Elaboration of Screening Scales for Mental Development Problems Detection in Russian Preschool Children: Psychometric Approach



Abstract

1. Introduction
2. Materials and Methods
3. Results
3.1. A Preliminary Selection of Items and the Scales Formation
3.2. Verification of Factor Validity and Reliability of the Scales
3.3. Verification of the Discriminative Validity of the Scales
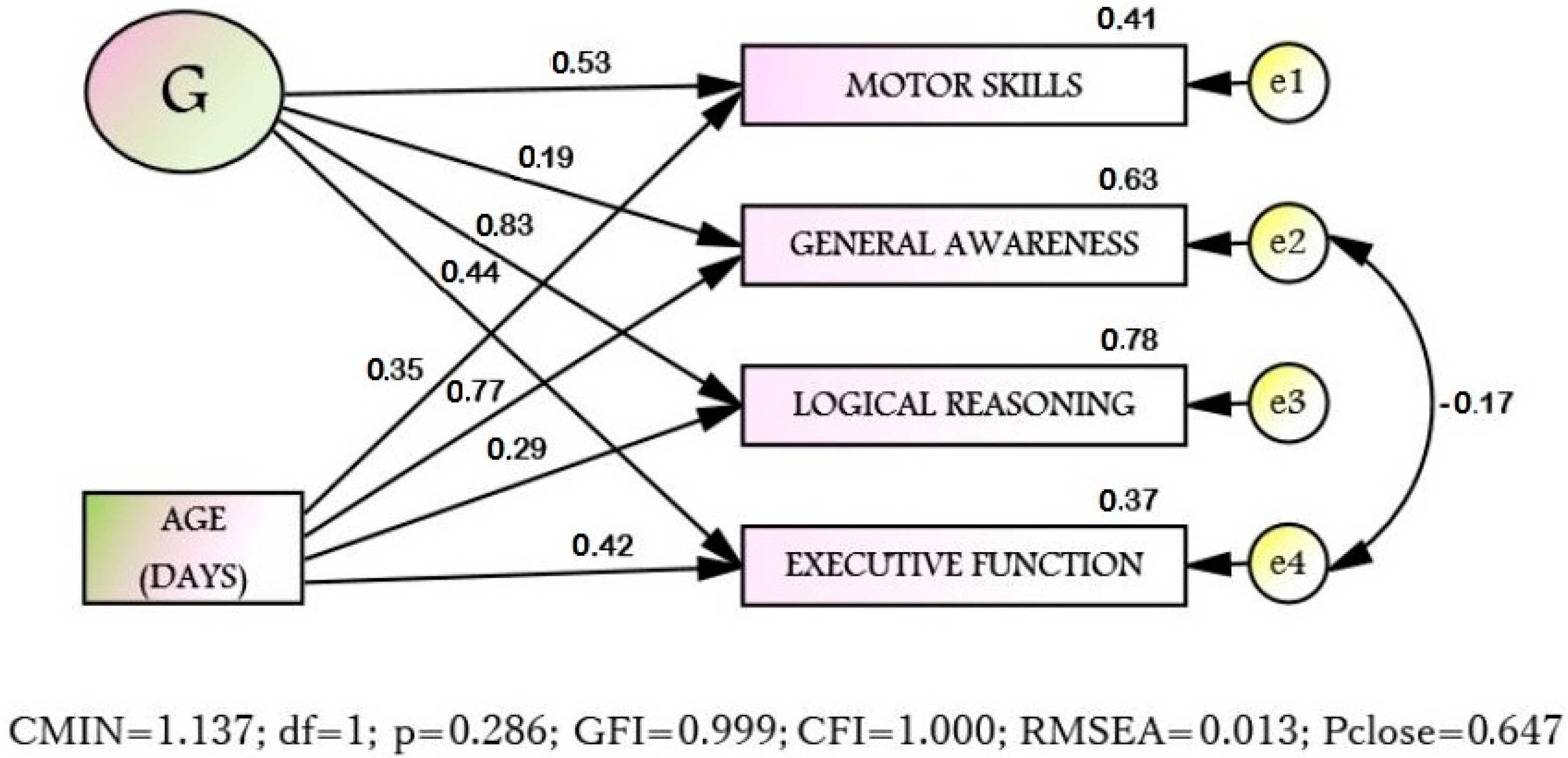
3.4. The Structure of Interconnections of the Scales with the Age
3.5. Scales Adjusting According to the Age
3.6. Test Norms Elaboration
4. Discussion
5. Conclusions
6. Limitations
Author Contributions
Funding
Conflicts of Interest
References
- Jeste, S.S. Neurodevelopmental behavioral and cognitive disorders. Contin. Lifelong Learn. Neurol. 2015, 21, 690–714. [Google Scholar] [CrossRef]
- Wiggins, L.D.; Levy, S.E.; Daniels, J.; Schieve, L.; Croen, L.A.; DiGuiseppi, C.; Blaskey, L.; Giarelli, E.; Lee, L.-C.; Pinto-Martin, J.; et al. Autism spectrum disorder symptoms among children enrolled in the Study to Explore Early Development (SEED). J. Autism Dev. Disord. 2015, 45, 3183–3194. [Google Scholar] [CrossRef] [PubMed]
- Crnic, K.; Hoffman, C.; Gaze, C.; Edelbrock, C. Understanding the emergence of behavior problems in young children with developmental delays. Infants Young Child. 2004, 17, 223–235. [Google Scholar] [CrossRef][Green Version]
- Feldman, M.A.; Hancock, C.L.; Rielly, N.; Minnes, P.; Cairns, C. Behavior problems in young children with or at risk for developmental delay. J. Child Fam. Stud. 2000, 9, 247–261. [Google Scholar] [CrossRef]
- Baker, B.L.; McIntyre, L.L.; Blacher, J.; Crnic, K.; Edelbrock, C.; Low, C. Pre-school children with and without developmental delay: Behaviour problems and parenting stress over time. J. Intellect. Disabil. Res. 2003, 47, 217–230. [Google Scholar] [CrossRef]
- Rice, C.E.; Rosanoff, M.; Dawson, G.; Durkin, M.S.; Croen, L.A.; Singer, A.; Yeargin-Allsopp, M. Evaluating changes in the prevalence of the Autism Spectrum Disorders (ASDs). Public Health Rev. 2012, 34, 1–22. [Google Scholar] [CrossRef]
- Howlin, P.; Moss, P.; Savage, S.; Rutter, M. Social outcomes in mid to later adulthood among individuals diagnosed with autism and average nonverbal IQ as children. J. Am. Acad. Child Adolesc. Psychiatry 2013, 52, 572–581.e1. [Google Scholar] [CrossRef]
- Henninger, N.A.; Taylor, J.L. Outcomes in adults with autism spectrum disorders: A historical perspective. Autism 2012, 17, 103–116. [Google Scholar] [CrossRef]
- Dawson, P.; Camp, B.W. Evaluating developmental screening in clinical practice. SAGE Open Med. 2014, 2, 205031211456257. [Google Scholar] [CrossRef]
- Sparrow, S.S. Vineland Adaptive Behavior Scales—Encyclopedia of Clinical Neuropsychology; Springer: New York, NY, USA, 2011. [Google Scholar]
- Lord, C.; Rutter, M.; DiLavore, P.C.; Risi, S.; Gotham, K.; Bishop, S. Autism Diagnostic Observation Schedule, 2nd ed.; (ADOS-2) Manual (Part I): Modules 1–4; Western Psychological Services: Torrance, CA, USA, 2012. [Google Scholar]
