
Through-Wall Multi-Subject Localization and Vital Signs Monitoring Using UWB MIMO Imaging Radar


Abstract
:
1. Introduction
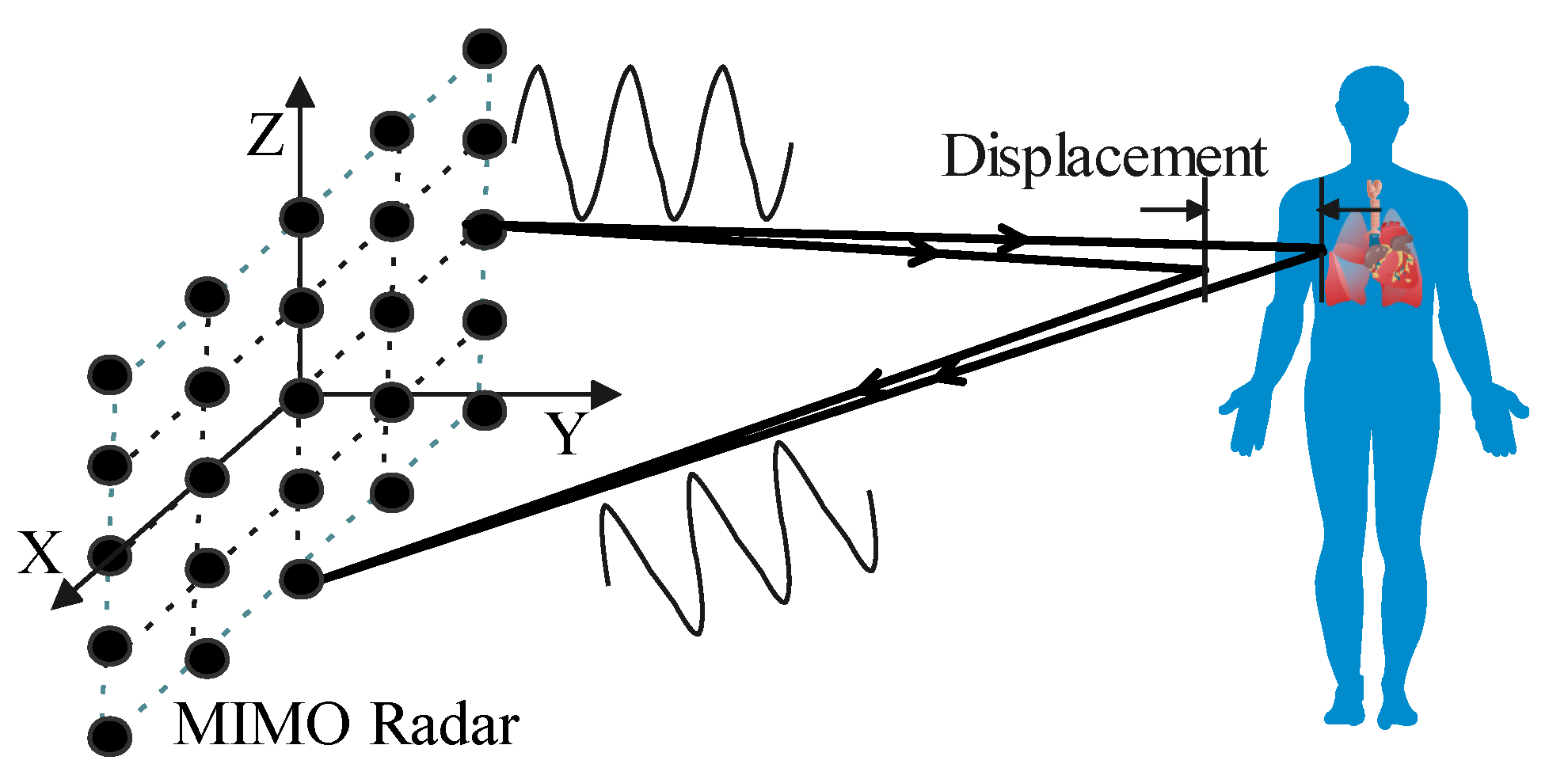
- We derive the relationship between vital signs signal and radar image in theory. It is proved that the thorax movement caused by respiration and heartbeat is linear with the phase of the radar image. The signal-to-noise ratio (SNR) of the extracted vital signs signal is improved by the factor of radar channel number times frequency number compared with CW Doppler radars;
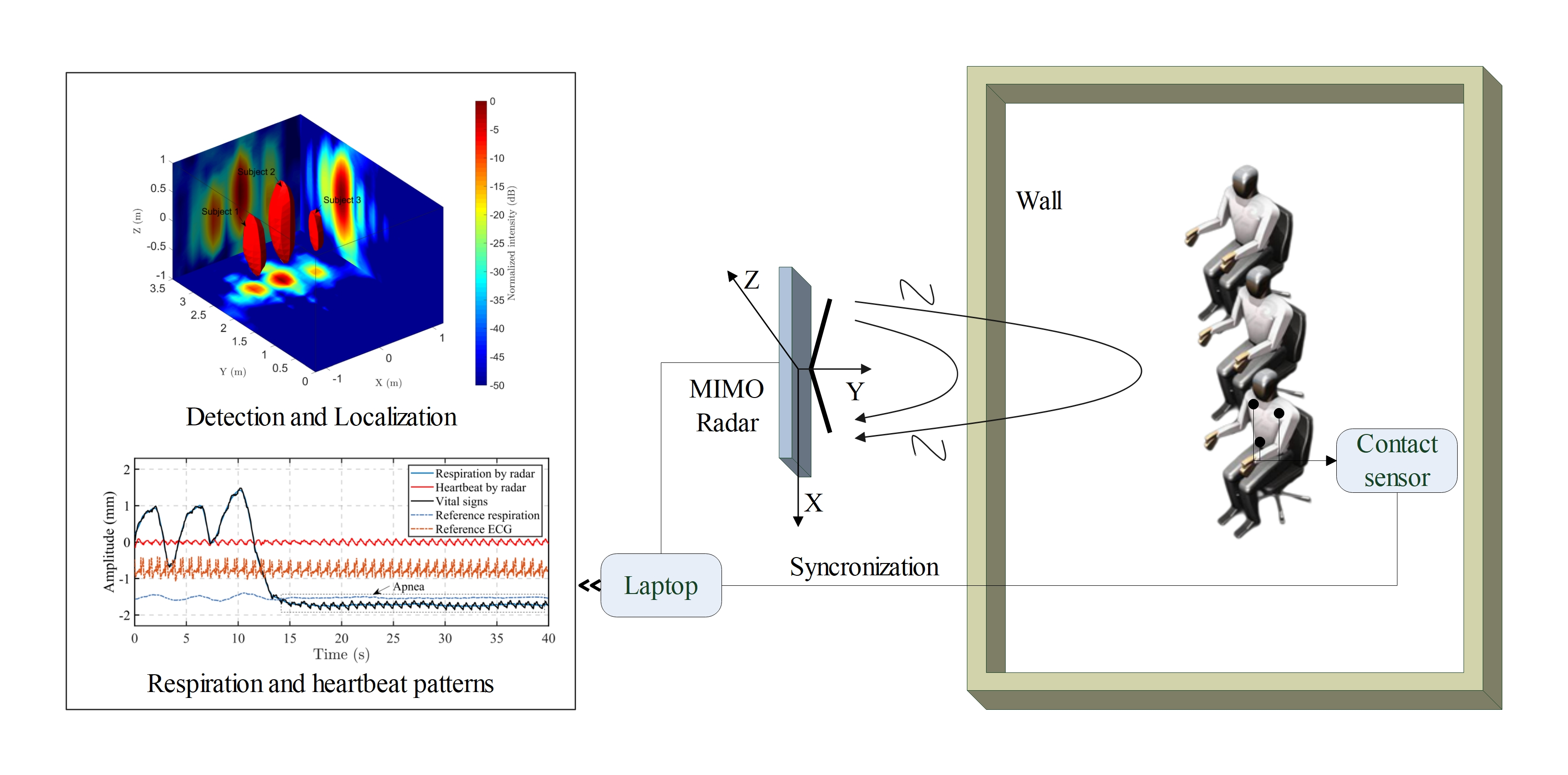
- We develop a processing scheme for through-wall multi-subject localization and vital signs separation. To localize multiple subjects through the wall, we introduce the higher-order cumulant (HOC) for 3-D radar imaging. The HOC-based localization significantly enhances the human body by suppressing the background clutter;
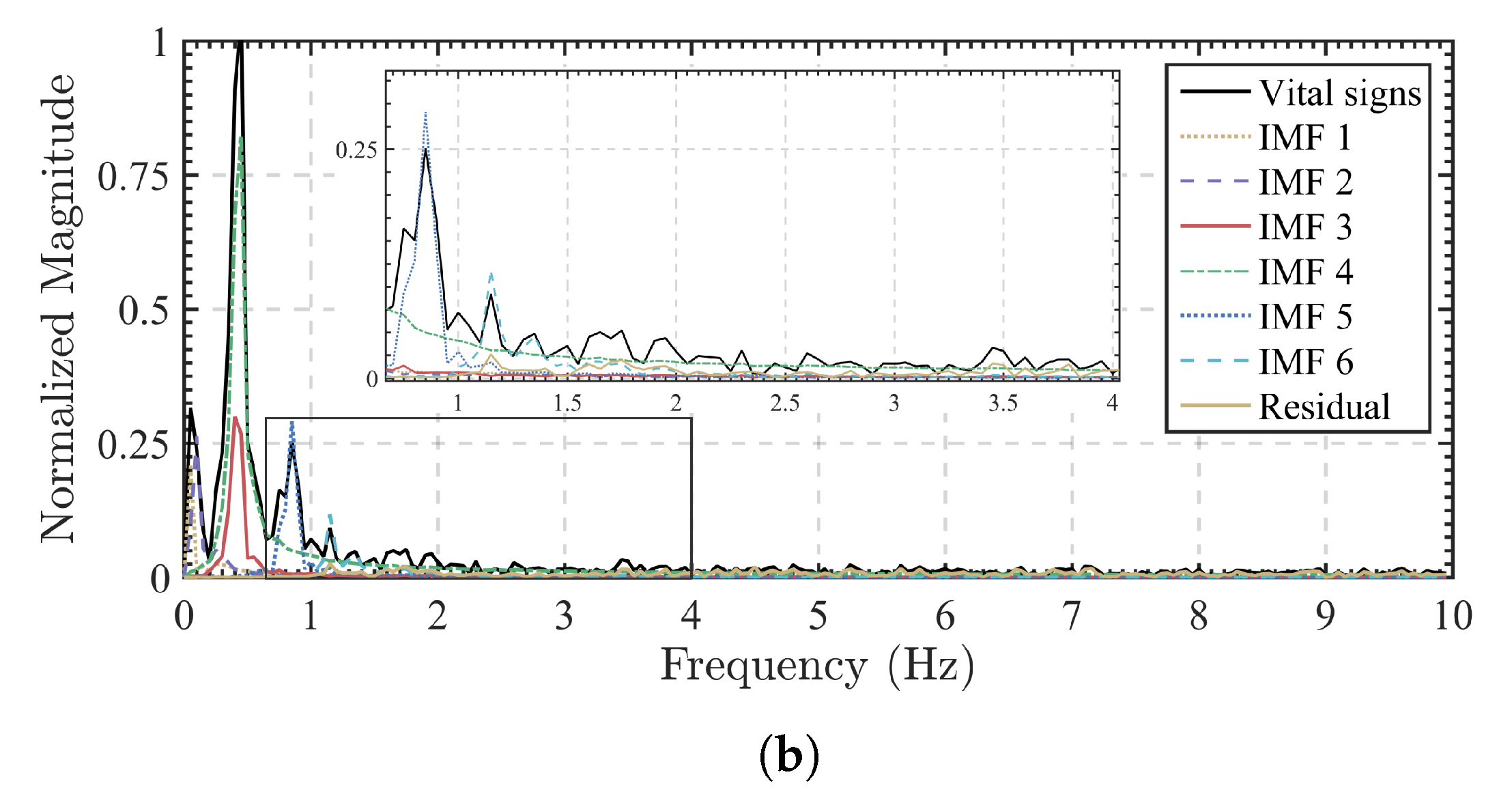
- We apply the VMD algorithm with a new grouping criterion to adaptively separate the respiration and heartbeat patterns by combining the decomposed intrinsic mode functions (IMFs) and the residual. The grouping criterion exploits the center frequency of each mode to separate the heartbeat pattern from the respiration harmonics.
