
May Argyrophilic Nucleolar Organizer Regions Be Used as a Biomarker for the Detection of the Degree of Ischemic Damage Instead of Tunel in Testicular Torsion?


Abstract
:1. Introduction
2. Materials and Methods
2.1. Experimental Design and Animal Groups
2.2. Experimental Testicular T/D Procedure
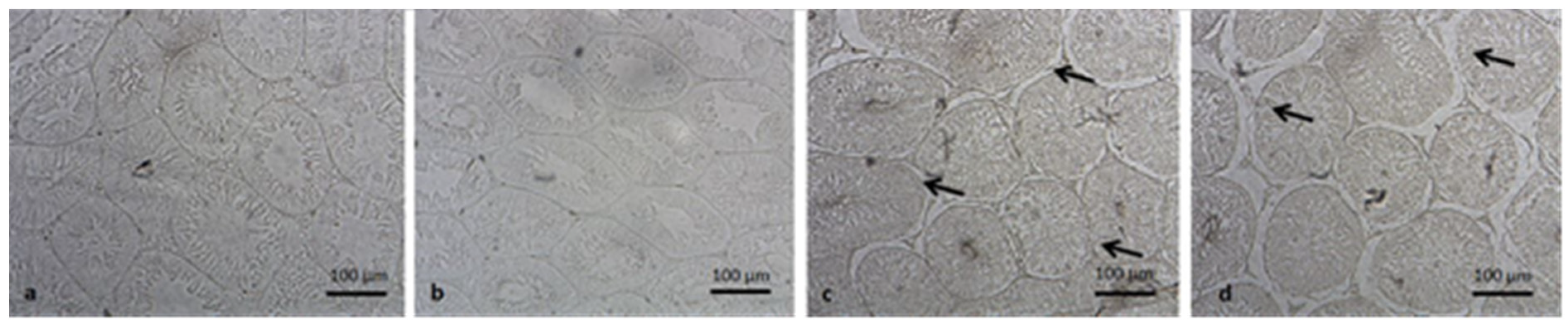
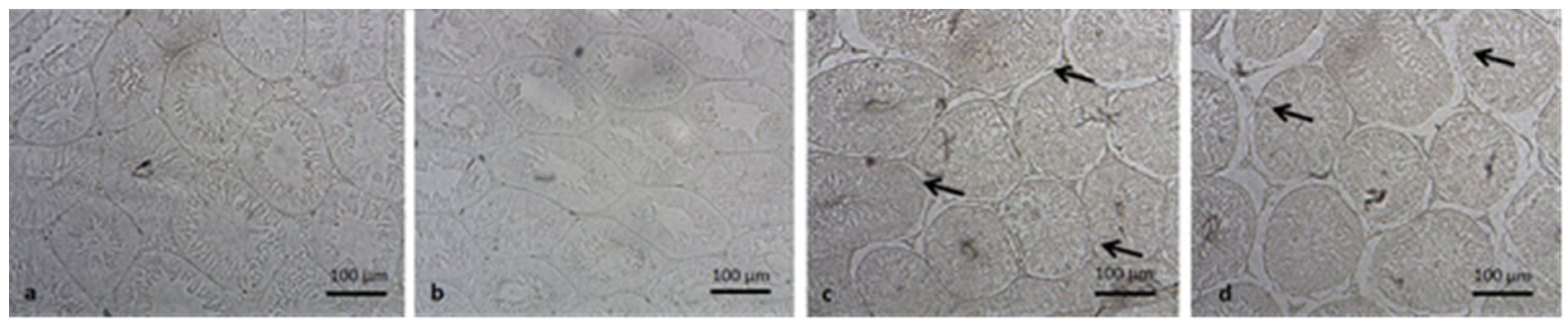
2.3. Evaluation of Germ Cell Apoptosis
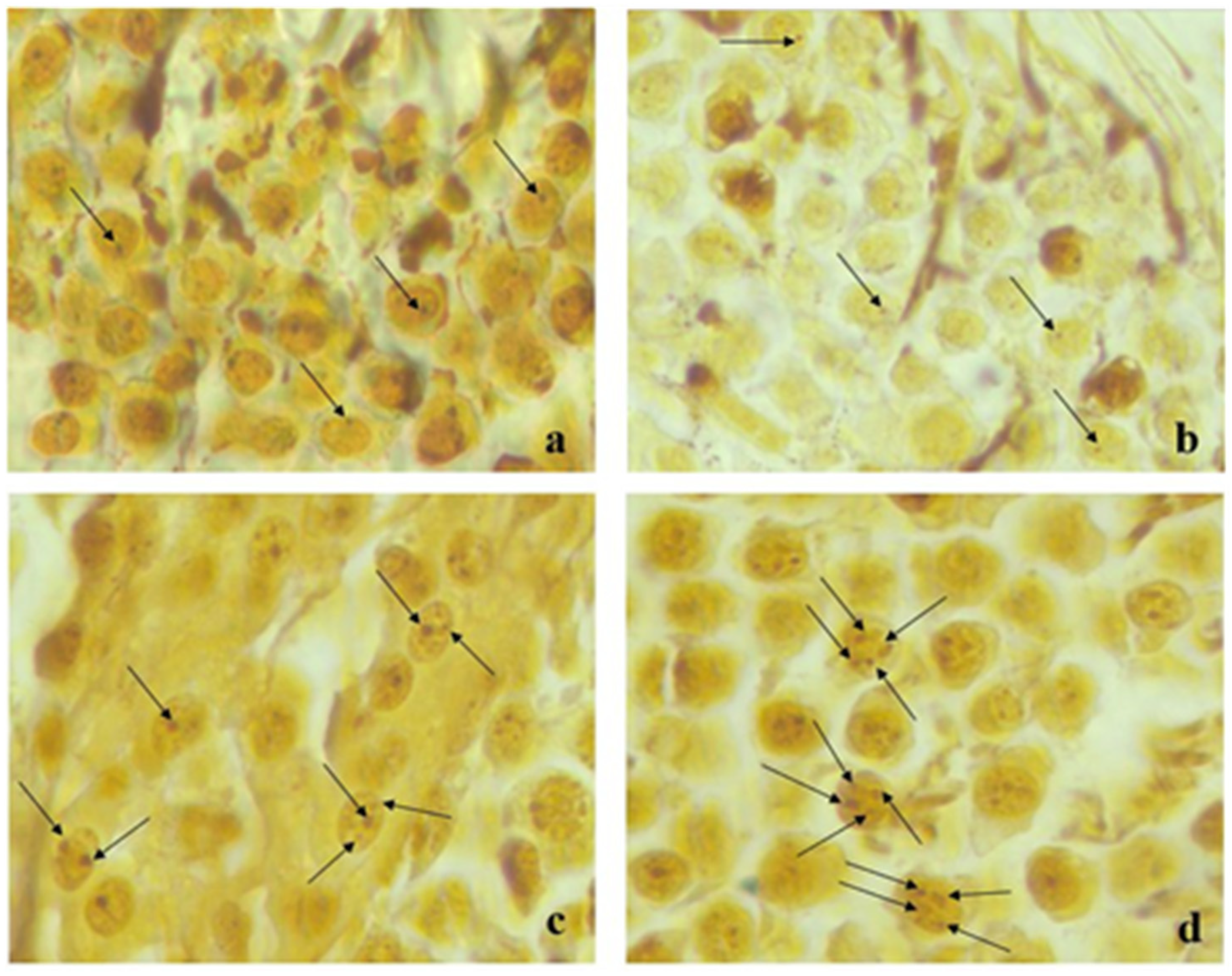
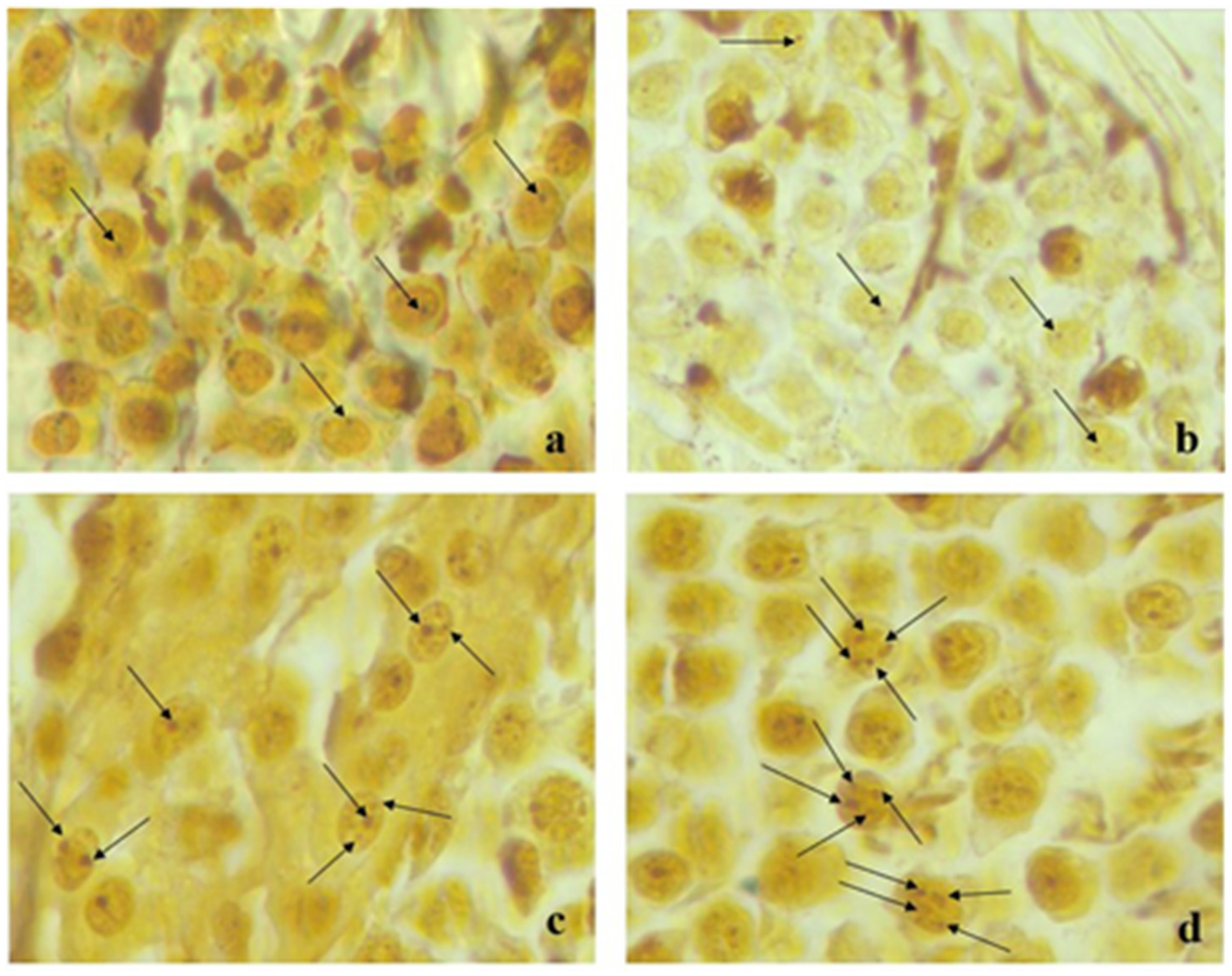
2.4. AgNOR Staining
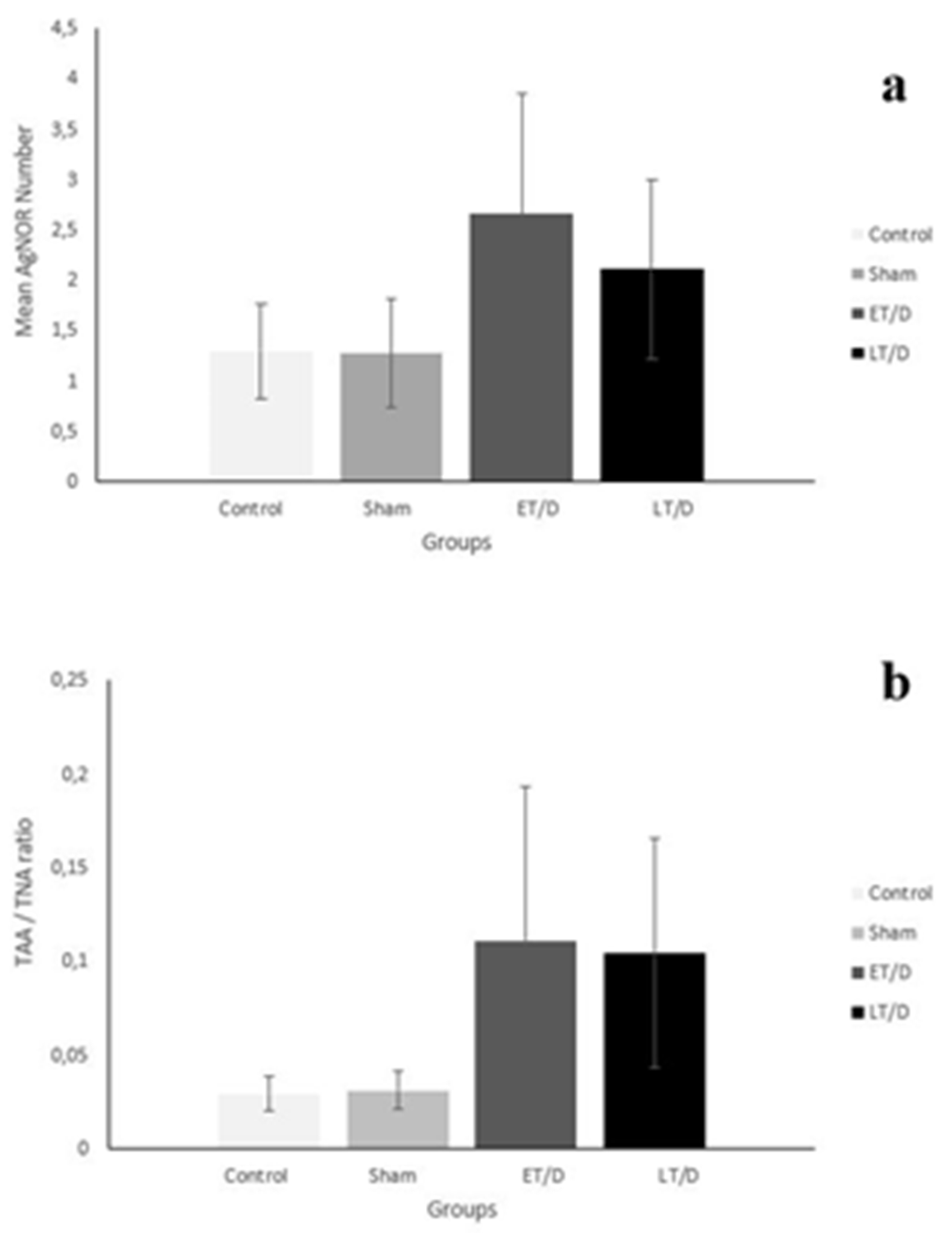
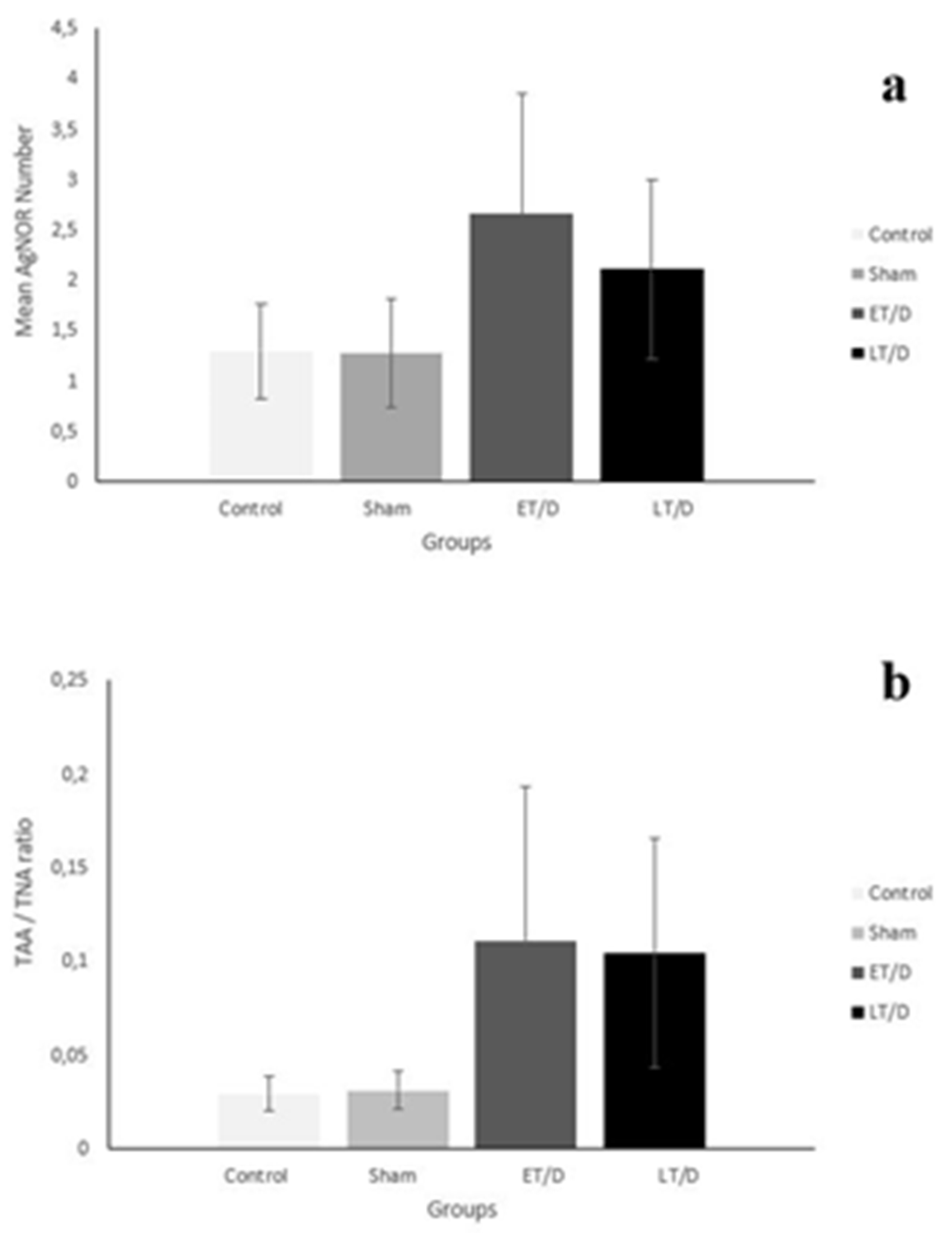
2.5. Image Analysis of Mean AgNOR Number and Total AgNOR Area/Total Nuclear Area
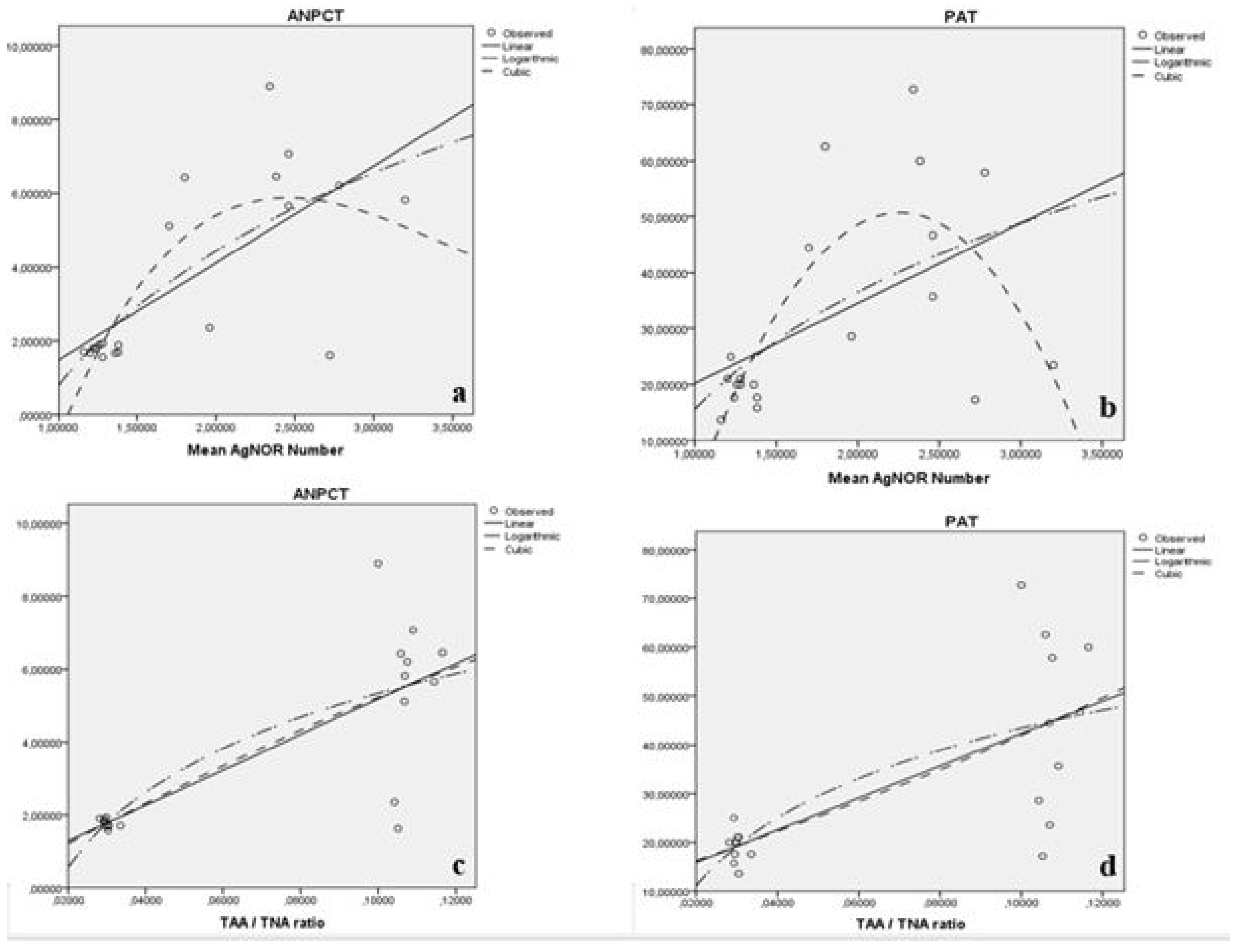
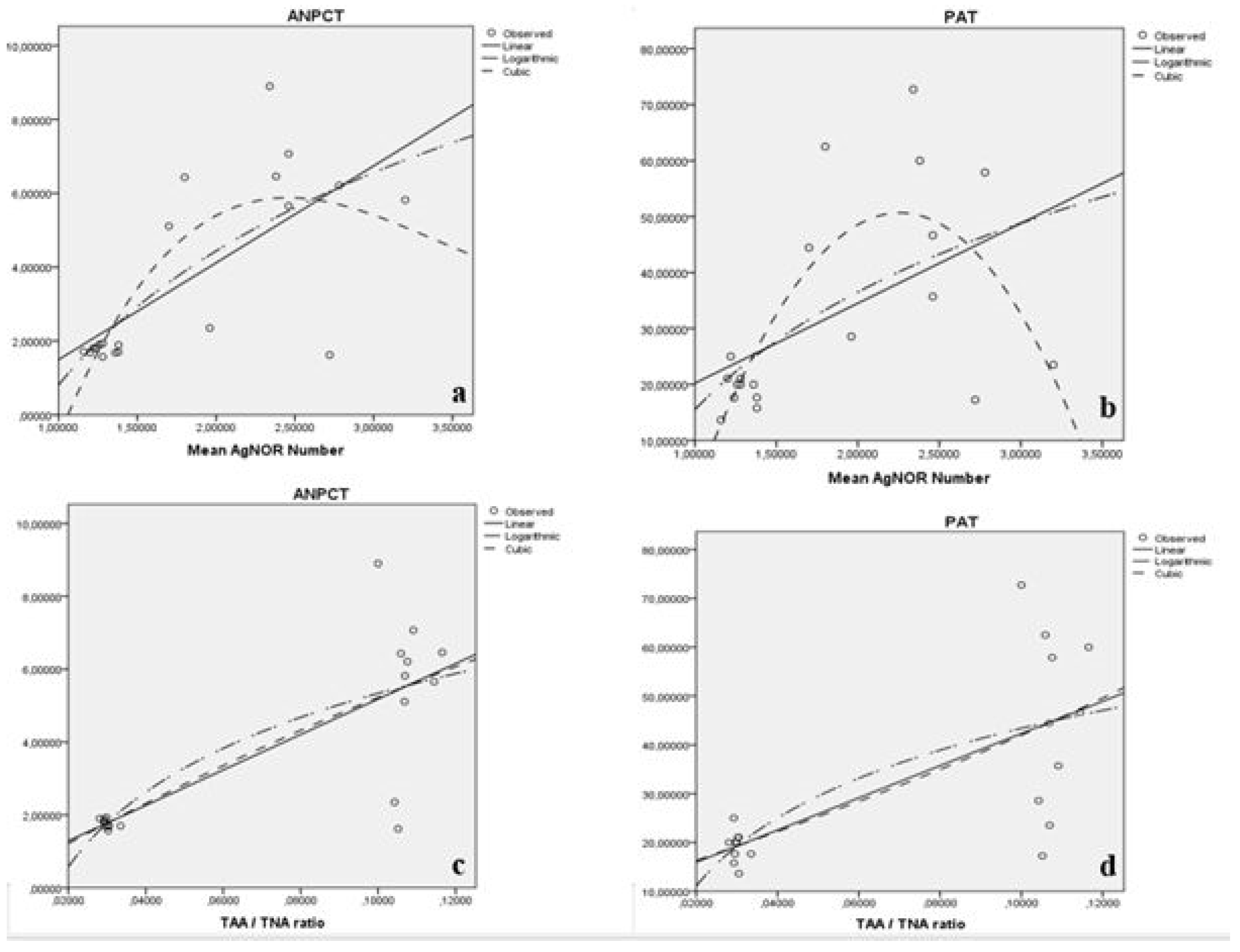
2.6. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| T/D | torsion-detorsion |
| I-R | ischemia-reperfusion |
| DNA | Deoxyribonucleic acid |
| ELISA | Enzyme-Linked ImmunoSorbent Assay |
| TUNEL | Terminal deoxynucleotidyl transferase nick end labeling method |
| NORs | Nucleolar-organizing regions |
