

Effects of Egg Consumption on Subjects with SLD or Hypertension: A MICOL Study
 , , , , ,
, , , , ,  and
and
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design and Population
2.2. Lifestyle, Clinical and Dietary Assessment
2.3. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Strengths and Limitations
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Powell, E.E.; Wong, V.W.S.; Rinella, M. Non-alcoholic fatty liver disease. Lancet 2021, 397, 2212–2224. [Google Scholar] [CrossRef] [PubMed]
- Younossi, Z.; Anstee, Q.M.; Marietti, M.; Hardy, T.; Henry, L.; Eslam, M.; Geroge, J.; Bugianesi, E. Global burden of NAFLD and NASH: Trends, predictions, risk factors and prevention. Nat. Rev. Gastroenterol. Hepatol. 2018, 15, 11–20. [Google Scholar] [CrossRef] [PubMed]
- Obesity epidemic results in Non-Alcoholic Fatty Liver Disease (NAFLD) becoming the most common cause of liver disease in Europe. EASL-The Home of Hepatology. Available online: https://www.ansa.it/pressrelease/english/2019/09/26/obesity-epidemic-results-in-non-alcoholic-fatty-liver-disease-nafld-becoming-the-most-common-cause_510e3913-3e9c-4d6a-bdd9-3edfec16c102.html (accessed on 5 October 2019).
- Masarone, M.; Federico, A.; Abenavoli, L.; Loguercio, C.; Persico, M. Non alcoholic fatty liver: Epidemiology and natural history. Rev. Recent. Clin. Trials 2014, 9, 126–133. [Google Scholar] [CrossRef] [PubMed]
- Marchesini, G.; Brizi, M.; Bianchi, G.; Tomassetti, S.; Bugianesi, E.; Lenzi, M.; McCullough, A.J.; Natale, S.; Forlani, G.; Melchionda, N. Nonalcoholic fatty liver disease: A feature of the metabolic syndrome. Diabetes 2001, 50, 1844–1850. [Google Scholar] [CrossRef] [PubMed]
- Marchesini, G.; Bugianesi, E.; Forlani, G.; Cerrelli, F.; Lenzi, M.M.; Manini, R.; Natale, S.; Vanni, E.; Villanova, N.; Melchionda, N.; et al. Nonalcoholic fatty liver, steatohepatitis, and the metabolic syndrome. Hepatology 2003, 37, 917–923. [Google Scholar] [CrossRef] [PubMed]
- Lewington, S.; Clarke, R.; Quzilbash, N.; Peto, R.; Collins, R. Prospective Studies Collaboration. Lancet 2002, 360, 1903–1913. [Google Scholar]
- Franco, C.; Sciatti, E.; Favero, G.; Bonomini, F.; Vizzardi, E.; Rezzani, R. Essential Hypertension and oxidative stress: Novel future perspectives. Int. J. Mol. Sci. 2022, 23, 14489. [Google Scholar] [CrossRef]
- Kearney, P.M.; Whelton, M.; Reynolds, K.; Muntner, P.; Whelton, P.K.; He, J. Global burden of hypertension: Analysis of worldwide data. Lancet 2005, 365, 217–223. [Google Scholar] [CrossRef]