2. Materials and Methods
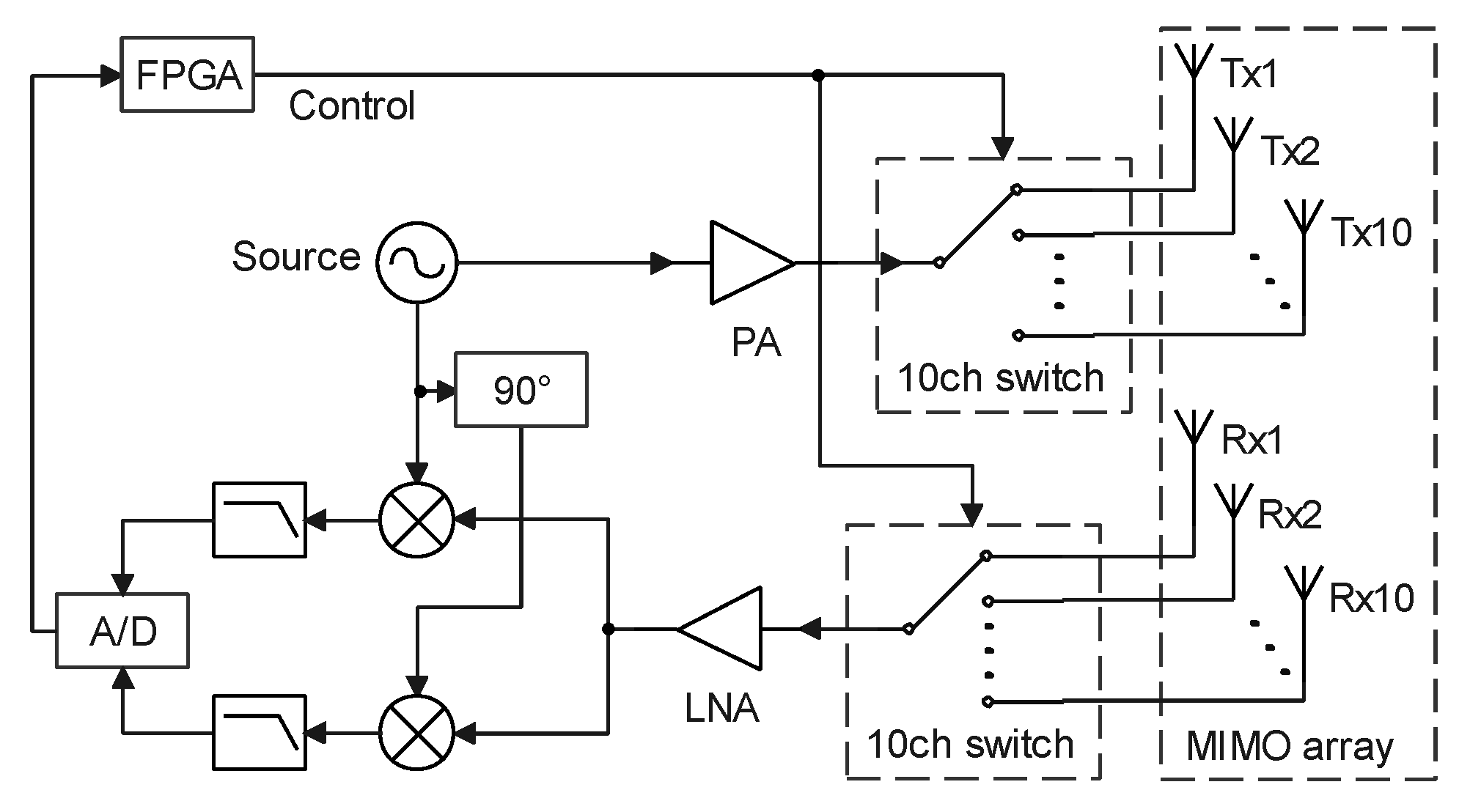
2.1. System Model
2.2. Scheme and Method
2.2.1. Multiple Subjects Detection and Localization
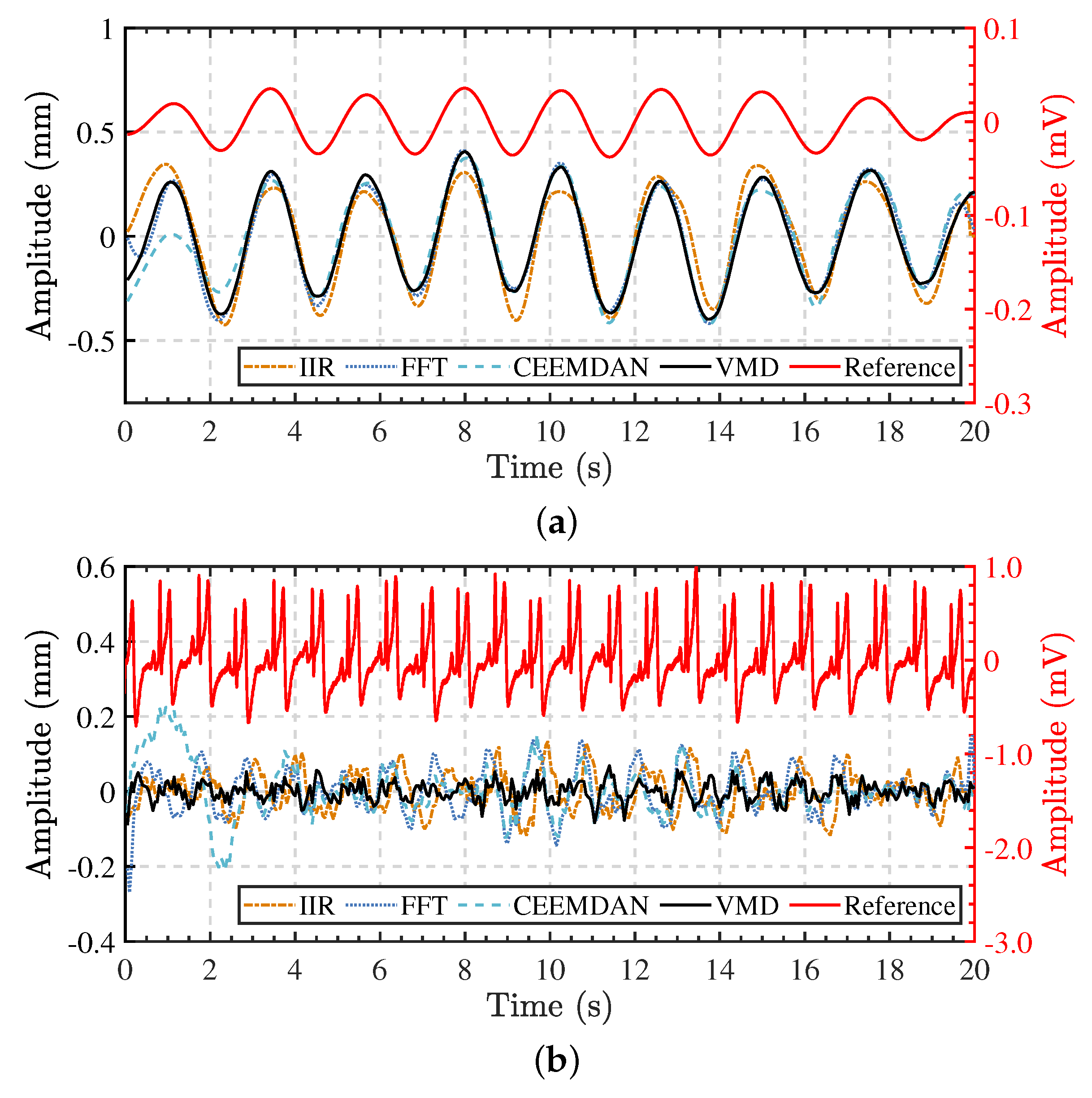
2.2.2. Respiration and Heartbeat Patterns Separation
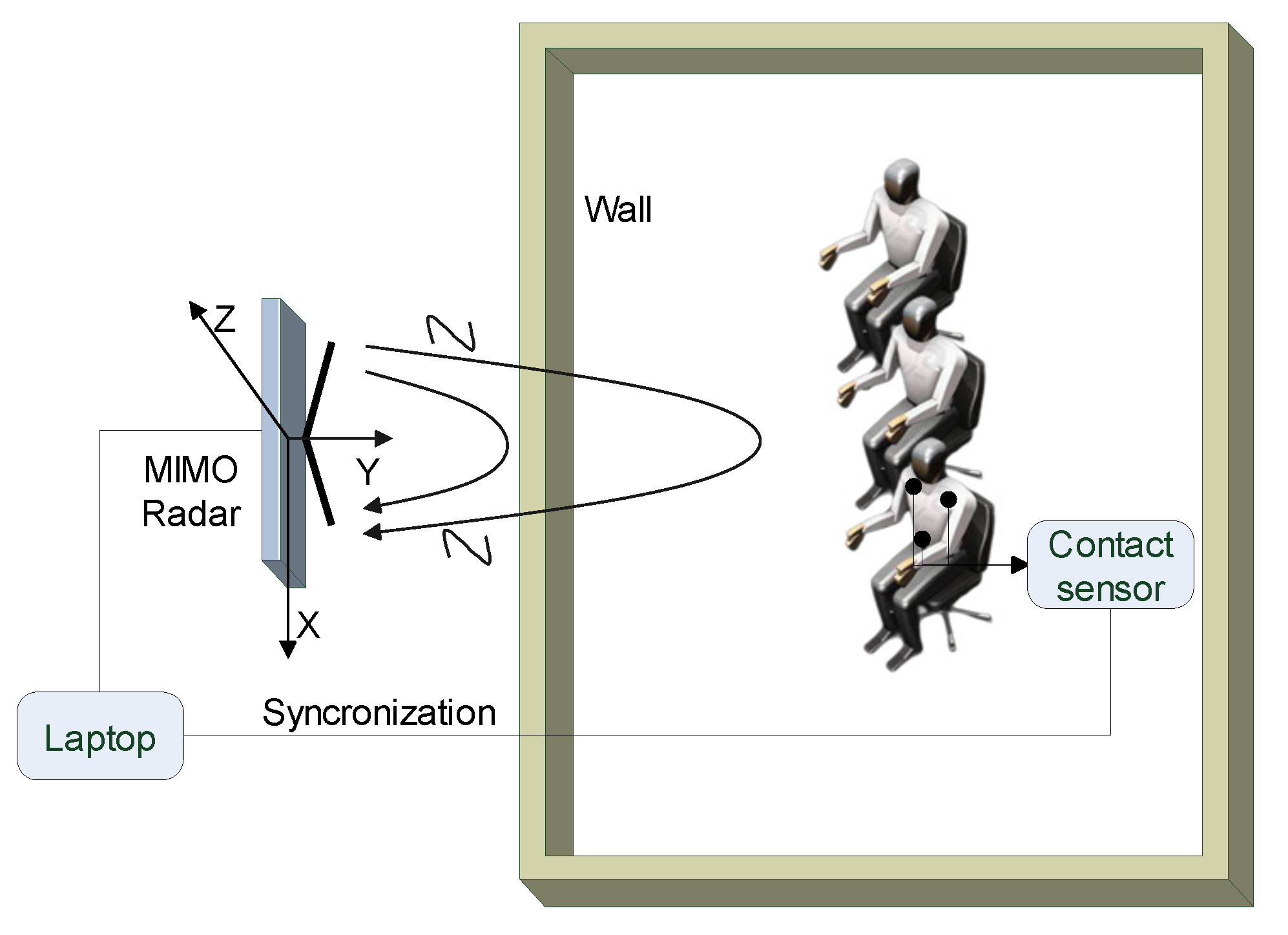
2.3. Experiments
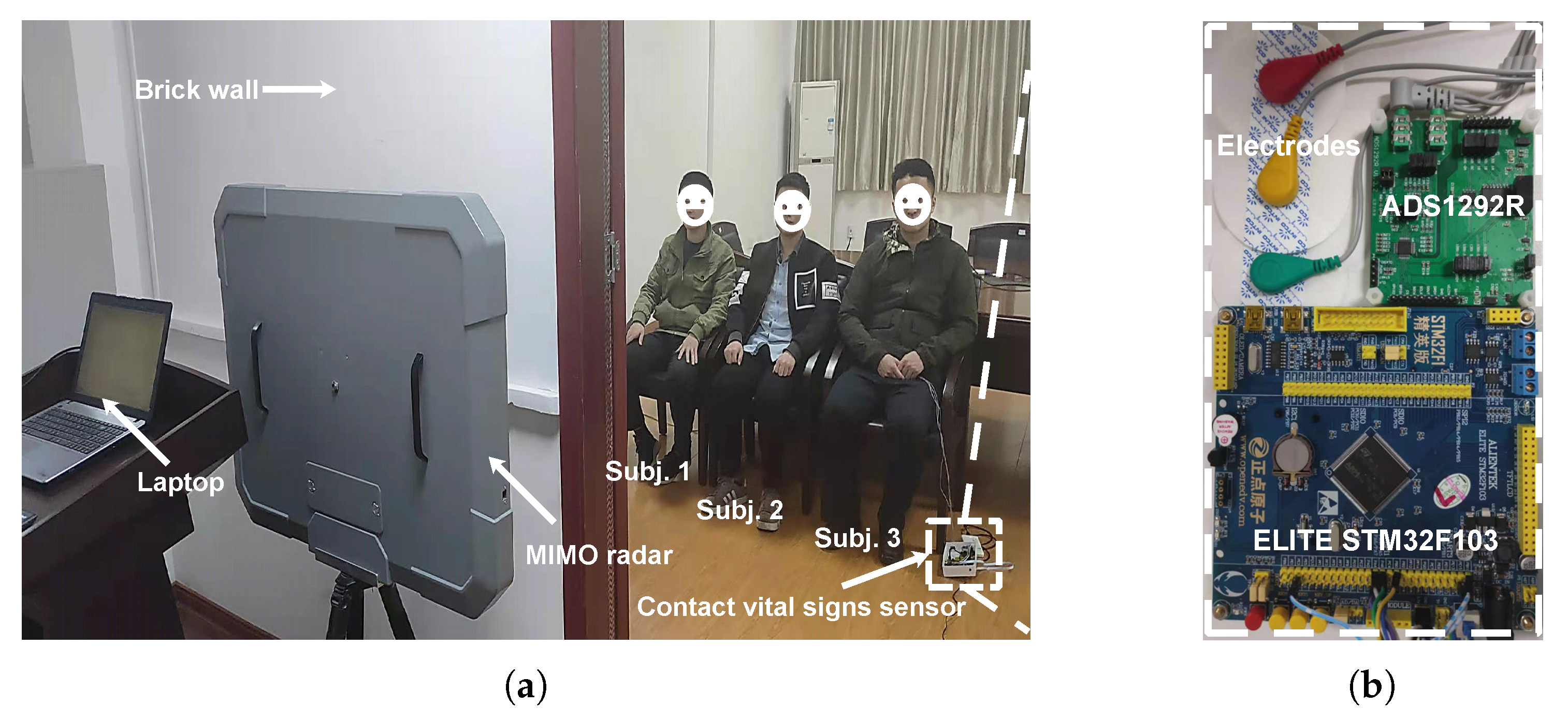
2.3.1. Measurement Equipment and Parameters
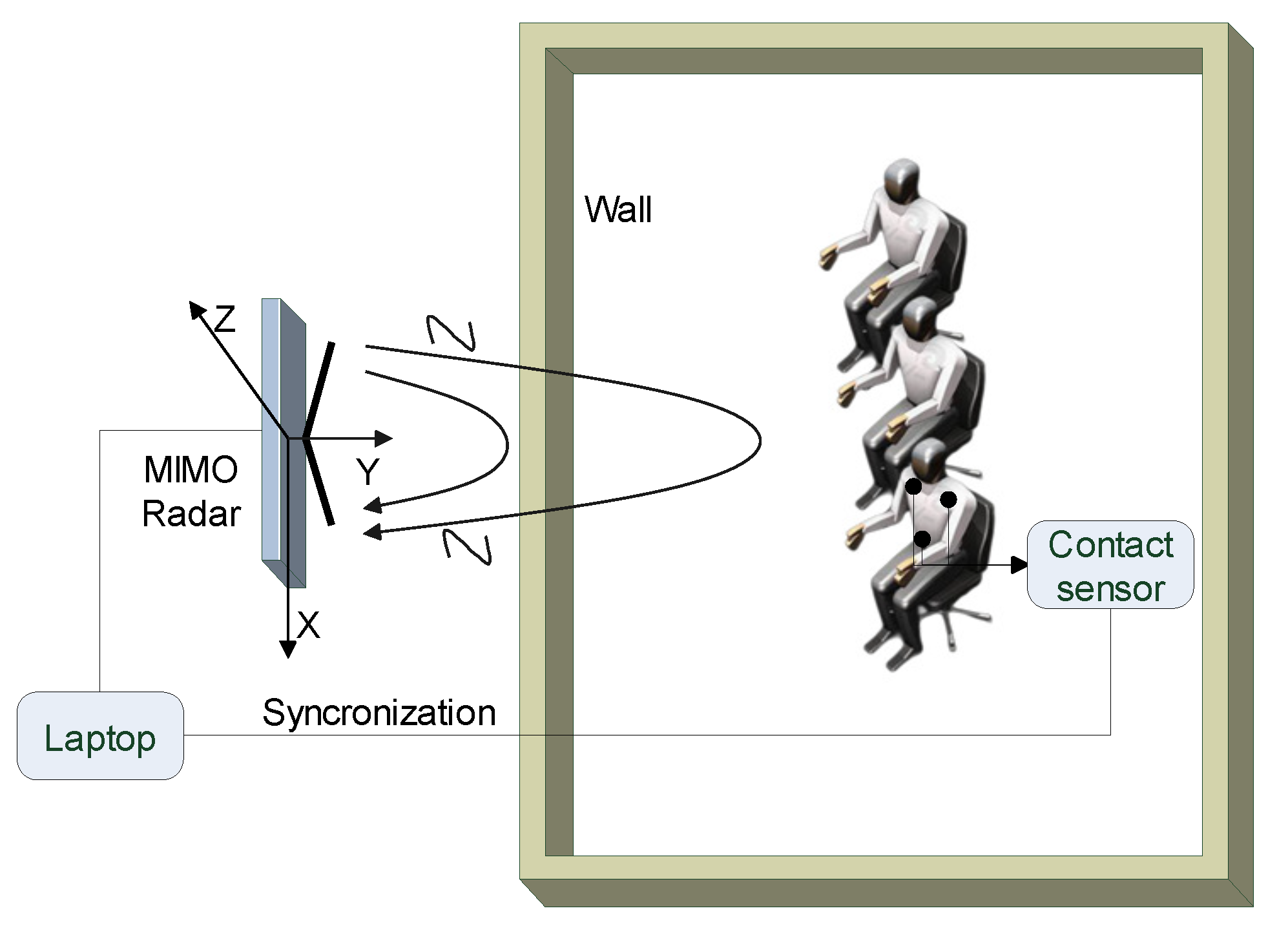
2.3.2. Measurements Setup and Scenarios
3. Results
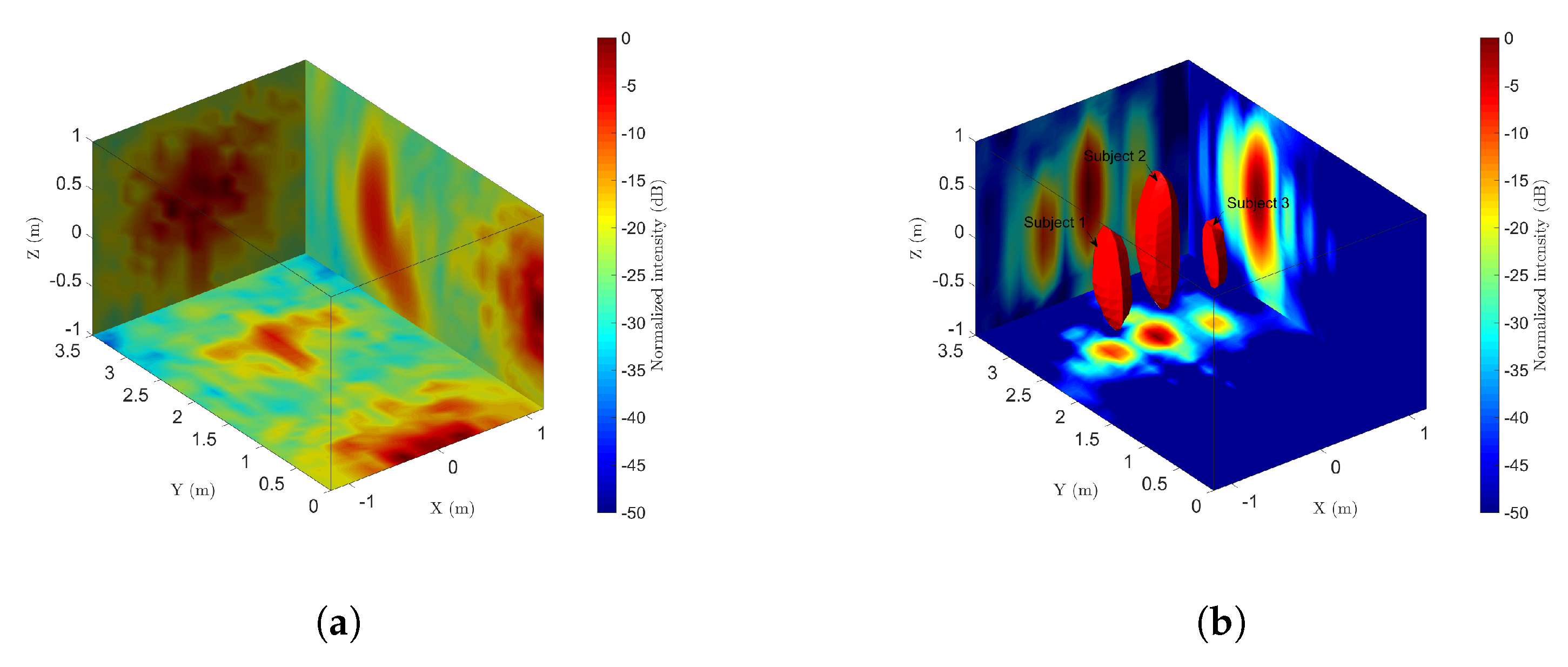
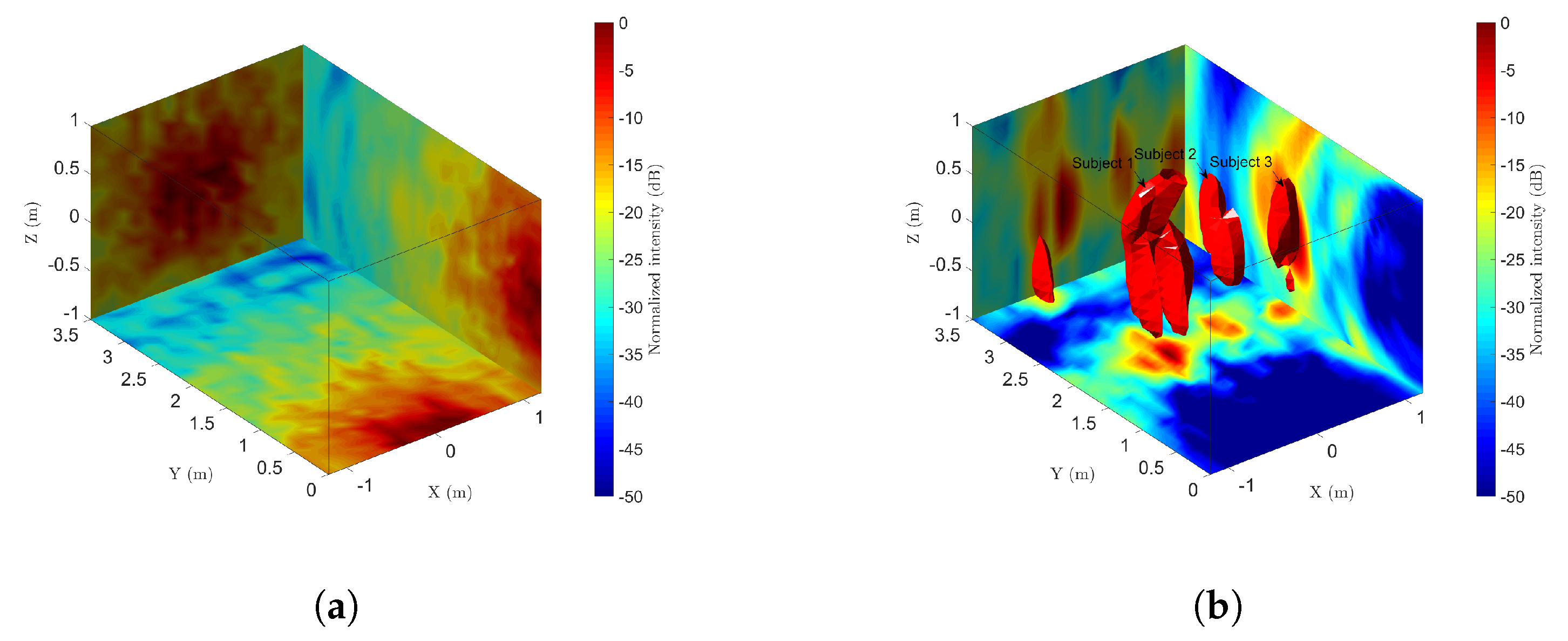
3.1. Detection and Localization Results
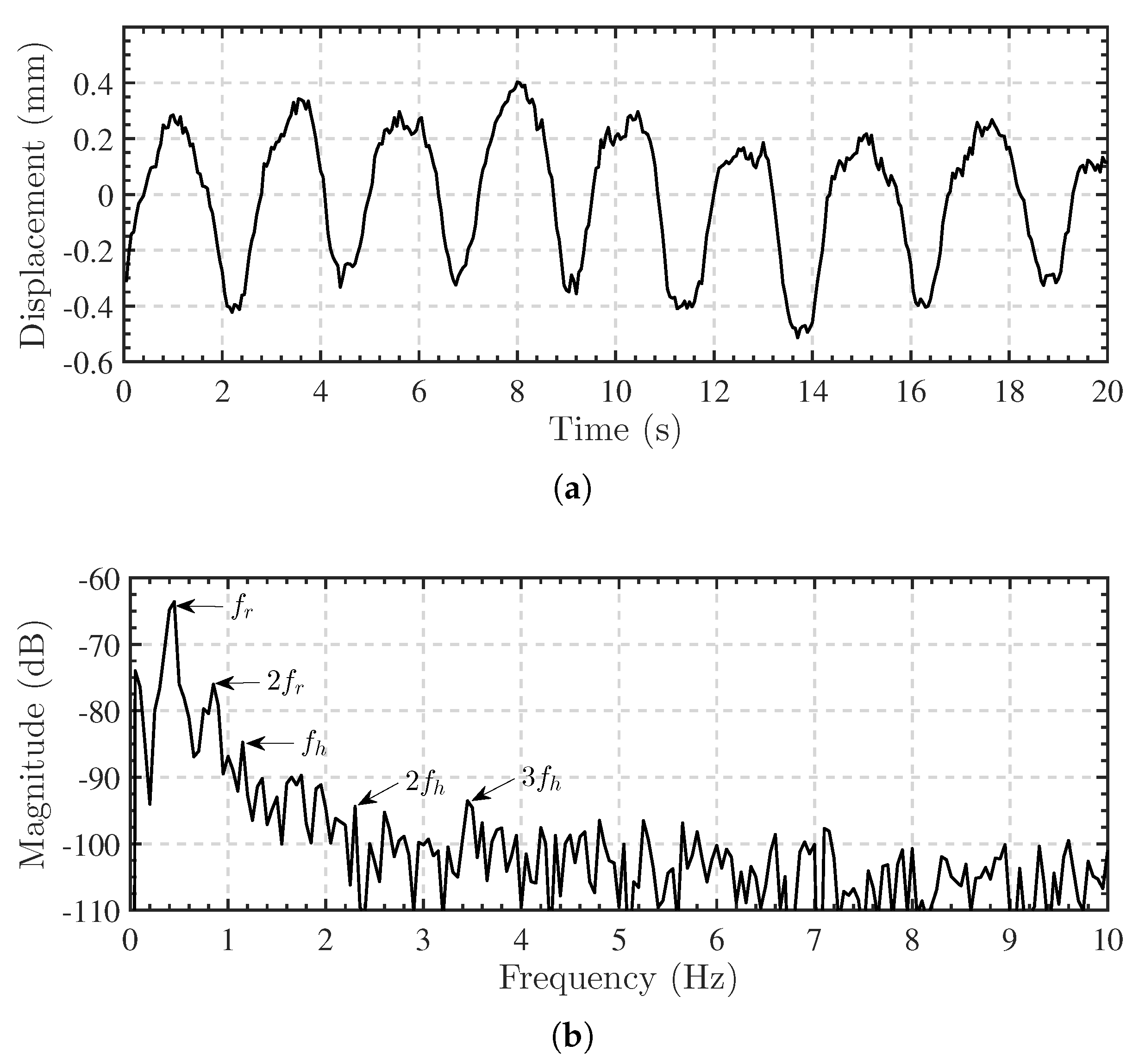
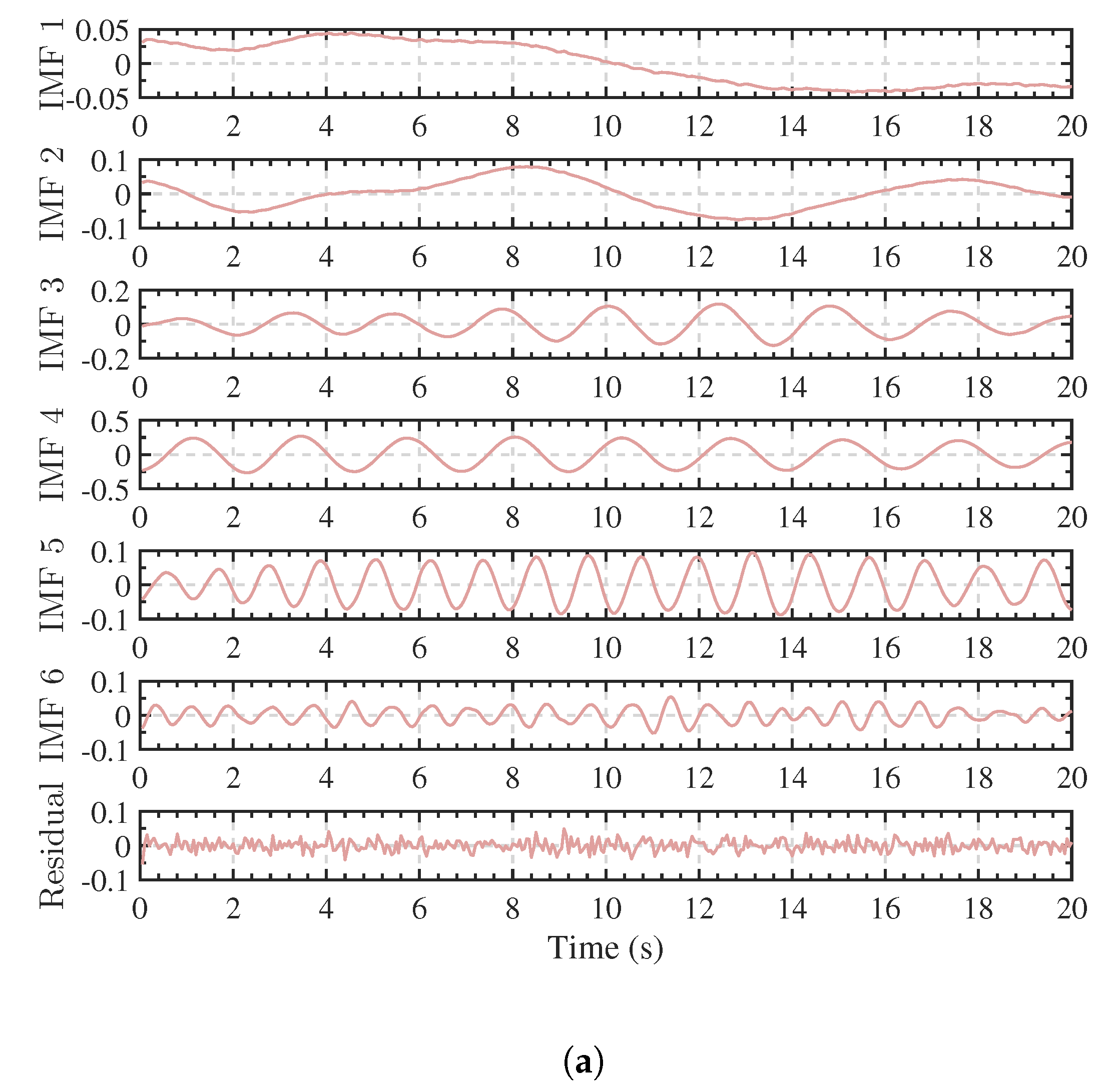
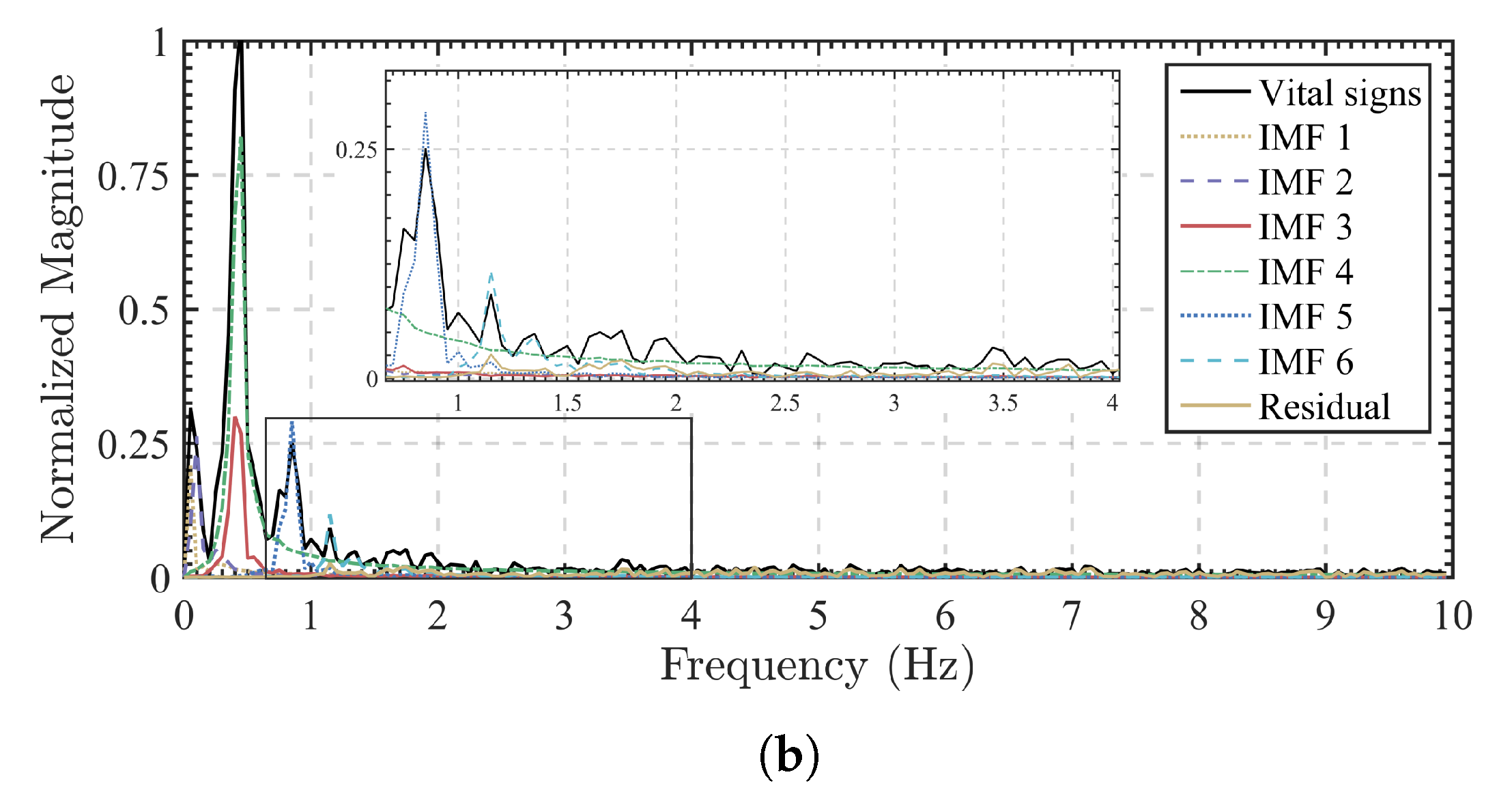
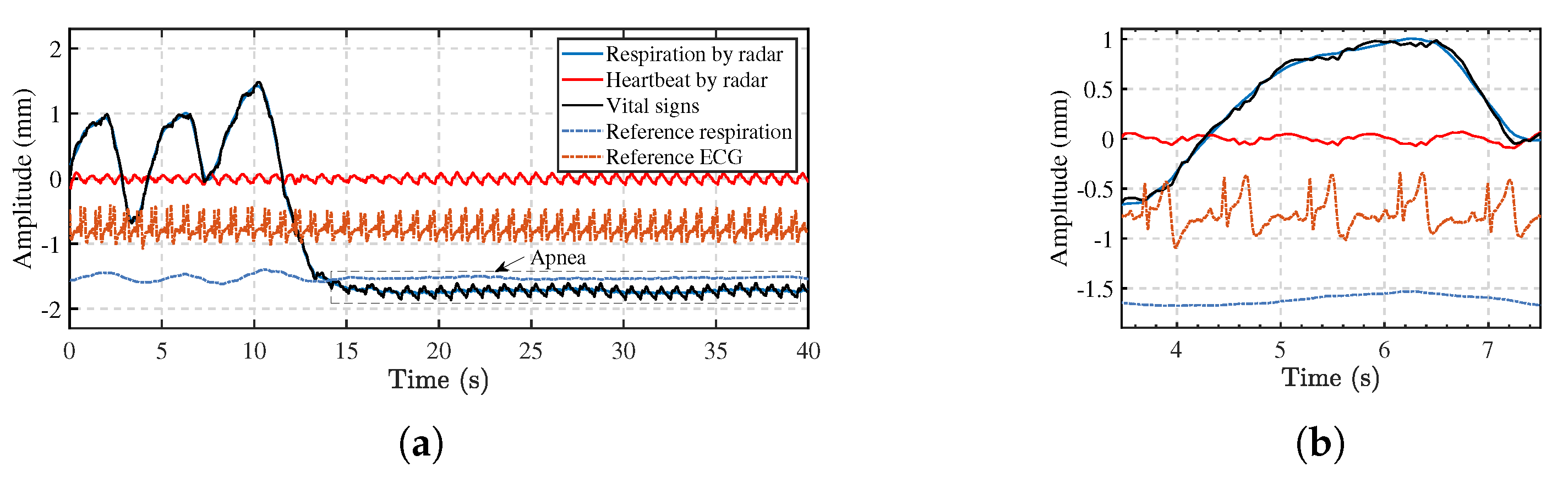
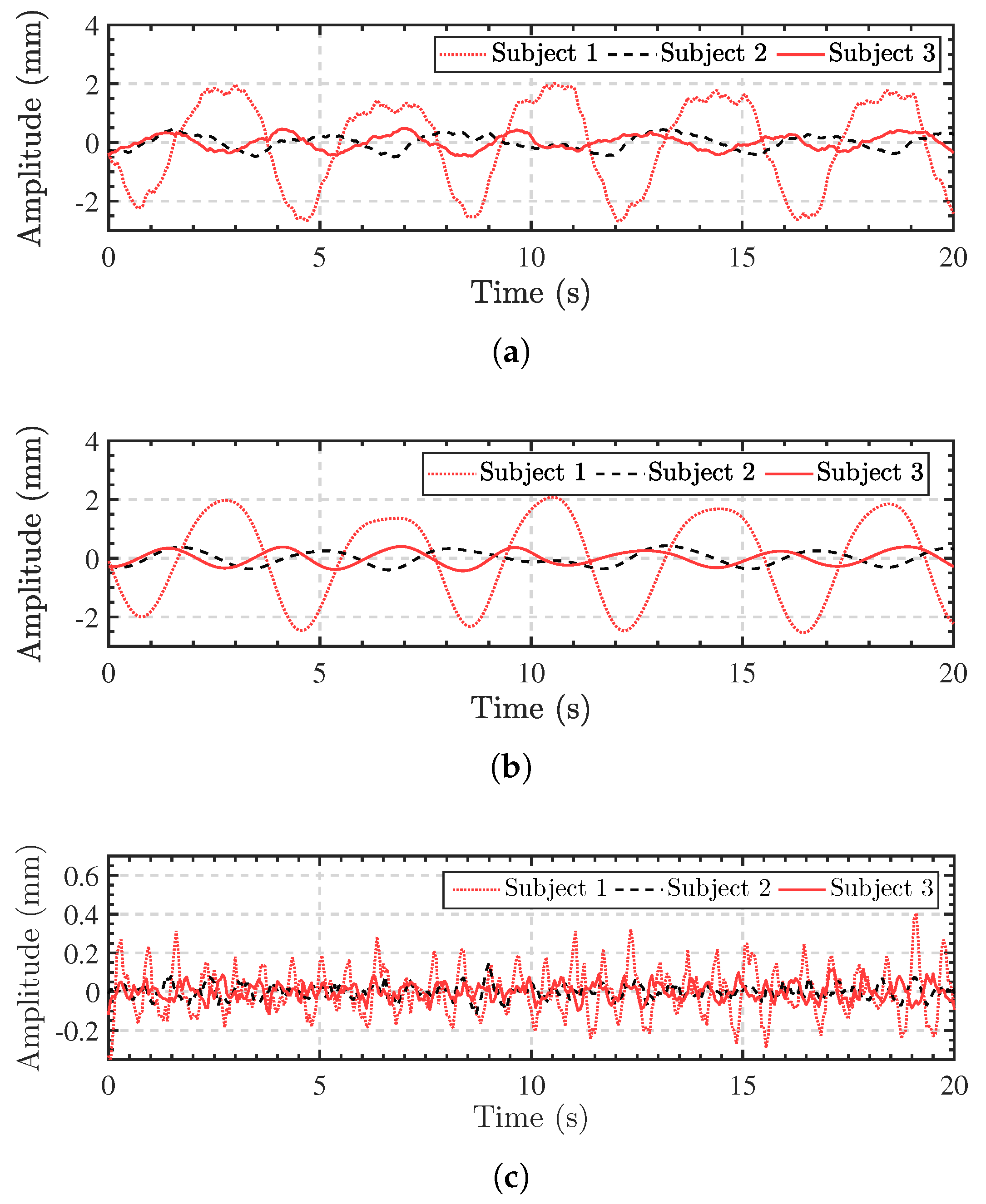
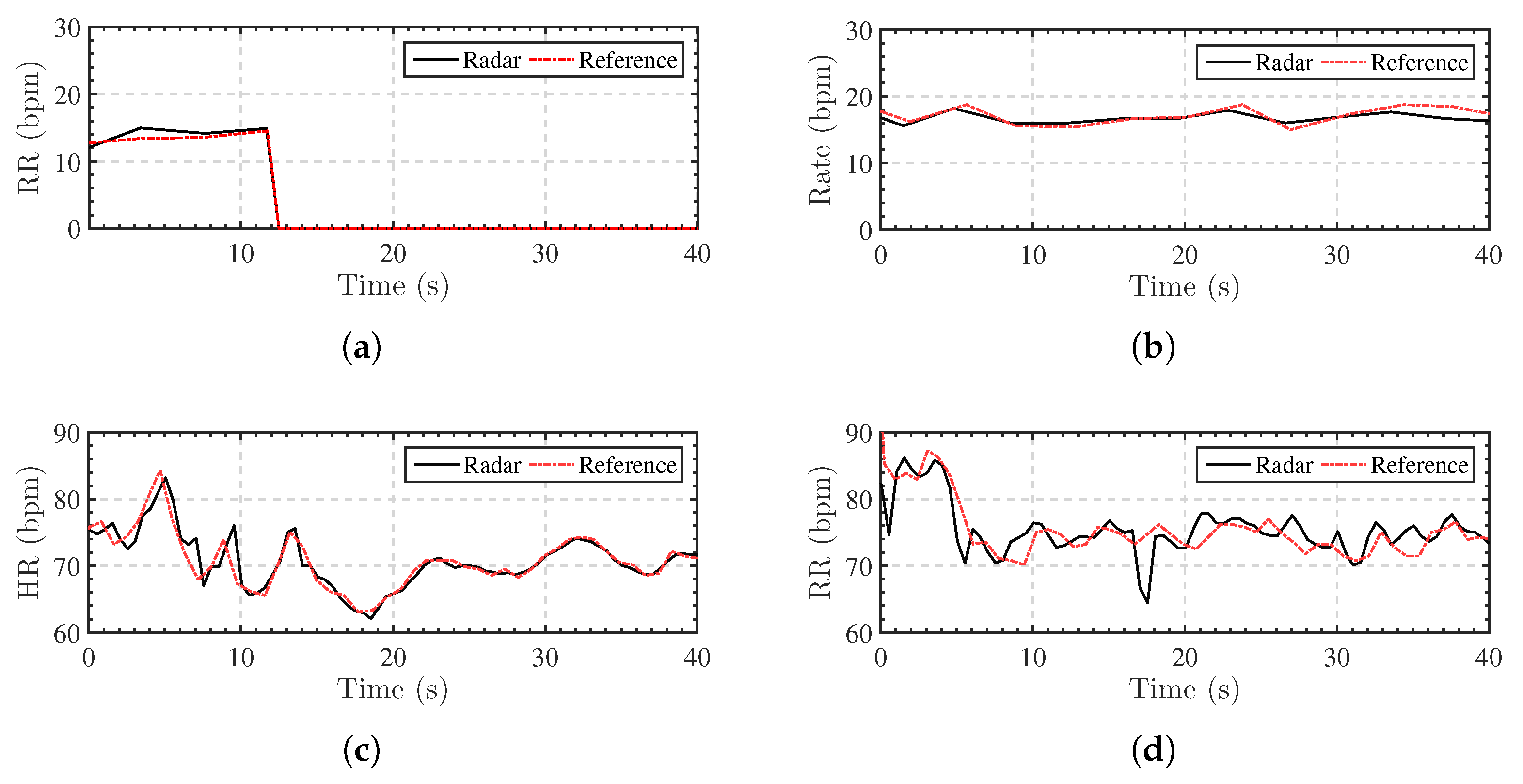
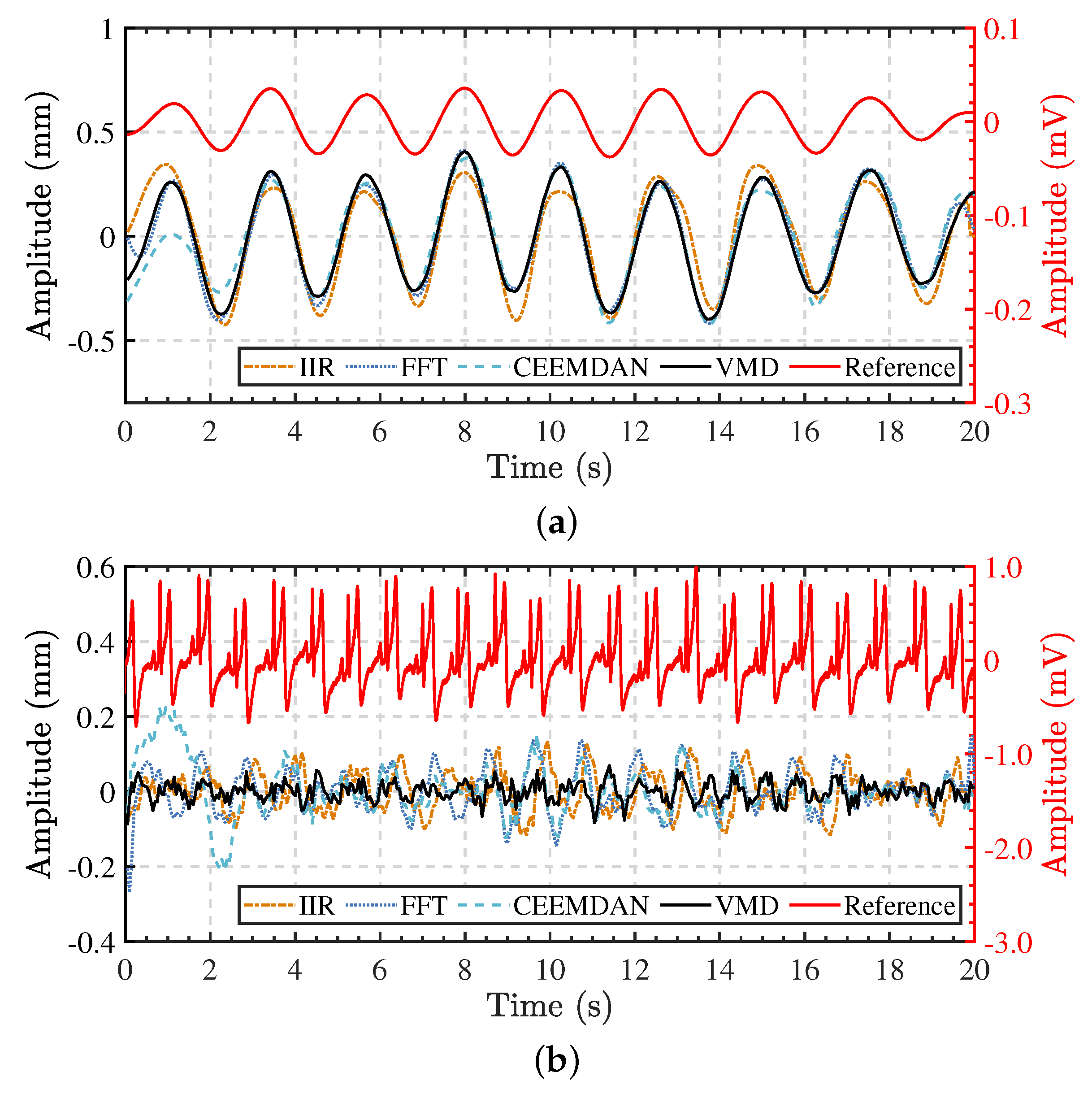
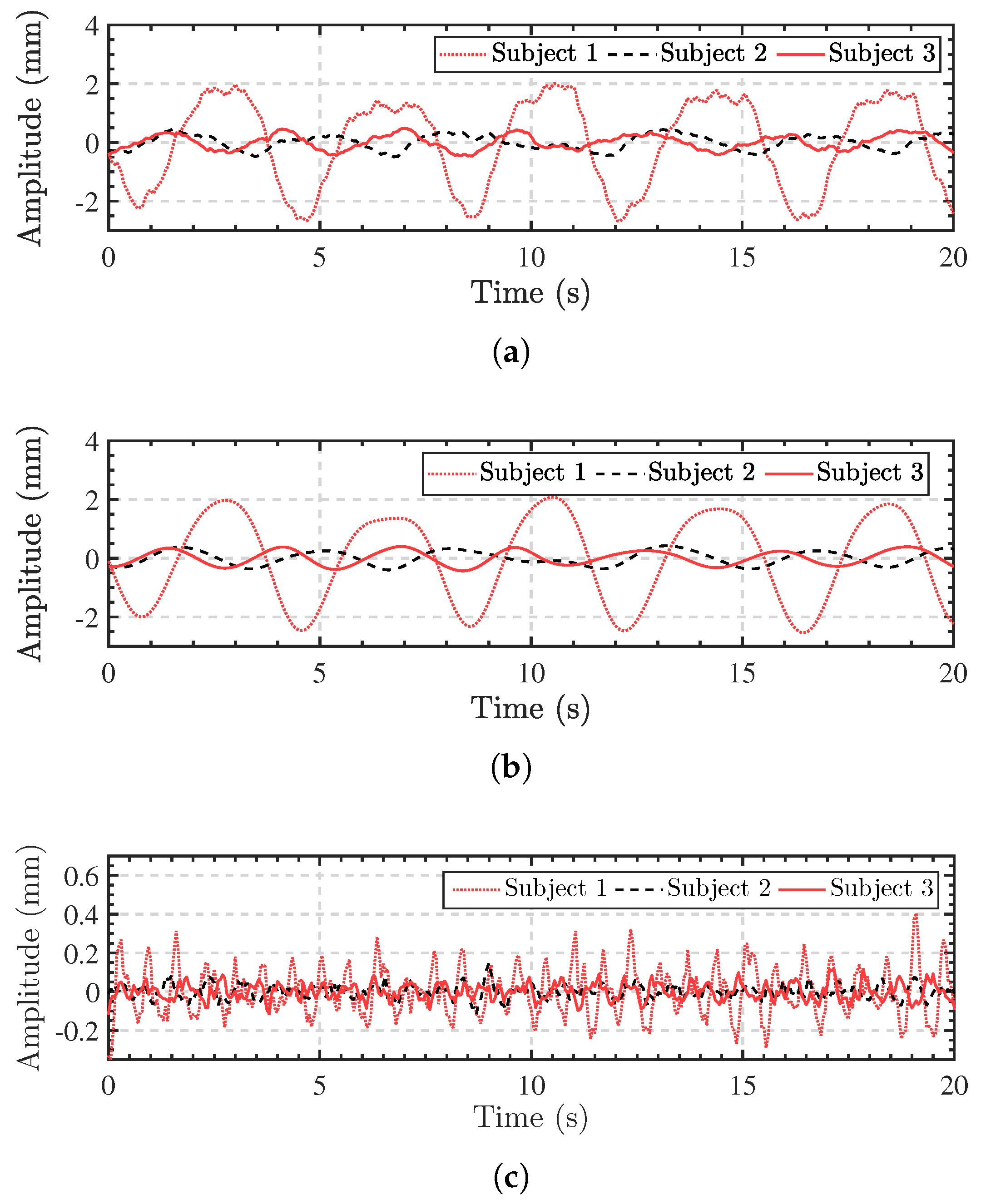
3.2. Vital Signs Separation Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| AD | Arctangent demodulation |
| BSS | Blind source separation |
| BP | Back-projection |
| CEEMDAN | Complete ensemble empirical mode decomposition with adaptive noise |
| CFAR | Constant false alarm rate |
| CW | Continuous-wave |
| DACM | Differentiate and cross multiply |
| DC | Direct Current |
| ECG | Electrocardiogram |
| EMD | Empirical mode decomposition |
| EEMD | Ensemble empirical mode decomposition |
| FMCW | Frequency-modulated continuous-wave |
| HOC | Higher-order cumulant |
| HR | Heart rate |
| IIR | Infinite impulse response |
| IMF | Intrinsic mode function |
| IR-UWB | Impulse radio ultra-wideband |
| MIMO | Multiple-input multiple-output |
| RMSE | Root mean square error |
| RR | Respiratory rate |
| SFCW | Stepped-frequency continuous-wave |
| STFT | Short-time Fourier transform |
| SIMO | Single-input multiple-output |
| SNR | Signal-to-noise ratio |
| UWB | Ultra-wideband |
| VMD | Variational mode decomposition |
References
- Clemente, C.; Balleri, A.; Woodbridge, K.; Soraghan, J.J. Developments in Target Micro-Doppler Signatures Analysis: Radar Imaging, Ultrasound and through-the-Wall Radar. EURASIP J. Adv. Signal Process. 2013, 2013, 47. [Google Scholar] [CrossRef] [Green Version]
- Liang, S.D. Sense-through-Wall Human Detection Based on UWB Radar Sensors. Signal Process. 2016, 126, 117–124. [Google Scholar] [CrossRef]
