
Service User and Carer Views and Expectations of Mental Health Nurses: A Systematic Review

 , , ,
, , ,  and
and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Eligibility Criteria
- Reported the views of service users and carers towards mental health nurses.
- Were conducted from July 2005 to December 2021. The July 2005 cut-off date was chosen to coincide with the last date of the search for a similar review [7].
- Were written in English.
2.2. Information Sources
- Medical Literature Analysis and Retrieval System Online [MEDLINE] (OVID)
- Cumulative Index to Nursing and Allied Health Literature [CINAHL] [EbscoHost]
- Excerpta Medica database [EMBASE] (OVID)
- Cochrane central (WILEY)
- PsychINFO (OVID)
2.3. Search Strategy
2.4. Selection Process
2.5. Data Collection Process
2.6. Data Items
2.7. Risk of Bias Assessment
2.8. Grouping Studies for Synthesis
2.9. Data Synthesis
2.10. Amendments to Information Provided at Registration
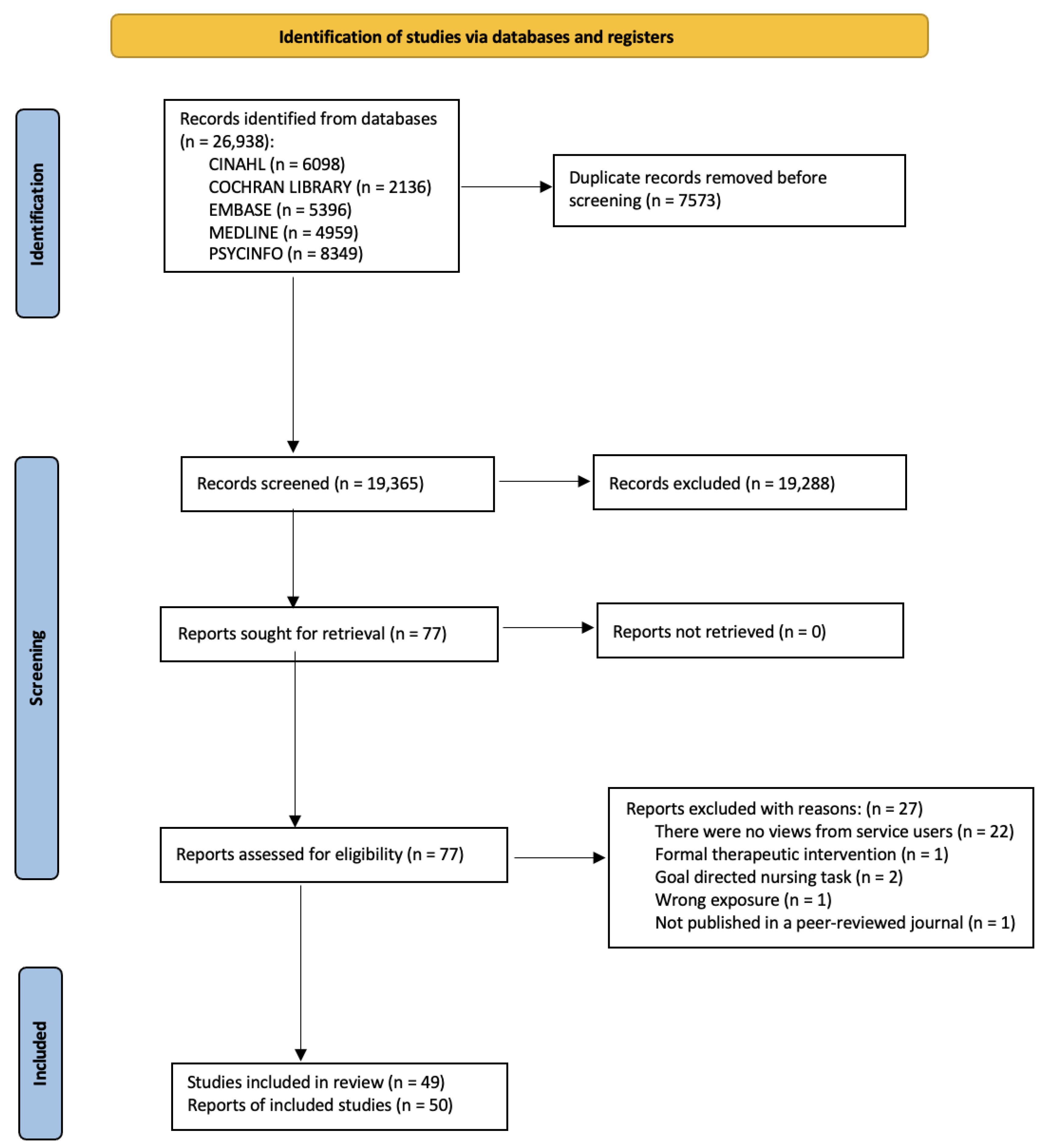
3. Results
3.1. Description of Included Studies
3.2. Quality Appraisal

{kind=link}
| Study Author | Digital Object Identifier (DOI) | Criteria 1 | Criteria 2 | Criteria 3 | Criteria 4 | Criteria 5 | Criteria 6 | Criteria 7 | Criteria 8 | Criteria 9 | Criteria 10 |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Ådnøy Eriksen et al. (2014) [18] | https://doi.org/10.1111/inm.12024 (accessed on 20 June 2022) | Yes | Yes | Yes | Yes | Yes | No | No | Yes | Yes | Yes |
| Askey et al. (2009) [19] | https://doi.org/10.1111/j.1467-6427.2009.00470.x (accessed on 20 June 2022) | Yes | Yes | Yes | Yes | Yes | No | No | Yes | Yes | Yes |
| Biringer et al. (2021) [20] | https://doi.org/10.1111/ppc.12633 (accessed on 20 June 2022) | Yes | Yes | Yes | Yes | Yes | Unclear | Unclear | Yes | Yes | Yes |
| Coatsworth-Puspoky et al. (2006) [22] | https://doi.org/10.1111/j.1365-2850.2006.00968.x (accessed on 20 June 2022) | Yes | Yes | Yes | Yes | Yes | No | No | Yes | Yes | Yes |
| Cunningham & Slevin (2005) [23] | https://doi.org/10.1111/j.1365-2850.2004.00769.x (accessed on 20 June 2022) | Yes | Unclear | Yes | Yes | Yes | No | No | Yes | No | Yes |
| Earle et al. (2011) [24] | https://doi.org/10.1111/j.1365-2850.2010.01672.x (accessed on 20 June 2022) | Yes | Yes | Yes | Yes | Yes | No | Yes | Yes | Yes | Yes |
| Evans et al. (2021) [25] | https://doi.org/10.1111/inm.12795 (accessed on 20 June 2022) | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
| Frain et al.l. (2021) [26] | https://doi.org/10.1080/01612840.2020.1820120 (accessed on 20 June 2022) | Yes | Yes | Yes | Yes | Yes | No | Yes | Yes | Yes | Yes |
| Gerace et al. (2018) [27] | https://doi.org/10.1111/inm.12298 (accessed on 27 July 2022) | Yes | Yes | Yes | Yes | Yes | No | No | Yes | Yes | Yes |
| Goodwin & Happell (2006) [29] | https://doi.org/10.1111/j.1447-0349.2006.00413.x (accessed on 27 July 2022) | Yes | Yes | Yes | Yes | Yes | No | No | Yes | Yes | Yes |
| Goodwin & Happell (2007) [30] | https://doi.org/10.1080/01612840701354596 (accessed on 27 July 2022) | Yes | Yes | Yes | Yes | Yes | No | No | Yes | Yes | Yes |
| Goodwin & Happell (2007) [31] | https://doi.org/10.1080/01612840701354612 (accessed on 27 July 2022) | Yes | Yes | Yes | Yes | Yes | No | No | Yes | Yes | Yes |
| Gray & Brown (2017) [32] | https://doi.org/10.1111/inm.12296 (accessed on 27 July 2022) | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
| Gunasekara et al. (2014) [33] | https://doi.org/10.1111/inm.12027 (accessed on 27 July 2022) | Yes | Yes | Yes | Yes | Yes | No | No | Yes | Yes | Yes |
| Happell & Palmer (2010) [35] | https://doi.org/10.3109/01612840.2010.488784 (accessed on 27 July 2022) (accessed on 27 July 2022) | Yes | Yes | Yes | Yes | Yes | No | Yes | Yes | Yes | Yes |
| Horgan et al. (2021) [36] | https://doi.org/10.1111/inm.12768 (accessed on 27 July 2022) | Yes | Yes | Yes | Yes | Yes | No | No | Yes | Yes | Yes |
| Jones et al. (2007) [37] | https://doi.org/10.1111/j.1365-2648.2007.04332.x (accessed on 27 July 2022) | Yes | Yes | Yes | Yes | Yes | No | Yes | Yes | Yes | Yes |
| Keogh et al. (2020) [38] | https://doi.org/10.1080/01612840.2020.1731889 (accessed on 27 July 2022) | Yes | Yes | Yes | Yes | Yes | No | Yes | Yes | Yes | Yes |
| Kertchok (2014) [39] | https://doi.org/10.3109/01612840.2014.908439 (accessed on 27 July 2022) | Yes | Yes | Yes | Yes | Yes | No | Yes | Yes | Yes | Yes |
| Lees et al. (2014) [42] | https://doi.org/10.1111/inm.12061 (accessed on 27 July 2022) | Yes | Yes | Yes | Yes | Yes | No | No | Yes | Yes | Yes |
| Lessard- Deschênes, & Goulet (2022) [43] | https://doi.org/10.1111/jpm.12800 (accessed on 27 July 2022) | Yes | Yes | Yes | Yes | Yes | No | No | Yes | Yes | Yes |
| Lim et al. (2019) [44] | http://hdl.handle.net/20.500.11937/77779 (accessed on 27 July 2022) | Yes | Yes | Yes | Yes | Yes | No | No | Yes | Yes | Yes |
| McAllister et al. (2021) [45] | https://doi.org/10.1111/inm.12835 (accessed on 27 July 2022) | Yes | Yes | Yes | Yes | Yes | No | Yes | Yes | Yes | Yes |
| McCann et al. (2012) [47] | https://doi.org/10.1111/j.1365-2702.2011.03836.x (accessed on 27 July 2022) | Yes | Yes | Yes | Yes | Yes | No | No | Yes | Yes | Yes |
| Moll et al. (2018) [49] | https://doi.org/10.3928/02793695-20180305-04 (accessed on 27 July 2022) | Yes | Yes | Yes | Yes | Yes | No | No | Yes | Yes | Yes |
| Montreuil et al. (2015) [50] | https://doi.org/10.3109/01612840.2015.1075235 (accessed on 27 July 2022) | Yes | Yes | Yes | Yes | Yes | Yes | Unclear | Yes | Yes | Yes |
| Pitkänen et al. (2008) [51] | https://doi.org/10.1016/j.ijnurstu.2008.03.003 (accessed on 27 July 2022) | Yes | Yes | Yes | Yes | Yes | Yes | No | Yes | Yes | Yes |
| Romeu-Labayen et al. (2022) [53] | https://doi.org/10.1111/jpm.12766 (accessed on 14 July 2022) | Yes | Yes | Yes | Yes | Yes | No | Yes | Yes | Yes | Yes |
| Rose et al. (2015) [54] | https://doi.org/10.1017/S2045796013000693 (accessed on 27 July 2022) | Yes | Yes | Yes | Yes | Yes | No | No | Yes | Yes | Yes |
| Rydon (2005) [55] | https://doi.org/10.1111/j.1440-0979.2005.00363.x (accessed on 27 July 2022) | Yes | Yes | Yes | Yes | Yes | No | No | Yes | Yes | Yes |
| Santangelo et al. (2018) [56] | https://doi.org/10.1111/inm.12317 (accessed on 27 July 2022) | Yes | Yes | Yes | Yes | Yes | No | No | Yes | Yes | Yes |
