
Vitamin Supplementation and Dementia: A Systematic Review


Abstract
1. Introduction
1.1. Dementia and Mild Cognitive Impairment: Definition and Clinical Characteristics
1.2. Subtypes of Dementia
1.3. Risk Factors
1.4. Justification and Aim
2. Materials and Methods
2.1. Search Strategy
2.2. Inclusion Criteria
2.3. Exclusion Criteria
2.4. Data Collection and Analysis
3. Results
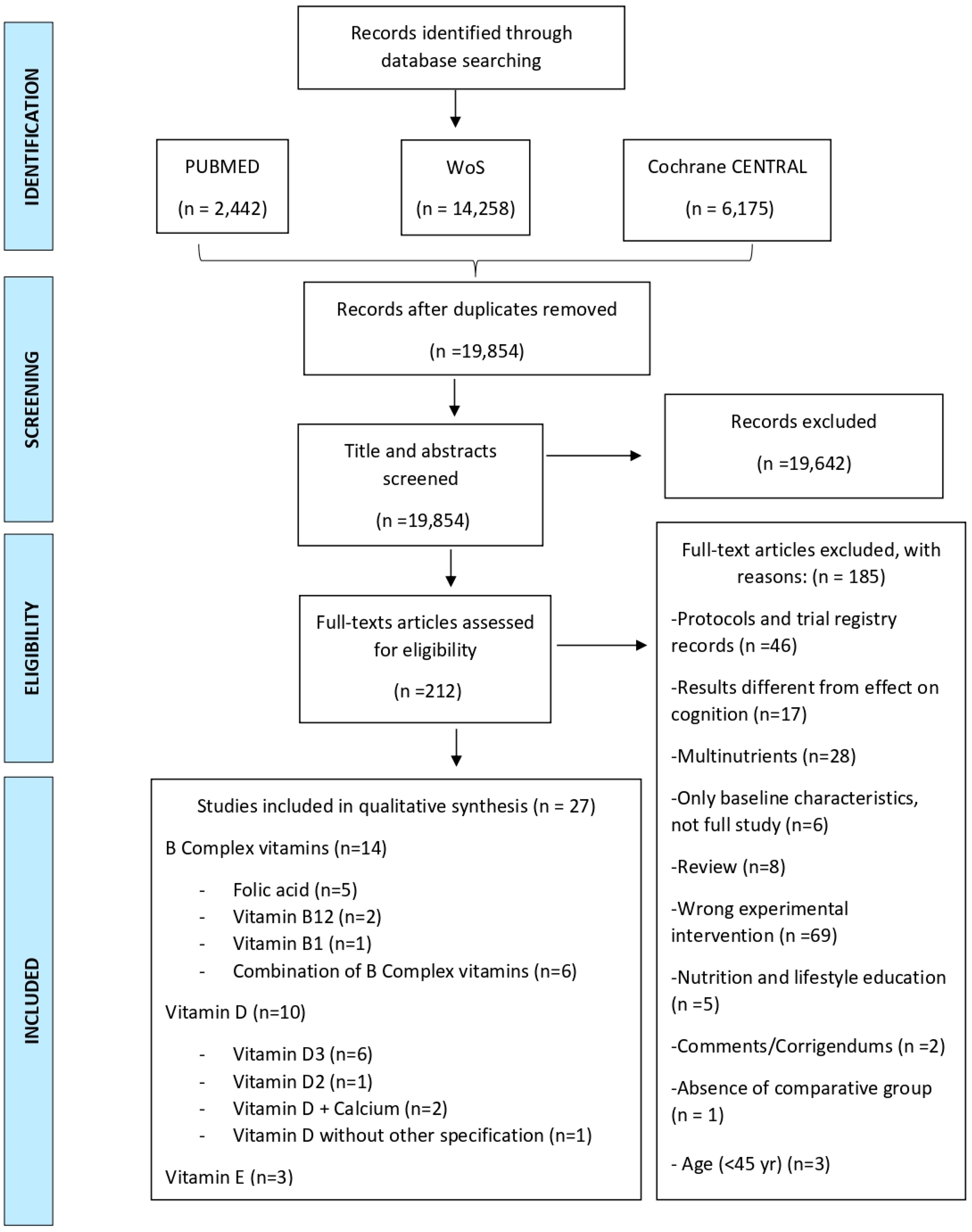
3.1. Search Results and Description of Studies
3.2. Analysis of Results
3.2.1. Vitamin B Complex
Comparison 1: B Complex Vitamins vs. Placebo
- Participants in Chen H. et al. received 1.2 mg folic acid and 50 µg vitamin B12 once daily for six months [39];
- People in the study by Dangour A. et al. received 1 mg vitamin B12 p.o (orally) daily for 12 months [43];
- In the trial by Walker J. et al., participants received 400 µg folic acid and 100 µg vitamin B12 supplementation p.o daily for 24 months [38];
- Participants in the RCT (Randomized controlled trial) by Kwok T. et al. were treated with 500 µg methylcobalamin and 400 µg folic acid p.o once daily for 24 months [42];
- Participants in Moore K. et al. received 400 µg folic acid, 10 µg vitamin B12, 10 mg vitamin B6, and 10 mg riboflavin over two years [44].
- Gibson G. et al. used, as intervention, a supplement of 300 mg benfotiamine b.i.d (twice a day) for 12 months [40];
- In the RCT by Chen H. et al., those in the intervention group received donepezil and a supplement of 1.25 mg folic acid daily for six months, and those in the control group only received placebo apart from donepezil [37];
- Finally, the study by Li M. et al. compared three intervention groups with placebo. The first IG received 800 µg folic acid plus 800 mg docosahexaenoic (DHA) p.o daily. The second IG only received 800 µg folic p.o daily and the third IG received 800 mg DHA p.o daily. The duration of the three treatments was six months [41].
Comparison 2: B Complex Vitamins vs. Conventional Treatment
- Participants in Ma F. et al. received 400 µg folic acid daily for six months [45];
- In another study by Ma F. et al., those in the intervention group also received 400 µg folic acid p.o daily, but in this case for twelve months [46];
- There was another study published by Ma. F. et al. where those in the intervention group also received 400 µg folic acid p.o daily. The duration of the treatment in this trial was 24 months [47];
- In the trial by Lu R. et al., participants received 90 mg thiamine and 30 mg folic acid daily for 96 weeks [49];
- Jiang B. et al. used, as an intervention, a supplement of 5 mg folic acid daily plus 500 µg vitamin B12 t.i.d. for 24 weeks [48].
Comparison 3: Vitamin B vs. Vitamin C
3.2.2. Vitamin D
Comparison 1: Vitamin D vs. Placebo
- Participants in Aspell N. et al. received supplementation of 50 µg vitamin D3 daily for six months [51];
- Those allocated in the intervention group by Stein M. et al. were treated with a high dose of vitamin D2 (6000 IU) daily for eight weeks [52];
- Participants recruited to the intervention arm of the VITAL trial received 2000 IU vitamin D3 p.o. daily accompanied with fish oil supplements [53];
- Rossom R.C. et al. decided to explore the supplementation of 400 IU vitamin D3 and 1000 mg calcium carbonate daily [54].
