
Adjustments in Food Choices and Physical Activity during Lockdown by Flemish Adults

Abstract
:1. Introduction
2. Materials and Methods
3. Results
3.1. Study Demographics
3.2. Overall Adjustments in Nutritional and PA Parameters during Lockdown
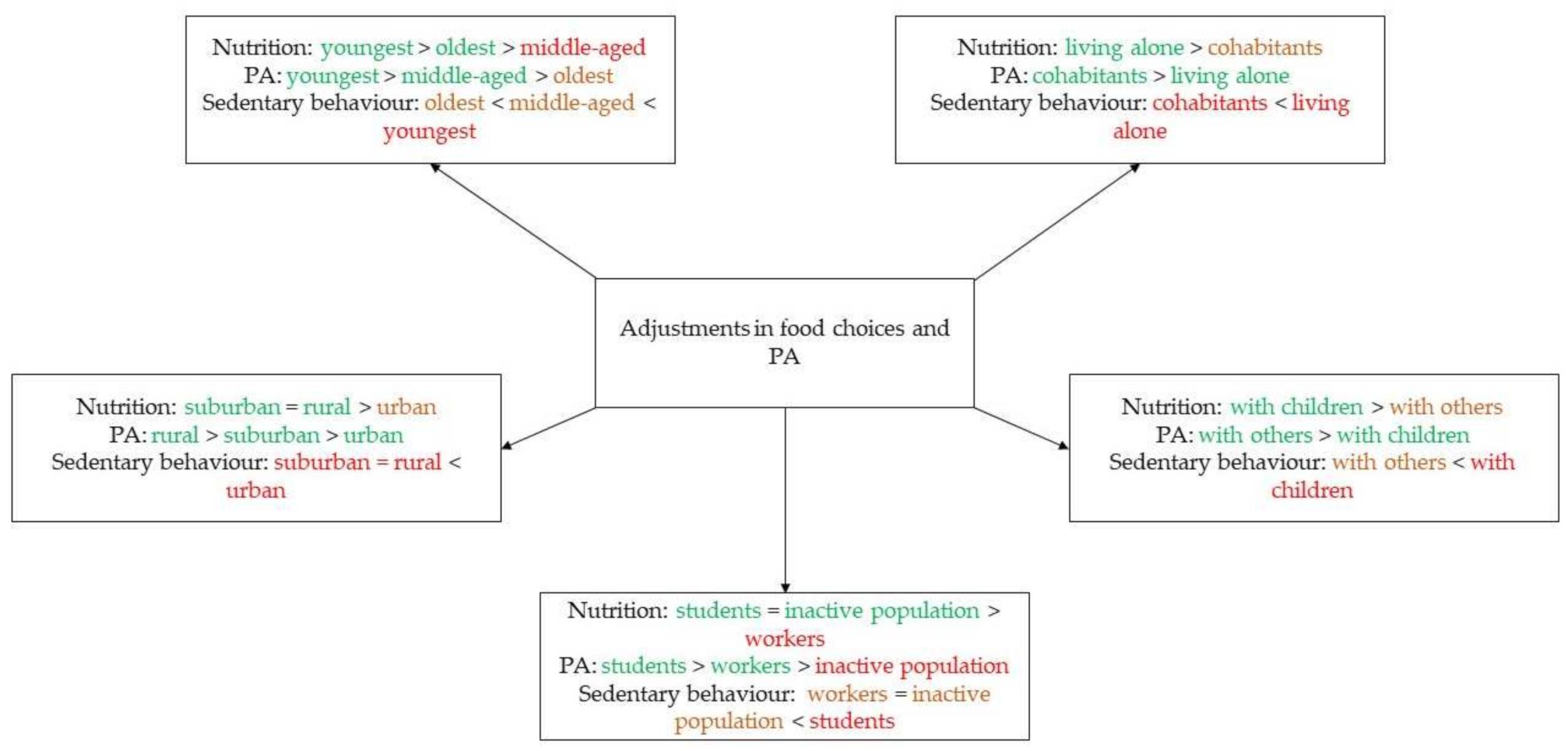
3.3. Changes in Nutritional and PA Parameters According to Age (18–34 Year Old versus 35–50 Year Old versus 51–81 Year old) and Gender
3.4. Changes in Nutritional and PA Parameters according to Area of Residence (Urban Area versus Suburban Area versus Countryside)
3.5. Changes in Nutritional and PA Parameters according to Home Situation (Living Alone versus Cohabiting)
3.6. Changes in Nutritional and PA Parameters According to Family Situation (Living with Others versus Living with Children)
3.7. Changes in Nutritional and PA Parameters according to Professional Situation (Students versus the Inactive Population versus the Employed)
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Wang, C.; Horby, P.W.; Haydetn, F.G.; Galo, G.F. A novel coronavirus outbreak of global health concern. Lancet 2020, 395, 470–473. [Google Scholar] [CrossRef] [Green Version]
- Li, Q.; Guan, X.H.; Wu, P.; Wang, X.Y.; Zhou, L.; Tong, Y.Q.; Ren, R.Q.; Leung, K.S.M.; Lau, E.H.Y. Early Transmission Dynamics in Wuhan, China, of Novel Coronavirus-Infected Pneumonia. N. Engl. J. Med. 2020, 382, 1199–1207. [Google Scholar] [CrossRef]
- Keane, M.; Neal, T. Consumer panic in the COVID-19 pandemic. J. Econom. 2021, 220, 86–105. [Google Scholar] [CrossRef] [PubMed]
- Dar, K.A.; Iqbal, N.; Mushtaq, A. Intolerance of uncertainty, depression, and anxiety: Examining the indirect and moderating effects of worry. Asian J. Psychiatry 2017, 29, 129–133. [Google Scholar] [CrossRef]
- Ahmed, M.Z.; Ahmed, O.; Aibaoa, Z.; Hanbina, S.; Siyu, L.; Ahmadd, A. Epidemic of COVID-19 in China and associated Psychological Problems. Asian J. Psychiatry 2020, 51, 102092. [Google Scholar] [CrossRef] [PubMed]
- Gibson, E.L. Emotional influences on food choice: Sensory, physiological and psychological pathways. Physiol. Behav. 2006, 89, 53–61. [Google Scholar] [CrossRef] [PubMed]
- Cruwys, T.; Bevelander, K.E.; Hermans, R.C. Social modeling of eating: A review of when and why social influence affects food intake and choice. Appetite 2015, 86, 3–18. [Google Scholar] [CrossRef]
- Leng, G.; Adan, R.A.H.; Belot, M.; Brunstrom, J.; De Graaf, K.; Dickson, S.; Hare, T.; Maier, S.; Menzies, J.; Preißl, H.; et al. The determinants of food choice. Proc. Nutr. Soc. 2017, 76, 316–327. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stults-Kolehmainen, M.A.; Sinha, R. The effects of stress on physical activity and exercise. Sports Med. 2014, 44, 81–121. [Google Scholar] [CrossRef]
- Bamia, C.; Trichopoulos, D.; Ferrari, P.; Overvad, K.; Bjerregaard, L.; Tjonneland, A.; Halkjær, J.; Clavel-Chapelon, F.; Kesse, E.; Boutron-Ruault, M.-C.; et al. Mediterranean diet, lifestyle factors, and 10-year mortality in elderly European men and women: The HALE project. JAMA 2004, 292, 1433–1439. [Google Scholar]