| AgNOR | Post-silver staining NORs |
| TAA | total AgNOR area |
| TNA | total nuclear area |
| i.p. | intraperitoneal injection |
| ANPCT | average number of apoptotic cells per tubule |
| PAT | percentage of apoptotic tubule values |
| SD | standard deviation |
| ET/D | early torsion-detorsion group |
| LT/D | late torsion-detorsion group |
References
- Zhao, L.C.; Lautz, T.B.; Meeks, J.J.; Maizels, M. Pediatric testicular torsion epidemiology using a national database: Incidence, risk of orchiectomy and possible measures toward improving the quality of care. J. Urol. 2011, 186, 2009–2013. [Google Scholar] [CrossRef]
- Sharp, V.J.; Kieran, K.; Arlen, A.M. Testicular torsion: Diagnosis, evaluation, and management. Am. Fam. Physician 2013, 88, 835–840. [Google Scholar] [PubMed]
- Cost, N.G.; Bush, N.C.; Barber, T.D.; Huang, R.; Baker, L.A. Pediatric testicular torsion: Demographics of national orchiopexy versus orchiectomy rates. J. Urol. 2011, 185, 2459–2463. [Google Scholar] [CrossRef]
- Visser, A.J.; Heyns, C.F. Testicular function after torsion of the spermatic cord. BJU Int. 2003, 92, 200–203. [Google Scholar] [CrossRef]