- Kim, G.H.; Shin, S.W.; Lee, J.; Hwang, J.H.; Park, S.W.; Moon, J.S.; Kim, H.J.; Ahn, H.S. Red meat and chicken consumption and its association with high blood pressure and obesity in South Korean children and adolescents: A cross-sectional analysis of KSHES, 2011–2015. Nutr. J. 2017, 16, 31. [Google Scholar] [CrossRef] [PubMed]
- Lampignano, L.; Tatoli, R.; Donghia, R.; Bortone, I.; Castellana, F.; Zupo, R.; Lozupone, M.; Panza, F.; Conte, C.; Sardone, R. Nutritional patterns as machine learning predictors of liver health in a population of elderly subjects. Nutr. Metab. Cardiovasc. Dis. 2023, 33, 2233–2241. [Google Scholar] [CrossRef] [PubMed]
- Papandreou, D.; Andreou, E. Role of diet on non-alcoholic fatty liver disease: An updated narrative review. World J. Hepatol. 2015, 7, 575–582. [Google Scholar] [CrossRef]
- Nseir, W.; Nassar, F.; Assy, N. Soft drinks consumption and nonalcoholic fatty liver disease. World J. Gastroenterol. 2010, 16, 2579–2588. [Google Scholar] [CrossRef]
- Zelber-Sagi, S.; Godos, J.; Salomone, F. Lifestyle changes for the treatment of nonalcoholic fatty liver disease: A review of observational studies and intervention trials. Therap Adv. Gastroenterol. 2016, 9, 392–407. [Google Scholar] [CrossRef]
- Souza, G.H.D.P.E.; Silva, L.D.; Vieira, D.A.; Rocha, G.A.; Lima, A.S.; Vidigal, P.V.T. High-density lipoprotein cholesterol and systemic arterial hypertension are associated with hepatic necroinflammatory activity in patients with chronic hepatitis C. Arq. Gastroenterol. 2023, 60, 287–299. [Google Scholar] [CrossRef]
- Enjoji, M.; Yasutake, K.; Kohjima, M.; Nakamuta, M. Nutrition and nonalcoholic Fatty liver disease: The significance of cholesterol. Int. J. Hepatol. 2012, 2012, 925807. [Google Scholar] [CrossRef]
- Kerr, T.A.; Davidson, N.O. Cholesterol and nonalcoholic fatty liver disease: Renewed focus on an old villain. Hepatology 2012, 56, 1995–1998. [Google Scholar] [CrossRef]
- Song, W.O.; Kerver, J.M. Nutritional contribution of eggs to American diets. J. Am. Coll. Nutr. 2000, 19, 556S–562S. [Google Scholar] [CrossRef] [PubMed]
- Expert Panel on Detection, Evaluation, and Treatment of hight Blood Cholesterol in Alduts. Executive Summary of The Third Report of The National Cholesterol Education Program (NCEP) Expert Panel on Detection, Evaluation, And Treatment of High Blood Cholesterol In Adults (Adult Treatment Panel III). JAMA 2001, 285, 2486–2497. [Google Scholar] [CrossRef] [PubMed]
