
The Clinical, Microbiological, and Immunological Effects of Probiotic Supplementation on Prevention and Treatment of Periodontal Diseases: A Systematic Review and Meta-Analysis

 , , ,
, , ,
Abstract
:1. Introduction
1.1. Etiology of Periodontal Disease
1.2. Periodontal Disease Assessment, Diagnosis, and Therapy
1.3. Periodontal Diseases and Probiotics
2. Materials and Methods
2.1. Eligibility Criteria
2.2. Information Sources, Search Strategy, and Study Selection
2.3. Data Items and Collection Process
2.4. Risk of Bias within Studies
2.5. Summary Measures and Synthesis of Results
2.6. Risk of Bias across Studies
2.7. Additional Analysis (Subgroup Analysis and Investigation of Heterogeneity)
3. Results
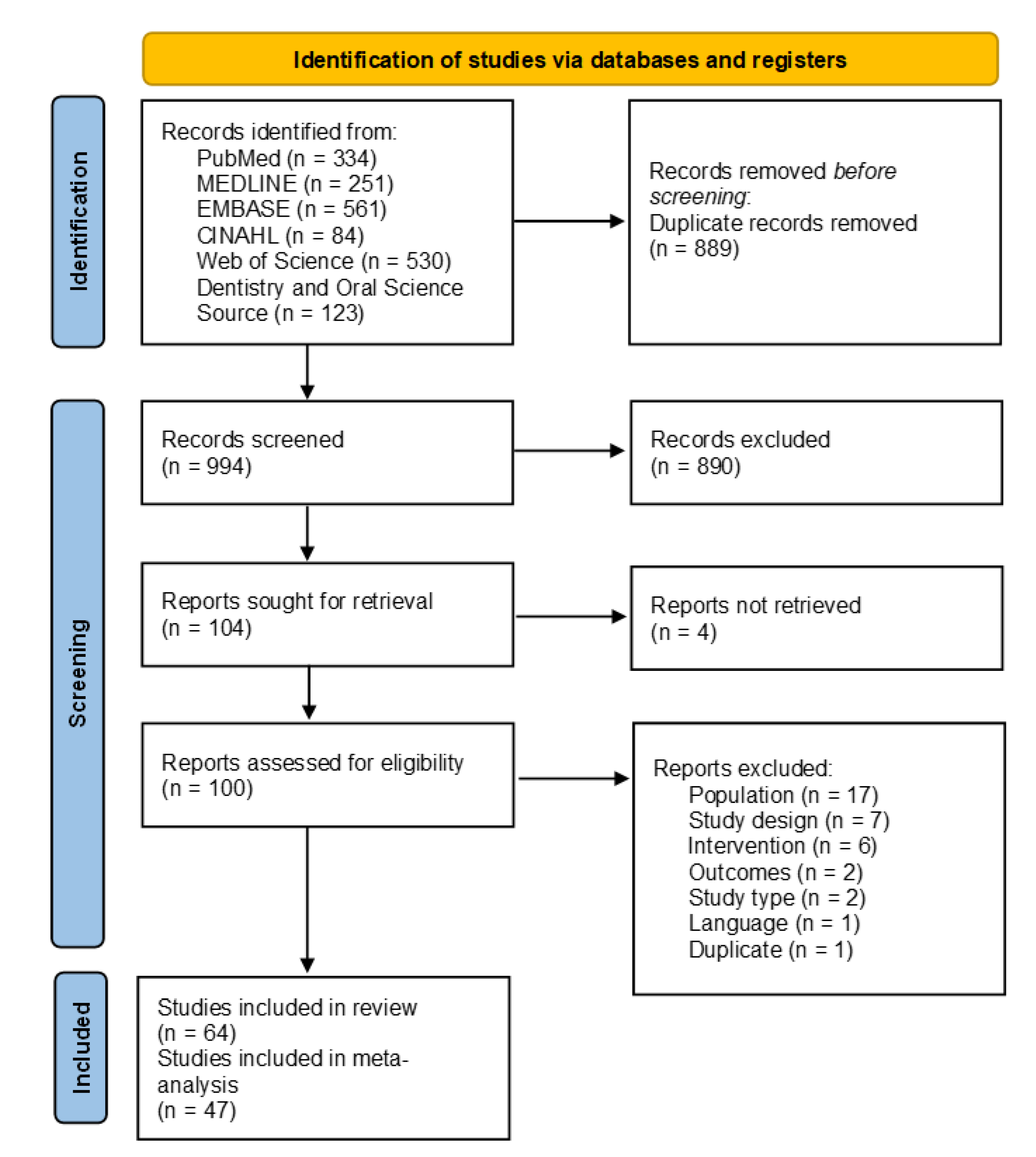
3.1. Study Selection
3.2. Study Characteristics
3.3. Risk of Bias within Studies
3.4. Synthesis of Results
3.4.1. Associations between Probiotic Supplementation and Clinical Outcomes in Periodontal Disease Patients
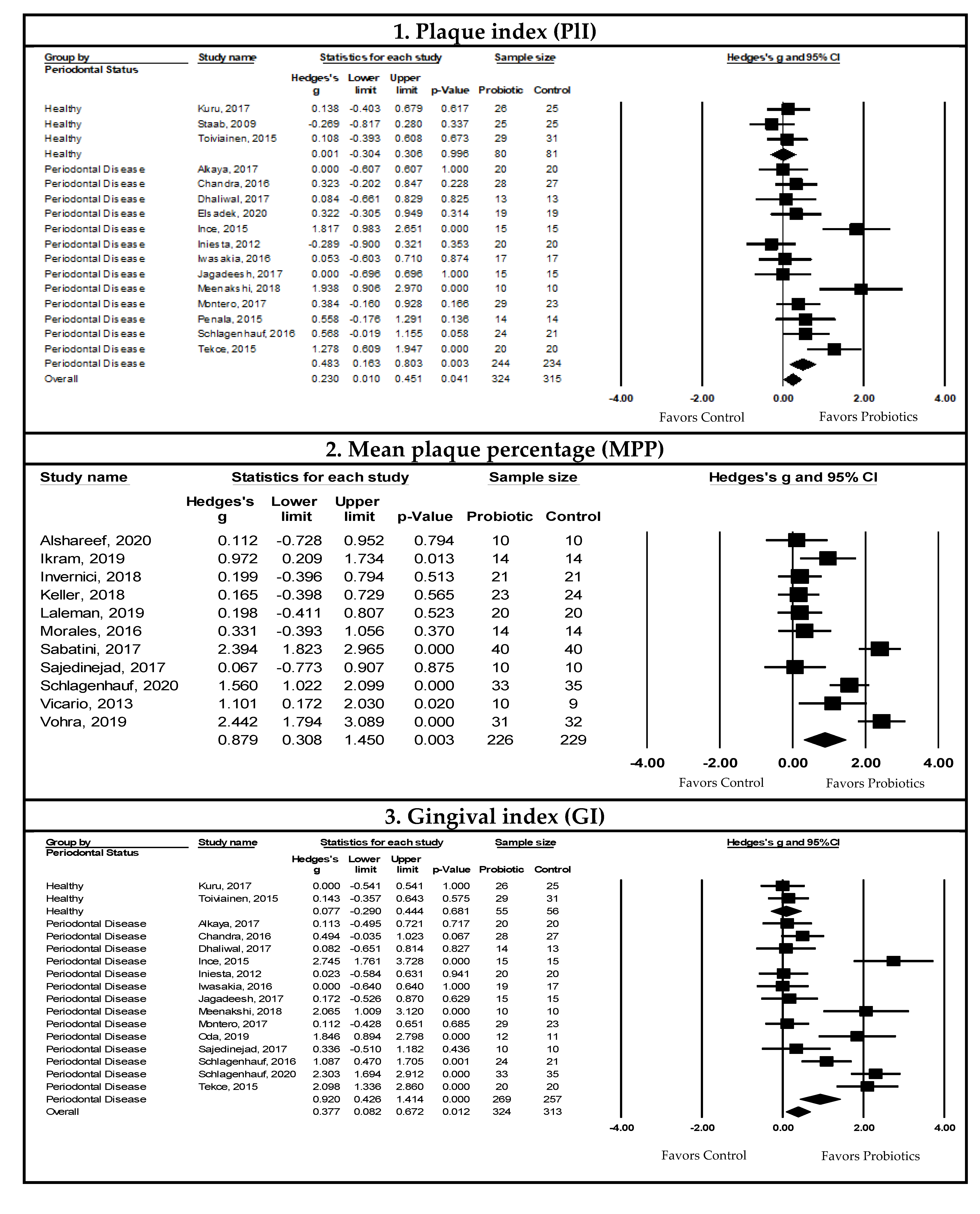
Pooled Meta-Analysis Examining the Effects of Probiotics on Plaque Index (PlI)
Pooled Meta-Analysis Examining the Effects of Probiotics on Mean Plaque Percentage (MPP)
Pooled Meta-Analysis Examining the Effects of Probiotics on Gingival Index (GI)
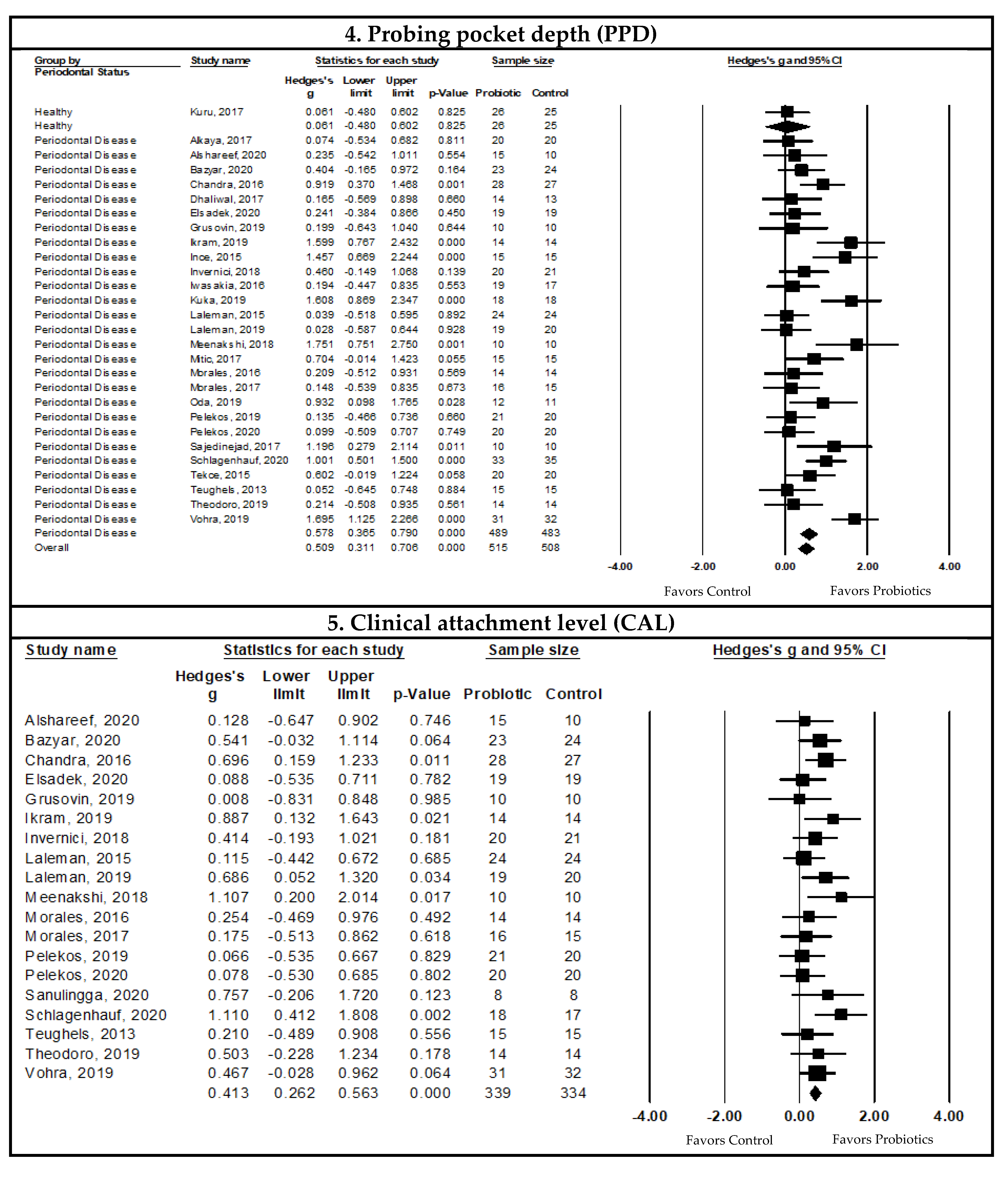
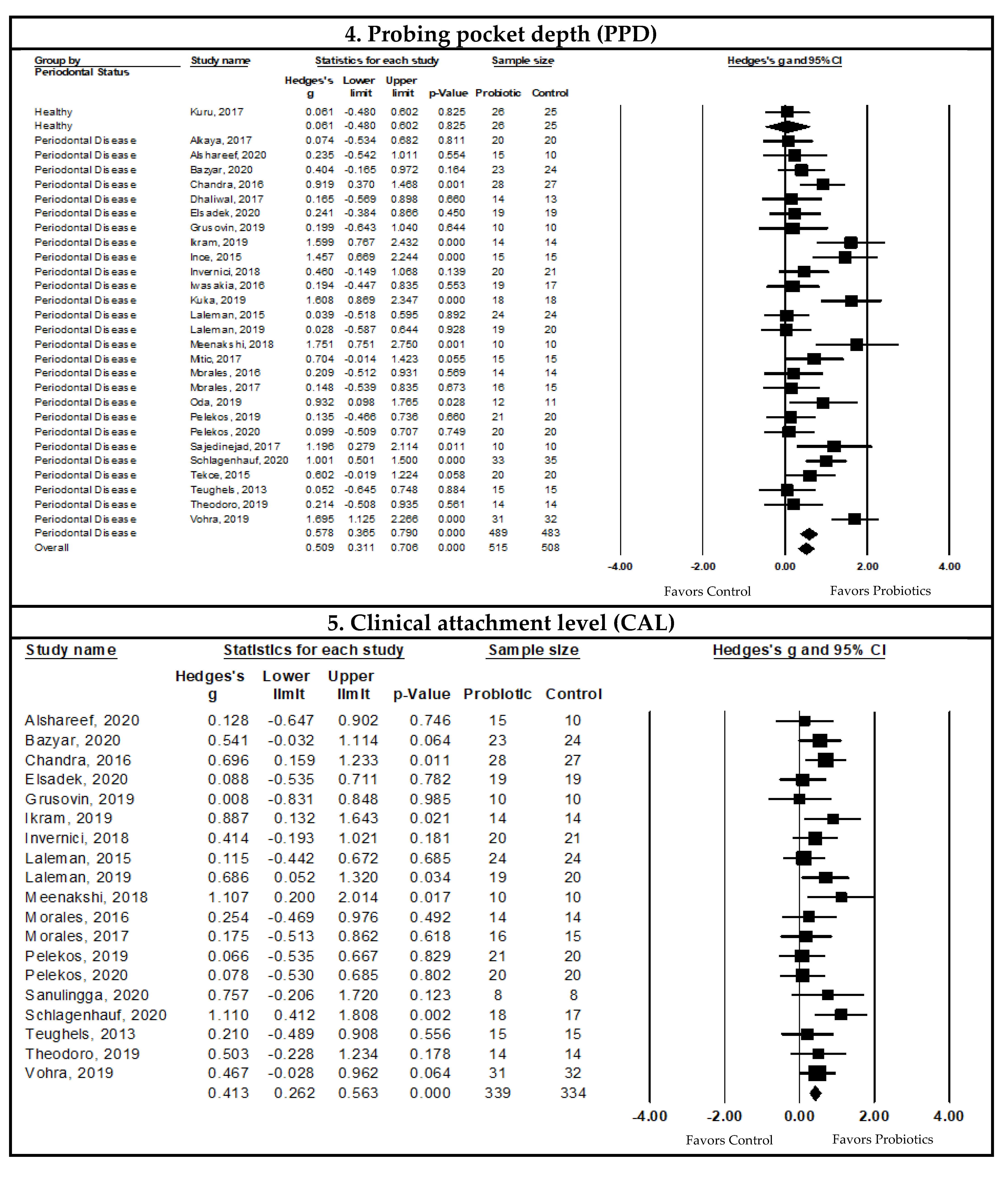
Pooled Meta-Analysis Examining the Effects of Probiotics on Probing Pocket Depth (PPD)
Pooled Meta-Analysis Examining the Effects of Probiotics on Clinical Attachment Level (CAL)
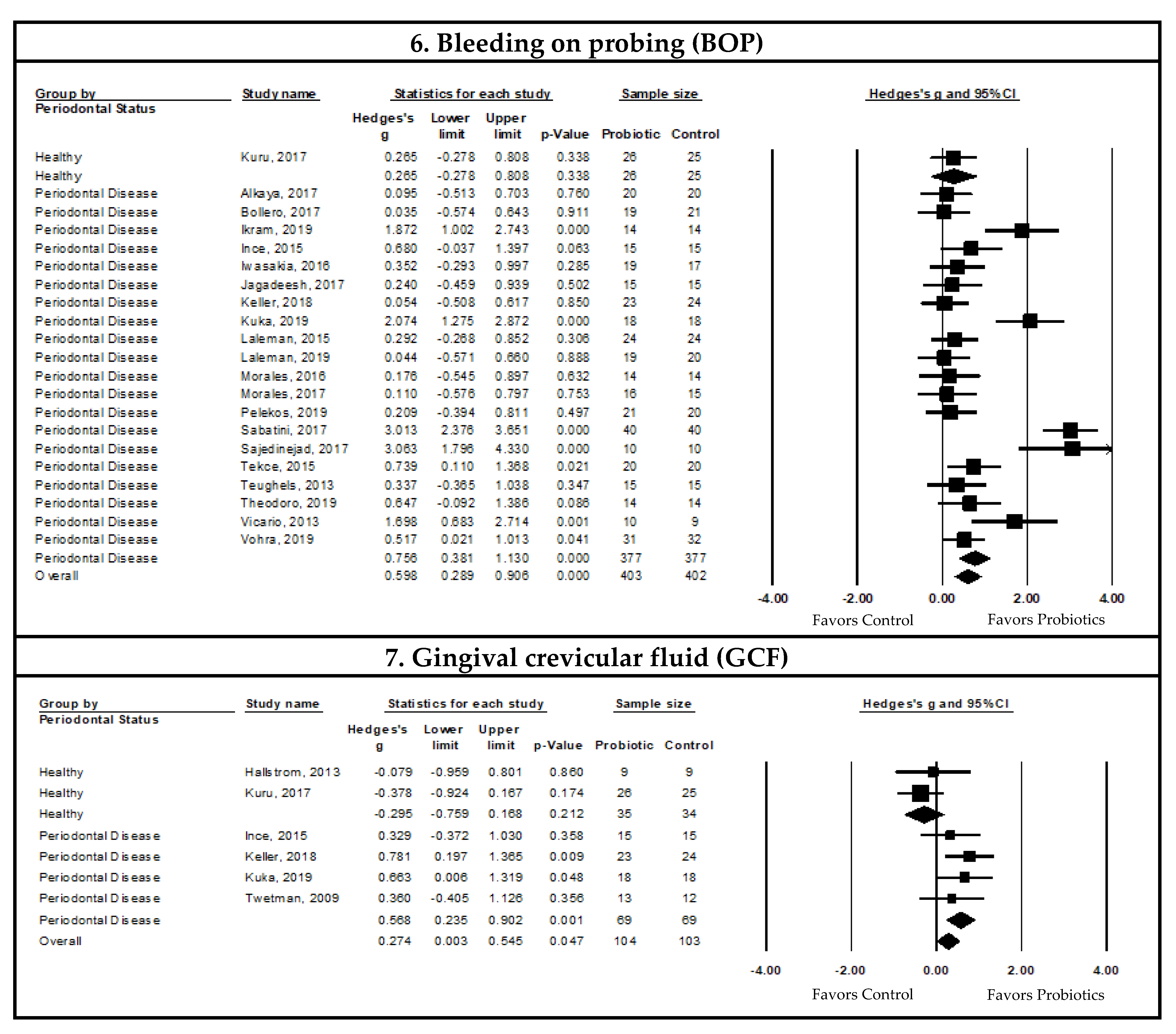
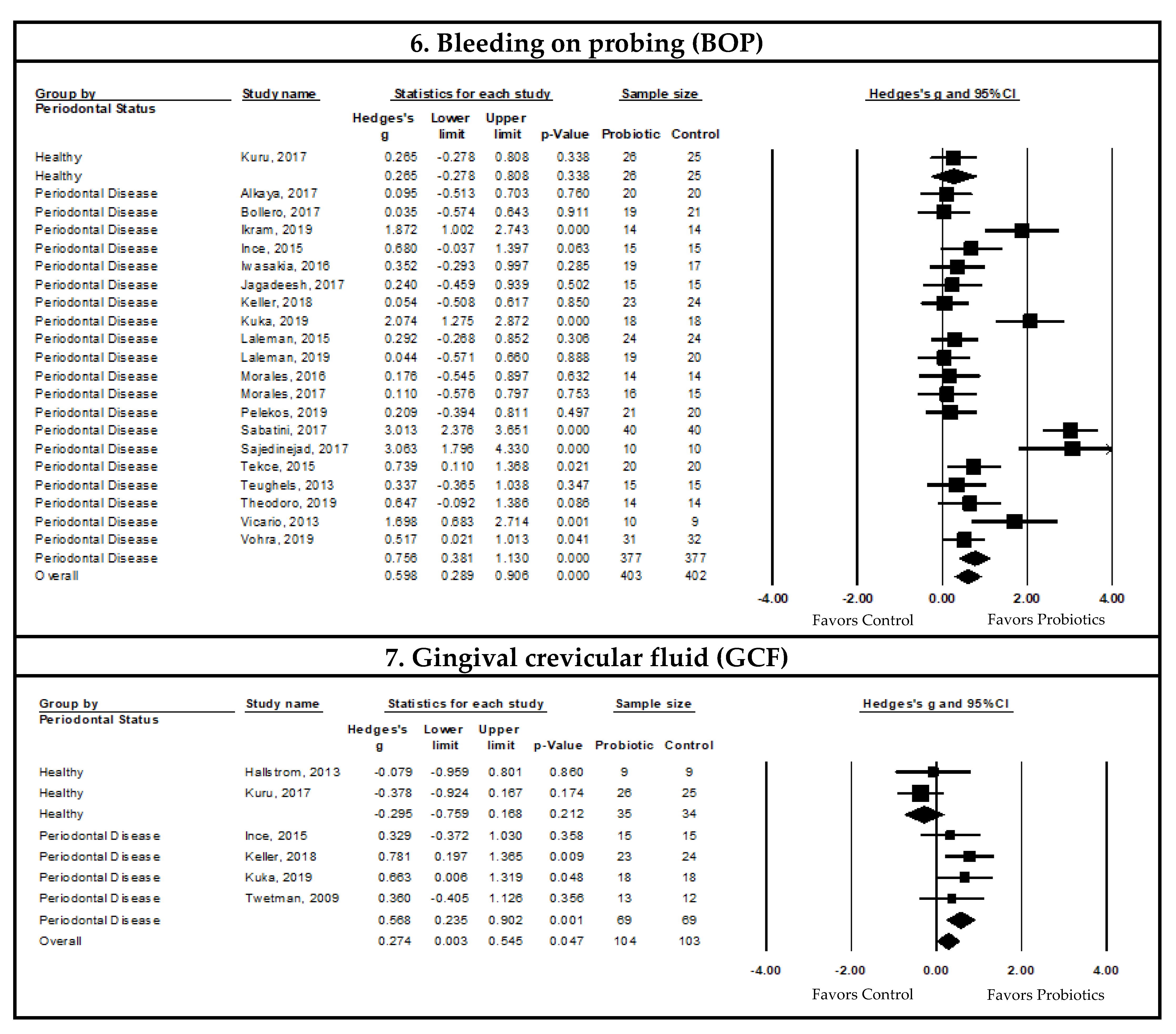
Pooled Meta-Analysis Examining the Effects of Probiotics on Bleeding on Probing (BOP)
Pooled Meta-Analysis Examining the Effects of Probiotics on Gingival Crevicular Fluid (GCF)
Pooled Meta-Analysis Examining the Effects of Probiotics on Gingival Recession (REC)
3.4.2. Associations between Probiotic Supplementation and Microbiological Outcomes in Periodontal Disease Patients
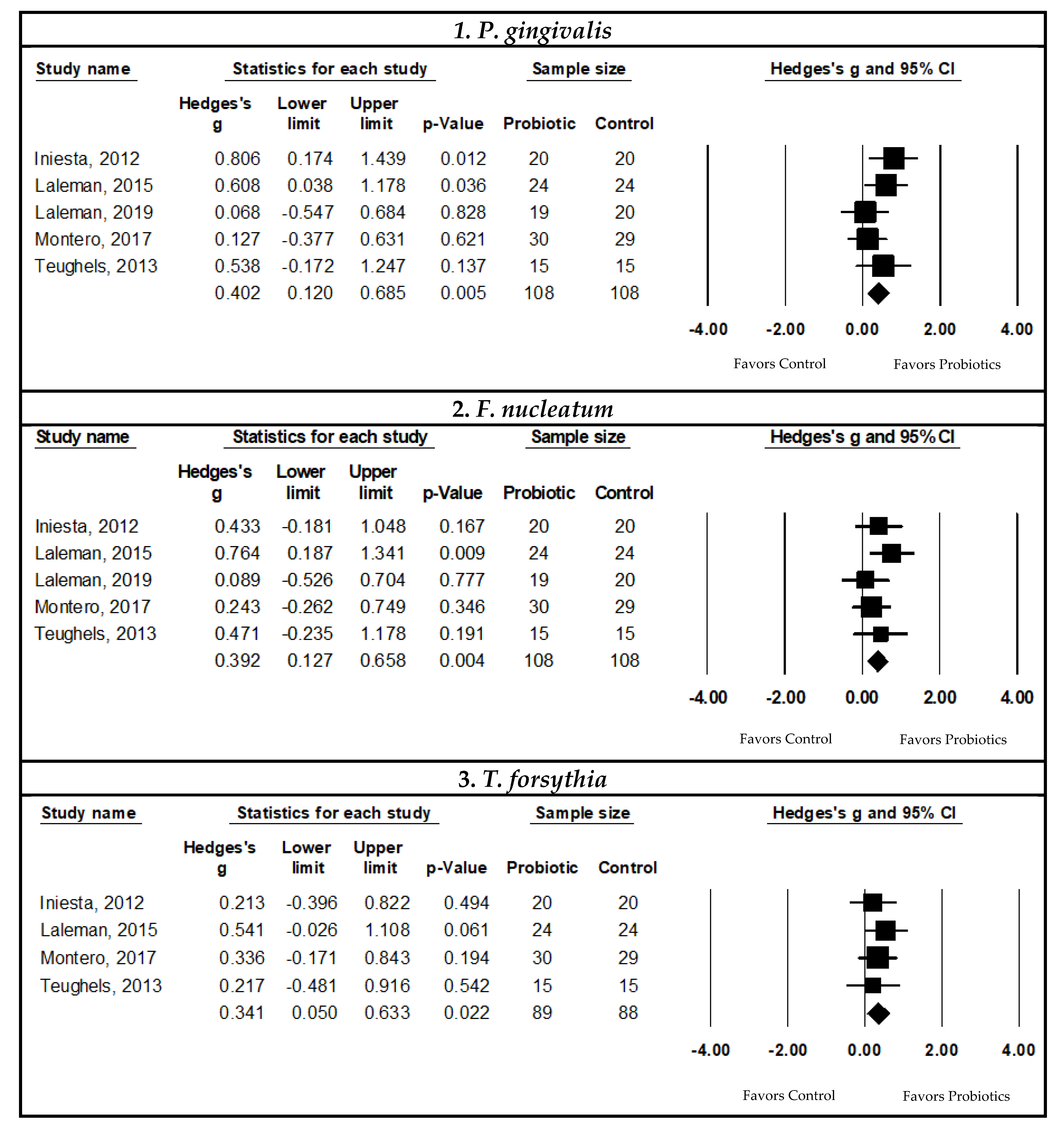
Pooled Meta-Analysis Examining the Effects of Probiotics on Subgingival Porphyromonas Gingivalis Count
Pooled Meta-Analysis Examining the Effects of Probiotics on Subgingival Fusobacterium nucleatum Count
Pooled Meta-Analysis Examining the Effects of Probiotic on Subgingival Tannerella forsythia Count
Pooled Meta-Analysis Examining the Effects of Probiotics on Subgingival Counts of Other periodonthopathogenes
3.4.3. Associations between Probiotic Supplementation and Immunological Outcomes in Periodontal Disease Patients
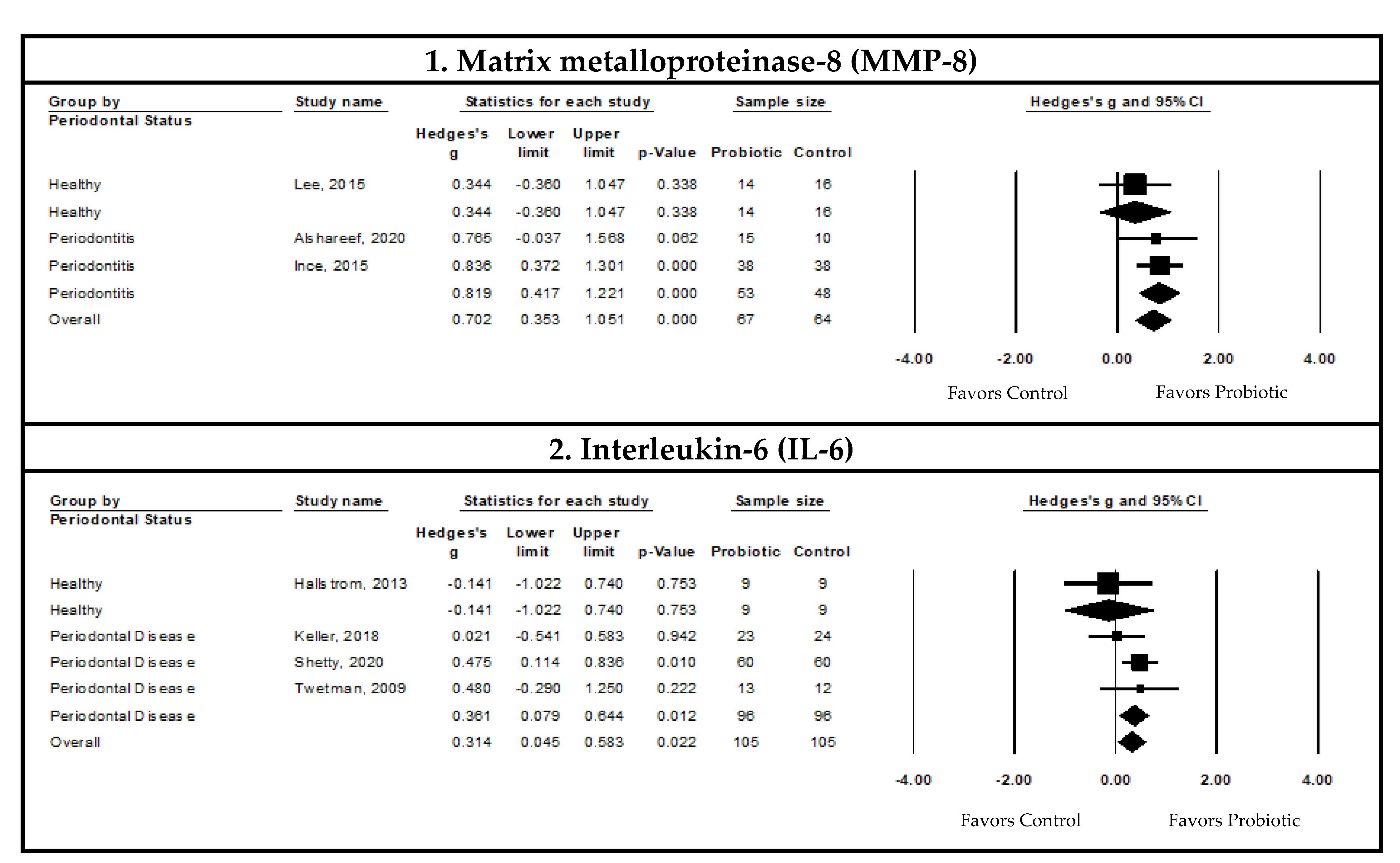
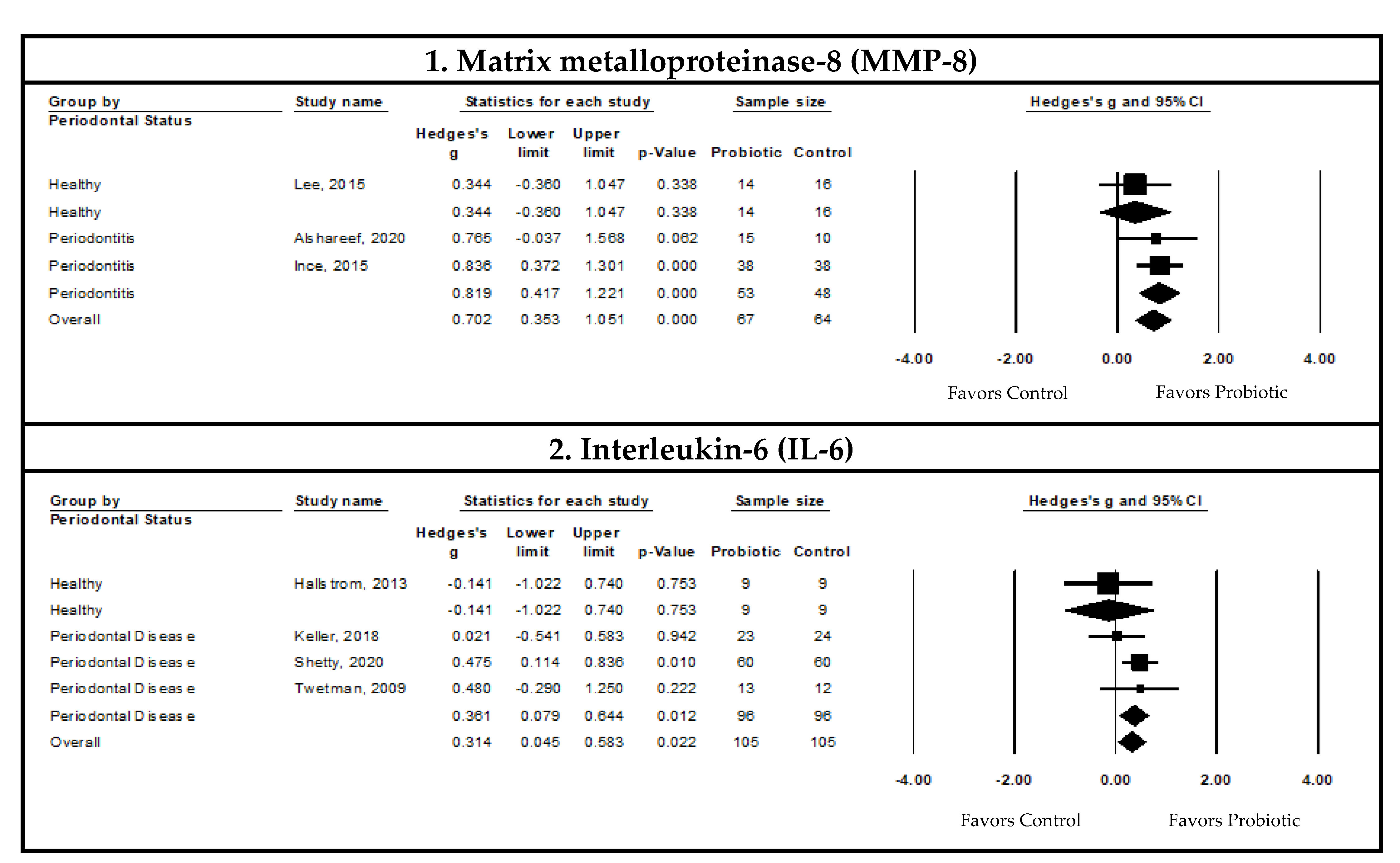
Pooled Meta-Analysis Examining the Effects of Probiotics on Matrix Metalloproteinase-8 (MMP-8) Levels in the Gingival Crevicular Fluid (GCF)
Pooled Meta-Analysis Examining the Effects of Probiotics on Interleukin-6 (IL-6) Levels in the Gingival Crevicular Fluid
Pooled Meta-Analysis Examining the Effects of Probiotics on Other Immunological Biomarkers in the Gingival Crevicular Fluid (GCF)
4. Discussion
- Type of periodontal disease, which indicated that probiotic supplementation improved clinical outcomes in patients with periodontitis, but not in those with gingivitis or healthy individuals. However, the GCF volume had statistically significant reductions in both gingivitis and periodontitis patients;
- Probiotic formulations consisting of Lactobacillus species and, more specifically, L. reuteri were associated with statistically significant improvements in all clinical outcomes in patients with periodontal disease;
- Probiotic treatment duration, which showed that probiotic supplementation resulted in statistically significant improvements in the clinical outcomes after one month of supplementation in periodontal disease patients;
- Mode of probiotic delivery, which indicated that probiotic supplementation through the “oral and ingestion” mode was associated with statistically significant improvements in all clinical outcomes in periodontal disease patients.
- Oral hygiene instructions along with probiotic supplementation improved PlI and BOP, while GI, PPD, and CAL improved with probiotic supplementation, irrespective of the presence or absence of oral hygiene instructions.
4.1. Probiotics and Severity of Periodontal Disease
4.2. Probiotics vs. Antibiotics
4.3. Probiotic Formulation and Duration
4.4. Probiotic Mode of Delivery
4.5. Probiotic Supplementation and Oral Hygiene Instructions
4.6. Probiotic Supplementation and GCF Volume
4.7. Probiotic Supplementation and Microbiological Outcomes
4.8. Probiotic Supplementation and Immunological Outcomes
4.9. Probiotic Supplementation and Periodontal Disease Prevention
4.10. Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| Plaque Index (PlI) | The plaque index is a clinical indicator of oral hygiene status that measures the level and rate of microbial plaque formation on the gingival margin of the tooth’s surface. PlI is also used to estimate the potential therapeutic or preventive roles of oral care products [24]. |
| Gingival Index (GI) | The gingival index is a numeric scoring system that assesses inflammation and structural changes in gingival tissue [27]. |
| Pocket Probing Depth (PPD) | The probing depth is the distance between the gingival margin and base of the periodontal pocket, providing one of the most accurate parameters for the clinical diagnosis of periodontal disease [23]. |
| Clinical Attachment Level (CAL) | CAL is measured between the fixed point of the cemento-enamel junction of the tooth and the base of the periodontal pocket. The CAL is one of the most accurate and widely used measures for the clinical diagnosis of periodontal disease [23]. |
| Bleeding on Probing (BOP) | BOP is a reliable indicator of gingival inflammation and refers to the bleeding of gingival tissue upon gentle probing [143]. |
| Gingival crevicular fluid (GCF) | GCF is an inflammatory exudate that permits non-invasive sampling from the oral cavity and is composed of serum, leukocytes, and structural cells from the periodontium and oral bacteria. It is found in the periodontal sulcus between the tooth and marginal gingiva. The GCF flow rate and volume is used as an indicator of gingival inflammation, which can be used to assess periodontal disease severity [25]. |
| Gingival recession (REC) | REC is a clinical measurement of the distance between the cemento-enamel junction and the free gingival margin measured in millimeters (mm) during periodontal probing [26]. |
References
- GBD 2016 Disease and Injury Incidence and Prevalence Collaborators. Global, regional, and national incidence, prevalence, and years lived with disability for 328 diseases and injuries for 195 countries, 1990–2016: A systematic analysis for the Global Burden of Disease Study 2016. Lancet 2017, 390, 1211–1259. [Google Scholar] [CrossRef] [Green Version]
- Nazir, M.; Al-Ansari, A.; Al-Khalifa, K.; Alhareky, M.; Gaffar, B.; Almas, K. Global Prevalence of Periodontal Disease and Lack of Its Surveillance. Sci. World J. 2020, 2020, 2146160. [Google Scholar] [CrossRef] [PubMed]
- Seminario-Amez, M.; Lopez-Lopez, J.; Estrugo-Devesa, A.; Ayuso-Montero, R.; Jane-Salas, E. Probiotics and oral health: A systematic review. Med. Oral Patol. Oral Cir. Bucal 2017, 22, E282–E288. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gasner, N.S.; Schure, R.S. Periodontal Disease. In StatPearls [Internet]; StatPearls Publishing: Treasure Island, FL, USA, 2021. [Google Scholar]
- Nazir, M.A. Prevalence of periodontal disease, its association with systemic diseases and prevention. Int. J. Health Sci. 2017, 11, 72–80. [Google Scholar]
- Ferreira, M.C.; Dias-Pereira, A.C.; Branco-de-Almeida, L.S.; Martins, C.C.; Paiva, S.M. Impact of periodontal disease on quality of life: A systematic review. J. Periodontal Res. 2017, 52, 651–665. [Google Scholar] [CrossRef] [PubMed]
- Hajishengallis, G.; Chavakis, T. Local and systemic mechanisms linking periodontal disease and inflammatory comorbidities. Nat. Rev. Immunol. 2021, 21, 426–440. [Google Scholar] [CrossRef] [PubMed]
- Cardoso, E.M.; Reis, C.; Manzanares-Céspedes, M.C. Chronic periodontitis, inflammatory cytokines, and interrelationship with other chronic diseases. Postgrad. Med. 2018, 130, 98–104. [Google Scholar] [CrossRef]
- Pihlstrom, B.L.; Michalowicz, B.S.; Johnson, N.W. Periodontal diseases. Lancet 2005, 366, 1809–1820. [Google Scholar] [CrossRef] [Green Version]
- Morales, A.; Gandolfo, A.; Bravo, J.; Carvajal, P.; Silva, N.; Godoy, C.; Garcia-Sesnich, J.; Hoare, A.; Diaz, P.; Gamonal, J. Microbiological and clinical effects of probiotics and antibiotics on nonsurgical treatment of chronic periodontitis: A randomized placebocontrolled trial with 9-month follow-up. J. Appl. Oral Sci. 2018, 26, e20170075. [Google Scholar] [CrossRef]
- Könönen, E.; Gursoy, M.; Gursoy, U.K. Periodontitis: A Multifaceted Disease of Tooth-Supporting Tissues. J. Clin. Med. 2019, 8, 1135. [Google Scholar] [CrossRef] [Green Version]
