
Non-Pharmacological Nursing Interventions for Prevention and Treatment of Delirium in Hospitalized Adult Patients: Systematic Review of Randomized Controlled Trials


Abstract
:1. Introduction
2. Materials and Methods
2.1. Selection Criteria
2.1.1. Inclusion Criteria
2.1.2. Exclusion Criteria
2.2. Search Strategy and Data Extraction Criteria
2.2.1. Search Strategy
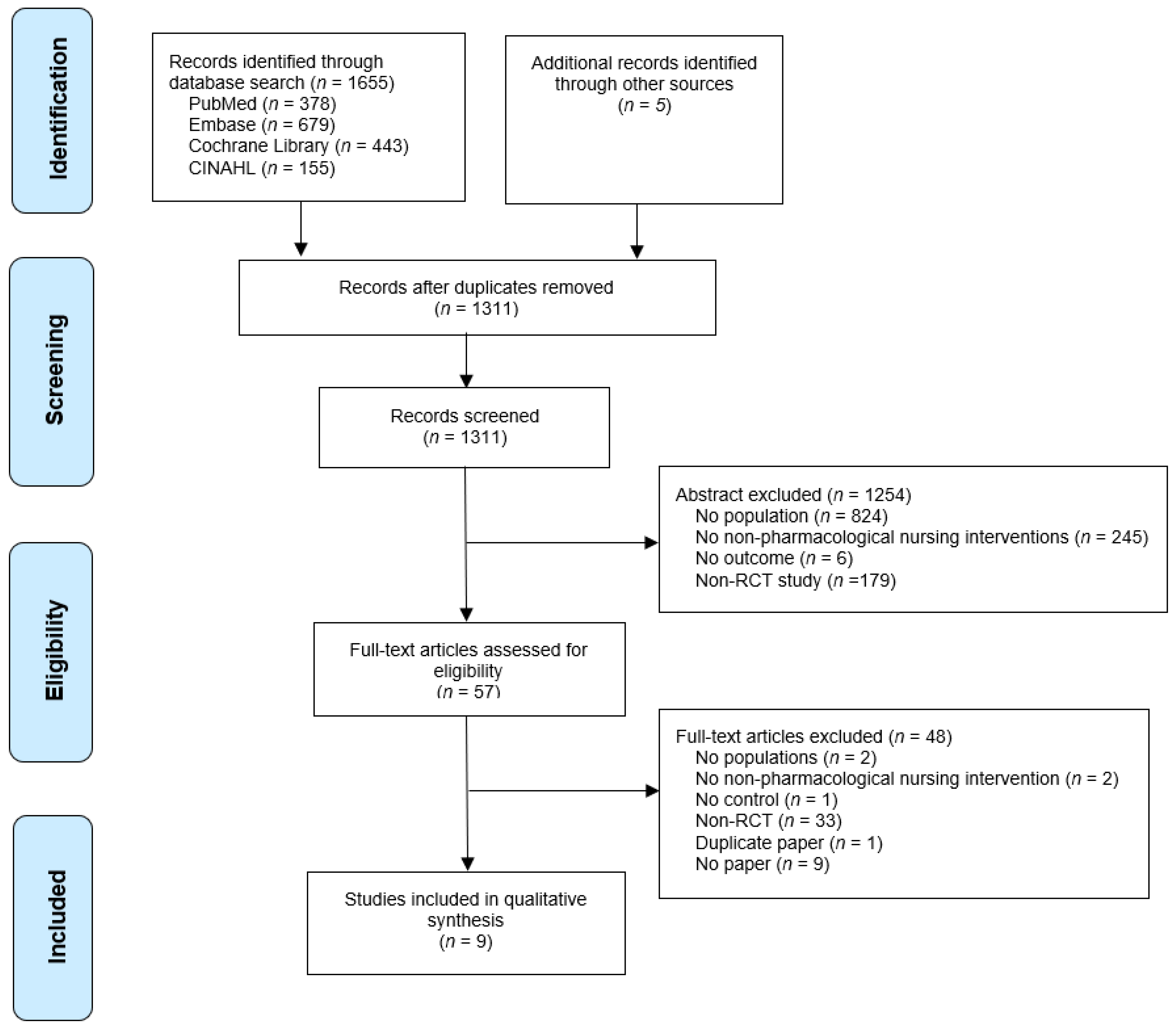
2.2.2. Study Selection
2.2.3. Data Extraction
2.3. Quality Assessment
3. Results
3.1. Selected Studies
3.2. Study Characteristics
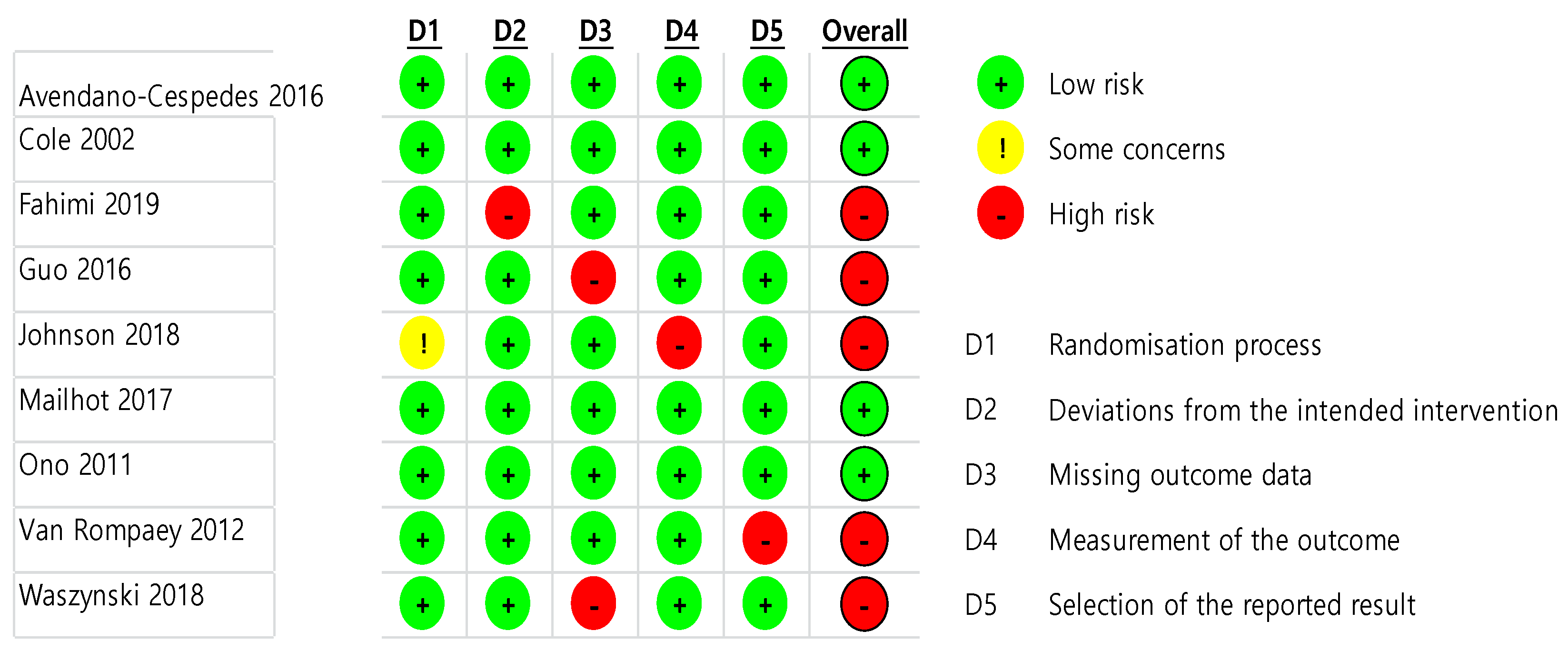
3.3. Risk of Bias Assessment
3.4. Intervention and Outcome Measures
4. Discussion
Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Ludolph, P.; Msc, J.S.; Kunzler, A.M.; Rösch, R.; Geschke, K.; Vahl, C.F.; Lieb, K. Non-Pharmacologic Multicomponent Interventions Preventing Delirium in Hospitalized People. J. Am. Geriatr. Soc. 2020, 68, 1864–1871. [Google Scholar] [CrossRef]
- Ekeozor, C.U.; Jeyaruban, D.; Lasserson, D. Where should patients with or at risk of delirium be treated in an acute care system? Comparing the rates of delirium in patients receiving usual care vs alternative care: A systematic review and meta-analysis. Int. J. Clin. Pr. 2020, 25, e13859. [Google Scholar] [CrossRef]
- Hauß, A.; Zilezinski, M.; Bergjan, M. Evidenzbasierte nicht-pharmakologische Delirprävention im allgemeinstationären Bereich—Eine systematische Übersichtsarbeit. Z. Evidenz Fortbild. Qual. Gesundheitswesen 2021, 160, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Lin, P.; Zhang, J.; Shi, F.; Liang, Z.-A. Can haloperidol prophylaxis reduce the incidence of delirium in critically ill patients in intensive care units? A systematic review and meta-analysis. Hear. Lung 2020, 49, 265–272. [Google Scholar] [CrossRef]
- Sahawneh, F.; Boss, L. Non-pharmacologic interventions for the prevention of delirium in the intensive care unit: An integrative review. Nurs. Crit. Care 2021, 26, 166–175. [Google Scholar] [CrossRef]
- Dylan, F.; Byrne, G.; Mudge, A.M. Delirium risk in non-surgical patients: Systematic review of predictive tools. Arch. Gerontol. Geriatr. 2019, 83, 292–302. [Google Scholar] [CrossRef]
- Zhu, C.; Wang, B.; Yin, J.; Xue, Q.; Gao, S.; Xing, L.; Wang, H.; Liu, W.; Liu, X. Risk factors for postoperative delirium after spinal surgery: A systematic review and meta-analysis. Aging Clin. Exp. Res. 2020, 32, 1417–1434. [Google Scholar] [CrossRef] [PubMed]
- Fahimi, K.; Abbasi, A.; Zahedi, M.; Amanpour, F.; Ebrahimi, H. The effects of multimedia education on postoperative delirium in patients undergoing coronary artery bypass graft: A randomized clinical trial. Nurs. Crit. Care 2020, 25, 346–352. [Google Scholar] [CrossRef]
