
Moderate and Severe Congenital Heart Diseases Adversely Affect the Growth of Children in Italy: A Retrospective Monocentric Study

 , ,
, ,
Abstract
1. Introduction
2. Materials and Methods
Statistical Analysis
3. Results
4. Discussion
5. Conclusions
6. Study Limitations
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Okoromah, C.A.N.; Ekure, E.N.; Lesi, F.E.A.; Okunowo, W.O.; Tijani, B.O.; Okeiyi, J.C. Prevalence, profile and predictors of malnutrition in children with congenital heart defects: A case-control observational study. Arch. Dis. Child. 2011, 96, 354–360. [Google Scholar] [CrossRef] [PubMed]
- Mitchell, I.M.; Logan, R.W.; Pollock, J.C.; Jamieson, M.P. Nutritional status of children with congenital heart disease. Heart 1995, 73, 277–283. [Google Scholar] [CrossRef]
- Varan, B.; Tokel, K.; Yilmaz, G. Malnutrition and growth failure in cyanotic and acyanotic congenital heart disease with and without pulmonary hypertension. Arch. Dis. Child. 1999, 81, 49–52. [Google Scholar] [CrossRef] [PubMed]
- Medoff-Cooper, B.; Ravishankar, C. Nutrition and growth in congenital heart disease: A challenge in children. Curr. Opin. Cardiol. 2013, 28, 122–129. [Google Scholar] [CrossRef] [PubMed]
- Roman, B. Nourishing Little Hearts: Nutritional Implications for Congenital Heart Defects. Pract. Gastroenterol. 2011, 8, 11–32. [Google Scholar]
- Soliman, A.T.; Madkour, A.; Galil, M.A.; El Zalabany, M.; Aziz, S.M.; Ansari, B.M. Growth Parameters and Endocrine Function in Relation to Echocardiographic Parameters in Children with Ventricular Septal Defect without Heart Failure. J. Trop. Pediatr. 2001, 47, 146–152. [Google Scholar] [CrossRef] [PubMed]
- Polat, S.; Okuyaz, C.; Hallioglu, O.; Mert, E.; Makharoblidze, K.; Hallioglu, O. Evaluation of growth and neurodevelopment in children with congenital heart disease. Pediatr. Int. 2011, 53, 345–349. [Google Scholar] [CrossRef]
- Krieger, I. Growth failure and congenital heart disease. Energy and nitrogen balance in infants. Am. J. Dis. Child. 1970, 120, 497–502. [Google Scholar] [CrossRef]
- Maurer, I.; Latal, B.; Geissmann, H.; Knirsch, W.; Bauersfeld, U.; Balmer, C. Prevalence and predictors of later feeding disorders in children who underwent neonatal cardiac surgery for congenital heart disease. Cardiol. Young 2011, 21, 303–309. [Google Scholar] [CrossRef]
- Ibrahim, M.K.; Zambruni, M.; Melby, C.L.; Melby, P.C. Impact of Childhood Malnutrition on Host Defense and Infection. Clin. Microbiol. Rev. 2017, 30, 919–971. [Google Scholar] [CrossRef]
- Gale, C.R.; O’Callaghan, F.J.; Bredow, M.; Martyn, C.N. Avon Longitudinal Study of Parents and Children Study Team. The influence of head growth in fetal life, infancy, and childhood on intelligence at the ages of 4 and 8 years. Pediatrics 2006, 118, 1486–1492. [Google Scholar] [CrossRef] [PubMed]
- Latal, B. Neurodevelopmental Outcomes of the Child with Congenital Heart Disease. Clin. Perinatol. 2016, 43, 173–185. [Google Scholar] [CrossRef] [PubMed]
- Heye, K.N.; Rousson, V.; Knirsch, W.; Beck, I.; Liamlahi, R.; Bernet, V.; Dave, H.; Latal, B. Growth and Intellectual Abilities of Six-Year-Old Children with Congenital Heart Disease. J. Pediatr. 2019, 204, 24–30.e10. [Google Scholar] [CrossRef] [PubMed]
- Batte, A.; Lwabi, P.; Lubega, S.; Kiguli, S.; Otwombe, K.; Chimoyi, L.; Nabatte, V.; Karamagi, C. Wasting, underweight and stunting among children with congenital heart disease presenting at Mulago hospital, Uganda. BMC Pediatr. 2017, 17, 10. [Google Scholar] [CrossRef] [PubMed]