- Thi Phuoc Van, N.; Tang, L.; Demir, V.; Hasan, S.F.; Duc Minh, N.; Mukhopadhyay, S. Review-Microwave Radar Sensing Systems for Search and Rescue Purposes. Sensors 2019, 19, 2879. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, C.; Lubecke, V.M.; Boric-Lubecke, O.; Lin, J. Sensing of Life Activities at the Human-Microwave Frontier. IEEE J. Microwaves 2021, 1, 66–78. [Google Scholar] [CrossRef]
- Li, C.; Cummings, J.; Lam, J.; Graves, E.; Wu, W. Radar Remote Monitoring of Vital Signs. IEEE Microw. Mag. 2009, 10, 47–56. [Google Scholar] [CrossRef]
- Li, C.; Peng, Z.; Huang, T.Y.; Fan, T.; Wang, F.K.; Horng, T.S.; Munoz-Ferreras, J.M.; Gomez-Garcia, R.; Ran, L.; Lin, J. A Review on Recent Progress of Portable Short-Range Noncontact Microwave Radar Systems. IEEE Trans. Microw. Theory Tech. 2017, 65, 1692–1706. [Google Scholar] [CrossRef]
- Cerasuolo, G.; Petrella, O.; Marciano, L.; Soldovieri, F.; Gennarelli, G. Metrological Characterization for Vital Sign Detection by a Bioradar. Remote Sens. 2017, 9, 996. [Google Scholar] [CrossRef] [Green Version]
- Will, C.; Shi, K.; Schellenberger, S.; Steigleder, T.; Michler, F.; Fuchs, J.; Weigel, R.; Ostgathe, C.; Koelpin, A. Radar-Based Heart Sound Detection. Sci. Rep. 2018, 8, 11551. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lazaro, A.; Girbau, D.; Villarino, R. Analysis of Vital Signs Monitoring Using an IR-UWB Radar. Prog. Electromagn. Res. 2010, 100, 265–284. [Google Scholar] [CrossRef] [Green Version]
- Pisa, S.; Pittella, E.; Piuzzi, E. A Survey of Radar Systems for Medical Applications. IEEE Aerosp. Electron. Syst. Mag. 2016, 31, 64–81. [Google Scholar] [CrossRef]
- Cardillo, E.; Caddemi, A. A Review on Biomedical MIMO Radars for Vital Sign Detection and Human Localization. Electronics 2020, 9, 1497. [Google Scholar] [CrossRef]
- Adib, F.; Mao, H.; Kabelac, Z.; Katabi, D.; Miller, R.C. Smart Homes That Monitor Breathing and Heart Rate. In Proceedings of the 33rd Annual ACM Conference on Human Factors in Computing Systems-CHI ’15; ACM Press: Seoul, Korea, 2015; pp. 837–846. [Google Scholar] [CrossRef]
- Ha, U.; Assana, S.; Adib, F. Contactless Seismocardiography via Deep Learning Radars. In Proceedings of the 26th Annual International Conference on Mobile Computing and Networking; ACM: London, UK, 2020; pp. 1–14. [Google Scholar] [CrossRef]
- Xia, Z.; Shandhi, M.M.H.; Li, Y.; Inan, O.; Zhang, Y. The Delineation of Fiducial Points for Non-Contact Radar Seismocardiogram Signals without Concurrent ECG. IEEE J. Biomed. Health Inform. 2020, 1031–1040. [Google Scholar] [CrossRef] [PubMed]
