
Do Vegetarian Diets Provide Adequate Nutrient Intake during Complementary Feeding? A Systematic Review

 , , , and
, , , and
Abstract
:1. Introduction
1.1. Why This Systematic Review Is Important
1.2. Objectives
1.3. Key Questions
- Does complementary feeding completely or partially free of animal-source foods in healthy infants result in significantly different auxological development and/or growth compared with that of infants on a balanced omnivorous diet?
- Does complementary feeding completely or partially free of animal-source foods in healthy infants/toddlers result in a psychomotor development that is significantly different from that of infants on a balanced omnivorous diet?
- Do healthy infants on a complementary feeding that is completely or partially free of any animal-based foods
- ◦
- have a different risk of developing NCDs (obesity/overweight, hypertension, diabetes mellitus)?
- ◦
- have a different risk of developing vitamin or other micronutrient deficiencies?
- ◦
- have a different risk of developing infections and related outcomes compared with infants on a balanced omnivorous diet?
2. Materials and Methods
2.1. Design of the Studies Included
- Randomized controlled trials (RCTs) and controlled trials (CTs) in which the effect of the caregivers’ feeding practices could be accurately assessed as an experimental intervention.
- Observational studies (cohort studies, longitudinal studies, case-control studies, and cross-sectional studies) in which this effect could be evaluated as an exposure factor while taking into account possible confounding factors.
2.2. Population
2.3. Intervention(s), Exposure(s)
2.4. Comparator(s)/Control
2.5. Inclusion Criteria
- Intervention and observational studies conducted in industrialized countries.
- Studies in which the intervention or exposure was present during the period of complementary feeding (6–24 months).
- Studies comparing vegetarian diets (LOV, vegan, macrobiotic and others, completely free of animal protein) and healthy diets (e.g., MD).
- Studies with follow-up greater than 12 months.
2.6. Exclusion Criteria