Comparison 2: Vitamin D vs. Non-Intervention or Conventional Treatment
- Firstly, in Anweiler C. et al., those in the intervention group received a supplementation of 800 IU vitamin D3 p.o daily or 100,000 IU p.o per month [55];
- The intervention arm by Lee Y. et al. explored the supplementation of 1000 IU vitamin D daily, accompanied with exercise programs for twelve weeks [56];
- Finally, Beauchet O. et al. allocated a total of 20 patients to an intervention of fortified yoghurts daily, that included 400 IU vitamin D3, as well as 800 mg calcium for three months [57];
- Bischoff-Ferrari H. et al. allocated 1076 participants to a 2000 IU vitamin D3 supplementation daily for three years [58].
Comparison 3: Two Different Dosage Regimens of Vitamin D
- Castle M. et al. allocated the participants into three intervention groups. The first one received a 600 IU vitamin D3 supplementation for a year, the second one received a 2000 IU vitamin D3 supplementation for a year and the third group was treated with 4000 IU vitamin D3 supplementation for a year [59];
- Those in the intervention group by Schietzel S. et al. received 2000 IU vitamin D3 daily, whereas the vitamin D3 supplementation in those in the control group was 800 IU daily [60].
3.2.3. Vitamin E
Comparison 1: Vitamin E vs. Placebo
- In the PREADVISE trial, participants were allocated into either one of three intervention groups or a placebo group. Those in the first intervention group (IG1) received 400 IU vitamin E daily, those in the second intervention group (IG2) were treated with 200 µg selenium daily, and finally, those assigned to the third intervention group (IG3) received a combination of vitamin E and selenium [61].
- In the study by Dysken. M.W. et al., participants were also allocated into either one of three intervention groups or a placebo group. Those in the first intervention group (IG1) received 1000 IU α-tocopherol p.o., b.i.d. Those in the second intervention group (IG2) were treated with 10 mg memantine p.o., b.i.d. Finally, those assigned to the third intervention group (IG3) received a combination of α-tocopherol and memantine [62].
Comparison 2: Vitamin E Plus Vitamin C vs. Placebo
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A. Search Strategy
- #1
- (vitamins) OR (dietary supplements) OR (multivitamin) OR (vitamin*) OR (supple*) OR (diet*) OR (supplement*)
- #2
- (vitamin A) OR (retinol) OR (retinoic acid)
- #3
- (vitamin D) OR (cholecalciferol) OR (vitamin D3) OR (ergocalciferol) OR (vitamin D2) OR (toxiferol) OR (calcitriol) OR (calcitriol derivative)
- #4
- (vitamin E)
- #5
- (vitamin K group) OR (vitamin K) OR (phylloquinone) OR (vitamin K1) OR (phytomenadione) OR (phytonadione)
- #6
- (vitamin B complex) OR (vitamin B group) OR (vitamin B1) OR (thiamine)
- #7
- (vitamin B2) OR (riboflavin)
- #8
- (vitamin B3) OR (niacin) OR (niacinamide) OR (nicotinamide) OR (nicotinic acid)
- #9
- (vitamin B6) OR (pyridoxine) OR (pyridoxal) OR (pyridoxamine) OR (pyridoxal 5′ phosphate) OR (pyridoxamine 5′ phosphate) OR (pyridoxine 5′ phosphate)
- #10
- (vitamin B9) OR (folic acid)
- #11
- (vitamin B12) OR (cobalamins) OR (cyanocobalamin) OR (hydroxocobalamin) OR (methylcobalamin)
- #12
- (vitamin B5) OR (pantothenic acid)
- #13
- (biotin) OR (vitamin H)
- #14
- (vitamin C) OR (l-ascorbic acid) OR (ascorbic acid) OR (ascorbate)
- #15
- (mild cognitive impairment) OR (MCI) OR (AAMI) OR (age-associated memory impairment) OR (age consistent memory impairment) OR (ACMI) OR (age related cognitive decline) OR (ARCD) OR (cognitive impairment with no dementia) OR (CIND)
- #16
- (cognition) OR (cognition disorders) OR (memory) OR (memory disorders) OR (mental performance) OR (mental perform*) OR (memory) OR (executive function) OR (attention)
- #17
- #1 OR #2 OR #3 OR #4 OR #5 OR #6 OR #7 OR #8 OR #9 OR #10 OR #11 OR #12 OR #13 OR #14
- #18
- #15 OR #16
- #19
- #18 AND #17
- #20
- #19 Filters: Filters: Free full text, Clinical Study, Clinical Trial, Clinical Trial, Phase I, Clinical Trial, Phase II, Clinical Trial, Phase III, Clinical Trial, Phase IV, Comparative Study, Controlled Clinical Trial, Meta-Analysis, Randomized Controlled Trial, in the last 10 years, English, German, Spanish Sort by: Publication Date
- #1
- TS = ((vitamins) OR (dietary supplements) OR (multivitamin) OR (vitamin*) OR (supple*) OR (diet*) OR (supplement*))
- #2
- TS = ((vitamin A) OR (retinol) OR (retinoic acid))
- #3
- TS = ((vitamin D) OR (cholecalciferol) OR (vitamin D3) OR (ergocalciferol) OR (vitamin D2) OR (toxiferol) OR (calcitriol) OR (calcitriol derivative))
- #4
- TS = ((vitamin E))
- #5
- TS = ((vitamin K group) OR (vitamin K) OR (phylloquinone) OR (vitamin K1) OR (phytomenadione) OR (phytonadione))
- #6
- TS = ((vitamin B complex) OR (vitamin B group) OR (vitamin B1) OR (thiamine))
- #7
- TS = ((vitamin B2) OR (riboflavin))
- #8
- TS = ((vitamin B3) OR (niacin) OR (niacinamide) OR (nicotinamide) OR (nicotinic acid))
- #9
- TS = ((vitamin B6) OR (pyridoxine) OR (pyridoxal) OR (pyridoxamine) OR (pyridoxal 5′ phosphate) OR (pyridoxamine 5′ phosphate) OR (pyridoxine 5′ phosphate))
- #10
- TS = ((vitamin B9) OR (folic acid))
- #11
- TS = ((vitamin B12) OR (cobalamins) OR (cyanocobalamin) OR (hydroxocobalamin) OR (methylcobalamin))
- #12