- Williams, R.C. Periodontal Disease. N. Engl. J. Med. 1990, 322, 373–382. [Google Scholar] [CrossRef] [PubMed]
- Laudenbach, J.M.; Simon, Z. Common Dental and Periodontal Diseases: Evaluation and Management. Med. Clin. N. Am. 2014, 98, 1239–1260. [Google Scholar] [CrossRef] [PubMed]
- Montero, E.; Iniesta, M.; Rodrigo, M.; Marín, M.J.; Figuero, E.; Herrera, D.; Sanz, M. Clinical and microbiological effects of the adjunctive use of probiotics in the treatment of gingivitis: A randomized controlled clinical trial. J. Clin. Periodontol. 2017, 44, 708–716. [Google Scholar] [CrossRef]
- Shi, B.; Chang, M.; Martin, J.; Mitreva, M.; Lux, R.; Klokkevold, P.; Sodergren, E.; Weinstock, G.M.; Haak, S.K.; Lia, H. Dynamic changes in the subgingival microbiome and their potential for diagnosis and prognosis of periodontitis. MBio 2015, 6, e01926-14. [Google Scholar] [CrossRef] [Green Version]
- Abusleme, L.; Dupuy, A.K.; Dutzan, N.; Silva, N.; Burleson, J.A.; Strausbaugh, L.D.; Gamonal, J.; Diaz, P.I. The subgingival microbiome in health and periodontitis and its relationship with community biomass and inflammation. ISME J. 2013, 7, 1016–1025. [Google Scholar] [CrossRef] [Green Version]
- Griffen, A.L.; Beall, C.J.; Campbell, J.H.; Firestone, N.D.; Kumar, P.S.; Yang, Z.K.; Podar, M.; Leys, E.J. Distinct and complex bacterial profiles in human periodontitis and health revealed by 16S pyrosequencing. ISME J. 2012, 6, 1176–1185. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liu, B.; Faller, L.L.; Klitgord, N.; Mazumdar, V.; Ghodsi, M.; Sommer, D.D.; Gibbons, T.R.; Treangen, T.J.; Chang, Y.C.; Li, S.; et al. Deep sequencing of the oral microbiome reveals signatures of periodontal disease. PLoS ONE 2012, 7, e37919. [Google Scholar] [CrossRef] [Green Version]
- Curtis, M.A.; Diaz, P.I.; Van Dyke, T.E. The role of the microbiota in periodontal disease. Periodontol. 2000 2020, 83, 14–25. [Google Scholar] [CrossRef]
- Mohanty, R.; Asopa, S.J.; Joseph, M.D.; Singh, B.; Rajguru, J.P.; Saidath, K.; Sharma, U. Red complex: Polymicrobial conglomerate in oral flora: A review. J. Fam. Med. Prim. Care 2019, 8, 3480–3486. [Google Scholar] [CrossRef]
- Kinane, D.F.; Stathopoulou, P.G.; Papapanou, P.N. Periodontal diseases. Nat. Rev. Dis. Primers 2017, 3, 17038. [Google Scholar] [CrossRef]
- Lamont, R.J.; Koo, H.; Hajishengallis, G. The oral microbiota: Dynamic communities and host interactions. Nat. Rev. Microbiol. 2018, 16, 745–759. [Google Scholar] [CrossRef] [PubMed]
- Armitage, G.C. The complete periodontal examination. Periodontol. 2000 2004, 34, 22–33. [Google Scholar] [CrossRef] [PubMed]
- Joiner, A.C. 4—The Cleaning of Teeth. In Handbook for Cleaning/Decontamination of Surfaces; Johansson, I., Somasundaran, P., Eds.; Elsevier Science B.V.: Amsterdam, The Netherlands, 2007; pp. 371–405. ISBN 978-0-444-51664-0. [Google Scholar]
- Subbarao, K.C.; Nattuthurai, G.S.; Sundararajan, S.K.; Sujith, I.; Joseph, J.; Syedshah, Y.P. Gingival Crevicular Fluid: An Overview. J. Pharm. Bioallied Sci. 2019, 11, S135–S139. [Google Scholar] [CrossRef] [PubMed]
- Handelman, C.S.; Eltink, A.P.; BeGole, E. Quantitative measures of gingival recession and the influence of gender, race, and attrition. Prog. Orthod. 2018, 19, 5. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rebelo, M.A.B.; de Queiroz, A.C. Gingival Indices: State of Art. In Gingival Diseases—Their Aetiology, Prevention and Treatment; Panagakos, F.S., Davies, R.M., Eds.; IntechOpen: Rijeka, Croatia, 2011; Chapter 3. [Google Scholar]
- Sweeting, L.A.; Davis, K.; Cobb, C.M. Periodontal Treatment Protocol (PTP) for the general dental practice. J. Dent. Hyg. JDH 2008, 82 (Suppl. 3), 16–26. [Google Scholar] [PubMed]
- Tonetti, M.S.; Greenwell, H.; Kornman, K.S. Staging and grading of periodontitis: Framework and proposal of a new classification and case definition. J. Clin. Periodontol. 2018, 45, S149–S161. [Google Scholar] [CrossRef] [Green Version]
- Tonetti, M.S.; Sanz, M. Implementation of the new classification of periodontal diseases: Decision-making algorithms for clinical practice and education. J. Clin. Periodontol. 2019, 46, 398–405. [Google Scholar] [CrossRef]
- Comprehensive Periodontal Therapy: A Statement by the American Academy of Periodontology. J. Periodontol. 2011, 82, 943–949. [CrossRef]
- Mirbod, S.; Matthews, D.C.; Ellis, L.; Marquez, I.C. Point of Care. JCDA 2007, 73, 137–147. [Google Scholar]
- Hung, H.-C.; Douglass, C.W. Meta-Analysis of the effect of scaling and root planing, surgical treatment and antibiotic therapies on periodontal probing depth and attachment loss. J. Clin. Periodontol. 2002, 29, 975–986. [Google Scholar] [CrossRef]
- Pelekos, G.; Ho, S.N.; Acharya, A.; Leung, W.K.; McGrath, C. A double-blind, paralleled-arm, placebo-controlled and randomized clinical trial of the effectiveness of probiotics as an adjunct in periodontal care. J. Clin. Periodontol. 2019, 46, 1217–1227. [Google Scholar] [CrossRef]
- Saini, K.; Minj, J. Multifunctional Aspects of Probiotics and Prebiotics in Health Management: An Overview BT. In Dairy Processing: Advanced Research to Applications; Minj, J., Sudhakaran, V.A., Kumari, A., Eds.; Springer: Singapore, 2020; pp. 119–131. ISBN 978-981-15-2608-4. [Google Scholar]
- Palai, S.; Derecho, C.M.P.; Kesh, S.S.; Egbuna, C.; Onyeike, P.C. Prebiotics, Probiotics, Synbiotics and Its Importance in the Management of Diseases BT. In Functional Foods and Nutraceuticals: Bioactive Components, Formulations and Innovations; Egbuna, C., Dable Tupas, G., Eds.; Springer International Publishing: Cham, Switzerland, 2020; pp. 173–196. ISBN 978-3-030-42319-3. [Google Scholar]
- McFarland, L.V.; Surawicz, C.M.; Greenberg, R.N.; Fekety, R.; Elmer, G.W.; Moyer, K.A.; Melcher, S.A.; Bowen, K.E.; Cox, J.L.; Noorani, Z.; et al. A Randomized Placebo-Controlled Trial of Saccharomyces boulardii in Combination with Standard Antibiotics for Clostridium difficile Disease. JAMA 1994, 271, 1913–1918. [Google Scholar] [CrossRef] [PubMed]
- Rodgers, B.; Kirley, K.; Mounsey, A.; Ewigman, B. Prescribing an antibiotic? Pair it with probiotics. J. Fam. Pract. 2013, 62, 148–150. [Google Scholar] [PubMed]
- Rondanelli, M.; Faliva, M.A.; Perna, S.; Giacosa, A.; Peroni, G.; Castellazzi, A.M. Using probiotics in clinical practice: Where are we now? A review of existing meta-analyses. Gut Microbes 2017, 8, 521–543. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Çaglar, E.; Cildir, S.K.; Ergeneli, S.; Sandalli, N.; Twetman, S. Salivary mutans streptococci and lactobacilli levels after ingestion of the probiotic bacterium Lactobacillus reuteri ATCC 55730 by straws or tablets. Acta Odontol. Scand. 2006, 64, 314–318. [Google Scholar] [CrossRef]
- Tekce, M.; Ince, G.; Gursoy, H.; Ipci, S.D.; Cakar, G.; Kadir, T.; Yılmaz, S. Clinical and microbiological effects of probiotic lozenges in the treatment of chronic periodontitis: A 1-year follow-up study. J. Clin. Periodontol. 2015, 42, 363–372. [Google Scholar] [CrossRef]
- Hallström, H.; Lindgren, S.; Yucel-Lindberg, T.T.; Dahlén, G.; Renvert, S.; Twetman, S. Effect of probiotic lozenges on inflammatory reactions and oral biofilm during experimental gingivitis. Acta Odontol. Scand. 2013, 71, 828–833. [Google Scholar] [CrossRef]
- Iniesta, M.; Herrera, D.; Montero, E.; Zurbriggen, M.; Matos, A.R.; Marín, M.J.; Sánchez-Beltrán, M.C.; Llama-Palacio, A.; Sanz, M. Probiotic effects of orally administered Lactobacillus reuteri-containing tablets on the subgingival and salivary microbiota in patients with gingivitis. A randomized clinical trial. J. Clin. Periodontol. 2012, 39, 736–744. [Google Scholar] [CrossRef]
- Yanine, N.; Araya, I.; Brignardello-Petersen, R.; Carrasco-Labra, A.; Gonzalez, A.; Preciado, A.; Villanueva, J.; Sanz, M.; Martin, C. Effects of probiotics in periodontal diseases: A systematic review. Clin. Oral Investig. 2013, 17, 1627–1634. [Google Scholar] [CrossRef]
- Akram, Z.; Shafqat, S.S.; Aati, S.; Kujan, O.; Fawzy, A. Clinical efficacy of probiotics in the treatment of gingivitis: A systematic review and meta-analysis. Aust. Dent. J. 2020, 65, 12–20. [Google Scholar] [CrossRef]
- Vives-Soler, A.; Chimenos-Kustner, E. Effect of probiotics as a complement to non-surgical periodontal therapy in chronic periodontitis: A systematic review. Med. Oral Patol. Oral Cir. Bucal 2020, 25, e161–e167. [Google Scholar] [CrossRef] [PubMed]
- Ho, S.N.; Acharya, A.; Sidharthan, S.; Li, K.Y.; Leung, W.K.; McGrath, C.; Pelekos, G. A Systematic Review and Meta-analysis of Clinical, Immunological, and Microbiological Shift in Periodontitis After Nonsurgical Periodontal Therapy with Adjunctive Use of Probiotics. J. Evid. Based Dent. Pract. 2020, 20, 101397. [Google Scholar] [CrossRef] [PubMed]
- Villafuerte, K.R.V.; Martinez, C.J.H.; Nobre, A.V.V.; Maia, L.P.; Tirapelli, C. What are microbiological effects of the adjunctive use of probiotics in the treatment of periodontal diseases? A systematic review. Benef. Microbes 2021, 12, 307–319. [Google Scholar] [CrossRef] [PubMed]