- Johnson, K.; Fleury, J.; McClain, D. Music intervention to prevent delirium among older patients admitted to a trauma intensive care unit and a trauma orthopaedic unit. Intensiv. Crit. Care Nurs. 2018, 47, 7–14. [Google Scholar] [CrossRef] [PubMed]
- Mailhot, T.; Cossette, S.; Côté, J.; Bourbonnais, A.; Côté, M.-C.; Lamarche, Y.; Denault, A. A post cardiac surgery intervention to manage delirium involving families: A randomized pilot study. Nurs. Crit. Care 2017, 22, 221–228. [Google Scholar] [CrossRef]
- Waszynski, C.M.; Milner, K.A.; Staff, I.; Molony, S.L. Using simulated family presence to decrease agitation in older hospitalized delirious patients: A randomized controlled trial. Int. J. Nurs. Stud. 2018, 77, 154–161. [Google Scholar] [CrossRef] [PubMed]
- Avendaño-Céspedes, A.; García-Cantos, N.; González-Teruel, M.D.M.; Martínez-García, M.; Villarreal-Bocanegra, E.; Oliver-Carbonell, J.L.; Abizanda, P. Pilot study of a preventive multicomponent nurse intervention to reduce the incidence and severity of delirium in hospitalized older adults: MID-Nurse-P. Maturitas 2016, 86, 86–94. [Google Scholar] [CrossRef] [PubMed]
- Cole, M.G.; McCusker, J.; Bellavance, F.; Primeau, F.J.; Bailey, R.F.; Bonnycastle, M.J.; Laplante, J. Systematic detection and multidisciplinary care of delirium in older medical inpatients: A randomized trial. Can. Med. Assoc. J. 2002, 167, 753–759. [Google Scholar]
- Guo, Y.; Sun, L.; Li, L.; Jia, P.; Zhang, J.; Jiang, H.; Jiang, W. Impact of multicomponent, nonpharmacologic interventions on perioperative cortisol and melatonin levels and postoperative delirium in elderly oral cancer patients. Arch. Gerontol. Geriatr. 2016, 62, 112–117. [Google Scholar] [CrossRef] [PubMed]
- McKenzie, J.; Joy, A. Family intervention improves outcomes for patients with delirium: Systematic review and meta-analysis. Australas. J. Ageing 2020, 39, 21–30. [Google Scholar] [CrossRef] [PubMed]
- Jeffs, K.J.; Berlowitz, D.; Grant, S.; Lawlor, V.; Graco, M.; De Morton, N.A.; Savige, J.A.; Lim, W.K. An enhanced exercise and cognitive programme does not appear to reduce incident delirium in hospitalised patients: A randomised controlled trial. BMJ Open 2013, 3, e002569. [Google Scholar] [CrossRef] [Green Version]
- Martinez, F.; Tobar, C.; Beddings, C.I.; Vallejo, G.; Fuentes, P. Preventing delirium in an acute hospital using a non-pharmacological intervention. Age Ageing 2012, 41, 629–634. [Google Scholar] [CrossRef] [Green Version]