- Vaidyanathan, B.; Nair, S.B.; Sundaram, K.R.; Babu, U.K.; Shivaprakasha, K.; Rao, S.G.; Kumar, R.K. Malnutrition in children with congenital heart disease (CHD) determinants and short term impact of corrective intervention. Indian Pediatr. 2008, 45, 6. [Google Scholar]
- Chinawa, A.T.; Chinawa, J.M.; Duru, C.O.; Chukwu, B.F.; Obumneme-Anyim, I. Assessment of Nutritional Status of Children With Congenital Heart Disease: A Comparative Study. Front. Nutr. 2021, 8, 644030. [Google Scholar] [CrossRef] [PubMed]
- Monteiro, F.P.M.; De Araujo, T.L.; Lopes, M.; Chaves, D.B.R.; Beltrão, B.A.; Costa, A.G.D.S. Nutritional status of children with congenital heart disease. Rev. Lat.-Am. Enferm. 2012, 20, 1024–1032. [Google Scholar] [CrossRef][Green Version]
- Woldesenbet, R.; Murugan, R.; Mulugeta, F.; Moges, T. Nutritional status and associated factors among children with congenital heart disease in selected governmental hospitals and cardiac center, Addis Ababa Ethiopia. BMC Pediatr. 2021, 21, 538. [Google Scholar] [CrossRef]
- Weintraub, R.G.; Menahem, S. Early surgical closure of a large ventricular septal defect: Influence on long-term growth. J. Am. Coll. Cardiol. 1991, 18, 552–558. [Google Scholar] [CrossRef]
- Levy, R.J.; Rosenthal, A.; Miettinen, O.S.; Nadas, A.S. Determinants of growth in patients with ventricular septal defect. Circulation 1978, 57, 793–797. [Google Scholar] [CrossRef]
- Williams, R.V.; Zak, V.; Ravishankar, C.; Altmann, K.; Anderson, J.; Atz, A.M.; Dunbar-Masterson, C.; Ghanayem, N.; Lambert, L.; Lurito, K.; et al. Factors Affecting Growth in Infants with Single Ventricle Physiology: A Report from the Pediatric Heart Network Infant Single Ventricle Trial. J. Pediatr. 2011, 159, 1017–1022.e2. [Google Scholar] [CrossRef]
- Hapuoja, L.; Kretschmar, O.; Rousson, V.; Dave, H.; Naef, N.; Latal, B. Somatic growth in children with congenital heart disease at 10 years of age: Risk factors and longitudinal growth. Early Hum. Dev. 2021, 156, 105349. [Google Scholar] [CrossRef] [PubMed]
- Burch, P.T.; Ravishankar, C.; Newburger, J.W.; Lambert, L.M.; Pemberton, V.L.; Granger, S.; Floh, A.A.; Anderson, J.B.; Hill, G.D.; Hill, K.D.; et al. Assessment of Growth 6 Years after the Norwood Procedure. J. Pediatr. 2016, 180, 270–274.e6. [Google Scholar] [CrossRef]
- Schuurmans, F.M.; Pulles-Heintzberger, C.F.; Gerver, W.J.; Kester, A.D.; Forget, P.P. Long-term growth of children with congenital heart disease: A retrospective study. Acta Paediatr. 1998, 87, 1250–1255. [Google Scholar] [CrossRef] [PubMed]
- Rhee, E.K.; Evangelista, J.K.; Nigrin, D.J.; Erickson, L.C. Impact of anatomic closure on somatic growth among small, asymptomatic children with secundum atrial septal defect. Am. J. Cardiol. 2000, 85, 1472–1475. [Google Scholar] [CrossRef] [PubMed]
- Schwartz, S.; Olsen, M.; Woo, J.; Madsen, N. Congenital heart disease and the prevalence of underweight and obesity from age 1 to 15 years: Data on a nationwide sample of children. BMJ Paediatr. Open 2017, 1, e000127. [Google Scholar] [CrossRef]
- Steele, J.M.; Preminger, T.J.; Erenberg, F.G.; Wang, L.; Dell, K.; Alsaied, T.; Zahka, K.G. Obesity trends in children, adolescents, and young adults with congenital heart disease. Congenit. Heart Dis. 2019, 14, 517–524. [Google Scholar] [CrossRef]
- Babaoğlu, K.; Deveci, M.; Kayabey, Ö.; Altun, G.; Binnetoğlu, K. Prevalence of overweight and obesity among patients with congenital and acquired heart disease in Kocaeli, Turkey. Cardiol. Young 2015, 25, 533–538. [Google Scholar] [CrossRef]
- Tamayo, C.; Manlhiot, C.; Patterson, K.; Lalani, S.; McCrindle, B.W. Longitudinal Evaluation of the Prevalence of Overweight/Obesity in Children With Congenital Heart Disease. Can. J. Cardiol. 2015, 31, 117–123. [Google Scholar] [CrossRef]