| Schneidtinger et al. (2019) [58] | https://doi.org/10.1111/jcap.12245 (accessed on 27 July 2022) | Yes | Yes | Yes | Yes | Yes | No | No | Yes | Yes | Yes |
| Shattell et al. (2007) [59] | https://doi.org/10.1111/j.1447-0349.2007.00477.x (accessed on 27 July 2022) | Yes | Yes | Yes | Yes | Yes | No | No | Yes | Yes | Yes |
| Stenhouse (2011) [61] | https://doi.org/10.1111/j.1365-2850.2010.01645.x (accessed on 27 July 2022) | Yes | Yes | Yes | Yes | Yes | No | Yes | Yes | Yes | Yes |
| Stewart et al. (2015) [62] | https://doi.org/10.1111/inm.12107 (accessed on 27 July 2022) | Yes | Yes | Yes | Yes | Yes | No | Yes | Yes | Yes | Yes |
| Terry (2020) [63] | https://doi.org/10.1111/inm.12676 (accessed on 27 July 2022) | Yes | Yes | Yes | Yes | Yes | No | No | Yes | Yes | Yes |
| Testerink et al. (2019) [64] | https://doi.org/10.1111/ppc.12275 (accessed on 27 July 2022) | Yes | Yes | Yes | Yes | Yes | No | Yes | Yes | Unclear | Yes |
| Wilson (2010) [66] | https://doi.org/10.1111/j.1365-2850.2010.01586.x (accessed on 27 July 2022) | Yes | Yes | Yes | Yes | Yes | No | Yes | Yes | No | Yes |
| Wortans et al. (2006) [67] | https://doi.org/10.1111/j.1365-2850.2006.00916.x (accessed on 27 July 2022) | Yes | Yes | Yes | Yes | Yes | No | Yes | Yes | Yes | Yes |
3.3. Service Users’ Views and Expectations of Mental Health Nurses
3.3.1. Satisfaction with Nursing Care
3.3.2. Service User-Centred Care
3.3.3. Recovery-Focused Care
3.3.4. Mental Health Nurse Flexibility
3.3.5. Therapeutic Relationships
3.3.6. Expectation of Interventions Delivered by Mental Health Nurses
3.3.7. Important Qualities of Mental Health Nurses
3.3.8. Negative Views of Mental Health Nurses
3.3.9. Views of Mental Health Nurse Prescribers
3.4. Views and Expectations of Carers
3.4.1. Collaborating with Carers
3.4.2. Negative Views
4. Discussion
4.1. Limitations of the Evidence Included in the Review
4.2. Limitations of the Review Processes
4.3. Implications of the Results for Practice
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization. Mental Health Atlas 2020; World Health Organization: Geneva, Switzerland, 2021. [Google Scholar]
- McKay, K.; Ariss, J.; Rudnick, A. RAISe-ing awareness: Person-centred care in coercive mental health care environments—A scoping review and framework development. J. Psychiatr. Ment. Health Nurs. 2021, 28, 251–260. [Google Scholar] [CrossRef] [PubMed]
- Rock, D.; Cross, S.P. Regional planning for meaningful person-centred care in mental health: Context is the signal not the noise. Epidemiol. Psychiatr. Sci. 2020, 29, e104. [Google Scholar] [CrossRef] [PubMed]
- Carey, T.A. Beyond patient-centered care: Enhancing the patient experience in mental health services through patient-perspective care. Patient Exp. J. 2016, 3, 46–49. [Google Scholar] [CrossRef]
- Stanhope, V.; Solomon, P. Getting to the Heart of Recovery: Methods for Studying Recovery and their Implications for Evidence-Based Practice. Br. J. Soc. Work 2008, 38, 885–899. [Google Scholar] [CrossRef]
- Javed, A.; Herrman, H. Involving patients, carers and families: An international perspective on emerging priorities. BJPsych Int. 2017, 14, 1–4. [Google Scholar] [CrossRef]
- Bee, P.; Playle, J.; Lovell, K.; Barnes, P.; Gray, R.; Keeley, P. Service user views and expectations of UK-registered mental health nurses: A systematic review of empirical research. Int. J. Nurs. Stud. 2008, 45, 442–457. [Google Scholar] [CrossRef]
- Khan, K.S.; Ter Riet, G.; Glanville, J.; Sowden, A.J.; Kleijnen, J. Undertaking Systematic Reviews of Research on Effectiveness: CRD’s Guidance for Carrying Out or Commissioning Reviews; No. 4 (2n); NHS Centre for Reviews and Dissemination: York, UK, 2001. [Google Scholar]
- Hungerford, C.; Fox, C. Consumer’s perceptions of Recovery-oriented mental health services: An Australian case-study analysis. Nurs. Health Sci. 2014, 16, 209–215. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- Adams, R.J.; Smart, P.; Huff, A.S. Shades of Grey: Guidelines for Working with the Grey Literature in Systematic Reviews for Management and Organizational Studies. Int. J. Manag. Rev. 2017, 19, 432–454. [Google Scholar] [CrossRef]
- Li, T.; Higgins, J.P.T.; Deeks, J.J. Chapter 5: Collecting data. In Cochrane Handbook for Systematic Reviews of Interventions Version 6.2; Higgins, J.P.T., Thomas, J., Chandler, J., Cumpston, M., Li, T., Page, M.J., Welch, V.A., Eds.; Updated February 2021. Cochrane. 2021; Available online: http://www.training.cochrane.org/handbook (accessed on 24 May 2022).
- Thomas, B.; Ciliska, D.; Dobbins, M.; Micucci, S. A process for systematically reviewing the literature: Providing the research evidence for public health nursing interventions. Worldviews Evid.-Based Nurs. 2004, 1, 176–184. [Google Scholar] [CrossRef]
- Armijo-Olivo, S.; Stiles, C.R.; Hagen, N.A.; Biondo, P.D.; Cummings, G.G. Assessment of study quality for systematic reviews: A comparison of the Cochrane Collaboration Risk of Bias Tool and the Effective Public Health Practice Project Quality Assessment Tool: Methodological research. J. Eval. Clin. Pract. 2012, 18, 12–18. [Google Scholar] [CrossRef]
- Hong, Q.; Pluye, P.; Fabregues, S.; Boardman, F.; Cargo, M.; Dagenais, F.; Gagnon, M.P.; Griffiths, F.; Nicolau, B.; O’Cathain, A.; et al. Mixed Methods Appraisal Tool (MMAT), Version 2018. Registration of Copyright (#1148552). Canadian Intellectual Property Office, Industry Canada. 2018. Available online: http://mixedmethodsappraisaltoolpublic.pbworks.com/w/file/fetch/127916259/MMAT_2018_criteria-manual_2018-08-01_ENG.pdf (accessed on 22 May 2022).
- Lockwood, C.; Munn, Z.; Porritt, K. Qualitative research synthesis: Methodological guidance for systematic reviewers utilizing meta-aggregation. Int. J. Evid.-Based Healthc. 2015, 13, 179–187. [Google Scholar] [CrossRef]
- Popay, J.; Roberts, H.; Sowden, A.; Petticrew, M.; Arai, L.; Rodgers, M.; Britten, N.; Roen, K.; Duffy, S. Guidance on the Conduct of Narrative Synthesis in Systematic Reviews. ESRC Methods Programme. 2006. Available online: https://www.lancaster.ac.uk/media/lancaster-university/content-assets/documents/fhm/dhr/chir/NSsynthesisguidanceVersion1-April2006.pdf (accessed on 19 August 2022).