- Xia, Z.; Shandhi, M.M.H.; Inan, O.T.; Zhang, Y. Non-Contact Sensing of Seismocardiogram Signals Using Microwave Doppler Radar. IEEE Sensors J. 2018, 18, 5956–5964. [Google Scholar] [CrossRef]
- Wang, D.; Yoo, S.; Cho, S.H. Experimental Comparison of IR-UWB Radar and FMCW Radar for Vital Signs. Sensors 2020, 20, 6695. [Google Scholar] [CrossRef] [PubMed]
- Islam, S.M.M.; Yavari, E.; Rahman, A.; Lubecke, V.M.; Boric-Lubecke, O. Separation of Respiratory Signatures for Multiple Subjects Using Independent Component Analysis with the JADE Algorithm. In Proceedings of the 2018 40th Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC), Honolulu, HI, USA, 18–21 July 2018; pp. 1234–1237. [Google Scholar] [CrossRef]
- Ding, C.; Yan, J.; Zhang, L.; Zhao, H.; Hong, H.; Zhu, X. Noncontact Multiple Targets Vital Sign Detection Based on VMD Algorithm. In Proceedings of the 2017 IEEE Radar Conference (RadarConf), Seattle, WA, USA, 8–12 May 2017; pp. 727–730. [Google Scholar] [CrossRef]
- Rong, Y.; Bliss, D.W. Harmonics-Based Multiple Heartbeat Detection at Equal Distance Using UWB Impulse Radar. In Proceedings of the 2018 IEEE Radar Conference (RadarConf18), Oklahoma City, OK, USA, 23–27 April 2018; pp. 1101–1105. [Google Scholar] [CrossRef]
- Singh, A.; Rehman, S.U.; Yongchareon, S.; Chong, P.H.J. Multi-Resident Non-Contact Vital Sign Monitoring Using Radar: A Review. IEEE Sensors J. 2021, 21, 4061–4084. [Google Scholar] [CrossRef]
- Lee, H.; Kim, B.H.; Park, J.K.; Yook, J.G. A Novel Vital-Sign Sensing Algorithm for Multiple Subjects Based on 24-GHz FMCW Doppler Radar. Remote Sens. 2019, 11, 1237. [Google Scholar] [CrossRef] [Green Version]
- Yang, Y.; Cao, J.; Liu, X.; Liu, X. Multi-Breath: Separate Respiration Monitoring for Multiple Persons with UWB Radar. In Proceedings of the 2019 IEEE 43rd Annual Computer Software and Applications Conference (COMPSAC), Milwaukee, WI, USA, 15–19 July 2019; pp. 840–849. [Google Scholar] [CrossRef]
- Mercuri, M.; Lorato, I.R.; Liu, Y.H.; Wieringa, F.; Hoof, C.V.; Torfs, T. Vital-Sign Monitoring and Spatial Tracking of Multiple People Using a Contactless Radar-Based Sensor. Nat. Electron. 2019, 2, 252–262. [Google Scholar] [CrossRef]
- Xiong, J.; Hong, H.; Zhang, H.; Wang, N.; Chu, H.; Zhu, X. Multitarget Respiration Detection With Adaptive Digital Beamforming Technique Based on SIMO Radar. IEEE Trans. Microw. Theory Tech. 2020, 68, 4814–4824. [Google Scholar] [CrossRef]