- Bamia, C.; Trichopoulos, D.; Ferrari, P.; Overvad, K.; Bjerregaard, L.; Tjonneland, A.; Halkjær, J.; Clavel-Chapelon, F.; Kesse, E.; Boutron-Ruault, M.-C.; et al. Dietary patterns and survival of older Europeans: The EPIC-Elderly Study (European Prospective Investigation into Cancer and Nutrition). Public Health Nutr. 2007, 10, 590–598. [Google Scholar] [CrossRef] [Green Version]
- Di Renzo, L.; Gualtieri, P.; Pivari, F.; Soldati, L.; Attinà, A.; Cinelli, G.; Leggeri, C.; Caparello, G.; Barrea, L.; Scerbo, F.; et al. Eating habits and lifestyle changes during COVID-19 lockdown: An Italian survey. J. Transl. Med. 2020, 18, 229. [Google Scholar] [CrossRef] [PubMed]
- Cancello, R.; Soranna, D.; Zambra, G.; Zambon, A.; Invitti, C. Determinants of the Lifestyle Changes during COVID-19 Pandemic in the Residents of Northern Italy. Int. J. Environ. Res. Public Health 2020, 17, 6287. [Google Scholar] [CrossRef] [PubMed]
- Rodriíguez-Peérez, C.; Molina-Montets, E.; Verardo, V.; Artacho, R.; García-Villanova, B.; Guerra-Hernández, E.J.; Ruíz-López, M.D. Changes in Dietary Behaviours during the COVID-19 Outbreak Confinement in the Spanish COVIDiet Study. Nutrients 2020, 12, 1730. [Google Scholar] [CrossRef]
- Cheikh Ismail, L.C.; Osaili, T.M.; Mohamad, M.N.; Al Marzouqi, A.; Jarrar, A.H.; Abu Jamous, D.O.; Magriplis, E.; Ali, H.I.; Al Sabbah, H.; Hasan, H.; et al. Eating Habits and Lifestyle during COVID-19 Lockdown in the United Arab Emirates: A Cross-Sectional Study. Nutrients 2020, 12, 3314. [Google Scholar] [CrossRef]
- Cheikh Ismail, L.C.; Osaili, T.M.; Mohamad, M.N.; Al Marzouqi, A.; Jarrar, A.H.; Zampelas, A.; Habib-Mourad, C.; Abu Jamous, D.O.; Ali, H.I.; Al Sabbah, H.; et al. Assessment of eating habits and lifestyle during the coronavirus 2019 pandemic in the Middle East and North Africa region: A cross-sectional study. Br. J. Nutr. 2021, 126, 757–766. [Google Scholar] [CrossRef] [PubMed]
- Kriaucioniene, V.; Bagdonaviciene, L.; Rodríguez-Pérez, C.; Petkeviciene, alJ. Associations between Changes in Health Behaviours and Body Weight during the COVID-19 Quarantine in Lithuania: The Lithuanian COVIDiet Study. Nutrients 2020, 12, 3119. [Google Scholar] [CrossRef]
- Bakaloudi, D.R.; Jeyakumar, D.T.; Jalyawardena, R.; Chourdakis, M. The impact of COVID-19 lockdown on snacking habits, fast-food and alcohol consumption: A systematic review of the evidence. Clin. Nutr. 2021. [Google Scholar] [CrossRef]
- Alhusseini, N.; Alqahtani, A. COVID-19 pandemic’s impact on eating habits in Saudi Arabia. J Public Health Res 2020, 9, 1868. [Google Scholar] [CrossRef]
- Blłaszczyk-Beębenek, E.; Jagietlski, P.; Bolesławska, I.; Jagielska, A.; Nitsch-Osuch, A.; Kawalec, P. Nutrition Behaviors in Polish Adults before and during COVID-19 Lockdown. Nutrients 2020, 12, 3084. [Google Scholar] [CrossRef]