- TS = ((vitamin B5) OR (pantothenic acid))
- #13
- TS = ((biotin) OR (vitamin H))
- #14
- TS = ((vitamin C) OR (l-ascorbic acid) OR (ascorbic acid) OR (ascorbate))
- #15
- TS = ((mild cognitive impairment) OR (MCI) OR (AAMI) OR (age-associated memory impairment) OR (age consistent memory impairment) OR (ACMI) OR (age related cognitive decline) OR (ARCD) OR (cognitive impairment with no dementia) OR (CIND))
- #16
- TS = ((cognition) OR (cognition disorders) OR (memory) OR (memory disorders) OR (mental performance) OR (mental perform*) OR (memory) OR (executive function) OR (attention))
- #17
- #1 OR #2 OR #3 OR #4 OR #5 OR #6 OR #7 OR #8 OR #9 OR #10 OR #11 OR #12 OR #13 OR #14
- #18
- #15 OR #16
- #19
- #18 AND #17
- #20
- #18 AND #17 and Open Access and 2022 or 2021 or 2020 or 2019 or 2018 or 2017 or 2016 or 2015 or 2014 or 2013 or 2012 or 2011 (Publication Years)
- #21
- #18 AND #17 and Open Access and 2022 or 2021 or 2020 or 2019 or 2018 or 2017 or 2016 or 2015 or 2014 or 2013 or 2012 or 2011 (Publication Years) and Articles (Document Types)
- #1
- MeSH descriptor: [Vitamins] explode all trees
- #2
- (vitamins) OR (dietary supplements) OR (multivitamin) OR (vitamin*) OR (supple*) OR (diet*) OR (supplement*)
- #3
- #1 OR #2
- #4
- MeSH descriptor: [Vitamin A] explode all trees
- #5
- (vitamin A) OR (retinol) OR (retinoic acid)
- #6
- #4 OR #5
- #7
- MeSH descriptor: [Vitamin D] explode all trees
- #8
- (vitamin D) OR (cholecalciferol) OR (vitamin D3) OR (ergocalciferol) OR (vitamin D2) OR (toxiferol) OR (calcitriol) OR (calcitriol derivative)
- #9
- #7 OR #8
- #10
- MeSH descriptor: [Vitamin E] explode all trees
- #11
- (vitamin E)
- #12
- #10 OR #11
- #13
- MeSH descriptor: [Vitamin K] explode all trees
- #14
- (vitamin K group) OR (vitamin K) OR (phylloquinone) OR (vitamin K1) OR (phytomenadione) OR (phytonadione)
- #15
- #13 OR #14
- #16
- MeSH descriptor: [Vitamin B Complex] explode all trees
- #17
- (vitamin B complex) OR (vitamin B group)
- #18
- #16 OR #17
- #19
- MeSH descriptor: [Thiamine] explode all trees
- #20
- (vitamin B1) OR (thiamine)
- #21
- #19 OR #20
- #22
- MeSH descriptor: [Riboflavin] explode all trees
- #23
- (vitamin B2) OR (riboflavin)
- #24
- #22 OR #23
- #25
- MeSH descriptor: [Niacinamide] explode all trees
- #26
- (vitamin B3) OR (niacin) OR (niacinamide) OR (nicotinamide) OR (nicotinic acid)
- #27
- #25 OR #26
- #28
- MeSH descriptor: [Vitamin B 6] explode all trees
- #29
- (vitamin B6) OR (pyridoxine) OR (pyridoxal) OR (pyridoxamine) OR (pyridoxal 5′ phosphate) OR (pyridoxamine 5′ phosphate) OR (pyridoxine 5′ phosphate)
- #30
- #28 OR #29
- #31
- MeSH descriptor: [Folic Acid] explode all trees
- #32
- (vitamin B9) OR (folic acid)
- #33
- #31 OR #32
- #34
- MeSH descriptor: [Vitamin B 12] explode all trees
- #35
- (vitamin B12) OR (cobalamins) OR (cyanocobalamin) OR (hydroxocobalamin) OR (methylcobalamin)
- #36
- #34 OR #35
- #37
- MeSH descriptor: [Pantothenic Acid] explode all trees
- #38
- (vitamin B5) OR (pantothenic acid)
- #39
- #37 OR #38
- #40
- MeSH descriptor: [Biotin] explode all trees
- #41
- (biotin) OR (vitamin H)
- #42
- #40 OR #41
- #43
- MeSH descriptor: [Ascorbic Acid] explode all trees
- #44
- (vitamin C) OR (l-ascorbic acid) OR (ascorbic acid) OR (ascorbate)
- #45
- #43 OR #44
- #46
- MeSH descriptor: [Cognitive Dysfunction] explode all trees
- #47
- (mild cognitive impairment) OR (MCI) OR (AAMI) OR (age-associated memory impairment) OR (age consistent memory impairment) OR (ACMI) OR (age related cognitive decline) OR (ARCD) OR (cognitive impairment with no dementia) OR (CIND)
- #48
- #46 OR #47
- #49
- MeSH descriptor: [Memory Disorders] explode all trees
- #50
- (cognition) OR (cognition disorders) OR (memory) OR (memory disorders) OR (mental performance) OR (mental perform*) OR (memory) OR (executive function) OR (attention)
- #51
- #49 OR #50
- #52
- #2 OR #5 OR #8 OR #11 OR #14 OR #17 OR #20 OR #23 OR #26 OR #29 OR #32 OR #35 OR #38 OR #41 OR #44
- #53
- #3 OR #6 OR #9 OR #12 OR #15 OR #18 OR #21 OR #24 OR #27 OR #30 OR #33 OR #36 OR #39 OR #42 OR #45
- #54
- #47 OR #50
- #55
- #48 OR #51
- #56
- #54 AND #52
- #57
- #55 AND #53
- #58
- #55 AND #53 with Publication Year from 2011 to 2021, in Trials
Appendix B

{kind=link}
| Reference/Register Number | Study Design/Population of Study | No. of Participants | Mean Age ± SD, Years | Sex  |
|---|---|---|---|---|
| Vitamin B12 + Folic acid vs. Placebo | ||||
| Kwok T. et al. [42] CUHK_CCT00373 | RCT (placebo-controlled)/People ≥65 yr with MCI and elevated levels of serum homocysteine ≥10 µmol/L | IG: n = 138; CG: n = 141 | IG: 76.9 ± 5.4; CG: 78.0 ± 5.3 | IG: 63.1%; CG: 56.1% |
| Vitamin B12 + Folic acid vs. Placebo | ||||
| Walker J. et al. [38] NCT00214682 | RCT/Community-dwelling adults between 60–74 yr with elevated psychological distress (Kessler Distress 10-scale; score >15) | IG: n = 447; CG: n = 453 | IG: 65.92 ± 4.3; CG: 65.97 ± 4.18 | IG: 40.5%; CG: 39.1% |
| Vitamin B12 + Folic acid vs. Conventional treatment | ||||
| Jiang B. et al. [48] | RCT/Patients with vascular cognitive impairment-no dementia (VCIND), complicated with hyperhomocystinemia | IG: n = 60; CG: n = 60 | Average age ±SD, years: 63 ± 1.87 | Total, %: 65% |
| Vitamin B12 + Folic acid vs. Placebo | ||||