- Sterne, J.A.C.; Savović, J.; Page, M.J.; Elbers, R.G.; Blencowe, N.S.; Boutron, I.; Cates, C.J.; Cheng, H.-Y.; Corbett, M.S.; Eldridge, S.M.; et al. RoB 2: A revised tool for assessing risk of bias in randomised trials. BMJ 2019, 366, l4898. [Google Scholar] [CrossRef] [Green Version]
- Faraone, S.V. Interpreting estimates of treatment effects: Implications for managed care. Pharm. Ther. 2008, 33, 700–711. [Google Scholar]
- Higgins, J.P.T.; Thompson, S.G.; Deeks, J.J.; Altman, D.G. Measuring inconsistency in meta-analyses. Br. Med. J. 2003, 327, 557–560. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Duval, S.; Tweedie, R. Trim and Fill: A Simple Funnel-Plot–Based Method of Testing and Adjusting for Publication Bias in Meta-Analysis. Biometrics 2000, 56, 455–463. [Google Scholar] [CrossRef]
- Alkaya, B.; Laleman, I.; Keceli, S.; Ozcelik, O.; Haytac, M.C.; Teughels, W. Clinical effects of probiotics containing Bacillus species on gingivitis: A pilot randomized controlled trial. J. Periodontal Res. 2017, 52, 497–504. [Google Scholar] [CrossRef]
- Alshareef, A.; Attia, A.; Almalki, M.; Alsharif, F.; Melibari, A.; Mirdad, B.; Azab, E.; Youssef, A.R.; Dardir, A. Effectiveness of Probiotic Lozenges in Periodontal Management of Chronic Periodontitis Patients: Clinical and Immunological Study. Eur. J. Dent. 2020, 14, 281–287. [Google Scholar] [CrossRef]
- Bazyar, H.; Maghsoumi-Norouzabad, L.; Yarahmadi, M.; Gholinezhad, H.; Moradi, L.; Salehi, P.; Haghighi-Zadeh, M.H.; Zare Javid, A. The impacts of synbiotic supplementation on periodontal indices and biomarkers of oxidative stress in type 2 diabetes mellitus patients with chronic periodontitis under non-surgical periodontal therapy. A double-blind, placebo-controlled trial. Diabetes Metab. Syndr. Obes. Targets Ther. 2020, 13, 19–29. [Google Scholar] [CrossRef] [Green Version]
- Bollero, P.; Di Renzo, L.; Franco, R.; Rampello, T.; Pujia, A.; Merra, G.; De Lorenzo, A.; Docimo, R. Effects of new probiotic mouthwash in patients with diabetes mellitus and cardiovascular diseases. Eur. Rev. Med. Pharmacol. Sci. 2017, 21, 5827–5836. [Google Scholar] [PubMed]
- Boyeena, L.; Koduganti, R.R.; Panthula, V.R.; Jammula, S.P. Comparison of efficacy of probiotics versus tetracycline fibers as adjuvant to scaling and root planing. J. Indian Soc. Periodontol. 2019, 23, 539–544. [Google Scholar] [PubMed]
- Chandra, R.V.; Swathi, T.; Reddy, A.A.; Chakravarthy, Y.; Nagarajan, S.; Naveen, A. Effect of a Locally Delivered Probiotic-Prebiotic Mixture as an Adjunct to Scaling and Root Planing in the Management of Chronic Periodontitis. J. Int. Acad. Periodontol. 2016, 18, 67–75. [Google Scholar] [PubMed]
- Deshmukh, M.A.; Dodamani, A.S.; Karibasappa, G.; Khairnar, M.R.; Naik, R.G.; Jadhav, H.C. Comparative Evaluation of the Efficacy of Probiotic, Herbal and Chlorhexidine Mouthwash on Gingival Health: A Randomized Clinical Trial. J. Clin. Diagn. Res. 2017, 11, ZC13–ZC16. [Google Scholar] [CrossRef] [PubMed]
- Dhaliwal, P.K.; Grover, V.; Malhotra, R.; Kapoor, A. Clinical and Microbiological Investigation of the Effects of Probiotics Combined with Scaling and Root Planing in the Management of Chronic Periodontitis: A Randomized, Controlled Study. J. Int. Acad. Periodontol. 2017, 19, 101–108. [Google Scholar] [PubMed]
- Duarte, C.; Al-Yagoob, A.; Al-Ani, A. Efficacy of probiotics used as a periodontal treatment aid: A pilot study. Saudi Dent. J. 2019, 31, 143–147. [Google Scholar] [CrossRef] [PubMed]
- Elsadek, M.F.; Ahmed, B.M.; Alkhawtani, D.M.; Zia Siddiqui, A. A comparative clinical, microbiological and glycemic analysis of photodynamic therapy and Lactobacillus reuteri in the treatment of chronic periodontitis in type-2 diabetes mellitus patients. Photodiagn. Photodyn. Ther. 2020, 29, 101629. [Google Scholar] [CrossRef]
- Ercan, N.; Olgun, E.; Kisa, U.; Yalim, M. Effect of synbiotics in the treatment of smokers and nonsmokers with gingivitis: Randomized controlled trial. Aust. Dent. J. 2020, 65, 210–219. [Google Scholar] [CrossRef]
- Grusovin, M.G.; Bossini, S.; Calza, S.; Cappa, V.; Garzetti, G.; Scotti, E.; Gherlone, E.F.; Mensi, M. Clinical efficacy of Lactobacillus reuteri-containing lozenges in the supportive therapy of generalized periodontitis stage III and IV, grade C: 1-year results of a double-blind randomized placebo-controlled pilot study. Clin. Oral Investig. 2020, 24, 2015–2024. [Google Scholar] [CrossRef]
- Ikram, S.; Hassan, N.; Baig, S.; Ansari, S.A.; Borges, K.J.J.; Raffat, M.A. Clinical Efficacy of Probiotics as An Adjunct to Scaling and Root Planning in The Treatment of Chronic Periodontitis. Ann. Abbasi Shaheed Hosp. Karachi Med. Dent. Coll. 2019, 24, 31–37. [Google Scholar]
- Ikram, S.; Hassan, N.; Baig, S.; Borges, K.J.J.; Raffat, M.A.; Akram, Z. Effect of local probiotic (Lactobacillus reuteri) vs systemic antibiotic therapy as an adjunct to non-surgical periodontal treatment in chronic periodontitis. J. Investig. Clin. Dent. 2019, 10, e12393. [Google Scholar] [CrossRef] [PubMed]
- İnce, G.; Gürsoy, H.; İpçi, Ş.D.; Cakar, G.; Emekli-Alturfan, E.; Yılmaz, S. Clinical and Biochemical Evaluation of Lozenges Containing Lactobacillus reuteri as an Adjunct to Non-Surgical Periodontal Therapy in Chronic Periodontitis. J. Periodontol. 2015, 86, 746–754. [Google Scholar] [CrossRef] [PubMed]
- Invernici, M.M.; Salvador, S.L.; Silva, P.H.F.; Soares, M.S.M.; Casarin, R.; Palioto, D.B.; Souza, S.L.S.; Taba, M.; Novaes, A.B.; Furlaneto, F.A.C.; et al. Effects of Bifidobacterium probiotic on the treatment of chronic periodontitis: A randomized clinical trial. J. Clin. Periodontol. 2018, 45, 1198–1210. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Iwasaki, K.; Maeda, K.; Hidaka, K.; Nemoto, K.; Hirose, Y.; Deguchi, S. Daily intake of heat-killed Lactobacillus plantarum L-137 decreases the probing depth in patients undergoing supportive periodontal therapy. Oral Health Prev. Dent. 2016, 14, 207–214. [Google Scholar] [CrossRef]
- Jagadeesh K., M.; Shenoy, N.; Talwar, A.; Shetty, S. Clinical effect of pro-biotic containing Bacillus coagulans on plaque induced gingivitis: A randomized clinical pilot study. J. Health Allied Sci. NU. 2017, 7, 7–12. [Google Scholar] [CrossRef] [Green Version]
- Jäsberg, H.; Tervahartiala, T.; Sorsa, T.; Söderling, E.; Haukioja, A. Probiotic intervention influences the salivary levels of Matrix Metalloproteinase (MMP)-9 and Tissue Inhibitor of metalloproteinases (TIMP)-1 in healthy adults. Arch. Oral Biol. 2018, 85, 58–63. [Google Scholar] [CrossRef] [Green Version]
- Keller, M.K.; Brandsborg, E.; Holmstrom, K.; Twetman, S. Effect of tablets containing probiotic candidate strains on gingival inflammation and composition of the salivary microbiome: A randomised controlled trial. Benef. Microbes 2018, 9, 487–494. [Google Scholar] [CrossRef]
- Krasse, P.; Carlsson, B.; Dahl, C.; Paulsson, A.; Nilsson, A.; Sinkiewicz, G. Decreased gum bleeding and reduced gingivitis by the probiotic Lactobacillus reuteri. Swed. Dent. J. 2006, 30, 55–60. [Google Scholar]
- Kuka, G.I.; Gursoy, H.; Emekli-Alturfan, E.; Ustundag, U.V.; Kuru, B. Evaluation of nitric oxide levels in chronic periodontitis patients treated with initial periodontal therapy and probiotic food supplements: A double blind, randomized controlled clinical trial. Biotechnol. Biotechnol. Equip. 2019, 33, 974–979. [Google Scholar] [CrossRef]
- Kuru, B.E.; Laleman, I.; Yalnızoğlu, T.; Kuru, L.; Teughels, W. The Influence of a Bifidobacterium animalis Probiotic on Gingival Health: A Randomized Controlled Clinical Trial. J. Periodontol. 2017, 88, 1115–1123. [Google Scholar] [CrossRef]
- Laleman, I.; Yilmaz, E.; Ozcelik, O.; Haytac, C.; Pauwels, M.; Herrero, E.R.; Slomka, V.; Quirynen, M.; Alkaya, B.; Teughels, W. The effect of a streptococci containing probiotic in periodontal therapy: A randomized controlled trial. J. Clin. Periodontol. 2015, 42, 1032–1041. [Google Scholar] [CrossRef] [PubMed]
- Laleman, I.; Pauwels, M.; Quirynen, M.; Teughels, W. A dual-strain Lactobacilli reuteri probiotic improves the treatment of residual pockets: A randomized controlled clinical trial. J. Clin. Periodontol. 2020, 47, 43–53. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, J.-K.; Kim, S.-J.; Ko, S.-H.; Ouwehand, A.C.; Ma, D.S. Modulation of the host response by probiotic Lactobacillus brevis CD2 in experimental gingivitis. Oral Dis. 2015, 21, 705–712. [Google Scholar] [CrossRef] [PubMed]
- Mayanagi, G.; Kimura, M.; Nakaya, S.; Hirata, H.; Sakamoto, M.; Benno, Y.; Shimauchi, H. Probiotic effects of orally administered Lactobacillus salivarius WB21-containing tablets on periodontopathic bacteria: A double-blinded, placebo-controlled, randomized clinical trial. J. Clin. Periodontol. 2009, 36, 506–513. [Google Scholar] [CrossRef]
- Swarna Meenakshi, S.; Varghese, S. Adjunctive effect of probiotic (Lactobacillus casei Shirota) to scaling and root planing in the management of chronic periodontitis. Drug Invent. Today 2018, 10, 1381–1386. [Google Scholar]