- Ådnøy Eriksen, K.; Arman, M.; Davidson, L.; Sundfør, B.; Karlsson, B. Challenges in relating to mental health professionals: Perspectives of persons with severe mental illness: Challenges in Relating to Professionals. Int. J. Ment. Health Nurs. 2014, 23, 110–117. [Google Scholar] [CrossRef]
- Askey, R.; Holmshaw, J.; Gamble, C.; Gray, R. What do carers of people with psychosis need from mental health services? Exploring the views of carers, service users and professionals. J. Fam. Ther. 2009, 31, 310–331. [Google Scholar] [CrossRef]
- Biringer, E.; Hove, O.; Johnsen, Ø.; Lier, H.Ø. “People just don’t understand their role in it.” Collaboration and coordination of care for service users with complex and severe mental health problems. Perspect. Psychiatr. Care 2021, 57, 900–910. [Google Scholar] [CrossRef]
- Brimbelecombe, N.; Tingle, A.; Murrells, T. How mental health nursing can best improve service users’ experiences and outcomes in inpatient settings: Responses to a national consultation. J. Psychiatr. Ment. Health Nurs. 2007, 14, 503–509. [Google Scholar] [CrossRef]
- Coatsworth-Puspoky, R.; Forchuk, C.; Ward-Griffin, C. Nurse-client processes in mental health: Recipients’ perspectives. J. Psychiatr. Ment. Health Nurs. 2006, 13, 347–355. [Google Scholar] [CrossRef]
- Cunningham, G.; Slevin, E. Community psychiatric nursing: Focus on effectiveness. J. Psychiatr. Ment. Health Nurs. 2005, 12, 14–22. [Google Scholar] [CrossRef]
- Earle, E.A.; Taylor, J.; Peet, M.; Grant, G. Nurse prescribing in specialist mental health (Part 1): The views and experiences of practising and non-practising nurse prescribers and service users. J. Psychiatr. Ment. Health Nurs. 2011, 18, 189–197. [Google Scholar] [CrossRef]
- Evans, A.M.; Quinn, C.; McKenna, B.; Willis, K. Consumers living with psychosis: Perspectives on sexuality. Int. J. Ment. Health Nurs. 2021, 30, 382–389. [Google Scholar] [CrossRef]
- Frain, S.; Chambers, L.; Higgins, A.; Donohue, G. “Not Left in Limbo”: Service User Experiences of Mental Health Nurse Prescribing in Home Care Settings. Issues Ment. Health Nurs. 2021, 42, 660–666. [Google Scholar] [CrossRef] [PubMed]
- Gerace, A.; Oster, C.; O’Kane, D.; Hayman, C.L.; Muir-Cochrane, E. Empathic processes during nurse–consumer conflict situations in psychiatric inpatient units: A qualitative study. Int. J. Ment. Health Nurs. 2018, 27, 92–105. [Google Scholar] [CrossRef] [PubMed]
- Giménez-Díez, D.; Maldonado Alía, R.; Rodríguez Jiménez, S.; Granel, N.; Torrent Solà, L.; Bernabeu-Tamayo, M.D. Treating mental health crises at home: Patient satisfaction with home nursing care. J. Psychiatr. Ment. Health Nurs. 2020, 27, 246–257. [Google Scholar] [CrossRef] [PubMed]
- Goodwin, V.; Happell, B. Conflicting agendas between consumers and carers: The perspectives of carers and nurses. Int. J. Ment. Health Nurs. 2006, 15, 135–143. [Google Scholar] [CrossRef]
- Goodwin, V.; Happell, B. Consumer and carer participation in mental health care: The carer’s perspective: Part 1—The importance of respect and collaboration. Issues Ment. Health Nurs. 2007, 28, 607–623. [Google Scholar] [CrossRef]
- Goodwin, V.; Happell, B. Consumer and carer participation in mental health care: The Carer’s Perspective: Part 2—Barriers to effective and genuine participation. Issues Ment. Health Nurs. 2007, 28, 625–638. [Google Scholar] [CrossRef]
- Gray, R.; Brown, E. What does mental health nursing contribute to improving the physical health of service users with severe mental illness? A thematic analysis. Int. J. Ment. Health Nurs. 2017, 26, 32–40. [Google Scholar] [CrossRef]
- Gunasekara, I.; Pentland, T.; Rodgers, T.; Patterson, S. What makes an excellent mental health nurse? A pragmatic inquiry initiated and conducted by people with lived experience of service use: What makes an excellent mental health nurse? Int. J. Ment. Health Nurs. 2014, 23, 101–109. [Google Scholar] [CrossRef]
- Happell, B.; Sundram, S.; Wortans, J.; Johnstone, H.; Ryan, R.; Lakshmana, R. Assessing Nurse-Initiated Care in a Mental Health Crisis Assessment and Treatment Team in Australia. Psychiatr. Serv. 2009, 60, 1527–1531. [Google Scholar] [CrossRef]
- Happell, B.; Palmer, C. The Mental Health Nurse Incentive Program: The Benefits from a Client Perspective. Issues Ment. Health Nurs. 2010, 31, 646–653. [Google Scholar] [CrossRef]
- Horgan, A.; O Donovan, M.; Manning, F.; Doody, R.; Savage, E.; Dorrity, C.; O’Sullivan, H.; Goodwin, J.; Greaney, S.; Biering, P.; et al. ‘Meet Me Where I Am’: Mental health service users’ perspectives on the desirable qualities of a mental health nurse. Int. J. Ment. Health Nurs. 2021, 30, 136–147. [Google Scholar] [CrossRef]
- Jones, M.; Bennett, J.; Lucas, B.; Miller, D.; Gray, R. Mental health nurse supplementary prescribing: Experiences of mental health nurses, psychiatrists and patients. J. Adv. Nurs. 2007, 59, 488–496. [Google Scholar] [CrossRef]
- Keogh, B.; Brady, A.M.; Downes, C.; Doyle, L.; Higgins, A.; McCann, T. Evaluation of a Traveller Mental Health Liaison Nurse: Service User Perspectives. Issues Ment. Health Nurs. 2020, 41, 799–806. [Google Scholar] [CrossRef]
- Kertchok, R. Building Collaboration in Caring for People with Schizophrenia. Issues Ment. Health Nurs. 2014, 35, 872–882. [Google Scholar] [CrossRef] [PubMed]
- King, B.M.; Linette, D.; Donohue-Smith, M.; Wolf, Z.R. Relationship between Perceived Nurse Caring and Patient Satisfaction in Patients in a Psychiatric Acute Care Setting. J. Psychosoc. Nurs. Ment. Health Serv. 2019, 57, 29–38. [Google Scholar] [CrossRef] [PubMed]
- Koga, M.; Furegato, A.R.F.; Santos, J.L.F. Opinions of the staff and users about the quality of the mental health care delivered at a Family Health Program. Rev. Latino-Am. Enferm. 2006, 14, 163–169. [Google Scholar] [CrossRef] [PubMed]
- Lees, D.; Procter, N.; Fassett, D. Therapeutic engagement between consumers in suicidal crisis and mental health nurses: Therapeutic Engagement and Suicidal Crisis. Int. J. Ment. Health Nurs. 2014, 23, 306–315. [Google Scholar] [CrossRef]
- Lessard-Deschênes, C.; Goulet, M. The therapeutic relationship in the context of involuntary treatment orders: The perspective of nurses and patients. J. Psychiatr. Ment. Health Nurs. 2022, 29, 287–296. [Google Scholar] [CrossRef]
- Lim, E.; Wynaden, D.; Heslop, K.D. Consumers’ Perceptions of Nurses Using Recovery-focused Care to Reduce Aggression in All Acute Mental Health Including Forensic Mental Health Services: A Qualitative Study. J. Recovery Ment. Health 2019, 2, 21–34. [Google Scholar]
- McAllister, S.; Simpson, A.; Tsianakas, V.; Robert, G. “What matters to me”: A multi-method qualitative study exploring service users’, carers’ and clinicians’ needs and experiences of therapeutic engagement on acute mental health wards. Int. J. Ment. Health Nurs. 2021, 30, 703–714. [Google Scholar] [CrossRef]
- McCann, T.V.; Clark, E. Attitudes of patients towards mental health nurse prescribing of antipsychotic agents. Int. J. Nurs. Pract. 2008, 14, 115–121. [Google Scholar] [CrossRef]
- McCann, T.V.; Lubman, D.I.; Clark, E. Primary caregivers’ satisfaction with clinicians’ response to them as informal carers of young people with first-episode psychosis: A qualitative study. J. Clin. Nurs. 2012, 21, 224–231. [Google Scholar] [CrossRef]
- McCloughen, A.; Gillies, D.; O’Brien, L. Collaboration between mental health consumers and nurses: Shared understandings, dissimilar experiences. Int. J. Ment. Health Nurs. 2011, 20, 47–55. [Google Scholar] [CrossRef]
- Moll, M.F.; Pires, F.C.; Ventura, C.A.A.; Boff, N.N.; da Silva, N.F. Psychiatric Nursing Care in a General Hospital: Perceptions and Expectations of the Family/Caregiver. J. Psychosoc. Nurs. Ment. Health Serv. 2018, 56, 31–36. [Google Scholar] [CrossRef]
- Montreuil, M.; Butler, K.J.D.; Stachura, M.; Pugnaire Gros, C. Exploring Helpful Nursing Care in Pediatric Mental Health Settings: The Perceptions of Children with Suicide Risk Factors and Their Parents. Issues Ment. Health Nurs. 2015, 36, 849–859. [Google Scholar] [CrossRef]
- Pitkänen, A.; Hätönen, H.; Kuosmanen, L.; Välimäki, M. Patients’ descriptions of nursing interventions supporting quality of life in acute psychiatric wards: A qualitative study. Int. J. Nurs. Stud. 2008, 45, 1598–1606. [Google Scholar] [CrossRef]
- Rask, M.; Brunt, D. Verbal and social interactions in Swedish forensic psychiatric nursing care as perceived by the patients and nurses. Int. J. Ment. Health Nurs. 2006, 15, 100–110. [Google Scholar] [CrossRef]
- Romeu-Labayen, M.; Tort-Nasarre, G.; Rigol Cuadra, M.A.; Giralt Palou, R.; Galbany-Estragués, P. The attitudes of mental health nurses that support a positive therapeutic relationship: The perspective of people diagnosed with BPD. J. Psychiatr. Ment. Health Nurs. 2022, 29, 317–326. [Google Scholar] [CrossRef]
- Rose, D.; Evans, J.; Laker, C.; Wykes, T. Life in acute mental health settings: Experiences and perceptions of service users and nurses. Epidemiol. Psychiatr. Sci. 2015, 24, 90–96. [Google Scholar] [CrossRef]
- Rydon, S.E. The attitudes, knowledge and skills needed in mental health nurses: The perspective of users of mental health services. Int. J. Ment. Health Nurs. 2005, 14, 78–87. [Google Scholar] [CrossRef]
- Santangelo, P.; Procter, N.; Fassett, D. Seeking and defining the ‘special’ in specialist mental health nursing: A theoretical construct. Int. J. Ment. Health Nurs. 2018, 27, 267–275. [Google Scholar] [CrossRef]
- Saur, C.D.; Steffens, D.C.; Harpole, L.H.; Fan, M.Y.; Oddone, E.Z.; Unützer, J. Satisfaction and Outcomes of Depressed Older Adults with Psychiatric Clinical Nurse Specialists in Primary Care. J. Am. Psychiatr. Nurs. Assoc. 2007, 13, 62–70. [Google Scholar] [CrossRef]
- Schneidtinger, C.; Haslinger-Baumann, E. The lived experience of adolescent users of mental health services in Vienna, Austria: A qualitative study of personal recovery. J. Child Adolesc. Psychiatr. Nurs. 2019, 32, 112–121. [Google Scholar] [CrossRef]
