Abstract
Background and Objectives: Significant progress has been made in skin cancer diagnosis, with a surge in available technologies in recent years. Despite this, the practical application and integration of these technologies in dermatology and plastic surgery remain uneven. Materials and Methods: A comprehensive 20-question survey was designed and distributed using online survey administration software (Google Forms, 2018, Google, Mountain View, CA, USA) from June 2023 to September 2023. The survey aimed to assess the knowledge and utilization of dermatologic diagnostic advancements among plastic surgeons in various European countries. Results: Data were obtained from 29 plastic surgeons across nine European countries, revealing a notable gap between diagnostic technologies and their routine use in surgical practice. The gap for some technologies was both cognitive and applicative; for electrical impedance spectroscopy (EIS) and multispectral imaging, only 6.9% of the sample knew of the technologies and no surgeons in the sample used them. In the case of other technologies, such as high-frequency ultrasound (HFUS), 72.4% of the sample knew about them but only 34.5% used them, highlighting a more significant application problem. Conclusions: Spotlighting this discrepancy provides a valuable foundation for initiating collaborative efforts between units and facilitating knowledge exchange among diverse specialists. This, in turn, contributes to advancing clinical practice by integrating the innovative opportunities presented by ongoing research.
Keywords:
surgery; plastic; search engine; dermatology; surgeons; Europe; software; surveys and questionnaires; dermato-oncology 1. Introduction
The incidence of skin cancer diagnoses globally is steadily rising due to an aging population and advances in diagnostic techniques [1].
Approximately one in three cancers diagnosed worldwide are skin cancers, with an estimated 2–3 million Nonmelanoma Skin Cancers (NMSCs) and 132,000 Melanoma Skin Cancers (MSCs) diagnosed annually [2]. Despite these alarming numbers, the integration of novel diagnostic approaches into clinical practice has been slow. Other data concerning the United States and Europe are even more impressive: 247,894 NMSC cases and 101,507 MSC cases in the European Union for the year 2022 [3] and 97,610 MSC cases in the United States for the year 2023 [4]. Moreover, especially with regard to NMSCs, the number appears to be greatly underestimated; actually, in some health systems, there is no requirement to report this type of diagnosis.
In recent years, technological advancements have transformed skin cancer diagnosis, moving from subjective clinical assessments to computer-assisted or artificial intelligence-driven systems. However, these advancements have not seamlessly integrated into everyday clinical practice, especially in smaller health care settings [5]. These systems compile a vast array of global data by accumulating the experience of numerous centers, resulting in sensitivity levels approaching 100 percent and specificities exceeding 90 percent.
The future looks promising as we steadily move closer to a more objective form of diagnosis. However, these diagnostic advancements are not accompanied by parallel progress in everyday clinical practice. It is important to note that these technologies primarily impact larger hospital and university settings and are less readily adaptable in smaller contexts [6].
This article addresses the noticeable gap between diagnostic advancements and daily surgical practices in the field of plastic surgery, where plastic surgeons often lack updated knowledge and access to cutting-edge diagnostic tools. To objectify this reflection, we focused our analysis on the knowledge and application of several diagnostic applications [7,8] (Table 1):

Table 1.
Main application modalities and diagnostic indications.
- − Adhesive patch biopsy (tape stripping mRNA);
- − EIS (electrical impedance spectroscopy);
- − Multispectral imaging;
- − High-frequency ultrasonography (HFUS);
- − Optical coherence tomography (OCT);
- − Reflectance confocal microscopy (RCM);
- − Artificial intelligence (AI) and computer analysis.
These various diagnostic instruments are useful in the diagnosis or indication for biopsy of suspicious skin neoformations for MSCs and NMSCs and have been newly introduced in dermato-oncology practice. Next, we analyzed their prevalence in the field of dermato-oncology in plastic surgery.
2. Materials and Methods
A 20-question survey was designed collaboratively by plastic surgeons and dermatologists actively engaged in dermato-oncologic surgery. The survey aimed to assess the understanding and utilization of diagnostic innovations in oncodermatologic surgery among plastic surgeons.
The purpose of the questionnaire was to assess, among an initial sample of plastic surgeons distributed throughout Europe, the level of understanding and effective utilization of diagnostic innovations in oncodermatologic surgery. The questionnaire was distributed by personal invitation through local and international networks to several members of national and international plastic surgery scientific societies to ascertain the perception, knowledge, and application of new diagnostic tools by plastic surgeons.
The surgeons contacted were all part of institutions considered to be referral centers for the treatment of cutaneous neoplasms. The inclusion criteria for these centers were the presence of a plastic surgery department and a dermatology department in the same hospital and the treatment of all cutaneous neoplasms (both NMSCs and MSCs), apart from sarcomas, the treatment of which is usually the responsibility of dedicated orthopedic teams (Table 2).
Table 2.
Inclusion criteria.
The survey was distributed anonymously to 50 plastic surgeons in nine European countries, all affiliated with institutions considered referral centers for cutaneous neoplasms. Twenty-nine complete questionnaires were obtained and rigorously analyzed. The questionnaire consisted of a total of 20 questions, with the first section focusing on physicians’ knowledge of diagnostic advances in oncodermatology and their involvement in treating patients. The second section addressed the routine use of emerging technologies in their daily practice, while the third section delved into the degree of collaboration with dermatology departments for skin cancer diagnosis and preoperative evaluations.
In addition, participants were asked to provide their perspectives on potential future applications of these new technologies, should they be available in their centers.
We selected a sample of surgeons to assay the knowledge and use of these technologies by plastic surgery specialists. We did not select dermatologists because, in this case, the problem would be mainly one of updating; as for surgeons, we essentially analyzed the distance between these professionals and the diagnostic advances in the field of oncologic dermatology. In fact, while the concept of division of expertise remains intact, the work of surgeons is strongly influenced by the lack of knowledge or application of these techniques.
Subsequently, the responses were meticulously reviewed and validated by the expert panel. This study was conducted in accordance with the Declaration of Helsinki. Personal data were processed in accordance with the European General Data Protection Regulation. Data were analyzed anonymously. Participants were informed in detail about the scope of the study and provided informed consent before initiation.