- Mitic, K.A. Probiotics and Oral Health Research. Res. J. Pharm. Biol. Chem. Sci. 2017, 8, 1021–1029. [Google Scholar]
- Morales, A.; Carvajal, P.; Silva, N.; Hernandez, M.; Godoy, C.; Rodriguez, G.; Cabello, R.; Garcia-Sesnich, J.; Hoare, A.; Diaz, P.I.; et al. Clinical Effects of Lactobacillus rhamnosus in Non-Surgical Treatment of Chronic Periodontitis: A Randomized Placebo-Controlled Trial With 1-Year Follow-Up. J. Periodontol. 2016, 87, 944–952. [Google Scholar] [CrossRef] [Green Version]
- Nadkerny, P.V.; Ravishankar, P.L.; Pramod, V.; Agarwal, L.A.; Bhandari, S. A comparative evaluation of the efficacy of probiotic and chlorhexidine mouthrinses on clinical inflammatory parameters of gingivitis: A randomized controlled clinical study. J. Indian Soc. Periodontol. 2015, 19, 633–639. [Google Scholar] [CrossRef]
- De Luca, P.; Carvalho, G.; Franco, A.; Kreve, S.; Avila, G.; Dias, S. Zirconia-Reinforced Lithium Silicate Biocompatibility Polished in Different Stages–An In Vitro Study. J. Int. Dent. Med. Res. 2018, 11, 759–764. [Google Scholar]
- Pelekos, G.; Acharya, A.; Eiji, N.; Hong, G.; Leung, W.K.; McGrath, C. Effects of adjunctive probiotic L. reuteri lozenges on S/RSD outcomes at molar sites with deep pockets. J. Clin. Periodontol. 2020, 47, 1098–1107. [Google Scholar] [CrossRef]
- Penala, S.; Kalakonda, B.; Pathakota, K.; Jayakumar, A.; Koppolu, P.; Lakshmi, B.; Pandey, R.; Mishra, A. Efficacy of local use of probiotics as an adjunct to scaling and root planing in chronic periodontitis and halitosis: A randomized controlled trial. J. Res. Pharm. Pract. 2016, 5, 86. [Google Scholar] [CrossRef] [PubMed]
- Pudgar, P.; Povšič, K.; Čuk, K.; Seme, K.; Petelin, M.; Gašperšič, R. Probiotic strains of Lactobacillus brevis and Lactobacillus plantarum as adjunct to non-surgical periodontal therapy: 3-month results of a randomized controlled clinical trial. Clin. Oral Investig. 2021, 25, 1411–1422. [Google Scholar] [CrossRef] [PubMed]
- Tomasello, G.; Tralongo, P.; Amoroso, F.; Damiani, P.; Sinagra, E.; Noto, M.; Arculeo, V.M.; Zein, R.J.; Saad, W.; Jurjus, A.; et al. Dysmicrobism, Inflammatory Bowel Disease and Thyroiditis: Analysis of the Literature. J. Biol. Regul. Homeost. Agents 2015, 29, 265–272. [Google Scholar] [PubMed]
- Sajedinejad, N.; Paknejad, M.; Houshmand, B.; Sharafi, H.; Jelodar, R.; Zahiri, H.S.; Noghabi, K.A. Lactobacillus salivarius NK02: A Potent Probiotic for Clinical Application in Mouthwash. Probiotics Antimicrob. Proteins 2018, 10, 485–495. [Google Scholar] [CrossRef]
- Scaryia, L.; Nagarathna, D.V.; Varghese, M. Probiotics in periodontal therapy. Int. J. Pharma Bio Sci. 2015, 6, 242–250. [Google Scholar]
- Schlagenhauf, U.; Jakob, L.; Eigenthaler, M.; Segerer, S.; Jockel-Schneider, Y.; Rehn, M. Regular consumption of Lactobacillus reuteri-containing lozenges reduces pregnancy gingivitis: An RCT. J. Clin. Periodontol. 2016, 43, 948–954. [Google Scholar] [CrossRef] [Green Version]
- Schlagenhauf, U.; Rehder, J.; Gelbrich, G.; Jockel-Schneider, Y. Consumption of Lactobacillus reuteri-containing lozenges improves periodontal health in navy sailors at sea: A randomized controlled trial. J. Periodontol. 2020, 91, 1328–1338. [Google Scholar] [CrossRef] [Green Version]
- Shah, M.P.; Gujjari, S.K.; Chandrasekhar, V.S. Evaluation of the effect of probiotic (inersan(R)) alone, combination of probiotic with doxycycline and doxycycline alone on aggressive periodontitis—A clinical and microbiological study. J. Clin. Diagn. Res. 2013, 7, 595–600. [Google Scholar] [CrossRef]
- Shah, M.P.; Gujjari, S.K.; Chandrasekhar, V.S. Long-term effect of Lactobacillus brevis CD2 (Inersan((R))) and/or doxycycline in aggressive periodontitis. J. Indian Soc. Periodontol. 2017, 21, 341–343. [Google Scholar] [CrossRef]
- Shetty, S.; Srigiri, S.K.; Sheikh, K.H. A Comparative Clinical, Microbiological and Biochemical Evaluation of Guided Periodontal Pocket Recolonisation (GPR) using Synbiotics as an Adjunct to Scaling and Root Planing in Patients with Chronic Periodontitis: A Pilot Project. Int. J. Med. Res. Health Sci. 2020, 9, 20–32. [Google Scholar] [CrossRef]
- Shimauchi, H.; Mayanagi, G.; Nakaya, S.; Minamibuchi, M.; Ito, Y.; Yamaki, K.; Hirata, H. Improvement of periodontal condition by probiotics with Lactobacillus salivarius WB21: A randomized, double-blind, placebo-controlled study. J. Clin. Periodontol. 2008, 35, 897–905. [Google Scholar] [CrossRef] [PubMed]
- Sinkiewicz, G.; Cronholm, S.; Ljunggren, L.; Dahlen, G.; Bratthall, G. Influence of dietary supplementation with Lactobacillus reuteri on the oral flora of healthy subjects. Swed. Dent. J. 2010, 34, 197–206. [Google Scholar]
- Slawik, S.; Staufenbiel, I.; Schilke, R.; Nicksch, S.; Weinspach, K.; Stiesch, M.; Eberhard, J. Probiotics affect the clinical inflammatory parameters of experimental gingivitis in humans. Eur. J. Clin. Nutr. 2011, 65, 857–863. [Google Scholar] [CrossRef] [PubMed]
- Sinulingga, R.T.N.; Soeroso, Y.; Lessang, R.; Sastradipura, D.F.S. Probiotic Lactobacillus reuteri effect’s on the levels of interleukin-4 in periodontitis patients after scaling and root planing. Int. J. Appl. Pharm. 2020, 12, 66–68. [Google Scholar] [CrossRef]
- Staab, B.; Eick, S.; Knöfler, G.; Jentsch, H. The influence of a probiotic milk drink on the development of gingivitis: A pilot study. J. Clin. Periodontol. 2009, 36, 850–856. [Google Scholar] [CrossRef]
- Suzuki, N.; Tanabe, K.; Takeshita, T.; Yoneda, M.; Iwamoto, T.; Oshiro, S.; Yamashita, Y.; Hirofuji, T. Effects of oil drops containing Lactobacillus salivarius WB21 on periodontal health and oral microbiota producing volatile sulfur compounds. J. Breath Res. 2012, 6, 017106. [Google Scholar] [CrossRef]
- Teughels, W.; Durukan, A.; Ozcelik, O.; Pauwels, M.; Quirynen, M.; Haytac, M.C. Clinical and microbiological effects of Lactobacillus reuteri probiotics in the treatment of chronic periodontitis: A randomized placebo-controlled study. J. Clin. Periodontol. 2013, 40, 1025–1035. [Google Scholar] [CrossRef] [Green Version]
- Theodoro, L.H.; Claudio, M.M.; Nuernberg, M.A.A.; Miessi, D.M.J.; Batista, J.A.; Duque, C.; Garcia, V.G. Effects of Lactobacillus reuteri as an adjunct to the treatment of periodontitis in smokers: Randomised clinical trial. Benef. Microbes 2019, 10, 375–384. [Google Scholar] [CrossRef]
- Tobita, K.; Watanabe, I.; Tomokiyo, M.; Saito, M. Effects of heat-treated Lactobacillus crispatus KT-11 strain consumption on improvement of oral cavity environment: A randomised double-blind clinical trial. Benef. Microbes 2018, 9, 585–592. [Google Scholar] [CrossRef]
- Toiviainen, A.; Jalasvuori, H.; Lahti, E.; Gursoy, U.; Salminen, S.; Fontana, M.; Flannagan, S.; Eckert, G.; Kokaras, A.; Paster, B.; et al. Impact of orally administered lozenges with Lactobacillus rhamnosus GG and Bifidobacterium animalis subsp. lactis BB-12 on the number of salivary mutans streptococci, amount of plaque, gingival inflammation and the oral microbiome in healthy adults. Clin. Oral Investig. 2015, 19, 77–83. [Google Scholar] [CrossRef] [Green Version]
- Twetman, S.; Derawi, B.; Keller, M.; Ekstrand, K.; Yucel-Lindberg, T.; Stecksén-Blicks, C. Short-term effect of chewing gums containing probiotic Lactobacillus reuteri on the levels of inflammatory mediators in gingival crevicular fluid. Acta Odontol. Scand. 2009, 67, 19–24. [Google Scholar] [CrossRef]
- Vicario, M.; Santos, A.; Violant, D.; Nart, J.; Giner, L. Clinical changes in periodontal subjects with the probiotic Lactobacillus reuteri Prodentis: A preliminary randomized clinical trial. ACTA Odontol. Scand. 2013, 71, 813–819. [Google Scholar] [CrossRef]
- Vivekananda, M.R.; Vandana, K.L.; Bhat, K.G. Effect of the probiotic Lactobacilli reuteri (Prodentis) in the management of periodontal disease: A preliminary randomized clinical trial. J. Oral Microbiol. 2010, 2, 5344. [Google Scholar] [CrossRef]
- Vohra, F.; Bukhari, I.A.; Sheikh, S.A.; Albaijan, R.; Naseem, M.; Hussain, M. Effectiveness of scalling and root plannng with and without adjunct probiotic therapy. J. Periodontol. 2020, 91, 1177–1185. [Google Scholar] [CrossRef] [PubMed]
- Oda, Y.; Furutani, C.; Mizota, Y.; Wakita, A.; Mimura, S.; Kihara, T.; Ohara, M.; Okada, Y.; Okada, M.; Nikawa, H. Effect of bovine milk fermented with lactobacillus rhamnosus l8020 on periodontal disease in individuals with intellectual disability: A randomized clinical trial. J. Appl. Oral Sci. 2019, 27, 1–9. [Google Scholar] [CrossRef] [Green Version]
- Corbet, E.; Smales, R. Oral diagnosis and treatment planning: Part 6. Preventive and treatment planning for periodontal disease. Br. Dent. J. 2012, 213, 277–284. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lang, N.P.; Bartold, P.M. Periodontal health. J. Periodontol. 2018, 89, S9–S16. [Google Scholar] [CrossRef] [Green Version]