- Shang, X.; Liu, J.; Li, J. Multiple Object Localization and Vital Sign Monitoring Using IR-UWB MIMO Radar. IEEE Trans. Aerosp. Electron. Syst. 2020, 56, 4437–4450. [Google Scholar] [CrossRef]
- Walterscheid, I.; Biallawons, O.; Berens, P. Contactless Respiration and Heartbeat Monitoring of Multiple People Using a 2-D Imaging Radar. In Proceedings of the 2019 41st Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC), Berlin, Germany, 23–27 July 2019; pp. 3720–3725. [Google Scholar] [CrossRef]
- Wang, S.; Kueppers, S.; Cetinkaya, H.; Herschel, R. 3D Localization and Vital Sign Detection of Human Subjects with a 120 GHz MIMO Radar. In Proceedings of the 2019 20th International Radar Symposium (IRS), Ulm, Germany, 26–28 June 2019; pp. 1–6. [Google Scholar] [CrossRef]
- Yang, Y.; Fathy, A. See-Through-Wall Imaging Using Ultra Wideband Short-Pulse Radar System. In Proceedings of the 2005 IEEE Antennas and Propagation Society International Symposium, Washington, DC, USA, 3–8 July 2005; Volume 3B, pp. 334–337. [Google Scholar] [CrossRef]
- Liu, L.; Liu, S. Remote Detection of Human Vital Sign With Stepped-Frequency Continuous Wave Radar. IEEE J. Sel. Top. Appl. Earth Obs. Remote Sens. 2014, 7, 775–782. [Google Scholar] [CrossRef]
- Tan, K.; Wu, S.; Chen, J.; Xia, Z.; Guangyou, F.; Meng, S. Improved Human Respiration Detection Method via Ultra-Wideband Radar in through-Wall or Other Similar Conditions. IET Radar Sonar Navig. 2016, 10, 468–476. [Google Scholar] [CrossRef]
- Liang, X.; Deng, J.; Zhang, H.; Gulliver, T.A. Ultra-Wideband Impulse Radar Through-Wall Detection of Vital Signs. Sci. Rep. 2018, 8, 13367. [Google Scholar] [CrossRef] [Green Version]
- Jia, Y.; Guo, Y.; Yan, C.; Sheng, H.; Cui, G.; Zhong, X. Detection and Localization for Multiple Stationary Human Targets Based on Cross-Correlation of Dual-Station SFCW Radars. Remote Sens. 2019, 11, 1428. [Google Scholar] [CrossRef] [Green Version]
- Harikesh.; Chauhan, S.S.; Basu, A.; Abegaonkar, M.P.; Koul, S.K. Through the Wall Human Subject Localization and Respiration Rate Detection Using Multichannel Doppler Radar. IEEE Sensors J. 2020, 21, 1510–1518. [Google Scholar] [CrossRef]
- Antolinos, E.; García-Rial, F.; Hernández, C.; Montesano, D.; Godino-Llorente, J.I.; Grajal, J. Cardiopulmonary Activity Monitoring Using Millimeter Wave Radars. Remote Sens. 2020, 12, 2265. [Google Scholar] [CrossRef]
- Ren, L.; Wang, H.; Naishadham, K.; Kilic, O.; Fathy, A.E. Phase-Based Methods for Heart Rate Detection Using UWB Impulse Doppler Radar. IEEE Trans. Microw. Theory Tech. 2016, 64, 3319–3331. [Google Scholar] [CrossRef]