- Welisch, E.; Rauch, R.; Seabrook, J.A.; Filler, G.; Norozi, K. Are the children and adolescents with congenital heart disease living in Southwestern Ontario really overweight and obese? Cardiol. Young 2014, 24, 848–853. [Google Scholar] [CrossRef]
- Shustak, R.J.; McGuire, S.B.; October, T.W.; Phoon, C.K.L.; Chun, A.J.L. Prevalence of Obesity among Patients with Congenital and Acquired Heart Disease. Pediatr. Cardiol. 2011, 33, 8–14. [Google Scholar] [CrossRef] [PubMed]
- Chen, C.-A.; Wang, J.-K.; Lue, H.-C.; Hua, Y.-C.; Chang, M.-H.; Wu, M.-H. A Shift from Underweight to Overweight and Obesity in Asian Children and Adolescents with Congenital Heart Disease. Paediatr. Périnat. Epidemiol. 2012, 26, 336–343. [Google Scholar] [CrossRef] [PubMed]
- Pasquali, S.K.; Marino, B.S.; Pudusseri, A.; Wernovsky, G.; Paridon, S.M.; Walker, S.A.; Cohen, M.S. Risk factors and comorbidities associated with obesity in children and adolescents after the arterial switch operation and Ross procedure. Am. Heart J. 2009, 158, 473–479. [Google Scholar] [CrossRef] [PubMed]
- Pinto, N.M.; Marino, B.S.; Wernovsky, G.; de Ferranti, S.D.; Walsh, A.Z.; Laronde, M.; Hyland, K.; Dunn, S.O.; Cohen, M.S. Obesity Is a Common Comorbidity in Children With Congenital and Acquired Heart Disease. Pediatrics 2007, 120, e1157–e1164. [Google Scholar] [CrossRef]
- Cacciari, E.; Milani, S.; Balsamo, A.; Spada, E.; Bona, G.; Cavallo, L.; Cerutti, F.; Gargantini, L.; Greggio, N.; Tonini, G.; et al. Italian cross-sectional growth charts for height, weight and BMI (2 to 20 yr). J. Endocrinol. Investig. 2006, 29, 581–593. [Google Scholar] [CrossRef]
- Baumgartner, H.; De Backer, J.; Babu-Narayan, S.V.; Budts, W.; Chessa, M.; Diller, G.P.; Lung, B.; Kluin, J.; Lang, I.M.; Meijboom, F.; et al. 2020 ESC Guidelines for the management of adult congenital heart disease. Eur. Heart J. 2021, 42, 563–645. [Google Scholar] [CrossRef]
- Weinberg, S.; Kern, J.; Weiss, K.; Ross, G. Developmental Screening of Children Diagnosed with Congenital Heart Defects. Clin. Pediatr. 2001, 40, 497–501. [Google Scholar] [CrossRef]
- De Staebel, O. Malnutrition in Belgian children with congenital heart disease on admission to hospital. J. Clin. Nurs. 2000, 9, 784–791. [Google Scholar] [CrossRef]
- Tefuarani, N.; Hawker, R.; Vince, J.; Sleigh, A.; Williams, G.M. Surgical programme at Royal Alexandra Hospital, Sydney, for Papua New Guinea children with congenital heart disease, 1978–1994. J. Paediatr. Child Health 2002, 38, 178–182. [Google Scholar] [CrossRef]
- Daymont, C.; Neal, A.; Prosnitz, A.; Cohen, M.S. Growth in Children With Congenital Heart Disease. Pediatrics 2013, 131, e236–e242. [Google Scholar] [CrossRef]
- Oyarzún, I.; Claveria, C.; Larios, G.; Le Roy, C. Nutritional recovery after cardiac surgery in children with congenital heart disease. Rev. Chil. Pediatr. 2018, 89, 24–31. [Google Scholar] [CrossRef] [PubMed]
- Dündar, B.; Saylam, A.A.G.; Ünal, N.; Meşe, Τ.; Hüdaoğlu, S.; Büyükgebiz, Β.; Böber, Ε.; Büyükgebiz, A. Chronic Hypoxemia Leads to Reduced Serum IGF-I Levels in Cyanotic Congenital Heart Disease. J. Pediatr. Endocrinol. Metab. 2000, 13, 431–436. [Google Scholar] [CrossRef] [PubMed]
- Simon, D. Puberty in Chronically Diseased Patients. Horm. Res. Paediatr. 2002, 57, 53–56. [Google Scholar] [CrossRef] [PubMed]
- GHO|By Category|Children Aged < 5 Years Wasted, Country Survey Results—Data by Country. WHO. World Health Organization. Available online: https://apps.who.int/gho/data/view.main.CHILDWASTEDv (accessed on 26 June 2022).