- Zajacova, A.; Jethn, A.; Stackhouse, M.; Denice, P.; Ramos, H. Changes in health behaviours during early COVID-19 and socio-demographic disparities: A cross-sectional analysis. Can. J. Public Health 2020, 111, 953–962. [Google Scholar] [CrossRef] [PubMed]
- Batlle-Bayer, L.; Aldaco, R.; Bala, A.; Puig, R.; Laso, J.; Margallo, M.; Vázquez-Rowe, I.; Antó, J.M.; Fullana-I-Palmer, P. Environmental and nutritional impacts of dietary changes in Spain during the COVID-19 lockdown. Sci. Total Environ. 2020, 748, 141410. [Google Scholar] [CrossRef] [PubMed]
- Goórnicka, M.; Drywietń, M.; Zielinskal, M.; Hamułka, J. Dietary and Lifestyle Changes During COVID-19 and the Subsequent Lockdowns among Polish Adults: A Cross-Sectional Online Survey PLifeCOVID-19 Study. Nutrients 2020, 12, 2324. [Google Scholar] [CrossRef] [PubMed]
- Constant, A.; Consetrve, D.F.; Gallopel-Morvan, K.; Raude, J. Socio-Cognitive Factors Associated With Lifestyle Changes in Response to the COVID-19 Epidemic in the General Population: Results From a Cross-Sectional Study in France. Front. Psychol. 2020, 11, 579460. [Google Scholar] [CrossRef] [PubMed]
- Malta, D.C.; Szwarcwald, C.L.; Barros, M.B.d.A.; Gomes, C.S.; Machado1, Í.E.M.; Júnior, P.R.B.d.S.; Romero, D.E.; Lima, M.G.; Damacena, G.N.; Pina, M.d.F.; et al. The COVID-19 Pandemic and changes in adult Brazilian lifestyles: A cross-sectional study. Epidemiol. Serv. Saude 2020, 29, e2020407. [Google Scholar] [CrossRef]
- Pellegrini, M.; Ponzo, V.; Rosato, R.; Scumaci, E.; Goitre, I.; Benso, A.; Belcastro, S.; Crespi, C.; De Michieli, F.; Ghigo, E.; et al. Changes in Weight and Nutritional Habits in Adults with Obesity during the “Lockdown” Period Caused by the COVID-19 Virus Emergency. Nutrients 2020, 12, 2016. [Google Scholar] [CrossRef] [PubMed]
- Scarmozzino, F.; Visioli, F. Covid-19 and the Subsequent Lockdown Modified Dietary Habits of Almost Half the Population in an Italian Sample. Foods 2020, 9, 675. [Google Scholar] [CrossRef]
- Sidor, A.; Rzymski, P. Dietary Choices and Habits during COVID-19 Lockdown: Experience from Poland. Nutrients 2020, 12, 1657. [Google Scholar] [CrossRef]
- Reyes-Olavarriía, D.; Latorre-Román, P.; Guzmán-Guzmán, I.; Jerez-Mayorga, D.; Caamaño-Navarrete, F.; Delgado-Floody, P. Positive and Negative Changes in Food Habits, Physical Activity Patterns, and Weight Status during COVID-19 Confinement: Associated Factors in the Chilean Population. Int. J. Environ. Res. Public Health 2020, 17, 5431. [Google Scholar] [CrossRef]
- Rolland, B.; Haesebaert, F.; Zante, E.; Benyamina, A.; Haesebaert, J.; Franck, N. Global Changes and Factors of Increase in Caloric/Salty Food Intake, Screen Use, and Substance Use During the Early COVID-19 Containment Phase in the General Population in France: Survey Study. JMIR Public Health Surveill. 2020, 6, e19630. [Google Scholar] [CrossRef]
- Zaccagni, L.; Toselli, S.; Barbieri, D. Physical Activity during COVID-19 Lockdown in Italy: A Systematic Review. Int. J. Environ. Res. Public Health 2021, 18, 6416. [Google Scholar] [CrossRef]
