1. Introduction
The complementary feeding phase is acknowledged as a critical period for addressing micronutrient imbalances, which may be even more important to very low birth weight (VLBW) infants [
1]. For term infants, the European Society for Pediatric Gastroenterology, Hepatology, and Nutrition (ESPGHAN) recommends introducing solids between the 17th and 26th week of life [
2]. However, evidence-based guidelines for preterm infants are still lacking. Observational studies indicate that preterm infants are introduced to solid foods at an earlier developmental stage than full-term infants [
3,
4].
Micronutrients such as iron, vitamin D, calcium, phosphorus, and zinc are of particular interest in VLBW infants due to diminished body stores, elevated micronutrient needs for catch-up growth, for example, and the nutrients’ critical roles in developmental processes [
5,
6].
Although some studies have investigated micronutrient intake during early postnatal phases, only a few studies are available regarding micronutrient intake during the complementary feeding period in VLBW infants, with most of them being outdated [
7,
8]. Notably, a recently published two-arm randomized interventional study investigated an early (between 10 and 12 weeks corrected age (CA)) versus late (between 16 and 18 weeks CA) introduction of solid foods in VLBW infants. Infants were fed a standardized, age-dependent, step-up feeding regimen until 12 months CA [
9,
10]. While this study made significant strides in elucidating micronutrient intake during complementary feeding in preterm infants, its exclusion of infants with comorbidities that may impede stable growth restricts its applicability to a broader VLBW population. Furthermore, the adequacy of current non-standardized micronutrient intakes and the potential influence of the timing of solids introduction, considering term infant guidelines (before vs. at or above 17 weeks CA) on critical micronutrient intakes, have yet to be determined.
Thus, this secondary analysis of a prospective observational study aims to investigate micronutrient intake patterns during complementary feeding in former VLBW infants, comparing the introduction of solids before and after 17 weeks CA. This study includes infants with preterm-birth-related comorbidities such as bronchopulmonary dysplasia (BPD), necrotizing enterocolitis (NEC), and intraventricular hemorrhage (IVH). Our objective was to gain a better understanding of complementary feeding practices in a representative VLBW cohort and to assess micronutrient intake in those with comorbidities. Additionally, this study aims to provide nutritional intake data comparing breastfed, formula-fed, and mixed-fed infants during the first year of life.
2. Materials and Methods
2.1. Study Design
This study constitutes a secondary analysis of nutritional intake data obtained from a prospective, observational study in VLBW infants. Infants with a birth weight below 1500 g and a gestational age < 32 weeks were included in the study. Exclusion criteria encompassed congenital heart disease, chromosomal aberrations, major congenital birth defects, and Hirschsprung disease. Study subjects were longitudinally monitored in the outpatient clinic of the Division of Neonatology at the Medical University of Vienna between April 2016 and November 2021.
Based on the parental decision to start complementary feeding, infants were categorized into either an early (<17th week CA) or late (≥17th week CA) complementary feeding group.
The study received ethical approval from the ethics committee of the Medical University of Vienna (EK: 1273/2016) and was registered on clinicaltrials.gov (NCT02936219). Informed consent was obtained from at least one parent or legal guardian for each participating infant. The primary outcome report of this study was previously published by Thanhaeuser et al. [
11].
2.2. Study Visits, Nutrient Intake Data Collection, and Evaluation
Infants were regularly followed up in the neonatal outpatient clinic of the Division of Neonatology. Within regular checkups, study visits were conducted covering term, 6 weeks, 12 weeks, and 6, 9, and 12 months CA. At the respective timepoints, standardized procedures for the collection of anthropometric measurements, including body weight, length, and head circumference, were conducted. Parents of participating infants underwent guidance from a nutritionist, equipping them to maintain food logs that documented enteral intake at specified intervals. At 6 weeks CA, parents were instructed to complete a 24 h recall, while 3-day dietary records were required at 12 weeks and at 6, 9, and 12 months CA. While 24 h recalls yielded retrospective information on foods and beverages consumed on a given day, prospective 3-day dietary records consisted of three consecutive days, including one weekend day. For both dietary assessments, parents were asked to include details on product brands and recipes of self-prepared meals.