- Shattell, M.M.; Starr, S.S.; Thomas, S.P. Take my hand, help me out: Mental health service recipients’ experience of the therapeutic relationship. Int. J. Ment. Health Nurs. 2007, 16, 274–284. [Google Scholar] [CrossRef] [PubMed]
- Sinclair, L.; Hunter, R.; Hagen, S.; Nelson, D.; Hunt, J. How effective are mental health nurses in A&E departments? Emerg. Med. J. 2006, 23, 687–692. [Google Scholar] [PubMed]
- Stenhouse, R.C. “They all said you could come and speak to us”: Patients’ expectations and experiences of help on an acute psychiatric inpatient ward. J. Psychiatr. Ment. Health Nurs. 2011, 18, 74–80. [Google Scholar] [CrossRef] [PubMed]
- Stewart, D.; Burrow, H.; Duckworth, A.; Dhillon, J.; Fife, S.; Kelly, S.; Marsh-Picksley, S.; Massey, E.; O’Sullivan, J.; Qureshi, M.; et al. Thematic analysis of psychiatric patients’ perceptions of nursing staff. Int. J. Ment. Health Nurs. 2015, 24, 82–90. [Google Scholar] [CrossRef]
- Terry, J. ‘In the middle’: A qualitative study of talk about mental health nursing roles and work. Int. J. Ment. Health Nurs. 2020, 29, 414–426. [Google Scholar] [CrossRef]
- Testerink, A.E.; Lankeren, J.E.; Daggenvoorde, T.H.; Poslawsky, I.E.; Goossens, P.J.J. Caregivers experiences of nursing care for relatives hospitalized during manic episode: A phenomenological study. Perspect. Psychiatr. Care 2019, 55, 23–29. [Google Scholar] [CrossRef]
- Wand, T.; Schaecken, P. Consumer evaluation of a mental health liaison nurse service in the Emergency Department. Contemp. Nurse J. Aust. Nurs. Prof. 2006, 21, 14–21. [Google Scholar] [CrossRef]
- Wilson, A.; Hutchinson, M.; Hurley, J. Literature review of trauma-informed care: Implications for mental health nurses working in acute inpatient settings in Australia. Int. J. Ment. Health Nurs. 2017, 26, 326–343. [Google Scholar] [CrossRef]
- Wortans, J.; Happell, B.; Johnstone, H. The role of the nurse practitioner in psychiatric/mental health nursing: Exploring consumer satisfaction. J. Psychiatr. Ment. Health Nurs. 2006, 13, 78–84. [Google Scholar] [CrossRef]
- Thomson, A.E.; Racher, F.; Clements, K. Person-centered Psychiatric Nursing Interventions in Acute Care Settings. Issues Ment. Health Nurs. 2019, 40, 682–689. [Google Scholar] [CrossRef]
- Bowen, M.; Mason, T. Forensic and non-forensic psychiatric nursing skills and competencies for psychopathic and personality disordered patients. J. Clin. Nurs. 2012, 21, 3556–3564. [Google Scholar] [CrossRef]
- Çelik Ince, S.; Partlak Günüşen, N.; Serçe, Ö. The opinions of Turkish mental health nurses on physical health care for individuals with mental illness: A qualitative study. J. Psychiatr. Ment. Health Nurs. 2018, 25, 245–257. [Google Scholar] [CrossRef]
- Cleary, A.; Dowling, M. Knowledge and attitudes of mental health professionals in Ireland to the concept of recovery in mental health: A questionnaire survey. J. Psychiatr. Ment. Health Nurs. 2009, 16, 539–545. [Google Scholar] [CrossRef]
- Cusack, E.; Killoury, F.; Nugent, L.E. The professional psychiatric/mental health nurse: Skills, competencies and supports required to adopt recovery-orientated policy in practice. J. Psychiatr. Ment. Health Nurs. 2017, 24, 93–104. [Google Scholar] [CrossRef]
- Giannouli, H.; Perogamvros, L.; Berk, A.; Svigos, A.; Vaslamatzis, G. Attitudes, knowledge and experience of nurses working in psychiatric hospitals in Greece, regarding borderline personality disorder: A comparative study. J. Psychiatr. Ment. Health Nurs. 2009, 16, 481–487. [Google Scholar] [CrossRef]
- Goodwin, V.; Happell, B. In our own words: Consumers’ views on the reality of consumer participation in mental health care. Contemp. Nurse 2006, 21, 4–13. [Google Scholar] [CrossRef]
- Goodwin, V.; Happell, B. To be treated like a person: The role of the psychiatric nurse in promoting consumer and carer participation in mental health service delivery. J. Contrib. 2008, 14, 1766–1775. [Google Scholar]
- Happell, B.; Palmer, C.; Tennent, R. The Mental Health Nurse Incentive Program: Desirable knowledge 2008, skills and attitudes from the perspective of nurses. J. Clin. Nurs. 2011, 20, 901–910. [Google Scholar] [CrossRef]
- Hawamdeh, S.; Fakhry, R. Therapeutic relationships from the psychiatric nurses’ perspectives: An interpretative phenomenological study. Perspect. Psychiatr. Care 2014, 50, 178–185. [Google Scholar] [CrossRef]
- Hurley, J. A qualitative study of mental health nurse identities: Many roles, one profession. Int. J. Ment. Health Nurs. 2009, 18, 383–390. [Google Scholar] [CrossRef]
- Kennedy, C.; Morrissey, J.; Donohue, G. Mental health nurses’ perceived preparedness to work with adults who have child sexual abuse histories. J. Psychiatr. Ment. Health Nurs. 2021, 28, 384–393. [Google Scholar] [CrossRef]
- Kim, H.-W.; Salyers, M.P. Attitudes and Perceived Barriers to Working with Families of Persons with Severe Mental Illness: Mental Health Professionals’ Perspectives. Community Ment. Health J. 2008, 44, 337–345. [Google Scholar] [CrossRef]
- Lakeman, R. What is good mental health nursing? A Survey of Irish Nurses. Arch. Psychiatr. Nurs. 2012, 26, 225–231. [Google Scholar] [CrossRef]
- McLeod, K.; Simpson, A. Exploring the value of mental health nurses working in primary care in England: A qualitative study. J. Psychiatr. Ment. Health Nurs. 2017, 24, 387–395. [Google Scholar] [CrossRef]
- Moreno-Poyato, A.R.; Rodríguez-Nogueira, Ó. The association between empathy and the nurse–patient therapeutic relationship in mental health units: A cross-sectional study. J. Psychiatr. Ment. Health Nurs. 2021, 28, 335–343. [Google Scholar] [CrossRef] [PubMed]
- Munro, A.; Watson, H.; McFadyen, A. Assessing the impact of training on mental health nurses’ therapeutic attitudes and knowledge about co-morbidity: A randomised controlled trial. Int. J. Nurs. Stud. 2007, 44, 1430–1438. [Google Scholar] [CrossRef] [PubMed]
- Nardella, N.; Hooper, S.; Lau, R.; Hutchinson, A. Developing acute care-based mental health nurses’ knowledge and skills in providing recovery-orientated care: A mixed methods study. Int. J. Ment. Health Nurs. 2021, 30, 1170–1182. [Google Scholar] [CrossRef] [PubMed]
- Pounds, K.G. Client-Nurse Interaction with Individuals with Schizophrenia: A Descriptive Pilot Study. Issues in Mental Health Nursing 2010, 31, 770–774. [Google Scholar] [CrossRef]
- Reid, R.; Escott, P.; Isobel, S. Collaboration as a process and an outcome: Consumer experiences of collaborating with nurses in care planning in an acute inpatient mental health unit. Int. J. Ment. Health Nurs. 2018, 27, 1204–1211. [Google Scholar] [CrossRef] [Green Version]
- Romeu-Labayen, M.; Cuadra, M.A.R.; Galbany-Estragués, P.; Corbal, S.B.; Palou, R.M.G.; Rn, G.T. Borderline personality disorder in a community setting: Service users’ experiences of the therapeutic relationship with mental health nurses. Int. J. Ment. Health Nurs. 2020, 29, 868–877. [Google Scholar] [CrossRef]
- Ryan, R.; Garlick, R.; Happell, B. Exploring the role of the mental health nurse in community mental health care for the aged. Issues Ment. Health Nurs. 2006, 27, 91–105. [Google Scholar] [CrossRef]
- Sclafani, M.; Caldwell, B.; Fitzgerald, E.; Mcquaide, T.A. Implementing the Clinical Nurse Specialist Role in a Regional State Psychiatric Hospital. Clin. Nurse Spec. 2008, 22, 66–71. [Google Scholar] [CrossRef]
- Varghese, B. Relationships between positive and negative attributes of self-compassion and perceived caring efficacy among psychiatric-mental health nurses. J. Psychosoc. Nurs. Ment. Health Serv. 2020, 58, 32–40. [Google Scholar] [CrossRef]
- Ward, L.; Gwinner, K. Have you got what it takes? Nursing in a Psychiatric Intensive Care Unit. J. Ment. Health Train. Educ. Pract. 2015, 10, 101–116. [Google Scholar] [CrossRef]
- White, M.R.; Stein-Parbury, J.; Orr, F.; Dawson, A. Working with consumers who hear voices: The experience of early career nurses in mental health services in Australia. Int. J. Ment. Health Nurs. 2019, 28, 605–615. [Google Scholar] [CrossRef]
- Wu, W.; Chen, S. Nurses’ perceptions on and experiences in conflict situations when caring for adolescents with anorexia nervosa: A qualitative study. Int. J. Ment. Health Nurs. 2021, 30, 1386–1394. [Google Scholar] [CrossRef]
- Wilson, D.W. Culturally competent psychiatric nursing care. J. Psychiatr. Ment. Health Nurs. 2010, 17, 715–724. [Google Scholar] [CrossRef]
- Le Boutillier, C.; Chevalier, A.; Lawrence, V.; Leamy, M.; Bird, V.J.; Macpherson, R.; Williams, J.; Slade, M. Staff understanding of recovery-orientated mental health practice: A systematic review and narrative synthesis. Implement. Sci. 2015, 10, 87. [Google Scholar] [CrossRef] [PubMed]
- Newman, D.; O’Reilly, P.; Lee, S.H.; Kennedy, C. Mental health service users’ experiences of mental health care: An integrative literature review: Service users’ experiences of Mental Health Care. J. Psychiatr. Ment. Health Nurs. 2015, 22, 171–182. [Google Scholar] [CrossRef] [Green Version]
- Eassom, E.; Giacco, D.; Dirik, A.; Priebe, S. Implementing family involvement in the treatment of patients with psychosis: A systematic review of facilitating and hindering factors. BMJ Open 2014, 4, e006108. [Google Scholar] [CrossRef] [PubMed]
- Moyo, N. Service User Views and Expectations of Mental Health Nurses: An Updated Systematic Review. 2022. (accessed on 1 September 2022). [CrossRef]
| Study Author (Year) | Digital Object Identifier (DOI) | Country Where Fieldwork Was Conducted | Study Aim | Study Setting Where Field Was Conducted | Population(s) under Investigation | Study Design | Sampling Procedure | Data Collection Procedures | Reported Psychometric Properties of Measures (For Cross Sectional, Quasi-Experimental, and Randomised Control Trial Study) | Data Analysis | Summary of Key Study Findings |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Ådnøy Eriksen et al. (2014) [18] | https://doi.org/10.1111/inm.12024 (accessed on 10 June 2022) | Norway | To explore how service users perceive their relationships with mental health nurses (MHNs) and how these relationships may hinder or promote recovery | Community Mental Health setting | Service users between 20 and 60 years with serious mental illness (n = 11) | Interpretative phonological analysis | Convenience sampling | One-on-one interviews | Interpretative phenomenological analysis | Service users’ relationships with MHNs were conditional. The individual’s autonomy was reduced when expected to match the MHNs’ expectations. Service users felt safe talking to MHNs who valued their ideas, beliefs, and ambitions. | |