3. Results
3.1. General Results
Out of the 29 plastic surgeons surveyed, 48.3% performed more than ten oncodermatology surgeries per week, highlighting the active involvement of plastic surgeons in treating skin cancers. However, only 48.3% of these centers offered dermoscopy services in daily clinical practice.
3.2. Knowledge of Diagnostic Instruments
- Adhesive patch biopsy (tape stripping mRNA): Only 20.7% (n = 6) of our cohort knew about this technology and only 6.9% (n = 2) applied it (Table 3) (Figure 1).
Table 3. The extent of understanding and the accessibility of key diagnostic methods in oncodermatology among plastic surgeons.
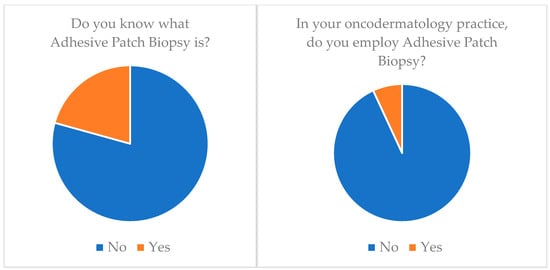 Figure 1. Adhesive patch biopsy (tape stripping mRNA) knowledge and application.
Figure 1. Adhesive patch biopsy (tape stripping mRNA) knowledge and application. - EIS (electrical impedance spectroscopy): Just 6.9% (n = 2) of our cohort knew about this technology and none of them applied it (n = 0) (Table 3) (Figure 2).
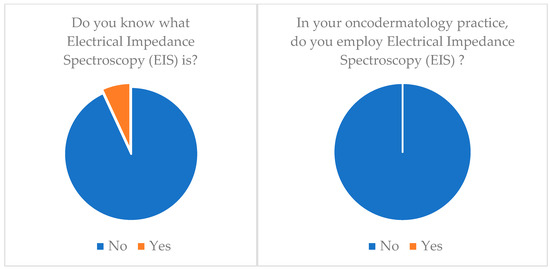 Figure 2. EIS (electrical impedance spectroscopy) knowledge and application.
Figure 2. EIS (electrical impedance spectroscopy) knowledge and application. - Multispectral imaging: Just 6.9% (n = 2) of our cohort knew about this technology and none of them applied it (n = 0) (Table 3).
- High-frequency ultrasonography (HFUS): 72.4% (n = 21) of our cohort knew about this technology but only 34.5% (n = 10) applied it (Table 3) (Figure 3).
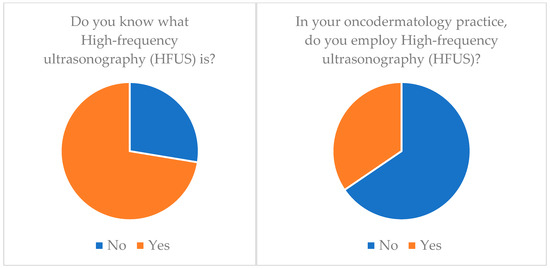 Figure 3. High-frequency ultrasonography (HFUS) knowledge and application.
Figure 3. High-frequency ultrasonography (HFUS) knowledge and application. - Optical coherence tomography (OCT): 55.2% (n = 16) of our cohort knew about this technology but only 20.7% (n = 6) applied it (Table 3) (Figure 4).
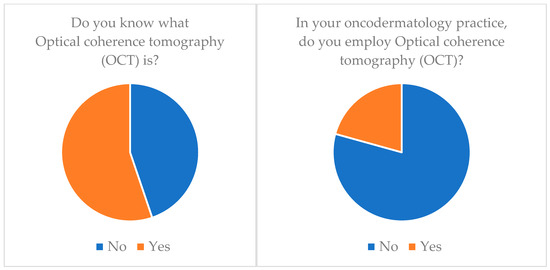 Figure 4. Optical coherence tomography (OCT) knowledge and application.
Figure 4. Optical coherence tomography (OCT) knowledge and application. - Confocal reflectance microscopy (RCM): Only 55.2% (n = 16) of our cohort knew about this technology and only 20.7% (n = 6) applied it (Table 3).
- Artificial intelligence (AI) and computer analysis: 72.4% (n = 21) of our cohort knew about this technology and only 13.8% (n = 4) applied it (Table 3).
In the case of skin cancer diagnosis, 72.4% (n = 21) of plastic surgery departments engaged in collaboration with a dermatology unit. However, when it comes to the preoperative evaluation of excision margins, only 27.6% (n = 8) of them worked in conjunction with dermatologists.
Regarding the consideration of these new diagnostic tools, they were considered useful in the totality of our sample. Of these, 34.5% (n = 10) said they planned to apply them in the future, 58.6% (n = 17) said they would employ them if they had them available at their center, and only 6.9% (n = 2) said they employed them regularly.
4. Discussion
The data from our sample quite clearly express the gap between surgical practice and diagnostic techniques (both basic techniques such as dermoscopy and more advanced ones). Although we have units that consistently practice dermatologic surgery, only 51.7% provide a dermoscopy service during daily clinical practice.
The study underscores a disconnect between surgical practices and diagnostic advancements, with only half of the surveyed plastic surgeons offering dermoscopy services. Despite awareness of technologies like high-frequency ultrasonography, optical coherence tomography, and artificial intelligence, their routine use in daily practice was limited.
Conversely, these methods would be particularly useful in different clinical scenarios. Here we explain its characteristics more extensively (Table 4).
Table 4.
Analysis of the characteristics and limitations of diagnostic techniques.
Adhesive patch biopsy (tape stripping mRNA) represents a noninvasive diagnostic technique with enormous potential and ease of use [9,10,17,18,19,20,21,22,23,24,25,26] (Table 5). Studies have focused on its utility in early melanoma diagnosis and prognostic definition, replacing or even in combination with classical histology. It is a procedure that involves simple taping of the pigmented neoformation and detection of the mRNA present in the stratum corneum; although there is no nucleus in this cell layer, in the case of neoplasia there is expression of these molecules through mechanisms not yet fully elucidated.