The subsequent analysis of dietary records was undertaken by a nutritionist using nut.s nutritional software, referencing the German nutrient database and the Austrian nutrient table (nut.s nutritional software, Vienna, Austria, Version II.3.1).
For infants who were breastfed, estimated average values for consumed mother’s milk, as published by Dewey et al., were utilized [
12]. Detailed information on infant formula had to be documented in each protocol. To ensure precise nutrient analysis, recipes of all infant formulas were sought from distinct manufacturers, and changes in formulations were factored into the calculations. Body weight at the corresponding date of the dietary record was employed to calculate protein intake per kilogram of body weight. For months without measurements, body weight was determined based on the daily increase between the closest two measurements.
Prior to March 2017, infants received a supplementation of 650 international units (IU)/d of vitamin D3 until reaching one year CA. However, in April 2017, this protocol was revised to 800 IU/d of vitamin D3 supplementation until one year CA. Moreover, infants were supplemented with 2–3 mg/kg/d iron (administered as Ferrum Hausmann®, iron oxide polymaltose complex, Vifor France, Paris, France) until a regular meat intake was established. Precise dosages, as well as the initiation and cessation dates of all supplements, were recorded and utilized for daily intake computation. Dietary intake refers exclusively to oral consumption from foods, while total intakes encompass both dietary and supplementary intake.
2.3. Outcome Data
The primary outcome of this analysis was iron intake (mg/kg/d) at 6 and 12 weeks and at 6, 9, and 12 months CA. Secondary outcomes included intake of total iron, dietary vitamin D, total vitamin D, calcium, phosphorus, and zinc. Additionally, we performed a subgroup analysis to compare micronutrient intakes between infants with BPD, NEC, or IVH and infants without comorbidities. Moreover, we compared micronutrient intakes in breastfed, formula-fed, and mixed-fed infants.
Nutrient intakes were compared with current dietary intake guidelines for preterm infants (iron, vitamin D). For zinc, phosphorus, and calcium, no specific dietary intake recommendations for preterm infants were available; hence, dietary intake recommendations for term infants were used for comparison.
2.4. Sample Size Calculation
The sample size calculation for this study was based on the assumption that a 5% difference in body length represents the minimally clinically relevant effect. A coefficient of variation of 11% was assumed to estimate the standard deviation, with the significance level set at 0.05. Using these parameters, along with a power of 80%, a sample size of 152 infants (76 per group) was calculated to detect a statistically significant difference in length gain between the early and late observation groups. To account for an anticipated 30% dropout rate, the final sample size required was 198 infants.
2.5. Statistical Analysis
Assessment of nutrient intake involved a comparative analysis between the early and late introduction of solid foods (before and after 17 weeks CA). Participants who were lost to follow-up, withdrew informed consent, or had insufficient dietary records were excluded from this secondary outcome analysis. However, dietary protocols up to the point of lost follow-up or withdrawal of informed consent, as well as protocols of infants without the primary outcome of the study, were included in this analysis.
Neonatal baseline characteristics are provided as mean with standard deviation (SD). To detect differences between baseline characteristics, the chi-squared test or the Mann–Whitney U-test was applied.
Statistical analysis of the primary and secondary outcomes employed linear mixed-effects models. These models incorporated relevant covariates such as group assignment (early vs. late introduction), sex, gestational age, and nutrition at 6 weeks CA (breastmilk, formula, or mixed feeding). A random intercept was used to account for potential correlations among siblings of multiple births. We conducted subgroup analyses to investigate micronutrient intake by comparing infants with and without comorbidities (BPD, NEC ≥ grade II, IVH ≥ grade II). BPD was defined as oxygen demand ≥ 36 + 0. Diagnosis of NEC was made by clinical and radiological findings according to Bell’s staging criteria for NEC. [
13] The degree of IVH was graded I through IV according to Papile et al. [
14].