- Clayton, Z.S.; Fusco, E.; Kern, M. Egg consumption and heart health: A review. Nutrition 2017, 37, 79–85. [Google Scholar] [CrossRef]
- Han, J.M.; Jo, A.N.; Lee, S.M.; Bae, H.S.B.; Jun, D.W.; Cho, Y.K.; Suk, K.T.; Yoon, J.H.; Ahn, S.B.; Cho, Y.J.; et al. Associations between intakes of individual nutrients or whole food groups and non-alcoholic fatty liver disease among Korean adults. J. Gastroenteerol. Hepatol. 2014, 29, 1265–1272. [Google Scholar] [CrossRef] [PubMed]
- Shi, L.; Liu, Z.W.; Li, Y.; Gong, C.; Zhang, H.; Song, L.J.; Huang, C.Y.; Li, M. The prevalence of nonalcoholic fatty liver disease and its association with lifestyle/dietary habits among university faculty and staff in Chengdu. Biomed. Environ. Sci. 2012, 25, 383–391. [Google Scholar]
- Zelber-Sagi, S.; Nitzan-Kaluski, D.; Goldsmith, R.; Webb, M.; Blendis, L.; Halpern, Z.; Oren, R. Long term nutritional intake and the risk for non-alcoholic fatty liver disease (NAFLD): A population based study. J. Hepatol. 2007, 47, 711–717. [Google Scholar] [CrossRef]
- Mokhtari, Z.; Poustchi, H.; Eslamparast, T.; Hekmatdoost, A. Egg consumption and risk of non-alcoholic fatty liver disease. World J. Hepatol. 2017, 9, 503–509. [Google Scholar] [CrossRef]
- Baumgartner, S.; Kelly, E.R.; van der Made, S.; Berendschot, T.T.; Husche, C.; Lütjohann, D.; Plat, J. The influence of consuming an egg or an egg-yolk buttermilk drink for 12 wk on serum lipids, inflammation, and liver function markers in human volunteers. Nutrition 2013, 29, 1237–1244. [Google Scholar] [CrossRef] [PubMed]
- Donghia, R.; Pesole, P.L.; Coletta, S.; Bonfiglio, C.; De Pergola, G.; De Nucci, S.; Rinaldi, R.; Giannelli, G. Food Network Analysis in Non-Obese Patients with or without Steatosis. Nutrients 2023, 15, 2713. [Google Scholar] [CrossRef] [PubMed]
- Misciagna, G.; Leoci, C.; Guerra, V.; Chiloiro, M.; Elba, S.; Petruzzi, J.; Mossa, A.; Noviello, M.R.; Coviello, A.; Minutolo, M.C.; et al. Epidemiology of cholelithiasis in southern Italy. Part II: Risk factors. Eur. J. Gastroenteerol. Hepatol. 1996, 8, 585–593. [Google Scholar] [CrossRef] [PubMed]
- Attili, A.F.; Capocaccia, R.; Carulli, N.; Festi, D.; Roda, E.; Barbare, L.; Capocaccia, L.; Menotti, A.; Okolicsanyi, L.; Ricci, G.; et al. Factors associated with gallstone disease in the MICOL experience. Multicenter Italian Study on Epidemiology of Cholelithiasis. Hepatology 1997, 26, 809–818. [Google Scholar] [CrossRef] [PubMed]
