
Systematic Review Shows Tele-Rehabilitation Might Achieve Comparable Results to Office-Based Rehabilitation for Decreasing Pain in Patients with Knee Osteoarthritis


Abstract
1. Introduction
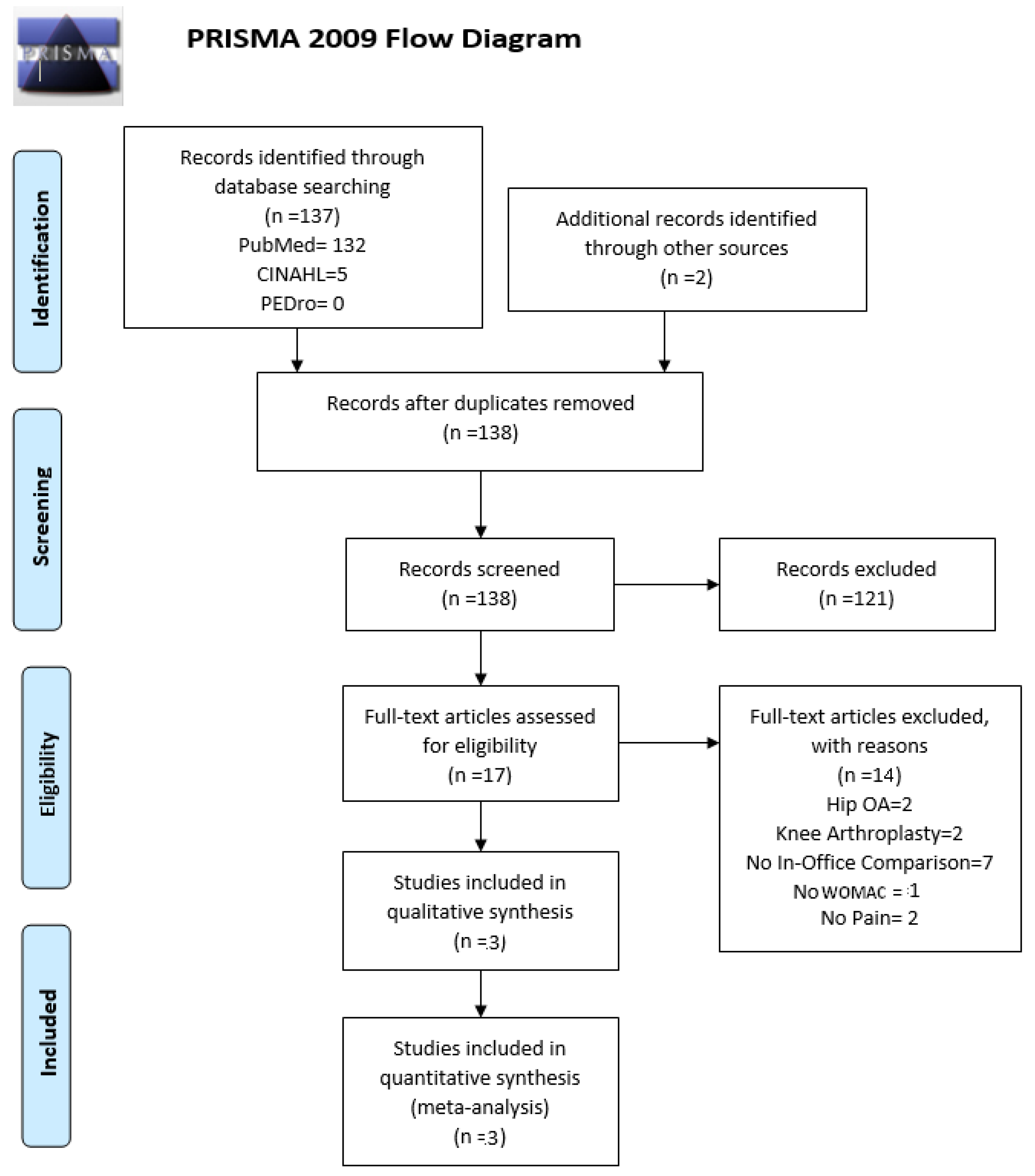
2. Materials and Methods
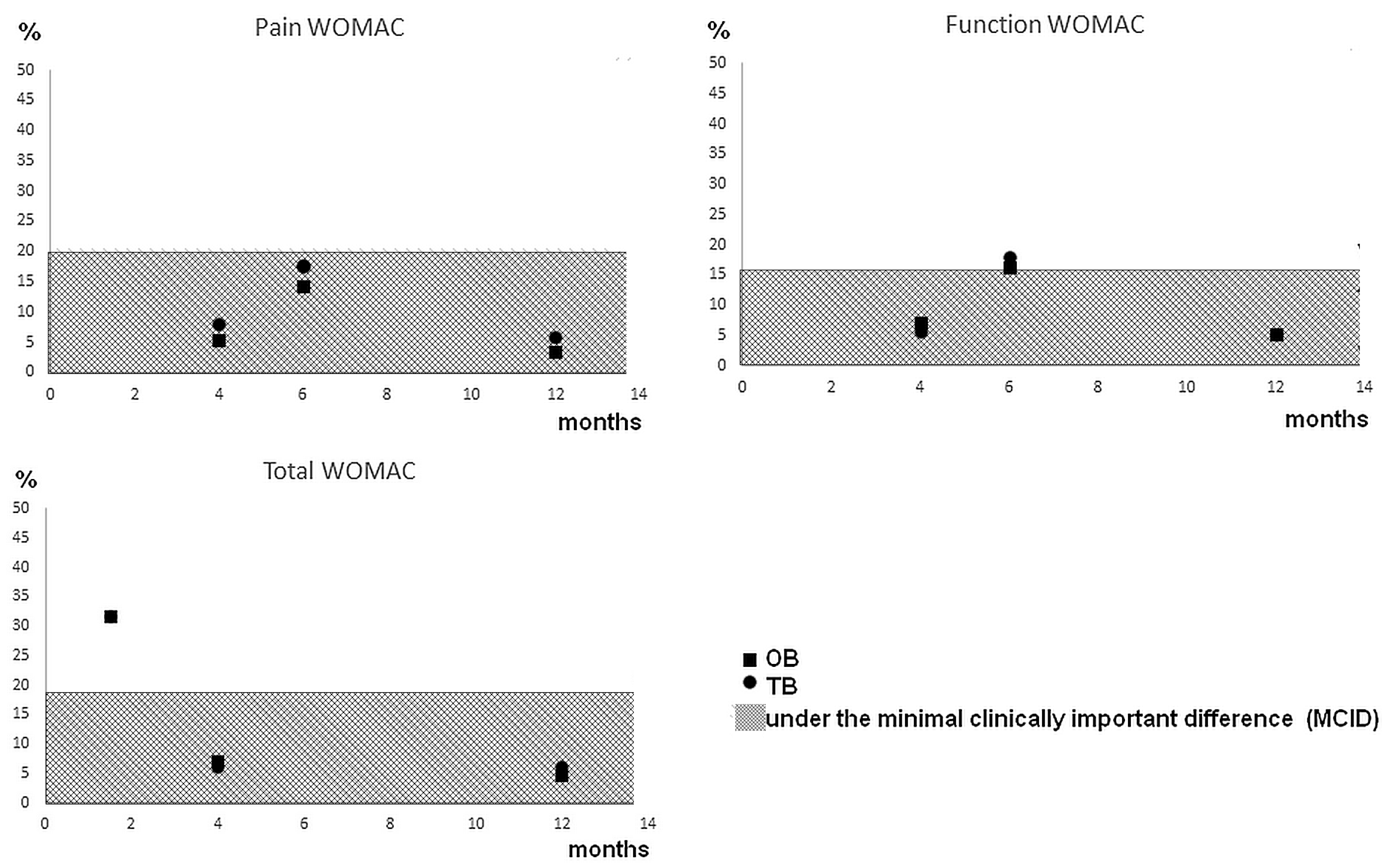
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Wieland, H.A.; Michaelis, M.; Kirschbaum, B.J.; Rudolphi, K.A. Osteoarthritis—An Untreatable Disease? Nat. Rev. Drug Discov. 2005, 4, 331–344. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Jordan, J.M. Epidemiology of Osteoarthritis. Clin. Geriatr. Med. 2010, 26, 355–369. [Google Scholar] [CrossRef]
- Berteau, J.-P.; Mielke, G.; Morlock, M.M.; Huber, G. Morphological and Biomechanical Analyses of the Subchondral Mineralized Zone in Human Sacral Facet Joints: Application to Improved Diagnosis of Osteoarthritis. Clin. Anat. 2015, 28, 538–544. [Google Scholar] [CrossRef]
- Manitta, L.; Fayolle, C.; Olive, L.; Berteau, J.-P. Nanoindentation of Subchondral Bone during Osteoarthritis Pathological Process Using Atomic Force Microscopy; Springer: Cham, Germany, 2019; pp. 505–517. [Google Scholar]
- Olive, L.; Gad, S.; Fining, M.; Thomas, L.; Berteau, J.P. Tissue and Movement Biomechanical Characterization of Osteoarthritis Progression in Mouse Knee Joint. Comput. Methods Biomech. Biomed. Engin. 2017, 20, 153–154. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Yelin, E.; Weinstein, S.; King, T. The Burden of Musculoskeletal Diseases in the United States. Semin. Arthritis Rheum. 2016, 46, 259–260. [Google Scholar] [CrossRef] [PubMed]
- Martin, A.B.; Hartman, M.; Benson, J.; Catlin, A.; National Health Expenditure Accounts Team. National Health Spending In 2014: Faster Growth Driven By Coverage Expansion And Prescription Drug Spending. Health Aff. 2016, 35, 150–160. [Google Scholar] [CrossRef] [PubMed]
- Brandt, K.D.; Dieppe, P.; Radin, E. Etiopathogenesis of Osteoarthritis. Med. Clin. N. Am. 2009, 93, 1–24. [Google Scholar] [CrossRef] [PubMed]