Additional subgroup analyses focused on nutritional intake based on the type of milk feeding (breastfed vs. formula-fed, breastfed vs. mixed-fed). Mixed feeding is defined as the consumption of both breastmilk and infant formula. For both subgroup analyses, either a Student’s t-test or the Mann–Whitney U test was used. Correlations between siblings of multiple births were not considered for subgroup analyses due to the smaller subgroup sample sizes.
Marginal means and means (subgroups), accompanied by corresponding standard errors (SE), were computed, with p-values used to evaluate the null hypothesis of no between-(sub)group differences. Graphical depictions illustrated estimated marginal means and standard errors through error bars, with significance set at p-values < 0.05. An additional analytical approach involved adjusting p-values for comparisons between (sub)groups for the same nutrient at distinct timepoints using the Bonferroni-Holm method (p-adj). All statistical analyses were performed using R version 4.1.1 (R Core Team, 2022).
4. Discussion
This secondary outcome analysis of a prospective observational study investigated critical micronutrient intake during the first year of life, comparing an early and late introduction of solids in VLBW infants. To our knowledge, this was the first trial reporting data on micronutrient intake patterns during complementary feeding in a representative VLBW cohort including those with preterm-birth-related comorbidities.
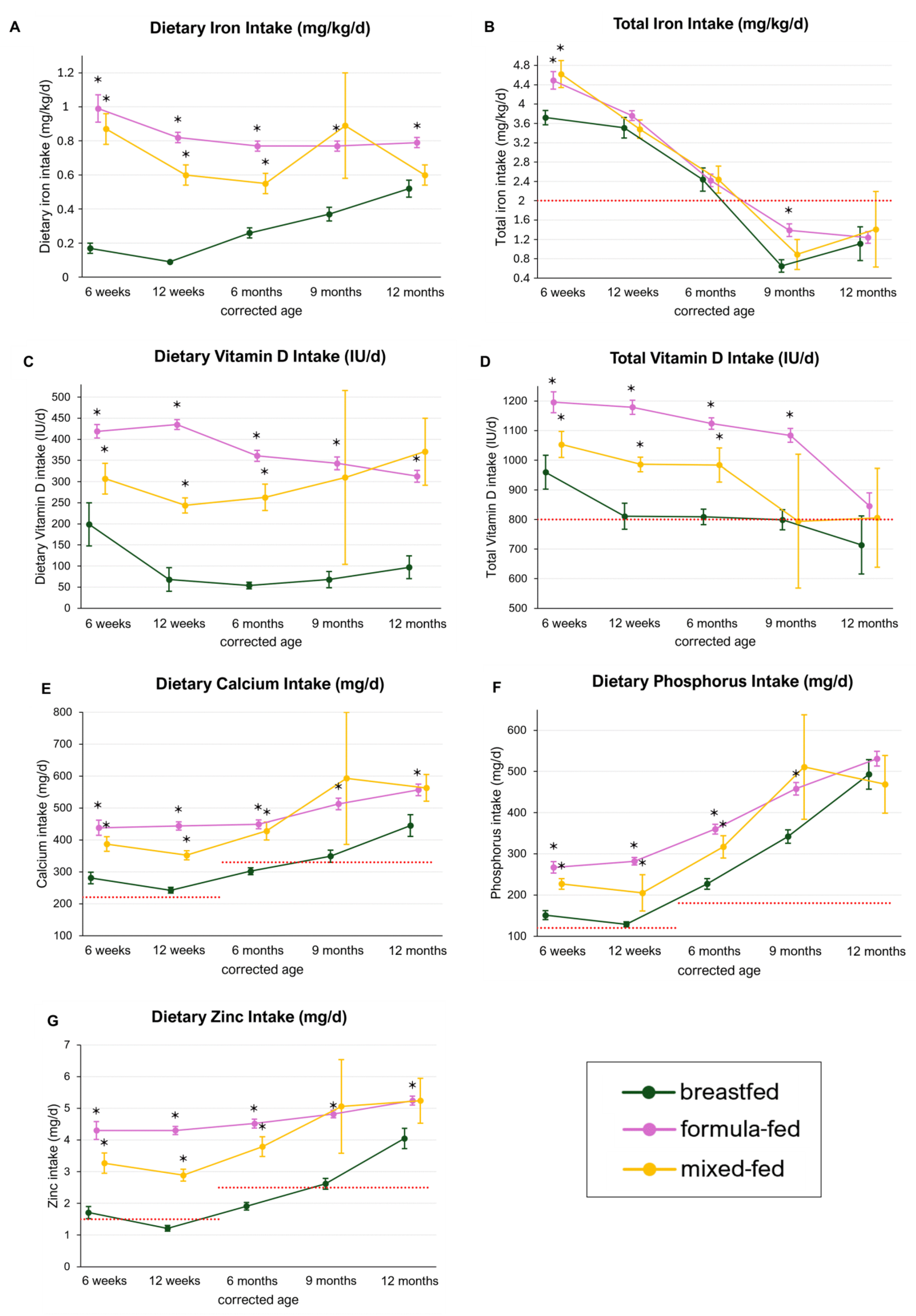
Overall, the timepoint of the introduction of solids did not have an impact on mean dietary iron intake, except for a higher iron and phosphorus intake at 6 months CA in the early group. Mean total iron intakes were adequate until 6 months CA; however, recommendations were not met during the second half year CA in both groups. Total vitamin D intakes met current intake recommendations in VLBW infants during the first year of life. Mean intakes of calcium, zinc, and phosphorus were slightly higher in the early group but were shown to be sufficient in both complementary feeding groups when compared with term infant recommendations. This study further revealed that micronutrient intakes were similar between infants with and without comorbidities. However, breastfed infants had significantly lower intakes of most micronutrients compared with formula- and mixed-fed infants.