- Stunting Prevalence among Children under 5 Years of Age (% Height-for-Age < −2 SD) (JME Country). Available online: https://www.who.int/data/gho/data/indicators/indicator-details/GHO/gho-jme-country-children-aged-5-years-stunted-(-height-for-age--2-sd) (accessed on 26 June 2022).
- Underweight Prevalence among Children under 5 Years of Age (% Weight-for-Age < −2 SD) (JME Country). Available online: https://www.who.int/data/gho/data/themes/topics/indicator-groups/indicator-group-details/GHO/prevalence-of-malnutrition-in-children (accessed on 26 June 2022).
- Country Nutrition Profiles. Available online: https://globalnutritionreport.org/resources/nutrition-profiles/europe/southern-europe/italy/ (accessed on 26 June 2022).
- Majnemer, A.; Limperopoulos, C.; Shevell, M.; Rohlicek, C.; Rosenblatt, B.; Tchervenkov, C. Health and well-being of children with congenital cardiac malformations, and their families, following open-heart surgery. Cardiol. Young 2006, 16, 157–164. [Google Scholar] [CrossRef]
- Cheuk, D.; Wong, S.M.Y.; Choi, Y.P.; Chau, A.K.T.; Cheung, Y.F. Parents’ understanding of their child’s congenital heart disease. Heart 2004, 90, 435–439. [Google Scholar] [CrossRef]
- Kaden, G.G.; McCarter, R.J.; Johnson, S.F.; Ferencz, C. Physician-patient communication. Understanding congenital heart disease. Am. J. Dis. Child. 1985, 139, 995–999. [Google Scholar] [CrossRef]