- Galleè, F.; Sabella, E.A.; Da Molin, G.; De Giglio, O.; Caggiano, G.; Di Onofrio, V.; Ferracuti, S.; Montagna, M.T.; Liguori, G.; Orsi, G.B.; et al. Understanding Knowledge and Behaviors Related to CoViD-19 Epidemic in Italian Undergraduate Students: The EPICO Study. Int. J. Environ. Res. Public Health 2020, 17, 3481. [Google Scholar] [CrossRef] [PubMed]
- Galleè, F.; Sabella, E.A.; Ferracuti, S.; De Giglio, O.; Caggiano, G.; Protano, C.; Valeriani, F.; Parisi, E.A.; Valerio, G.; Liguori, G.; et al. Sedentary Behaviors and Physical Activity of Italian Undergraduate Students during Lockdown at the Time of CoViD-19 Pandemic. Int. J. Environ. Res. Public Health 2020, 17, 6171. [Google Scholar] [CrossRef]
- Luciano, F.; Cetnacchi, V.; Vegro, V.; Palvei, G. COVID-19 lockdown: Physical activity, sedentary behaviour and sleep in Italian medicine students. Eur. J. Sport Sci. 2020, 21, 1459–1468. [Google Scholar] [CrossRef]
- Tornaghi, M.; Lovetcchio, N.; Vandoni, M.; Chirico, A.; Codella, R. Physical activity levels across COVID-19 outbreak in youngsters of Northwestern Lombardy. J. Sports Med. Phys. Fit. 2021, 61, 971–976. [Google Scholar]
- Di Corrado, D.; Magnano, P.; Muzii, B.; Coco, M.; Guarnetra, M.; De Lucia, S.; Maldonato, N.M. Effects of social distancing on psychological state and physical activity routines during the COVID-19 pandemic. Sport Sci. Health 2020, 16, 619–624. [Google Scholar] [CrossRef]
- Maugeri, G.; Castrogiovanni, P.; Battaglia, G.; Pippi, R.; D’Agata, V.; Palma, A.; Di Rosa, M.; Musumeci, G. The impact of physical activity on psychological health during Covid-19 pandemic in Italy. Heliyon 2020, 6, e04315. [Google Scholar] [CrossRef] [PubMed]
- Kang, H. Sample size determination and power analysis using the G*Power software. J. Educ. Eval. Health Prof. 2021, 18, 17. [Google Scholar] [CrossRef]
- Epel, E.; Lapidus, R.; McEtwen, aB.; Brownell, K. Stress may add bite to appetite in women: A laboratory study of stress-induced cortisol and eating behavior. Psychoneuroendocrinology 2001, 26, 37–49. [Google Scholar] [CrossRef]
- Zellner, D.A.; Loaiza, S.; Gonzalez, Z.; Pita, J.; Morales, J.; Pecora, D.; Wolf, A. Food selection changes under stress. Physiol. Behav. 2006, 87, 789–793. [Google Scholar] [CrossRef] [PubMed]
- Oliver, G.; Wardle, J.; Gibson, E.L. Stress and food choice: A laboratory study. Psychosom. Med. 2000, 62, 853–865. [Google Scholar] [CrossRef] [PubMed]
- Maier, S.U.; Makwana, A.B.; Hare, T.A. Acute Stress Impairs Self-Control in Goal-Directed Choice by Altering Multiple Functional Connections within the Brain’s Decision Circuits. Neuron 2015, 87, 621–631. [Google Scholar] [CrossRef] [Green Version]
- Wansink, B.; Cheney, M.M.; Chan, N. Exploring comfort food preferences across age and gender. Physiol. Behav. 2003, 79, 739–747. [Google Scholar] [CrossRef]