- Studies conducted on populations with characteristics different from those established in the PICOs (e.g., children living in LICs (low-income countries), preterm infants, low birth weight infants, children who developed peri-neonatal diseases and children with chronic diseases).
- Non-comparative studies.
- Comparisons between vegetarian and Western-type diets or other non-healthy diets are excluded as wholly inappropriate.
- Studies on so-called dietary patterns in the absence of a precise definition/documentation of what in the individual study was considered a “vegetarian pattern or diet”.
- Follow-up of fewer than 12 months.
- Case reports and case series, despite low quality, have been included in this SR, being a large part of the literature on this topic.
2.7. Outcomes
2.7.1. Main Outcomes
- General growth parameters assessed in prospective differential terms (different increase in weight (W) or length (L) over time) or assessed at a specific time point (with differing frequencies of weights and lengths in the populations being compared: W, L, W/L z-score ratio, body mass index (BMI), BMI z-score (BMIz).
- Risk of wasted and/or stunted growth.
- Risk of impaired neurodevelopment.
- Risk of NCDs (overweight/obesity).
2.7.2. Additional Outcomes
- Risk of deficiency of vitamins and micronutrients.
- Risk of infections.
- Risk of NCDs (T2DM, and hypertension) later in life.
2.8. Keywords and Search Strategy
2.9. Measures of Effect
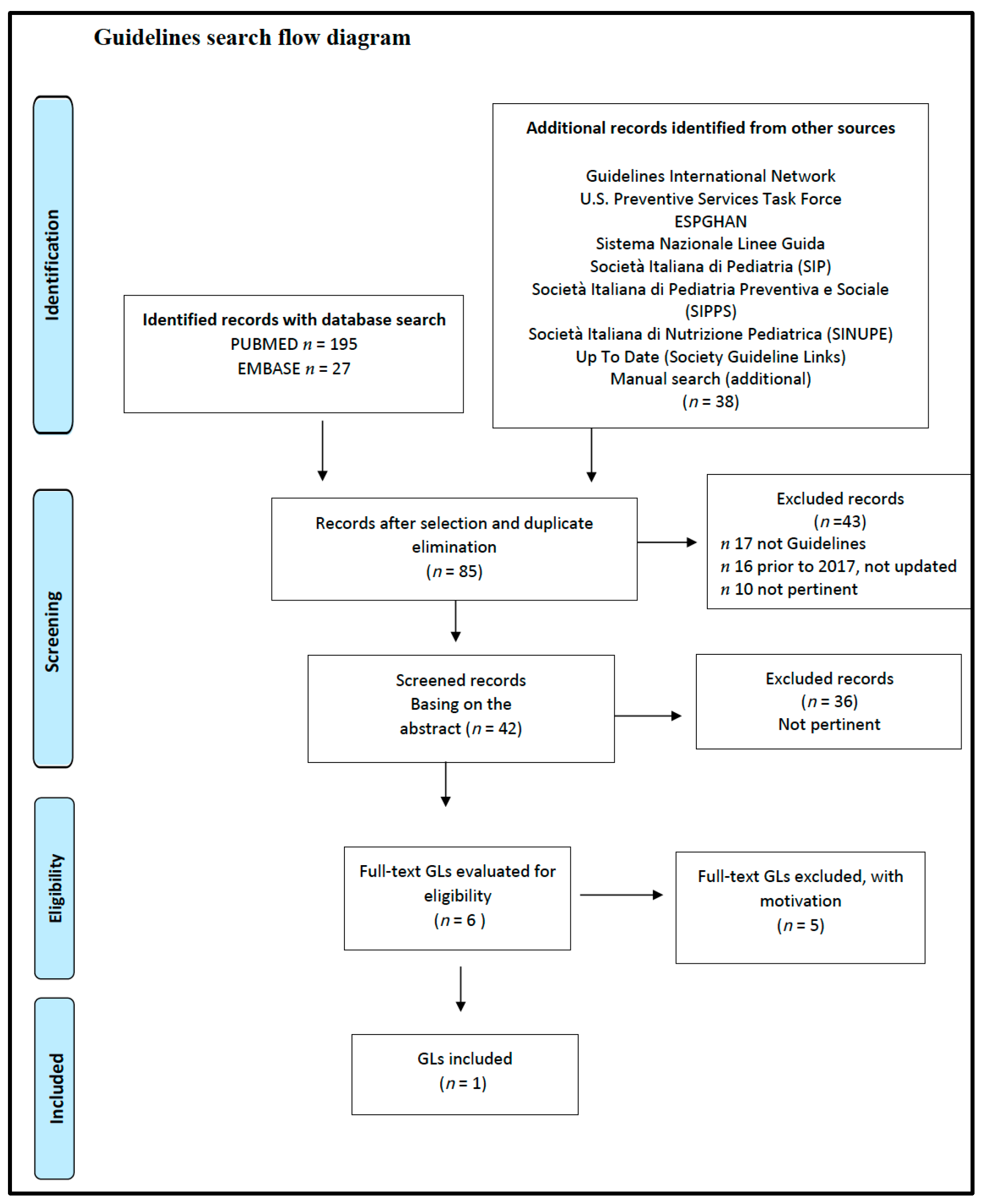
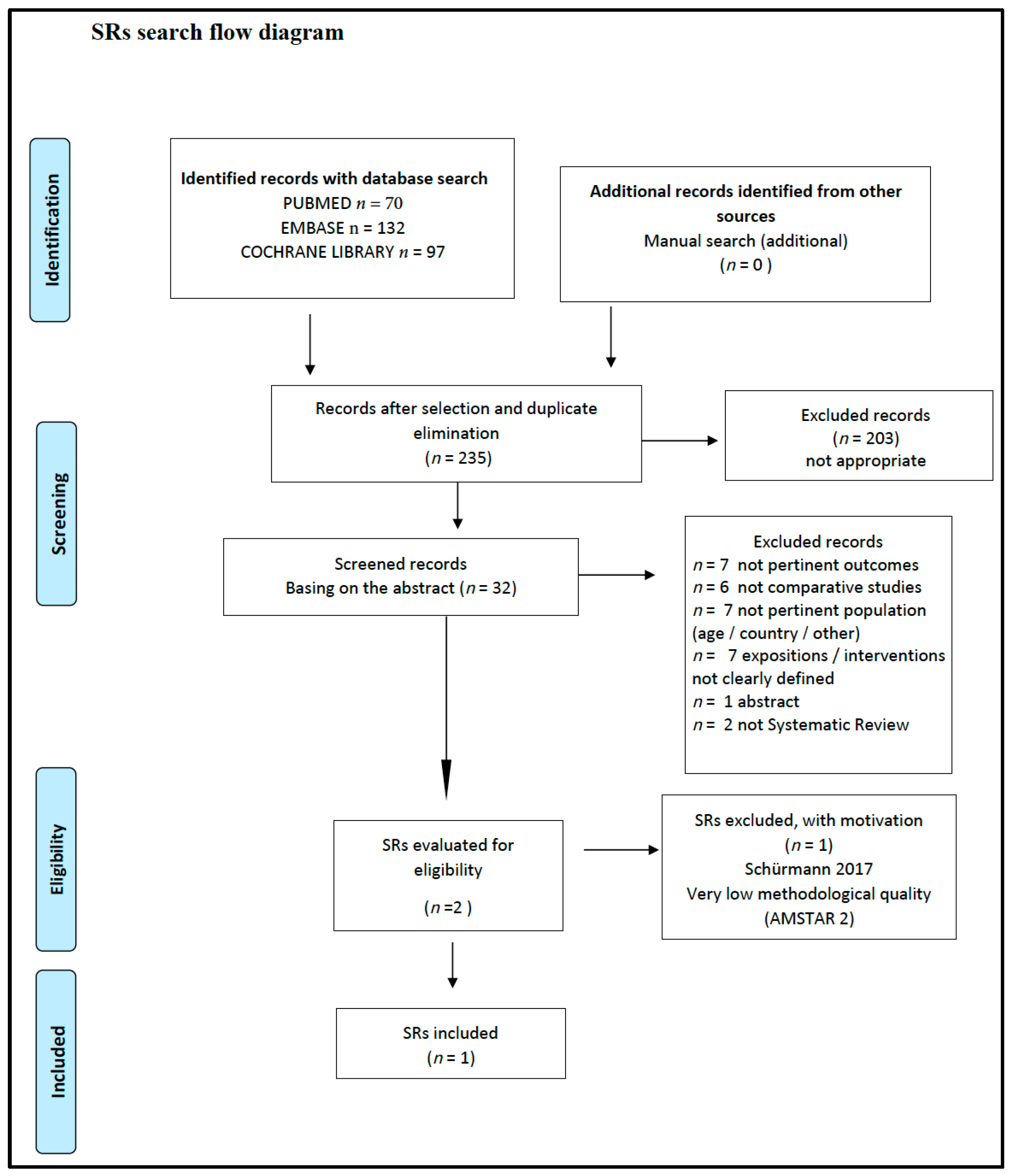
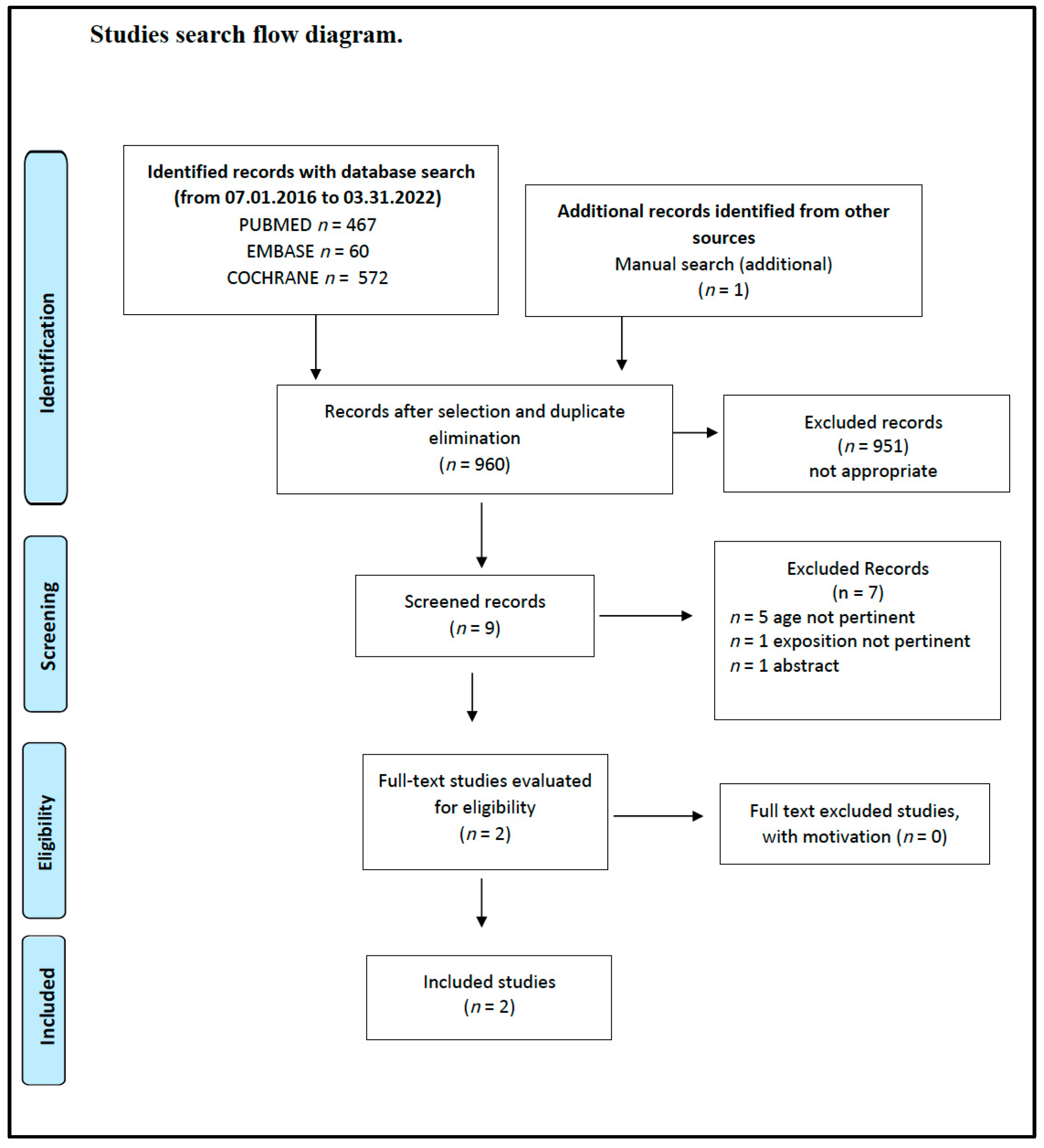
2.10. Study Selection
2.11. Strategy for Data Synthesis. Additional Analysis of the Results
2.12. Software
3. Results
3.1. Does Complementary Feeding Completely or Partially Free of Animal-Source Foods in Healthy Infants Result in Significantly Different Auxological Development and/or Growth Compared with That of Infants on a Balanced Omnivorous Diet?
3.2. Does Complementary Feeding Completely or Partially Free of Animal-Source Foods in Healthy Infants/Toddlers Result in a Psychomotor Development That Is Significantly Different from That of Infants on a Balanced Omnivorous Diet?
- Gross Motor DevelopmentSitting balance and head control SD = −0.48; p = 0.04.Walking SD = −0.60; p = 0.001.Overall score SD = −0.63; p < 0.001.
