Abstract
Background: The aim of the present study is to report a rare occurrence of a successful twin pregnancy in a woman with pure 46,XY gonadal dysgenesis. Result(s): A patient with Swyer syndrome (pure 46,XY gonadal dysgenesis) presented with a twin pregnancy after in vitro fertilization. Due to unidentified conditions, the patient developed selective intrauterine growth restriction in one of the fetuses. Twins were born at 33 weeks of pregnancy due to the risk of asphyxia. Nonetheless, the patient did not develop gonadal malignancies before the pregnancy and, despite receiving estrogen, remained amenorrheic. Conclusion(s): The aim of this case report is to show the course of twin pregnancy in patients with Swyer syndrome through assisted reproduction. Due to certain disorders in the development of their reproductive organs, such as the less mature uterus, such pregnancies may be associated with an increased risk. The above case report demonstrates the need to systematize methods of pregnancy management in patients with Swyer syndrome, such as: preparation for the pregnancy, assessment of the uterus, medications used, and necessary checkups. Capsule: This case report and review shows clinicians that patients with Swyer syndrome may become pregnant. Twin pregnancies may occur without any major problems through assisted reproduction.
1. Introduction
Swyer syndrome, also known as 46,XY pure gonadal dysgenesis, is a rare condition that affects sexual development. It was described by Swyer in 1955 [1]. It is classified as a disorder of sex development (DSD), or a situation in which chromosomal, gonadal or anatomic sex development is abnormal. It occurs in approximately 1 in 80,000 people depending on the described population. Patients with Swyer syndrome present with typical female external genitalia. The uterus and fallopian tubes of such patients may be smaller or normally formed, but the gonads are not functional. Instead of sex glands, women with Swyer syndrome present with gonadal streaks, i.e., the ovaries are replaced by a form of fibrous tissue [2]. Between 10% and 20% of women with Swyer syndrome have a deletion in the DNA-binding region of the SRY gene, while in the remaining 80–90% of cases, the SRY gene is normal, and mutations in other testis-determining factors (MAP3K1, DHH, NR5A1) are present [3].
2. A Case Report
In this manuscript, we want to present the case of a dichorionic diamniotic twin pregnancy that occurred in a patient with Swyer syndrome who was treated with assisted reproductive techniques.
The described patient was diagnosed with Swyer syndrome at 15 years of age due to primary amenorrhea [4]. Following diagnosis by karyotype, she underwent removal of the streak gonads to minimalize the risk of malignancy in the future. The patient presented with a female phenotype, external genitalia, and female hair on her body and in the genital area. During the periconception period, the patient’s body mass index (BMI) was 29.37 kg/m2. She was 177 cm tall and weighed 97 kg. Her breast development was also normal. A pelvic ultrasound examination revealed a uterus with a longitudinal diameter of 60 mm, anteroposterior diameter of 35 mm, and transverse diameter of 39 mm. The patient had been using hormone replacement therapy (HRT) since the age of 18 and had regular cycles. Most of the time, until the age of 38, she had been using 2 mg of estradiol with 0.5 mg of norgestrel. The patient also presented with hypothyroidism, and she took oral levothyroxine 50 mcg daily. A detailed description of the drugs used during pregnancy can be found in Table 1.

Table 1.
Pharmacotherapy in the presented case.
Moreover, the hypoplastic uterus in patients with Swyer syndrome may be able to sustain pregnancy. One year before starting the donor egg procedure, the abovementioned HRT was changed to 1.5 mg of estradiol with 2.5 mg of nomegestrol. The patient underwent an office hysteroscopy in order to assess the shape and condition of the endometrial cavity (Figure 1). The histopathological samples at the time of the hysteroscopy were characterized by an atrophic endometrium. After the hysteroscopy, the patient was referred to the ART center, where the egg donor procedure was performed.
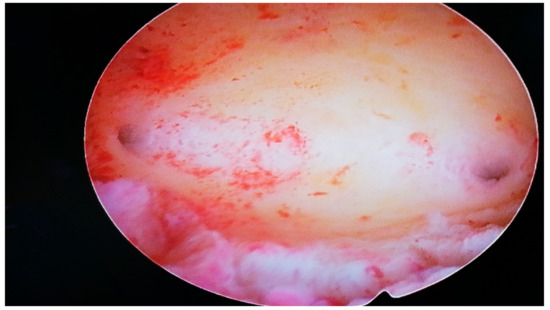
Figure 1.
