
Association of Lifestyle Changes Due to the COVID-19 Pandemic with Nutrient Intake and Physical Activity Levels during Pregnancy in Japan



Abstract
:1. Introduction
2. Materials and Methods
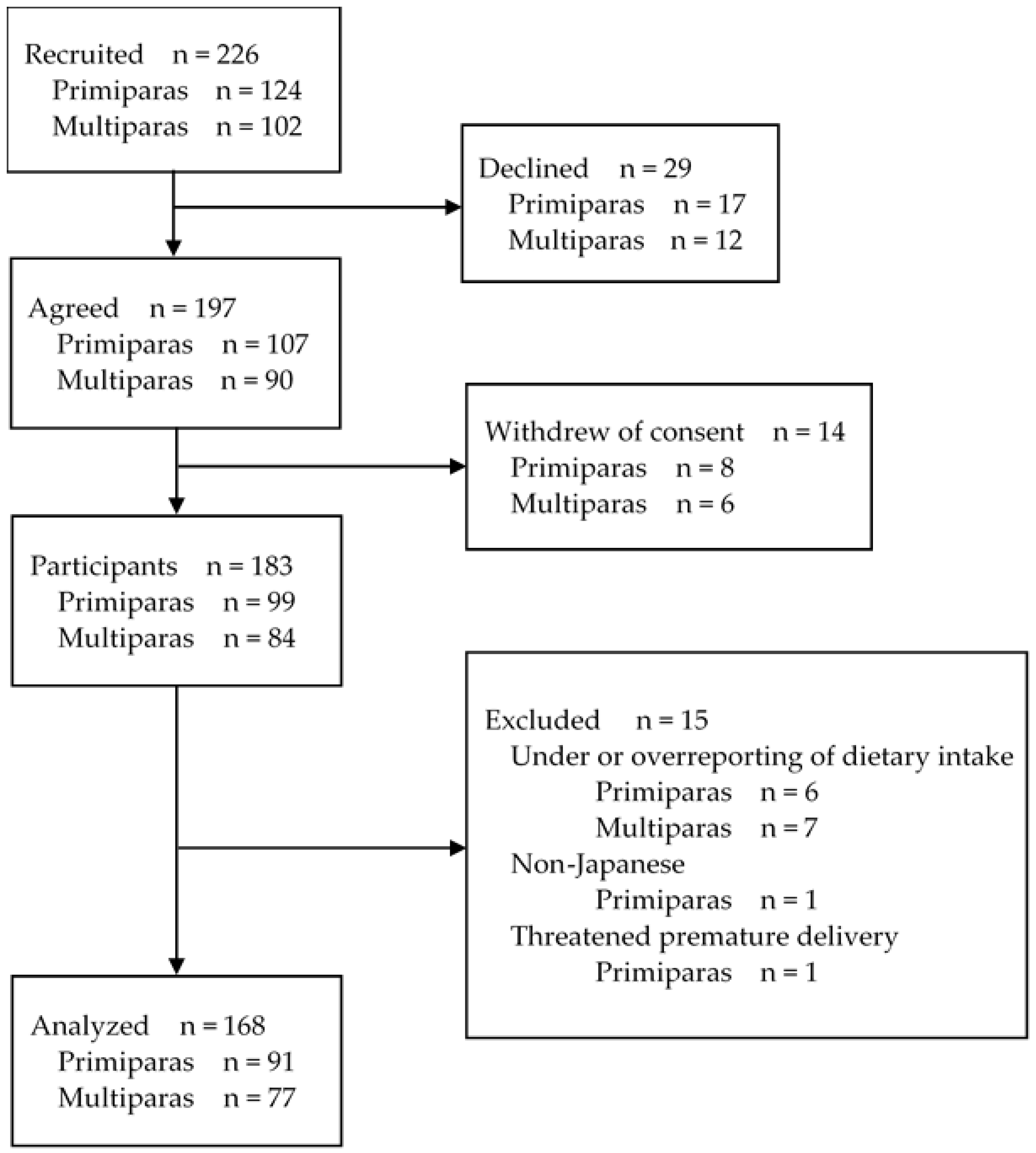
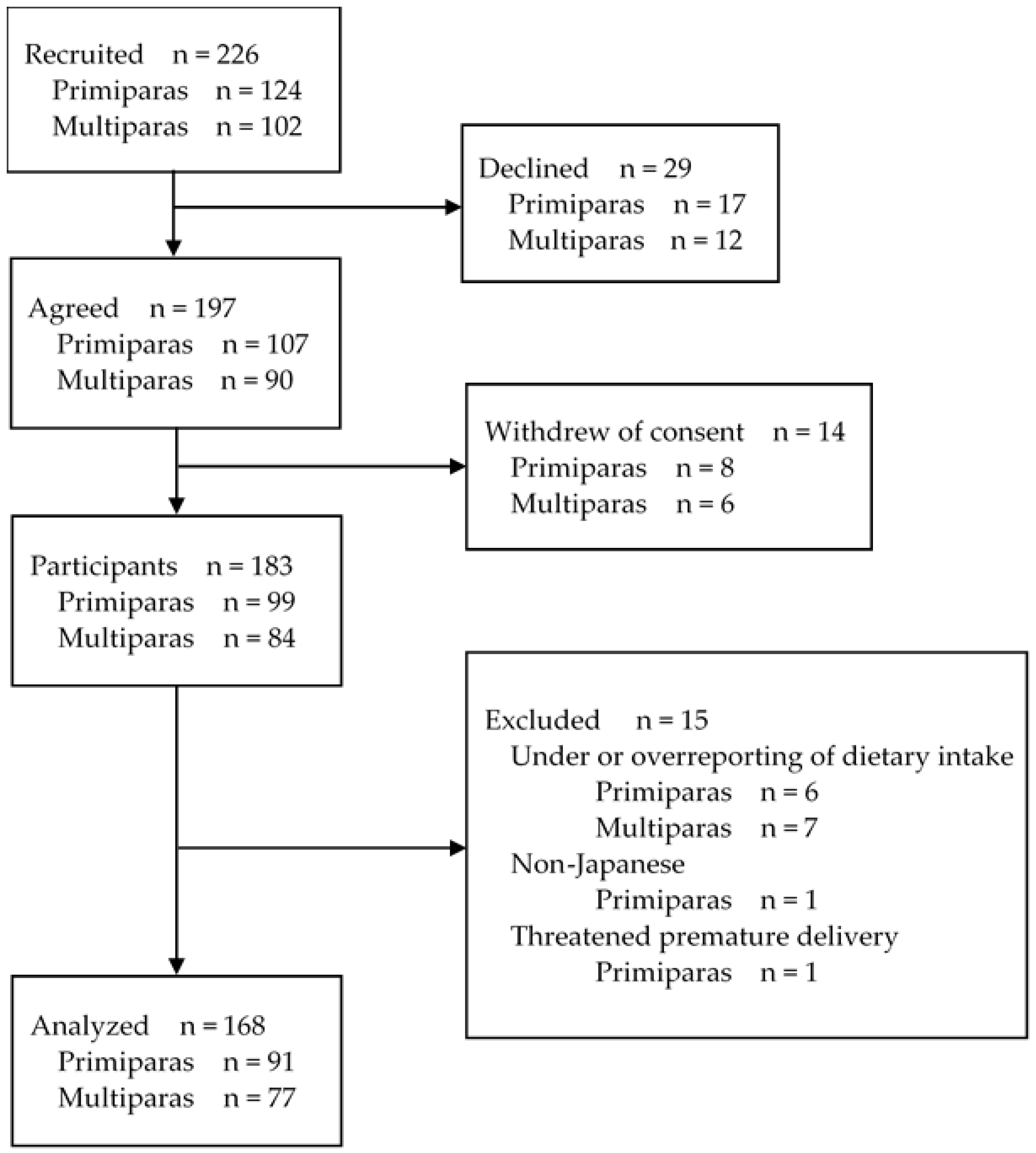
2.1. Overview of the Recruitment Process and Study Design
2.2. Variables and Their Measurement
2.2.1. Demographic Variables
2.2.2. Lifestyle Changes Due to the COVID-19 Pandemic
2.2.3. Nutrient Intake
2.2.4. Physical Activity
2.2.5. Psychosocial Variables
2.3. Statistical Analyses
3. Results
4. Discussion
4.1. Association of Lifestyle Changes Due to the COVID-19 Pandemic with Nutrient Intake
4.2. Association of Lifestyle Changes Due to the COVID-19 Pandemic with Physical Activity Levels
4.3. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Velavan, T.P.; Meyer, C.G. The COVID-19 epidemic. Trop. Med. Int. Health 2020, 25, 278–280. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Whitaker, K.M.; Hung, P.; Alberg, A.J.; Hair, N.L.; Liu, J. Variations in health behaviors among pregnant women during the COVID-19 pandemic. Midwifery 2021, 95, 102929. [Google Scholar] [CrossRef]
- Kumari, A.; Ranjan, P.; Sharma, K.A.; Sahu, A.; Bharti, J.; Zangmo, R.; Bhatla, N. Impact of COVID-19 on psychosocial function-ing of peripartum women: A qualitative study comprising focus group discussions and in-depth interviews. Int. J. Gynaecol. Obstet. 2020, 152, 321–327. [Google Scholar] [CrossRef] [PubMed]
- Biviá-Roig, G.; La Rosa, V.L.; Gómez-Tébar, M.; Serrano-Raya, L.; Amer-Cuenca, J.J.; Caruso, S.; Commodari, E.; Barrasa-Shaw, A.; Lisón, J.F. Analysis of the Impact of the Con-finement Resulting from COVID-19 on the Lifestyle and Psychological Wellbeing of Spanish Pregnant Women: An Inter-net-Based Cross-Sectional Survey. Int. J. Environ. Res. Public Health 2020, 17, 5933. [Google Scholar] [CrossRef] [PubMed]
- Sato, K.; Kobayashi, S.; Yamaguchi, M.; Sakata, R.; Sasaki, Y.; Murayama, C.; Kondo, N. Working from home and dietary changes during the COVID-19 pandemic: A longitudinal study of health app (CALO mama) users. Appetite 2021, 165, 105323. [Google Scholar] [CrossRef] [PubMed]
- Suka, M.; Yamauchi, T.; Yanagisawa, H. Changes in health status, workload, and lifestyle after starting the COVID-19 pan-demic: A web-based survey of Japanese men and women. Environ. Health Prev. Med. 2021, 26, 37. [Google Scholar] [CrossRef]
- World Health Organization. Obesity: Preventing and managing the global epidemic. Report of a WHO consultation. World Health Organ. Tech. Rep. Ser. 2000, 894, 1–253. [Google Scholar]