- Butera, A.; Gallo, S.; Maiorani, C.; Molino, D.; Chiesa, A.; Preda, C.; Esposito, F.; Scribante, A. Probiotic alternative to chlorhexidine in periodontal therapy: Evaluation of clinical and microbiological parameters. Microorganisms 2021, 9, 69. [Google Scholar] [CrossRef]
- Allaker, R.P.; Stephen, A.S. Use of Probiotics and Oral Health. Curr. Oral Health Rep. 2017, 4, 309–318. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mu, Q.; Tavella, V.J.; Luo, X.M. Role of Lactobacillus reuteri in Human Health and Diseases. Front. Microbiol. 2018, 9, 757. [Google Scholar] [CrossRef]
- Romani Vestman, N.; Chen, T.; Lif Holgerson, P.; Öhman, C.; Johansson, I. Oral Microbiota Shift after 12-Week Supplementation with Lactobacillus reuteri DSM 17938 and PTA 5289; A Randomized Control Trial. PLoS ONE 2015, 10, e0125812. [Google Scholar] [CrossRef]
- Narwal, A. Probiotics in Dentistry—A Review. J. Nutr. Food Sci. 2011, 1. [Google Scholar] [CrossRef]
- Bartlett, A.; Gullickson, R.G.; Singh, R.; Ro, S.; Omaye, S.T. The link between oral and gut microbiota in inflammatory bowel disease and a synopsis of potential salivary biomarkers. Appl. Sci. 2020, 10, 6421. [Google Scholar] [CrossRef]
- Laleman, I.; Pauwels, M.; Quirynen, M.; Teughels, W. The usage of a lactobacilli probiotic in the non-surgical therapy of peri-implantitis: A randomized pilot study. Clin. Oral Implant. Res. 2020, 31, 84–92. [Google Scholar] [CrossRef]
- Olsen, I.; Yamazaki, K. Can oral bacteria affect the microbiome of the gut? J. Oral Microbiol. 2019, 11, 1586422. [Google Scholar] [CrossRef] [Green Version]
- Çaglar, E.; Kargul, B.; Tanboga, I. Bacteriotherapy and probiotics’ role on oral health. Oral Dis. 2005, 11, 131–137. [Google Scholar] [CrossRef]
- Kim, S.-K.; Guevarra, R.B.; Kim, Y.-T.; Kwon, J.; Kim, H.; Cho, J.H.; Kim, H.B.; Lee, J.-H. Role of Probiotics in Human Gut Microbiome-Associated Diseases. J. Microbiol. Biotechnol. 2019, 29, 1335–1340. [Google Scholar] [CrossRef]
- Belkaid, Y.; Harrison, O.J. Homeostatic Immunity and the Microbiota. Immunity 2017, 46, 562–576. [Google Scholar] [CrossRef] [Green Version]
- Wu, H.-J.; Wu, E. The role of gut microbiota in immune homeostasis and autoimmunity. Gut Microbes 2012, 3, 4–14. [Google Scholar] [CrossRef] [Green Version]
- Carra, M.C.; Detzen, L.; Kitzmann, J.; Woelber, J.P.; Ramseier, C.A.; Bouchard, P. Promoting behavioural changes to improve oral hygiene in patients with periodontal diseases: A systematic review. J. Clin. Periodontol. 2020, 47 (Suppl. S2), 72–89. [Google Scholar] [CrossRef] [Green Version]
- Bouchard, P.; Carra, M.C.; Boillot, A.; Mora, F.; Rangé, H. Risk factors in periodontology: A conceptual framework. J. Clin. Periodontol. 2017, 44, 125–131. [Google Scholar] [CrossRef] [PubMed]
- Singla, S.; Gupta, P.; Lehl, G.; Talwar, M. Effects of Reinforced Oral Hygiene Instruction Program With and Without Professional Tooth Cleaning on Plaque Control and Gingival Health of Orthodontic Patients Wearing Multibracket Appliances. J. Indian Orthod. Soc. 2019, 53, 272–277. [Google Scholar] [CrossRef]
- Newton, J.T.; Asimakopoulou, K. Managing oral hygiene as a risk factor for periodontal disease: A systematic review of psychological approaches to behaviour change for improved plaque control in periodontal management. J. Clin. Periodontol. 2015, 42, S36–S46. [Google Scholar] [CrossRef] [PubMed]
- Barros, S.P.; Williams, R.; Offenbacher, S.; Morelli, T. Gingival crevicular fluid as a source of biomarkers for periodontitis. Periodontol. 2000 2016, 70, 53–64. [Google Scholar] [CrossRef]
- Teles, R.; Sakellari, D.; Teles, F.; Konstantinidis, A.; Kent, R.; Socransky, S.; Haffajee, A. Relationships among gingival crevicular fluid biomarkers, clinical parameters of periodontal disease, and the subgingival microbiota. J. Periodontol. 2010, 81, 89–98. [Google Scholar] [CrossRef]
- Bourgeois, D.; Inquimbert, C.; Ottolenghi, L.; Carrouel, F. Periodontal Pathogens as Risk Factors of Cardiovascular Diseases, Diabetes, Rheumatoid Arthritis, Cancer, and Chronic Obstructive Pulmonary Disease-Is There Cause for Consideration? Microorganisms 2019, 7, 424. [Google Scholar] [CrossRef] [Green Version]
- Brennan, C.A.; Garrett, W.S. Fusobacterium nucleatum—Symbiont, opportunist and oncobacterium. Nat. Rev. Microbiol. 2019, 17, 156–166. [Google Scholar] [CrossRef]
- Javed, F.; Ahmed, H.B.; Saeed, A.; Mehmood, A.; Bain, C. Whole Salivary Interleukin-6 and Matrix Metalloproteinase-8 Levels in Patients with Chronic Periodontitis With and Without Prediabetes. J. Periodontol. 2014, 85, e130–e135. [Google Scholar] [CrossRef] [Green Version]
- Ebersole, J.L.; Dawson, D.R.; Morford, L.A.; Peyyala, R.; Miller, C.S.; Gonzaléz, O.A. Periodontal disease immunology: “Double indemnity” in protecting the host. Periodontol. 2000 2013, 62, 163–202. [Google Scholar] [CrossRef] [Green Version]
- Zhang, L.; Li, X.; Yan, H.; Huang, L. Salivary matrix metalloproteinase (MMP)-8 as a biomarker for periodontitis: A PRISMA-compliant systematic review and meta-analysis. Medicine 2018, 97, e9642. [Google Scholar] [CrossRef]
- Al-Majid, A.; Alassiri, S.; Rathnayake, N.; Tervahartiala, T.; Gieselmann, D.-R.; Sorsa, T. Matrix Metalloproteinase-8 as an Inflammatory and Prevention Biomarker in Periodontal and Peri-Implant Diseases. Int. J. Dent. 2018, 2018, 7891323. [Google Scholar] [CrossRef]
- Sorsa, T.; Alassiri, S.; Grigoriadis, A.; Räisänen, I.T.; Pärnänen, P.; Nwhator, S.O.; Gieselmann, D.-R.; Sakellari, D. Active MMP-8 (aMMP-8) as a Grading and Staging Biomarker in the Periodontitis Classification. Diagnostics 2020, 10, 61. [Google Scholar] [CrossRef] [Green Version]
- Pan, W.; Wang, Q.; Chen, Q. The cytokine network involved in the host immune response to periodontitis. Int. J. Oral Sci. 2019, 11, 30. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stadler, A.F.; Angst, P.D.M.; Arce, R.M.; Gomes, S.C.; Oppermann, R.V.; Susin, C. Gingival crevicular fluid levels of cytokines/chemokines in chronic periodontitis: A meta-analysis. J. Clin. Periodontol. 2016, 43, 727–745. [Google Scholar] [CrossRef] [PubMed]
- Teles, R.P.; Likhari, V.; Socransky, S.S.; Haffajee, A.D. Salivary cytokine levels in subjects with chronic periodontitis and in periodontally healthy individuals: A cross-sectional study. J. Periodontal Res. 2009, 44, 411–417. [Google Scholar] [CrossRef] [Green Version]
- Goutoudi, P.; Diza, E.; Arvanitidou, M. Effect of periodontal therapy on crevicular fluid interleukin-6 and interleukin-8 levels in chronic periodontitis. Int. J. Dent. 2012, 2012, 362905. [Google Scholar] [CrossRef] [Green Version]
- Ross, J.H.; Hardy, D.C.; Schuyler, C.A.; Slate, E.H.; Mize, T.W.; Huang, Y. Expression of periodontal interleukin-6 protein is increased across patients with neither periodontal disease nor diabetes, patients with periodontal disease alone and patients with both diseases. J. Periodontal Res. 2010, 45, 688–694. [Google Scholar] [CrossRef] [PubMed]
- Checchi, L.; Montevecchi, M.; Checchi, V.; Zappulla, F. The Relationship Between Bleeding on Probing and Subgingival Deposits. An Endoscopical Evaluation. Open Dent. J. 2009, 3, 154–160. [Google Scholar] [CrossRef] [Green Version]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Author, Year, Country | Study Sample Characteristics | Probiotic Formulation | Treatment Duration/ Immediate Follow-Up | Mode of Probiotic Delivery | Other Treatments | Oral Hygiene Instructions | Outcomes Investigated | Key Findings | ||
|---|---|---|---|---|---|---|---|---|---|---|
| Disease Status | Sample Size | |||||||||
| Probiotic | Control | |||||||||
| Alkaya, 2016 [53] Turkey | Gingivitis | 20 | 20 | B. megaterium, B. pumulus, B. subtilis | 8 weeks/ 8 weeks | Toothpaste, mouth rinse, and toothbrush | Supragingival scaling and/or oral prophylaxis | Yes | PlI *, GI *, PPD *, BOP * | No statistically significant difference attributed to probiotic use in gingivitis patients. |
| Alshareef, 2020 [54] Saudi Arabia | Periodontitis | 15 | 10 | B. bifidum, L. acidophilus, L. casei, L. rhamnosus, L. salivarius | 30 days/ 30 days | Lozenge | SRP | Yes | PlI *, CAL *, PPD *, GBI +, GCF *, MMP-8 * | Statistically significant improvement in GBI and greater improvement in GCF with probiotic use. |
| Bazyar, 2020 [55] Iran | Periodontitis | 23 | 24 | Bifidobacterium, B. longum, L. acidophilus, L. bulgaricus, L. casei, L. rhamnosus, S. thermophilus | 8 weeks/ 8 weeks | Capsule | NSPT | No | PlI +, CAL+, BOP +, PPD *, IL1β +, MDA +, TAC +, SOD *, CAT, GPx + | Probiotic supplementation and NSPT in type 2 diabetes patients with chronic periodontitis may improve antioxidant, anti-inflammatory, and periodontal parameters. |
| Bollero, 2017 [56] Italy | Gingivitis | 19 | 21 | B. animalis, B. bifidum, L. acidophilus, L. delbrueckii, L. plantarum, L. reuteri, L. lactis, S. thermophilus | 1 week/ 1 week | Mouthwash | None | Not mentioned | BOP +, PCR + | Probiotic mouthwash may serve as an additional prophylactic to standard oral hygiene procedures. |