- Firozjayi, D.A.; Gorji, M.A.H.; Habibi, V. Nursing preventive measures against the incidence of delirium in hospitalized patients: A narrative review. J. Nurs. Midwifery Sci. 2017, 4, 58–67. [Google Scholar] [CrossRef]
- Ozga, D.; Krupa, S.; Witt, P.; Mędrzycka-Dąbrowska, W. Nursing Interventions to Prevent Delirium in Critically Ill Patients in the Intensive Care Unit during the COVID19 Pandemic—Narrative Overview. Healthcare 2020, 8, 578. [Google Scholar] [CrossRef]
- Moher, D.; Shamseer, L.; Clarke, M.; Ghersi, D.; Liberati, A.; Petticrew, M.; Shekelle, P.; Stewart, L.A.; PRISMA-P Group. Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015 statement. Syst. Rev. 2015, 4, 1–9. [Google Scholar] [CrossRef] [Green Version]
- Sterne, J.A.C.; Savović, J.; Page, M.J.; Elbers, R.G.; Blencowe, N.S.; Boutron, I.; Cates, C.J.; Cheng, H.-Y.; Corbett, M.S.; Eldridge, S.M.; et al. RoB 2: A revised tool for assessing risk of bias in randomised trials. BMJ 2019, 366, l4898. [Google Scholar] [CrossRef] [Green Version]
- Ono, H.; Taguchi, T.; Kido, Y.; Fujino, Y.; Doki, Y. The usefulness of bright light therapy for patients after oesophagectomy. Intensiv. Crit. Care Nurs. 2011, 27, 158–166. [Google Scholar] [CrossRef]
- Van Rompaey, B.; Elseviers, M.M.; Van Drom, W.; Fromont, V.; Jorens, P.G. The effect of earplugs during the night on the onset of delirium and sleep perception: A randomized controlled trial in intensive care patients. Crit. Care 2012, 16, R73. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pessoa, L.S.C.; Menezes, T.M.O.; Gomes, N.P.; Pereira, G.S.; Batista, V.M.; de Alencar, L.M.V. Nursing care for elderly patients with delirium in intensive care units. J. Nurs. UFPE 2019, 13, 372–378. [Google Scholar]
- Pieri, M.; De Simone, A.; Rose, S.; De Domenico, P.; Lembo, R.; Denaro, G.; Landoni, G.; Monaco, F. Trials Focusing on Prevention and Treatment of Delirium After Cardiac Surgery: A systematic Review of Randomized Evidence. J. Cardiothorac. Vasc. Anesth. 2020, 34, 1641–1654. [Google Scholar] [CrossRef]
- Haley, M.N.; Casey, P.; Kane, R.Y.; Dārziņš, P.; Lawler, K. Delirium management: Let’s get physical? A systematic review and meta-analysis. Australas. J. Ageing 2019, 38, 231–241. [Google Scholar] [CrossRef]
- Hebert, C. Evidence-Based Practice in Perianesthesia Nursing: Application of the American Geriatrics Society Clinical Practice Guideline for Postoperative Delirium in Older Adults. J. Peri Anesth. Nurs. 2017, 33, 253–264. [Google Scholar] [CrossRef] [PubMed]
- Gillick, M.R.; Serrell, N.A.; Gillick, L.S. Adverse consequences of hospitalization in the elderly. Soc. Sci. Med. 1982, 16, 1033–1038. [Google Scholar] [CrossRef]