- Tamamura, M.; Saito, M.; Kinoshita, Y.; Shimizu, S.; Satoh, I.; Shomori, K.; Dimitriadis, F.; Satoh, K. Protective effect of edaravone, a free-radical scavenger, on ischaemia-reperfusion injury in the rat testis. BJU Int. 2010, 105, 870–876. [Google Scholar] [CrossRef] [PubMed]
- Grimsby, G.M.; Schlomer, B.J.; Menon, V.S.; Ostrov, L.; Keays, M.; Sheth, K.R.; Villanueva, C.; Granberg, C.; Dajusta, D.; Hill, M.; et al. Prospective Evaluation of Predictors of Testis Atrophy After Surgery for Testis Torsion in Children. Urology 2018, 116, 150–155. [Google Scholar] [CrossRef] [PubMed]
- Kockx, M.M.; Muhring, J.; Knaapen, M.W.; de Meyer, G.R. RNA synthesis and splicing interferes with DNA in situ end labeling techniques used to detect apoptosis. Am. J. Pathol. 1998, 152, 885–888. [Google Scholar] [PubMed]
- Eroz, R.; Tasdemir, S.; Dogan, H. Is there any relationship between decreased AgNOR protein synthesis and human hair loss? Biotech. Histochem. 2012, 87, 494–498. [Google Scholar] [CrossRef]