- Fine Motor Development SD = −0.13; p = 0.49.
- Language Development SD = −0.42; p = 0.03.
3.3. Do Healthy Infants on a Complementary Feeding That Is Completely or Partially Free of Any Animal-Based Foods
- Have a different risk of developing NCDs (Obesity/Overweight/Hypertension, Diabetes Mellitus)?
- Have a different risk of developing vitamin or other micronutrient deficiencies?
- Have a different risk of developing infections and related outcomes compared to infants on a balanced omnivorous diet?
3.3.1. Risk of Developing NCDs
3.3.2. Risk of Developing Vitamin or Other Micronutrient Deficiencies
3.3.3. Risk of Developing Infections
4. Discussion
4.1. Scientific Evidence on the Safety and Efficacy of Vegetarian Diets in Children and Adolescents
4.1.1. Weight–Length Gain
4.1.2. Psychomotor Development
4.1.3. Risk of NCDs (Obesity/Overweight, Hypertension, Diabetes Mellitus)
4.1.4. Risk of Vitamin or Other Micronutrient Deficiencies
4.1.5. Risk of Infection
4.2. Assessment of Vegetarian Diets: Main Issues
4.2.1. The Definition of a Healthy Diet
4.2.2. The Quality of Scientific Evidence
- Limited numbers of studies specific to some ages, particularly in the CF period.
- Lack of robust, evidence-based GLs where recommendations are not supported by reliable evidence.
- Lack of high-quality comparative studies, even if observational, and lack of RCTs in pediatric age.
- Results too often referred to intakes rather than robust outcomes such as growth and risk of developing conditions (e.g., anemia, overweight/obesity).
- Small samples or outdated cross-sectional studies;
- Unclear differentiation between different types of diets (non-pure VG or VN), as there is often uncertainty on the exposure factors (incorrect definition of “vegetarian diet”, supplementation, diet not strictly followed with occasional consumption of foods of animal origin);
- Studies, more often than not, relying on self-reported data;
- Comparative study with unbalanced omnivorous diets (Western diet) or not precisely defined (generically “omnivorous”), resulting in unclear results that are not transferable to patients with healthy eating habits.