- Sasaki, S.; Yanagibori, R.; Amano, K. Self-Administered Diet History Questionnaire Developed for Health Education: A Relative Validation of The Test-Version by Comparison with 3-Day Diet Record in Women. J. Epidemiol. 1998, 8, 203–215. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sasaki, S.; Yanagibori, R.; Amano, K. Validity of a self-administered diet history questionnaire for assessment of sodium and potassium: Comparison with single 24-h urinary excretion. Jpn. Circ. J 1998, 62, 431–435. [Google Scholar] [CrossRef] [Green Version]
- Sasaki, S.; Ushio, F.; Amano, K.; Morihara, M.; Todoriki, T.; Uehara, Y.; Toyooka, T. Serum Biomarker-based Validation of a Self-administered Diet History Questionnaire for Japanese Subjects. J. Nutr. Sci. Vitaminol. 2000, 46, 285–296. [Google Scholar] [CrossRef]
- Kobayashi, S.; Honda, S.; Murakami, K.; Sasaki, S.; Okubo, H.; Hirota, N.; Notsu, A.; Fukui, M.; Date, C. Both Comprehensive and Brief Self-Administered Diet History Questionnaires Satisfactorily Rank Nutrient Intakes in Japanese Adults. J. Epidemiol. 2012, 22, 151–159. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shiraishi, M.; Haruna, M.; Matsuzaki, M.; Murayama, R.; Sasaki, S.; Murashima, S. Validity and reproducibility of folate and vitamin B12 intakes estimated from a self-administered diet history questionnaire in Japanese pregnant women. Nutr. J. 2012, 11, 15. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shiraishi, M.; Haruna, M.; Matsuzaki, M.; Murayama, R.; Sasaki, S. Validity of a diet history questionnaire estimating β-carotene, vitamin C and α-tocopherol intakes in Japanese pregnant women. Int. J. Food Sci. Nutr. 2013, 64, 694–699. [Google Scholar] [CrossRef] [PubMed]
- Shiraishi, M.; Haruna, M.; Matsuzaki, M.; Murayama, R.; Kitanaka, S.; Sasaki, S. Validity of a self-administered diet history questionnaire for estimating vitamin D intakes of Japanese pregnant women. Matern. Child Nutr. 2015, 11, 525–536. [Google Scholar] [CrossRef]
- Shiraishi, M.; Haruna, M.; Matsuzaki, M.; Murayama, R.; Yatsuki, Y.; Sasaki, S. Estimation of eicosapentaenoic acid and do-cosahexaenoic acid intakes in pregnant Japanese women without nausea by using a self-administered diet history question-naire. Nutr. Res. 2013, 33, 473–478. [Google Scholar] [CrossRef] [PubMed]
- Shiraishi, M.; Haruna, M.; Matsuzaki, M.; Murayama, R.; Sasaki, S. Availability of two self-administered diet history ques-tionnaires for pregnant Japanese women: A validation study using 24-hour urinary markers. J. Epidemiol. 2017, 27, 172–179. [Google Scholar] [CrossRef]
- Willett, W.C.; Howe, G.R.; Kushi, L. Adjustment for total energy intake in epidemiologic studies. Am. J. Clin. Nutr. 1997, 65, 1220S–1228S. [Google Scholar] [CrossRef] [PubMed]
- Matsuzaki, M.; Haruna, M.; Ota, E.; Yeo, S.; Murayama, R.; Murashima, S. Translation and cross-cultural adaptation of the Pregnancy Physical Activity Questionnaire (PPAQ) to Japanese. Biosci. Trends 2010, 4, 170–177. [Google Scholar] [PubMed]