- Eroz, R.; Yilmaz, S.; Cucer, N. Argyrophilic nucleolar organizing region associated protein synthesis in hair root cells of humans at different developmental stages and sex. Biotech. Histochem. 2013, 88, 267–271. [Google Scholar] [CrossRef] [PubMed]
- Selvi, B.; Demirtas, H.; Eroz, R.; Imamoglu, N. Investigation of the age-dependent AgNOR protein level in buccal epithelial cells of healthy individuals. Aging Clin. Exp. Res. 2015, 27, 201–208. [Google Scholar] [CrossRef]
- Çolakoğlu, S.; Saritas, A.; Eroz, R.; Oktay, M.; Yaykasli, K.O.; Akoz, A.; Kaya, E.; Kandis, H. Is one-time carbon monoxide intoxication harmless? Evaluation by argyrophilic nucleolar-organizing regions staining method. Hum. Exp. Toxicol. 2015, 34, 24–31. [Google Scholar] [CrossRef]
- Kandiş, H.; Afacan, M.A.; Eröz, R.; Colakoglu, S.; Bayramoglu, A.; Oktay, M.; Saritas, A.; Colak, S.; Kaya, M.; Kara, İ.H. Can argyrophilic nucleolar organizing region-associated protein amount be used for the detection of cardiac damage? Hum. Exp. Toxicol. 2016, 35, 323–331. [Google Scholar] [CrossRef]