- Velázquez-López, L.; Santiago-Díaz, G.; Nava-Hernández, J.; Muñoz-Torres, A.V.; Medina-Bravo, P.; Torres-Tamayo, M. Mediterranean-style diet reduces metabolic syndrome components in obese children and adolescents with obesity. BMC Pediatr. 2014, 14, 175. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| *CHD | Absent (n = 91) | Mild (n = 255) | Moderate (n = 223) | Severe (n = 88) | Tot (n = 657) | p-Value |
|---|---|---|---|---|---|---|
| ∆HZ, mean ± SD | 0.62 ± 1.2 | 0.38 ± 1.37 | 0.04 ± 1.39 ** | −0.29 ± 1.48 ** | 0.21 ± 1.39 | <0.001 |
| °WZ, mean ± SD | 0.37 ± 1.01 | 0.16 ± 1.23 | −0.09 ± 1.30 ** | −0.67 ± 1.41 ** | −0.01 ± 1.29 | <0.001 |
| ¥BMIZ, mean ± SD (≥2 Ys) | −0.07 ± 1.13 | −0.03 ± 1.24 | −0.16 ± 1.29 | −0.65 ± 1.3 ** | −0.19 ± 1.42 | 0.004 |
| §WHZ, mean ± SD | 0.43 ± 1.07 | 0.02 ± 1.45 | 0.01 ± 0.1.42 ** | −0.40 ± 1.71 | 0.04 ± 1.4 | 0.009 |
| ∆HZ < −2 SD, N (%) | 1 (1.1%) | 8 (3.1%) | 20 (8.9%) ** | 9 (12.3%) ** | 38 (5.8%) | 0.003 |
| °WZ < −2 SD, N (%) | 0 (0%) | 8 (3.1%) | 16 (7.1%) | 15 (17%) ** | 39 (5.9%) | <0.001 |
| ¥BMIZ < −2 SD, N (%) (≥2 Ys) | 2 (2.2%) | 8 (3.8%) | 8 (4.9%) | 11 (15.7%) ** | 29 (4.4%) | 0.001 |
| §WHZ < −2 SD, N (%) (<2 Ys) | 0 (0%) | 4 (8.8%) | 7 (11.9%) | 4 (22.2%) | 15 (10.1%) | 0.107 |
| ∆HZ > 2 SD, N (%) | 12 (13%) | 35 (13.7%) | 11 (4.9%) ** | 2 (2.3%) ** | 60 (9.1%) | <0.001 |
| °WZ > 2 SD, N (%) | 6 (6%) | 16 (6.3%) | 12 (5.4%) | 3 (3.4%) | 37 (5.6%) | 0.757 |