- Burr, D.B.; Gallant, M.A. Bone Remodelling in Osteoarthritis. Nat. Rev. Rheumatol. 2012, 8, 665–673. [Google Scholar] [CrossRef] [PubMed]
- Novak, S.; Guerron, G.; Zou, Z.; Cheung, G.; Berteau, J.-P. New Guidelines for Electrical Stimulation Parameters in Adult Patients with Knee Osteoarthritis Based on a Systematic Review of the Current Literature. Am. J. Phys. Med. Rehabil. 2020, 99, 682–688. [Google Scholar] [CrossRef]
- Deyle, G.D.; Henderson, N.E.; Matekel, R.L.; Ryder, M.G.; Garber, M.B.; Allison, S.C. Effectiveness of Manual Physical Therapy and Exercise in Osteoarthritis of the Knee: A Randomized, Controlled Trial. Ann. Intern. Med. 2000, 132, 173. [Google Scholar] [CrossRef]
- Farr, J.N.; Going, S.B.; McKnight, P.E.; Kasle, S.; Cussler, E.C.; Cornett, M. Progressive Resistance Training Improves Overall Physical Activity Levels in Patients With Early Osteoarthritis of the Knee: A Randomized Controlled Trial. Phys. Ther. 2010, 90, 356–366. [Google Scholar] [CrossRef] [PubMed]
- Richmond, J.; Hunter, D.; Irrgang, J.; Jones, M.H.; Levy, B.; Marx, R.; Snyder-Mackler, L.; Watters, W.C.; Haralson, R.H.; Turkelson, C.M.; et al. Treatment of Osteoarthritis of the Knee (Nonarthroplasty). J. Am. Acad. Orthop. Surg. 2009, 17, 591–600. [Google Scholar] [CrossRef] [PubMed]
- Shorter, E.; Sannicandro, A.J.; Poulet, B.; Goljanek-Whysall, K. Skeletal Muscle Wasting and Its Relationship With Osteoarthritis: A Mini-Review of Mechanisms and Current Interventions. Curr. Rheumatol. Rep. 2019, 21, 40. [Google Scholar] [CrossRef] [PubMed]
- Turolla, A.; Rossettini, G.; Viceconti, A.; Palese, A.; Geri, T. Musculoskeletal Physical Therapy During the COVID-19 Pandemic: Is Telerehabilitation the Answer? Phys. Ther. 2020, 100, 1260–1264. [Google Scholar] [CrossRef] [PubMed]