- Maldonado, J.R. Acute Brain Failure. Crit. Care Clin. 2017, 33, 461–519. [Google Scholar] [CrossRef]
- Kyziridis, T.C. Post-operative delirium after hip fracture treatment—A review of the current literature. GMS Psycho-Soc. Med. 2006, 3, Doc01. [Google Scholar]
- Lat, I.; McMillian, W.; Taylor, S.; Janzen, J.M.; Papadopoulos, S.; Korth, L.; Ehtisham, A.; Nold, J.; Agarwal, S.; Azocar, R.; et al. The impact of delirium on clinical outcomes in mechanically ventilated surgical and trauma patients. Crit. Care Med. 2009, 37, 1898–1905. [Google Scholar] [CrossRef] [PubMed]
- Sibanda, A.; Carnes, D.; Visentin, D.; Cleary, M. A systematic review of the use of music interventions to improve outcomes for patients undergoing hip or knee surgery. J. Adv. Nurs. 2018, 75, 502–516. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
| First Author, Publication Year, Country | Study Design | Patients | Intervention | Control Condition | Delirium Screening Scale | Outcome | Time points of Measurements | Delirium-Related Results | |
|---|---|---|---|---|---|---|---|---|---|
| 1 | Avendaño-Céspedes 2016 Spain [12] | Parallel-group double-blind RCT | •50 hospitalized older adults Acute Geriatric Units •Exp: 21 patients Cont: 29 patients •Age: 65 years or older •No severe cognitive decline | Intervention: Multicomponent non-pharmacologic intervention (orientation, sensorial deficit, sleep, mobilization, hydration, nutrition, drug chart review, elimination, oxygenation, pain) Provider: intervention nurses Timing: Start—within 24 h of admission Duration—daily (from admission to discharge) | Usual care | Incidence: CAM Severity: Delirium Rating Scale-Revised-98 (DRS) | Primary outcomes: incidence, duration, severity Secondary outcomes: mortality, length of stay, use of physical restraint measures, and use of drugs for delirium control | From admission to 16 days Daily delirium evaluation in the afternoon | Incidence p = 0.039 Exp: 3 (14.3%) Cont: 12 (41.4%) Severity p = 0.040 Exp 35.0 (15.0%) Cont 65.0 (45.9%) Duration Exp: 1.7 (0.8) Cont: 3.4 (2.2) |
| 2 | Cole 2002 Canada | RCT | •218 older patients Five general medical units •Exp: 106 patients Cont: 112 patients •Age: 65 years or older •Prescreening: Short Portable Mental Status Questionnaire (scored 3–9 errors) or delirium recorded in the nursing notes + CAM | Intervention: Multidisciplinary care Consultation and follow up by a geriatric internist or psychiatrist and follow-up in hospital by the study nurse Nursing intervention protocol (environment, orientation, familiarity, communication, activity) Provider: intervention