| ¥BMIZ > 2 SD, N (%) (≥2 Ys) | 0 (0%) | 6 (2.8%) | 6 (3.6%) | 0 (0%) | 12 (2.3%) | 0.193 |
| §WHZ > 3 SD, N (%) (<2 Ys) | 0 (0%) | 1 (2.2%) | 0 (0%) | 0 (0%) | 1 (0.6%) | 0.512 |
| *CHD | Absent (n = 91) | CHD (n = 566) | p-Value | |
|---|---|---|---|---|
| ∆HZ, mean ± SD | <2 years (n = 148) | 0.22 ± 1.39 | −0.42 ± 1.82 | 0.0926 |
| 2–5 years (n = 61) | 1.08 ± 0.88 | 0.37 ± 1.12 | 0.0194 | |
| ≥5–18 years (n = 448) | 0.66 ± 1.16 | 0.29 ± 1.25 | 0.0502 | |
| °WZ, mean ± SD | <2 years (n = 148) | 0.03 ± 1.05 | −0.42 ± 1.54 | 0.0201 |
| 2–5 years (n = 61) | 0.49 ± 1.12 | −0.16 ± 1.21 | 0.0499 | |
| ≥5–18 years (n = 448) | 0.23 ± 1.18 | 0.04 ± 1.23 | 0.3360 | |
| §WHZ, mean ± SD | <2 years (n = 148) | 0.43 ± 1.07 | −0.05 ± 1.47 | 0.1187 |
| ¥BMIZ, mean ± SD | 2–5 years (n = 61) | −0.34 ± 1.32 | −0.43 ± 1.09 | 0.7746 |
| ≥5–18 years (n = 448) | −0.27 ± 2.37 | −0.15 ± 1.30 | 0.5845 |
| *CHD | Age Groups | Absent (n = 91) | Mild (n = 255) | Moderate (n = 223) | Severe (n = 88) | p-Value | p-Value Bonferroni Analysis |
|---|---|---|---|---|---|---|---|
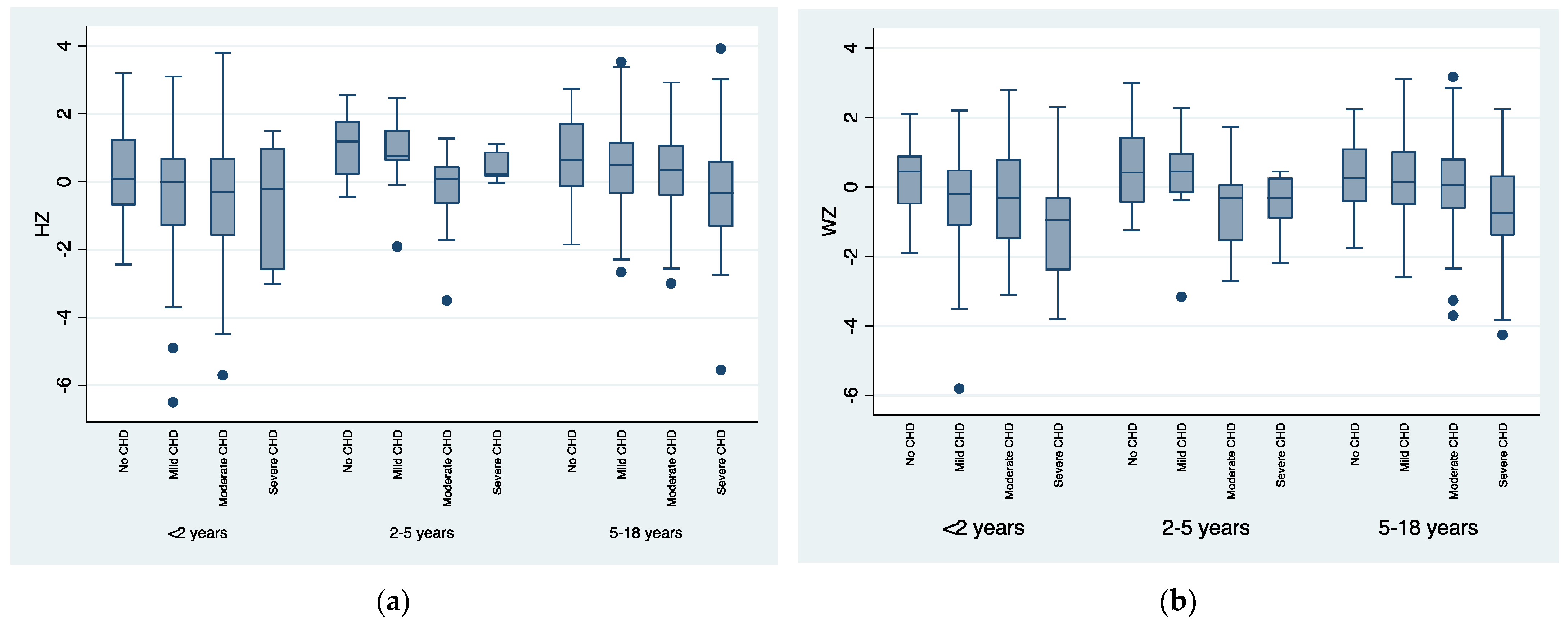
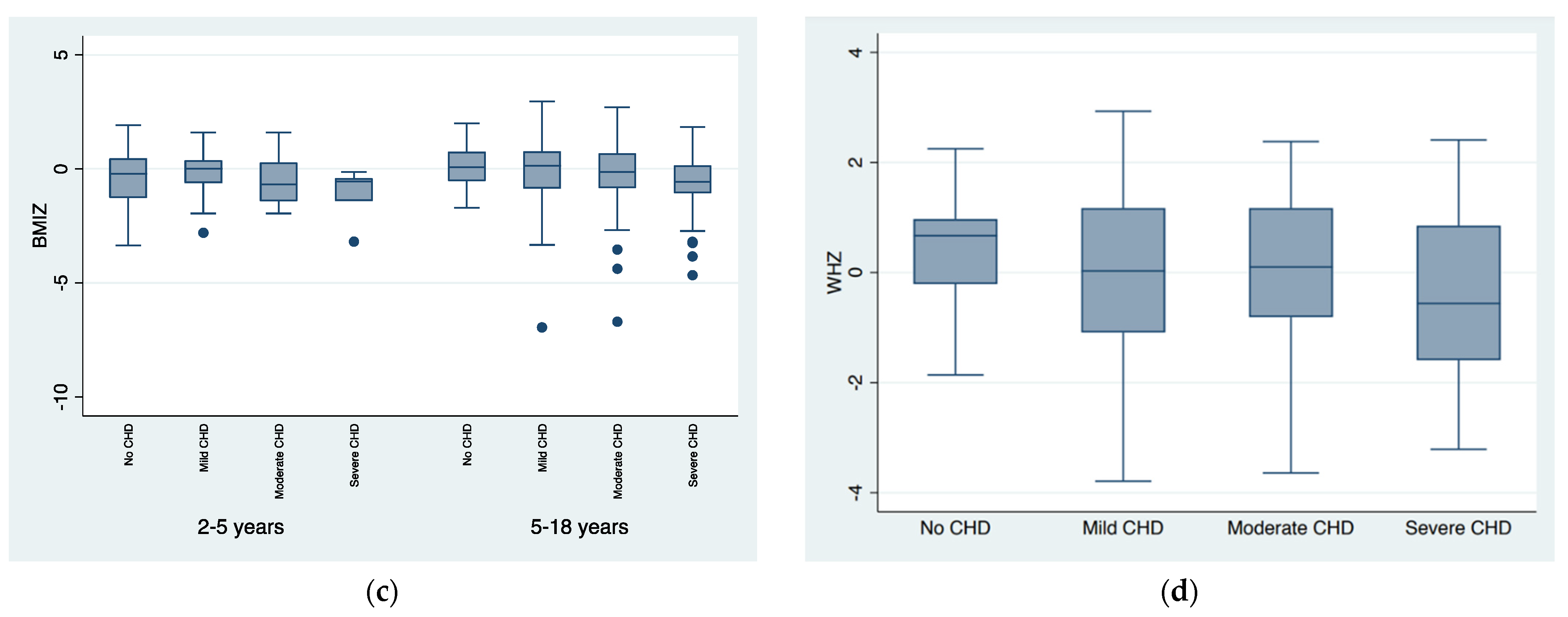
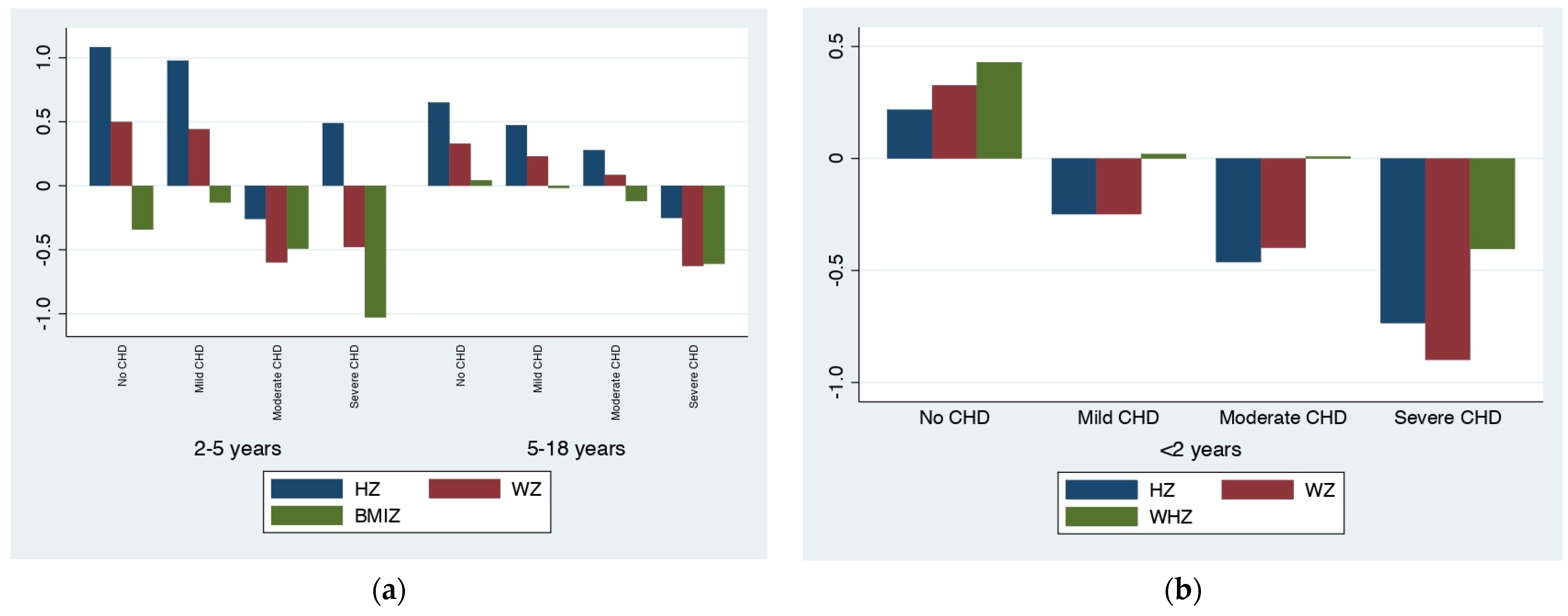
| ∆HZ, mean ± SD | ≤2 years (n = 148) | 0.22 ± 1.39 | −0.25 ± 1.91 | −0.46 ± 1.81 | −0.74 ± 1.67 | 0.279 | |
| 2–5 years (n = 61) | 1.08 ± 0.88 | 0.97 ± 1.06 | −0.26 ± 1.13 | 0.48 ± 0.45 | 0.0005 | Moderate vs. Mild or Absent 0.001 and 0.003 | |