- Saritas, A.; Gunes, H.; Colakoglu, S.; Eroz, R.; Akoz, A.; Oktay, M.; Buyukkaya, A.; Kandis, H.; Ozkan, A. Are there any effects of chronic carbon monoxide exposure on argyrophilic nucleolar-organizing region-associated protein synthesis in rat myocardium? Hum. Exp. Toxicol. 2016, 35, 921–928. [Google Scholar] [CrossRef]
- Eroz, R.; Saritas, A.; Colakoglu, S.; Oktay, M.; Kandis, H. Evaluation of argyrophilic nucleolar organizing region–associated protein synthesis in femoral muscle cells of rats exposed 3000 ppm carbon monoxide gas. Konuralp Med. J. 2016, 8, 9–13. [Google Scholar]
- Gunes, H.; Saritas, A.; Eroz, R.; Colakoglu, S. Use of argyrophilic nucleolar–organizer region-associated protein synthesis in skeletal muscle cells for prediction of chronic carbon monoxide exposure. Toxin Rev. 2020, 39, 349–354. [Google Scholar]
- Eroz, R.; Cucer, N.; Karaca, Z.; Unluhizarci, K.; Ozturk, F. The evaluation of argyrophilic nucleolar organizing region proteins in fine needle aspiration samples of thyroid. Endocr. Pathol. 2011, 22, 74–78. [Google Scholar] [CrossRef] [PubMed]