- Wang, C.-C.; Chao, J.-K.; Chang, Y.-H.; Chou, C.-L.; Kao, C.-L. Care for Patients with Musculoskeletal Pain during the COVID-19 Pandemic: Physical Therapy and Rehabilitation Suggestions for Pain Management. J. Chin. Med. Assoc. 2020, 83, 822–824. [Google Scholar] [CrossRef]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gotzsche, P.C.; Ioannidis, J.P.A.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA Statement for Reporting Systematic Reviews and Meta-Analyses of Studies That Evaluate Healthcare Interventions: Explanation and Elaboration. BMJ 2009, 339, b2700. [Google Scholar] [CrossRef]
- Allen, K.D.; Arbeeva, L.; Callahan, L.F.; Golightly, Y.M.; Goode, A.P.; Heiderscheit, B.C.; Huffman, K.M.; Severson, H.H.; Schwartz, T.A. Physical Therapy vs Internet-Based Exercise Training for Patients with Knee Osteoarthritis: Results of a Randomized Controlled Trial. Osteoarthr. Cartil. 2018, 26, 383–396. [Google Scholar] [CrossRef] [PubMed]
- Azma, K.; RezaSoltani, Z.; Rezaeimoghaddam, F.; Dadarkhah, A.; Mohsenolhosseini, S. Efficacy of Tele-Rehabilitation Compared with Office-Based Physical Therapy in Patients with Knee Osteoarthritis: A Randomized Clinical Trial. J. Telemed. Telecare 2018, 24, 560–565. [Google Scholar] [CrossRef] [PubMed]
- Bennell, K.L.; Campbell, P.K.; Egerton, T.; Metcalf, B.; Kasza, J.; Forbes, A.; Bills, C.; Gale, J.; Harris, A.; Kolt, G.S.; et al. Telephone Coaching to Enhance a Home-Based Physical Activity Program for Knee Osteoarthritis: A Randomized Clinical Trial: Exercise and Telephone Coaching for Knee OA. Arthritis Care Res. 2017, 69, 84–94. [Google Scholar] [CrossRef]
- Clement, N.D.; Bardgett, M.; Weir, D.; Holland, J.; Gerrand, C.; Deehan, D.J. What Is the Minimum Clinically Important Difference for the WOMAC Index After TKA? Clin. Orthop. 2018, 476, 2005–2014. [Google Scholar] [CrossRef] [PubMed]
- Odole, A.C.; Ojo, O.D. A Telephone-Based Physiotherapy Intervention for Patients with Osteoarthritis of the Knee. Int. J. Telerehabil. 2013, 5, 11–20. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Inclusion | Exclusion |