Mini-hysteroscopy view in the patient with Swyer syndrome.
The patient received 150 mg of acetylsalicylic acid daily to decrease the risk of pre-eclampsia. Her blood pressure was normal (below 140/90 mmHg) throughout the pregnancy. Moreover, the patient used estrogens and progesterone intravaginally and orally (we have provided the exact hormonal treatment scheme during each trimester in Table 1). We checked her liver parameters each month due to several risk factors associated with pre-eclampsia. Liver enzymes (AST aspartate aminotransferase and ALT alanine aminotransferase) were elevated to approximately 60 UL/l at weeks 26/27 of pregnancy. Therefore, we decreased the dose of hormones. In addition, the patient used prednisone 5 mg orally per day.
During the first and second trimesters, the twins developed normally. Around 28 weeks of pregnancy, the discrepancy between the estimated fetal weight equaled 18.6%, but during weeks 31/32, it rose to 27.1%. At 32 weeks and 5 days, the dichorionic diamniotic (Figure 2) twin pregnancy was hospitalized due to suspected selective intrauterine growth restriction (sIUGR) in one of the fetuses. This was a diagnostic stay in a tertiary center that is experienced in the management of twin pregnancies. The stay in the hospital made it possible to coordinate specialist consultations and perform reference ultrasound examinations. An ultrasound scan and fetal biometry were performed. Fetal well-being was assessed with an ultrasound Doppler examination of the middle cerebral artery (MCA) and umbilical artery (UA). The cerebroplacental ratio (CPR) and amniotic fluid index (AFI) were calculated (see Table 2 and Table 3). Both fetuses were in a transverse position, with details presented in Figure 3 and Figure 4. The abovementioned scan revealed a growth disturbance in one of the fetuses, and type 1 sIUGR was confirmed. A CTG recording showed deep, prolonged late deceleration in both fetuses (heart rate <80 beats/minute, lasting 7 minutes). The deceleration resolved after an intravenous injection of 25 μg of fenoterol. According to the FIGO consensus guidelines on intrapartum fetal monitoring, the risk of asphyxia was diagnosed, and the patients qualified for an emergency caesarean section (Figure 5) FIGO consensus guidelines on intrapartum fetal monitoring: Cardiotocography, 2015 [5] A female (1800 g, length 42 cm) and a male (2040 g, length 46 cm) neonate were born. The puerperium was uneventful. The patient breastfed for 4 weeks.

Figure 2.
USG scan of twin pregnancy (dichorionic diamniotic—7 week of pregnancy) in patient with Swyer syndrome.
Table 2.
First trimester scan.
Table 3.
Ultrasound growth patterns in the second and third trimesters.
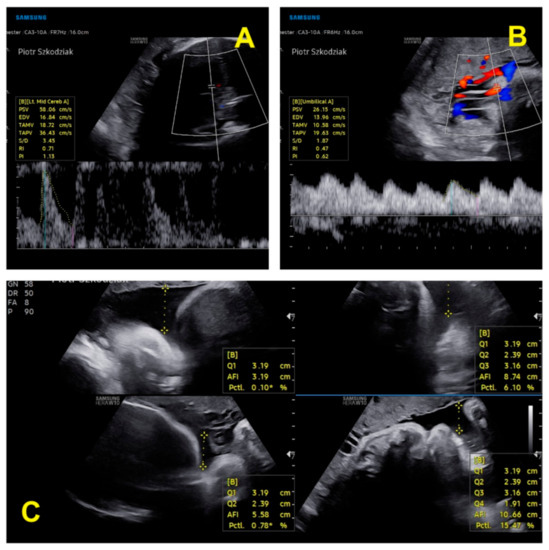
Figure 3.
Ultrasound parameters of the first twin’s well-being: (A) assessment of blood flow in the MCA; (B) assessment of blood flow in the UA; (C) amniotic fluid index [6,7].
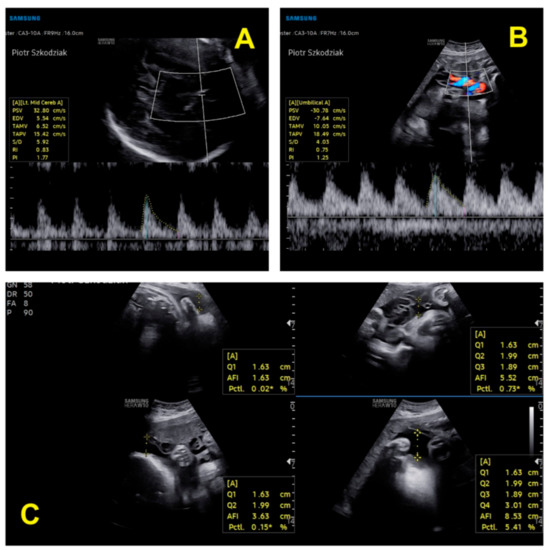
Figure 4.