- Wu, T.; Rappaport, T.S.; Collins, C.M. The Human Body and Millimeter-Wave Wireless Communication Systems: Interactions and Implications. In Proceedings of the 2015 IEEE International Conference on Communications (ICC), London, UK, 8–12 June 2015; pp. 2423–2429. [Google Scholar] [CrossRef] [Green Version]
- De Groote, A.; Wantier, M.; Cheron, G.; Estenne, M.; Paiva, M. Chest Wall Motion during Tidal Breathing. J. Appl. Physiol. 1997, 83, 1531–1537. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ramachandran, G.; Singh, M. Three-Dimensional Reconstruction of Cardiac Displacement Patterns on the Chest Wall during the P, QRS and T-Segments of the ECG by Laser Speckle Inteferometry. Med Biol. Eng. Comput. 1989, 27, 525–530. [Google Scholar] [CrossRef]
- Wang, J.; Wang, X.; Chen, L.; Huangfu, J.; Li, C.; Ran, L. Noncontact Distance and Amplitude-Independent Vibration Measurement Based on an Extended DACM Algorithm. IEEE Trans. Instrum. Meas. 2014, 63, 145–153. [Google Scholar] [CrossRef]
- Ferris, D.D.; Currie, N.C. Microwave and Millimeter-Wave Systems for Wall Penetration. In Proceedings of the Aerospace/Defense Sensing and Controls, Orlando, FL, USA, 7 July 1998; pp. 269–279. [Google Scholar]
- Shanhong, G.; Jintao, S.; Renhong, X.; Yibin, R.; Peng, L. Attenuation Characteristics of Electromagnetic Wave Penetrating Walls. High Power Laser Part. Beams 2009, 21, 113–117. [Google Scholar]
- Jin, T.; Chen, B.; Zhou, Z. Image-Domain Estimation of Wall Parameters for Autofocusing of Through-the-Wall SAR Imagery. IEEE Trans. Geosci. Remote Sens. 2013, 51, 8. [Google Scholar] [CrossRef]
- Mendel, J. Tutorial on Higher-Order Statistics (Spectra) in Signal Processing and System Theory: Theoretical Results and Some Applications. Proc. IEEE 1991, 79, 278–305. [Google Scholar] [CrossRef]
- Khan, F.; Cho, S. A Detailed Algorithm for Vital Sign Monitoring of a Stationary/Non-Stationary Human through IR-UWB Radar. Sensors 2017, 17, 290. [Google Scholar] [CrossRef] [Green Version]
- Yang, S.; Qin, H.; Liang, X.; Gulliver, T. Clutter Elimination and Harmonic Suppression of Non-Stationary Life Signs for Long-Range and Through-Wall Human Subject Detection Using Spectral Kurtosis Analysis (SKA)-Based Windowed Fourier Transform (WFT) Method. Appl. Sci. 2019, 9, 355. [Google Scholar] [CrossRef] [Green Version]