| Boyeena, 2019 [57] India | Periodontitis | 10 | 10 | B. bifidum, B. longum, L. acidophilus, L. rhamnosus | Once/ 45 days | Paste | 1) SRP + tetracycline fibers 2) SRP + tetracycline fibers + Probiotic | Yes | PlI *, PPD +, SBI +, total bacteria * | Probiotic and tetracycline may act synergistically in the treatment of periodontitis. |
| Chandra, 2016 [58] India | Periodontitis | 28 | 27 | S. boulardii | Once/ 1 week | Paste | SRP | Yes | PI, MGI *, CAL +, PPD + | S. boulardii and SRP significantly improved periodontal disease parameters compared to SRP alone. |
| Deshmukh, 2017 [59] India | Healthy | 15 | 15 | Bifidobacterium, Lactobacillus, S. Boulardii | 14 days/ 14 days | Sachet | Supragingival scaling + chlorhexidine mouthwash control | Yes | PlI *, GI * | Probiotic mouthwashes have similar efficacy to chlorhexidine and are a potential alternative with fewer side effects. |
| Dhaliwal, 2017 [60] India | Periodontitis | 14 | 13 | B. mesentericus, C. butyricum, L. sporogenes, S. faecalis | 21 days/ 30 days | Lozenge | SRP | Not mentioned | PI *, GI *, PPD *, RAL *, A. actinomycetemcomitans, P. gingivalis +, P. intermedia | Probiotics may be used as an adjunctive treatment for the management of chronic periodontitis. |
| Duarte, 2019 [61] United Arab Emirates | Gingivitis | 5 | 5 | S. oralis, S. rattus, S. uberis | 30 days/ 30 days | Mouthwash | 1) SRP 2) SRP + chlorhexidine mouthwash | Yes | GI *, OHI +, PI * | Changes may be attributed to type and duration of intervention. Probiotics showed similar efficacy to chlorhexidine and better results compared to SRP alone. |
| Elsadek, 2020 [62] Saudi Arabia | Periodontitis | 19 | 19 | L. reuteri | 3 weeks/ 12 weeks | Lozenge | 1) RSD + Photodynamic therapy 2) RSD alone | Yes | CAL *, BOP *, PPD *, PS*, P. gingivalis +, T. Forsythia +, T. denticola + | Photodynamic therapy showed greater benefits for deeper periodontal pockets. Probiotics reduced bacterial counts more than RSD alone. |
| Ercan, 2020 [63] Turkey | Gingivitis | 40 | 40 | B. lactis, B. longum, E. faecium, L. acidophilus, L. plantarum, S. thermophilus, | 1 month/ 1 month | Chewing tablet | SRP | Yes | PlI+, GI *, GCF *, IL-6 +, IL8 +, IL10 + | Adjunct synbiotics improved clinical and immunological outcomes in gingivitis patients, irrespective of smoking status. |
| Grusovin, 2019 [64] Italy | Periodontitis | 10 | 10 | L. reuteri | 3 months, 3-month washout, 3 months/ 3 months, 9 months | Lozenge | FM-GBT | Yes | BOP +, PPD +, PAL +, tooth survival | Probiotics improved clinical parameters with periodontal maintenance therapy. |
| Hallström, 2013 [42] Sweden | Healthy | 9 | 9 | L. reuteri | 3 weeks/ 3 weeks | Lozenge | None | No | PI, GI, BOP, GCF, IL-1β *, IL6, IL8 *, IL10, IL-18 *, MIP-1β *, TNF-α, A. actinomycetemcomitan, A. naeslundii, C. rectus, F. alocis, F. nucleatum *, L. reuteri, L. fermentum, P. micra, P. endodontis, P. intermedia, P. gingivalis, S. intermedia, S. mutans, S. oralis *, S. sanguinis, T. forsythia, T. denticola, V. parvula * | Probiotic supplementation did not significantly affect plaque accumulation, inflammatory reactions in the gingiva, and the microbiological composition in healthy individuals with experimental gingivitis. |
| Ikram, 2018 [65] Pakistan | Periodontitis | 15 | 15 | L. reuteri | 3 months/ 4 months | Sachet | SRP + amoxicillin + metronidazole | Yes | PlI *, CAL *, BOP *, PPD * | Probiotics showed similar efficacy in the improvement of periodontal clinical outcomes as antibiotics. |
| Ikram, 2019 [66] Pakistan | Periodontitis | 14 | 14 | L. reuteri | 12 weeks/ 12 weeks | Sachet | SRP | Yes | PlI *, CAL +, BOP +, PPD + | Probiotics may be used as an adjunctive treatment with SRP to treat chronic periodontitis. |
| Ince, 2015 [67] Turkey | Periodontitis | 15 | 15 | L. reuteri | 3 weeks/ 3 weeks | Lozenge | SRP | Yes | PlI +, GI +, BOP +, PPD +, CAL +, GCF *, MMP-8 +, TIMP-1 + | Adjuvant probiotic treatment improved clinical and immunological outcomes in periodontitis patients. |
| Iniesta, 2012 [43] Spain | Gingivitis | 20 | 20 | L. reuteri | 4 weeks/ 4 weeks | Chewing tablet | None | No | PlI, GI, Lactobacillus spp., A. actinomycetemcomitan, C. rectus, Capnocytophaga spp., E. corrodens, F. nucleatum, P. micra, P. intermedia, P. gingivalis, Tannerella forsythia, total bacteria | Probiotic administration reduced subgingival periodontopathogen count. |
| Invernici, 2018 [68] Brazil | Periodontitis | 20 | 21 | B. lactis | 30 days/ 30 days | Lozenge | SRP | Yes | PlI +, CAL +, PPD +, BOP +, REC, IL-1β +, IL-8 +, IL-10 *, B. animalis +, | Probiotic supplementation in addition to SRP may improve clinical, microbiological, and immunological outcomes in generalized chronic periodontitis patients. |
| Iwasakia, 2016 [69] Japan | Periodontitis | 19 | 17 | L. plantarum | 12 weeks/ 12 weeks | Capsule | SPT | Not mentioned | PlI, GI, BOP, PPD + | Chronic periodontitis patients with adjunctive probiotic treatment may lead to improvements in periodontal pockets. |
| Jagadeesh, 2017 [70] India | Gingivitis | 15 | 15 | B. coagulans | 3 weeks/ 3 weeks | Chewing tablet | None | Not mentioned | PlI, GI *, BOP +, GPx | Probiotic use led to a statistically significant decrease in BOP. |
| Jäsberg, 2018 [71] Finland | Healthy | 29 | 31 | B. animalis, L. rhamnosus | 4 weeks/ 4 weeks | Lozenge | None | Not mentioned | PlI +, GI +, MMP-8, MMP-9 +, TIMP-1 +, S. mutans, lactobacilli | Probiotics may immunomodulate the oral cavity. |
| Keller, 2018 [72] Denmark | Gingivitis | 23 | 24 | L. curvatus, L. rhamnosus | 4 weeks/ 4 weeks | Tablet | None | No | PlI *, BOP +, GCF +, IL-1β, IL-6, IL-8, IL-10, TNF-α | Probiotic use may improve gingival health without affecting the oral microbiome and immune response. |
| Krasse, 2005 [73] Sweden | Gingivitis | 20 | 18 | L. reuteri | 14 days/ 14 days | Chewing gum | None | Yes | PlI +, GI +, L. reuteri +, Total lactobacillus + | L. reuteri can reduce PlI and GI in gingivitis patients. |
| Kuka, 2019 [74] Turkey | Periodontitis | 18 | 18 | L. reuteri | 3 weeks/ 12 weeks | Tablet | IPT | Yes | BOP +, PPD +, GCF +, NO + | Probiotics may be an adjunct to IPT. NO in GCF is a potential inflammatory marker in periodontal diseases. |
| Kuru, 2017 [75] Turkey | Healthy | 26 | 25 | B. animalis | 4 weeks/ 4 weeks | Yogurt | None | Yes | PlI +, GI +, BOP +, PPD +, GCF +, IL-1β + | Probiotics improved clinical and immunological outcomes compared to controls after a 5-day non-brushing period. |
| Laleman, 2015 [76] Turkey | Periodontitis | 24 | 24 | S. oralis, S. rattus, S. uberis | 12 weeks/ 12 weeks | Tablet | SRP | Not mentioned | CAL *, BOP *, PPD *, REC *, F. nucleatum *, P. gingivalis *, P. intermedia +, T. forsythia * | Probiotic formulation used did not show statistically significant improvements in clinical or microbiological outcomes. |
| Laleman, 2019 [77] Belgium | Periodontitis | 19 | 20 | L. reuteri | 12 weeks/12 weeks | Lozenge | NSPT | Yes | PlI *, CAL *, BOP *, PPD +, REC *, A. actinomycetemcomitans, F. nucleatum, P. intermedia, P. gingivalis | Adjunctive use of probiotics after NSPT reduced PPD and the percentage of sites in need of surgery. |
| Lee, 2015 [78] Korea | Healthy | 14 | 16 | L. brevis | 14 days/ 14 days | Lozenge | Scaling and polishing | Yes | PlI *, GI *, BOP *, NO, MMP-8, PGE2 * | Probiotic supplementation may decrease inflammatory cascades through NO and PGE2. |
| Mayanagi, 2009 [79] Japan | Periodontitis | 34 | 32 | L. salivarius | 8 weeks/ 8 weeks | Tablet | None | No | A. actinomycetemcomitans, P. intermedia, P. gingivalis, T. forsythia +, T. denticola, total bacteria * | Probiotics decreased the subgingival T. forsythia count at 4 and 8 weeks and the total bacteria count at 4 weeks. |
| Meenakshi, 2018 [80] India | Periodontitis | 10 | 10 | L. casei | 1 month/ 1 month | Drink | SRP | No | PlI +, GI +, CAL +, PPD+, total bacteria+ | Probiotics as an adjunct to SRP improved clinical outcomes and reduced total bacterial count. |
| Mitic, 2017 [81] Macedonia | Periodontitis | 15 | 15 | B. bifidum, B. coagulans, L. acidophilus, L. bulgaricus, S. thermophilus | 15 days/ 1 month | Lozenge | SRP | Yes | PlI *, GI *, GBI *, CAL *, PPD +, anaerobic bacterial count+ | Probiotics may improve clinical outcomes and bacterial count in periodontitis patients. |
| Montero, 2017 [14] Spain | Gingivitis | 30 | 29 | L. brevis, L. plantarum, P. acidilactici | 6 weeks/ 6 weeks | Chewing tablet | PMPR | Yes | PlI *, GI *, AngBs +, A. actinomycetemcomitans *, C. rectus, Fusobacterium spp., P. gingivalis, T. forsythia * | Decreased number of sites with severe inflammation compared to placebo group in gingivitis patients. Decreased T. forsythia count. |
| Morales, 2016 [82] Chile | Periodontitis | 14 | 14 | L. rhamnosus | 3 months/ 3 months | Sachet | SRP | Yes | CAL *, PlI *, BOP, PPD * | Probiotic use improved clinical symptoms similar to SRP alone. |