- Chasan-Taber, L.; Schmidt, M.; Roberts, D.E.; Hosmer, D.; Markenson, G.; Freedson, P.S. Development and Validation of a Pregnancy Physical Activity Questionnaire. Med. Sci. Sports Exerc. 2004, 36, 1750–1760. [Google Scholar] [CrossRef]
- Ainsworth, B.E.; Haskell, W.L.; Herrmann, S.D.; Meckes, N.; Bassett, D.R., Jr.; Tudor-Locke, C.; Greer, J.L.; Vezina, J.; Whitt-Glover, M.C.; Leon, A.S. Compendium of physical activities: A second update of codes and MET values. Med. Sci. Sports Exerc. 2011, 43, 1575–1581. [Google Scholar] [CrossRef] [Green Version]
- Souma, M. The relation between maternal-fetal attachment and behavior in daily life of primigravid women. J. Jpn. Acad. Midwif. 2011, 25, 203–214. [Google Scholar] [CrossRef]
- Muller, M.E.; Mercer, R.T. Development of the Prenatal Attachment Inventory. West. J. Nurs. Res. 1993, 15, 199–215. [Google Scholar] [CrossRef] [PubMed]
- Tsujino, J.; Oyama, M.; Inuihara, T.; Kohmura, H. The relationship of maternal attachment towards children before and after their birth and the factors that influence maternal attachment: An analysis using the knowledge discovery method. J. Educ. Psychol. 2000, 26, 35–40. [Google Scholar]
- Shiraishi, M.; Haruna, M.; Matsuzaki, M.; Murayama, R.; Sasaki, S. Pre-pregnancy BMI, gestational weight gain and body image are associated with dietary under-reporting in pregnant Japanese women. J. Nutr. Sci. 2018, 7, e12. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kikuchi-Noguchi, H.; Shiraishi, M.; Matsuzaki, M.; Haruna, M. Physical activity levels in the second trimester of pregnancy and related demographic factors: A cross-sectional secondary data analysis. Cogent Med. 2019, 6, 6. [Google Scholar] [CrossRef]
- Nishijima, C.; Miyagawa, N.; Tsuboyama-Kasaoka, N.; Chiba, T.; Miyachi, M. Association between Lifestyle Changes and at-Home Hours during and after the State of Emergency Due to the COVID-19 Pandemic in Japan. Nutrients 2021, 13, 2698. [Google Scholar] [CrossRef]
- Ministry of Agriculture, Forestry and Fisheries. Promotion of Shokuiku (Food and Nutrition Education). Available online: https://www.maff.go.jp/j/press/syouan/hyoji/210331.html (accessed on 18 June 2021).
- Matsumoto, M.; Saito, A.; Okada, C.; Okada, E.; Tajima, R.; Takimoto, H. Consumption of meals prepared away from home is associated with inadequacy of dietary fiber, vitamin C and mineral intake among Japanese adults: Analysis from the 2015 National Health and Nutrition Survey. Nutr. J. 2021, 20, 1–13. [Google Scholar] [CrossRef]
- Yamada, S.; Inui, T.; Igarashi, T. The process of changing the dietary habits of primiparas through a midwife-led birth system in a hospital. Bull. Fac. Nurs. Sch. Med. Nara Med. Univ. 2017, 13, 17–26. [Google Scholar]