4.2.3. Supplementation: Compliance and Costs
5. Quality of Evidence
- The uncertainty of exposure (self-reported diet), and/or
- The unclear definition of the comparison diet, generically described as “omnivorous”;
- The time of assessment of the outcome, and/or
- The absence of the outcome of interest at the start of the study is not demonstrated.
6. Agreements and Disagreements with Other Studies or Reviews
7. Limitations of the SR and Potential Bias in the Review Process
8. Implications for Research
- A design including the most important confounding factors: any supplements and breast/formula feeding. This will support the reliability of the results obtained, as well as the real impact of the type of diet on relevant outcomes.
- A clear definition of the exposure (in terms of type of diet), which should be limited to the sole period of CF (i.e., 6 months to 2 years of age) and be carefully monitored over time to ensure their real and continuous presence.
- Strict criteria to define which categories of infants and families can be enrolled as control groups; this will avoid similar expositions in subjects pertaining to different groups, as well as differences that might influence the results (e.g., different percentages of breastfed infants between the intervention and control groups).
- An appropriate follow-up period of time, possibly of at least three years, to collect data on predefined outcomes.
- The most limited drop-off possible, even in observational studies.
- A uniform instrumental documentation of specific outcomes, namely the anthropometric ones, that should be collected by qualified health care professionals.
9. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Cancer Research Fund; American Institute for Cancer Research. Food, Nutrition, Physical Activity and the Prevention of Cancer: A Global Perspective; World Cancer Research Fund; American Institute for Cancer Research: Washington, DC, USA, 2007. [Google Scholar]
- Rahe, C.; Unrath, M.; Berger, K. Dietary patterns and the risk of depression in adults: A systematic review of observational studies. Eur. J. Nutr. 2014, 53, 997–1013. [Google Scholar] [CrossRef] [PubMed]
- WHO. Fifty-Fifth World Health Assembly, Provisional Agenda Item 13.10. Infant and Young Child Nutrition, Global Strategy on Infant and Young Child Feeding. Geneva 16-04-2002. Available online: https://apps.who.int/iris/handle/10665/78470 (accessed on 30 July 2022).
- Fox, N.; Ward, K. Health, ethics and environment: A qualitative study of vegetarian motivations. Appetite 2008, 50, 422–429. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.; Rotundo, L.; Song, D. The Prevalence and Characteristics of Vegetarian in the United States: A Population-Based Study. Gastroenterology 2017, 152 (Suppl. 1), S1016. [Google Scholar] [CrossRef]
- Daniel, C.R.; Cross, A.J.; Koebnick, C.; Sinha, R. Trends in meat consumption in the USA. Public Health Nutr. 2011, 14, 575–583. [Google Scholar] [CrossRef]
- Phillips, F. Vegetarian nutrition. Br. Nutr. Found. Nutr. Bull. 2005, 30, 132–167. [Google Scholar] [CrossRef]
- Mensink, G.B.M.; Kleiser, C.; Richter, A. Lebensmittelverzehr bei Kindern und Jugendlichen in Deutschland. Bundesgesundheitsblatt Gesundheitsforschung Gesundheitsschutz 2007, 50, 609–623. [Google Scholar] [CrossRef]
- Eurispes. RI2022, Summary Document, 34th Italy Report. page 86–87. Available online: https://eurispes.eu/wp-content/uploads/2022/05/sintesi-ri2022_en-.pdf (accessed on 30 July 2022).
- Schürmann, S.; Kersting, M.; Alexy, U. Vegetarian diets in children: A systematic review. Eur. J. Nutr. 2017, 56, 1797–1817. [Google Scholar] [CrossRef]
- Le, L.T.; Sabaté, J. Beyond Meatless, the Health Effects of Vegan Diets: Findings from the Adventist Cohorts. Nutrients 2014, 6, 2131–2147. [Google Scholar] [CrossRef]
- Hoek, A.C.; Luning, P.A.; Stafleu, A.; de Graaf, C. Food-related lifestyle and health attitudes of Dutch vegetarians, non-vegetarian. Appetite 2004, 42, 265–272. [Google Scholar] [CrossRef]
- Lea, E.; Worsley, A. Influences on meat consumption in Australia. Appetite 2001, 36, 127–136. [Google Scholar] [CrossRef]
- Rees, K.; Hartley, L.; Flowers, N.; Clarke, A.; Hooper, L.; Thorogood, M.; Stranges, S. ‘Mediterranean’ dietary pattern for the primary prevention of cardiovascular disease. Cochrane Database Syst. Rev. 2013, 12, CD009825. [Google Scholar] [CrossRef] [PubMed]
- Fessler, D.M.; Arguello, A.P.; Mekdara, J.M.; Macias, R. Disgust sensitivity and meat consumption: A test of an emotivist account of moral vegetarianism. Appetite 2003, 41, 31–41. [Google Scholar] [CrossRef]
- Kenyon, P.M.; Barker, M.E. Attitudes towards meat-eating in vegetarian and non-vegetarian teenage girls in England—An ethnographic approach. Appetite 1998, 30, 185–198. [Google Scholar] [CrossRef] [PubMed]
- Santos, M.L.; Booth, D.A. Influences on meat avoidance among British students. Appetite 1996, 27, 197–205. [Google Scholar] [CrossRef]
- Melina, V.; Craig, W.; Levin, S. Position of the Academy of Nutrition and Dietetics: Vegetarian Diets. J. Acad. Nutr. Diet. 2016, 116, 1970–1980. [Google Scholar] [CrossRef]
- National Health and Medical Research Council (Hg). Eat for Health. Australian Dietary Guidelines; National Health and Medical Research Council: Canberra, Australia, 2013.
- Direção-Geral da Saúde (Hg). National Programme for the Promotion of a Healthy Diet, Guidelines for a Healthy Vegetarian Diet; Direção-Geral da Saúde: Lissabon, Portugal, 2015.