| Chen H. et al. [39] ChiCTR-IOR-16009731 | RCT (single-blind, placebo-controlled, single-center, parallel-group)/Patients >45 yr diagnosed clinically as probable AD and in a stable condition (MoCA less than 22) | IG: n = 60; CG: n = 60 | IG: 68.58 ± 7.29; CG: 68.02 ± 8.34 | IG: 50%; CG: 43.33% |
| Vitamin B12 vs. Placebo | ||||
| Dangour A. et al. [43] ISRCTN54195799 | RCT (double-blind, placebo-controlled)/People ≥75 yr with MMSE ≥ 24 and moderate vitamin B12 deficiency (serum vitamin B12 concentrations 107–210 pmol/L) and absence of anemia | IG: n = 99; CG: n = 102 | IG: 79.9 ± 3.5; CG: 80.1 ± 3.7 | IG: 46.5%; CG: 47.1% |
| Folic acid vs. Placebo | ||||
| Ma F. et al. [46] | RCT (single blind experimental design)/People ≥65 yr with MCI | IG: n = 84; CG: n = 84 | IG: 73.71 ± 2.57; CG: 73.52 ± 3.03 | IG: 32.14%; CG: 30.95% |
| Folic acid + DHA vs. Placebo | ||||
| Li M. et al. [41] Chi-CTR-IOR-16008351 | RCT (double-blind, placebo-controlled, two-center)/Elderly with MCI ≥60 yr and absence of mental disorders | IG1: n = 60; IG2: n = 60; IG3: n = 60; CG: n = 60 | IG1: 70.33 ± 7.7; IG2: 70.20 ± 6.13; IG3: 71.55 ± 6.62; CG: 70.38 ± 6.73 | IG1: 40%; IG2: 40%; IG3: 40%; CG: 45% |
| Folic acid vs. Placebo | ||||
| Ma F. et al. [45] ChiCTR-TRC-13003227 | RCT (single-center)/Chinese adults ≥65 yr with MCI who are unexposed to folic acid fortification | IG: n = 90; CG: n = 90 | IG: 74.82 ± 2.75; CG: 74.63 ± 3.21 | IG: 36.25%; CG: 34.18% |
| Folic acid vs. Conventional treatment | ||||
| Ma F. et al. [47] ChiCTR-TRC-13003227 | RCT (single-center)/Chinese adults ≥65 yr with MCI | IG: n = 90; CG: n = 90 | IG: 74.82 ± 2.75; CG: 74.63 ± 3.21 | IG: 43.33%; CG: 42.22% |
| Folic acid + Donepezil vs. Placebo + Donepezil | ||||
| Chen H. et al. [37] ChiCTR-TRC-13003246 | RCT (single-center, single-blind)/Patients with a new diagnosis of possible AD of mild or moderate severity (defined as an MMSE total score between 3 and 26) and currently being treated with Donepezil | IG: n = 61; CG: n = 60 | IG: 68.10 ± 8.50; CG: 67.63 ± 7.92 | IG: 54.10%; CG: 46.67% |
| Vitamin B1 (Benfotiamine) vs. Placebo | ||||
| Gibson G.E. et al. [40] NCT02292238 | RCT (placebo-controlled, Phase IIa, double blind)/Amyloid positive patients ≥60 yr with amnestic MCI or mild dementia due to AD and MMSE > 21 | IG: n = 34; CG: n = 36 | IG: 75.74 ± 6.91; CG: 75.81 ± 7.19 | IG: 32.4%; CG: 50% |
| Vitamin B1 (Thiamin) vs. Non Intervention | ||||
| Lu R. et al. [49] ChiCTR-IPR-17012210 | RCT (single-center)/adults with end-stage kidney disease and cognitive impairment (MoCA score <26) | IG: n = 25; CG: n = 25 | IG: 66.16 ± 7.61; CG: 69.00 ± 10.80 | IG: 72%; CG: 76% |
| (Vitamin B12+ Vitamin B6 + Vitamin B2+ Folic acid) vs. Placebo | ||||
| Moore K. et al. [44] | RCT/Generally healthy older adults ≥70 yr | IG: n = 124; CG: n = 125 | IG: 77.9 ± 4.2; CG: 78.2 ± 4.7 | IG: 48.5%; CG: 41.1% |
| Vitamin B12 vs. Vitamin C | ||||
| Vijayakumar T.M. et al. [50] CTRI No: REF/2016/02/010726 | RCT (double-blind, parallel-group)/Postmenopausal women (50–75 yr) with mild to moderate cognitive dysfunction | IG: n = 28; CG: n = 28 | IG: 57.56 ± 7.72; CG: 55.88 ± 6.01 | IG: 0%; CG: 0% |
| High Dose Vitamin D2 vs. Placebo | ||||
| Stein M. et al. [52] ACTRN12606000324516 | RCT (double-blind)/Community-dwelling participants ≥60 yr with mild-moderate AD (MMSE score 12–24) | IG: n = 16; CG: n = 16 | Median age [IQR],yr: IG: 75 [64.5–80] CG: 79 [74.5–82] | IG: 43.75%; CG: 50% |
| Vitamin D3 vs. Placebo | ||||
| Anweiler C. et al. [55] | Retrospective pre-post cohort study/Elderly outpatients visiting a memory clinic without recent vitamin D supplementation and without prescription of antidementia drugs | IG: n = 20; CG: n = 24 | Median age [IQR],yr: IG: 81.9 [13.2] CG: 75.9 [15.0] | IG: 45%; CG: 45.8% |
| Vitamin D3 (2000 IU/d) vs. Vitamin D3 (800 IU/d) | ||||
| Schietzel S. et al. [60] NCT00599807 | RCT (double-blind)/Community-dwelling older adults ≥60 yr with an MMSE ≥ 24 at baseline undergoing elective surgery for unilateral total knee replacement due to severe osteoarthritis | IG: n = 137; CG: n = 136 | IG: 70.2 ± 6.8; CG: 70.5 ± 6.0 | IG: 49.6%; CG: 43.4% |
| Vitamin D3 vs. Placebo | ||||
| Aspell N. et al. [51] NCT02804841 | RCT (placebo-controlled, double-blind)/Patients ≥60 yr without cognitive impairment (MMSE < 23) and with measured serum vitamin D <125 mmol/L. | IG: n = 30; CG: n = 29 | 68.5 ± 4.9 | 46.7% |
| Vitamin D + Exercise programs vs. Exercise programs | ||||
| Lee Y. et al. [56] KCT0002490 | Non-equivalent, control-group experimental study (Pre-test-post-test design)/Adults >65 yr with serum vitamin D levels <20 ng/mL | IG: n = 46; CG: n = 48 | IG: 77.8 ± 6.0; CG: 76.9 ± 6.5 | IG: 21.74%; CG: 18.75% |
| Vitamine D3 vs. No supplementation | ||||
| Bischoff-Ferrari H. et al. [58] NCT01745263 | RCT (placebo-controlled, double-blind, 2 × 2 × 2 factorial)/Adults ≥70 yr without major health problems in the 5 yr prior to enrollment and MMSE ≥ 24 | IG: n = 1076; CG: n = 1081 | IG: 75 ± 4.5; CG: 74.9 ± 4.4 | IG: 38%; CG: 38.6% |
| Vitamin D3 (600 IU/d) vs. Vitamin D3 (2000 IU/d) vs. Vitamin D3 (4000 IU/d) | ||||
| Castle M. et al. [59] NCT01631292 | RCT (double-blind)/Overweight/obese postmenopausal women with serum 25-hydroxyvitamin D <30 ng/mL | IG1: n = 15; IG2: n = 15; IG3: n = 12; | IG1: 58 ± 6.8; IG2: 58.5 ± 5.3; IG3: 57.2 ± 5.9; | IG1: 0%; IG2: 0%; IG3: 0%; |
