
Differential Effects of Resistance- and Endurance-Based Exercise Programs on Muscular Fitness, Body Composition, and Cardiovascular Variables in Young Adult Women: Contextualizing the Efficacy of Self-Selected Exercise Modalities




Abstract
:1. Introduction
2. Methods
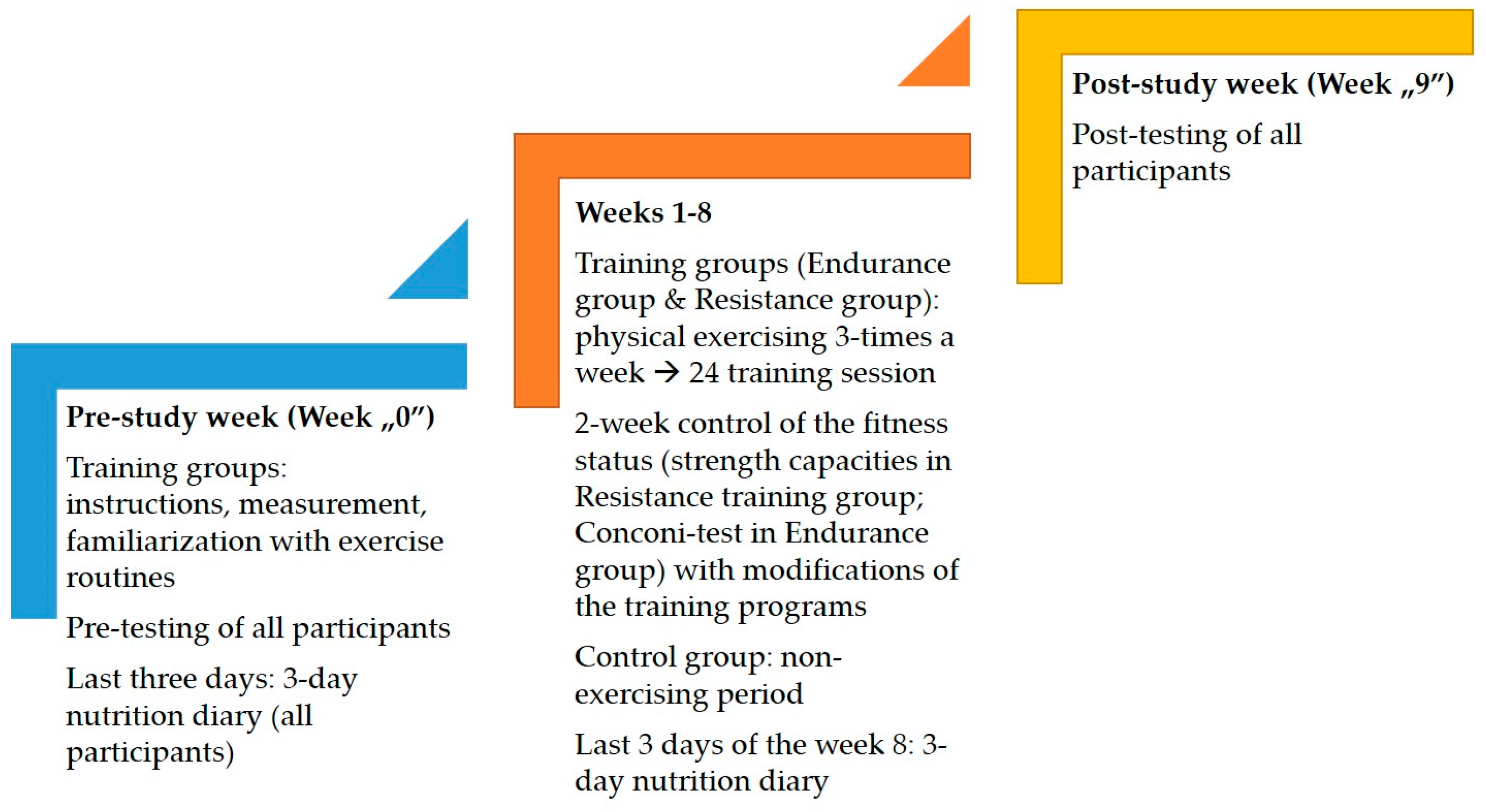
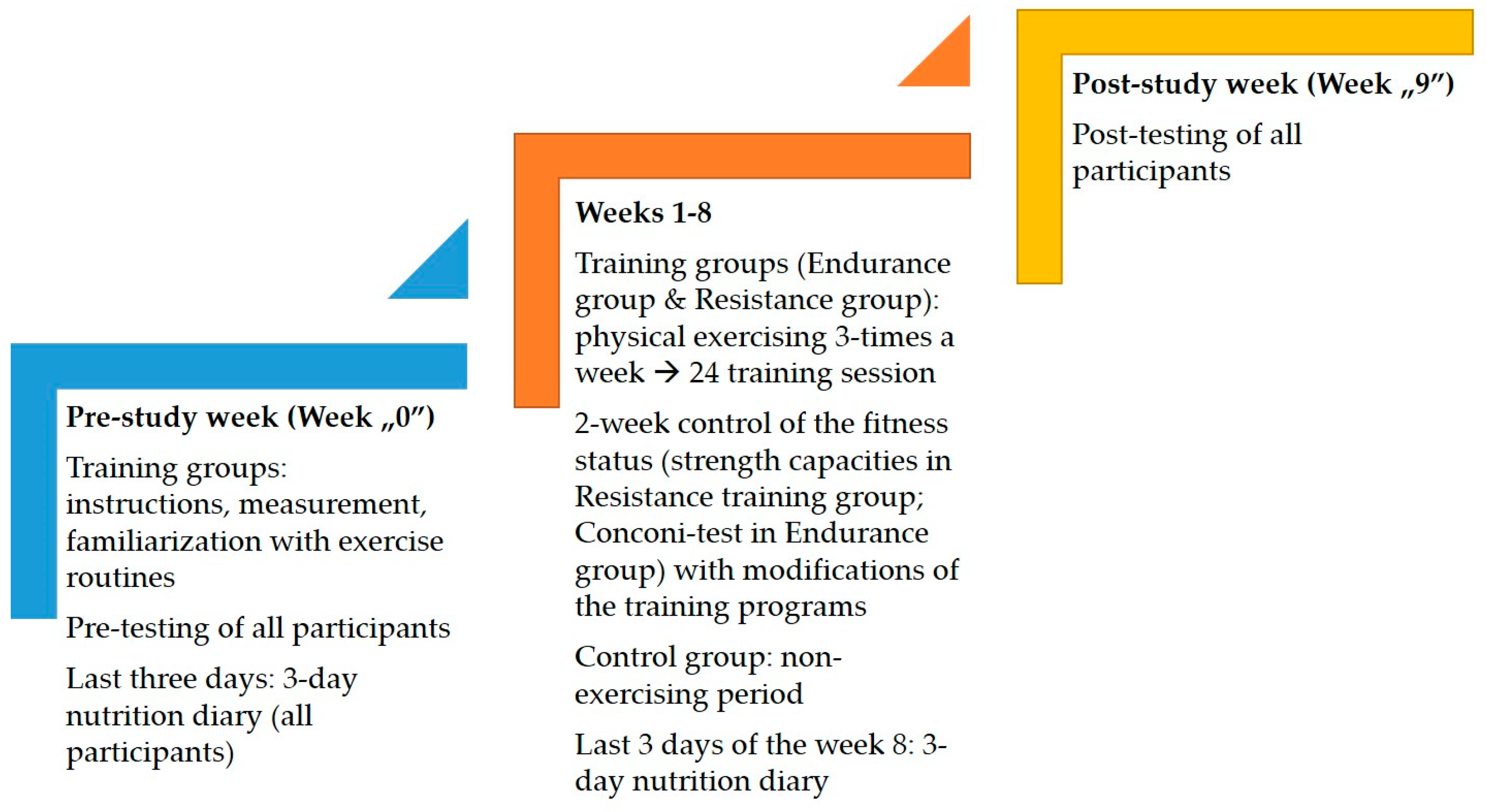
2.1. Participants and Design of the Study
2.2. Variables
2.3. Training Programs
2.4. Statistics
3. Results
4. Discussion
4.1. Anthropometry/Body Composition
4.2. BP and Heart Rate
4.3. Muscular Fitness
4.4. Limitations and Strengths
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Wilkins, E.; Wilson, L.; Wickramasinghe, K.; Bhatnagar, P.; Leal, J.; Luengo-Fernandez, R.; Burns, R.; Rayner, M.; Townsend, N. European Cardiovascular Disease Statistics 2017; European Heart Network: Brussels, Belgium, 2017. [Google Scholar]
- Yüksel, S.; Çoksevim, M.; Meriç, M.; Şahin, M. The Association of Body Composition Parameters and Simultaneously Measured Inter-Arm Systolic Blood Pressure Differences. Medicina 2021, 57, 384. [Google Scholar] [CrossRef]
- Moczulska, B.; Zechowicz, M.; Leśniewska, S.; Osowiecka, K.; Gromadziński, L. The Impact of Obesity on Nighttime Blood Pressure Dipping. Medicine 2020, 56, 700. [Google Scholar] [CrossRef]
- Cornelissen, V.A.; Smart, N.A. Exercise training for blood pressure: A systematic review and meta-analysis. J. Am. Heart Assoc. 2013, 2, e004473. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Santos, L.D.R.; de Araujo, S.S.; Vieira, E.F.D.S.; Estevam, C.D.S.; dos Santos, J.L.; Wichi, R.B.; Lima, F.B.; Carvalho, C.R.O.; Aidar, F.J.; Marçal, A.C. Effects of 12 Weeks of Resistance Training on Cardiovascular Risk Factors in School Adolescents. Medicina 2020, 56, 220. [Google Scholar] [CrossRef] [PubMed]
- Saqlain, M.; Riaz, A.; Malik, M.N.; Khan, S.; Ahmed, A.; Kamran, S.; Ali, H. Medication Adherence and Its Association with Health Literacy and Performance in Activities of Daily Livings among Elderly Hypertensive Patients in Islamabad, Pakistan. Medicine 2019, 55, 163. [Google Scholar] [CrossRef] [Green Version]
- Cornelissen, V.; Fagard, R.; Vanhees, L. The Impact of Dynamic Resistance Training on Blood Pressure and Other Cardiovascular Risk Factors: A Meta-Analysis of Randomized Controlled Trials: 5D.03. J. Hypertens. 2010, 28, e229–e230. [Google Scholar] [CrossRef]
- Ortega, F.B.; Ruiz, J.R.; Castillo, M.J.; Sjöström, M. Physical fitness in childhood and adolescence: A powerful marker of health. Int. J. Obes. 2008, 32, 1–11. [Google Scholar] [CrossRef] [Green Version]
- Pate, R.R. The Evolving Definition of Physical Fitness. Quest 1988, 40, 174–179. [Google Scholar] [CrossRef]