In this way, the presence of mRNA bound to different genes is detected; several proposals have been made on the batteries of genes to be analyzed. The use of 17 genes proposed by Wachsman provided 100% sensitivity and 88% specificity [19].
Gerami et al. proposed using only two genes (LINC00518 and PRAME) with a sensitivity of 91% and specificity of 69%, a method known as PLA (pigmented lesion assay) [17,18].
In contrast, the review by Thomsen et al. [9] indicates a sensitivity of 86.9% and specificity of 82.4% for a two-gene assay (LINC00518 and PRAME), while in an analysis of studies that included other genes, the sensitivity and specificity values ranged from 68.8 to 100 percent and 69.1 to 100 percent, respectively.
From an economic point of view, moreover, the method has costs comparable to those of classical histological examinations according to some authors, while according to a study by Hornberger, the economic savings of using PLA compared to a visualization and surgical biopsy procedure with histological examination would be 47% [24].
It thus represents an additional resource that can avoid unnecessary excisional biopsies and improve clinical and prognostic framing by detecting the presence of several genes.
EIS (electrical impedance spectroscopy) [5,21,27,28,29,30] (Table 5) is a method that studies changes in tissue electrical impedance, a value that changes as the histological characteristics of the neoplasm change. The variation in this value depends on tissue cellularity and water content. It should not be understood as a primarily diagnostic tool, but as an auxiliary tool in the choice between excision and observation; it can detect both MSCs and NMSCs, although it has critical issues with regard to the differential diagnosis of seborrheic keratoses and other limitations related to the presence of ulcerated or bleeding lesions and the variation in values related to skin characteristics in different body areas. It also has high sensitivity in the diagnosis of melanoma but significantly lower specificity.
Multispectral imaging (Table 5), on the other hand, is a noninvasive and fully automated lesion analysis tool.
The most studied device using this technology is the MelaFind (STRATA Skin Sciences; MELA Sciences Inc., Irvington, NY, USA) [11]. This instrument allows imaging up to 2.5 mm below the skin surface and analyzes 10 digital images by scanning the light reflectance distribution pattern.
It appears to possess high sensitivity (98.3%) but low specificity (9.9%), although the data vary widely among studies; its role should be to assist clinical and dermoscopy decision making, not to replace it. The ratio of MSC to benign pigmented lesions is 1:8–1:10, which coincides with that of good dermoscopy combined with clinical assessments.
The picture is slightly different regarding high-frequency ultrasound (HFUS) [31,32,33] (Table 5). In fact, only 27.6 percent of the sample did not know what it was, but in this case, despite knowledge, 65.5 percent of the sample did not employ it in daily practice (Table 2).
HFUS is an imaging technique that uses high-frequency sound waves to produce high-resolution, real-time images of tissues below the skin surface to a depth of about 15 mm. It is particularly useful for assessing the depth and characteristics of skin lesions. It provides valuable information about the extent of tumor infiltration and helps plan surgical procedures.
HFUS helps dermatologists and plastic surgeons determine the appropriate treatment approach for skin cancers and other dermatologic conditions.
Indeed, among the advantages of this procedure is that it provides different patterns depending on the lesions, thus being applicable as a diagnostic aid for both MSCs and NSCs and other types of skin pathology. Its disadvantages, on the other hand, include the fact that it is an operator-dependent method and lacks the ability to distinguish the cellularity of the tissue; for these reasons, although it is of great interest, it is not yet a tool capable of making diagnoses and is not able to replace histology.
Optical coherence tomography (OCT) [34,35,36] (Table 5) and confocal reflection microscopy (RCM), on the other hand, were known to only part of the sample, but their use was still minimal (employed by only 20.7% of our cohort). Optical coherence tomography (OCT) is a noninvasive imaging technique that uses light waves to capture detailed, high-resolution cross-sectional images of biological tissues, including skin. It operates on the principle of measuring the time delay of reflected light to create detailed images of tissue microstructures. It allows clinicians to visualize skin layers and structures in real time. It is particularly useful for assessing skin lesions, measuring their depth, and differentiating between benign and malignant skin conditions. OCT provides valuable information for diagnosis and treatment planning.
On the other hand, reflectance confocal microscopy (RCM) [37,38] (Table 5) is an advanced imaging technique that enables real-time, high-resolution visualization of skin at the cellular level. It utilizes a laser to capture images of skin tissue by measuring the reflection of light from different depths within the skin. RCM is particularly valuable in dermatology for in vivo diagnosis of skin lesions. It allows dermatologists to examine cellular structures, identify abnormal cells, and assess the margins of skin lesions. RCM aids in the early detection and accurate diagnosis of skin cancers, including melanoma. The possibilities of this technology are remarkable; in fact, it allows in vivo histology, enabling the patterns of different skin lesions to be distinguished; the disadvantages, however, are many, starting with the depth of analysis, which is limited to the papillary dermis (about 200 μm), followed by the cost of the machine and the limited dissemination and expertise in reading the results.
Finally, most of the sample said they knew what machine learning and computer diagnostics are, but at the same time many of them did not employ them in their daily practice. Artificial intelligence (AI) [39,40] (Table 5) and computer-based diagnosis refer to the integration of machine learning algorithms and computer technology in oncodermatology. These systems analyze and interpret dermatological images, including photographs and histopathological slides, to assist in diagnosing skin conditions. AI and computer-based diagnosis can rapidly process large datasets, identify patterns, and provide diagnostic recommendations. These tools are increasingly used in dermatology for the early detection of skin cancers, such as melanoma, and for the automated analysis of skin lesions. They enhance diagnostic accuracy and efficiency in clinical practice.
Further thought needs to be given to the possibility of applying machine learning and artificial intelligence to smartphone applications. The use of smartphone applications to diagnose skin lesions by capturing them with increasingly better-resolution cameras is not a new idea. A number of apps capable of making diagnoses have long been placed in app stores, but often these apps have turned out to be unsupported by real scientific evidence, while still others were based on partly outdated basic principles, such as the ABCDE criteria [39].
The basic idea, however, is intriguing, and the use of artificial intelligence and machine learning could enable the development of more reliable applications supported by stronger evidence.
At the same time, it would allow remote dermatology consultations to be provided with greater confidence, expanding treatment options in economically disadvantaged or rural settings [6,41].