| Askey et al. (2009) [19] | https://doi.org/10.1111/j.1467-6427.2009.00470.x (accessed on 10 June 2022) | United Kingdom | To examine the perspectives and experiences of carers and service users regarding what carers of people with psychosis require from mental health services | Community Mental Health setting (n = 2 centres) | Service users aged between 16 and 64 years (n = 12) Carers (n = 22) | Qualitative study | Convenience sampling | One-on-one interviews and focus group | Thematic analysis | Increasing carer engagement was perceived as critical by all groups. Carers perceive that MHNs should be more respectful and listen to carers. The service users thought carers must be educated about psychosis. | |
| Biringer et al. (2021) [20] | https://doi.org/10.1111/ppc.12633 (accessed on 10 June 2022) | Norway | To examine how service providers collaborate and coordinate to help service users recover | Community mental health setting | Service users with complex and severe mental illness (n = 6) | Qualitative study | Convenience sampling | Group interviews | Thematic analysis | Participants want to be involved in making decisions about the nursing care. Service users expected nurses to be accessible and flexible in their help. They desired MHNs to visit their homes. | |
| Brimblecombe et al. (2007) [21] | https://doi.org/10.1111/j.1365-2850.2007.01119.x (accessed on 10 June 2022) | United Kingdom | To explore the perspectives of multiple stakeholders on how MHNs can improve service users’ experiences and outcomes in inpatient care settings. | Community setting | Service users (n = 11) Carers (n = 3) | Consultation | Convenience sampling | Survey and open meetings | Content analysis | Service users desire more privacy and security. Carers expect MHNs to provide meaningful activities to service users. Service users believe inpatient MHNs need more training. | |
| Coatsworth-Puspoky et al. (2006) [22] | https://doi.org/10.1111/j.1365-2850.2006.00968.x (accessed on 10 June 2022) | Canada | To explore the cultural and contextual factors that influence the development of the nurse-service user relationship. | Consumer-survivor organisations (n = 2 centres) | Service users with mood disorders, panic disorder, personality disorder & schizophrenia (n = 14) | Mini-ethnography design | Convenience sampling | One-on-one interviews and field notes | Thematic analysis | There are two types of relationship. (1) The service user feels accepted by the MHN, is treated with respect, and discloses personal problems. (2) The MHN is not very helpful, and the service user feels frustrated. So, the nurse and the service user ignore one another. | |
| Cunningham & Slevin (2005) [23] | https://doi.org/10.1111/j.1365-2850.2004.00769.x (accessed on 14 July 2022) | Ireland | The aim of the study was not explicitly stated. The author states in the discussion that the study collected the views of service users on the role of the community MHNs | Community mental health setting (n = 2 centres) | Service users with depression, anxiety, eating disorders and schizophrenia (n = 13) | Qualitative | Convenience sampling | Focus group | Thematic content analysis | Some service users considered MHNs helpful. The roles of MHNs and other professionals in multidisciplinary teams were not well understood by service users. Service users perceive that people with lived experiences of mental illness should be included in the multidisciplinary team | |
| Earle et al. (2011) [24] | https://doi.org/10.1111/j.1365-2850.2010.01672.x (accessed on 14 July 2022) | United Kingdom | To find out what service users thought about the care they got from MHN prescribers | Early intervention service | Service users aged between 16 and 35 years with first episode of psychosis (n = 6) | Qualitative case study | Convenience sampling | One-on-one interview | Interpretative phenomenological analysis | Service users preferred getting their medications from MHN prescribers because it was more convenient and less stressful. MHN prescribers gave service users the option of selecting their own medication. The potential benefits of medication were not adequately explained. | |
| Evans et al. (2021) [25] | https://doi.org/10.1111/inm.12795 (accessed on 10 June 2022) | Australia | To explore how service users residing in longer-stay mental health rehabilitation services were able (or not) to negotiate and sustain sexual expression | Mental health rehabilitation setting | Service users aged between 16 and 64 years with schizophrenia and schizo-affective disorder (n = 11) | Qualitative case study | Purposive sampling | One-on-one interviews | Thematic analysis | MHNs policed the facility’s physical area and restricted sexual expression. MHNs entered service users’ bedrooms without warning or permission, violating their right to privacy. Service users felt that sexual expression limits hindered recovery. | |
| Frain et al. (2021) [26] | https://doi.org/10.1080/01612840.2020.1820120 (accessed on 10 June 2022) | Ireland | To examine the experiences of service users with MHN prescribers in a homecare setting | Community mental health setting (n = 2 centres) | Service users aged from 16 to 64 years (n = 12) | Qualitative exploratory | Purposive sampling | One-on-one interviews | Thematic analysis | The MHN prescriber helped the service users to feel heard and understood. Participants highly valued the continuity of treatment provided by the MHN prescriber. The nurse prescription service increased compliance and decreased non-disclosure. | |
| Gerace et al. (2018) [27] | https://doi.org/10.1111/inm.12298 (accessed on 14 July 2022) | Australia | To investigate how empathy is developed and maintained when MHNs and service users disagree. | Community setting | Service users (mean age of 45 years) (n = 7) | Qualitative | Purposive sampling | One-on-one interviews | Thematic analysis | Showing empathy creates trust and reduces anger as well as paranoia. Empathy emerges when MHNs strive to understand the dispute from the service users’ viewpoints. Service users felt empathised with when MHNs listened, respected, and were non-judgmental. | |
| Giménez-Díez D et al. (2020) [28] | https://doi.org/10.1111/jpm.12573 (accessed on 14 July 2022) | Spain | To examine the satisfaction of service users and their families with the nursing care provided through a hospital’s home care programme that promotes person-centred care | Mental health crisis assessment and treatment team | Service users (n = 20) Carers (n = 20) | A cross-sectional study including quantitative survey data and qualitative interview | Convenience sampling | One-on-one interviews | The CARE Q questionnaire measured the nurse’s behaviour and had a Cronbach’s alpha of 0.853. The CSQ-8 measured satisfaction with nursing care and had a Cronbach’s alpha of 0.85. | Descriptive statistics and framework analysis | Both service users and carers were satisfied with nursing care, but service users were more so. Service users’ satisfaction was associated with staff flexibility and experience. MHNs were regarded as professional, reliable, and caring. |
| Goodwin et al. (2006) [29] | https://doi.org/10.1111/j.1447-0349.2006.00413.x (accessed on 14 July 2022) | Australia | To examine how service users and carers participate in mental health care from the perspective of the carers | Mental health services (n = 2 centres) | Carers (n = 19) | Exploratory qualitative | Convenience sampling | Focus group | Content analysis | Service users and carers often have conflicting agendas. When service users and carers had competing interests, MHNs prioritised service users’ demands. Carers viewed conflicting agendas as barriers to care participation. | |
| Goodwin et al. (2007) * [30] | https://doi.org/10.1080/01612840701354596 (accessed on 14 July 2022) | Australia | To explore carers’ attitudes and perceptions of their involvement in mental health care | A combination of bed- based and community units (n = 2 centres) | Service users (n = Not reported) Carers (n = not reported) | Exploratory qualitative | Convenience sampling | Focus group | Content analysis | Participants believed that mutual trust and respect were necessary for effective collaboration to occur. MHNs were compassionate and inclusive. Carers valued the accessibility of MHNs to both the service user and the carer. | |
| Goodwin et al. (2007) * [31] | https://doi.org/10.1080/01612840701354612 (accessed on 14 July 2022) | Australia | To explore carers’ perceptions of their involvement in mental health care | A combination of bed- based and community units and team services (n = 2 centres) | Service users (n = Not reported) | Goodwin et al. (2007) | https://doi.org/10.1080/01612840701354612 (accessed on 14 July 2022) | Australia | To explore carers’ perceptions of their involvement in mental health care | A combination of bed- based and community units and team services (n = 2 centres) | |
| Gray & Brown (2017) [32] | https://doi.org/10.1111/inm.12296 (accessed on 10 June 2022) | United Kingdom | To assess and contrast the service user and clinician perspectives about the practice of MHNs in promoting physical health in people with severe mental illness | Inpatient mental health, rehabilitation, and community settings (n = 2 centres) | Service users (mean age of 30 years) with schizophrenia bipolar disorder, Constipation and Hypertension (n = 15) | Qualitative | Convenience sampling | One-on-one interviews | Thematic analysis | Service users reported that MHNs rarely helped them with common adverse effects of medication. MHNs had no time to assist service users in changing their unhealthy habits. Service users expect MHNs to be more skilled in providing physical health care. | |