- Ma, Y.; Ratnasabapathy, R.; Gardiner, J. Carbohydrate craving: Not everything is sweet. Curr. Opin. Clin. Nutr. Metab. Care 2017, 20, 261–265. [Google Scholar] [CrossRef] [PubMed]
- Taylor, S. Understanding and managing pandemic-related panic buying. J. Anxiety Disord. 2021, 78, 102364. [Google Scholar] [CrossRef]
- Buman, M.P.; Tuccitto, D.E.; Giacobbi, P.R. Predicting daily reports of leisure-time exercise from stress appraisals and coping using a multilevel modeling approach. J. Sport Exerc. Psychol. 2007, 29, S150. [Google Scholar]
- Cottini, M.; Lombardi, C.; Berti, A.; Gregis, M.; Gregis, G.; Bello, L.; Mazid, M.; Putignano, T.; Corbellini, A.; Belotti, S.; et al. Obesity is a Major Risk Factor for Hospitalization in Community-Managed COVID-19 Pneumonia. Mayo Clin. Proc. 2021, 96, 921–931. [Google Scholar] [CrossRef]
- May, A.M.; Adema, L.E.; Romaguera, D.; Vergnaud, A.-C.; Agudo, A.; Ekelund, U.; Steffen, A.; Orfanos, P.; Slimani, N.; Rinaldi, S.; et al. Determinants of non-response to a second assessment of lifestyle factors and body weight in the EPIC-PANACEA study. BMC Med. Res. Methodol. 2012, 12, 148. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
| Number of main meals |
| Number of snacks |
| Portion size of the main meals |
| Portion size of the snacks |
| Takeaway/delivery: French fries |
| Takeaway/delivery: pizza |
| Takeaway/delivery: food international |
| Takeaway/delivery: (local) restaurant/brasserie/bistro |
| Takeaway/delivery: meal boxes |
| Fresh fruit |
| Frozen fruit |
| Canned fruit/fruit in a jar |
| Freeze-(dried) fruit |
| Fresh vegetables |
| Frozen vegetables |
| Canned vegetables/vegetables in a jar |
| Fresh potatoes |
| Ready-made potato preparations |
| Fried potato preparations |
| Pasta |
| Rice |
| Couscous, bulgur, quinoa, buckwheat, Ebly, etc. |
| Fresh meat |
| Canned meat/meat in jar |
| Fozen meat |
| Red meat |
| White meat |
| Minced meat (preparations) |
| Processed meat products |
| Fresh fish |
| Canned fish/fish in a jar |
| Frozen fish |
| Smoked fish |
| White fish/lean fish |
| Colored fish/fatty fish |
| Fresh seafood |
| Canned seafood/seafood in a jar |
| Frozen seafood |
| Eggs |
| Dried legumes |
| Canned legumes/legumes in a jar |
| Seitan, tempeh, tofu |
| More processed vegetarian/vegan protein sources such as burgers, sausages, etc. |
| Milk and dairy |
| Plant-based alternatives to milk and dairy products |
| Fresh cheese |
| Slices of cheese |
| Soft cheese |
| Cheese spread |
| Margarine to bake |
| Margarine to spread |
| Oils |
| Ready-made meals from the fresh market and frozen in the supermarket |
| Candy |
| Chocolate |
| Cookies, cake and/or pie |
| Ice cream and/or sorbet |
| Crisps |
| Sweet spreads |
| Savory spreads |
| Sauces |
| Unsalted nuts |
| Salted nuts |
| Beer |
| Wine |
| Liquor |
| Soft drinks |
| Diet soda |
| Water (including sparkling water and flavoured water) |
| Coffee and/of tea |
| Walking |
| Cycling |
| Jogging/running |
| Strength training with own body weight |