Table 5.
Some of the main and more recent studies on reviewed techniques.
Table 5.
Some of the main and more recent studies on reviewed techniques.
| Author | Year | Journal | Methodology | Techniques |
|---|---|---|---|---|
| Lassau et al. [33] | 1997 | Radiographics | Original Article | HFUS |
| Moncrieff et al. [22] | 2002 | Br J Dermatol | Original Article | MI |
| Bessoud et al. [12] | 2003 | Ultrasound Med Biol | Original Article | HFUS |
| Glickman et al. [42] | 2003 | Skin Res Technol | Original Article | EIS |
| Ruocco et al. [43] | 2004 | Dermatol Surg | Review Article | RCM |
| Har-shai et al. [44] | 2005 | Plast Reconstr Surg | Multicenter Study | EIS |
| Machet et al. [45] | 2009 | Ultrasound Med Biol | Review Article | HFUS |
| Wachsman et al. [19] | 2011 | Br J Dermatol | Original Article | APB |
| Monheit et al. [11] | 2011 | Arch Dermatol | Original Article | MI |
| Crisan et al. [31] | 2013 | Arch Dermatol Res | Original Article | HFUS |
| Gerami et al. [10] | 2014 | J Am Acad Dermatol | Original Article | APB |
| Malvehy et al. [5] | 2014 | Br J Dermatol | Clinical Trial | MI |
| Meyer et al. [46] | 2014 | Br J Dermatol | Original Article | HFUS, OCT |
| Longo et al. [47] | 2014 | J Am Acad Dermatol | Original Article | RCM |
| March et al. [8] | 2015 | J Am Acad Dermatol | Review Article | EIS, MI |
| Markowitz et al. [13] | 2015 | J Clin Aesthet Dermatol | Original Article | OCT |
| Gambichler et al. [14] | 2015 | J Eur Acad Dermatol Venereol | Original Article | OCT |
| Olsen et al. [34] | 2016 | Photodiagn Photodyn Ther | Original Article | OCT |
| Que et al. [15] | 2016 | Dermatol Clin | Original Article | RCM |
| Borsari et al. [16] | 2016 | JAMA Dermatol | Original Article | RCM |
| Guilera et al. [48] | 2016 | Dermatol Clin | Review Article | RCM |
| Ferris et al. [17] | 2017 | JAMA Dermatol | Original Article | APB |
| Gerami et al. [18] | 2017 | J Am Acad Dermatol | Original Article | APB |
| Welzel et al. [28] | 2017 | J Dtsch Dermatol Ges | Review Article | EIS, OCT, RCM, MI |
| Braun et al. [29] | 2017 | Dermatol Clin | Original Article | EIS |
| Niculescu et al. [49] | 2017 | Photodiagn Photodyn Ther | Original Article | OCT |
| Heibel et al. [7] | 2020 | Am J Clin Dermatol | Review Article | APB; EIS, MI; HFUS; OCT; RCM |
| Chu et al. [39] | 2020 | Front Med | Review Article | AI |
| Pathania et al. [25] | 2022 | J Cosmet Dermatol | Review Article | APB; EIS, MI; HFUS; OCT; RCM: AI |
| Owida et al. [50] | 2022 | J Skin Cancer | Review Article | MI; HUFS; OCT; RCM |
| Thomsen et al. [9] | 2023 | Skin Res Technol | Systematic Review | APB |
APB: adhesive patch biopsy; EIS: electrical impedance spectroscopy; MI: multispectral imaging; HFUS: high-frequency ultrasonography; OCT: optical coherence tomography; RCM: reflectance confocal microscopy; AI: computer-assisted diagnosis and artificial intelligence.
Our sample data reveal a significant disconnection between dermatological and surgical practices. To illustrate this point, dermoscopy is available in only 50% of cases, with collaboration with dermatology units for diagnosis occurring in 72.4% of cases but only in 27.6% of cases for preoperative margin assessment. Clearly, there exists a noticeable gap in health care practices [31,51].
Although theoretically available, these technologies are not being applied due to lack of communication and knowledge integration. Today, health care systems tend to separate the clinical and diagnostic aspects from the surgical procedure required for the same pathology.
From the perspective of plastic surgeons, moreover, the approach to pathology is often surgical even when it may not be necessary. Indeed, the possibilities and reconstructive capabilities of dermato-oncology drive the surgeon to an often more aggressive approach than the dermatologist. Greater integration here, too, would lead to better selection of surgical patients; for example, consider the 1:8 ratio in diagnoses of excised melanomas versus excised benign pigmented lesions of experienced dermatologists compared with the ratio of more than 1:30 of other specialists such as plastic surgeons [7]. In plastic surgery, moreover, functionally and aesthetically adequate reconstruction is the standard of care [52,53,54,55]. Increasing attention is being paid to decreasing the surgical impact, both demolitive and reconstructive, for the patient, seeking solutions that are satisfactory in terms of form and function and minimally invasive and debilitating. An example of this trend comes to us from orthoplastic and breast oncoplasty, which represent two important examples of the development of plastic surgery from the perspective of knowledge integration [56,57].
4.1. Skin Cancer Units
Disconnection of expertise is not uncommon in medicine; the distance and compartmentalization of expertise has been addressed before, as seen in the case of breast cancer. The creation of Breast Units, for example, stems from the need to centralize expertise within larger, more experienced centers and to coordinate the various clinical specialists needed for comprehensive management of the disease. Moreover, the criteria for establishing these centers are particularly rigorous and complex, thus ensuring better quality of care. Similarly, centralization is also desirable for an extremely prevalent disease such as skin cancer. Some examples of Skin Cancer Units already exist, but they are not yet sufficiently widespread. Similar reasoning has also been applied by some to the teaching of the subject, which should be considered as a single disease and not as two separate entities [58].
In our idea, this model of development should provide for common programs in the training pathway that would allow plastic surgeons, dermatologists, oncologists, radiotherapists, immunotherapists, and all the figures who revolve around the diagnosis and treatment of cutaneous oncologic pathology to work together during training, developing knowledge and awareness of the possibilities offered by the work of their colleagues.