- Brown, D.A.; Miller, W.C. Normative data for strength and flexibility of women throughout life. Graefe’s Arch. Clin. Exp. Ophthalmol. 1998, 78, 77–82. [Google Scholar] [CrossRef] [PubMed]
- Mayeuf-Louchart, A.; Staels, B.; Duez, H. Skeletal muscle functions around the clock. Diabetes Obes. Metab. 2015, 17, 39–46. [Google Scholar] [CrossRef]
- de Baranda, P.S.; Ayala, F. Chronic flexibility improvement after 12 week of stretching program utilizing the ACSM recommendations: Hamstring flexibility. Int. J. Sports Med. 2010, 31, 389–396. [Google Scholar] [CrossRef] [PubMed]
- Mann, S.; Beedie, C.; Jimenez, A. Differential Effects of Aerobic Exercise, Resistance Training and Combined Exercise Modalities on Cholesterol and the Lipid Profile: Review, Synthesis and Recommendations. Sports Med. 2014, 44, 211–221. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Paoli, A.; Pacelli, Q.F.; Moro, T.; Marcolin, G.; Neri, M.; Battaglia, G.; Sergi, G.; Bolzetta, F.; Bianco, A. Effects of high-intensity circuit training, low-intensity circuit training and endurance training on blood pressure and lipoproteins in middle-aged overweight men. Lipids Health Dis. 2013, 12, 131. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ahmeti, G.B.; Idrizovic, K.; Elezi, A.; Zenic, N.; Ostojic, L. Endurance Training vs. Circuit Resistance Training: Effects on Lipid Profile and Anthropometric/Body Composition Status in Healthy Young Adult Women. Int. J. Environ. Res. Public Health 2020, 17, 1222. [Google Scholar] [CrossRef] [Green Version]
- Idrizovic, K.; Ahmeti, G.; Sekulic, D.; Zevrnja, A.; Ostojic, L.; Versic, S.; Zenic, N. Indices of Cardiovascular Health, Body Composition and Aerobic Endurance in Young Women; Differential Effects of Two Endurance-Based Training Modalities. Healthcare 2021, 9, 449. [Google Scholar] [CrossRef]
- Stangier, C.; Abel, T.; Mierau, J.; Hollmann, W.; Strüder, H.K. Effects of Cycling Versus Running Training on Sprint and Endurance Capacity in Inline Speed Skating. J. Sports Sci. Med. 2016, 15, 41–49. [Google Scholar]
- Hottenrott, K.; Ludyga, S.; Schulze, S. Effects of high intensity training and continuous endurance training on aerobic capacity and body composition in recreationally active runners. J. Sports Sci. Med. 2012, 11, 483–488. [Google Scholar]
- Hagstrom, A.D.; Marshall, P.W.; Halaki, M.; Hackett, D.A. The Effect of Resistance Training in Women on Dynamic Strength and Muscular Hypertrophy: A Systematic Review with Meta-analysis. Sports Med. 2019, 50, 1075–1093. [Google Scholar] [CrossRef]
- Evans, J.W. Periodized Resistance Training for Enhancing Skeletal Muscle Hypertrophy and Strength: A Mini-Review. Front. Physiol. 2019, 10, 13. [Google Scholar] [CrossRef]