- Abu-Saad, K.; Fraser, D. Maternal Nutrition and Birth Outcomes. Epidemiol. Rev. 2010, 32, 5–25. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mousa, A.; Naqash, A.; Lim, S. Macronutrient and Micronutrient Intake during Pregnancy: An Overview of Recent Evi-dence. Nutrients 2019, 11, 443. [Google Scholar] [CrossRef] [Green Version]
- Takimoto, H.; Yoshiike, N.; Katagiri, A.; Ishida, H.; Abe, S. Nutritional status of pregnant and lactating women in Japan: A comparison with non-pregnant/non-lactating controls in the National Nutrition Survey. J. Obstet. Gynaecol. Res. 2003, 29, 96–103. [Google Scholar] [CrossRef] [PubMed]
- Shimokihara, S.; Maruta, M.; Hidaka, Y.; Akasaki, Y.; Tokuda, K.; Han, G.; Ikeda, Y.; Tabira, T. Relationship of Decrease in Frequency of Socialization to Daily Life, Social Life, and Physical Function in Community-Dwelling Adults Aged 60 and Over after the COVID-19 Pandemic. Int. J. Environ. Res. Public Health 2021, 18, 2573. [Google Scholar] [CrossRef] [PubMed]
- Shamim, K.; Ahmad, S.; Alam, A. COVID-19 health safety practices: Influence on grocery shopping behavior. J. Public Aff. 2021, e2624. [Google Scholar] [CrossRef]
- Schmidt, S.; Benke, C.; Pané-Farré, C.A. Purchasing under threat: Changes in shopping patterns during the COVID-19 pan-demic. PLoS ONE 2021, 16, e0253231. [Google Scholar] [CrossRef] [PubMed]
- Xu, Q.; Tao, Y.; Zhang, Y.; Zhang, X.; Xue, C.; Liu, Y. Dietary fiber intake, dietary glycemic load, and the risk of gestational diabetes mellitus during the second trimester: A nested case-control study. Asia Pac. J. Clin. Nutr. 2021, 30, 477–486. [Google Scholar] [PubMed]
- Strobel, M.; Tinz, J.; Biesalski, H.K. The importance of beta-carotene as a source of vitamin A with special regard to pregnant and breastfeeding women. Eur. J. Nutr. 2007, 46, 1–20. [Google Scholar] [CrossRef]
- Azuma, K.; Nojiri, T.; Kawashima, M.; Hanai, A.; Ayaki, M.; Tsubota, K.; on behalf of the TRF-Japan Study Group. Possible favorable lifestyle changes owing to the coronavirus disease 2019 (COVID-19) pandemic among middle-aged Japanese women: An ancillary survey of the TRF-Japan study using the original “Taberhythm” smartphone app. PLoS ONE 2021, 16, e0248935. [Google Scholar] [CrossRef] [PubMed]
- Haruna, M.; Yeo, S.; Watanabe, E.; Matsuzaki, M.; Ota, E.; Nakayama, K.; Murashima, S. Perceptions of women and health-care providers in Tokyo of appropriate weight gain during pregnancy. Nurs. Health Sci. 2010, 12, 21–26. [Google Scholar] [CrossRef] [PubMed]
- Ministry of Health, Labour and Welfare. Summary of Annual Vital Statistics Monthly Report (Approximate) for 2019 Annual Change in the Number of Births. Available online: https://www.mhlw.go.jp/toukei/saikin/hw/jinkou/geppo/nengai19/dl/h3-4.pdf (accessed on 2 October 2021).