This would lead to growth in terms of integration and interchange of knowledge; indeed, the different figures would be accustomed to calling on the professionalism of their colleagues knowing well the type of work or procedure needed on a case-by-case basis.
The centrality of training would thus shift from a “ specialist” to a “ pathological” view, while maintaining the profile of expertise and ultra-specialization needed to achieve optimal results.
The presence of dedicated units specializing in the treatment of cutaneous oncologic pathology, rather than the presence of plastic surgery or dermatology units dealing with it, underlies the same idea: responding quickly, effectively, and all-inclusively to the practical and clinical needs of the patient, rather than remaining anchored in our idea of specialization. We reiterate how this reasoning of ours does not challenge the system of specialization but proposes its better practical application.
This model of development also sees many difficulties in its application in relation to the material and economic possibilities of different health care systems and responds to health policy logic that is beyond the scope of our discussion.
As evidence of this reasoning and the need to integrate knowledge, it is sufficient to analyze the responses given in our sample regarding what people think about the use of these technologies in dermato-oncology surgery. The entire sample believed that these technologies are useful, and 58.6% of the sample said they would employ them if only they had the opportunity (Figure 5).
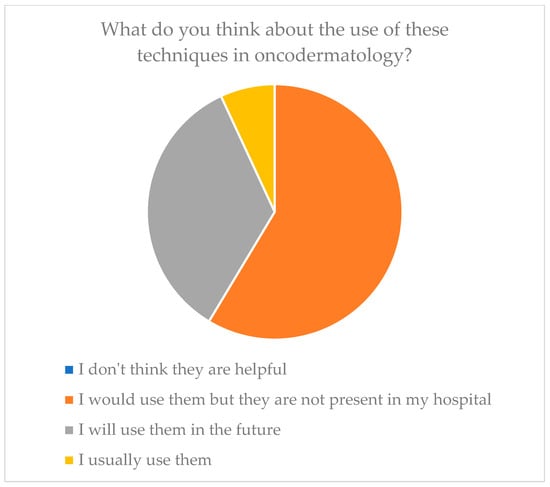
Figure 5.
Future resolutions of plastic surgeons toward these technologies.
It is also interesting to consider the duplicity of this gap. On the one hand, there is a cognizance gap; essentially, the surgeon does not know of the available technologies. Second, there is an application gap that lies in the material lack of these devices. Interesting examples of this dual gap are OCT and HFUS; in fact, 55.2% of the sample knew what OCT is but only 20.7% employed it, and at the same time 72.4% of the sample knew what HFUS is but only 34.5% employed it.
In the case of EIS and multispectral imaging, however, this double gap is more uniform, lacking both the knowledge and application components.
The problem of disconnection of clinical practice from diagnostic possibilities thus seems to have a dual motivation: cognizant and material.
4.2. Limitations of the Study
The purpose of our study was to verify the level of knowledge of these technologies and their effective use. The data provided by the study are interesting and highlight a phenomenon of deviation of clinical practice in plastic surgery from the state of the art in the diagnosis of skin neoformations.
However, our study has limitations related to the sample; in fact, on the one hand, the selection of plastic surgeons belonging to national and international scientific societies distributed over a wide geographic area and the choice of different health care and administrative contexts allows us to have a broad view of the problem; on the other hand, in order to have a global view, we would need to enlarge our sample.
In this context, these initial data of ours are intended to highlight a phenomenon and inspire further studies and actions aimed at bridging this gap between practice and theory.
5. Conclusions
In conclusion, the trends that emerged from our data suggest the need for better integration and communication between different disciplines. In particular, the creation of clinical pathways, dedicated treatment units, and common training paths [58,59] for multiple specialties in dermatosurgery could lead to a greater mixing of expertise and a more uniform and comprehensive patient care capability.
In the case of skin cancers, in fact, daily practice seems to be far from the possibilities that research offers us, although there is a good willingness on the part of clinicians for greater collaboration. The perspective for the future should be to combine diagnostic and surgical expertise and provide skin cancer patients with comprehensive, disease-centered care.
Hence, again, the importance of establishing the concept of comprehensive patient care, perhaps through the establishment of Skin Cancer Units.
Author Contributions
Conceptualization, G.D. and M.S.; methodology, M.P., G.D. and J.H.; software, L.L.; validation, E.C. and A.B.; formal analysis, V.M.M.; investigation, G.D.; resources, F.G.L., J.H. and M.P.; data curation, M.S.; writing—original draft preparation, G.D.; writing—review and editing, M.S.; visualization, G.D.; supervision, L.L.; project administration, L.L. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki. This study did not require ethical approval.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The data presented in this study are available on request from the corresponding author. The data are not publicly available due toprivacy of research participants.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Urban, K.; Mehrmal, S.; Uppal, P.; Giesey, R.L.; Delost, G.R. The global burden of skin cancer: A longitudinal analysis from the Global Burden of Disease Study, 1990–2017. JAAD Int. 2021, 2, 98–108. [Google Scholar] [CrossRef] [PubMed]
- WHO. Cancer Today, International Agency for Research on Cancer. Available online: https://gco.iarc.fr/today/online-analysis-table?v=2020&mode=cancer&mode_population=continents&population=900&populations=900&key=asr&sex=0&cancer=39&type=0&statistic=5&prevalence (accessed on 25 September 2023).
- ECIS—European Cancer Information System. Available online: https://ecis.jrc.ec.europa.eu/explorer.php?$0-0$1-All$2-All$4-1,2$3-27$6-0,85$5-2022,2022$7-7$CEstByCountry$X0_8-3$X0_19-AE27$X0_20-No$CEstBySexByCountry$X1_8-3$X1_19-AE27$X1_-1-1$CEstByIndiByCountry$X2_8-3$X2_19-AE27$X2_20-No$CEstRelative$X3_8-3$X3_9-AE27$X3_19-AE27$CEstByCountryTable$X4_19-AE27 (accessed on 12 September 2023).
- American Cancer Society. Facts & Figures 2023; American Cancer Society: Atlanta, GA, USA, 2023; Available online: https://www.cancer.org/cancer/types/melanoma-skin-cancer/about/key-statistics.html#:~:text=About%2097%2C610%20new%20melanomas%20will,5%2C420%20men%20and%202%2C570%20women (accessed on 13 September 2023).