| Strength training with external weights and/or machines |
| Sedentary behaviour |
| Sports through (computer) games |
| Mean | SD | Minimum | Maximum | |
|---|---|---|---|---|
| Age (years) | 34.9 | 14.3 | 18.0 | 81.0 |
| n | % | |||
| Men | 253 | 22.4 | ||
| Women | 870 | 77.1 | ||
| X | 6 | 0.5 | ||
| n | % | |||
| Urban | 325 | 28.8 | ||
| Suburban | 452 | 40.0 | ||
| Rural | 352 | 31.2 | ||
| n | % | |||
| Living alone | 163 | 14.4 | ||
| Living together | 966 | 85.6 | ||
| n | % | |||
| Living with others | 613 | 54.3 | ||
| Living with children | 353 | 31.3 | ||
| n | % | |||
| Students | 389 | 34.5 | ||
| Inactive population £ | 118 | 10.4 | ||
| Active population § | 622 | 55.1 | ||
| n | % | |||
| Less time preparing meals | 20 | 1.8 | ||
| Just as much time preparing meals | 362 | 32.1 | ||
| More time preparing meals | 344 | 30.5 |
| Most Stable Parameters—Least Changes in Both Directions £ | Least Stable Parameters—Most Changes in Both Directions § |
|---|---|
| Margarine to bake (84.4%) | Number of snacks (45.5%) |
| Margarine to spread (84.1%) | Takeaway/delivery: (local) restaurant/brasserie/bistro (46.8%) |
| Oils (83.4%) | Chocolate (44.6%) |
| Red meat (83.1%) | Cookies. cake and/or pie (48.0%) |
| Rice (82.3%) | Water (including sparkling water and flavoured water) (49.6%) |
| White meat (81.9%) | Walking (19.7%) |
| Cheese spread (81.2%) | Cycling (41.3%) |
| Number of main meals (81.2%) | Sedentary behaviour (33.0%) |
| Processed meat products (80.3%) | |
| Canned seafood/seafood in a jar (80.3%) |
| Strongest Risers £ | Strongest Fallers § |
|---|---|
| 36.5% cookies, cake and/or pie | 46.0% takeaway/delivery: food international |
| 37.1% coffee and/or tea | 44.4% takeaway/delivery: French fries |
| 37.9% cycling | 43.4% takeaway/delivery: (local) restaurant/brasserie/bistro |
| 39.2% fresh vegetables | 42.8% takeaway/delivery: pizza |
| 40.3% eggs | |
| 40.3% chocolate | |
| 42.4% fresh fruit | |
| 44.8% water (including sparkling water and flavoured water) | |
| 55.3% sedentary behaviour | |
| 62.7% walking |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mertens, E.; Deriemaeker, P.; Van Beneden, K. Adjustments in Food Choices and Physical Activity during Lockdown by Flemish Adults. Nutrients 2021, 13, 3794. https://doi.org/10.3390/nu13113794
Mertens E, Deriemaeker P, Van Beneden K. Adjustments in Food Choices and Physical Activity during Lockdown by Flemish Adults. Nutrients. 2021; 13(11):3794. https://doi.org/10.3390/nu13113794
Chicago/Turabian StyleMertens, Evelien, Peter Deriemaeker, and Katrien Van Beneden. 2021. "Adjustments in Food Choices and Physical Activity during Lockdown by Flemish Adults" Nutrients 13, no. 11: 3794. https://doi.org/10.3390/nu13113794
APA StyleMertens, E., Deriemaeker, P., & Van Beneden, K. (2021). Adjustments in Food Choices and Physical Activity during Lockdown by Flemish Adults. Nutrients, 13(11), 3794. https://doi.org/10.3390/nu13113794