- Amit, M. Vegetarian diets in children and adolescents. Paediatr. Child Health 2010, 15, 303–314, [reaffirmed 2014]. [Google Scholar]
- Richter, M.; Boeing, H.; Grünewald-Funk, D.; Heseker, H.; Kroke, A.; Leschik-Bonnet, E.; Oberritter, H.; Strohm, D.; Watzl, B. Vegan Diet Position of the German Nutrition Society (DGE). Ernaehrungs Umsch. Int. 2016, 63, 92–102. [Google Scholar]
- SIPPS; FIMP; SIMA; SIMP. Position Paper—Diete vegetariane in gravidanza ed età evolutiva. Riv. Ital. Pediatr. Prev. Soc. 2017, 12 (Suppl. 3), 119–193. Available online: https://www.sipps.it/attivita-editoriale/position-paper-diete-vegetariane-in-gravidanza-ed-in-eta-evolutiva/ (accessed on 30 July 2022).
- Kennedy, E.T.; Ohls, J.; Carlson, S.; Fleming, K. The Healthy Eating Index: Design and applications. J. Am. Diet. Assoc. 1995, 95, 1103–1108. [Google Scholar] [CrossRef]
- Guenther, P.M.; Casavale, K.O.; Reedy, J.; Kirkpatrick, S.I.; Hiza, H.A.B.; Kuczynski, K.J.; Kahle, L.L.; Krebs-Smith, S.M. Update of the Healthy Eating Index: HEI2010. J. Acad. Nutr. Diet. 2013, 113, 569–580. [Google Scholar] [CrossRef]
- Sotos-Prieto, M.; Moreno-Franco, B.; Ordovas, J.M.; León, M.; Casasnovas, J.A.; Peñalvo, J.L. Design and development of an instrument to measure overall lifestyle habits for epidemiological research: The Mediterranean Lifestyle Index. Public Health Nutr. 2015, 18, 959–967. [Google Scholar] [CrossRef] [PubMed]
- Schwingsbachl, L.; Hoffmann, G. Diet quality as assessed by the Healthy Eating Index, the Alternate Healthy Index, the Dietary Approaches to Stop Hypertension score, and health outcomes: A systematic review and meta-analysis of cohort studies. J. Acad. Nutr. Diet. 2015, 115, 780–800. [Google Scholar] [CrossRef] [PubMed]
- Prospero—International Prospective Register of Systematic Reviews. Available online: https://www.crd.york.ac.uk/prospero/display_record.php?ID=CRD42021273592 (accessed on 15 July 2022).
- Brouwers, M.; Kho, M.E.; Browman, G.P.; Burgers, J.S.; Cluzeau, F.; Feder, G.; Fervers, B.; Graham, I.D.; Grimshaw, J.; Hanna, S.E.; et al. AGREE II: Advancing guideline development, reporting, and evaluation in healthcare. Can. Med. Assoc. J. 2010, 182, E839–E842. Available online: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3001530/ (accessed on 15 July 2022). [CrossRef] [Green Version]
- Shea, B.J.; Reeves, B.C.; Wells, G.; Thuku, M.; Hamel, C.; Moran, J.; Moher, D.; Tugwell, P.; Welch, V.; Kristjansson, E.; et al. AMSTAR 2: A critical appraisal tool for systematic reviews that include randomised or non-randomised studies of healthcare interventions, or both. BMJ 2017, 358, j4008. [Google Scholar] [CrossRef]
- Higgins, J.P.T.; Green, S. (Eds.) Cochrane Handbook for Systematic Reviews of Interventions [Updated March 2011]; Wiley-Blackwell: Chichester, UK, 2011. [Google Scholar]
- Wells, G.A.; Shea, B.; O’Connell, D.; Peterson, J.; Welch, V.; Losos, M.; Tugwell, P. The Newcastle-Ottawa Scale (NOS) for Assessing the Quality of Nonrandomized Studies in Meta-Analyses. Available online: http://www.ohri.ca/programs/clinical_epidemiology/oxford.asp (accessed on 15 July 2022).
- Schünemann, H.J.; Oxman, A.D.; Brozek, J.; Glasziou, P.; Jaeschke, R.; Vist, G.E.; Williams, J.W.; Kunz, R.; Craig, J.; Montori, V.M.; et al. GRADE Working Group. Grading quality of evidence and strength of recommendations for diagnostic tests and strategies. BMJ 2008, 336, 1106–1110. [Google Scholar] [CrossRef] [PubMed]
- Guyatt, G.H.; Oxman, A.D.; Kunz, R.; Falck-Ytter, Y.; Vist, G.E.; Liberati, A.; Schünemann, H.J. GRADE Working Group. Going from evidence to recommendations. BMJ 2008, 336, 1049–1051. [Google Scholar] [CrossRef]
- Guyatt, G.H.; Oxman, A.D.; Kunz, R.; Jaeschke, R.; Helfand, M.; Liberati, A.; Vist, G.E.; Schünemann, H.J. GRADE working group. Incorporating considerations of resource use into grading recommendations. BMJ 2008, 336, 1170–1173. [Google Scholar] [CrossRef]
- Caroli, M.; Vania, A.; Verga, M.C.; Di Mauro, G.; Bergamini, M.; Cuomo, B.; D’Anna, R.; D’Antonio, G.; Dello Iacono, I.; Dessì, A.; et al. Recommendations on Complementary Feeding as a Tool for Prevention of Non-Communicable Diseases (NCDs)—Paper Co-Drafted by the SIPPS, FIMP, SIDOHaD, and SINUPE Joint Working Group. Nutrients 2022, 14, 257. [Google Scholar] [CrossRef]
- Higgins, J.P.T.; Thomas, J.; Chandler, J.; Cumpston, M.; Li, T.; Page, M.J.; Welch, V.A. (Eds.) Cochrane Handbook for Systematic Reviews of Interventions Version 6.2; John Wiley & Sons: Chichester, UK, 2019; (Updated February 2021); Available online: www.training.cochrane.org/handbook (accessed on 15 July 2022).