- Rutter, M.; Le Couteur, A.; Lord, C. ADI-R. Autism Diagnostic Interview Revised. Manual; Western Psychological Services: Los Angeles, LA, USA, 2003. [Google Scholar]
- Nasledov, A.D.; Miroshnikov, S.A.; Tkacheva, L.O. Elaboration of screening scales for early diagnosis of developmental delay in four- to five-year-old children in Russia. Psychol. Russ. State Art 2018, 11, 166–176. [Google Scholar] [CrossRef]
- Ivanova, A.E.; Miroshnikov, S.A. Metodicheskie Materialy k Ekspertnoi Sisteme Individual’nogo Soprovozhdeniya «Longityud» [Methodical Materials for the Expert System of Individual Tracking «Longitude»]; S.-Peterb. gos. Universitet St.: Petersburg, Russia, 2001. [Google Scholar]
- Nasledov, A.D.; Miroshnikov, S.; Zashchirinskaya, O.; Tkacheva, L. Differential diagnosis of cognitive and psychomotor development of children of four years. Psikhologicheskii Zhurnal 2018, 39, 59–75. [Google Scholar] [CrossRef]
- Miroshnikov, S.A.; Nasledov, A.D.; Zashchirinskaya, O.V. Criterion validation of the Scale of Psychomotor Development (SPMD) in developmental delay study of pre-school children. Procedia Soc. Behav. Sci. 2016, 233, 220–224. [Google Scholar] [CrossRef]
- Carroll, A.E.; Bauer, N.S.; Dugan, T.M.; Anand, V.; Saha, C.; Downs, S.M. Use of a computerized decision aid for developmental surveillance and screening. JAMA Pediatr. 2014, 168, 815–821. [Google Scholar] [CrossRef] [PubMed]
- Linting, M.; Meulman, J.J.; Groenen, P.J.F.; Van Der Koojj, A.J. Nonlinear principal components analysis: Introduction and application. Psychol. Methods 2007, 12, 336–358. [Google Scholar] [CrossRef] [PubMed]
- Byrne, B.M. Structural Equation Modeling with AMOS: Basic Concepts, Applications, and Programming; Taylor & Francis Group: New York, NY, USA, 2010. [Google Scholar]
- Kline, R.B. Principles and Practice of Structural Equation Modeling, 3rd ed.; Guilford Press: New York, NY, USA, 2011. [Google Scholar]
- Vodopyanova, N.E.; Nasledov, A.D. Standardized questionnaire “Loses and gains of resources” for socioeconomic specialists. Pedagog. Psychol. 2013, 4, 8–22. [Google Scholar]
- Glascoe, F.P.; Cairney, J. Best practices in test construction for developmental-behavioral measures: Quality standards for reviewers and researchers. In Follow-Up for NICU Graduates; Needelman, H., Jackson, B., Eds.; Springer: Cham, Switzerland, 2018; pp. 255–279. [Google Scholar] [CrossRef]
- Camp, B.W. Evaluating bias in validity studies of developmental/behavioral screening tests. J. Dev. Behav. Pediatr. 2007, 28, 234–240. [Google Scholar] [CrossRef] [PubMed]
- Gale, C.M.; Eikeseth, S.; Klintwall, L. Children with autism show atypical preference for non-social stimuli. Sci. Rep. 2019, 9, 10355. [Google Scholar] [CrossRef]
- Mody, M.; Belliveau, J.W. Speech and language impairments in autism: Insights from behavior and neuroimaging. Am. Chin. J. Med. Sci. 2013, 5, 157–161. [Google Scholar] [CrossRef]