- Chiloiro, M.; Caruso, M.G.; Cisternino, A.M.; Inguaggiato, R.; Reddavide, R.; Bonfiglio, C.; Guerra, V.; Notarnicola, M.; De Michele, G.; Correale, M.; et al. Ultrasound evaluation and correlates of fatty liver disease: A population study in a Mediterranean area. Metab. Syndr. Relat. Disord. 2013, 11, 349–358. [Google Scholar] [CrossRef] [PubMed]
- Sever, P. New hypertension guidelines from the National Institute for Health and Clinical Excellence and the British Hypertension Society. J. Renin Angiotensin Aldosterone Syst. 2006, 7, 61–63. [Google Scholar] [CrossRef] [PubMed]
- Leoci, C.C.S.; Guerra, V.; Cisternino, A.M.; Misciagna, G. Reliability and validity of a self administrered semi-quantitative food frequency questionnaire. Giorn. Italy Nutr. Clin. Prev. 1993, 71, 1269–1324. [Google Scholar]
- Musso, G.; Gambino, R.; De Michieli, F.D.; Cassader, M.; Rizzetto, M.; Durazzo, M.; Fagà, E.; Silli, B.; Pagano, G. Dietary habits and their relations to insulin resistance and postprandial lipemia in nonalcoholic steatohepatitis. Hepatology 2003, 37, 909–916. [Google Scholar] [CrossRef]
- Yasutake, K.; Nakamuta, M.; Shima, Y.; Ohyama, A.; Masuda, K.; Haruta, N.; Fujino, T.; Aoyagi, Y.; Fukuizumi, K.; Yoshimoto, T.; et al. Nutritional investigation of non-obese patients with non-alcoholic fatty liver disease: The significance of dietary cholesterol. Scand. J. Gastoenterol. 2009, 44, 471–477. [Google Scholar] [CrossRef] [PubMed]
- Goodrow, E.F.; Wilson, T.A.; Houde, S.C.; Vishwanathan, R.; Scollin, P.A.; Handelman, G.; Nicolosi, R.J. Consumption of one egg per day increases serum lutein and zeaxanthin concentrations in older adults without altering serum lipid and lipoprotein cholesterol concentrations. J. Nutr. 2006, 136, 2519–2524. [Google Scholar] [CrossRef] [PubMed]
- Reaven, G.M.; Abbasi, F.; Bernhart, S.; Coulston, A.; Darnell, B.; Dashti, N.; Kim, H.; Kulkarni, K.; Lamendola, C.; McLaughlin, T.; et al. Insulin resistance, dietary cholesterol, and cholesterol concentration in postmenopausal women. Metabolism 2001, 50, 594–597. [Google Scholar] [CrossRef]
- Mayurasakorn, K.; Srisura, W.; Sitphahul, P.; Hongto, P. High-density lipoprotein cholesterol changes after continuous egg consumption in healthy adults. J. Med. Assoc. Thai. 2008, 91, 400–407. [Google Scholar] [PubMed]