- Da, G.A.K.; Kelley, K.A.; Tran, Z. Aerobic Exercise and Resting Blood Pressure: A Meta-Analytic Review of Randomized, Controlled Trials. Prev. Cardiol. 2001, 4, 73–80. [Google Scholar] [CrossRef]
- Sillanpää, E.; Laaksonen, D.E.; Häkkinen, A.; Karavirta, L.; Jensen, B.; Kraemer, W.J.; Nyman, K.; Häkkinen, K. Body composition, fitness, and metabolic health during strength and endurance training and their combination in middle-aged and older women. Graefe’s Arch. Clin. Exp. Ophthalmol. 2009, 106, 285–296. [Google Scholar] [CrossRef]
- Cunha, P.; Tomeleri, C.M.; Nascimento, M.A.; Mayhew, J.L.; Fungari, E.; Cyrino, L.T.; Barbosa, D.S.; Venturini, D.; Cyrino, E.S. Comparision of Low and High Volume of Resistance Training on Body Fat and Blood Biomarkers in Untrained Older Women: A Randomized Clinical Trial. J. Strength Cond. Res. 2021, 35, 1–8. [Google Scholar] [CrossRef] [PubMed]
- de Castro Franco, C.M.; da Silva Carneiro, M.A.; Alves, L.T.H.; de Oliveira Júnior, G.N.; de Sousa, J.d.F.R.; Orsatti, F.L. Lower-load is more effective than higher-load resistance training in increasing muscle mass in young women. J. Strength Cond. Res. 2019, 33, S152–S158. [Google Scholar] [CrossRef]
- Aleksovska, K.; Puggina, A.; Giraldi, L.; Buck, C.; Burns, C.; Cardon, G.; Carlin, A.; Chantal, S.; Ciarapica, D.; Colotto, M.; et al. Biological determinants of physical activity across the life course: A “Determinants of Diet and Physical Activity” (DEDIPAC) umbrella systematic literature review. Sports Med.-Open 2019, 5, 1–18. [Google Scholar] [CrossRef]
- Gordon, J.R.; Whelan-Berry, K.S. Contributions to Family and Household Activities by the Husbands of Midlife Professional Women. J. Fam. Issues 2005, 26, 899–923. [Google Scholar] [CrossRef]
- Dubbert, P.M. Physical activity and exercise: Recent advances and current challenges. J. Consult. Clin. Psychol. 2002, 70, 526. [Google Scholar] [CrossRef]
- Schaie, K.W.; Leventhal, H.; Willis, S.L. Effective Health Behavior in Older Adults; Springer Publishing Company: Berlin/Heidelberg, Germany, 2002. [Google Scholar]
- Conconi, F.; Grazzi, G.; Casoni, I.; Guglielmini, C.; Borsetto, C.; Ballarín, E.; Mazzoni, G.; Patracchini, M.; Manfredini, F. The Conconi Test: Methodology After 12 Years of Application. Int. J. Sports Med. 1996, 17, 509–519. [Google Scholar] [CrossRef] [PubMed]
- Williams, C.B.; Zelt, J.G.; Castellani, L.N.; Little, J.P.; Jung, M.E.; Wright, D.C.; Tschakovsky, M.E.; Gurd, B.J. Changes in mechanisms proposed to mediate fat loss following an acute bout of high-intensity interval and endurance exercise. Appl. Physiol. Nutr. Metab. 2013, 38, 1236–1244. [Google Scholar] [CrossRef]