- Ministry of Health, Labour and Welfare. Summary of “Statistics on Changes in Employment before and after Birth” (Special Report on Vital Statistics 2003). Available online: https://www.mhlw.go.jp/toukei/saikin/hw/jinkou/tokusyu/04/3.html#3-3 (accessed on 2 October 2021).
- Statistics Bureau of Japan. 2020 Population Census—Summary of the Results and Statistical Tables. Available online: https://www.e-stat.go.jp/en/stat-search/files?page=1&layout=datalist&toukei=00200521&tstat=000001136464&cycle=0&year=20200&month=24101210&tclass1=000001136465&tclass2=000001154388 (accessed on 20 July 2021).

{kind=link}
| All Participants (n = 91) | Lifestyle Changes Due to the COVID-19 Pandemic | p | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Lifestyle-Affected (n = 14) | Unaffected (n = 77) | |||||||||
| Mean ± SD or n (%) | Range | Mean ± SD or n (%) | Range | Mean ± SD or n (%) | Range | |||||
| Age [year] | 30.9 | ±6.1 | 20–45 | 34.4 | ±5.7 | 26–44 | 30.2 | ±6.0 | 20–45 | 0.018 |
| Gestational period [n (%)] | ||||||||||
| Second trimester | 46 | (50.5) | 7 | (50.0) | 39 | (50.6) | 1.000 * | |||
| Third trimester | 45 | (49.5) | 7 | (50.0) | 38 | (49.4) | ||||
| Working status [n (%)] | ||||||||||
| Working or Student | 39 | (42.9) | 6 | (42.9) | 33 | (42.9) | 1.000 * | |||
| Housewife | 52 | (57.1) | 8 | (57.1) | 44 | (57.1) | ||||
| Education level [n (%)] | ||||||||||
| University or above | 22 | (24.2) | 3 | (21.4) | 19 | (24.7) | 0.023 * | |||
| Junior or technical college | 31 | (34.1) | 9 | (64.3) | 22 | (28.6) | ||||
| High school/Junior high school | 38 | (41.8) | 2 | (14.3) | 36 | (46.8) | ||||
| Annual income [n (%)] | ||||||||||
| ≥9 million yen | 7 | (7.7) | 2 | (14.3) | 5 | (6.5) | 0.485 * | |||
| 5–9 million yen | 30 | (33.0) | 4 | (28.6) | 26 | (33.8) | ||||
| 0–5 million yen | 54 | (59.3) | 8 | (57.1) | 46 | (59.7) | ||||
| Prepregnancy BMI [n (%)] | ||||||||||
| Underweight (BMI < 18.5 kg/m2) | 13 | (14.3) | 0 | (0.0) | 13 | (16.9) | 0.247 † | |||
| Normal weight (18.5–24.9 kg/m2) | 68 | (74.7) | 12 | (85.7) | 56 | (89.6) | ||||
| Overweight or obese (BMI > 24.9 kg/m2) | 10 | (11.0) | 2 | (14.3) | 8 | (10.4) | ||||
| PAI [score] | 53.5 | ±10.8 | 28–77 | 47.4 | ±11.3 | 28–63 | 54.6 | ±10.3 | 35–77 | 0.076 |
| All Participants (n = 77) | Lifestyle Changes Due to the COVID-19 Pandemic | p | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Lifestyle-Affected (n = 13) | Unaffected (n = 64) | |||||||||
| Mean ± SD or n (%) | Range | Mean ± SD or n (%) | Range | Mean ± SD or n (%) | Range | |||||
| Age [year] | 33.8 | ±5.1 | 23–47 | 34.6 | ± 5.9 | 26–47 | 33.6 | ±5.0 | 23–43 | 0.693 |
| Gestational period [n (%)] | ||||||||||
| Second trimester | 40 | (51.9) | 4 | (30.8) | 36 | (56.3) | 0.130 * | |||
| Third trimester | 37 | (48.1) | 9 | (69.2) | 28 | (43.8) | ||||
| Working status [n (%)] | ||||||||||
| Working or Student | 38 | (49.4) | 5 | (38.5) | 33 | (51.6) | 0.545 * | |||
| Housewife | 39 | (50.6) | 8 | (61.5) | 31 | (48.4) | ||||
| Education level [n (%)] | ||||||||||
