5.0 | 31.7 ± 5.1 | 37.8 ± 8.3 * | 34.8 ± 5.6 * | 40.3 ± 9.3 *,† |
| LV GLS (%) | −10.0 ± 2.8 | −9.3 ± 2.6 | −10.6 ± 2.8 | −12.2 ± 4.4 * | −10.1 ± 3.6 | −14.3 ± 4.1 *,† |
| LV Mass (g/m2) | 81.1 ± 17.5 | 80.2 ± 14.0 | 81.9 ± 20.3 | 72.2 ± 16.0 * | 72.8 ± 13.0 * | 71.6 ± 18.4 * |
| RV EDVi (mL/m2) | 67.3 ± 24.2 | 62.8 ± 14.2 | 71.0 ± 29.8 | 60.1 ± 21.1 * | 57.0 ± 11.2 * | 62.6 ± 26.6 * |
| RV ESVi (mL/m2) | 37.4 ± 14.2 | 34.4 ± 8.8 | 39.9 ± 17.2 | 32.1 ± 12.6 * | 31.6 ± 9.2 * | 32.6 ± 15.0 * |
| RV EF (%) | 44.7 ± 7.8 | 45.1 ± 8.3 | 44.3 ± 7.5 | 47.1 ± 7.1 * | 45.4 ± 7.5 | 48.4 ± 6.5 * |
| RV FW strain (%) | −22.0 ± 6.3 | −24.0 ± 7.3 | −20.5 ± 4.8 † | −25.8 ± 7.1 * | −25.6 ± 7.0 | −26.0 ± 7.4 * |
| Baseline | 6MFU | |||||
|---|---|---|---|---|---|---|
| All (n = 40) | IHD (n = 20) | Non-IHD (n = 20) | All (n = 40) | IHD (n = 20) | Non-IHD (n = 20) | |
| E wave | 63 [46–79] | 64 [52–79] | 63 [42–87] | 54 [43–62] * | 49 [40–64] * | 57 [46–62] |
| A wave | 61 [35–82] | 66 [29–85] | 58 [45–82] | 75 [51–92] * | 72 [43–85] | 79 [59–98] * |
| E/A | 0.8 [0.6–2.4] | 0.8 [0.6–2.5] | 0.8 [0.6–2.2] | 0.6 [0.5–0.9] * | 0.7 [0.6–1.1] * | 0.6 [0.6–0.7] |
| E/e’ average | 11 [8–15]] | 12 [9–16] | 9 [6–15] | 10 [8–14] * | 9 [8–12] * | 10 [7–14] |
| Diastolic dysfunction (n, %) | ||||||
| Class I | 23 (57.5) | 11 (55.0) | 12 (60.0) | 34 (85.0) * | 16 (80.0) * | 18 (90.0) * |
| Class II | 4 (10.0) | 1 (5.0) | 3 (15.0) | 2 (5.0) * | 2 (10.0) * | 0 * |
| Class III | 13 (32.5) | 8 (40.0) | 5 (25.0) | 4 (10.0) * | 2 (10.0) * | 2 (10.0) * |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mantegazza, V.; Volpato, V.; Mapelli, M.; Sassi, V.; Salvioni, E.; Mattavelli, I.; Tamborini, G.; Agostoni, P.; Pepi, M. Cardiac Reverse Remodelling by 2D and 3D Echocardiography in Heart Failure Patients Treated with Sacubitril/Valsartan. Diagnostics 2021, 11, 1845. https://doi.org/10.3390/diagnostics11101845
Mantegazza V, Volpato V, Mapelli M, Sassi V, Salvioni E, Mattavelli I, Tamborini G, Agostoni P, Pepi M. Cardiac Reverse Remodelling by 2D and 3D Echocardiography in Heart Failure Patients Treated with Sacubitril/Valsartan. Diagnostics. 2021; 11(10):1845. https://doi.org/10.3390/diagnostics11101845
Chicago/Turabian StyleMantegazza, Valentina, Valentina Volpato, Massimo Mapelli, Valentina Sassi, Elisabetta Salvioni, Irene Mattavelli, Gloria Tamborini, Piergiuseppe Agostoni, and Mauro Pepi. 2021. "Cardiac Reverse Remodelling by 2D and 3D Echocardiography in Heart Failure Patients Treated with Sacubitril/Valsartan" Diagnostics 11, no. 10: 1845. https://doi.org/10.3390/diagnostics11101845
APA StyleMantegazza, V., Volpato, V., Mapelli, M., Sassi, V., Salvioni, E., Mattavelli, I., Tamborini, G., Agostoni, P., & Pepi, M. (2021). Cardiac Reverse Remodelling by 2D and 3D Echocardiography in Heart Failure Patients Treated with Sacubitril/Valsartan. Diagnostics, 11(10), 1845. https://doi.org/10.3390/diagnostics11101845