Ultrasound parameters of the second twin’s well-being: (A) assessment of blood flow in the MCA; (B) assessment of blood flow in the UA; (C) amniotic fluid index [6,7].

Figure 5.
CTG recordings showed prolonged deceleration of both twins, lasting 7 minutes, and a decrease in the heart rate of both fetuses to 80 beats/minute (FIGO consensus guidelines on intrapartum fetal monitoring: Cardiotocography, 2015).
3. Discussion
Swyer syndrome is still infrequent. The phenotype of patients with Swyer syndrome is female, but the genotype is male. The external genitalia are normal. Moreover, the vagina is normal, but the uterus is usually hypoplastic, and the gonads are dysgenetic. The most common and documented symptom of Swyer syndrome is primary amenorrhea. Treatment of Swyer syndrome requires estrogen therapy to induce puberty and long-term combined replacement therapy [8,9,10,11,12,13,14,15]. One of the main clinical problems in women with Swyer syndrome is related to reproductive health issues. Patients with Swyer syndrome rarely become pregnant, and twin pregnancies are especially rare. As the gonads of patients with Swyer syndrome are not functional, they are infertile. However, with the use of assisted reproductive techniques and proper preparation of the uterus, patients may become pregnant via egg donation and in vitro fertilization [16].
Each feature of our patient was in accordance with the respective descriptions in the literature. A well-chosen HRT is necessary for the patient to develop normal sex characteristics and to prepare the patient to seek reproduction. Before the egg donation procedure, we recommended a mini-hysteroscopy to ensure that the shape and size of the uterine cavity was correct.
As described in the available literature, patients with Swyer syndrome present with an increased risk of gonadal cancer (gonadoblastoma), which could be a precursor of dysgerminoma. The risk is estimated at about 30% [16]. Therefore, prophylactic removal of the dysgenetic gonads is recommended [8,9,10]. The timing depends on the age at diagnosis [11], but gonadal tumors may develop at any age, including during childhood. HRT therapy must be introduced after the removal of the gonads. Dural et al. [14] described the possibility of a diagnosis of Swyer syndrome in the presence of normal pubertal development and normal sex steroid levels, which is considered to be produced by gonadoblastoma [14]. The side effects of ovary removal mostly include osteoporosis and hypoestrogenism. HRT promotes the development of breasts, regulates menstrual cycles, and prevents uterine hypoplasia.
Women with Swyer syndrome present with a hypoplastic uterus. Pregnancy might be achieved using hormone therapy and assisted reproduction techniques with egg donation. The studies conducted by Van der Hoorn et al., 2010, and Savasi et al., 2016, showed that oocyte donation (OD) pregnancies were at an increased risk of obstetric complications, especially pre-eclampsia (PE) [17,18].
Specific complications, such as hypertension, pre-eclampsia, and proteinuria, may be associated with pregnancies in Swyer syndrome. Taneja et al. [19], Sauer et al. [20], Kan et al. [21], Ko et al. [22], and Michala et al. [2] reported gestational hypertension and/or pre-eclampsia (see Table 4). Case reports published by Tulic et al. [23] and Cretsas et al. [24] described patients with oligohydramnios. Cases reported by Selvaraj et al. [25], Lutjen et al. [26], Cornet et al. [27], Dirnfeld et al. [28], Plante and Fritz [29], and Chen et al. [15] did not develop any complications during pregnancy. Further information on the remaining cases reported by Bardeguez et al. [30] and Bianco et al. [31] was not included. Obesity, maternal age (40 years old), and in vitro fertilization procedure constituted additional risk factors in our patient. To the best of our knowledge, we present the first case of a successful pregnancy achieved in a patient with Swyer syndrome with intrauterine growth restriction in one of the fetuses. Cesarean section was the mode of delivery in the predominant number of cases [32,33,34,35,36,37,38]. Only three patients delivered vaginally, i.e., two cases reported by Michala et al. [2] and one case by Kan et al. [21]. The vast majority of patients delivered a baby at term, between 37 and 41 weeks of pregnancy. Patients described by Sauer et al. [20], Kan et al. [21], Ko et al. [22], and Michala et al. [2], as well as our patient, delivered preterm neonates before 37 weeks of pregnancy. Most cases of Swyer syndrome are sporadic, but some familial cases have also been described [39]. Gupta et al. [39] described two sisters who presented with primary infertility and conceived following in vitro fertilization (IVF) with ovum donation. The results of pregnancies in patients with Swyer syndrome are reviewed in Table 4.