- Liang, F.; Qi, F.; An, Q.; Lv, H.; Chen, F.; Li, Z.; Wang, J. Detection of Multiple Stationary Humans Using UWB MIMO Radar. Sensors 2016, 16, 1922. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dragomiretskiy, K.; Zosso, D. Variational Mode Decomposition. IEEE Trans. Signal Process. 2014, 62, 531–544. [Google Scholar] [CrossRef]
- Xu, Y.; Dai, S.; Wu, S.; Chen, J.; Fang, G. Vital Sign Detection Method Based on Multiple Higher Order Cumulant for Ultrawideband Radar. IEEE Trans. Geosci. Remote Sens. 2012, 50, 1254–1265. [Google Scholar] [CrossRef]
- Torres, M.E.; Colominas, M.A.; Schlotthauer, G.; Flandrin, P. A Complete Ensemble Empirical Mode Decomposition with Adaptive Noise. In Proceedings of the 2011 IEEE International Conference on Acoustics, Speech and Signal Processing (ICASSP), Prague, Czech Republic, 22–27 May 2011; pp. 4144–4147. [Google Scholar] [CrossRef]
- Sun, L.; Huang, S.; Li, Y.; Gu, C.; Pan, H.; Hong, H.; Zhu, X. Remote Measurement of Human Vital Signs Based on Joint-Range Adaptive EEMD. IEEE Access 2020, 8, 68514–68524. [Google Scholar] [CrossRef]
- Xiong, Y.; Peng, Z.; Gu, C.; Li, S.; Wang, D.; Zhang, W. Differential Enhancement Method for Robust and Accurate Heart Rate Monitoring via Microwave Vital Sign Sensing. IEEE Trans. Instrum. Meas. 2020, 69, 7108–7118. [Google Scholar] [CrossRef]
- Oyamada, Y.; Koshisaka, T.; Sakamoto, T. Experimental Demonstration of Accurate Noncontact Measurement of Arterial Pulse Wave Displacements Using 79-GHz Array Radar. IEEE Sensors J. 2021, 21, 9128–9137. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Configuration | Waveform | Frequency (GHz) | No. of Subjects | Detection Range (m) | Through-Wall | Measured Parameters |
|---|---|---|---|---|---|---|
| SISO [8] | CW | 24.17 | 1 | 0.2 | - | Breathing and heart sound waveforms |
| SISO [14] | CW | 5.8 | 1 | 0.5 | - | Heart sound waveforms and HR |
| SISO [35] | IR-UWB | 1.5–4.5 | 1 | 0.8 | - | RR and HR |
| SISO [19] | IR-UWB | 6.54–8.04 | 2 | 2 | - | RR and HR |
| SISO [31] | IR-UWB | 0.4 | 1 | 3–12 | Yes | Range detection, RR and HR |
| SISO [12] | FMCW | 5.46–7.25 | 3 | 1–8 | Yes | RR and HR |
| SISO [21] | FMCW | 24–24.25 | 2 | 1.3–3 | - | Range detection, RR and HR |
| SISO [23] | FMCW | 7.3–8.05 | 2 | 2.6–5.4 | - | Range detection, RR and HR |
| SISO [34] | FMCW | 114–130 | 2 | 1.2–1.6 | - | Range detection, respiration pattern, heartbeat pattern, RR and HR |
| SIMO (1T × 8R) [24] | CW | 5.8 | 3 | 2 | - | Angle detection, respiration waveform and RR |