- Malvehy, J.; Hauschild, A.; Curiel-Lewandrowski, C.; Mohr, P.; Hofmann-Wellenhof, R.; Motley, R.; Berking, C.; Grossman, D.; Paoli, J.; Loquai, C.; et al. Clinical performance of the Nevisense system in cutaneous melanoma detection: An international, multicentre, prospective and blinded clinical trial on efficacy and safety. Br. J. Dermatol. 2014, 171, 1099–1107. [Google Scholar] [CrossRef]
- Townsend, T. Diagnosis and management of melanoma in a rural general practice. J. Prim. Health Care 2018, 10, 207–209. [Google Scholar] [CrossRef]
- Heibel, H.D.; Hooey, L.; Cockerell, C.J. A Review of Noninvasive Techniques for Skin Cancer Detection in Dermatology. Am. J. Clin. Dermatol. 2020, 21, 513–524. [Google Scholar] [CrossRef] [PubMed]
- March, J.; Hand, M.; Grossman, D. Practical application of new technologies for melanoma diagnosis: Part I. Noninvasive approaches. J. Am. Acad. Dermatol. 2015, 72, 929–941, quiz 941–942; Erratum in J. Am. Acad. Dermatol. 2015, 73, 720. [Google Scholar] [CrossRef]
- Thomsen, I.M.N.; Heerfordt, I.M.; Karmisholt, K.E.; Mogensen, M. Detection of cutaneous malignant melanoma by tape stripping of pigmented skin lesions—A systematic review. Skin Res. Technol. 2023, 29, e13286. [Google Scholar] [CrossRef] [PubMed]
- Gerami, P.; Alsobrook JP 2nd Palmer, T.J.; Robin, H.S. Development of a novel noninvasive adhesive patch test for the evaluation of pigmented lesions of the skin. J. Am. Acad. Dermatol. 2014, 71, 237–244. [Google Scholar] [CrossRef] [PubMed]
- Monheit, G.; Cognetta, A.B.; Ferris, L.; Rabinovitz, H.; Gross, K.; Martini, M.; Grichnik, J.M.; Mihm, M.; Prieto, V.G.; Googe, P.; et al. The performance of MelaFind: A prospective multicenter study. Arch. Dermatol. 2011, 147, 188–194. [Google Scholar] [CrossRef] [PubMed]
- Bessoud, B.; Lassau, N.; Koscielny, S.; Longvert, C.; Avril, M.F.; Duvillard, P.; Rouffiac, V.; Leclère, J.; Roche, A. High-frequency sonography and color Doppler in the management of pigmented skin lesions. Ultrasound. Med. Biol. 2003, 29, 875–879. [Google Scholar] [CrossRef]
- Markowitz, O.; Schwartz, M.; Feldman, E.; Bienenfeld, A.; Bieber, A.K.; Ellis, J.; Alapati, U.; Lebwohl, M.; Siegel, D.M. Evaluation of Optical Coherence Tomography as a Means of Identifying Earlier Stage Basal Cell Carcinomas while Reducing the Use of Diagnostic Biopsy. J. Clin. Aesthet. Dermatol. 2015, 8, 14–20. [Google Scholar]
- Gambichler, T.; Schmid-Wendtner, M.H.; Plura, I.; Kampilafkos, P.; Stücker, M.; Berking, C.; Maier, T. A multicentre pilot study investigating high-definition optical coherence tomography in the differentiation of cutaneous melanoma and melanocytic naevi. J. Eur. Acad. Dermatol. Venereol. 2015, 29, 537–541. [Google Scholar] [CrossRef] [PubMed]
- Que, S.K.; Grant-Kels, J.M.; Rabinovitz, H.S.; Oliviero, M.; Scope, A. Application of Handheld Confocal Microscopy for Skin Cancer Diagnosis: Advantages and Limitations Compared with the Wide-Probe Confocal. Dermatol. Clin. 2016, 34, 469–475. [Google Scholar] [CrossRef]
- Borsari, S.; Pampena, R.; Lallas, A.; Kyrgidis, A.; Moscarella, E.; Benati, E.; Raucci, M.; Pellacani, G.; Zalaudek, I.; Argenziano, G.; et al. Clinical Indications for Use of Reflectance Confocal Microscopy for Skin Cancer Diagnosis. JAMA Dermatol. 2016, 152, 1093–1098. [Google Scholar] [CrossRef] [PubMed]
- Ferris, L.K.; Jansen, B.; Ho, J.; Busam, K.J.; Gross, K.; Hansen, D.D.; Alsobrook, J.P.; Yao, Z.; Peck, G.L.; Gerami, P. Utility of a Noninvasive 2-Gene Molecular Assay for Cutaneous Melanoma and Effect on the Decision to Biopsy. JAMA Dermatol. 2017, 153, 675–680. [Google Scholar] [CrossRef] [PubMed]
- Gerami, P.; Yao, Z.; Polsky, D.; Jansen, B.; Busam, K.; Ho, J.; Martini, M.; Ferris, L.K. Development and validation of a noninvasive 2-gene molecular assay for cutaneous melanoma. J. Am. Acad. Dermatol. 2017, 76, 114–120.e2. [Google Scholar] [CrossRef]
- Wachsman, W.; Morhenn, V.; Palmer, T.; Walls, L.; Hata, T.; Zalla, J.; Scheinberg, R.; Sofen, H.; Mraz, S.; Gross, K.; et al. Noninvasive genomic detection of melanoma. Br. J. Dermatol. 2011, 164, 797–806. [Google Scholar] [CrossRef]
- Tran, K.T.; Wright, N.A.; Cockerell, C.J. Biopsy of the pigmented lesion--when and how. J. Am. Acad. Dermatol. 2008, 59, 852–871. [Google Scholar] [CrossRef]
- Wassef, C.; Rao, B.K. Uses of non-invasive imaging in the diagnosis of skin cancer: An overview of the currently available modalities. Int. J. Dermatol. 2013, 52, 1481–1489. [Google Scholar] [CrossRef]
- Moncrieff, M.; Cotton, S.; Claridge, E.; Hall, P. Spectrophotometric intracutaneous analysis: A new technique for imaging pigmented skin lesions. Br. J. Dermatol. 2002, 146, 448–457. [Google Scholar] [CrossRef]