nurse, primary care nurses, geriatric internist, or psychiatrist Timing: Start—within 24 h of admission to detect prevalent delirium Duration—daily sessions with mean duration of 35.7 min for 8 weeks | Usual care | Incidence: Mini-Mental State Examination (MMSE) score Severity: Delirium Index CAM | Primary outcomes: incidence, severity | Up to 8weeks Three times during the first week and weekly thereafter for up to 8 weeks in hospital or until discharge | Incidence HR = 1.15, 95% CI 0.48–2.79 Severity HR = 1.09, 95% CI 0.74–1.60 |
| 3 | Fahimi 2019 Iran | RCT | •110 patients undergoing a coronary artery bypass graft •Exp: 55 patients Cont: 55 patients •Age: 18 years or older •Prescreening: Richmond Agitation-Sedation Scale (RASS) | Intervention: Multimedia education multimedia CD containing three short educational videos of 4–6 min 1st video—provides information about the disease process and procedures for CABG 2nd video—describes postoperative measures and special care provided in the Department of Cardiac Surgery, patient visitation schedule and procedure, respiratory exercises, exercise for the foot that undergoes surgery and possible complications, and bed leave time 3rd video-pre- and postoperative experiences with the patient Provider: 1st video—cardiologist, 2nd video—heart surgical ICU nurse 3rd video—person who has already undergone CABG Timing: Start—5–7 d before surgery Duration—4–6 min | Usual care | Incidence: CAM-ICU | Primary outcome: Incidence | 1~4 Postoperative day Twice a day(morning and afternoon) from admission to discharge from the ICU | Incidence Total p = 0.003 Exp: 13 (11.8) Cont: 28 (25.5) POD#2 morning p = 0.003 Exp: 4 (3.6) Cont: 16 (14.5) POD#3 morning p = 0.007 Exp: 0 (0) Cont: 8 (7.3) POD#4 morning p = 0.035 Exp: 0 (0) Cont: 6 (5.5) |
| 4 | Guo 2016 China | RCT | •160 elderly oral cancer patients who underwent tumor resection surgery Surgical intensive care unit •Exp: 81 patients Cont: 79 patients •Age: 65–80 years •Prescreening: MMSE score <24 | Intervention: Multicomponent, non-pharmacologic interventions: stimulating cognitive activities Preoperative health education was strengthened and providing psychological guidance to the patients Invited the patients to visit the SICU to become acquainted with the environment Calendars, clocks, cell phones, radios, glasses, and hearing aids were repeatedly offered to accomplish time, place, and character orientation three times per day Effective communication using a communication card and WordPad Noise was decreased as much as possible Good sleep–wake cycle was adopted Between 23:00 and 05:00, all nursing