| University or above | 20 | (26.0) | 1 | (7.7) | 19 | (29.7) | 0.283 * | |||
| Junior or technical college | 23 | (29.9) | 5 | (38.5) | 18 | (28.1) | ||||
| High school/Junior high school | 34 | (44.2) | 7 | (53.8) | 27 | (42.2) | ||||
| Annual income [n (%)] | ||||||||||
| ≥9 million yen | 3 | (3.9) | 0 | (0.0) | 3 | (4.7) | 0.216 * | |||
| 5–9 million yen | 34 | (44.2) | 3 | (23.1) | 31 | (48.4) | ||||
| 0–5 million yen | 40 | (51.9) | 10 | (76.9) | 30 | (46.9) | ||||
| Prepregnancy BMI [n (%)] | ||||||||||
| Underweight (BMI < 18.5 kg/m2) | 12 | (15.6) | 1 | (7.7) | 11 | (17.2) | 0.403 † | |||
| Normal weight (18.5–24.9 kg/m2) | 53 | (68.8) | 11 | (84.6) | 42 | (65.6) | ||||
| Overweight or obese (BMI > 24.9 kg/m2) | 12 | (15.6) | 1 | (7.7) | 11 | (17.2) | ||||
| PAI [score] | 48.3 | ±10.4 | 34–79 | 49.2 | ±9.4 | 37–66 | 48.2 | ±10.7 | 22–79 | 0.678 |
| Lifestyle Changes Due to the COVID-19 Pandemic | ANOVA | ANCOVA * | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Lifestyle-Affected (n = 14) | Unaffected (n = 77) | ||||||||
| Unit | Mean | SD | Mean | SD | F | p | F | p | |
| Energy | (kcal/day) | 1675 | 305 | 1668 | 430 | 0.004 | 0.952 | 0.038 | 0.847 |
| Protein | (% energy) | 15 | 1 | 13 | 2 | 5.845 | 0.018 | 4.988 | 0.028 |
| Fat | (% energy) | 33 | 5 | 33 | 6 | 0.001 | 0.978 | 0.021 | 0.884 |
| n-3 polyunsaturated fatty acid | (% energy) | 1.2 | 0.3 | 1.1 | 0.3 | 0.258 | 0.613 | 0.067 | 0.796 |
| n-6 polyunsaturated fatty acid | (% energy) | 6.0 | 1.0 | 5.9 | 1.2 | 0.215 | 0.644 | 0.020 | 0.887 |
| Eicosapentaenoic acid | (% energy) | 0.06 | 0.03 | 0.05 | 0.04 | 0.408 | 0.524 | 0.138 | 0.711 |
| Docosahexaenoic acid | (% energy) | 0.12 | 0.05 | 0.10 | 0.05 | 0.913 | 0.342 | 0.232 | 0.632 |
| Carbohydrate | (% energy) | 52 | 6 | 53 | 7 | 0.376 | 0.541 | 0.136 | 0.713 |
| Total dietary fiber | (g/1000 kcal) | 6.6 | 1.5 | 6.3 | 1.8 | 0.388 | 0.535 | 0.744 | 0.391 |
| Sodium | (mg/1000 kcal) | 2120 | 380 | 2093 | 465 | 0.041 | 0.841 | 0.221 | 0.640 |
| Potassium | (mg/1000 kcal) | 1296 | 257 | 1132 | 246 | 5.251 | 0.024 | 8.518 | 0.005 |
| Calcium | (mg/1000 kcal) | 341 | 107 | 272 | 89 | 6.641 | 0.012 | 9.087 | 0.003 |
| Iron | (mg/1000 kcal) | 3.9 | 0.5 | 3.6 | 0.7 | 1.991 | 0.162 | 2.223 | 0.140 |
| Magnesium | (mg/1000 kcal) | 132 | 22 | 116 | 22 | 6.791 | 0.011 | 10.040 | 0.002 |
| Zinc | (mg/1000 kcal) | 4.2 | 0.3 | 4.0 | 0.5 | 2.004 | 0.160 | 1.523 | 0.221 |
| Copper | (mg/1000 kcal) | 0.56 | 0.08 | 0.55 | 0.11 | 0.132 | 0.717 | 0.466 | 0.497 |
| Vitamin D | (μg/1000 kcal) | 2.8 | 0.9 | 2.6 | 1.6 | 0.173 | 0.678 | 0.052 | 0.821 |
| α-tocopherol | (mg/1000 kcal) | 4.5 | 0.9 | 4.2 | 0.9 | 0.919 | 0.340 | 0.708 | 0.403 |
| Vitamin B1 | (mg/1000 kcal) | 0.48 | 0.06 | 0.46 | 0.14 | 0.085 | 0.771 | 0.049 | 0.825 |
| Vitamin B2 | (mg/1000 kcal) | 0.83 | 0.24 | 0.73 | 0.19 | 3.191 | 0.077 | 3.819 | 0.054 |
| Vitamin B6 | (mg/1000 kcal) | 0.61 | 0.14 | 0.53 | 0.12 | 5.039 | 0.027 | 6.547 | 0.012 |
| Vitamin B12 | (μg/1000 kcal) | 2.5 | 0.5 | 2.1 | 0.9 | 1.797 | 0.183 | 1.465 | 0.230 |