- Cohn, J.S.; Kamili, A.; Wat, E.; Chung, R.W.S.; Tandy, S. Reduction in intestinal cholesterol absorption by various food components: Mechanisms and implications. Atheroscler. Suppl. 2010, 11, 45–48. [Google Scholar] [CrossRef]
- Gunness, P.; Gidley, M.J. Mechanisms underlying the cholesterol-lowering properties of soluble dietary fibre polysaccharides. Food Funct. 2010, 1, 149–155. [Google Scholar] [CrossRef]
- Campanella, A.; Misciagna, G.; Mirizzi, A.; Caruso, M.G.; Bonfiglio, C.; Aballay, L.R.; de Arruda Silveira, L.V.; Bianco, A.; Franco, I.; Sorino, P.; et al. The effect of the Mediterranean Diet on lifespan: A treatment-effect survival analysis of a population-based prospective cohort study in Southern Italy. Int. J. Epidemiol. 2021, 50, 245–255. [Google Scholar] [CrossRef]
- Ordovas, J.M.; Lopez-Miranda, J.; Mata, P.; Perez-Jimenez, F.; Lichtenstein, A.H.; Schaefer, E.J. Gene-diet interaction in determining plasma lipid response to dietary intervention. Atherosclerosis 1995, 118, S11–S27. [Google Scholar] [CrossRef]
- Ostlund, R.E., Jr.; Bosner, M.S.; Stenson, W.F. Cholesterol absorption efficiency declines at moderate dietary doses in normal human subjects. J. Lipid Res. 1999, 40, 1453–1458. [Google Scholar] [CrossRef]
- Jones, P.J.; Pappu, A.S.; Hatcher, L.; Li, Z.C.; Illingworth, D.R.; Connor, W.E. Dietary cholesterol feeding suppresses human cholesterol synthesis measured by deuterium incorporation and urinary mevalonic acid levels. Arterioscler. Thromb. Vasc. Biol. 1996, 16, 1222–1228. [Google Scholar] [CrossRef] [PubMed]
- Preli, R.B.; Klein, K.P.; Herrington, D.M. Vascular effects of dietary L-arginine supplementation. Atherosclerosis 2002, 162, 1–15. [Google Scholar] [CrossRef] [PubMed]
- Wallin, A.; Forouhi, N.G.; Wolk, A.; Larsson, S.C. Egg consumption and risk of type 2 diabetes: A prospective study and dose-response meta-analysis. Diabetologia 2016, 59, 1204–1213. [Google Scholar] [CrossRef] [PubMed]
- Noureddin, M.; Mato, J.M.; Lu, S.C. Nonalcoholic fatty liver disease: Update on pathogenesis, diagnosis, treatment and the role of S-adenosylmethionine. Exo Biol. Med. 2015, 240, 809–820. [Google Scholar] [CrossRef] [PubMed]
- Talari, H.R.; Molaqanbari, M.R.; Mokfi, M.; Taghizadeg, M.; Bahmani, F.; Tabatabei, S.M.H.; Sharifi, N. The effects of vitamin B12 supplementation on metabolic profile of patients with non-alcoholic fatty liver disease: A randomized controlled trial. Sci. Rep. 2022, 12, 14047. [Google Scholar] [CrossRef] [PubMed]