|---|---|
| Male or female | Knee arthroplasty |
| Randomized study | Osteoarthritis in other joints |
| Remote treatment | No-exercise treatments |
| Exercise | (e.g., injection therapy) |
| Age 35+ | |
| Western Ontario and McMaster Universities Osteoarthritis Index |
| Study | Interventions | n(Group) = Sample Size | Mean within-Group Difference from Baseline | Relative Risk Reduction | TR vs. OB (p Values) |
|---|---|---|---|---|---|
| Allen et al. [18] | Pain WOMAC-Month 4 | Pain WOMAC-Month 4 | 0.20 | ||
| TR | n(TR) = 112 | TR: 1.59 | RRR TR: 7.9% | ||
| OB | n(OB) = 129 | OB: 1.11 | RRR OB: 5.5% | ||
| CL | n(CL) = 63 | CL: 0.66 | RRR CL: 3.3% | ||
| Pain WOMAC-Month 12 | Pain WOMAC-Month 12 | 0.22 | |||
| TR: 1.15 | RRR TR: 5.7% | ||||
| OB: 0.7 | RRR OB: 3.5% | ||||
| CL: 0.64 | RRR CL: 3.2% | ||||
| Function WOMAC-Month 4 | Function WOMAC-Month 4 | 0.33 | |||
| TR: 3.74 | RRR TR: 5.5% | ||||
| OB: 4.77 | RRR OB: 7.0% | ||||
| CL: 2.3 | RRR CL: 3.4% | ||||
| Function WOMAC-Month 12 | Function WOMAC-Month12 | 0.93 | |||
| TR: 3.4 | RRR TR: 5.0% | ||||
| OB: 3.3 | RRR OB: 4.8% | ||||
| CL: 1.51 | RRR CL: 2.2% | ||||
| Total WOMAC-Month 4 | Total WOMAC-Month 4 | 0.65 | |||
| TR: 6.06 | RRR TR: 6.3% | ||||
| OB: 6.73 | RRR OB: 7.0% | ||||
| CL: 3.37 | RRR CL: 3.5% | ||||
| Total WOMAC-Month 12 | Total WOMAC-Month 12 | 0.51 | |||
| TR: 5.46 | RRR TR: 5.6% | ||||
| OB: 4.42 CL: 2.83 | RRR OB: 4.6% RRR CL: 2.9% | ||||
| Azma et al. [19] | Total WOMAC-Week 6 | Total WOMAC-Week 6 | 0.66 | ||
| TR | n(TR) = 27 | TR: 31.79 | RRR TR: 31.8% | ||
| OB | n(OB) = 27 | OB: 31.54 | RRR OB: 31.5% | ||
| Bennell et al. [20] | Pain WOMAC-Month 6 | Pain WOMAC-Month 6 | >0.05 | ||
| Rehabilitation + TR | n(TR) = 84 | TR: 3.5 | RRR TR: 17.5% | ||
| OB | n(OB) = 84 | OB: 2.9 | RRR OB: 14.5% | ||
| Function WOMAC-Month 6 | Function WOMAC-Month 6 | >0.05 | |||
| TR: 11.8 | RRR TR: 17.3% | ||||
| OB: 11.4 | RRR OB: 16.8% |