| Gunasekara et al. (2014) [33] | https://doi.org/10.1111/inm.12027 (accessed on 10 June 2022) | Australia | To assess the perspectives of service users and carers on mental health nursing care. | Inpatient mental health setting | Service users (n = 10) Carers (n = 10) | Qualitative | Purposive sampling | One-on-one interviews | Thematic analysis | Service users expected MHNs to respect and educate them about their treatment. Carers wanted to be included in care planning and believed they could help the care team if appropriately supported. MHNs viewed advocating for service users as critical to building therapeutic relationships. | |
| Happell et al. (2009) [34] | https://doi.org/10.1176/ps.2009.60.11.1527 (accessed on 14 July 2022) | Australia | To compare the level of satisfaction between service users receiving nurse-initiated care (experimental group) and those receiving treatment as usual (control group). | Mental health crisis assessment and treatment team | Service users with schizophrenia, schizoaffective disorder, depression, anxiety disorders (n = 103) Carers (n = not reported) | Quasi-experimental study | Service users were randomly assigned to receive care from the nurse practitioner candidate or to treatment as usual. | Survey | Content validity of the questionnaire was established in the study referenced by the authors. Cronbach’s alpha coefficient was 0.91. | Descriptive analysis | Participants’ perspectives were not adequately described. Service users and carers were satisfied with the mental health nursing care. |
| Happell & Palmer (2010) [35] | https://doi.org/10.3109/01612840.2010.488784 (accessed on 10 June 2022) | Australia | To assess the service users’ experiences and perspectives on the care they received from the Mental Health Nurses Incentive Program | Primary health care setting | Service users (n = 14) | A descriptive, exploratory qualitative study | Snowballing sampling | One-on-one interviews | Thematic analysis | Service users perceived MHNs as flexible, and this increased treatment compliance. Participants described nurses as having a broad knowledge of the health care system. Service users viewed the services offered by MHNs as providing more privacy than the public mental health system. | |
| Horgan et al. (2021) [36] | https://doi.org/10.1111/inm.12768 (accessed on 10 June 2022) | Australia and Europe | To examine the views of mental health service users on the required qualities of a mental health nurse as an input for the development of a learning module | University and community settings (n = 7 centres) | Service users (n = 50) | Qualitative | Convenience sampling | Focus group | Thematic analysis | Service users valued MHNs who respected them, gave them hope and were non-judgemental. MHNs were expected to know the referral process and the organisations that assist service users. Service users desire MHNs to treat them with empathy and to assist them in coping with their challenges. | |
| Jones et al. (2007) [37] | https://doi.org/10.1111/j.1365-2648.2007.04332.x (accessed on 14 July 2022) | United Kingdom | To assess the perspectives of service users towards the MHN prescribers | Mental healthcare organization | Service users (mean age of 43 years) (n = 12) a | Qualitative | Purposive sampling | One-on-one interviews | Thematic analysis | The participants viewed supplemental prescribing by MHNs as satisfactory. They also felt that MHNs provided more in-depth descriptions of treatment alternatives. Service users perceived MHNs prescribers paid close attention to physical health. | |
| Keogh et al. (2020) [38] | https://doi.org/10.1080/01612840.2020.1731889 (accessed on 10 June 2022) | Ireland | To find out how Irish travellers perceive the Traveller Mental Health Liaison Nurse (TMHLN) | Community mental health setting | Service users (n = 10) | Descriptive qualitative study | Convenience sampling | One-on-one interviews | Thematic analysis | Service users viewed the TMHLN as providing confidentiality and privacy, allowing them to feel at ease and discuss their issues. The TMHLN was described as kind, understanding, and trustworthy. Participants thought that they were assisted in resolving some of the social problems that were bothering them. | |
| Kertchok (2014) [39] | https://doi.org/10.3109/01612840.2014.908439 (accessed on 10 June 2022) | Thailand | To examine the relationship between carers of people with schizophrenia and community MHNs | Community mental health setting | Carers (n = 17) | Grounded theory methodology | Purposive theoretical sampling | One-on-one interviews | Constant comparative methods | MHNs were described as kind. Carers felt MHNs provided them with information about care and were involved in the care of service users. MHNs encouraged carers to express their concerns and needs. | |
| King et al. (2019) [40] | https://doi.org/10.3928/02793695-20190225-01 (accessed on 14 July 2022) | United States of America | To examine service users’ satisfaction with nursing care at an inpatient mental health unit. | Inpatient mental health setting | Service users aged between 18 to 91 years (n = 169) | Cross sectional | Convenience sampling | Survey | The Caring Behaviours Inventory-16 measured the competencies of nurses: Cronbach’s alpha coefficients = 0.968. The Client Satisfaction with Care measured service user satisfaction with care: Part 1, Cronbach’s alpha = 0.883; and Part 2, Cronbach’s alpha = 0.898 | Descriptive statistics | Confidentiality of service user information, feeling safe in the ward, and receiving medication on time were all highly rated by service users. Service users were highly satisfied with the nursing care. However, the time spent with MHNs was less satisfactory for service users. |
| Koga et al. (2006) [41] | https://doi.org/10.1590/S0104-11692006000200003 (accessed on 14 July 2022) | Brazil | To assess mental health care in the Family Health Care Program through the views of service users and their carers | Community mental health setting | Service users aged between 21 to 70 years with anxiety, depression (n = 18) Carers aged between 20 to 74 years (n = 29) | Survey | Convenience sampling | Survey | Not reported. | Descriptive analysis | Service users reported that MHNs rarely explained medications. Carers perceived they did not receive enough information about medication. Service users reported that they received care when required. |
| Lees et al. (2014) [42] | https://doi.org/10.1111/inm.12061 (accessed on 14 July 2022) | Australia | To examine service users’ needs and experiences during suicidal crises, and the role of MHNs | Community and inpatient settings | Service users (average age of 41 years) with Suicidal crises (n = 9) | Qualitative | Convenience sampling | Interviews | Constant comparative, classical content analysis | Participants perceived MHNs as not interested in discovering what precipitated their suicidal crisis. They believed that MHNs abused their power. Service users felt they had few therapeutic interactions with MHNs. | |
| Lessard-Deschênes & Goulet (2021) [43] | https://doi.org/10.1111/jpm.12800 (accessed on 14 July 2022) | Canada | To explore the therapeutic relationship in the context of involuntary treatment orders as perceived by service users | Inpatient mental health setting | Service users aged between 30 to 62 years with schizophrenia and bipolar disorder (n = 6) | Secondary data analysis of qualitative interviews | Convenience sampling | One-on-one interviews | Content analysis | The relationships between the service users and MHNs were superficial and never reached a therapeutic level. Service users viewed forced treatment as impeding the establishment of a trusting relationship. The safety-oriented strategy used by MHNs was considered abusive. | |
| Lim et al. (2019) [44] | http://hdl.handle.net/20.500.11937/77779 (accessed on 10 June 2022) | Australia | Determine how service users perceive MHNs’ use of recovery-oriented care to address aggressive behaviour | Inpatient mental health setting | Service users aged 18 or older with mood, substance-related, post-traumatic stress disorders, schizophrenia & other psychotic disorders (n = 31) | Grounded theory methodology | Purposive and theoretical sampling | One-on-one interviews and Focus group | Constant comparative method | Participants stated that MHNs must treat them as individuals. Service users thought MHNs were quick to identify and judge them as potentially aggressive when they displayed negative emotions. Participants emphasised the importance of MHNs interacting positively with them. | |
| McAllister et al. (2021) [45] | https://doi.org/10.1111/inm.12835 (accessed on 10 June 2022) | United Kingdom | To explore how engagement is experienced in acute units and the requirements of service users, carers, and clinicians to develop a collaborative intervention | Inpatient mental health setting | Service users aged between 18 to 64 years with psychotic, mood & personality disorders (n = 14) Carers aged between 18 to 64 years (n = 2) | Experience-based Co-design (EBCD) Qualitative study | Convenience sampling | One-on-one interviews, observations, and field notes | Thematic analysis | Service users and carers reported a lack of high-quality, person-centred, collaborative engagement. Service users and carers frequently felt that their concerns were not heard. All participants perceived that there was a need to strengthen nurse-patient engagement. | |
| McCann & Clark (2008) [46] | https://doi.org/10.1111/j.1440-172X.2008.00674.x (accessed on 10 June 2022) | Australia | To explore the perceptions of service users with schizophrenia regarding unrestricted autonomous non-medical prescription of antipsychotic medications by MHNs | Community mental health settings (n = 3 centres) | Service users aged between 19 to 65 years with schizophrenia (n = 81) | Cross sectional | Non-probability sampling | Survey | The Factors Influencing Neuroleptic Medication Taking Scale measured service users’ views of prescription of antipsychotic medication by nurses. Cronbach’s alpha values were not reported | Descriptive analysis | More than half of the participants favoured MHNs having prescriptive authority. Participants under the age of 36 were more likely than those over the age of 36 to support allowing specially trained MHNs to stop prescribing medication. Many participants reported being satisfied with their relationship with MHNs. |