- Sterne, J.A.C.; Hernán, M.A.; Reeves, B.C.; Savović, J.; Berkman, N.D.; Viswanathan, M.; Henry, D.; Altman, D.G.; Ansari, M.T.; Boutron, I.; et al. ROBINS-I: A tool for assessing risk of bias in non-randomized studies of interventions. BMJ 2016, 355, i4919e. [Google Scholar] [CrossRef]
- Nordic Cochrane Centre, The Cochrane Collaboration. Review Manager 5 (RevMan 5). Version 5.3; Nordic Cochrane Centre, The Cochrane Collaboration: Copenhagen, Denmark, 2014. [Google Scholar]
- McMaster University (Developed by Evidence Prime). GRADEpro GDT; McMaster University (Developed by Evidence Prime): Hamilton, ON, Canada; Available online: https://gradepro.org/ (accessed on 15 July 2022).
- English, L.K.; Obbagy, J.E.; Wong, Y.P.; Butte, N.F.; Dewey, K.G.; Fox, M.K.; Greer, F.R.; Krebs, N.F.; Scanlon, K.S.; Stoody, E.E. Types and amounts of complementary foods and beverages consumed and growth, size, and body composition: A systematic review. Am. J. Clin. Nutr. 2019, 109 (Suppl. 7), 956S–977S. [Google Scholar]
- Dagnelie, P.C.; van Staveren, W.A. Macrobiotic nutrition and child health: Results of a population-based, mixed-longitudinal cohort study in The Netherlands. Am. J. Clin. Nutr. 1994, 59, 1187s–1196s. [Google Scholar] [CrossRef] [PubMed]
- Weder, S.; Hoffmann, M.; Becker, K.; Alexy, U.; Keller, M. Energy, macronutrient intake, and anthropometrics of vegetarian, vegan, and omnivorous children (1–3 years) in Germany (VeChi diet study). Nutrients 2019, 11, 832. [Google Scholar] [CrossRef] [PubMed]
- Smeets, F.W.M.; Dagnelie, P.C.; Van Staveren, W.A.; Van Kuik, M.J.J.A.; Matze, M.; Schlatmann, A.M. Implementation of nutrition recommendations by macrobiotic families in the Netherlands and growth of macrobiotic children until 9 years of age. Tijdschr. Soc. Gezondheidsz 1992, 70, 227–233. [Google Scholar]
- DGE; ÖGE; SGE. Referenzwerte für die Nährstozufuhr, 2. Auflage, 2., Aktualisierte Ausgabe; Deutsche Gesellschaft für Ernährung, Österreichische Gesellschaft für Ernährung, Schweizerische Gesellschaft für Ernährung: Bonn, Germany, 2016. [Google Scholar]
- Blasco-Alonso, J.; Gil-Gómez, R.; García Ruiz, A.; Cortés Hernández, M.; Gutiérrez Schiaffino, G. Encefalopatía grave y deficiencia de vitamina B12: Reversibilidad tras la terapia nutricional. Nutr. Hosp. 2020, 37, 1285–1288. [Google Scholar] [PubMed]
- Lemoine, A.; Giabicani, E.; Lockhart, V.; Grimprel, E.; Tounian, P. Case report of nutritional rickets in an infant following a vegan diet. Arch. Pediatr. 2020, 27, 219–222. [Google Scholar] [CrossRef]
- Lund, A.M. Questions about a vegan diet should be included in differential diagnostics of neurologically abnormal infants with failure to thrive. Acta Paediatr. 2019, 108, 1377–1379. [Google Scholar] [CrossRef]
- Smolka, V.; Bekárek, V.; Hlídková, E.; Bucil, J.; Mayerová, D.; Skopková, Z.; Adam, T.; Hrubá, E.; Kozich, V.; Buriánková, L.; et al. Metabolické komplikace a neurologické projevy pri deficitu vitaminu B12 u dĕtí vegetariánských matek. Cas. Lek. Ces. 2001, 140, 732–735. [Google Scholar]
- von Schenck, U.; Bender-Götze, C.; Koletzko, B. Persistence of neurological damage induced by dietary vitamin B-12 deficiency in infancy. Arch. Dis. Child. 1997, 77, 137–139. [Google Scholar] [CrossRef]
- Lövblad, K.; Ramelli, G.; Remonda, L.; Nirkko, A.C.; Ozdoba, C.; Schroth, G. Retardation of myelination due to dietary vitamin B12 deficiency: Cranial MRI findings. Pediatr. Radiol. 1997, 27, 155–158. [Google Scholar] [CrossRef]
- Grattan-Smith, P.J.; Wilcken, B.; Procopis, P.G.; Wise, G.A. The neurological syndrome of infantile cobalamin deficiency: Developmental regression and involuntary movements. Mov. Disord. 1997, 12, 39–46. [Google Scholar] [CrossRef]
- Taylor, A.; Redworth, E.W.; Morgan, J.B. Influence of diet on iron, copper, and zinc status in children under 24 months of age. Biol. Trace Elem. Res. 2004, 97, 197–214. [Google Scholar] [CrossRef]
- Georgieff, M.K.; Brunette, K.E.; Tran, P.T. Early life nutrition and neural plasticity. Dev. Psychopathol. 2015, 27, 411–423. [Google Scholar] [CrossRef]
- Stonehouse, W. Does consumption of LC ω-3 PUFA enhance cognitive performance in healthy schoolaged children and throughout adulthood? Evidence from clinical trials. Nutrients 2014, 6, 2730–2758. [Google Scholar] [CrossRef] [PubMed]
- Kristensen, N.B.; Madsen, M.L.; Hansen, T.H.; Allin, K.H.; Hoppe, C.; Fagt, S.; Lausten, M.S.; Gøbel, R.J.; Vestergaard, H.; Hansen, T.; et al. Intake of macro- and micronutrients in Danish vegans. Nutr. J. 2015, 14, 115. [Google Scholar] [CrossRef] [PubMed]
- Lozoff, B.; Georgieff, M.K. Iron deficiency and brain development. Semin. Pediatr. Neurol. 2006, 13, 158–165. [Google Scholar] [CrossRef] [PubMed]
- Algarín, C.; Nelson, C.A.; Peirano, P.; Westerlund, A.; Reyes, S.; Lozoff, B. Iron-deficiency anemia in infancy and poorer cognitive inhibitory control at age 10 years. Dev. Med. Child. Neurol. 2013, 55, 453–458. [Google Scholar] [CrossRef]