4.1. Dietary and Total Iron Intake
This study demonstrated that infants introduced to solids early had similar mean dietary iron intakes compared with those introduced later, except for a higher intake observed at 6 months CA. Marriot et al. reported significantly higher iron intakes (9.2 vs. 6.7 mg/d) at 12 months CA in preterm infants that were introduced to solids early (early: 13 weeks uncorrected age, late: 17 weeks uncorrected age). Parents of infants that were in the early introduction group were specifically advised to provide foods that are rich sources of iron [
8]. However, this study seems to be no longer applicable, as it was conducted at a time when post-discharge formula was not available. Similarly, Kattelman et al. found that an early introduction of solids led to higher dietary iron intakes (16.2 vs. 13.2 mg/day), partly due to the introduction of iron-fortified cereals as the initial solid food [
17]. In contrast, a randomized intervention trial comparing early (10–12 weeks CA) versus late (16–18 weeks CA) introduction of solids in VLBW infants using a standardized step-up complementary feeding approach found similar iron intakes between both groups throughout the first year of life [
10].
In our study, breastfed infants had a significantly lower mean dietary iron intake compared with formula-fed infants (0.26 vs. 0.77 mg/kg/d; p < 0.001). Thus, we believe that the higher intake observed in the early introduction group at 6 months CA in our study most likely resulted from higher intakes in formula-fed infants and lower breastfeeding rates in the early introduction group.
Iron intake levels remained consistently low, with a maximum mean intake of 0.75 mg/kg/day. Notably, dietary iron intake showed only minimal increases throughout the observation period, even when meat meals and iron-rich solids were regularly included. Additionally, absolute dietary iron intakes (mg/day) did not exceed 6.3 mg/day, falling short of the recommended intake of 11 mg/day for term infants aged 4 to 12 months CA during the observation period [
15]. Accordingly, introducing meat or iron-rich foods did not significantly enhance iron intake and may not sufficiently replace supplementation.