| Folate | (μg/1000 kcal) | 159 | 46 | 148 | 43 | 0.716 | 0.400 | 1.206 | 0.276 |
| Vitamin C | (mg/1000 kcal) | 55 | 28 | 54 | 25 | 0.016 | 0.900 | 0.001 | 0.975 |
| β-carotene | (μg/1000 kcal) | 1358 | 717 | 1183 | 609 | 0.920 | 0.340 | 0.916 | 0.342 |
| Lifestyle Changes Due to the COVID-19 Pandemic | ANOVA | ANCOVA * | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Lifestyle-Affected (n = 13) | Unaffected (n = 64) | ||||||||
| Unit | Mean | SD | Mean | SD | F | p | F | p | |
| Energy | (kcal/day) | 1773 | 639 | 1735 | 405 | 0.076 | 0.784 | 0.000 | 0.995 |
| Protein | (% energy) | 14 | 2 | 14 | 2 | 0.045 | 0.833 | 0.138 | 0.712 |
| Fat | (% energy) | 34 | 5 | 31 | 6 | 2.500 | 0.118 | 1.033 | 0.313 |
| n-3 polyunsaturated fatty acid | (% energy) | 1.3 | 0.3 | 1.2 | 0.3 | 0.730 | 0.396 | 0.421 | 0.519 |
| n-6 polyunsaturated fatty acid | (% energy) | 6.4 | 0.9 | 5.9 | 1.4 | 1.367 | 0.247 | 0.545 | 0.463 |
| Eicosapentaenoic acid | (% energy) | 0.07 | 0.05 | 0.06 | 0.05 | 0.015 | 0.902 | 0.005 | 0.946 |
| Docosahexaenoic acid | (% energy) | 0.13 | 0.08 | 0.12 | 0.08 | 0.219 | 0.641 | 0.095 | 0.759 |
| Carbohydrate | (% energy) | 51 | 6 | 54 | 7 | 2.389 | 0.126 | 0.787 | 0.278 |
| Total dietary fiber | (g/1000 kcal) | 5.5 | 1.3 | 6.8 | 1.8 | 5.312 | 0.024 | 6.399 | 0.014 |
| Sodium | (mg/1000 kcal) | 2240 | 561 | 2230 | 727 | 0.002 | 0.961 | 0.111 | 0.740 |
| Potassium | (mg/1000 kcal) | 1064 | 219 | 1063 | 298 | 1.302 | 0.257 | 1.666 | 0.201 |
| Calcium | (mg/1000 kcal) | 251 | 75 | 283 | 116 | 0.952 | 0.332 | 1.653 | 0.203 |
| Iron | (mg/1000 kcal) | 3.6 | 0.8 | 3.8 | 0.9 | 0.494 | 0.484 | 2.054 | 0.157 |
| Magnesium | (mg/1000 kcal) | 114 | 19 | 119 | 28 | 0.389 | 0.535 | 1.207 | 0.276 |
| Zinc | (mg/1000 kcal) | 4.0 | 0.6 | 4.1 | 0.7 | 0.170 | 0.681 | 0.930 | 0.338 |
| Copper | (mg/1000 kcal) | 0.52 | 0.08 | 0.56 | 0.10 | 2.391 | 0.126 | 3.353 | 0.072 |
| Vitamin D | (μg/1000 kcal) | 2.8 | 1.6 | 2.7 | 1.4 | 0.039 | 0.845 | 0.023 | 0.881 |
| α-tocopherol | (mg/1000 kcal) | 4.3 | 0.9 | 4.3 | 1.1 | 0.002 | 0.969 | 0.063 | 0.802 |
| Vitamin B1 | (mg/1000 kcal) | 0.44 | 0.09 | 0.46 | 0.10 | 0.281 | 0.598 | 0.957 | 0.332 |
| Vitamin B2 | (mg/1000 kcal) | 0.77 | 0.19 | 0.77 | 0.24 | 0.001 | 0.979 | 0.209 | 0.649 |
| Vitamin B6 | (mg/1000 kcal) | 0.52 | 0.14 | 0.54 | 0.13 | 0.242 | 0.625 | 0.350 | 0.556 |
| Vitamin B12 | (μg/1000 kcal) | 2.4 | 1.1 | 2.5 | 1.4 | 0.021 | 0.886 | 0.206 | 0.651 |
| Folate | (μg/1000 kcal) | 143 | 37 | 158 | 53 | 0.951 | 0.333 | 1.576 | 0.214 |
| Vitamin C | (mg/1000 kcal) | 43 | 14 | 51 | 23 | 1.370 | 0.245 | 1.169 | 0.284 |
| β-carotene | (μg/1000 kcal) | 1030 | 396 | 1518 | 787 | 4.696 | 0.034 | 4.499 | 0.038 |
| Lifestyle Changes Due to the COVID-19 Pandemic | ANOVA | ANCOVA * | ||||||
|---|---|---|---|---|---|---|---|---|
| Lifestyle-Affected (n = 14) | Unaffected (n = 77) | |||||||
| Mean | SD | Mean | SD | F | p | F | p | |
| Total physical activity | 34.41 | 15.33 | 30.66 | 14.22 | 1.158 | 0.285 | 1.082 | 0.301 |