- Logan, S.; Martin, S.; Gilbert, R. Iron therapy for improving psychomotor development and cognitive function in children under the age of three with iron deficiency anaemia. Cochrane Database Syst. Rev. 2001. [Google Scholar] [CrossRef]
- Beard, J. Recent evidence from human and animal studies regarding iron status and infant development. J. Nutr. 2007, 134, 524S–530S. [Google Scholar] [CrossRef]
- Black, M.M. Effects of vitamin B12 and folate deficiency on brain development in children. Food Nutr. Bull. 2008, 29, S126–S131. [Google Scholar] [CrossRef]
- Al, M.D.; van Houwelingen, A.C.; Kester, A.D.; Hasaart, T.H.; de Jong, A.E.; Hornstra, G. Maternal essential fatty acid patterns during normal pregnancy and their relationship to the neonatal essential fatty acid status. Br. J. Nutr. 1995, 74, 55–68. [Google Scholar] [CrossRef]
- Ward, E. Addressing nutritional gaps with multivitamin and mineral supplements. Nutr. J. 2014, 13, 72–81. [Google Scholar] [CrossRef]
- SIPPS; FIMP; SIMA. Consensus VIS—Vitamine Integratori Supplementi. Riv. Ital. Pediatr. Prev. Soc. 2017, 12 (Suppl. 3), 195–360. [Google Scholar]
- Fernandez-Lazaro, C.I.; García-González, J.M.; Adams, D.P.; Fernandez-Lazaro, D.; Mielgo-Ayuso, J.; Caballero-Garcia, A.; Moreno Racionero, F.; Córdova, A.; Miron-Canelo, J.A. Adherence to treatment and related factors among patients with chronic conditions in primary care: A cross-sectional study. BMC Fam. Pract. 2019, 20, 132. [Google Scholar] [CrossRef]
- Jüngst, C.; Gräber, S.; Simons, S.; Wedemeyer, H.; Lammert, F. Medication adherence among patients with chronic diseases: A survey-based study in pharmacies. QJM 2019, 112, 505–512. [Google Scholar] [CrossRef]
- Fewtrell, M.; Bronsky, J.; Campoy, C.; Domellöf, M.; Embleton, N.; Mis, N.F.; Hojsak, I.; Hulst, J.M.; Indrio, F.; Lapillonne, A.; et al. Complementary Feeding: A Position Paper by the European Society for Paediatric Gastroenterology, Hepatology, and Nutrition (ESPGHAN) Committee on Nutrition. J. Pediatr. Gastroenterol. Nutr. 2017, 64, 119–132. [Google Scholar] [CrossRef]
- Agnoli, C.; Baroni, L.; Bertini, I.; Ciappellano, S.; Fabbri, A.; Papa, M.; Pellegrini, N.; Sbarbati, R.; Scarino, M.; Siani, V.; et al. Position paper on vegetarian diets from the working group of the Italian Society of Human Nutrition. Nutr. Metab. Cardiovasc. Dis. 2017, 27, 1037–1052. [Google Scholar] [CrossRef]
- U.S. Department of Agriculture and U.S. Department of Health and Human Services. Dietary Guidelines for Americans, 2020–2025, 9th ed.December 2020. Available online: https://www.dietaryguidelines.gov/ (accessed on 30 July 2022).
- Dietary Guidelines Advisory Committee. Scientific Report of the 2020 Dietary Guidelines Advisory Committee: Advisory Report to the Secretary of Agriculture and Secretary of Health and Human Services; U.S. Department of Agriculture, Agricultural Research Service: Washington, DC, USA, 2020. [CrossRef]
- Redecilla Ferreiro, S.; Moráis López, A.; Moreno Villares, J.M.; Leis Trabazo, R.; José Díaz, J.; Sáenz de Pipaón, M.; Blesa, L.; Campoy, C.; Ángel Sanjosé, M.; Gil Campos, M.; et al. Position paper on vegetarian diets in infants and children. Committee on Nutrition and Breastfeeding of the Spanish Paediatric Association. An. Pediatr. 2020, 92, e1–e306. [Google Scholar] [CrossRef]
- Lemale, J.; Mas, E.; Jung, C.; Bellaiche, M.; Tounian, P. Vegan diet in children and adolescents. Recommendations from the French-speaking Pediatric Hepatology, Gastroenterology and Nutrition Group (GFHGNP). Archives de Pédiatrie 2019, 26, 442–450. [Google Scholar] [CrossRef]
- Sievers, E.; Dörner, K.; Hamm, E.; Janisch, C.; Schaub, J. Vergleichende Untersuchungen zur Eisenversorgunglakto-ovo-vegetabil ernährter Säuglinge. Ärztez Naturheilverfahr. 1991, 2, 106–108. [Google Scholar]

{kind=link}
{kind=link}
{kind=link}
| Diet Definition | Food Not Allowed | Food Allowed |
|---|---|---|
| Pescatarian/pescotarian | Meat (terrestrial animals, birds) | Fish, mollusks, crustaceans, seafood. Any plant-based food: cereals, legumes, vegetables, fruit, algae. Eggs, milk, dairy products, honey, royal jelly §, propolis §, mushrooms, yeasts, lactic ferments and brewer’s yeast |
| Lacto-ovo vegetarian | Meat, fish, mollusks | Any plant-based food: cereals, legumes, vegetables, fruit, algae. Eggs, milk, dairy products, honey, royal jelly §, propolis §. Mushrooms, yeasts, lactic ferments and brewer’s yeast |
| Lacto-vegetarian | Meat, fish, mollusks, crustaceans, milk and dairy products | Any plant-based food: cereals, legumes, vegetables, fruit, algae. Milk, dairy products, honey, royal jelly §, propolis §. Mushrooms, yeasts, lactic ferments and brewer’s yeast |
| Ovo-vegetarian | Meat, fish, mollusks, crustaceans, milk and dairy products | Any plant-based food: cereals, legumes, vegetables, fruit, algae. Eggs, honey, royal jelly §, propolis §. Mushrooms, yeasts, lactic ferments and brewer’s yeast |