| Vitamin D3 + fish oil supplements vs. Placebo | ||||
| Kang J. et al. [53] VITAL trial: NCT01169259. Two substudies:
| Large RCT (placebo-controlled, double-blind, 2 × 2 factorial)/People >60 yr free of vascular disease and cancer | VITAL-Cog substudy: IG: n = 1710; CG: n = 1714 CTSC-Cog substudy: IG: n = 396; CG: n = 398 | VITAL-Cog substudy: IG: 71.9 ± 5.4; CG: 71.8 ± 5.4 CTSC-Cog substudy: IG: 66.9 ± 5.2; CG: 67.3 ± 5.4 | VITAL-Cog substudy: IG: 40.9%; CG: 41.4% CTSC-Cog substudy: IG: 48.2%; CG: 51.0% |
| Vitamin D3 + Calcium carbonate vs. Placebo | ||||
| Rossom R.C. et al. [54] | Post-hoc analysis of an RCT (double-blind, placebo-controlled)/Women ≥65 yr without cognitive impairment at baseline | IG: n = 2034; CG: n = 2109 | IG: 70.7; CG: 70.9 | IG: 0%; CG: 0% |
| Fortified yogurts with vitamin D3 and Calcium vs. Non-fortified yogurts | ||||
| Beauchet O. et al. [57] NCT02086409 | RCT (Unicentre, single-blind, in 2 parallel groups)/Female ≥65 yr with hypovitaminosis D (seum 25 OHD concentration <75 nmol/L), calcemia <2.65 mmol/L and free of dementia | IG: n = 20; CG: n = 20 | IG: 71 ± 3.7; CG: 71.5 ± 5.2 | IG: 0%; CG: 0% |
| Vitamine E (+ selenium) vs. Placebo | ||||
| Kryscio R.J. et al. [61] NCT00040378 | First an RCT (double-blind, 4 arm); then transformed into a cohort study/men ≥60 yr in absence of dementia | IG1: n = 1799; IG2: n = 1881; IG3: n = 1828; CG: n = 1830 | IG1: 67.5 ± 5.2; IG2: 67.6 ± 5.3; IG3: 67.6 ± 5.3; CG: 67.3 ± 5.2 | IG1: 100%; IG2: 100%; IG3: 100%; CG: 100% |
| Vitamin E (+ Memantine) vs. Placebo | ||||
| Dysken M. et al. [62] NCT00235716 | RCT (double-blind, placebo-controlled, parallel-group)/People with mild to moderate AD (MMSE 12–26) currently taking AChEI | IG1: n = 152; IG2: n = 155; IG3: n = 154; CG: n = 152 | IG1: 78.6 ± 7.2; IG2: 78.8 ± 7.2; IG3: 78.3 ± 7.0; CG: 79.4 ± 7.0 | IG1: 96%; IG2: 96%; IG3: 97%; CG: 98% |
| Vitamin E + Vitamin C vs. Placebo | ||||
| Alavi Naeini A.M. et al. [63] | RCT (double-blind, placebo-controlled)/Elderly aged 60–75 yr with MCI and MMSE between 21–26 scores | IG: n = 127; CG: n = 129 | IG: 66.5 ± 0.39; CG: 66.3 ± 0.38 | IG: 49.6%; CG: 44.2% |
: male.References
- Chertkow, H.; Feldman, H.H.; Jacova, C.; Massoud, F. Definitions of dementia and predementia states in Alzheimer’s disease and vascular cognitive impairment: Consensus from the Canadian conference on diagnosis of dementia. Alzheimer’s Res. Ther. 2013, 5, S2–S8. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Dementia. Available online: https://www.who.int/news-room/fact-sheets/detail/dementia (accessed on 26 February 2020).
- Qiu, C.; Fratiglioni, L. Aging without Dementia is Achievable: Current Evidence from Epidemiological Research. J. Alzheimer’s Dis. 2018, 62, 933–942. [Google Scholar] [CrossRef] [PubMed]
- ICD-11 for Mortality and Morbidity Statistics. Available online: https://icd.who.int/browse11/l-m/en (accessed on 1 October 2019).
- Duong, S.; Patel, T.; Chang, F. Dementia. Can. Pharm. J./Rev. Pharm. Can. 2017, 150, 118–129. [Google Scholar] [CrossRef] [PubMed]
- Smith, M.; Buckwalter, K. Behaviors associated with dementia. AJN Am. J. Nurs. 2005, 105, 40–52. [Google Scholar] [CrossRef] [PubMed]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, 5th ed.; American Psychiatric Publishing, Inc.: Arlington, VA, USA, 2013. [Google Scholar] [CrossRef]
- Libon, D.; Delano-Wood, L.; Bondi, M.; Au, R. Mild Cognitive Impairment. In Encyclopedia of the Neurological Sciences; Elsevier: Amsterdam, The Netherlands, 2014; pp. 72–75. [Google Scholar] [CrossRef]
- Petersen, R.C. Mild cognitive impairment as a diagnostic entity. J. Intern. Med. 2004, 256, 183–194. [Google Scholar] [CrossRef] [PubMed]
- Dumurgier, J.; Sabia, S. Life expectancy in dementia subtypes: Exploring a leading cause of mortality. Lancet Healthy Longev. 2021, 2, e449–e450. [Google Scholar] [CrossRef]
- Long, J.M.; Holtzman, D.M. Alzheimer Disease: An Update on Pathobiology and Treatment Strategies. Cell 2019, 179, 312–339. [Google Scholar] [CrossRef]
- Alzheimer’s Association. Alzheimer’s Disease Facts and Figures. Alzheimer Dement. 2020, 16, 391–460. [Google Scholar] [CrossRef]
- Smith, E.E. Clinical presentations and epidemiology of vascular dementia. Clin. Sci. 2017, 131, 1059–1068. [Google Scholar] [CrossRef]
- Korczyn, A.; Vakhapova, V.; Grinberg, L.T. Vascular dementia. J. Neurol. Sci. 2012, 322, 2–10. [Google Scholar] [CrossRef]
- Greaves, C.V.; Rohrer, J.D. An update on genetic frontotemporal dementia. J. Neurol. 2019, 266, 2075–2086. [Google Scholar] [CrossRef] [PubMed]
- Schumacher, J.; Peraza, L.; Firbank, M.; Thomas, A.J.; Kaiser, M.; Gallagher, P.; O’brien, J.T.; Blamire, A.M.; Taylor, J.-P. Dysfunctional brain dynamics and their origin in Lewy body dementia. Brain 2019, 142, 1767–1782. [Google Scholar] [CrossRef]
- Donaghy, P.C.; McKeith, I. The clinical characteristics of dementia with Lewy bodies and a consideration of prodromal diagnosis. Alzheimer’s Res. Ther. 2014, 6, 46. [Google Scholar] [CrossRef]
- World Health Organization. Risk Reduction of Cognitive Decline and Dementia. Available online: https://www.who.int/publications/i/item/risk-reduction-of-cognitive-decline-and-dementia. (accessed on 2 January 2022).