| Morales, 2017 [10] Chile | Periodontitis | 16 | 15 | L. rhamnosus | 3 months/ 9 months | Sachet | 1) SRP 2) SRP + Antibiotic | Yes | CAL *, BOP, PPD *, PA *, A. actinomycetemcomitans, P. gingivalis *, T. forsythia, total bacteria * | Probiotic and antibiotic groups had similar clinical and microbiological improvements to placebo. |
| Nadkerny, 2015 [83] India | Gingivitis | 15 | 15 | B. longum, L. acidophilus, L. rhamnosus, L. sporogenes, S. boulardii | 4 weeks/ 4 weeks | Sachet | Scaling and polishing 1) Chlorhexidine 2) Normal saline | Yes | PlI +, GI +, OHI-S + | Probiotic mouthwash effectively reduced plaque accumulation and gingival inflammation. |
| Nasry, 2018 [84] Egypt | Gingivitis | 20 | 20 | L. rhamnosus | 2 weeks/ 2 weeks | Spray | Scaling and polishing | Yes | PlI +, GI +, SI + | Miswak and probiotic formulation led to the greatest reduction in plaque and gingival indices. |
| Pelekos, 2019 [34] Hong Kong | Periodontitis | 21 | 20 | L. reuteri | 28 days/ 90 days | Lozenge | NSPT | Yes | CAL *, BOP *, PPD * | Adjunctive use of probiotics did not show increased effectiveness compared to control. |
| Pelekos, 2020 [85] Hong Kong | Periodontitis | 20 | 20 | L. reuteri | 28 days/ 90 days | Lozenge | NSPT | Yes | CAL+, BOP *, PPD + | Probiotic supplementation improved periodontal pockets ≥ 5 mm and CAL. |
| Penala, 2015 [86] India | Periodontitis | 15 | 14 | L. reuteri, L. salivarius | 15 days/ 3 months | Capsule & Mouthwash | SRP | Yes | PlI +, MGI +, GBI +, PPD *, CAL *, BANA, ORG | Probiotic use improved clinical outcomes and oral malodor parameters. |
| Pudgar, 2020 [87] Slovenia | Periodontitis | 20 | 20 | L. brevis, L. plantarum | Once (gel) 3 months (lozenge)/ 3 months | Local gel & Lozenge | SRP | Yes | DS *, PlI *, CAL *, BOP *, PPD *, REC*, GBI * | Probiotic and control groups both had significant clinical improvements, but there was no statistically significant difference between the two groups. |
| Sabatini, 2017 [88] Italy | Gingivitis | 40 | 40 | L. reuteri | 30 days/ 30 days | Tablet | None | Yes | PlI +, BOP + | Probiotics were effective in reducing plaque and BOP in type 2 diabetes patients with gingivitis. |
| Sajedinejad, 2017 [89] Iran | Periodontitis | 10 | 10 | L. salivarius | 4 weeks/ 4 weeks | Mouthwash | SRP | Yes | PlI, GI +, BOP +, PPD *, A. actinomycetemcomitans + | Probiotic use improved clinical and microbiological outcomes. |
| Scariya, 2015 [90] India | Gingivitis and Periodontitis | 14 | 14 | S. salivarius | 30 days/ 30 days | Tablet | None | Yes | PlI +, GI +, SBI +, PPD+ | Probiotic use improved clinical outcomes compared to controls. |
| Schlagenhauf, 2018 [91] Germany | Gingivitis | 24 | 21 | L. reuteri | Within 2 days after delivery (41.9 ± 16.0 days) | Lozenge | None | No | PlI +, GI +, TNF-α | Probiotics may be a useful adjunct for pregnancy-related gingivitis. |
| Schlagenhauf, 2020 [92] Germany | Gingivitis & Periodontitis | 33 | 35 | L. reuteri | 42 days/ 42 days | Lozenge | None | No | PCR +, GI +, BOP +, PAL +, PPD + | Probiotic use improved all clinical outcomes compared to controls. |
| Shah, 2013 [93] India | Periodontitis | 10 | 10 (Control) 10 (Antibiotic) | L. brevis | 2 weeks/ 2 months | Tablet | SRP 1) Probiotic + Doxycycline 2) Doxycycline alone | No | PlI *, GI *, CAL *, PPD *, lactobacilli+, A. actinomycetemcomitans * | Probiotic use decreased clinical and microbiological parameters when used alone or in combination with doxycycline. |
| Shah, 2017 [94] India | Periodontitis | 6 | 6 | L. brevis | 14 days/ 5 months | Lozenge | SRP 1) Probiotics + Doxycycline 2) Doxycycline alone | No | GI +, PlI, PPD, CAL, A. actinomycetemcomitans, Lactobacillus spp. | No synergy at 5 months when probiotics and doxycycline were both given. No statistically significant difference between antibiotic and probiotic supplementation. |
| Shetty, 2020 [95] India | Periodontitis | 60 | 60 | B. mesentericus, C. butyricum, L. sporogenes. S. faecalis | Once (local)/ 3 months | Local | SRP | Not mentioned | PlI *, GI *, PPD *, IL-6 +, ALP *, P.Gingivalis *, P. intermedia * | Synbiotic treatment may improve clinical, microbiological, and immunological outcomes in patients with chronic periodontitis. |
| Shimauchi, 2008 [96] Japan | Healthy | 34 | 32 | L. salivarius | 8 weeks/ 8 weeks | Tablet | None | No | PlI *, GI *, BOP *, PPD *, L. salivarius +, Lactoferritin * (Saliva) | Probiotics may be useful for maintenance and/or improvement of oral health in individuals at risk of periodontal diseases. |
| Sinkiewicz, 2010 [97] Sweden | Healthy | 11 | 12 | L. reuteri | 12 weeks/ 12 weeks | Chewing gum | None | No | PlI, A. naeslundii *, A. actinomycetemcomitans *, C. rectus *, F. alocis *, F. nucleatum *, L. acidophilus, L. fermentum *, L. reuteri *, P. micra, P. gingivalis *, P. endodontalis *, P. intermedia *, T. forsythia *, T. denticola *, S. intermedia, S. mutans *, S. oralis, S. sanguinis *, V. parvula * | There was a statistically significant increase in plaque in the controls, but not the probiotics group. No changes between probiotics and control groups in the oral microbiota. |
| Slawik, 2011 [98] Germany | Healthy | 11 | 17 | L. casei | 14 days/ 14 days | Drink | None | No | PlI *, GI *, BOP +, GCF+ | Probiotics may have an anti-inflammatory effect. |
| Snulingga, 2020 [99] Indonesia | Periodontitis | 8 | 8 | L. reuteri | 14 days/ 14 days | Lozenge | SRP | Not mentioned | CAL +, IL-4 | Probiotic use as an adjunct decreased CAL and increased IL-4. |
| Staab, 2009 [100] Germany | Healthy | 25 | 25 | L. casei | 8 weeks/ 8 weeks | Drink | None | No | PlI +, PBI *, MPO +, MMP-3 +, Elastase * | Probiotics may improve periodontal health through immunomodulation. |
| Suzuki, 2012 [101] Japan | Periodontitis | 20 | 22 | L. salivarius | 2 weeks/ 2 weeks | Oil drops | None | No | BOP +, PPD *, Ubiquitous bacteria *, F. nucleatum, P. gingivalis, L. salivarius *, P. intermedia, S. mutans, T. forsythia, T. denticola | Probiotics improved BOP and had a decreased periodontopathogen count compared to controls. |
| Tekce, 2015 [41] Turkey | Periodontitis | 20 | 20 | L. reuteri | 3 weeks/ 3 weeks | Lozenge | SRP | Yes | PlI +, GI +, BOP +, PPD +, RAL *, Anaerobic bacteria +, TVC + | Probiotics as an adjuvant can improve clinical and microbiological outcomes. |
| Teughels, 2013 [102] Turkey | Periodontitis | 15 | 15 | L. reuteri | 12 weeks/ 12 weeks | Lozenge | SRP | Yes | PlI *, CAL +, GBI +, BOP *, PPD+, REC, A. actinomycetemcomitans *, F. nucleatum *, T. forsythia *, P. gingivalis +, P. intermedia *, Total bacteria * | Probiotics as an adjuvant can improve clinical and microbiological outcomes. |
| Theodoro, 2019 [103] Brazil | Periodontitis | 14 | 14 | L. reuteri | 21 days/ 90 days | Chewing tablet | SRP | Yes | BOP +, CAL, PPD +, REC | Adjuvant use of probiotics to treat chronic periodontitis in smokers reduced gingival inflammation. |
| Tobita, 2018 [104] Japan | Healthy | 8 | 8 | L. crispatus | 4 weeks/ 4 weeks | Tablet | None | No | PS +, A. actinomycetemcomitans, F. nucleatum *, T. forsythia, P. gingivalis +, P. intermedia, T. denticola. | Probiotic use can improve the oral environment and hence may help prevent periodontal disease. |
| Toiviainen, 2015 [105] Finland | Healthy | 29 | 31 | B. lactis, L. rhamnosus | 4 weeks/ 4 weeks | Lozenge | None | Not mentioned | PlI*, GI*, Lactobacillus, S. mutans | Probiotics improved clinical outcomes but not microbiological. |
| Twetman, 2009 [106] Denmark | Gingivitis | 14 | 13 | L. reuteri | 2 weeks/ 2 weeks | Chewing gum | None | Yes | BOP*, IL-1β, TNF-α, GCF*, IL-6*, IL-8*, IL-10 | Probiotics are beneficial to gingival health in a dose dependent manner. |
| Vicario, 2013 [107] Spain | Periodontitis | 10 | 9 | L. reuteri | 1 month/ 1 month | Tablet | None | Yes | PlI*, BOP*, PPD* | Probiotic supplementation can improve inflammatory and clinical outcomes in patients with mild to moderate periodontitis. |
| Vivekananda, 2010 [108] India | Periodontitis | 15 | 15 | L. reuteri | 21 days/ 42 days | Lozenge | 1) SRP 2) Without SRP | Yes | PlI*, GI*, GBI*, CAL*, PPD*, A. actinomycetemcomitans*, P. gingivalis*, P. intermedia* | Probiotic use can improve periodontal health through plaque inhibition, anti-inflammatory and antimicrobial effects. |
| Vohra, 2019 Saudi [109] Arabia | Periodontitis | 31 | 32 | L. reuteri | 21 days/ 3 months | Lozenge | SRP | Yes | PlI*, CAL*, BOP*, PPD* | Probiotic use is not an effective adjunct to SRP in chronic periodontitis patients. |
| Yuki, 2019 [110] Japan | Periodontal disease | 12 | 11 | L. rhamnosus | 90 days/ 90 days | Yogurt | None | Yes | GI*, PPD*, PMA+ | Probiotic use improved clinical parameters under study. |
| Clinical Outcomes | Subgroup | Level of Subgroup | SMD | 95% CI | I2 | p-Value | Sample Size | |
|---|---|---|---|---|---|---|---|---|
| Probiotic | Control | |||||||
| Plaque index (PlI) | Type of periodontal disease | Gingivitis | 0.153 | −0.152, 0.457 | 20.906 | 0.281 | 108 | 99 |
| Periodontitis | 0.736 | 0.267, 1.206 | 71.842 | 0.001 | 136 | 135 | ||
| Type of probiotic strain | Lactobacillus | 0.639 | 0.169, 1.110 | 75.533 | <0.001 | 154 | 151 | |