Table 4.
Cases of pregnancies in patients with Swyer syndrome.
Despite the available descriptions, a model of care for pregnant patients with Swyer syndrome has not been developed yet. Furthermore, all the descriptions are rather empirical. In our opinion, one must establish patterns, thereby facilitating the management of such patients in order to avoid pregnancy complications as much as possible.
4. Conclusions
The treatment of Swyer syndrome requires a multidisciplinary approach. The prophylaxis of malignancy, osteoporosis, induction of puberty, fertility, and psychological support are important aspects of patients’ lives. The aim of this case report and review is to show clinicians that patients with Swyer syndrome may become pregnant without any major problems through assisted reproduction. Due to certain abnormalities in organ development, i.e., a less mature uterus, such cases may be higher-risk pregnancies. The above case report indicates the need to systematize methods of pregnancy management in patients with Swyer syndrome.
Author Contributions
I.W. is responsible for the conception and study design, acquisition and interpretation of data, writing the manuscript, performing the hysteroscopy, and preparation of tables; I.J. is responsible for writing the manuscript; K.S. is responsible for writing the manuscript; M.S., M.C. and M.G. are responsible for the collection of data and giving final approval of the version to be published; P.S. and T.P. are responsible for writing the manuscript, giving final approval of the version to be published, and performing the USG scan. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Bioethics Committee of the Medical University of Lublin (KE-0254/170/2021 and date of approval was 24 June 2021) for studies involving humans.
Informed Consent Statement
The patient provided written informed consent to participate in the study. Informed consent was obtained from all subjects involved in the study. Written informed consent has been obtained from the patient(s) to publish this paper.
Data Availability Statement
The datasets used and/or analyzed in the current study are available from the corresponding author on reasonable request.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Swyer, G.I. Male pseudohermaphroditism: A hitherto undescribed form. Br. Med. J. 1955, 2, 709–712. [Google Scholar] [CrossRef] [Green Version]
- Michala, L.; Goswami, D.; Creighton, S.; Conway, G. Swyer syndrome: Presentation and outcomes. BJOG Int. J. Obstet. Gynaecol. 2008, 115, 737–741. [Google Scholar] [CrossRef] [PubMed]
- Jager, R.J.; Anvret, M.; Hall, K.; Scherer, G. A human XY female with a frame shift mutation in the candidate testis-determining gene SRY. Nature 1990, 348, 452–454. [Google Scholar] [CrossRef] [PubMed]
- Available online: https://www.uptodate.com/contents/causes-of-primary-amenorrhea (accessed on 21 October 2021).
- Ayres-de-Campos, D.; Spong, C.Y.; Chandraharan, E. FIGO consensus guidelines on intrapartum fetal monitoring: Cardiotocography. Int. J. Gynecol. Obstet. 2015, 131, 13–24. [Google Scholar] [CrossRef] [Green Version]
- Nicolaides, K.H.; Wright, D.; Syngelaki, A.; Wright, A.; Akolekar, R. Fetal Medicine Foundation fetal and neonatal population weight charts. Ultrasound. Obstet. Gynecol. 2021, 52, 44–51. [Google Scholar] [CrossRef] [Green Version]
- Fetal Medicine Foundation. The Fetal Medicine Foundation. Accredit 11-13+6 Week Scan. 2010. Available online: https://fetalmedicine.org/research/assess/growth (accessed on 21 October 2021).