| Study | Was the Assignment of Patients to Treatments Randomized? | Were the Groups Similar at the Start of the Trial? | Aside from the Allocated Treatment, Were Groups Treated Equally? | Were All Patients Who Entered the Trial Accounted for? | Were Measures Objective or Were the Patients and Clinicians Kept “Blind” to Which Treatment Was Being Received? |
|---|---|---|---|---|---|
| Allen et al. [18] | Yes | Unclear | Yes | Yes | Unclear |
| Azma et al. [19] | Yes | Yes | Yes | Yes | Unclear |
| Bennell et al. [20] | Yes | Yes | Yes | Yes | Yes |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Latif-Zade, T.; Tucci, B.; Verbovetskaya, D.; Bialkin, E.; Ng, B.; Heddon, S.; Berteau, J.-P. Systematic Review Shows Tele-Rehabilitation Might Achieve Comparable Results to Office-Based Rehabilitation for Decreasing Pain in Patients with Knee Osteoarthritis. Medicina 2021, 57, 764. https://doi.org/10.3390/medicina57080764
Latif-Zade T, Tucci B, Verbovetskaya D, Bialkin E, Ng B, Heddon S, Berteau J-P. Systematic Review Shows Tele-Rehabilitation Might Achieve Comparable Results to Office-Based Rehabilitation for Decreasing Pain in Patients with Knee Osteoarthritis. Medicina. 2021; 57(8):764. https://doi.org/10.3390/medicina57080764
Chicago/Turabian StyleLatif-Zade, Tamila, Brian Tucci, Danna Verbovetskaya, Elizabeth Bialkin, Brian Ng, Stephan Heddon, and Jean-Philippe Berteau. 2021. "Systematic Review Shows Tele-Rehabilitation Might Achieve Comparable Results to Office-Based Rehabilitation for Decreasing Pain in Patients with Knee Osteoarthritis" Medicina 57, no. 8: 764. https://doi.org/10.3390/medicina57080764
APA StyleLatif-Zade, T., Tucci, B., Verbovetskaya, D., Bialkin, E., Ng, B., Heddon, S., & Berteau, J.-P. (2021). Systematic Review Shows Tele-Rehabilitation Might Achieve Comparable Results to Office-Based Rehabilitation for Decreasing Pain in Patients with Knee Osteoarthritis. Medicina, 57(8), 764. https://doi.org/10.3390/medicina57080764