| McCann et al. (2012) [47] | https://doi.org/10.1111/j.1365-2702.2011.03836.x (accessed on 10 June 2022) | Australia | To assess the perspectives of first-time carers regarding how MHNs respond to them as carers of young people with first-episode psychosis. | Community mental health setting | Carers of service users with first-episode psychosis (n = 20) | Qualitative interpretative phenomenological analysis | Purposive sampling | Interviews | Interpretative phenomenological analysis | Two competing themes emerged. Carers perceived MHNs and other mental health professionals as accessible, attentive, and responsive to their needs. Second, carers believed some clinicians undervalued their role and excluded them from clinical decision-making about the young person. | |
| McCloughen et al. (2011) [48] | https://doi.org/10.1111/j.1447-0349.2010.00708.x (accessed on 14 July 2022) | Australia | To assess if service users and nurses in a mental health rehabilitation setting had common understandings, attitudes, values, and experiences of collaboration | Mental health rehabilitation setting | Service users with severe mental illnesses (n = 18) | Mixed-method approach comprising focus groups and surveys | Purposive and convenience sampling | Focus group and survey | Not reported | Descriptive statistics and thematic analysis | Service users viewed collaboration as a partnership centred on the service users’ goals and wellness. They also perceived that active participation was essential. Collaboration requires effective communication and mutual recognition of one another’s expertise and skills. |
| Moll et al. (2018) [49] | https://doi.org/10.3928/02793695-20180305-04 (accessed on 14 July 2022) | Brazil | To examine the carers’ views and expectations of nursing care provided to mental health inpatients in a general hospital | Inpatient mental health setting | Carers (n = 10) | Descriptive–exploratory qualitative | Convenience sampling | Interviews | Content analysis | Carers were satisfied with the nursing care provided to their relatives. Establishing good interpersonal relationships with service users requires professionalism, care, and clinical competencies. Many carers had no higher expectations for nursing care than what was already being provided. | |
| Montreuil et al. (2015) [50] | https://doi.org/10.3109/01612840.2015.1075235 (accessed on 10 June 2022) | Canada | To examine service users at risk of suicide and their carers’ perceptions of nursing care in paediatric mental health settings | Paediatric mental health inpatient, outpatient, and day hospital settings. | Service users aged between 11 to 14 years with suicide risk factors (n = 5) Carers (n = 5) | Exploratory qualitative design | Convenience sampling | One-on-one interviews, observation, debriefing sessions, and survey | Thematic analysis | Participants felt that helpful nursing care for service users and carers is based on nursing interventions that help them collaborate with MHNs. Service users and carers felt that MHNs could help carers by being accessible and reassuring. All participants thought MHNs were vital in controlling shared and private places. | |
| Pitkänen et al. (2008) [51] | https://doi.org/10.1016/j.ijnurstu.2008.03.003 (accessed on 10 June 2022) | Finland | To assess how the nursing care in acute mental health inpatient units impacts the quality of life of service users. | Inpatient mental health settings (n = 7 centres) | Service users with schizophrenia, schizotypal disorder (n = 35) | Explorative descriptive qualitative study | Convenience sampling | One-on-one interviews | Content analysis | Service users perceived that MHNs empowered them by allowing them to make choices. Participants valued the opportunities provided by MHNs to participate in recreational activities. Service users expected MHNs to provide them with information about their illnesses and treatment. | |
| Rask & Brunt (2006) [52] | https://doi.org/10.1111/j.1447-0349.2006.00409.x (accessed on 14 July 2022) | Sweden | To determine the perspective of service users on the frequency and significance of verbal and social nursing interactions in inpatient mental health settings. | Inpatient mental health setting | Service users aged between 20 to 46 years with Mood disorders, sexual disorders, substance abuse, personality disorders, schizophrenia & other psychotic disorders (n = 20) | Cross sectional | Convenience sampling | Survey | Verbal and Social Interactions (VSI) measured the frequency and importance of nursing interactions. Cronbach’s alpha = 0.95). | Descriptive statistics | Service users thought it was important that MHNs explain what they could do to help themselves. Participants felt MHNs frequently encouraged them to learn new things. Service users thought it was vital for them to discuss their feelings with MHNs. |
| Romeu-Labayen et al. (2022) [53] # | https://doi.org/10.1111/jpm.12766 (accessed on 14 July 2022) | Spain | To explore how service users with borderline personality disorder perceive the role of MHNs in building a positive therapeutic relationship | Community mental health setting | Service users with borderline personality disorder (n = 12) | Qualitative descriptive design | Purposive sampling | One-on-one interviews | Thematic analysis | Service users trusted the MHNs more after being listened to and seeing empathy. Inspiring service users to change and heal was positively received by the service users. Participants saw MHNs as genuine when they used humour and felt accepted. | |
| Rose et al. (2015) [54] | https://doi.org/10.1017/S2045796013000693 (accessed on 14 July 2022) | United Kingdom | To examine the views and experiences of service users about life in an acute mental health ward | Inpatient mental health setting | Service users with schizophrenia and psychotic disorders (n = 37) | In-depth secondary analysis of focus group data | Purposive sampling | Focus group | Thematic analysis | The consensus among service users was that the ward was not therapeutic. Service users perceived MHNs as unavailable and uncaring. Participants felt forceful interventions were unneeded and overbearing. | |
| Rydon (2005) [55] | https://doi.org/10.1111/j.1440-0979.2005.00363.x (accessed on 14 July 2022) | New Zealand | To identify the attitudes, knowledge, and skills expected of mental health nurses | Support groups for users of mental health services | Service users (n = 21) Carers (n = not reported) | Qualitative descriptive methodology | Convenience sampling | Focus group | Thematic analysis | Service users highly regarded the therapeutic work of MHNs. Participants did not always experience therapeutic interactions in their encounters with MHNs. Service users identified positive attitudes towards service users as an important characteristic of MHNs. | |
| Santangelo et al. (2018) [56] | https://doi.org/10.1111/inm.12317 (accessed on 14 July 2022) | Australia | To create a theoretical model of mental health nursing practice that focuses on identifying qualities that contribute to favourable outcomes for service users | Community | Service users (n = 5) | Constructivist grounded theory | Purposive sampling | One-on-one interviews | Constant comparative method | Positive therapeutic relationships were considered essential in mental health nursing by service users. MHNs were described as spending more time with service users than any other professionals. Participants perceived that MHNs provided holistic care. | |
| Saur et al. (2007) [57] | https://doi.org/10.1177/1078390307301938 (accessed on 14 July 2022) | United States of America | To find out how satisfied service users are with the treatment they received from MHN specialists and their preferences for future depression therapy | Primary health care setting | Service users aged 60 years or older with depression (n = 105) | Cross sectional | Random sampling | Survey | Questionnaire measured service user satisfaction with nursing care. Psychometric properties not reported. | Descriptive statistics | The majority of service users expressed satisfaction with the quality of care provided by MHNs. Service users viewed the therapeutic relationship with MHNs as highly positive. Most of the service users are willing to seek care from MHNs in the future. |
| Schneidtinger et al. (2019) [58] | https://doi.org/10.1111/jcap.12245 (accessed on 14 July 2022) | Austria | To investigate how adolescents receiving mental health services experienced personal recovery | Community mental health setting | Service users aged between 15 to 19 years (n = 9) | Qualitative exploratory study | Self-selection sampling | One-on-one interviews | Content analysis | Service users reported that MHNs aided their recovery by teaching them coping strategies. The participants perceived that MHNs were always available for conversations. The presence of nurses gave service users a sense of security. | |
| Shattell et al. (2007) [59] | https://doi.org/10.1111/j.1447-0349.2007.00477.x (accessed on 14 July 2022) | United States of America | To explore service users’ experience of the therapeutic relationship | Community Mental Health setting | Service users aged between 21 to 65 years with mood, anxiety, antisocial personality disorders and schizophrenia (n = 20) | Secondary analysis of qualitative | Purposeful sampling | One-on-one interviews | Existential phenomenological approach | Service users had positive therapeutic relationships with MHNs. Participants thought building therapeutic relationships required providing psychological support, information, and referral recommendations to service users. Service users expect MHNs to know them as people, not as diagnoses or statistics. | |