- McTiernan, A.; Sorensen, B.; Irwin, M.L.; Morgan, A.; Yasui, Y.; Rudolph, R.E.; Surawicz, C.; Lampe, J.W.; Lampe, P.D.; Ayub, K.; et al. Exercise Effect on Weight and Body Fat in Men and Women. Obesity 2007, 15, 1496–1512. [Google Scholar] [CrossRef]
- Després, J.P.; Pouliot, M.C.; Moorjani, S.; Nadeau, A.; Tremblay, A.; Lupien, P.J.; Thériault, G.; Bouchard, C. Loss of abdominal fat and metabolic response to exercise training in obese women. Am. J. Physiol. Metab. 1991, 261, E159–E167. [Google Scholar] [CrossRef]
- Stasiulis, A.; Mockienė, A.; Vizbaraitė, D.; Mockus, P. Aerobic exercise-induced changes in body composition and blood lipids in young women. Medicina 2010, 46, 129. [Google Scholar] [CrossRef] [Green Version]
- Poehlman, E.T.; Dvorak, R.V.; DeNino, W.F.; Brochu, M.; Ades, P.A. Effects of Resistance Training and Endurance Training on Insulin Sensitivity in Nonobese, Young Women: A Controlled Randomized Trial1. J. Clin. Endocrinol. Metab. 2000, 85, 2463–2468. [Google Scholar] [CrossRef] [Green Version]
- Izquierdo, M.; Häkkinen, K.; Ibáñez, J.; Kraemer, W.J.; Gorostiaga, E.M. Effects of combined resistance and cardiovascular training on strength, power, muscle cross-sectional area, and endurance markers in middle-aged men. Graefe’s Arch. Clin. Exp. Ophthalmol. 2004, 94, 70–75. [Google Scholar] [CrossRef]
- Gettman, L.R.; Pollock, M.L. Circuit Weight Training: A Critical Review of Its Physiological Benefits. Phys. Sportsmed. 1981, 9, 44–60. [Google Scholar] [CrossRef]
- Ferreira, F.C.; De Medeiros, A.I.; Nicioli, C.; Nunes, J.E.D.; Shiguemoto, G.E.; Prestes, J.; Verzola, R.M.M.; Baldissera, V.; Perez, S.E.D.A. Circuit resistance training in sedentary women: Body composition and serum cytokine levels. Appl. Physiol. Nutr. Metab. 2010, 35, 163–171. [Google Scholar] [CrossRef]
- Franklin, N.; Robinson, A.T.; Bian, J.-T.; Ali, M.; Norkeviciute, E.; McGinty, P.; Phillips, S.A. Circuit Resistance Training Attenuates Acute Exertion-Induced Reductions in Arterial Function but Not Inflammation in Obese Women. Metab. Syndr. Relat. Disord. 2015, 13, 227–234. [Google Scholar] [CrossRef] [Green Version]
- Cornelissen, V.A.; Fagard, R.H. Effects of Endurance Training on Blood Pressure, Blood Pressure–Regulating Mechanisms, and Cardiovascular Risk Factors. Hypertension 2005, 46, 667–675. [Google Scholar] [CrossRef] [Green Version]
- Christensen, N.J.; Galbo, H. Sympathetic Nervous Activity During Exercise. Annu. Rev. Physiol. 1983, 45, 139–153. [Google Scholar] [CrossRef]
- Fountain, J.H.; Lappin, S.L. Physiology, Renin Angiotensin System; StatPearls Publishing: Treasure Island, FL, USA, 2017. [Google Scholar]
- Stefanick, M.L.; Mackey, S.; Sheehan, M.; Ellsworth, N.; Haskell, W.L.; Wood, P.D. Effects of Diet and Exercise in Men and Postmenopausal Women with Low Levels of HDL Cholesterol and High Levels of LDL Cholesterol. N. Engl. J. Med. 1998, 339, 12–20. [Google Scholar] [CrossRef]