- Koplay, M.; Gulcan, E.; Ozkan, F. Association between serum vitamin B12 levels and the degree of steatosis in patients with nonalcoholic fatty liver disease. J. Investig. Med. 2011, 59, 1137–1140. [Google Scholar] [CrossRef]
- Cordero, P.; Gomez-Uriz, A.M.; Campion, J.; Milagro, F.I.; Martinez, J.A. Dietary supplementation with methyl donors reduces fatty liver and modifies the fatty acid synthase DNA methylation profile in rats fed an obesogenic diet. Genes Nutr. 2013, 8, 105–113. [Google Scholar] [CrossRef]
- Zhang, Y.; Zhang, D.Z. Red meat, poultry, and egg consumption with the risk of hypertension: A meta-analysis of prospective cohort studies. J. Hum. Hypertens. 2018, 32, 507–517. [Google Scholar] [CrossRef]
- Miguel, M.; Aleixandre, A. Antihypertensive peptides derived from egg proteins. J. Nutr. 2006, 136, 1457–1460. [Google Scholar] [CrossRef]
- Hong, F.; Ming, L.M.; Yi, S.; Zhanxia, L.; Yongquan, W.; Chi, L. The antihypertensive effect of peptides: A novel alternative to drugs? Peptides 2008, 29, 1062–1071. [Google Scholar] [CrossRef] [PubMed]
- Miguel, M.; López-Fandiño, R.; Ramos, M.; Aleixandre, A. Short-term effect of egg-white hydrolysate products on the arterial blood pressure of hypertensive rats. Br. J. Nutr. 2005, 94, 731–737. [Google Scholar] [CrossRef] [PubMed]
- Aleixandre, A.; Miguel, M.; Muguerza, B. Peptides with antihypertensive activity from milk and egg proteins. Nutr. Hosp. 2008, 23, 313–318. [Google Scholar] [PubMed]

{kind=link}
| Parameters * | Disease Condition | p ^ | Multiple Comparisons ψ | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| SLD (No)/ HTN (No) (n = 236) (a) | SLD (No)/ HTN (Yes) (n = 176) (b) | SLD (Yes)/ HTN (No) (n = 209) (c) | SLD (Yes)/ HTN (Yes) (n = 287) (d) | (b) vs. (a) | (c) vs. (a) | (d) vs. (a) | (c) vs. (b) | (d) vs. (b) | (d) vs. (c) | ||
| Gender (M) (%) | 116 (49.15) | 88 (50.00) | 126 (60.29) | 164 (57.14) | 0.05 ¥ | 0.86 † | 0.01 † | 0.48 † | 0.04 † | 0.13 † | 0.48 † |
| Age (yrs) | 61.34 ± 12.16 | 70.54 ± 9.33 | 61.72 ± 10.35 | 69.24 ± 8.44 | 0.001 | <0.0001 | 0.44 | <0.0001 | <0.0001 | 0.07 | <0.0001 |
| Degree of Education (%) | <0.001 ¥ | ||||||||||
| No | 59 (25.11) | 77 (43.75) | 47 (22.71) | 114 (40.00) | 0.0001 † | <0.0001 † | 0.0001 † | 0.04 † | 0.13 † | 0.48 † | |