Iron deficiency can have long-lasting effects on neurodevelopment. Studies show that iron deficiency during infancy is associated with cognitive impairment, attention deficits, lower educational performance, and poorer emotional health during adulthood, highlighting the critical need for adequate iron intake to support healthy development [
18,
19].
The ESPGHAN recommends iron supplementation of 2–3 mg/kg/day until 6–12 months, depending on the infant’s diet [
5]. Our data indicated that iron supplementation was appropriate until 6 months CA. However, it significantly decreased afterwards, falling short of the recommendations during the second half of the first year CA. Given that the dietary iron intake (mg/kg/d) did not sufficiently increase at the time when supplementation decreased, we suggest that iron supplementation intake may be prolonged. Special attention should be drawn to breastfed infants, as total iron intakes were significantly lower at 9 months CA compared with formula-fed infants, with levels decreasing to 0.65 mg/kg/d. The data presented in this study suggest that current clinical guidelines for iron supplementation may require revision. First, the discontinuation of iron supplementation should be guided by monitoring iron status rather than solely by the introduction of regular meat and iron-rich meals. Additionally, iron supplementation guidelines may need to be tailored specifically for breastfed and formula-fed infants to ensure appropriate management of iron status in each group.
This study further included infants with preterm-birth-related comorbidities such as BPD, NEC, or IVH. Chronic stress, inflammation, heightened respiratory effort, and lung damage may increase nutrient demands in infants with BPD [
20,
21]. We found similar dietary and total iron intakes in infants with and without BPD. However, it remains unclear whether this is sufficient to cover the needs of infants with BPD. Karatza et al. suggests that infants with BPD require iron intakes of 4 mg/kg/day until 12 months of age [
22]. Our study indicated that these values were not met beyond 6 weeks CA in infants with BPD, suggesting that those infants were at a high risk of iron deficiency. Unfortunately, this study did not investigate iron status; thus, we are unaware whether iron deficiency was more prevalent in infants with BPD. Furthermore, infants with NEC may be at risk for malabsorption and limited nutrient intake, necessitating higher nutritional intakes in the long term [
23]. We observed similar dietary iron intakes but higher total iron intakes in infants with NEC compared with those without, likely due to increased supplementation. Data on iron requirements for VLBW infants with NEC during complementary feeding are lacking, making it difficult to assess iron intake adequacy. Thus, studies are needed to investigate iron requirements in infants with comorbidities during the first year of life.
In general, iron intake of VLBW infants can be further optimized, particularly during the later stages of complementary feeding. This can be achieved through prolonged iron supplementation, nutritional guidance, and educating parents about iron-rich dietary sources. Previous studies have shown that iron-fortified cereals effectively increase iron intake and reduce the risk of iron deficiency [
24,
25]. Introducing iron-fortified cereals as one of the first solids may improve iron status, especially in at-risk infants.
4.2. Dietary and Total Vitamin D Intake
We found no significant difference in mean dietary vitamin D intake between the early and late feeding groups. Mean vitamin D intakes were consistently low, ranging between 255 and 328 IU/day. It is widely acknowledged that dietary sources alone are insufficient to meet vitamin D requirements [
26]. While vitamin D can be synthesized through sun exposure, infants need protection from sunlight, making them reliant on enteral vitamin D supply [
27]. Therefore, the ESPGHAN recommends vitamin D supplementation of 800–1000 IU/day until 12 months of age in VLBW infants [
16].
Total vitamin D intake was similar among both groups, and ESPGHAN recommendations were met until 9 months CA in the early group and throughout the observation period in the late group. However, our study indicated that vitamin D supplementation decreased before reaching 12 months CA in both groups. Advocating for continued vitamin D supplementation until 12 months CA could enhance vitamin D status and reduce the risk of deficiency. This is especially important because previous studies have shown a high prevalence of deficiency in VLBW infants at 12 months CA (81–89%). [
28] Therefore, as emphasized by Thanhaeuser et al., current recommendations for vitamin D supplementation in preterm infants may need to be revised, and regular monitoring of vitamin D status to tailor supplementation individually would be beneficial in preventing and treating low vitamin D levels [
28].