- Cornelissen, V.A.; Verheyden, B.; Aubert, A.E.; Fagard, R.H.; Cornelissen, V.A.; Verheyden, B.; Aubert, A.E.; Fagard, R.H. Effects of aerobic training intensity on resting, exercise and post-exercise blood pressure, heart rate and heart-rate variability. J. Hum. Hypertens. 2009, 24, 175–182. [Google Scholar] [CrossRef]
- Alcaraz, P.E.; Sánchez-Lorente, J.; Blazevich, A. Physical Performance and Cardiovascular Responses to an Acute Bout of Heavy Resistance Circuit Training versus Traditional Strength Training. J. Strength Cond. Res. 2008, 22, 667–671. [Google Scholar] [CrossRef] [Green Version]
- Carter, J.B.; Banister, E.W.; Blaber, A.P. Effect of Endurance Exercise on Autonomic Control of Heart Rate. Sports Med. 2003, 33, 33–46. [Google Scholar] [CrossRef]
- Brenner, I.K.M.; Thomas, S.; Shephard, R.J. Spectral analysis of heart rate variability during heat exposure and repeated exercise. Graefe’s Arch. Clin. Exp. Ophthalmol. 1997, 76, 145–156. [Google Scholar] [CrossRef] [PubMed]
- Bangsbo, J. Physiology of training. Sci. Soccer 2003, 2, 47–58. [Google Scholar]
- Paton, C.D.; Hopkins, W.G. Effects of high-intensity training on performance and physiology of endurance athletes. Sportscience 2004, 8, 25–41. [Google Scholar]
- Kraemer, W.J.; Fleck, S.J.; Deschenes, M. Exercise Physiology Corner: A ReviewFactors in exercise prescription of resistance training. Strength Cond. J. 1988, 10, 36–42. [Google Scholar] [CrossRef]
- Schoenfeld, B.J.; Grgic, J.; Ogborn, D.; Krieger, J.W. Strength and Hypertrophy Adaptations Between Low- vs. High-Load Resistance Training: A Systematic Review and Meta-analysis. J. Strength Cond. Res. 2017, 31, 3508–3523. [Google Scholar] [CrossRef]
- Brentano, M.A.; Cadore, E.L.; Da Silva, E.M.; Ambrosini, A.B.; Coertjens, M.; Petkowicz, R.; Viero, I.; Kruel, L.F. Physiological adaptations to strength and circuit training in postmenopausal women with bone loss. J. Strength Cond. Res. 2008, 22, 1816–1825. [Google Scholar] [CrossRef] [Green Version]
- Kraemer, W.J.; Ratamess, N.A.; French, D.N. Resistance Training for Health and Performance. Curr. Sports Med. Rep. 2002, 1, 165–171. [Google Scholar] [CrossRef]
- Vaara, J.P.; Kyröläinen, H.; Niemi, J.; Ohrankämmen, O.; Häkkinen, A.; Kocay, S.; Häkkinen, K. Associations of Maximal Strength and Muscular Endurance Test Scores with Cardiorespiratory Fitness and Body Composition. J. Strength Cond. Res. 2012, 26, 2078–2086. [Google Scholar] [CrossRef]
- Lima, C.D.; Ruas, C.V.; Behm, D.G.; Brown, L.E. Acute effects of stretching on flexibility and performance: A narrative re-view. J. Sci. Sport Exerc. 2019, 1, 29–37. [Google Scholar] [CrossRef] [Green Version]