| Sinclair et al. (2006) [60] | https://doi.org/10.1136/emj.2005.033175 (accessed on 14 July 2022) | United Kingdom | To examine the perception of service users about the care provided by MHNs in an accident and emergency department | Mental health crisis assessment and treatment team (n = 2 centres) | service users with Mental health disorders (n = 511) | Crossover design | Convenience sampling | Survey | Survey measured provision of information, care and treatment received. Psychometric properties not reported. | Descriptive statistics, linear and multinomial regression, and content analysis | Levels of satisfaction recorded were high for all service users with no significant differences between intervention and non-intervention periods. There were no concerns about MHNs. |
| Stenhouse (2011) [61] | https://doi.org/10.1111/j.1365-2850.2010.01645.x (accessed on 14 July 2022) | United Kingdom | To obtain insight into the experience of being a service user on an acute inpatient mental health ward | Inpatient mental health setting | Service users aged between 18 to 65 years (n = 13) | Qualitative | Convenience sampling | One-on-one interviews | Holistic analyses | Service users anticipated that MHNs would interact with them. However, MHNs did not approach them to initiate conversation, which was viewed as disinterest and a lack of caring. Participants believed nurses were frequently too busy to engage in conversation. | |
| Stewart et al. (2015) [62] | https://doi.org/10.1111/inm.12107 (accessed on 14 July 2022) | United Kingdom | To explore service users’ views of the personal and professional qualities of MHNs and how these contribute to the ward environment | Inpatient mental health setting (n = 16 centres) | Service users (62% were under 40 years) (n = 119) | Qualitative | Random sampling | One-on-one interviews | Thematic analysis | Service users recognised that MHNs have challenging and demanding work. Service users frequently expressed anger and hopelessness about their ward experience. Participants were frustrated that MHNs could not comprehend or sympathise with their concerns. | |
| Terry (2020) [63] | https://doi.org/10.1111/inm.12676 (accessed on 14 July 2022) | United Kingdom | To assess how mental health nursing was perceived by services users. | Community setting | Service users (n = 13) | Qualitative | Purposive sampling | One-on-one interviews and focus group | Thematic analysis | Participants labelled MHNs as “bridging the gap’ because they require various skills to meet the needs of different people. Service users viewed listening and helping as the most important nursing roles. Participants valued their therapeutic relationships with MHNs. | |
| Testerink et al. (2019) [64] | https://doi.org/10.1111/ppc.12275 (accessed on 14 July 2022) | Netherlands | To explore the experiences of carers with nursing care provided to their relatives during admission to closed wards for mania | Inpatient mental health setting (n = 3 centres) | Carers of service users with mania (n = 9) | Descriptive phenomenological design | Convenience sampling | One-on-one interviews | Stevick-Colaizzi-Keen method | Some carers described nurses as polite and helpful, while others perceived them as lacking passion for their work. Participants were disappointed that nurses were not listening to their advice. Carers desired to be involved in care planning, and some even requested to participate. | |
| Wand & Schaecken (2006) [65] | https://doi.org/10.5172/conu.2006.21.1.14 (accessed on 14 July 2022) | Australia | To assess the role of a mental health liaison nurse in the emergency department in Australia | Mental health crisis assessment and treatment team | Service users aged between 19 to 82 years (n = 59) | Cross sectional | Convenience sampling | Survey | Consumer satisfaction survey designed by Gillette et al. (1996) measured service users’ satisfaction levels with nursing care. We could not retrieve the referenced study (Gillette et al., 1996) to check the validity of the questionnaire | Descriptive statistics and thematic analysis | Most respondents acknowledged that the MHN was too willing to listen and provide emotional support. Service users reported that the MHN had expert knowledge of mental illnesses. Most of the service users described the MHN as empathetic, compassionate, and friendly. |
| Wilson (2010) [66] | https://doi.org/10.1111/j.1365-2850.2010.01586.x (accessed on 14 July 2022) | United States of America | To examine the views of service users about the competencies of MHN in providing culturally congruent care | Primary health care setting | Service users aged between 18 to 65 years (n = 15) | Qualitative descriptive study | Snowballing sampling | One-on-one interviews and qualitative survey | Thematic content analysis | Service users perceived that medication administration was the most important nursing intervention. Participants were allowed to participant in their religious practice. Service users struggled to identify culture-specific nursing interventions that improved their mental health. | |
| Wortans et al. (2006) [67] | https://doi.org/10.1111/j.1365-2850.2006.00916.x (accessed on 14 July 2022) | Australia | To establish the feasibility of implementing a nurse practitioner role in a variety of settings in Victoria, Australia | Mental health crisis assessment and treatment team (n = 4 centres) | Service users with schizophrenia, personality disorder and situational crises (n = 7) | Qualitative exploratory study | Convenience sampling | One-on-one interviews | Thematic content analysis | Except for one person, every participant expressed unequivocal support for the role of the nurse practitioner candidate. All participants indicated that they could relate to the nurse practitioner more easily than doctors. Service users reported that they would not hesitate to seek care and treatment from a nurse practitioner in the future. |
| Study Characteristics | Number of Studies [%] |
|---|---|
| Study design | |
| Qualitative studies | 38 [78%] |
| Cross sectional | 7 [14%] |
| Quasi-experimental | 1 [2%] |
| Mixed methods | 2 [4%] |
| Consultation | 1 [2%] |
| Settings | |
| Inpatient | 12 [24%] |
| Community | 31 [63%] |
| Mixed services | 6 [12%] |
| Population | |
| Adults | 21 [43%] |
| Children and adolescents | 2 [4%] |
| Elderly | 1 [2%] |
| Not reported | 25 [51%] |
| Study centres | |
| Multiple centres | 13 [27%] |
| Single centres | 36 [73%] |
| Countries where studies were conducted | |
| Australia | 16 [33%] |
| United Kingdom | 11 [22%] |
| United States of America | 4 [8%] |
| Canada | 3 [6%] |
| Ireland | 3 [6%] |
| Norway | 2 [4%] |
| Spain | 2 [4%] |
| Brazil | 2 [4%] |
| Thailand | 1 [2%] |
| Finland | 1 [2%] |
| Sweden | 1 [2%] |
| New Zealand | 1 [2%] |
| Netherlands | 1 [2%] |
| Study Author | Digital Object Identifier (DOI) | Selection Bias | Study Design | Confounders | Blinding | Data Collection Method | Withdrawals and Dropouts | Global Rating |
|---|---|---|---|---|---|---|---|---|
| King et al. (2019) [40] | https://doi.org/10.3928/02793695-20190225-01 (accessed on 20 June 2022) | Weak | Weak | Weak | Weak | Strong | Moderate | Weak |
| Koga et al. (2006) [41] | https://doi.org/10.1590/S0104-11692006000200003 (accessed on 20 June 2022) | Weak | Weak | Weak | Weak | Weak | Moderate | Weak |
| Happel et al. (2009) [34] | https://doi.org/10.1176/ps.2009.60.11.1527 (accessed on 20 June 2022) | Moderate | Moderate | Weak | Weak | Strong | Moderate | Weak |
| McCann & Clark (2008) [46] | https://doi.org/10.1111/j.1440-172X.2008.00674.x (accessed on 20 June 2022) | Weak | Weak | Weak | Weak | Moderate | Moderate | Weak |
| Rask & Brunt (2006) [52] | https://doi.org/10.1111/j.1447-0349.2006.00409.x (accessed on 20 June 2022) | Weak | Weak | Weak | Weak | Strong | Moderate | Weak |
| Saur et al. (2007) [57] | https://doi.org/10.1177/1078390307301938 (accessed on 20 June 2022) | Moderate | Weak | Weak | Weak | Weak | Moderate | Weak |
| Sinclair et al. (2006) [60] | https://doi.org/10.1136/emj.2005.033175 (accessed on 20 June 2022) | Weak | Weak | Weak | Weak | Weak | Moderate | Weak |
| Wand et al. (2006) [65] | https://doi.org/10.5172/conu.2006.21.1.14 (accessed on 20 June 2022) | Weak | Weak | Weak | Weak | Weak | Moderate | Weak |
| Study Authors | Digital Object Identifier (DOI) | Criteria 1 | Criteria 2 | Criteria 3 | Criteria 4 | Criteria 5 |
|---|---|---|---|---|---|---|
| Giménez-Díez D et al. (2020) [28] | https://doi.org/10.1111/jpm.12573 (accessed on 20 June 2022) | No | Yes | Yes | Can’t tell | Yes a |
| McCloughen et al. (2011) [48] | https://doi.org/10.1111/j.1447-0349.2010.00708.x (accessed on 20 June 2022) | Yes | Yes | Yes | Can’t tell | No |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Moyo, N.; Jones, M.; Kushemererwa, D.; Arefadib, N.; Jones, A.; Pantha, S.; Gray, R. Service User and Carer Views and Expectations of Mental Health Nurses: A Systematic Review. Int. J. Environ. Res. Public Health 2022, 19, 11001. https://doi.org/10.3390/ijerph191711001
Moyo N, Jones M, Kushemererwa D, Arefadib N, Jones A, Pantha S, Gray R. Service User and Carer Views and Expectations of Mental Health Nurses: A Systematic Review. International Journal of Environmental Research and Public Health. 2022; 19(17):11001. https://doi.org/10.3390/ijerph191711001
Chicago/Turabian StyleMoyo, Nompilo, Martin Jones, Diana Kushemererwa, Noushin Arefadib, Adrian Jones, Sandesh Pantha, and Richard Gray. 2022. "Service User and Carer Views and Expectations of Mental Health Nurses: A Systematic Review" International Journal of Environmental Research and Public Health 19, no. 17: 11001. https://doi.org/10.3390/ijerph191711001
APA StyleMoyo, N., Jones, M., Kushemererwa, D., Arefadib, N., Jones, A., Pantha, S., & Gray, R. (2022). Service User and Carer Views and Expectations of Mental Health Nurses: A Systematic Review. International Journal of Environmental Research and Public Health, 19(17), 11001. https://doi.org/10.3390/ijerph191711001