A 43-year-old male underwent implantable cardioverter defibrillator (ICD) insertion, 8 months after an out-of-hospital cardiac arrest following acute ST segment-elevation myocardial infarction. Following the cardiac arrest, he was treated with primary percutaneous coronary intervention (PCI) to his left anterior descending coronary artery and subsequent PCI to his posterior descending artery. He had a chronic total occlusion of the posterolateral branch of the right coronary artery that could not be crossed. With partial percutaneous revascularisation, his left ventricular function improved. However, episodes of non-sustained ventricular tachycardia were noticed on 24-hour Holter monitoring, and he underwent ICD insertion. Of note, he had never previously had a pacemaker or ICD inserted.
Access was gained to the left subclavian vein without difficulty. After injection of contrast, it was thought that the patient might have a congenital absence of the left innominate vein, and that a large collateral vessel had formed from the left subclavian vein to the right internal jugular vein. A right ventricular defibrillation lead (Boston Scientific, Model 0593, 64-cm active fixation) was passed through this collateral and through the right subclavian vein into the superior vena cava and connected to a single chamber ICD lead (Boston Scientific Resonate EL D432) (Figure 1).
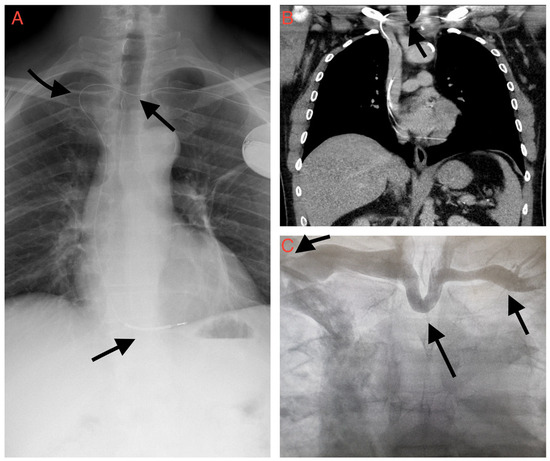
Figure 1.
(A) Chest radiograph after the procedure showing the ICD lead traversing the midline collateral vein anomaly (arrow) from left subclavian vein to right internal jugular and down the right brachiocephalic (arrow) into the superior vena cava with the lead in the right ventricle (arrow). (B) Computerised tomography of the thorax showing the ICD lead traversing the venous anomaly (arrow). (C) Fluorographic intra-procedural imaging showing abnormal venous anatomy. Previously undiagnosed left brachiocephalic vein obstruction, with large anterior collateral between left subclavian vein (arrow) and right internal jugular vein (arrow).
Computerised tomography of the thorax demonstrated a chronic left brachiocephalic vein obstruction (Figure 1). A large anterior jugular venous collateral had formed as a result of longstanding obstruction. The scan showed the ICD lead traversing this anomalous vein from left to right.
On literature review, we found numerous instances of subclavian vein stenosis, mainly in cases with history of previous pacemaker/ICD insertions or central venous access for dialysis. We did not find any prior reports of complete venous occlusion with in a vessel that had not been used as access for previous percutaneous procedures.
Conflicts of Interest
The authors of this paper do not declare any conflict of interest.
© 2022 by the author. Attribution - Non-Commercial - NoDerivatives 4.0.