- Medeiros, D.M.; Cini, A.; Sbruzzi, G.; Lima, C.S. Influence of static stretching on hamstring flexibility in healthy young adults: Systematic review and meta-analysis. Physiother. Theory Pr. 2016, 32, 438–445. [Google Scholar] [CrossRef] [PubMed]
- Clark, M.; Lucett, S. NASM Essentials of Corrective Exercise Training; Lippincott Williams & Wilkins: Philadelphia, PA, USA, 2010. [Google Scholar]
- Mann, D.P.; Jones, M.T. Guidelines to the implementation of a dynamic stretching program. Strength Cond. J. 1999, 21, 53–58. [Google Scholar] [CrossRef]
- Bandy, W.D.; Irion, J.M.; Briggler, M. The Effect of Time and Frequency of Static Stretching on Flexibility of the Hamstring Muscles. Phys. Ther. 1997, 77, 1090–1096. [Google Scholar] [CrossRef]
- Feland, J.B.; Myrer, J.W.; Schulthies, S.S.; Fellingham, G.W.; Measom, G.W. The effect of duration of stretching of the ham-string muscle group for increasing range of motion in people aged 65 years or older. Phys. Ther. 2001, 81, 1110–1117. [Google Scholar] [CrossRef]
- Behm, D.G.; Chaouachi, A. A review of the acute effects of static and dynamic stretching on performance. Graefe’s Arch. Clin. Exp. Ophthalmol. 2011, 111, 2633–2651. [Google Scholar] [CrossRef]
- Perrier, E.T.; Pavol, M.J.; Hoffman, M.A. The acute effects of a warm-up including static or dynamic stretching on counter-movement jump height, reaction time, and flexibility. J. Strength Cond. Res. 2011, 25, 1925–1931. [Google Scholar] [CrossRef]
- Talma, H.; Chinapaw, M.J.M.; Bakker, B.; HiraSing, R.A.; Terwee, C.B.; Altenburg, T.M. Bioelectrical impedance analysis to estimate body composition in children and adolescents: A systematic review and evidence appraisal of validity, responsiveness, reliability and measurement error. Obes. Rev. 2013, 14, 895–905. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
| Body Region | Exercise | 1st Week | 2nd Week | 3rd Week | 4th Week | 5th Week | 6th Week | 7th Week | 8th Week |
|---|---|---|---|---|---|---|---|---|---|
| Abdominals | Abdominal curls | # | # | # | # | ||||
| Abdominals | Abdominal curls (added weights) | ## | ## | ## | ## | ||||
| Abdominals | Leg raises | # | |||||||
| Lower back | Hyperextension bench | # | # | # | ## | ## | ## | # | # |
| Thigs | Knee extension | # | # | ||||||
| Hamstrings | Hamstring curl | # | # | # | # | # | # | # | |
| Legs/gluteus | Lunges | # | # | # | |||||
| Legs/gluteus | Lunges (added weights) | # | # | ||||||
| Legs/gluteus/lower back | Squats | # | # | # | |||||
| Legs/gluteus/lower back | Squats (plus weights) | # | # | ||||||
| Upper legs | Legg adductions | # | # | # | # | # | |||
| Upper legs | Legg abductions | # | # | # | # | # | |||