| >5 years (n = 448) | 0.65 ± 1.16 | 0.47 ± 1.19 | 0.27 ± 1.14 | −0.25 ± 1.47 | 0.0002 | Severe vs. other groups 0.01, <0.001 and 0.25 | |
| °WZ, mean ± SD | ≤2 years (n = 148) | 0.33 ± 1.05 | −0.25 ± 1.53 | −0.39 ± 1.45 | −0.89 ± 1.77 | 0.048 | Severe vs. Absent 0.042 |
| 2–5 years (n = 61) | 0.49 ± 1.12 | 0.44 ± 1.22 | −0.59 ± 1.12 | −0.48 ± 0.91 | 0.0097 | Moderate vs. Mild or Absent 0.027 and 0.051 | |
| >5 years (n = 448) | 0.33 ± 0.96 | 0.23 ± 1.13 | 0.08 ± 1.22 | −0.63 ± 1.36 | <0.001 | Severe vs. other groups < 0.001 | |
| §WHZ, mean ± SD | ≤2 years (n = 148) | 0.43 ± 1.07 | 0.02 ± 1.45 | 0.01 ± 1.41 | −0.40 ± 1.71 | 0.289 | |
| ¥BMIZ, mean ± SD | 2–5 years (n = 61) | −0.34 ± 1.32 | −0.13 ± 1.11 | −0.49 ± 1.05 | −1.03 ± 1.04 | 0.379 | |
| >5 years (n = 448) | 0.04 ± 1.03 | −0.02 ± 1.26 | −0.12 ± 1.32 | −0.61 ± 1.33 | 0.010 | Severe vs. absent or mild 0.049 and 0.008 |
| N° Surgery | No Surgery | One Surgical Procedure | Two Surgical Procedures | Three Surgical Procedures | Four Surgical Procedures | Five Surgical Procedures | |
|---|---|---|---|---|---|---|---|
| CHD Severity | |||||||
| Mild CHD (255 patients) | 194 (76%) | 55 (21.6%) | 5 (2%) | 1 (0.4%) | 0 | 0 | |
| Moderate CHD (223 patients) | 71 (31.8%) | 117 (52.4%) | 27 (12.1%) | 6 (2.7%) | 2 (0.9%) | 0 | |