- Eroz, R.; Cucer, N.; Unluhizarcı, K.; Ozturk, F. Detection and comparison of cutoff values for total AgNOR area/nuclear area and AgNOR number/nucleus in benign thyroid nodules and normal thyroid tissue. Cell Biol. Int. 2013, 37, 257–261. [Google Scholar] [CrossRef] [PubMed]
- Eroz, R.; Unluhizarc, K.; Cucer, N.; Ozturk, F. Value of argyrophilic nucleolar organizing region protein determinations in nondiagnostic fine needle aspiration samples (due to insufficient cell groups) of thyroid nodules. Anal. Quan. Cytol. 2013, 35, 226–232. [Google Scholar]
- Oktay, M.; Eroz, R.; Oktay, N.A.; Erdem, H.; Başar, F.; Akyol, L.; Cucer, N.; Bahadir, A. Argyrophilic nucleolar organizing region associated protein synthesis for cytologic discrimination of follicular thyroid lesions. Biotech. Histochem. 2015, 90, 179–183. [Google Scholar] [CrossRef] [PubMed]
- Sonmez, F.T.; Eroz, R. The role of argyrophilic nucleolar organizing region-associated proteins in clinical exacerbation of chronic obstructive pulmonary disease. J. Int. Med. Res. 2018, 46, 4995–5003. [Google Scholar] [CrossRef] [PubMed]