- Arboleda, V.A.; Sandberg, D.E.; Vilain, E. DSDs: Genetics, underlying pathologies and psychosexual differentiation. Nat. Rev. Endocrinol. 2014, 10, 603–615. [Google Scholar] [CrossRef] [PubMed]
- Wünsch, L.; Holterhus, P.M.; Wessel, L.; Hiort, O. Patients with disorders of sex development (DSD) at risk of gonadal tumour development: Management based on laparoscopic biopsy and molecular diagnosis. BJU Int. 2012, 110, E958–E965. [Google Scholar] [CrossRef]
- Rocha, V.B.; Guerra-Júnior, G.; Marques-de-Faria, A.P.; de Mello, M.P.; Maciel-Guerra, A.T. Complete gonadal dysgenesis in clinical practice: The 46,XY karyotype accounts for more than one third of cases. Fertil. Steril. 2011, 96, 1431–1434. [Google Scholar] [CrossRef]
- Huang, H.; Wang, C.; Tian, Q. Gonadal tumour risk in 292 phenotypic female patients with disorders of sex development containing Y chromosome or Y-derived sequence. Clin. Endocrinol. 2017, 86, 621–627. [Google Scholar] [CrossRef]
- Massanyi, E.Z.; Dicarlo, H.N.; Migeon, C.J.; Gearhart, J.P. Review and management of 46,XY disorders of sex development. J. Pediatr. Urol. 2013, 9, 368–379. [Google Scholar] [CrossRef]
- Available online: https://www.eshre.eu/-/media/sitecore-files/Guidelines/POI/ESHRE-guideline_POI-2015_summary_01122015.pdf?la=en&hash=04AFBA15E89FAAD0D81BB41DD64403BE6B04678E (accessed on 21 October 2021).
- Dural, O.; Evruke, I.; Can, S.; Yasa, C.; Ugurlucan, F.G.; Akhan, S.E. Atypical Presentation of Swyer Syndrome. J. Pediatr. Adolesc. Gynecol. 2019, 32, 645–647. [Google Scholar] [CrossRef] [PubMed]
- Coutin, A.S.; Hamy, A.; Fondevilla, M.; Sauvigny, B.; Paineau, J.; Visset, J. La dysgenesie gonadidique pure a 46 XY. J. Gynecol. Obstet. Biol. Reprod. 1996, 25, 792–796. [Google Scholar]
- Chen, M.J.; Yang, J.H.; Mao, T.L.; Ho, H.N.; Yang, Y.S. Successful pregnancy in a gonadectomised woman with 46, XY gonadal dysgenesis and gonadoblastoma. Fertil. Steril. 2005, 84, 217. [Google Scholar] [CrossRef] [PubMed]
- Van Der Hoorn, M.L.; Lashley, E.E.; Bianchi, D.W.; Claas, F.H.; Schonkeren, C.M.; Scherjon, S.A. Clinicaland immunologic aspects of oocyte donation pregnancies: A systematic review. Hum. Reprod. Update 2010, 16, 704–712. [Google Scholar] [CrossRef]
- Savasi, V.M.; Mandia, L.; Laoreti, A.; Cetin, I. Maternal and fetal outcomes in oocyte donation pregnancies. Hum. Reprod. Update 2016, 22, 620–633. [Google Scholar] [CrossRef]
- Taneja, J.; Ogutu, D.; Ah-Moye, M. Rare successful pregnancy in a patient with Swyer Syndrome. Case Rep. Women’s Health 2014, 12, 1–2. [Google Scholar] [CrossRef] [Green Version]
- Sauer, M.V.; Lobo, R.A.; Paulson, R.J. Successful twin pregnancy after embryo donation to a patient with XY gonadal dysgenesis. Am. J. Obstet. Gynecol. 1989, 161, 380–381. [Google Scholar] [CrossRef]
- Kan, A.K.; Abdalla, H.I.; Oskarsson, T. Two successful pregnancies in a 46, XY patient. Hum. Reprod. 1997, 12, 1434–1435. [Google Scholar] [CrossRef] [Green Version]
- Ko, P.C.; Peng, H.H.; Soong, Y.K.; Chang, S.D. Triplet pregnancy complicated with one hydatidiform mole and preeclampsia in a 46, XY female with gonadal dysgenesis. Taiwan J. Obstet. Gynecol. 2007, 46, 276–280. [Google Scholar] [CrossRef] [Green Version]
- Tulic, I.; Tulic, L.; Micic, J. Pregnancy in patient with Swyer syndrome. Fertil. Steril. 2011, 95, 1789. [Google Scholar] [CrossRef]