| Severe CHD (88 patients) | 8 (9.1%) | 19 (21.6%) | 36 (40.9%) | 24 (27.3%) | 0 | 1 (1.1%) | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Palleri, D.; Bartolacelli, Y.; Balducci, A.; Bonetti, S.; Zanoni, R.; Ciuca, C.; Gesuete, V.; Bulgarelli, A.; Hasan, T.; Ragni, L.; et al. Moderate and Severe Congenital Heart Diseases Adversely Affect the Growth of Children in Italy: A Retrospective Monocentric Study. Nutrients 2023, 15, 484. https://doi.org/10.3390/nu15030484
Palleri D, Bartolacelli Y, Balducci A, Bonetti S, Zanoni R, Ciuca C, Gesuete V, Bulgarelli A, Hasan T, Ragni L, et al. Moderate and Severe Congenital Heart Diseases Adversely Affect the Growth of Children in Italy: A Retrospective Monocentric Study. Nutrients. 2023; 15(3):484. https://doi.org/10.3390/nu15030484
Chicago/Turabian StylePalleri, Daniela, Ylenia Bartolacelli, Anna Balducci, Simone Bonetti, Rossana Zanoni, Cristina Ciuca, Valentina Gesuete, Ambra Bulgarelli, Tammam Hasan, Luca Ragni, and et al. 2023. "Moderate and Severe Congenital Heart Diseases Adversely Affect the Growth of Children in Italy: A Retrospective Monocentric Study" Nutrients 15, no. 3: 484. https://doi.org/10.3390/nu15030484
APA StylePalleri, D., Bartolacelli, Y., Balducci, A., Bonetti, S., Zanoni, R., Ciuca, C., Gesuete, V., Bulgarelli, A., Hasan, T., Ragni, L., Angeli, E., Gargiulo, G. D., & Donti, A. (2023). Moderate and Severe Congenital Heart Diseases Adversely Affect the Growth of Children in Italy: A Retrospective Monocentric Study. Nutrients, 15(3), 484. https://doi.org/10.3390/nu15030484