- Posar, A.; Visconti, P. Sensory abnormalities in children with autism spectrum disorder. J. Pediatr. 2017, 94, 342–350. [Google Scholar] [CrossRef]
- Dube, W.V.; Farber, R.S.; Mueller, M.R.; Grant, E.; Lorin, L.; Deutsch, C.K. Stimulus overselectivity in autism, down syndrome, and typical development. Am. J. Intellect. Dev. Disabil. 2016, 121, 219–235. [Google Scholar] [CrossRef][Green Version]
- Kleberg, J.L.; Högström, J.; Nord, M.; Bölte, S.; Serlachius, E.; Falck-Ytter, T. Autistic traits and symptoms of social anxiety are differentially related to attention to others’ eyes in social anxiety disorder. J. Autism Dev. Disord. 2017, 47, 3814–3821. [Google Scholar] [CrossRef] [PubMed]
- Nasledov, A.; Miroshnikov, S.; Tkacheva, L.; Zashchirinskaya, O.; Goncharov, V. Elaborating screening scales for early diagnosis of developmental delay in five- to six-year-old children in russia. Psychol. Russia 2020, 13, 18–33. [Google Scholar]
- Anderson, V.; Reidy, N. Assessing executive function in preschoolers. Neuropsychol. Rev. 2012, 22, 345–360. [Google Scholar] [CrossRef] [PubMed]
- Fiske, A.; Holmboe, K. Neural substrates of early executive function development. Dev. Rev. 2019, 52, 42–62. [Google Scholar] [CrossRef] [PubMed]
- Delehanty, A.D.; Stronach, S.; Guthrie, W.; Slate, E.; Wetherby, A.M. Verbal and nonverbal outcomes of toddlers with and without autism spectrum disorder, language delay, and global developmental delay. Autism Dev. Lang. Impair. 2018, 3, 1–18. [Google Scholar] [CrossRef]
- Kinzler, K.D.; Spelke, E.S. Core systems in human cognition. Prog. Brain Res. 2007, 164, 257–264. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
| Item | Norm (n = 814) | DD (n = 26) | Total (n = 840) | |||
|---|---|---|---|---|---|---|
| Count | % | Count | % | Count | % | |
| n182 | 719 | 88.33 | 5 | 19.23 | 724 | 86.19 |
| n187 | 525 | 64.50 | 4 | 15.38 | 529 | 62.98 |
| n189 | 662 | 81.33 | 1 | 3.85 | 663 | 78.93 |
| n195 | 640 | 78.62 | 4 | 15.38 | 644 | 76.67 |
| n238 | 685 | 84.15 | 5 | 19.23 | 690 | 82.14 |
| n248 | 504 | 61.92 | 2 | 7.69 | 506 | 60.24 |
| n260 | 464 | 57.00 | 2 | 7.69 | 466 | 55.48 |
| n266 | 687 | 84.40 | 5 | 19.23 | 692 | 82.38 |
| n270 | 553 | 67.94 | 1 | 3.85 | 554 | 65.95 |
| n288 | 394 | 48.40 | 2 | 7.69 | 396 | 47.14 |
| n289 | 597 | 73.34 | 0 | 0.00 | 597 | 71.07 |
| n291 | 556 | 68.30 | 3 | 11.54 | 559 | 66.55 |
| n295 | 476 | 58.48 | 4 | 15.38 | 480 | 57.14 |
| n302 | 323 | 39.68 | 1 | 3.85 | 324 | 38.57 |
| n325 | 404 | 49.63 | 1 | 3.85 | 405 | 48.21 |
| n355 | 448 | 55.04 | 1 | 3.85 | 449 | 53.45 |
| n361 | 588 | 72.24 | 4 | 15.38 | 592 | 70.48 |
| n362 | 605 | 74.32 | 5 | 19.23 | 610 | 72.62 |
| n385 | 266 | 32.68 | 1 | 3.85 | 267 | 31.79 |
| n548 | 748 | 91.89 | 8 | 30.77 | 756 | 90.00 |
| n628 | 407 | 50.00 | 4 | 15.38 | 411 | 48.93 |
| n629 | 293 | 36.00 | 2 | 7.69 | 295 | 35.12 |