- Livingston, G.; Sommerlad, A.; Orgeta, V.; Costafreda, S.G.; Huntley, J.; Ames, D.; Ballard, C.; Banerjee, S.; Burns, A.; Cohen-Mansfield, J.; et al. Dementia prevention, intervention, and care. Lancet 2017, 390, 2673–2734. [Google Scholar] [CrossRef]
- Livingston, G.; Huntley, J.; Sommerlad, A.; Ames, D.; Ballard, C.; Banerjee, S.; Brayne, C.; Burns, A.; Cohen-Mansfield, J.; Cooper, C.; et al. Dementia prevention, intervention, and care: 2020 report of the Lancet Commission. Lancet 2020, 396, 413–446. [Google Scholar] [CrossRef]
- Morris, M.C. Nutrition and risk of dementia: Overview and methodological issues. Ann. N. Y. Acad. Sci. 2016, 1367, 31–37. [Google Scholar] [CrossRef]
- Del Parigi, A.; Panza, F.; Capurso, C.; Solfrizzi, V. Nutritional factors, cognitive decline, and dementia. Brain Res. Bull. 2006, 69, 1–19. [Google Scholar] [CrossRef]
- Tardy, A.-L.; Pouteau, E.; Marquez, D.; Yilmaz, C.; Scholey, A. Vitamins and Minerals for Energy, Fatigue and Cognition: A Narrative Review of the Biochemical and Clinical Evidence. Nutrients 2020, 12, 228. [Google Scholar] [CrossRef]
- Del Mondo, A.; Smerilli, A.; Sané, E.; Sansone, C.; Brunet, C. Challenging microalgal vitamins for human health. Microb. Cell Factories 2020, 19, 201. [Google Scholar] [CrossRef]
- Norton, S.; Matthews, F.; Barnes, D.E.; Yaffe, K.; Brayne, C. Potential for primary prevention of Alzheimer’s disease: An analysis of population-based data. Lancet Neurol. 2014, 13, 788–794. [Google Scholar] [CrossRef]
- Meydani, M. Antioxidants and cognitive function. Nutr. Rev. 2001, 59, S75–S82. [Google Scholar] [CrossRef] [PubMed]
- Llibre Rodríguez, J.; Gutiérrez Herrera, R.F. Demencias y enfermedad de Alzheimer en América Latina y el Caribe. Rev. Cuba Salud Pública 2014, 40, 378–387. [Google Scholar]
- World Health Organization. Draft Global Action Plan on the Public Health Response to Dementia: Report by the Director-General. Available online: https://apps.who.int/iris/handle/10665/273318. (accessed on 12 November 2021).
- Patterson, C.; World Alzheimer Report 2018. The State of the Art of Dementia Research: New Frontiers. Available online: https://apo.org.au/node/260056. (accessed on 9 January 2022).
- Suh, S.W.; Kim, H.S.; Han, J.H.; Bin Bae, J.; Oh, D.J.; Kim, K.W. Efficacy of Vitamins on Cognitive Function of Non-Demented People: A Systematic Review and Meta-Analysis. Nutrients 2020, 12, 1168. [Google Scholar] [CrossRef]
- Forbes, S.C.; Holroyd-Leduc, J.M.; Poulin, M.J.; Hogan, D.B. Effect of Nutrients, Dietary Supplements and Vitamins on Cognition: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Can. Geriatr. J. 2015, 18, 231–245. [Google Scholar] [CrossRef] [PubMed]
- Li, S.; Guo, Y.; Men, J.; Fu, H.; Xu, T. The preventive efficacy of vitamin B supplements on the cognitive decline of elderly adults: A systematic review and meta-analysis. BMC Geriatr. 2021, 21, 367. [Google Scholar] [CrossRef] [PubMed]
- Farina, N.; Llewellyn, D.; Isaac, M.G.E.K.N.; Tabet, N. Vitamin E for Alzheimer’s dementia and mild cognitive impairment. Cochrane Database Syst. Rev. 2017, 4, CD002854. [Google Scholar] [CrossRef] [PubMed]
- Gestuvo, M.; Hung, W. Common dietary supplements for cognitive health. Aging Health 2012, 8, 89–97. [Google Scholar] [CrossRef] [PubMed]
- Puga, A.M.; Ruperto, M.; Samaniego-Vaesken, M.D.L.; Montero-Bravo, A.; Partearroyo, T.; Varela-Moreiras, G. Effects of Supplementation with Folic Acid and Its Combinations with Other Nutrients on Cognitive Impairment and Alzheimer’s Disease: A Narrative Review. Nutrients 2021, 13, 2966. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; Prisma Group. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. BMJ 2009, 339, b2535. [Google Scholar] [CrossRef]
- Chen, H.; Liu, S.; Ji, L.; Wu, T.; Ji, Y.; Zhou, Y.; Zheng, M.; Zhang, M.; Xu, W.; Huang, G. Folic Acid Supplementation Mitigates Alzheimer’s Disease by Reducing Inflammation: A Randomized Controlled Trial. Mediat. Inflamm. 2016, 2016, 5912146. [Google Scholar] [CrossRef]
- Walker, J.G.; Batterham, P.J.; Mackinnon, A.J.; Jorm, A.F.; Hickie, I.; Fenech, M.; Kljakovic, M.; Crisp, D.; Christensen, H. Oral folic acid and vitamin B-12 supplementation to prevent cognitive decline in community-dwelling older adults with depressive symptoms—The Beyond Ageing Project: A randomized controlled trial. Am. J. Clin. Nutr. 2011, 95, 194–203. [Google Scholar] [CrossRef] [PubMed]
- Chen, H.; Liu, S.; Ge, B.; Zhou, D.; Li, M.; Li, W.; Ma, F.; Liu, Z.; Ji, Y.; Huang, G. Effects of Folic Acid and Vitamin B12 Supplementation on Cognitive Impairment and Inflammation in Patients with Alzheimer’s Disease: A Randomized, Single-Blinded, Placebo-Controlled Trial. J. Prev. Alzheimer’s Dis. 2021, 8, 249–256. [Google Scholar] [CrossRef] [PubMed]
- Gibson, G.E.; Luchsinger, J.A.; Cirio, R.; Chen, H.; Franchino-Elder, J.; Hirsch, J.A.; Bettendorff, L.; Chen, Z.; Flowers, S.A.; Gerber, L.M.; et al. Benfotiamine and Cognitive Decline in Alzheimer’s Disease: Results of a Randomized Placebo-Controlled Phase IIa Clinical Trial. J. Alzheimer’s Dis. 2020, 78, 989–1010. [Google Scholar] [CrossRef]