- Lezcano, C.; Jungbluth, A.A.; Nehal, K.S.; Hollmann, T.J.; Busam, K.J. PRAME Expression in Melanocytic Tumors. Am. J. Surg. Pathol. 2018, 42, 1456–1465. [Google Scholar] [CrossRef]
- Hornberger, J.; Siegel, D.M. Economic Analysis of a Noninvasive Molecular Pathologic Assay for Pigmented Skin Lesions. JAMA Dermatol. 2018, 154, 1025–1031. [Google Scholar] [CrossRef]
- Pathania, Y.S.; Apalla, Z.; Salerni, G.; Patil, A.; Grabbe, S.; Goldust, M. Non-invasive diagnostic techniques in pigmentary skin disorders and skin cancer. J. Cosmet. Dermatol. 2022, 21, 444–450. [Google Scholar] [CrossRef]
- Ferris, L.K.; Gerami, P.; Skelsey, M.K.; Peck, G.; Hren, C.; Gorman, C.; Frumento, T.; Siegel, D.M. Real-world performance and utility of a noninvasive gene expression assay to evaluate melanoma risk in pigmented lesions. Melanoma Res. 2018, 28, 478–482. [Google Scholar] [CrossRef] [PubMed]
- Svoboda, R.M.; Prado, G.; Mirsky, R.S.; Rigel, D.S. Assessment of clinician accuracy for diagnosing melanoma on the basis of electrical impedance spectroscopy score plus morphology versus lesion morphology alone. J. Am. Acad. Dermatol. 2019, 80, 285–287. [Google Scholar] [CrossRef]
- Welzel, J.; Schuh, S. Noninvasive diagnosis in dermatology. J. Dtsch. Dermatol. Ges. 2017, 15, 999–1016. [Google Scholar] [CrossRef]
- Braun, R.P.; Mangana, J.; Goldinger, S.; French, L.; Dummer, R.; Marghoob, A.A. Electrical Impedance Spectroscopy in Skin Cancer Diagnosis. Dermatol. Clin. 2017, 35, 489–493. [Google Scholar] [CrossRef] [PubMed]
- Aberg, P.; Nicander, I.; Holmgren, U.; Geladi, P.; Ollmar, S. Assessment of skin lesions and skin cancer using simple electrical impedance indices. Skin Res. Technol. 2003, 9, 257–261. [Google Scholar] [CrossRef] [PubMed]
- Crisan, M.; Crisan, D.; Sannino, G.; Lupsor, M.; Badea, R.; Amzica, F. Ultrasonographic staging of cutaneous malignant tumors: An ultrasonographic depth index. Arch. Dermatol. Res. 2013, 305, 305–313. [Google Scholar] [CrossRef]
- Crisan, D.; Wortsman, X.; Alfageme, F.; Catalano, O.; Badea, A.; Scharffetter-Kochanek, K.; Sindrilaru, A.; Crisan, M. Ultrasonography in dermatologic surgery: Revealing the unseen for improved surgical planning. J. Dtsch. Dermatol. Ges. 2022, 20, 913–926. [Google Scholar] [CrossRef]
- Lassau, N.; Spatz, A.; Avril, M.F.; Tardivon, A.; Margulis, A.; Mamelle, G.; Vanel, D.; Leclere, J. Value of high-frequency US for preoperative assessment of skin tumors. Radiographics 1997, 17, 1559–1565. [Google Scholar] [CrossRef]
- Olsen, J.; Themstrup, L.; De Carvalho, N.; Mogensen, M.; Pellacani, G.; Jemec, G.B. Diagnostic accuracy of optical coherence tomography in actinic keratosis and basal cell carcinoma. Photodiagn. Photodyn. Ther. 2016, 16, 44–49. [Google Scholar] [CrossRef] [PubMed]
- Boone, M.A.L.M.; Suppa, M.; Pellacani, G.; Marneffe, A.; Miyamoto, M.; Alarcon, I.; Ruini, C.; Hofmann-Wellenhof, R.; Malvehy, J.; Jemec, G.B.E.; et al. High-definition optical coherence tomography algorithm for discrimination of basal cell carcinoma from clinical BCC imitators and differentiation between common subtypes. J. Eur. Acad. Dermatol. Venereol. 2015, 29, 1771. [Google Scholar] [CrossRef] [PubMed]
- Boone, M.A.L.M.; Marneffe, A.; Suppa, M.; Miyamoto, M.; Alarcon, I.; Hofmann-Wellenhof, R.; Malvehy, J.; Pellacani, G.; Del Marmol, V. High-definition optical coherence tomography algorithm for the discrimination of actinic keratosis from normal skin and from squamous cell carcinoma. J. Eur. Acad. Dermatol. Venereol. 2015, 29, 1606–1615. [Google Scholar] [CrossRef]
- Haroon, A.; Shafi, S.; Rao, B.K. Using Reflectance Confocal Microscopy in Skin Cancer Diagnosis. Dermatol. Clin. 2017, 35, 457–464. [Google Scholar] [CrossRef] [PubMed]
- Carrera, C.; Marghoob, A.A. Discriminating Nevi from Melanomas: Clues and Pitfalls. Dermatol. Clin. 2016, 34, 395–409. [Google Scholar] [CrossRef]
- Chu, Y.S.; An, H.G.; Oh, B.H.; Yang, S. Artificial Intelligence in Cutaneous Oncology. Front. Med. 2020, 7, 318. [Google Scholar] [CrossRef]
- Yee, J.; Rosendahl, C.; Aoude, L.G. The role of artificial intelligence and convolutional neural networks in the management of melanoma: A clinical, pathological, and radiological perspective. Melanoma Res. 2023. [Google Scholar] [CrossRef]
- Giavina Bianchi, M.; Santos, A.; Cordioli, E. Dermatologists’ perceptions on the utility and limitations of teledermatology after examining 55,000 lesions. J. Telemed. Telecare 2021, 27, 166–173. [Google Scholar] [CrossRef]