| Activity intensity | ||||||||
| Sedentary (<1.5 METs) | 11.81 | 5.00 | 11.14 | 5.58 | 0.248 | 0.619 | 0.637 | 0.427 |
| Light (1.5–<3.0 METs) | 15.86 | 8.08 | 13.59 | 6.93 | 1.655 | 0.201 | 1.286 | 0.260 |
| Moderate (3.0–<6.0 METs) | 6.07 | 11.93 | 5.38 | 8.62 | 0.090 | 0.765 | 0.226 | 0.636 |
| Vigorous (≧6.0 METs) | 0.05 | 0.17 | 0.11 | 0.65 | 0.148 | 0.701 | 0.009 | 0.924 |
| Activity type | ||||||||
| Household/Caregiving | 6.81 | 2.63 | 6.96 | 3.57 | 0.033 | 0.857 | 0.266 | 0.607 |
| Occupation | 9.54 | 17.09 | 5.51 | 10.35 | 1.869 | 0.175 | 2.355 | 0.128 |
| Sports/Exercise | 0.96 | 1.1 | 1.41 | 2.26 | 0.782 | 0.379 | 0.889 | 0.348 |
| Transportation | 2.49 | 0.54 | 2.82 | 1.24 | 1.339 | 0.250 | 0.792 | 0.376 |
| Inactivity | 15.14 | 6.21 | 14.24 | 7.40 | 0.253 | 0.616 | 0.772 | 0.382 |
| Lifestyle Changes Due to the COVID-19 Pandemic | ANOVA | ANCOVA * | ||||||
|---|---|---|---|---|---|---|---|---|
| Lifestyle-Affected (n = 13) | Unaffected (n = 64) | |||||||
| Mean | SD | Mean | SD | F | p | F | p | |
| Total physical activity | 36.86 | 16.50 | 38.59 | 14.96 | 0.157 | 0.693 | 0.309 | 0.580 |
| Activity intensity | ||||||||
| Sedentary (<1.5 METs) | 7.86 | 3.36 | 7.46 | 4.53 | 1.347 | 0.148 | 1.990 | 0.317 |
| Light (1.5–<3.0 METs) | 20.10 | 8.36 | 20.02 | 8.31 | 0.001 | 0.975 | 0.002 | 0.964 |
| Moderate (3.0–<6.0 METs) | 11.14 | 9.15 | 11.66 | 9.53 | 0.037 | 0.847 | 0.036 | 0.851 |
| Vigorous (≧6.0 METs) | 0.00 | 0.00 | 0.07 | 0.31 | 0.786 | 0.378 | 1.246 | 0.268 |
| Activity type | ||||||||
| Household/Caregiving | 19.02 | 7.22 | 20.47 | 11.18 | 0.231 | 0.632 | 0.528 | 0.470 |
| Occupation | 7.55 | 11.77 | 6.16 | 8.90 | 0.264 | 0.609 | 0.768 | 0.384 |
| Sports/Exercise | 0.60 | 0.87 | 0.91 | 1.49 | 0.597 | 0.442 | 1.172 | 0.283 |
| Transportation | 1.28 | 0.45 | 1.44 | 0.68 | 0.542 | 0.466 | 0.221 | 0.641 |
| Inactivity | 7.99 | 5.01 | 9.80 | 6.21 | 0.812 | 0.373 | 0.308 | 0.582 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hori, N.; Shiraishi, M.; Harada, R.; Kurashima, Y. Association of Lifestyle Changes Due to the COVID-19 Pandemic with Nutrient Intake and Physical Activity Levels during Pregnancy in Japan. Nutrients 2021, 13, 3799. https://doi.org/10.3390/nu13113799
Hori N, Shiraishi M, Harada R, Kurashima Y. Association of Lifestyle Changes Due to the COVID-19 Pandemic with Nutrient Intake and Physical Activity Levels during Pregnancy in Japan. Nutrients. 2021; 13(11):3799. https://doi.org/10.3390/nu13113799
Chicago/Turabian StyleHori, Natsuki, Mie Shiraishi, Rio Harada, and Yuki Kurashima. 2021. "Association of Lifestyle Changes Due to the COVID-19 Pandemic with Nutrient Intake and Physical Activity Levels during Pregnancy in Japan" Nutrients 13, no. 11: 3799. https://doi.org/10.3390/nu13113799
APA StyleHori, N., Shiraishi, M., Harada, R., & Kurashima, Y. (2021). Association of Lifestyle Changes Due to the COVID-19 Pandemic with Nutrient Intake and Physical Activity Levels during Pregnancy in Japan. Nutrients, 13(11), 3799. https://doi.org/10.3390/nu13113799