- Creatsas, G.; Deligeoroglou, E.; Tsimaris, P.; Pantos, K.; Kreatsa, M. Successful pregnancy in a Swyer syndrome patient with preexisting hypertension. Fertil. Steril. 2011, 96, e83–e85. [Google Scholar] [CrossRef]
- Selvaraj, K.; Ganesh, V.; Selvaraj, P. Successful pregnancy in a patient with a 46,XY karyotype. Fertil. Steril. 2002, 78, 419–420. [Google Scholar] [CrossRef]
- Lutjen, P.; Trounson, A.; Leeton, J.; Findlay, J.; Wood, C.; Renou, P. The establishment and maintenance of pregnancy using in vitro fertilization and embryo donation in a patient with primary ovarian failure. Nature 1984, 307, 174–175. [Google Scholar] [CrossRef]
- Cornet, D.; Alvarez, S.; Antoine, J.; Tibi, C.; Mandelbaum, J.; Plachot, M.; Salat-Baroux, J. Pregnancies following ovum donation in gonadal dysgenesis. Hum. Reprod. 1990, 5, 291–293. [Google Scholar] [CrossRef] [PubMed]
- Dirnfeld, M.; Bider, D.; Abramovicia, H.; Calderon, I.; Blumenfeld, Z. Subsequent successful pregnancy and delivery after intracytoplasmic sperm injection in a patient with XY gonadal dysgenesisms. Eur. J Obstet. Gynecol. Reprod. Biol. 2000, 88, 101–102.1789. [Google Scholar] [CrossRef]
- Plante, B.J.; Fritz, M.A. A case report of successful pregnancy in a patient with pure 46, XY gonadal dysgenesis. Fertil. Steril. 2008, 90, 2015.e1–2015.e2. [Google Scholar] [CrossRef]
- Bardeguez, A.D.; De Ziegler, D.; Weiss, G. Multifetal pregnancy in a gonadal dysgenesis mosaic. Obstet. Gynecol. 1990, 76, 502–504. [Google Scholar]
- Bianco, S.; Agrifoglio, V.; Mannino, F.; Cefalù, E.; Cittadini, E. Successful pregnancy in a pure gonadal dysgenesis with karyotype 46,XY patient (Swyer’s syndrome) following oocyte donation and hormonal treatment. Acta Eur. Fertil. 1992, 23, 37–38. [Google Scholar] [PubMed]
- Frydman, R.; Parneix, I.; Fries, N.; Testart, J.; Raymond, J.P.; Bouchard, P. Pregnancy in a 46, XY patient. Fertil. Steril. 1988, 50, 813–814. [Google Scholar] [CrossRef]
- De Santis, M.; Spagnuolo, T.; Barone, D.; Licameli, A. Successful twin pregnancy in a 46,XY pure gonadal dysgenesis. J. Obstet. Gynaecol. 2013, 33, 737–738. [Google Scholar] [CrossRef]
- Gao, S.S.; Sheng, Y.; Li, Y.; Li, M.; Yang, H.J.; Chen, Z.J. Twin delivery of a 46,XY gonadal dysgenetic woman following vitrified oocytes donation. Chin. Med. J. Engl. 2011, 124, 1109–1110. [Google Scholar] [PubMed]
- Murtinger, M.; Hradecký, L.; Spitzer, D.; Zech, N.H. Unexpected labor and successful twin birth to a pure gonadal dysgenetic woman. Arch. Gynecol. Obstet. 2013, 288, 1425–1426. [Google Scholar] [CrossRef] [PubMed]
- Kalra, A.; Nadkarni, P.K.; Singh, P.P.; Nadkarni, A.A. Successful pregnancy outcome in a case of Swyer Syndrome with hypertension and morbid obesity. Int. J. Reprod. Contracept. Obstet. Gynecol. 2016, 5, 2061–2064. [Google Scholar] [CrossRef]
- Shah, J.S.; Viteri, O.A.; Longo, M.; Abdallah, M.; Sibai, B. Twin gestation in a Swyer syndrome patient with superimposed pre-eclampsia. J. Obstet. Gynecol. 2018, 38, 719–720. [Google Scholar] [CrossRef] [PubMed]
- Urban, A.; Knap-Wielgus, W.; Grymowicz, M.; Smolarczyk, R. Two successful pregnancies after in vitro fertilisation with oocyte donation in a patient with Swyer syndrome—A case report. Prz. Menopauzalny 2021, 20, 158–161. [Google Scholar] [CrossRef] [PubMed]
- Gupta, A.; Bajaj, R.; Jindal, U.N. A rare case of Swyer syndrome in two sisters with successful pregnancy outcome in both. J. Hum. Reprod. Sci. 2019, 12, 267–269. [Google Scholar] [PubMed]
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).