| Mixed | 0.280 | −0.159, 0.719 | 0.000 | 0.523 | 42 | 36 | ||
| Other | 0.185 | −0.212, 0.582 | 0.000 | 0.431 | 48 | 47 | ||
| Type of Lactobacillus species | L. Reuteri | 0.707 | 0.034, 1.381 | 80.976 | <0.001 | 98 | 95 | |
| Other | 0.590 | −0.456, 1.636 | 81.557 | 0.004 | 42 | 42 | ||
| Treatment duration | ≤1 month | 0.615 | 0.146, 1.084 | 75.448 | <0.001 | 154 | 153 | |
| >1 to 2 months | 0.328 | −0.006, 0.661 | 0.000 | 0.406 | 73 | 64 | ||
| > 2 months | 0.053 | −0.603, 0.710 | 0.000 | 1.000 | 17 | 17 | ||
| Mode of delivery | Ingestion | 0.952 | −0.894, 2.797 | 89.037 | 0.003 | 27 | 27 | |
| Local | 0.323 | −0.202, 0.847 | 0.000 | 1.000 | 28 | 27 | ||
| Oral | 0.239 | −0.302, 0.780 | 0.251 | 0.251 | 34 | 34 | ||
| Oral and Ingestion | 0.495 | 0.061, 0.930 | 0.001 | <0.001 | 155 | 146 | ||
| Oral hygiene instructions | Yes | 0.622 | 0.204, 1.040 | 66.923 | 0.006 | 145 | 138 | |
| No | 0.665 | −0.415, 1.746 | 85.436 | <0.001 | 54 | 51 | ||
| Mean plaque percentage (MPP) | Type of periodontal disease | Gingivitis | 1.279 | −0.905, 3.463 | 96.629 | <0.001 | 63 | 64 |
| Periodontitis | 0.681 | 0.072, 1.290 | 82.212 | <0.001 | 130 | 130 | ||
| Type of probiotic strain | Lactobacillus | 1.037 | 0.391, 1.683 | 88.278 | <0.001 | 195 | 198 | |
| Mixed | 0.112 | −0.728, 0.952 | 0.000 | 1.000 | 10 | 10 | ||
| Other | 0.199 | −0.396, 0.794 | 0.000 | 1.000 | 21 | 21 | ||
| Type of Lactobacillus species | L. Reuteri | 1.458 | 0.724, 2.191 | 86.723 | <0.001 | 148 | 150 | |
| Other | 0.193 | −0.200, 0.586 | 0.000 | 0.889 | 47 | 48 | ||
| Treatment duration | ≤1 month | 0.937 | 0.076, 1.798 | 90.960 | <0.001 | 145 | 146 | |
| >1 to 2 months | 1.560 | 1.022, 2.099 | 0.000 | 1.000 | 33 | 35 | ||
| > 2 months | 0.460 | 0.008, 0.912 | 21.718 | 0.279 | 48 | 48 | ||
| Mode of delivery | Ingestion | 0.969 | −0.506, 2.445 | 94.211 | <0.001 | 77 | 78 | |
| Oral | 0.537 | −0.348, 1.423 | 59.024 | 0.118 | 24 | 24 | ||
| Oral and Ingestion | 0.942 | 0.159, 1.725 | 87.844 | <0.001 | 125 | 127 | ||
| Oral hygiene instructions | Yes | 0.880 | 0.197, 1.564 | 88.210 | <0.001 | 170 | 170 | |
| No | 0.865 | −0.502, 2.232 | 91.878 | <0.001 | 56 | 59 | ||
| Gingival index (GI) | Type of periodontal disease | Gingivitis | 0.298 | −0.089, 0.684 | 49.985 | 0.092 | 108 | 99 |
| Periodontitis | 1.069 | 0.296, 1.841 | 86.299 | <0.001 | 116 | 112 | ||
| Type of probiotic strain | Lactobacillus | 1.236 | 0.574, 1.897 | 87.366 | <0.001 | 178 | 174 | |
| Mixed | 0.101 | −0.333, 0.535 | 0.000 | 0.949 | 43 | 36 | ||
| Other | 0.329 | −0.070, 0.729 | 0.000 | 0.354 | 48 | 47 | ||
| Type of Lactobacillus species | L. Reuteri | 1.621 | 0.648, 2.595 | 89.871 | <0.001 | 112 | 111 | |
| Other | 0.817 | 0.018, 1.616 | 79.137 | 0.001 | 66 | 63 | ||
| Treatment duration | ≤1 month | 0.949 | 0.270, 1.628 | 85.079 | <0.001 | 132 | 130 | |
| >1 to 2 months | 0.900 | −0.116, 1.915 | 91.498 | <0.001 | 106 | 99 | ||
| >2 months | 0.888 | −0.920, 2.696 | 89.949 | 0.002 | 31 | 28 | ||
| Mode of delivery | Ingestion | 1.258 | −0.169, 2.686 | 87.547 | <0.001 | 41 | 38 | |
| Local | 0.494 | −0.035, 1.023 | 0.000 | 1.000 | 28 | 27 | ||
| Oral | 0.189 | −0.305, 0.682 | 0.000 | 0.674 | 30 | 30 | ||
| Oral and Ingestion | 1.051 | 0.306, 1.797 | 89.846 | <0.001 | 170 | 162 | ||
| Oral hygiene instructions | Yes | 1.051 | 0.327, 1.775 | 86.466 | <0.001 | 134 | 126 | |
| No | 1.344 | 0.261, 2.427 | 89.898 | <0.001 | 87 | 86 | ||
| Pocket probing depth (PPD) | Type of periodontal disease | Gingivitis | 0.997 | −0.853, 2.848 | 92.406 | <0.001 | 35 | 38 |
| Periodontitis | 0.578 | 0.355, 0.801 | 62.720 | <0.001 | 442 | 434 | ||
| Type of probiotic strain | Lactobacillus | 0.674 | 0.386, 0.962 | 69.524 | <0.001 | 330 | 329 | |
| Mixed | 0.387 | 0.045, 0.729 | 0.000 | 0.740 | 67 | 62 | ||
| Other | 0.379 | −0.037, 0.795 | 51.535 | 0.103 | 92 | 92 | ||
| Type of Lactobacillus species | L. Reuteri | 0.677 | 0.315, 1.040 | 74.541 | <0.001 | 249 | 252 | |
| Other | 0.657 | 0.169, 1.144 | 56.911 | 0.041 | 81 | 77 | ||
| Treatment duration | ≤1 month | 0.737 | 0.430, 1.044 | 66.736 | <0.001 | 270 | 264 | |
| >1 to 2 months | 0.514 | −0.030, 1.059 | 65.160 | 0.057 | 76 | 79 | ||
| > 2 months | 0.326 | 0.015, 0.636 | 43.082 | 0.080 | 143 | 140 | ||
| Mode of delivery | Ingestion | 0.514 | 0.106, 0.922 | 47.870 | 0.088 | 94 | 91 | |
| Local | 0.919 | 0.370, 1.468 | 0.000 | 1.000 | 28 | 27 | ||
| Oral | 0.918 | −0.071, 1.907 | 79.291 | 0.008 | 44 | 44 | ||
| Oral and Ingestion | 0.525 | 0.251, 0.800 | 66.577 | <0.001 | 323 | 321 | ||
| Oral hygiene instructions | Yes | 0.592 | 0.343, 0.841 | 63.935 | <0.001 | 366 | 360 | |
| No | 0.953 | 0.308, 1.597 | 65.707 | 0.054 | 66 | 69 | ||
| Disease severity | Deep | 0.735 | 0.209, 1.261 | 73.585 | 0.002 | 112 | 114 | |
| Moderate | 0.499 | 0.043, 0.955 | 66.202 | 0.011 | 112 | 114 | ||
| Clinical attachment level (CAL) | Type of probiotic strain | Lactobacillus | 0.417 | 0.225, 0.609 | 8.881 | 0.355 | 229 | 228 |
| Mixed | 0.395 | −0.066, 0.855 | 0.000 | 0.401 | 38 | 34 | ||
| Other | 0.415 | 0.076, 0.755 | 7.610 | 0.339 | 72 | 72 | ||
| Type of Lactobacillus species | L. Reuteri | 0.416 | 0.201, 0.631 | 12.027 | 0.330 | 189 | 189 | |
| Other | 0.445 | −0.086, 0.975 | 31.016 | 0.235 | 40 | 39 | ||
| Treatment duration | ≤1 month | 0.388 | 0.185, 0.592 | 0.000 | 0.547 | 186 | 181 | |
| >1 to 2 months | 0.789 | 0.236, 1.343 | 34.507 | 0.217 | 41 | 41 | ||
| > 2 months | 0.330 | 0.071, 0.588 | 0.000 | 0.571 | 112 | 112 | ||
| Mode of delivery | Ingestion | 0.464 | 0.116, 0.812 | 0.276 | 0.390 | 63 | 63 | |
| Local | 0.696 | 0.159, 1.233 | 0.000 | 1.000 | 28 | 27 | ||
| Oral | 0.887 | 0.132, 1.643 | 0.000 | 1.000 | 14 | 14 | ||
| Oral and Ingestion | 0.339 | 0.159, 0.520 | 0.000 | 0.543 | 234 | 230 | ||
| Oral hygiene instructions | Yes | 0.351 | 0.178, 0.523 | 0.000 | 0.789 | 256 | 251 | |
| No | 0.835 | 0.437, 1.233 | 0.000 | 0.376 | 51 | 51 | ||
| Disease severity | Deep | 0.373 | 0.088, 0.657 | 0.000 | 0.690 | 92 | 94 | |
| Moderate | 0.422 | 0.137, 0.706 | 0.000 | 0.886 | 92 | 94 | ||
| Bleeding on probing (BOP) | Type of periodontal disease | Gingivitis | 0.685 | −0.438, 1.808 | 93.899 | <0.001 | 117 | 120 |
| Periodontitis | 0.749 | 0.404, 1.094 | 72.526 | <0.001 | 260 | 257 | ||
| Type of probiotic strain | Lactobacillus | 0.878 | 0.442, 1.313 | 85.057 | <0.001 | 314 | 312 | |
| Mixed | 0.035 | −0.574, 0.643 | 0.000 | 1.000 | 19 | 21 | ||
| Other | 0.202 | −0.210, 0.613 | 0.000 | 0.640 | 44 | 44 | ||
| Type of Lactobacillus species | L. Reuteri | 1.054 | 0.485, 1.622 | 86.818 | <0.001 | 217 | 217 | |
| Other | 0.502 | −0.078, 1.081 | 74.262 | 0.002 | 97 | 95 | ||
| Treatment duration | ≤1 month | 1.024 | 0.454, 1.595 | 88.021 | <0.001 | 236 | 238 | |
| >1 to 2 months | 0.095 | −0.513, 0.703 | 0.000 | 1.000 | 20 | 20 | ||
| > 2 months | 0.402 | 0.020, 0.785 | 55.314 | 0.037 | 121 | 119 | ||
| Mode of delivery | Ingestion | 0.742 | −0.391, 1.876 | 93.499 | <0.001 | 112 | 110 | |
| Oral | 1.166 | −0.037, 2.370 | 89.525 | <0.001 | 63 | 65 | ||
| Oral and Ingestion | 0.616 | 0.296, 0.936 | 60.339 | 0.005 | 202 | 202 | ||
| Oral hygiene instructions | No | 0.054 | −0.508, 0.617 | 0.000 | 1.000 | 23 | 24 | |
| Yes | 0.966 | 0.478, 1.454 | 86.250 | <0.001 | 277 | 276 | ||
| Gingival crevicular fluid (GCF) | Type of periodontal disease | Gingivitis | 0.626 | 0.162, 1.091 | 0.000 | 0.392 | 36 | 36 |
| Periodontitis | 0.507 | 0.027, 0.986 | 0.000 | 0.496 | 33 | 33 | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gheisary, Z.; Mahmood, R.; Harri shivanantham, A.; Liu, J.; Lieffers, J.R.L.; Papagerakis, P.; Papagerakis, S. The Clinical, Microbiological, and Immunological Effects of Probiotic Supplementation on Prevention and Treatment of Periodontal Diseases: A Systematic Review and Meta-Analysis. Nutrients 2022, 14, 1036. https://doi.org/10.3390/nu14051036
Gheisary Z, Mahmood R, Harri shivanantham A, Liu J, Lieffers JRL, Papagerakis P, Papagerakis S. The Clinical, Microbiological, and Immunological Effects of Probiotic Supplementation on Prevention and Treatment of Periodontal Diseases: A Systematic Review and Meta-Analysis. Nutrients. 2022; 14(5):1036. https://doi.org/10.3390/nu14051036
Chicago/Turabian StyleGheisary, Zohre, Razi Mahmood, Aparna Harri shivanantham, Juxin Liu, Jessica R. L. Lieffers, Petros Papagerakis, and Silvana Papagerakis. 2022. "The Clinical, Microbiological, and Immunological Effects of Probiotic Supplementation on Prevention and Treatment of Periodontal Diseases: A Systematic Review and Meta-Analysis" Nutrients 14, no. 5: 1036. https://doi.org/10.3390/nu14051036
APA StyleGheisary, Z., Mahmood, R., Harri shivanantham, A., Liu, J., Lieffers, J. R. L., Papagerakis, P., & Papagerakis, S. (2022). The Clinical, Microbiological, and Immunological Effects of Probiotic Supplementation on Prevention and Treatment of Periodontal Diseases: A Systematic Review and Meta-Analysis. Nutrients, 14(5), 1036. https://doi.org/10.3390/nu14051036