- Li, M.; Li, W.; Gao, Y.; Chen, Y.; Bai, D.; Weng, J.; Du, Y.; Ma, F.; Wang, X.; Liu, H.; et al. Effect of folic acid combined with docosahexaenoic acid intervention on mild cognitive impairment in elderly: A randomized double-blind, placebo-controlled trial. Z. Ernährungswissenschaft 2021, 60, 1795–1808. [Google Scholar] [CrossRef] [PubMed]
- Kwok, T.; Wu, Y.; Lee, J.; Lee, R.; Yung, C.Y.; Choi, G.; Lee, V.; Harrison, J.; Lam, L.; Mok, V. A randomized placebo-controlled trial of using B vitamins to prevent cognitive decline in older mild cognitive impairment patients. Clin. Nutr. 2020, 39, 2399–2405. [Google Scholar] [CrossRef]
- Dangour, A.D.; Allen, E.; Clarke, R.; Elbourne, D.; Fletcher, A.E.; Letley, L.; Richards, M.; Whyte, K.; Uauy, R.; Mills, K. Effects of vitamin B-12 supplementation on neurologic and cognitive function in older people: A randomized controlled trial. Am. J. Clin. Nutr. 2015, 102, 639–647. [Google Scholar] [CrossRef]
- Moore, K.; Porter, K.; Doherty, L.; Hughes, C.; Ward, M.; Hoey, L.; Strain, J.; Pentieva, K.; McNulty, H. A randomised controlled trial of B-vitamin supplementation on neuropsychiatric performance: Results from the BrainHOP trial. Proc. Nutr. Soc. 2018, 77. [Google Scholar] [CrossRef]
- Ma, F.; Wu, T.; Zhao, J.; Han, F.; Marseglia, A.; Liu, H.; Huang, G. Effects of 6-Month Folic Acid Supplementation on Cognitive Function and Blood Biomarkers in Mild Cognitive Impairment: A Randomized Controlled Trial in China. J. Gerontol. Ser. A 2015, 71, 1376–1383. [Google Scholar] [CrossRef]
- Ma, F.; Wu, T.; Zhao, J.; Song, A.; Liu, H.; Xu, W.; Huang, G. Folic acid supplementation improves cognitive function by reducing the levels of peripheral inflammatory cytokines in elderly Chinese subjects with MCI. Sci. Rep. 2016, 6, 37486. [Google Scholar] [CrossRef]
- Ma, F.; Li, Q.; Zhou, X.; Zhao, J.; Song, A.; Li, W.; Liu, H.; Xu, W.; Huang, G. Effects of folic acid supplementation on cognitive function and Aβ-related biomarkers in mild cognitive impairment: A randomized controlled trial. Z. Ernährungswissenschaft 2017, 58, 345–356. [Google Scholar] [CrossRef]
- Jiang, B.; Ding, C.; Yao, G.; Yao, C.; Zhang, Y.; Ge, J.; Qiu, E. Intervention effect of folic acid and vitamin b12 on vascular cognitive impairment complicated with hyperhomocysteinemia/efekat intervencije folnom kiselinom i vitaminom b12 na vaskularni kognitivni poremećaj komplikovan hiperhomocisteinemijom. J. Med. Biochem. 2013, 33, 169–174. [Google Scholar] [CrossRef][Green Version]
- Lu, R.; Fang, Y.; Zhou, Y.; Che, M.; Shen, J.; Liu, Q.; Zhang, H.; Pan, S.; Lin, Y.; Wang, Q.; et al. A pilot study of thiamin and folic acid in hemodialysis patients with cognitive impairment. Ren. Fail. 2021, 43, 766–773. [Google Scholar] [CrossRef] [PubMed]
- Vijayakumar, T.M.; Pavitra, K.; Muthunarayanan, L. Comparative assessment of methylcobalamin and ascorbic acid on cognitive function in post-menopausal women—A randomized, double-blind trial. Contemp. Clin. Trials Commun. 2017, 8, 175–180. [Google Scholar] [CrossRef]
- Aspell, N.; Healy, M.; Mc Partlin, J.; Lawlor, B.; O’Sullivan, M. Effects of vitamin D supplementation on cognitive function in healthy, community dwelling older adults: Results from a randomised double-blind placebo-controlled pilot trial. Proc. Nutr. Soc. 2017, 76. [Google Scholar] [CrossRef]
- Stein, M.S.; Scherer, S.C.; Ladd, K.S.; Harrison, L.C. A Randomized Controlled Trial of High-Dose Vitamin D2 Followed by Intranasal Insulin in Alzheimer’s Disease. J. Alzheimer’s Dis. 2011, 26, 477–484. [Google Scholar] [CrossRef] [PubMed]
- Kang, J.H.; Vyas, C.M.; Okereke, O.I.; Ogata, S.; Albert, M.; Lee, I.-M.; D’agostino, D.; Buring, J.E.; Cook, N.R.; Grodstein, F.; et al. Effect of vitamin D on cognitive decline: Results from two ancillary studies of the VITAL randomized trial. Sci. Rep. 2021, 11, 23253. [Google Scholar] [CrossRef]
- Rossom, R.C.; Espeland, M.A.; Manson, J.E.; Dysken, M.W.; Johnson, K.C.; Lane, D.S.; Leblanc, E.S.; Lederle, F.A.; Masaki, K.H.; Margolis, K.L. Calcium and Vitamin D Supplementation and Cognitive Impairment in the Women’s Health Initiative. J. Am. Geriatr. Soc. 2012, 60, 2197–2205. [Google Scholar] [CrossRef]
- Annweiler, C.; Fantino, B.; Gautier, J.; Beaudenon, M.; Thiery, S.; Beauchet, O. Cognitive Effects of Vitamin D Supplementation in Older Outpatients Visiting a Memory Clinic: A Pre-Post Study. J. Am. Geriatr. Soc. 2012, 60, 793–795. [Google Scholar] [CrossRef]
- Lee, Y.J.; Sohng, K.Y. Effects of Vitamin D on depression, cognitive function, and physical function in elderly individuals living alone. Int. J. Gerontol. 2019, 13, 196–201. [Google Scholar] [CrossRef]
- Beauchet, O.; Launay, C.; Galery, K.; Vilcocq, C.; Dontot-Payen, F.; Rousseau, B.; Benoit, V.; Allali, G. Effects of Vitamin D and Calcium Fortified Yogurts on Gait, Cognitive Performances, and Serum 25-Hydroxyvitamin D Concentrations in Older Community-Dwelling Females: Results from the GAit, MEmory, Dietary and Vitamin D (GAME-D2) Randomized Controlled Trial. Nutrients 2019, 11, 2880. [Google Scholar] [CrossRef]
- Bischoff-Ferrari, H.A.; Vellas, B.; Rizzoli, R.; Kressig, R.W.; da Silva, J.A.P.; Blauth, M.; Felson, D.T.; McCloskey, E.V.; Watzl, B.; Hofbauer, L.C.; et al. Effect of Vitamin D Supplementation, Omega-3 Fatty Acid Supplementation, or a Strength-Training Exercise Program on Clinical Outcomes in Older Adults. JAMA: J. Am. Med Assoc. 2020, 324, 1855–1868. [Google Scholar] [CrossRef] [PubMed]