| Vegan | All foods of animal origin, including: eggs, honey, milk and dairy products, propolis, royal jelly | Any plant-based food: cereals, legumes, vegetables, fruit, algae. Mushrooms, yeasts. |
| Raw vegan (vegetarian variant) | All foods heated above 46 °C | Only vegetable foods not heated above 42 °C. Dried vegetable foods allowed. Fruits, vegetables, nuts, seeds, cereals, sprouted legumes. |
| Fruitarian | All foods of animal origin including milk and dairy products, eggs; legumes, cereals, vegetables, algae, mushrooms. Fruits and vegetables deriving from roots, flowers and leave and they are not the real fruit of the plant (strawberries, figs…) | Fresh or dry fruits (apple, pear, apricot, peach…), fruit vegetables (tomatoes, peppers, cucumbers…), high-fat fruits (olives, avocados). |
| Windfall vegan (vegetarian variant) | All foods that do not fall spontaneously from trees | Seeds or fruits that have fallen naturally from the trees/plants |
| [Complementary Feeding Completely or Partially Free of Animal-Source Foods] Compared to [Balanced Omnivorous Diet] for [Different Auxological Development and/or Growth] | |||||
|---|---|---|---|---|---|
| Patient or population: [different auxological development and/or growth] Setting: Primary care Intervention: [complementary feeding completely or partially free of animal-source foods] Comparison: [balanced omnivorous diet] | |||||
| Outcomes | № of participants (studies) Follow-up | Certainty of the evidence (GRADE) | Relative effect (95% CI) | Anticipated absolute effects | |
| Risk with [balanced omnivorous diet] | * Risk difference with [complementary feeding completely or partially free of animal-source foods] | ||||
| Risk of wasted grow thassessed with: % infant with major skin and muscle wasting follow-up: 2 years | 106 (1 observational study) [42] | ⨁⨁⨁◯ Moderate a,b,c | RR 17.45 (2.39 to 127.38) | 18 per 1000 | 289 more per 1000 (24 more to 2217 more) |
| Risk of stunted or wasted growth assessed with: % children with stunted growth | 430 (1 observational study) [43] | ⨁⨁⨁◯ Moderate c,d | OR 13.97 (1.86 to 104.88) | 6 per 1000 | 73 more per 1000 (5 more to 385 more) |
| [Complementary Feeding Completely or Partially Free of Animal-Source Foods] Compared to [Balanced Omnivorous Diet] for [Psychomotor Development That Is Significantly Different] | |||||
|---|---|---|---|---|---|
| Patient or population: [psychomotor development that is significantly different] Setting: Primary care Intervention: [complementary feeding completely or partially free of animal-source foods] Comparison: [balanced omnivorous diet] | |||||
| Outcomes | № of participants (studies) Follow-up | Certainty of the evidence (GRADE) | Relative effect (95% CI) | Anticipated absolute effects | |
| Risk with [balanced omnivorous diet] | * Risk difference with [complementary feeding completely or partially free of animal-source foods] | ||||
| Psychomotor development assessed with: standardized psychomotor checklist (score) | 106 (1 observational study) [42] | ⨁⨁◯◯ Low a,b | - | The mean psychomotor development was 0 | −0.63 0 (0 to 0) |
| Psychomotor development assessed with: case report e case series | (7 observational studies) [43] | ⨁⨁⨁◯ Moderate c | 10 cases of children aged 8–18 months: all of them exhibit severe neurological outcomes and growth deficits resulting from low vitamin B12 and vitamin D levels, with anemia, stunting, brain abnormalities, and demyelination. Cases with persistent outcomes are reported with no long-term follow-up data for any other disorders. | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Simeone, G.; Bergamini, M.; Verga, M.C.; Cuomo, B.; D’Antonio, G.; Iacono, I.D.; Mauro, D.D.; Mauro, F.D.; Mauro, G.D.; Leonardi, L.; et al. Do Vegetarian Diets Provide Adequate Nutrient Intake during Complementary Feeding? A Systematic Review. Nutrients 2022, 14, 3591. https://doi.org/10.3390/nu14173591
Simeone G, Bergamini M, Verga MC, Cuomo B, D’Antonio G, Iacono ID, Mauro DD, Mauro FD, Mauro GD, Leonardi L, et al. Do Vegetarian Diets Provide Adequate Nutrient Intake during Complementary Feeding? A Systematic Review. Nutrients. 2022; 14(17):3591. https://doi.org/10.3390/nu14173591
Chicago/Turabian StyleSimeone, Giovanni, Marcello Bergamini, Maria Carmen Verga, Barbara Cuomo, Giuseppe D’Antonio, Iride Dello Iacono, Dora Di Mauro, Francesco Di Mauro, Giuseppe Di Mauro, Lucia Leonardi, and et al. 2022. "Do Vegetarian Diets Provide Adequate Nutrient Intake during Complementary Feeding? A Systematic Review" Nutrients 14, no. 17: 3591. https://doi.org/10.3390/nu14173591
APA StyleSimeone, G., Bergamini, M., Verga, M. C., Cuomo, B., D’Antonio, G., Iacono, I. D., Mauro, D. D., Mauro, F. D., Mauro, G. D., Leonardi, L., Miniello, V. L., Palma, F., Scotese, I., Tezza, G., Vania, A., & Caroli, M. (2022). Do Vegetarian Diets Provide Adequate Nutrient Intake during Complementary Feeding? A Systematic Review. Nutrients, 14(17), 3591. https://doi.org/10.3390/nu14173591