| Upper backs/arms | Latt pulldowns | # | # | # | # | ||||
| Upper backs/arms | Rowing torso | # | # | # | # | ||||
| Arms | Biceps curls | # | # | # | # | # | |||
| Arms | Triceps extension | # | # | # | |||||
| Chest | Butterfly machine | # | # | # | |||||
| Chest/arms | Bench press | # | # | # | # | # | |||
| Chest/arms/shoulders | Inclined bench press | ||||||||
| Shoulders/arms | French press | # | # | # | |||||
| Number of circuits per training session | 2 | 2 | 3 | 3 | 2 | 3 | 3 | 2 | |
| Time of work per set (in seconds) | 30 | 30 | 25 | 30 | 30 | 30 | 30 | 30 | |
| Rest between sets (in seconds) | 30 | 30 | 35 | 30 | 30 | 30 | 30 | 30 | |
| Rest between circuits (in minutes) | 5 | 5 | 5 | 5 | 5 | 5 | 5 | 5 | |
| Warm-up (in minutes) | 10 | 10 | 10 | 10 | 10 | 10 | 10 | 10 | |
| Cool-down (in minutes) | 10 | 10 | 10 | 10 | 10 | 10 | 10 | 10 | |
| Main Effects | Interaction | ||||||||
|---|---|---|---|---|---|---|---|---|---|
| Group | Measurement | Group × Measurement | |||||||
| F Test | p | ŋ2 | F Test | p | ŋ2 | F Test | p | ŋ2 | |
| Body mass | 0.29 | 0.76 | 0.01 | 374.01 | 0.001 | 0.87 | 77.15 | 0.001 | 0.73 |
| Body mass index | 0.65 | 0.52 | 0.02 | 147.62 | 0.001 | 0.72 | 63.19 | 0.001 | 0.69 |
| Body fat | 3.59 | 0.03 | 0.11 | 203.01 | 0.001 | 0.78 | 53.08 | 0.001 | 0.65 |
| Lean body mass | 4.39 | 0.01 | 0.13 | 26.87 | 0.001 | 0.32 | 9.55 | 0.001 | 0.25 |
| Sit and Reach | 0.83 | 0.43 | 0.02 | 160.13 | 0.001 | 0.73 | 3.23 | 0.04 | 0.11 |
| Shoulder circumduction | 4.31 | 0.02 | 0.13 | 71.41 | 0.001 | 0.56 | 18.3 | 0.001 | 0.39 |
| Dynamometric force Right | 3.05 | 0.06 | 0.09 | 83.3 | 0.001 | 0.59 | 60.76 | 0.001 | 0.68 |
| Dynamometric force Left | 1.4 | 0.25 | 0.05 | 118.87 | 0.001 | 0.67 | 20.5 | 0.001 | 0.41 |
| Squats 30 s | 7.13 | 0.001 | 0.2 | 35.45 | 0.001 | 0.39 | 17.42 | 0.001 | 0.38 |
| Push-ups | 20.85 | 0.001 | 0.42 | 231.58 | 0.001 | 0.8 | 49.59 | 0.001 | 0.63 |
| Resting heart rate | 0.25 | 0.77 | 0.001 | 27.87 | 0.001 | 0.32 | 14.22 | 0.001 | 0.33 |
| Systolic BP | 0.61 | 0.54 | 0.01 | 2.69 | 0.10 | 0.05 | 1.7 | 0.19 | 0.05 |
| Diastolic BP | 0.07 | 0.93 | 0.001 | 2.91 | 0.09 | 0.08 | 0.91 | 0.41 | 0.03 |
| Control | Resistance Training | Endurance Training | ||||
|---|---|---|---|---|---|---|
| Pre-Test | Post-Test | Pre-Test | Post-Test | Pre-Test | Post-Test | |
| Body mass (kg) | 65.38 ± 8.32 | 64.79 ± 9.12 | 66.56 ± 6.34 | 60.5 ± 6.42 * | 67.35 ± 8.39 | 59.38 ± 8.56 * |
| Body mass index (kg/m2) | 23.77 ± 2.71 | 24.2 ± 2.49 | 24.16 ± 2.41 | 21.98 ± 2.43 * | 25.11 ± 2.69 | 22.09 ± 2.79 * |
| Body fat (%) | 33.94 ± 6.06 | 34.02 ± 6.22 | 35.17 ± 5.75 | 24.19 ± 4.5 *,C | 36.43 ± 5.43 | 27.14 ± 4.04 *,C |