| n640 | 320 | 39.31 | 7 | 26.92 | 327 | 38.93 |
| n655 | 194 | 23.83 | 3 | 11.54 | 197 | 23.45 |
| n818 | 564 | 69.29 | 3 | 11.54 | 567 | 67.50 |
| n847 | 631 | 77.52 | 4 | 15.38 | 635 | 75.60 |
| n890 | 157 | 19.29 | 0 | 0.00 | 157 | 18.69 |
| Mean | 497 | 61 | 3 | 12 | 500 | 59 |
| Rotated Component Loadings of 27 Items (n = 814), α = 0.874, 43.92% of Variance | CL 1 |
|---|---|
| Factor 1: “Motor skills” (S1; 13.48% of variance), α = 0.755 (9 items) | |
| 195. Draws a cross by himself looking at the example | 0.710 |
| 248. Draws a cross without looking at the example | 0.640 |
| 260. Draws a person (“head and legs”). | 0.591 |
| 325. Can cut with scissors in a straight line | 0.571 |
| 187. Buttons buttons | 0.553 |
| 238. Can complete the picture of a person with missing arms and legs | 0.553 |
| 355. Walks “heel to toes” | 0.515 |
| 302. Can copy a triangle | 0.502 |
| 266. Can hold back on signal | 0.413 |
| Factor 2: “General awareness” (S2; 11.00% of variance), α = 0.792 (6 items) | |
| 640. (639–640) The child knows the names of wild animals 2 | 0.777 |
| 628. The child gives a correct answer to the question: “How many ears have you got?” | 0.746 |
| 655. (654–655) The child knows the names of cubs of some animals 2 | 0.717 |
| 385. Can find true and false in the picture. | 0.673 |
| 890. The child gives the correct answer to the question: “What is left on the ground after raining?” | 0.545 |
| 629. The child knows all seasons | 0.506 |
| Factor 3: “Logical reasoning” (S3; 10.54% of variance), α = 0.745 (7 items) | |
| 291. Counts the fingers correctly | 0.662 |
| 289. The child gives the correct answers to the questions: “When do you go to bed, in the morning or in the evening? When do you have lunch, at night or in the afternoon? When do you sleep?” | 0.640 |
| 189. Can answer the questions, like: “What do you do, if you feel cold? when you are tired? when you are hungry?” | 0.585 |
| 270. Knows six colours | 0.579 |
| 182. Says his first name and his surname | 0.480 |
| 295. The child uses grammatically correct sentences in his speech | 0.471 |
| 288. “The child gives the correct answers to the question: “What season is it now? During which season it can snow/During which season the leaves get yellow and fall?” | 0.453 |
| Factor 4: “Executive functions” (S4; 8.90% of variance), α = 0.759 (5 items) | |
| 548. (547–548) The child finds 10 pictures of 20, which you showed to him before 2 | 0.667 |
| 847. (846–847) The child can answer the questions: “What do you think, what is in common between a spoon and a fork?” 2 | 0.667 |
| 362. Can count up to 5 objects | 0.661 |
| 818. (816–818) Counts the objects correctly. 2 | 0.658 |
| 361. Finds a picture in a row, which differs from the rest | 0.560 |
| Model | CMIN 1 | df2; p3 | CFI 4 | GFI 5 | RMSEA 6 | 90% CI 7 |
|---|---|---|---|---|---|---|
| 1 | 2783.405 | 324; p < 0.001 | 0.588 | 0.763 | 0.097 | 0.093–0.100 |