procedures were minimized Eyeshade and acoustic earplugs were allocated No restraint straps or indwelling catheters were applied Bedside MP3 players were provided to play light music through headphones for 1 h three times daily Nasal feeding was administered as soon as possible Usual care also provided Provider: MNI team (including nurse) Timing: Start/duration—preoperation to SICU admission (total time: 3 d) | Usual care | Incidence: CAM-ICU QoR40 (40-item quality of recovery score) | Primary outcomes: incidence, duration Secondary outcome: melatonin sulfate | First three postoperative days Twice daily 07:00–08:00 (T1, T3, T5) 19:00–20:00 (T2,T4,T6) | Incidence Total p = 0.006 Exp: 10 (15%) Cont: 25 (31.6%) POD#1 p = 0.035 Exp: 4 (7.5%) Cont: 13 (16.25%) POD#2 p = 0.374 Exp: 5 (6.25%) Cont: 9 (11.25%) POD#3 p = 0.364 Exp: 1 (1.25%) Cont: 4 (5%) Duration p = 0.001 Exp: 28.1 (8.6) Cont: 60.2 (15.8) |
| 5 | Johnson 2018 United States | RCT | •40 patients Trauma Intensive Care and Trauma Orthopaedic Unit •Exp: 20 patients Cont: 20 patients •Age: 55 years or older •Prescreening: CAM-ICU negative on admission | Intervention: Music listening headphones and a numbered iPod shuffle preloaded with 60 min of pre-selected music (a) simple repetitive rhythm, (b) self-selection, and (c) slow tempo (60–80 BPM) Provider: nurses Timing: Start—following admission Duration—60 min, two times per day, at 14:00 and 20:00 over a 3-d period (total time: 360 min) | Usual care | Incidence: CAM-ICU | Primary outcome: incidence Secondary outcome: physiologic signs | From admission to three day Every twelve hours at the beginning of each shift; from 07:00 to 19:00 and 19:00 to 07:00 | Incidence All participants screened negative for delirium. |
| 6 | Mailhot 2017 Canada | RCT | •30 patients Surgical intensive care unit (ICU) or the surgery unit •Exp: 16 patients Cont: 14 patients •Prescreening: Score ≥4 on the Intensive Care Delirium Screening Checklist (ICDSC) | Intervention: Mentoring of family caregivers concerning delirium management (MENTOR_D) Observe signs of delirium, communicate observations with the nurse, reorient patients, talk about family memories, use clear and simple sentences, verify if loved ones is wearing eyeglasses or hearing aids Usual care also provided Provider: intervention nurse (as a mentor who provided information on delirium and guidance to the FC in their new role of intervening in delirium management) Timing: Start—within 24 h of delirium onset with a total of seven encounters Duration—the first six encounters were 60 min, with 30 min for pre-bedside phase, 15 min for the bedside