| Elementary School | 68 (28.94) | 43 (24.43) | 81 (39.13) | 89 (31.23) | 0.31 † | 0.002 † | 0.07 † | 0.002 † | 0.12 † | 0.07 † | |
| Secondary School | 75 (31.91) | 29 (16.48) | 52 (25.12) | 45 (15.79) | 0.0004 † | 0.04 † | 0.01 † | 0.04 † | 0.84 † | 0.01 † | |
| High School | 27 (11.49) | 6 (3.41) | 17 (8.21) | 10 (3.51) | 0.003 † | 0.05 † | 0.02 † | 0.05 † | 0.95 † | 0.02 † | |
| Degree | 6 (2.55) | 21 (11.93) | 10 (4.83) | 27 (9.47) | 0.0001 † | 0.01 † | 0.05 † | 0.01 † | 0.40 † | 0.05 † | |
| Smoker (Yes) (%) | 36 (15.32) | 18 (10.29) | 33 (15.79) | 31 (10.84) | 0.18 ¥ | 0.14 † | 0.89 † | 0.13 † | 0.11 † | 0.85 † | 0.10 † |
| BMI (kg/m2) | 25.27 ± 3.32 | 27.32 ± 4.20 | 28.80 ± 4.33 | 31.56 ± 5.39 | 0.0001 | <0.0001 | <0.0001 | <0.0001 | 0.0001 | <0.0001 | <0.0001 |
| Diabetes (Yes) (%) | 10 (4.26) | 24 (13.64) | 17 (8.13) | 65 (22.65) | <0.001 ¥ | 0.0006 † | 0.09 † | <0.0001 † | 0.08 † | 0.001 † | <0.0001 † |
| MetS (Yes) (%) | 37 (15.68) | 77 (43.75) | 84 (40.19) | 198 (68.99) | <0.001 ¥ | <0.0001 † | <0.0001 † | <0.0001 † | 0.48 † | <0.0001 † | <0.0001 † |
| Parameters * | Disease Condition | p ^ | Multiple Comparisons ψ | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| SLD (No)/ HTN (No) (n = 236) (a) | SLD (No)/ HTN (Yes) (n = 176) (b) | SLD (Yes)/ HTN (No) (n = 209) (c) | SLD (Yes)/ HTN (Yes) (n = 287) (d) | (b) vs. (a) | (c) vs. (a) | (d) vs. (a) | (c) vs. (b) | (d) vs. (b) | (d) vs. (c) | ||
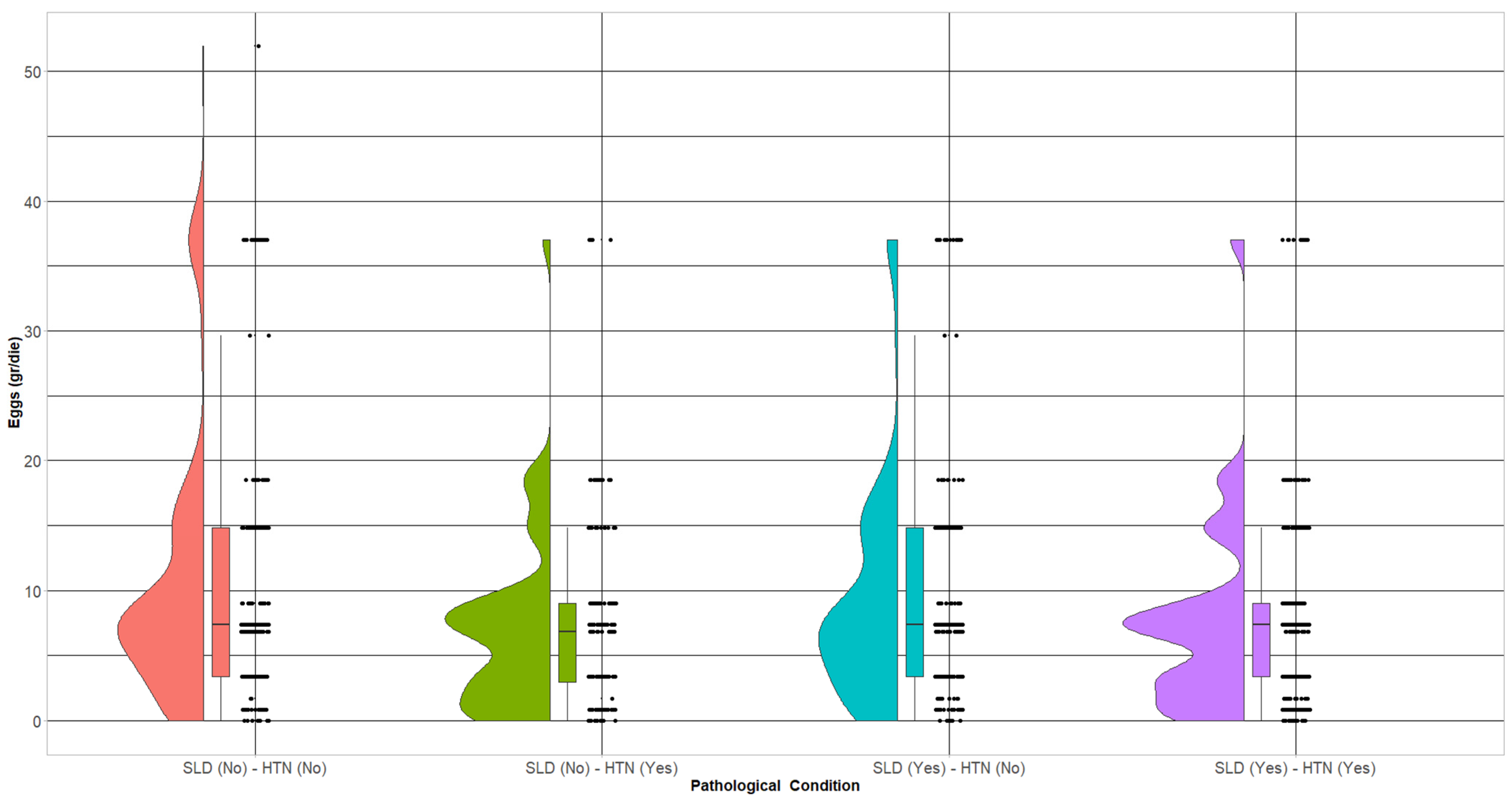
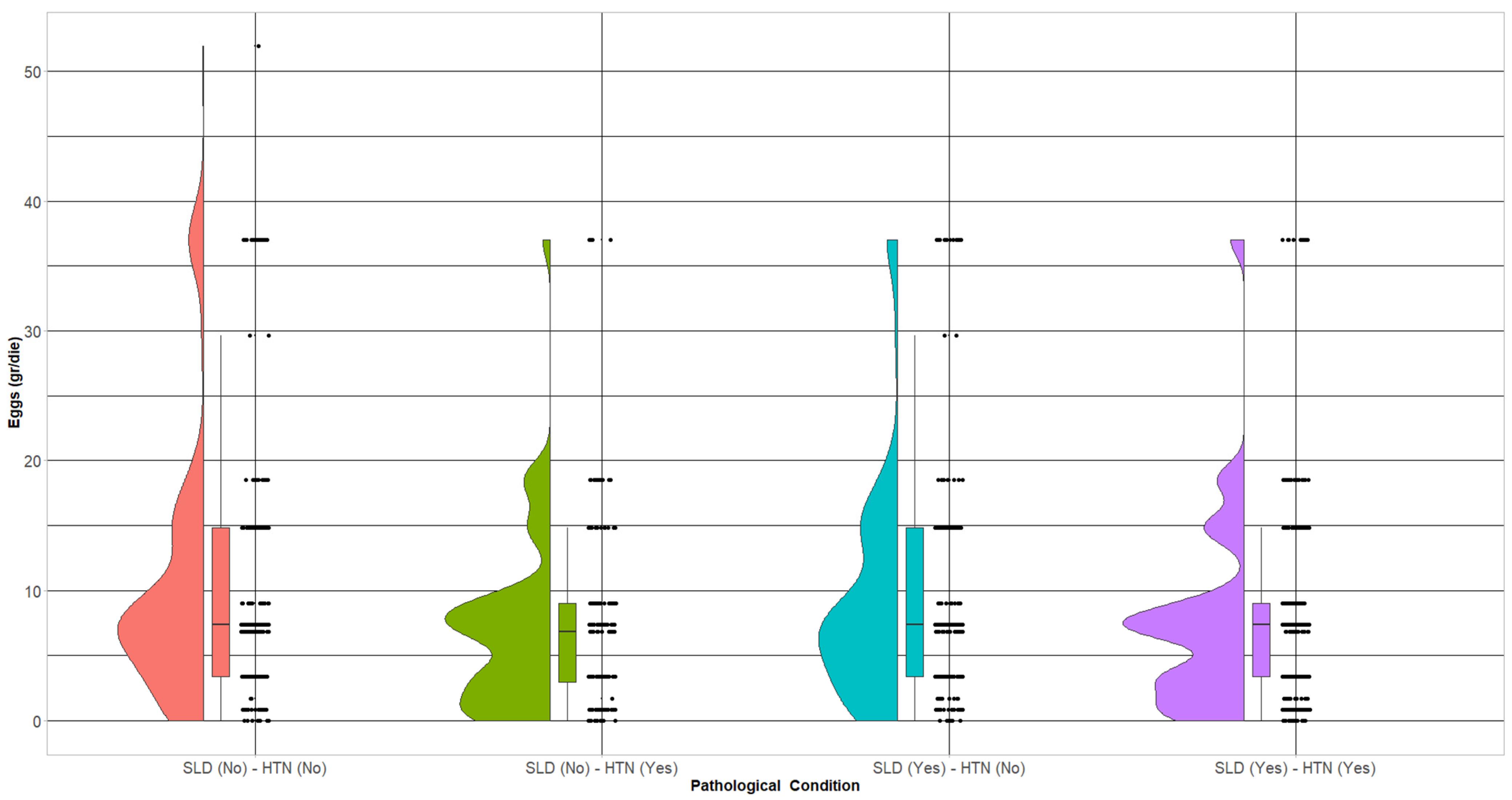
| Eggs (g/die) | 10.43 ± 9.85 | 7.23 ± 6.98 | 9.45 ± 8.77 | 7.82 ± 7.63 | 0.001 | 0.0005 | 0.12 | 0.0007 | 0.02 | 0.30 | 0.03 |
| Eggs (n#/week) (%) | 0.004 ¥ | ||||||||||
| <2 | 168 (71.19) | 146 (82.95) | 147 (70.33) | 227 (79.09) | 0.005 † | 0.84 † | 0.04 † | 0.004 † | 0.31 † | 0.02 † | |
| 2–3 | 46 (19.49) | 26 (14.77) | 48 (22.97) | 50 (17.42) | 0.21 † | 0.37 † | 0.55 † | 0.04 † | 0.45 † | 0.12 † | |
| >3 | 22 (9.32) | 4 (2.27) | 14 (6.70) | 10 (3.48) | 0.004 † | 0.31 † | 0.005 † | 0.07 † | 0.64 † | 0.10 † | |
| Parameters | SLD (No) and HTN (Yes) ¥ | SLD (Yes) and HTN (No) ¥ | SLD (Yes) and HTN (Yes) ¥ | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| RRR | se (RRR) | p | 95% C.I. | RRR | se (RRR) | p | 95% C.I. | RRR | se (RRR) | p | 95% C.I. | |
| Model 1 | ||||||||||||
| Eggs (g/die) | 0.95 | 0.01 | <0.001 | 0.93 to 0.98 | 0.99 | 0.01 | 0.29 | 0.97 to 1.01 | 0.96 | 0.01 | 0.001 | 0.94 to 0.98 |
| Eggs (n#/week) | ||||||||||||