| 2 | 1368.936 | 318; p < 0.001 | 0.824 | 0.888 | 0.064 | 0.060–0.067 |
| 3 | 1375.091 | 320; p < 0.001 | 0.823 | 0.887 | 0.064 | 0.060–0.067 |
| 4 | 883.726 | 314; p < 0.001 | 0.904 | 0.926 | 0.047 | 0.044–0.051 |
| Scales | Diagnosis | Means | Std. Dev. | Cohen’s d |
|---|---|---|---|---|
| Motor skills (S1) | Norm | 14.7494 | 2.39127 | 2.394 |
| DD | 9.9615 | 1.50946 | ||
| General awareness (S2) | Norm | 8.0111 | 1.93781 | 0.842 |
| DD | 6.6538 | 1.19808 | ||
| Logical reasoning (S3) | Norm | 11.8612 | 1.95248 | 2.795 |
| DD | 7.6154 | 0.89786 | ||
| Executive functions (S4) | Norm | 8.8526 | 1.47480 | 1.956 |
| DD | 5.9231 | 1.52113 | ||
| Sum (SS) | Norm | 43.4742 | 5.84327 | 2.709 |
| DD | 30.1538 | 3.77033 |
| Age | S1 | S2 | S3 | S4 | SS | |
|---|---|---|---|---|---|---|
| Age (days) | 1 | 0.352 | 0.771 | 0.285 | 0.420 | 0.601 |
| Motor skills (S1) | 0.352 | 1 | 0.358 | 0.543 | 0.392 | 0.808 |
| Awareness (S2) | 0.771 | 0.358 | 1 | 0.382 | 0.327 | 0.688 |
| Logical reasoning (S3) | 0.285 | 0.543 | 0.382 | 1 | 0.481 | 0.805 |
| Executive functions (S4) | 0.420 | 0.392 | 0.327 | 0.481 | 1 | 0.682 |
| Sum (SS) | 0.601 | 0.808 | 0.688 | 0.805 | 0.682 | 1 |
| SScor 1 (Upper Limit) | 30.19 | 32.83 | 35.8 | 38.57 | 41.46 | 44.05 | 46.26 | 47.95 | 49.37 | 50.88 | >50.9 |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Sten | 0 | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 |
| Norm, % | 0.6 | 1.7 | 4.3 | 9.2 | 15.0 | 19.2 | 19.2 | 15.0 | 9.2 | 4.3 | 2.3 |
| DD, % | 61.5 | 23.1 | 7.7 | 3.8 | 3.8 | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 |
| Statistic | Value | 95% CI |
|---|---|---|
| Sensitivity | 92.31% | 74.87–99.05 |
| Specificity | 93.37% | 91.43–94.98 |
| Positive Predict Value | 99.62% | 99.50–99.72 |
| Accuracy | 92.36% | 90.35–94.07 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nasledov, A.; Miroshnikov, S.; Tkacheva, L.; Goncharov, V. Elaboration of Screening Scales for Mental Development Problems Detection in Russian Preschool Children: Psychometric Approach. Diagnostics 2020, 10, 646. https://doi.org/10.3390/diagnostics10090646
Nasledov A, Miroshnikov S, Tkacheva L, Goncharov V. Elaboration of Screening Scales for Mental Development Problems Detection in Russian Preschool Children: Psychometric Approach. Diagnostics. 2020; 10(9):646. https://doi.org/10.3390/diagnostics10090646
Chicago/Turabian StyleNasledov, Andrey, Sergey Miroshnikov, Liubov Tkacheva, and Vadim Goncharov. 2020. "Elaboration of Screening Scales for Mental Development Problems Detection in Russian Preschool Children: Psychometric Approach" Diagnostics 10, no. 9: 646. https://doi.org/10.3390/diagnostics10090646
APA StyleNasledov, A., Miroshnikov, S., Tkacheva, L., & Goncharov, V. (2020). Elaboration of Screening Scales for Mental Development Problems Detection in Russian Preschool Children: Psychometric Approach. Diagnostics, 10(9), 646. https://doi.org/10.3390/diagnostics10090646