phase, and 15 min for post-bedside phase; and 30 min for the seventh discharge encounter (total time-150 min) | Usual care | Severity: Delirium Index (DI) CAM-ICU | Primary outcomes: severity, duration Secondary outcomes: complications during delirium, postoperative hospital stay, psycho-functional recovery, FC’s anxiety, self-efficacy | Days 1, 2, and 3 following study entry | Severity similar trajectories on days 1, 2, and 3 in both groups p = 0.27 Exp: Day 1: 10.56 (3.5%) Day 2: 5.38(5.45%) Day 3: 3.43 (4.96%) Cont: Day 1: 12.07 (4.05%) Day 2: 8 (6.34%) Day 3: 5.5 (7%) Duration Exp: 1.94 (1.34%) Cont: 4.14 (4.04%) |
| 7 | Ono 2011 Japan | RCT | •22 patients following esophagectomy ICU •Exp: 10 patients Cont:12 patients •Age: 18 years or older •Prescreening: NEECHAM Scale | Intervention: Bright light exposure Light at 2500 lx for the first 15 min (07:30–07:45), 4000 lx for the following 15 min (07:45–08:00), 5000 lx for 1 h (08:00–09:00), 4000 lx for 15 min (09:00–09:15) and 2500 lx for final 15 min (09:15–09:30) The light was a combination of daylight shining through the window, room lighting, and bright light exposure device. Provider: nurse Timing Start—postoperative day 2 Duration—2 h light exposure starting at 07:30 for 4 days (total time: 480 min) | Usual care | Incidence: DSM-IV-TR | Primary outcome: incidence Secondary outcome: rhythms in the activity and amount of movements at night as a proxy for sleeplessness, Heart rate variability and autonomic nervous system, and postoperative arrhythmia | From postoperative day 2 to postoperative day 5 Twice daily in the daytime and at night time | Incidence Exp: 1 (10%) Cont: 5 (42.7%) no significant difference |
| 8 | Van Rompaey 2012 Belgium | RCT | •136 patients ICU •Exp: 69 patients Cont: 67 patients •Age: 18 years or older •Prescreening: NEECHAM Scale | Intervention: ear plugs polyurethane Bilsom type Provider: assigned critical care nurse Timing 22:00–06:00 | No action | Incidence: NEECHAM | Primary outcome: Incidence Secondary outcome: Sleep perception | From 0hours to 96hrs Maximum of five nights assessed during each nursing shift, at 08.00, 16.00, and 22.00 | Incidence Exp: 20.3% Cont: 19.4% |
| 9 | Waszynski, 2018 United States | Single site RCT | •111 patients Acute care level one trauma center •Exp 1: 34 patients Exp 2: 41 patients Cont: 37 patients •Age: 18 years or older •Prescreening: Hospitalized patients experiencing hyperactive or mixed delirium and receiving continuous observation | Intervention: simulated family presence using pre-recorded video messages Watched a video on a DVD player placed on the over