| SIMO (1T × 4R) [33] | CW | 2.49 | 2 | 1.68–1.87 | Yes | Angle detection, respiration waveform and RR |
| MIMO (2T × 2R) [25] | IR-UWB | 0.7–7 | 2 | 0.4–1.5 | - | 2-D Localization, RR and HR |
| MIMO (2T × 8R) [27] | FMCW | 115–123 | 2 | 1.8–2.3 | - | 3-D Localization, RR and HR |
| MIMO (10T × 10R) [This work] | SFCW | 1.75–2.25 | 3 | 2.0–2.5 | Yes | 3-D Localization, respiration pattern, heartbeat pattern, RR and HR |
| Parameters | Value |
|---|---|
| transmitting wave mode | SFCW |
| center frequency | 2 |
| bandwidth | 500 |
| frequency step | 4 |
| power of transmitted signal | 20 dBm |
| frame rate | 20 |
| antenna element number | 10 Tx, 10 Rx |
| array size | |
| antenna element gain | 5dB–6dB |
| beam width of each antenna element ( 3 dB) |
| Truth (m) | Estimation (m) | Error (m) | ||
|---|---|---|---|---|
| Line-of-sight | Subj. 1 | (−0.50, 2.50, −0.10) | (−0.44, 2.51, −0.26) | (0.06, 0.01, −0.16) |
| Subj. 2 | (0, 2.50, −0.06) | (0.06, 2.51, 0.05) | (0.06, 0.01, 0.11) | |
| Subj. 3 | (0.50, 2.50, 0.05) | (0.69, 2.52, 0.16) | (0.19, 0.02, 0.11) | |
| Through-wall | Subj. 1 | (−0.3, 2.00, −0.10) | (−0.19, 1.88, −0.26) | (0.11, −0.12, −0.16) |
| Subj. 2 | (0.50, 2.00, −0.06) | (0.44, 2.06, 0.16) | (−0.06, 0.06, 0.22) | |
| Subj. 3 | (1.00, 2.00, 0.05) | (1.07, 1.97, −0.16) | (0.07, −0.03, −0.21) | |
| Subject | RMSE (bpm) | |||
|---|---|---|---|---|
| RR without Wall | RR with Wall | HR without Wall | HR with Wall | |
| Subj. 1 | 0.8565 | 1.1757 | 2.2209 | 3.5461 |
| Subj. 2 | 0.7058 | 1.2485 | 2.8609 | 4.0297 |
| Subj. 3 | 0.9571 | 1.2701 | 2.8079 | 3.4779 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Li, Z.; Jin, T.; Dai, Y.; Song, Y. Through-Wall Multi-Subject Localization and Vital Signs Monitoring Using UWB MIMO Imaging Radar. Remote Sens. 2021, 13, 2905. https://doi.org/10.3390/rs13152905
Li Z, Jin T, Dai Y, Song Y. Through-Wall Multi-Subject Localization and Vital Signs Monitoring Using UWB MIMO Imaging Radar. Remote Sensing. 2021; 13(15):2905. https://doi.org/10.3390/rs13152905
Chicago/Turabian StyleLi, Zhi, Tian Jin, Yongpeng Dai, and Yongkun Song. 2021. "Through-Wall Multi-Subject Localization and Vital Signs Monitoring Using UWB MIMO Imaging Radar" Remote Sensing 13, no. 15: 2905. https://doi.org/10.3390/rs13152905
APA StyleLi, Z., Jin, T., Dai, Y., & Song, Y. (2021). Through-Wall Multi-Subject Localization and Vital Signs Monitoring Using UWB MIMO Imaging Radar. Remote Sensing, 13(15), 2905. https://doi.org/10.3390/rs13152905