- Kanter, M. Protective effects of melatonin on testicular torsion/detorsion-induced ischemia-reperfusion injury in rats. Exp. Mol. Pathol. 2010, 89, 314–320. [Google Scholar] [CrossRef]
- Negoescu, A.; Lorimier, P.; Labat-Moleur, F.; Drouet, C.; Robert, C.; Guillermet, C.; Brambilla, C.; Brambilla, E. In situ apoptotic cell labeling by the TUNEL method: Improvement and evaluation on cell preparations. J. Histochem. Cytochem. 1996, 44, 959–968. [Google Scholar] [CrossRef]
- Benn, P.A.; Perle, M. Chromosome staining and banding techniques. In Human Cytogenetics, Constitutional Analysis, Practical Approach; Rooney, D.E., Czepulkowski, B.H., Eds.; Oxford University Press: Oxford, UK, 1986; Volume 1, pp. 91–118. [Google Scholar]
- Lindner, L.E. Improvements in the silver-staining technique for nucleolar organizer regions (AgNOR). J. Histochem. Cytochem. 1993, 41, 439–445. [Google Scholar] [CrossRef] [Green Version]
- Rasband, W.S. ImageJ, U. S. National Institutes of Health, Bethesda, Maryland, USA. Available online: https://imagej.nih.gov/ij/ (accessed on 28 September 2021).