Dietary and total vitamin D intakes were similar in infants with BPD, NEC, and IVH compared with those without these comorbidities. However, infants with NEC (740 IU/d) or IVH (719 IU/d) fell short of recommendations at 12 months CA.
Low vitamin D levels have been shown to increase the risk of NEC in preterm infants [
29]. Therefore, infants diagnosed with NEC may already have lower baseline vitamin D levels. Furthermore, malabsorption of vitamin D may occur in infants with NEC, especially in those who have undergone bowel resection, thereby heightening nutritional requirements. The severity of NEC and associated gastrointestinal complications can further impair the absorption and utilization of vitamin D, putting these infants at high risk of vitamin D deficiency [
30]. Thus, ensuring adequate vitamin D supplementation until at least 12 months CA or even longer is particularly crucial. However, further studies are warranted to define vitamin D requirements in infants with varying severity grades of NEC over the long term.
Additionally, a special focus should be given to breastfed infants, as mean total vitamin D intakes were at the borderline of meeting recommendations from 12 weeks CA onwards (714–811 IU/d). Breastmilk contains only a little vitamin D, and the nutritional supply from solids is minimal. Við Streym and colleagues have shown that breastfed term infants receive less than 20% of the daily recommended vitamin D intake from breastmilk [
31]. As the vitamin D requirements of preterm infants are higher, the proportional amount that can be covered from supplied breastmilk is even lower [
28]. Thus, vitamin D supplementation in these infants should be promoted, and parents should be educated on the importance of compliance with vitamin D supplementation until 12 months CA. Regular monitoring in high-risk patients offers individually tailored supplementation and the prevention of abnormal bone health. Current vitamin D guidelines do not differentiate between breastfed and formula-fed infants. However, the data presented in this study suggest that such distinctions may be necessary to optimize vitamin D intake, particularly for breastfed infants.
4.3. Dietary Calcium and Phosphorus Intake
Appropriate levels of calcium and phosphorus are crucial for optimal bone health. Insufficient intake of these minerals can lead to inadequate osteoid mineralization and reduced bone mineral content, potentially resulting in rickets, especially in premature infants [
32]. Thus, both calcium and phosphorus are crucial in preventing metabolic bone disease, highlighting the need for adequate dietary intakes [
33].
Our study showed that the timepoint of solid food introduction did not affect calcium intake. Additionally, both groups met the recommended dietary calcium intake for term infants (calcium: 0–3 months: 220 mg/day; 4–12 months: 330 mg/day) at all investigated timepoints [
15]. This is in line with other studies that reported similar calcium intakes from 3 to 12 months CA (342–520 mg/d), exceeding current intake recommendations [
10,
28]. Moreover, phosphorus intake was similar between the early and late introduction groups, except for 6 months CA, where the early group had significantly higher intakes (
p = 0.01). Formula-fed infants had significantly higher phosphorus intakes until 9 months CA compared with breastfed infants. Consequently, the higher phosphorus intake in the early group potentially resulted from the higher intake and the increased prevalence of formula-fed infants in the early group. Despite these differences, phosphorus intakes met the guidelines for term infants (0–3 months: 120 mg/day; 4–12 months: 180 mg/day) throughout the study in both groups [
15]. However, it remains to be determined if the recommendations for term infants can be directly applied to preterm infants, particularly those with long-term health conditions.
Infants with BPD and IVH had similar calcium and phosphorus intakes compared with those without these conditions, but those with NEC had a significantly lower phosphorus intake at 12 months CA compared with infants without comorbidities. This study did not evaluate bone health; hence, we are unable to conclude whether the observed intakes are adequate for infants with critical illness. Randomized controlled trials are essential to determine adequate dietary calcium and phosphorus intakes during this critical period for infants with comorbidities.