bed table located two feet in front of the participant Exp 1: view a 1-min family video message The message contained a personalized greeting delivered by one or more family members intended to provide a sense of calm and familiarity for the delirious participant Exp 2: view a 1-min nature videoA 1-min segment of a nature video containing images and sound of rain falling on colorful tropical plants or flowers was the attention control intervention Usual care also provided Provider: primary investigator (nurse) Timing: Start—administered the intervention immediately if the participant displayed any behaviors listed on the ABS Duration—1 min | Usual care | Severity: Agitated Behavior Scale | Primary outcome: agitation | immediately post intervention; 30-min post intervention Four time points (pre-intervention/baseline; during intervention; immediately post intervention; 30-min post intervention) | Severity Four time periods p < 0.001 Exp 1: 94.1% Cont: 29.7% Pre-intervention/baseline p = 0.071 Exp 1: 16 Exp 2: 17 Cont: 16 During intervention p < 0.001, d = 0.194 Exp 1: 14 Exp 2: 15 Cont: 16 Immediately post intervention p = 0.158 Exp 1: 14 Exp 2: 16 Cont: 16 30 min post intervention p = 0.971 Exp 1: 15 Exp 2: 15 Cont: 15 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lee, Y.; Lee, J.; Kim, J.; Jung, Y. Non-Pharmacological Nursing Interventions for Prevention and Treatment of Delirium in Hospitalized Adult Patients: Systematic Review of Randomized Controlled Trials. Int. J. Environ. Res. Public Health 2021, 18, 8853. https://doi.org/10.3390/ijerph18168853
Lee Y, Lee J, Kim J, Jung Y. Non-Pharmacological Nursing Interventions for Prevention and Treatment of Delirium in Hospitalized Adult Patients: Systematic Review of Randomized Controlled Trials. International Journal of Environmental Research and Public Health. 2021; 18(16):8853. https://doi.org/10.3390/ijerph18168853
Chicago/Turabian StyleLee, Yoonyoung, Jongmin Lee, Jeounghee Kim, and Youngsun Jung. 2021. "Non-Pharmacological Nursing Interventions for Prevention and Treatment of Delirium in Hospitalized Adult Patients: Systematic Review of Randomized Controlled Trials" International Journal of Environmental Research and Public Health 18, no. 16: 8853. https://doi.org/10.3390/ijerph18168853
APA StyleLee, Y., Lee, J., Kim, J., & Jung, Y. (2021). Non-Pharmacological Nursing Interventions for Prevention and Treatment of Delirium in Hospitalized Adult Patients: Systematic Review of Randomized Controlled Trials. International Journal of Environmental Research and Public Health, 18(16), 8853. https://doi.org/10.3390/ijerph18168853