| Lean body mass (kg) | 42.96 ± 3.87 | 42.55 ± 3.94 | 43.29 ± 2.78 | 46.91 ± 3.99 *,C | 44.23 ± 4.06 | 47.57 ± 4.4 *,C |
| Sit and Reach (cm) | 25.75 ± 3.26 | 28.1 ± 3.39 * | 26.6 ± 3.9 | 30.2 ± 4.26 * | 25.7 ± 3.87 | 29.55 ± 3.66 * |
| Shoulder circumduction (cm) | 89.75 ± 8.39 | 89.75 ± 7.4 | 82.1 ± 15.21 | 76.15 ± 15.38 * | 87.5 ± 10.47 | 80.25 ± 10.46 * |
| Dynamometric force Right (kg) | 66 ± 16.44 | 64.1 ± 16.58 | 65.55 ± 7.21 | 79.25 ± 6.12 *,C,ET | 62.25 ± 9.27 | 66.4 ± 9.77 |
| Dynamometric force Left (kg) | 61.9 ± 13.69 | 66.1 ± 13.91 | 60.6 ± 9.33 | 75.25 ± 5.62 * | 60.15 ± 8.99 | 65.35 ± 9.52 |
| Squats 30 s (reps) | 19.46 ± 6.44 | 19.83 ± 5.73 | 19.07 ± 6.39 | 30.71 ± 10.93 *,C,ET | 16.79 ± 3.76 | 19.48 ± 4.89 |
| Push-ups (reps) | 12.75 ± 3.74 | 14.2 ± 3.19 | 15.65 ± 5.59 | 30.15 ± 8.01 *,C,ET | 13.55 ± 4.48 | 22.05 ± 3.78 *,C |
| Resting heart rate (bpm) | 72.6 ± 4.82 | 73.1 ± 4.23 | 72.95 ± 4.26 | 70.95 ± 4.26 * | 73.3 ± 3.47 | 71.3 ± 3.47 * |
| Systolic BP (mmHg) | 116.75 ± 8.16 | 118 ± 6.96 | 119.5 ± 9.45 | 115.25 ± 7.86 | 121 ± 8.05 | 117.5 ± 7.52 |
| Diastolic BP (mmHg) | 81.25 ± 5.82 | 79.5 ± 6.05 | 83 ± 6.37 | 78.75 ± 3.93 | 81.5 ± 6.9 | 79.25 ± 5.45 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Versic, S.; Idrizovic, K.; Ahmeti, G.B.; Sekulic, D.; Majeric, M. Differential Effects of Resistance- and Endurance-Based Exercise Programs on Muscular Fitness, Body Composition, and Cardiovascular Variables in Young Adult Women: Contextualizing the Efficacy of Self-Selected Exercise Modalities. Medicina 2021, 57, 654. https://doi.org/10.3390/medicina57070654
Versic S, Idrizovic K, Ahmeti GB, Sekulic D, Majeric M. Differential Effects of Resistance- and Endurance-Based Exercise Programs on Muscular Fitness, Body Composition, and Cardiovascular Variables in Young Adult Women: Contextualizing the Efficacy of Self-Selected Exercise Modalities. Medicina. 2021; 57(7):654. https://doi.org/10.3390/medicina57070654
Chicago/Turabian StyleVersic, Sime, Kemal Idrizovic, Gentiana Beqa Ahmeti, Damir Sekulic, and Matej Majeric. 2021. "Differential Effects of Resistance- and Endurance-Based Exercise Programs on Muscular Fitness, Body Composition, and Cardiovascular Variables in Young Adult Women: Contextualizing the Efficacy of Self-Selected Exercise Modalities" Medicina 57, no. 7: 654. https://doi.org/10.3390/medicina57070654
APA StyleVersic, S., Idrizovic, K., Ahmeti, G. B., Sekulic, D., & Majeric, M. (2021). Differential Effects of Resistance- and Endurance-Based Exercise Programs on Muscular Fitness, Body Composition, and Cardiovascular Variables in Young Adult Women: Contextualizing the Efficacy of Self-Selected Exercise Modalities. Medicina, 57(7), 654. https://doi.org/10.3390/medicina57070654