- Glickman, Y.A.; Filo, O.; David, M.; Yayon, A.; Topaz, M.; Zamir, B.; Ginzburg, A.; Rozenman, D.; Kenan, G. Electrical impedance scanning: A new approach to skin cancer diagnosis. Skin Res. Technol. 2003, 9, 262–268. [Google Scholar] [CrossRef] [PubMed]
- Ruocco, E.; Argenziano, G.; Pellacani, G.; Seidenari, S. Noninvasive imaging of skin tumors. Dermatol. Surg. 2004, 30 Pt 2, 301–310. [Google Scholar] [CrossRef]
- Har-Shai, Y.; Glickman, Y.A.; Siller, G.; McLeod, R.; Topaz, M.; Howe, C.; Ginzburg, A.; Zamir, B.; Filo, O.; Kenan, G.; et al. Electrical impedance scanning for melanoma diagnosis: A validation study. Plast. Reconstr. Surg. 2005, 116, 782–790. [Google Scholar] [CrossRef]
- Machet, L.; Belot, V.; Naouri, M.; Boka, M.; Mourtada, Y.; Giraudeau, B.; Laure, B.; Perrinaud, A.; Machet, M.C.; Vaillant, L. Preoperative measurement of thickness of cutaneous melanoma using high-resolution 20 MHz ultrasound imaging: A monocenter prospective study and systematic review of the literature. Ultrasound. Med. Biol. 2009, 35, 1411–1420. [Google Scholar] [CrossRef]
- Meyer, N.; Lauwers-Cances, V.; Lourari, S.; Laurent, J.; Konstantinou, M.P.; Lagarde, J.M.; Krief, B.; Batatia, H.; Lamant, L.; Paul, C. High-frequency ultrasonography but not 930-nm optical coherence tomography reliably evaluates melanoma thickness in vivo: A prospective validation study. Br. J. Dermatol. 2014, 171, 799–805. [Google Scholar] [CrossRef] [PubMed]
- Longo, C.; Lallas, A.; Kyrgidis, A.; Rabinovitz, H.; Moscarella, E.; Ciardo, S.; Zalaudek, I.; Oliviero, M.; Losi, A.; Gonzalez, S.; et al. Classifying distinct basal cell carcinoma subtype by means of dermatoscopy and reflectance confocal microscopy. J. Am. Acad. Dermatol. 2014, 71, 716–724.e1. [Google Scholar] [CrossRef]
- Guilera, J.M.; Barreiro Capurro, A.; Carrera Alvárez, C.; Puig Sardá, S. The Role of Reflectance Confocal Microscopy in Clinical Trials for Tumor Monitoring. Dermatol. Clin. 2016, 34, 519–526. [Google Scholar] [CrossRef]
- Niculescu, L.; Bierhoff, E.; Hartmann, D.; Ruzicka, T.; Berking, C.; Braunmühl, T.V. Optical coherence tomography imaging of basal cell carcinoma undergoing photodynamic therapy: A pilot study. Photodiagn. Photodyn. Ther. 2017, 18, 133–137. [Google Scholar] [CrossRef] [PubMed]
- Owida, H.A. Developments and Clinical Applications of Noninvasive Optical Technologies for Skin Cancer Diagnosis. J. Skin Cancer. 2022, 2022, 9218847. [Google Scholar] [CrossRef]
- Marino, M.L.; Carrera, C.; Marchetti, M.A.; Marghoob, A.A. Practice Gaps in Dermatology: Melanocytic Lesions and Melanoma. Dermatol. Clin. 2016, 34, 353–362. [Google Scholar] [CrossRef] [PubMed]
- Losco, L.; Bolletta, A.; Pierazzi, D.M.; Spadoni, D.; Cuomo, R.; Marcasciano, M.; Cavalieri, E.; Roxo, A.C.; Ciamarra, P.; Cantisani, C.; et al. Reconstruction of the Nose: Management of Nasal Cutaneous Defects According to Aesthetic Subunit and Defect Size. A Review. Medicina 2020, 56, 639. [Google Scholar] [CrossRef]
- Bolletta, A.; Losco, L.; Pozzi, M.; Schettino, M.; Cigna, E. A Retrospective Study on Single-Stage Reconstruction of the Ear following Skin Cancer Excision in Elderly Patients. J. Clin. Med. 2022, 11, 838. [Google Scholar] [CrossRef]
- Paolino, G.; Cardone, M.; Didona, D.; Moliterni, E.; Losco, L.; Corsetti, P.; Schipani, G.; Lopez, T.; Calvieri, S.; Bottoni, U. Prognostic factors in head and neck melanoma according to facial aesthetic units. G. Ital. Dermatol. Venereol. 2020, 155, 41–45. [Google Scholar] [CrossRef]
- Lo Torto, F.; Redi, U.; Cigna, E.; Losco, L.; Marcasciano, M.; Casella, D.; Ciudad, P.; Ribuffo, D. Nasal Reconstruction with Two Stages versus Three Stages Forehead Fap: What is Better for Patients with High Vascular Risk? J. Craniofac. Surg. 2020, 31, e57–e60. [Google Scholar] [CrossRef] [PubMed]
- Govshievich, A.; Bauder, A.; Kovach, S.J.; Levin, L.S. Aesthetic Considerations in Extremity Salvage and Reconstruction. Plast. Reconstr. Surg. 2023, 151, 679e–687e. [Google Scholar] [CrossRef]
- Kenkel, J.M. Introducing Aesthetic Breast Reconstruction and Aesthetic Breast Surgery. Aesthetic Surg. J. 2023, 43, 525–526. [Google Scholar] [CrossRef] [PubMed]
- Al-Ghamdi, H.S. A novel approach to teaching dermatology and plastic surgery in a combined module for undergraduate medical students. Adv. Med. Educ. Pract. 2019, 10, 147–155. [Google Scholar] [CrossRef] [PubMed]
- Au, A.; Kim, J.B. Integration of plastic surgery into the undergraduate medical curriculum: The Norwich model and experience. Int. J. Med. Educ. 2012, 3, 14–16. [Google Scholar] [CrossRef]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).