- Castle, M.; Fiedler, N.; Pop, L.C.; Schneider, S.J.; Schlussel, Y.; Sukumar, D.; Hao, L.; Shapses, S.A. Three Doses of Vitamin D and Cognitive Outcomes in Older Women: A Double-Blind Randomized Controlled Trial. J. Gerontol. Ser. A 2020, 75, 835–842. [Google Scholar] [CrossRef] [PubMed]
- Schietzel, S.; Fischer, K.; Brugger, P.; Orav, E.J.; Renerts, K.; Gagesch, M.; Freystaetter, G.; Stähelin, H.B.; Egli, A.; Bischoff-Ferrari, H.A. Effect of 2000 IU compared with 800 IU vitamin D on cognitive performance among adults age 60 years and older: A randomized controlled trial. Am. J. Clin. Nutr. 2019, 110, 246–253. [Google Scholar] [CrossRef] [PubMed]
- Kryscio, R.J.; Abner, E.L.; Caban-Holt, A.; Lovell, M.; Goodman, P.; Darke, A.; Yee, M.; Crowley, J.; Schmitt, F.A. Association of Antioxidant Supplement Use and Dementia in the Prevention of Alzheimer’s Disease by Vitamin E and Selenium Trial (PREADViSE). JAMA Neurol. 2017, 74, 567–573. [Google Scholar] [CrossRef]
- Dysken, M.W.; Sano, M.; Asthana, S.; Vertrees, J.E.; Pallaki, M.; Llorente, M.; Love, S.; Schellenberg, G.D.; McCarten, J.R.; Malphurs, J.; et al. Effect of Vitamin E and Memantine on Functional Decline in Alzheimer Disease: The TEAM-AD VA cooperative randomized trial. JAMA 2014, 311, 33–44. [Google Scholar] [CrossRef]
- Naeini, A.M.A.; Elmadfa, I.; Djazayery, A.; Barekatain, M.; Ghazvini, M.R.A.; Djalali, M.; Feizi, A. The effect of antioxidant vitamins E and C on cognitive performance of the elderly with mild cognitive impairment in Isfahan, Iran: A double-blind, randomized, placebo-controlled trial. Z. Ernährungswissenschaft 2013, 53, 1255–1262. [Google Scholar] [CrossRef]
- Ritchie, K. Mild cognitive impairment: An epidemiological perspective. Dialog. Clin. Neurosci. 2004, 6, 401–408. [Google Scholar] [CrossRef]
- Kumar, A.; Sidhu, J.; Goyal, A.; Tsao, J.W. Alzheimer Disease. In StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2022. Available online: https://www.ncbi.nlm.nih.gov/books/NBK499922/ (accessed on 31 January 2022).
- Dominguez, L.J.; Barbagallo, M. Nutritional prevention of cognitive decline and dementia. Acta Biomed. 2018, 89, 276–290. [Google Scholar]
- McCleery, J.; Abraham, R.P.; Denton, D.A.; Rutjes, A.W.S.; Chong, L.-Y.; Al-Assaf, A.S.; Griffith, D.J.; Rafeeq, S.; Yaman, H.; Malik, M.A.; et al. Vitamin and mineral supplementation for preventing dementia or delaying cognitive decline in people with mild cognitive impairment. Cochrane Database Syst. Rev. 2018, 2019, CD011905. [Google Scholar] [CrossRef]
- Beauchet, O.; Cooper-Brown, L.A.; Allali, G. Vitamin D Supplementation and Cognition in Adults: A Systematic Review of Randomized Controlled Trials. CNS Drugs 2021, 35, 1249–1264. [Google Scholar] [CrossRef]

| Alzheimer’s disease |
|
| Vascular dementia |
|
| Frontotemporal lobar degeneration |
|
| Lewy body dementia (LBD) |
|
| Patient (P) | Adults with normal cognition, MCI, or Alzheimer’s disease with an age > 45 yr. There were no restrictions on sex, ethnicity, or severity of the cognitive impairment at baseline. |
| Intervention (I) | Vitamins as dietary supplements (A, B1, B2, B3, B5, B6, B9, B12, H, C, D, E, K). Co-interventions between vitamins were allowed. |
| Comparison (C) | Standard of care, no intervention, placebo, another dosage regimen, or other intervention (including but not limited to vitamins). |
| Outcome (O) |
|
| Type of studies (S) |
|
| Intervention Group | Control Group | p Value | |
|---|---|---|---|
| Mean MMSE Scores ± SD after 6 months of supplementation | 18.72 ± 6.56 | 16.80 ± 8.26 | 0.041 |
| Mean ADL scores ± SD after 6 months of treatment | 32.93 ± 10.93 | 34.10 ± 14.15 | 0.895 |
| At Baseline | At 6 Months | p Value | |
|---|---|---|---|
| Mean FSIQ score ± SD in IG1 (FA + DHA) | 100.45 ± 3.90 | 104.04 ± 2.72 | p < 0.001 |
| Mean FSIQ score ± SD in CG | 101.68 ± 4.18 | 102.63 ± 2.61 |
| Pre-Intervention | Post-Intervention | p Value | |
|---|---|---|---|
| Mean FAB total score | IG (15.1) vs. CG (14.7) | IG (14.7) vs. CG (14.4) | p = 0.485 |
| Mean RBANS total score | IG (93.4) vs. CG (93.3) | IG (97.8) vs. CG (95.5) | p = 0.117 |
| Intervention Group | Control Group | p Value | |
|---|---|---|---|
| MMSE score after treatment, median (IQR) | 28.0 (4.0) | 24.0 (4.0) | p = 0.04 |
| CAB score after treatment, median (IQR) | 90 (12.0) | 89 (6.0) | p = 0.03 |
| FAB score after treatment, median (IQR) | 16.0 (2.0) | 15.0 (3.0) | p = 0.04 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gil Martínez, V.; Avedillo Salas, A.; Santander Ballestín, S. Vitamin Supplementation and Dementia: A Systematic Review. Nutrients 2022, 14, 1033. https://doi.org/10.3390/nu14051033
Gil Martínez V, Avedillo Salas A, Santander Ballestín S. Vitamin Supplementation and Dementia: A Systematic Review. Nutrients. 2022; 14(5):1033. https://doi.org/10.3390/nu14051033
Chicago/Turabian StyleGil Martínez, Victoria, Ana Avedillo Salas, and Sonia Santander Ballestín. 2022. "Vitamin Supplementation and Dementia: A Systematic Review" Nutrients 14, no. 5: 1033. https://doi.org/10.3390/nu14051033
APA StyleGil Martínez, V., Avedillo Salas, A., & Santander Ballestín, S. (2022). Vitamin Supplementation and Dementia: A Systematic Review. Nutrients, 14(5), 1033. https://doi.org/10.3390/nu14051033