| <2 [Ref.] | -- | -- | -- | -- | -- | -- | -- | -- | -- | -- | -- | -- |
| 2–3 | 0.65 | 0.17 | 0.11 | 0.38 to 1.10 | 1.19 | 0.28 | 0.45 | 0.75 to 1.89 | 0.80 | 0.18 | 0.34 | 0.51 to 1.26 |
| >3 | 0.21 | 0.12 | 0.005 | 0.07 to 0.62 | 0.73 | 0.26 | 0.38 | 0.36 to 1.47 | 0.34 | 0.13 | 0.006 | 0.15 to 0.73 |
| Model 2 | ||||||||||||
| Eggs (g/die) | 0.96 | 0.01 | 0.006 | 0.94 to 0.99 | 0.99 | 0.01 | 0.33 | 0.97 to 1.01 | 0.97 | 0.01 | 0.01 | 0.95 to 0.99 |
| Eggs (n#/week) | ||||||||||||
| <2 [Ref.] | -- | -- | -- | -- | -- | -- | -- | -- | -- | -- | -- | -- |
| 2–3 | 0.93 | 0.26 | 0.79 | 0.53 to 1.62 | 1.22 | 0.29 | 0.40 | 0.76 to 1.96 | 1.10 | 0.26 | 0.70 | 0.68 to 1.76 |
| >3 | 0.27 | 0.15 | 0.02 | 0.09 to 0.81 | 0.71 | 0.26 | 0.36 | 0.35 to 1.46 | 0.40 | 0.16 | 0.03 | 0.18 to 0.90 |
| Model 3 | ||||||||||||
| Eggs (g/die) | 0.96 | 0.01 | 0.009 | 0.94 to 0.99 | 0.99 | 0.01 | 0.22 | 0.97 to 1.01 | 0.97 | 0.01 | 0.008 | 0.95 to 0.99 |
| Eggs (n#/week) | ||||||||||||
| <2 [Ref.] | -- | -- | -- | -- | -- | -- | -- | -- | -- | -- | -- | -- |
| 2–3 | 0.99 | 0.29 | 0.96 | 0.56 to 1.75 | 1.17 | 0.28 | 0.51 | 0.73 to 1.89 | 1.03 | 0.25 | 0.91 | 0.63 to 1.67 |
| >3 | 0.27 | 0.16 | 0.02 | 0.09 to 0.84 | 0.62 | 0.23 | 0.19 | 0.30 to 1.28 | 0.34 | 0.14 | 0.009 | 0.15 to 0.76 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tatoli, R.; Bonfiglio, C.; Cuccaro, F.; Campanella, A.; Coletta, S.; Pesole, P.L.; Giannelli, G.; Donghia, R. Effects of Egg Consumption on Subjects with SLD or Hypertension: A MICOL Study. Nutrients 2024, 16, 430. https://doi.org/10.3390/nu16030430
Tatoli R, Bonfiglio C, Cuccaro F, Campanella A, Coletta S, Pesole PL, Giannelli G, Donghia R. Effects of Egg Consumption on Subjects with SLD or Hypertension: A MICOL Study. Nutrients. 2024; 16(3):430. https://doi.org/10.3390/nu16030430
Chicago/Turabian StyleTatoli, Rossella, Caterina Bonfiglio, Francesco Cuccaro, Angelo Campanella, Sergio Coletta, Pasqua Letizia Pesole, Gianluigi Giannelli, and Rossella Donghia. 2024. "Effects of Egg Consumption on Subjects with SLD or Hypertension: A MICOL Study" Nutrients 16, no. 3: 430. https://doi.org/10.3390/nu16030430
APA StyleTatoli, R., Bonfiglio, C., Cuccaro, F., Campanella, A., Coletta, S., Pesole, P. L., Giannelli, G., & Donghia, R. (2024). Effects of Egg Consumption on Subjects with SLD or Hypertension: A MICOL Study. Nutrients, 16(3), 430. https://doi.org/10.3390/nu16030430