We found that breastfed infants had significantly lower calcium and phosphorus intakes throughout the observation period compared with formula-fed infants. Additionally, breastfed infants did not meet calcium intake recommendations at 6 months CA (227 ± 13 mg/d). Inadequate calcium intake can result in stunted growth and decreased bone mineral content [
34]. To decrease the risk of calcium deficiency, solids high in bioavailable calcium, such as dairy products, beans, broccoli, and spinach, should be offered [
35].
4.4. Dietary Zinc Intake
Zinc plays a crucial role as a trace element, impacting growth, tissue differentiation, and immune function [
36]. However, preterm infants face an increased risk of zinc deficiency due to their low body stores at birth [
37].
Our study found that an early introduction of solid foods resulted in marginally higher dietary zinc intake at both 6 weeks and 6 months CA compared with late introduction. While this hints at a potential increase in zinc intake through early solid food introduction, a recent randomized trial in VLBW infants did not definitively show the benefits of early introduction in improving zinc intake [
10]. The higher zinc intake in the early introduction group in our study may stem from an earlier transition to zinc-rich foods like meats and fish [
38] or from lower zinc intakes in breastfed infants and the higher breastfeeding rate in the late group (breastfed: 1.21–4.05 mg/d; formula-fed: 4.3–5.24 mg/d).
The recorded zinc intakes align with previous studies, but specific recommendations for VLBW infants during complementary feeding are lacking [
10,
17]. Comparing our results with term infant recommendations, set at 1.5 mg/day for ages 0–3 months and 2.5 mg/day for ages 4–12 months, both groups met the recommended intake levels for term infants at all investigated timepoints [
15]. However, it remains uncertain if these intakes suffice during the complementary feeding period, especially in preterm infants with comorbidities that may affect nutrient intake and absorption or who require higher needs due to long-term disease burden. This gap persists, as we did not assess zinc status, and other trials on VLBW infants are lacking. Despite this, advocating for zinc-rich solid foods is presumed to be beneficial for preterm infants [
1]. In particular, this applies to exclusively breastfed infants, considering that zinc intake recommendations were not met at 6 months CA in breastfed infants as well as the declining zinc content in human milk postpartum [
39].
Future studies are crucial to ascertain if zinc intake recommendations for term infants apply to VLBW infants or if this population requires specific guidelines or supplementation.
4.5. Strength and Limitation
This secondary analysis of a prospective observational trial yields significant insights into complementary feeding practices among preterm infants, offering valuable perspectives on their micronutrient intakes during the critical first year of life. The inclusion of a diverse cohort of VLBW infants with comorbidities enhances the generalizability of the findings. Nevertheless, the study’s reliance on average breastmilk intake data constitutes a notable limitation. Additionally, the trial was not powered to detect significant differences in nutritional intake between the study groups. The number of infants in the subgroups (type of feeding, comorbidities) was limited; therefore, these results should be interpreted cautiously. Furthermore, the observational design of the study, while reducing its quality in terms of causal inference, facilitates the provision of valuable information on current nutrient intakes in a representative population of Austrian VLBW infants.
5. Conclusions
In conclusion, this observational study indicates that the timing of solid introduction was not associated with micronutrient intakes during the first year of life. Dietary intakes of zinc, calcium, and phosphorus were adequate. However, dietary intakes of iron were insufficient to equal the iron quantity from supplements; hence, prolonged iron supplementation may be necessary beyond the introduction of meat and iron-rich solids. A decrease in total vitamin D intake by the end of the first year CA calls for improved adherence to vitamin D supplementation until 12 months CA. Although micronutrient levels were similar between infants with and without NEC, BPD, or IVH, it remains to be determined whether current dietary intakes are adequate for these infants. This underscores the need for future research to establish specific micronutrient requirements for these subgroups. Additionally, special attention should be given to breastfed infants, as they are at the highest risk for micronutrient deficiencies

 ,
, 





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}