- Eroz, R.; Alpay, M. Investigation of the effect of capsaicin on AgNOR protein synthesis using staining intensity degree in human colon adenocarcinoma. Edorium J. Cell Biol. 2018, 4, 100007C06RE2018. [Google Scholar]
- Ertekin, T.; Bozkurt, O.; Eroz, R.; Nisari, M.; Bircan, D.; Nisari, M.; Unur, E. May argyrophilic nucleolar organizing region-associated protein synthesis be used for selecting the most reliable dose of drugs such as rhamnetin in cancer treatments? Bratisl. Lek. Listy. 2016, 117, 653–658. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Eroz, R. Argyrophilic nucleolar organizing regions associated proteins in oncocytology. Oncocytology 2015, 5, 21–24. [Google Scholar]
- Nakayama, A.; Ide, H.; Osaka, A.; Inoue, Y.; Shimomura, Y.; Iwahata, T.; Kobori, Y.; Saito, K.; Soh, S.; Okada, H. The Diagnostic Accuracy of Testicular Torsion by Doctors on Duty Using Sonographic Evaluation with Color Doppler. Am. J. Men’s Health 2020, 14. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Groups | Mean AgNOR Number ± SD (n = 50) | Mean TAA/TNA ± SD (n = 50) | Average AgNOR Number of Group/Median (Range) (n = 250) | Mean TAA/TNA of Group/Median (Range) (n = 250) | χ2 | p |
|---|---|---|---|---|---|---|
| C1 | 1.28 ± 0.536 | 0.03 ± 0.008 | 1.288 ± 0.471/1 (2) | 0.029 ± 0.009/0.028 (0.093) | 355.977 * 730.555 & | 0.000 * 0.000 & |
| C2 | 1.38 ± 0.490 | 0.029 ± 0.007 | ||||
| C3 | 1.28 ± 0.454 | 0.03 ± 0.012 | ||||
| C4 | 1.24 ± 0.431 | 0.03 ± 0.009 | ||||
| C5 | 1.26 ± 0.443 | 0.028 ± 0.008 | ||||
| S1 | 1.22 ± 0.419 | 0.029 ± 0.009 | 1.264 ± 0.540/1(3) | 0.031 ± 0.01/0.03 (0.056) | ||
| S2 | 1.36 ± 0.663 | 0.03 ± 0.012 | ||||
| S3 | 1.2 ± 0.404 | 0.03 ± 0.011 | ||||
| S4 | 1.38 ± 0.697 | 0.034 ± 0.011 | ||||
| S5 | 1.16 ± 0.422 | 0.031 ± 0.009 | ||||
| ET/D 1 | 2.46 ± 1.147 | 0.109 ± 0.028 | 2.656 ± 1.183/3 (6) | 0.111 ± 0.082/0.098 (0.919) | ||
| ET/D 2 | 3.2 ± 1.212 | 0.107 ± 0.032 | ||||
| ET/D 3 | 2.78 ± 1.298 | 0.108 ± 0.033 | ||||
| ET/D 4 | 2.46 ± 1.073 | 0.115 ± 0.125 | ||||
| ET/D 5 | 2.38 ± 1.008 | 0.117 ± 0.125 | ||||
| LT/D 1 | 1.96 ± 0.88 | 0.104 ± 0.023 | 2.104 ± 0.89/2 (4) | 0.104 ± 0.061/0.103 (0.96) | ||
| LT/D 2 | 2.72 ± 1.011 | 0.105 ± 0.029 | ||||
| LT/D 3 | 2.34 ± 0.798 | 0.1 ± 0.028 | ||||
| LT/D 4 | 1.8 ± 0.606 | 0.106 ± 0.025 | ||||
| LT/D 5 | 1.7 ± 0.707 | 0.107 ± 0.127 |
| Groups | C | S | ET/D | LT/D | ||||
|---|---|---|---|---|---|---|---|---|
| Z | p | Z | p | Z | p | Z | p | |
| C | −1.299 | 0.194 | −14.086 | 0.000 | −11.534 | 0.000 | ||
| S | −1.299 | 0.194 | −14.348 | 0.000 | −12.026 | 0.000 | ||
| ET/D | −14.086 | 0.000 | −14.348 | 0.000 | −5.480 | 0.000 | ||
| LT/D | −11.534 | 0.000 | −12.026 | 0.000 | −5.480 | 0.000 | ||
| Groups | C | S | ET/D | LT/D | ||||
|---|---|---|---|---|---|---|---|---|
| Z | p | Z | p | Z | p | Z | p | |
| C | −1.280 | 0.201 | −19.227 | 0.001 | −18.948 | 0.001 | ||
| S | −1.280 | 0.201 | −19.267 | 0.001 | −18.948 | 0.001 | ||
| ET/D | −19.227 | 0.001 | −19.267 | 0.001 | −0.356 | 0.722 | ||
| LT/D | −18.948 | 0.001 | −18.948 | 0.001 | −0.356 | 0.722 | ||
| Groups | ANPCT | Mean ± SD/Median (Range) for ANPCT | PAT | Mean ± SD/Median (Range) for PAT | χ2 | p |
|---|---|---|---|---|---|---|
| C1 | 1.93 | 1.82 ± 0.147/1.89 (0.36) | 20.00 | 18.894 ± 2.143/20 (5.27) | 11.031 * 9.798 & | 0.012 * 0.020 & |
| C2 | 1.89 | 15.78 | ||||
| C3 | 1.57 | 21.05 | ||||
| C4 | 1.81 | 17.64 | ||||
| C5 | 1.90 | 20.00 | ||||
| S1 | 1.81 | 1.716 ± 0.054/1.7 (0.13) | 25.00 | 19.464 ± 4.208/20 (11.37) | ||
| S2 | 1.68 | 20.00 | ||||
| S3 | 1.68 | 21.05 | ||||
| S4 | 1.70 | 17.64 | ||||
| S5 | 1.71 | 13.63 | ||||
| ET/D 1 | 7.07 | 6.244 ± 0.559/6.21 (1.41) | 35.71 | 44.756 ± 15.34/46.66 (36.48) | ||
| ET/D 1 | 5.82 | 23.52 | ||||
| ET/D 1 | 6.21 | 57.89 | ||||
| ET/D 1 | 5.66 | 46.66 | ||||
| ET/D 1 | 6.46 | 60.00 | ||||
| LT/D 1 | 2.35 | 4.882 ± 2.985/5.11 (7.28) | 28.57 | 45.096 ± 23/44.44 (55.49) | ||
| LT/D 2 | 1.62 | 17.24 | ||||
| LT/D 3 | 8.90 | 72.73 | ||||
| LT/D 4 | 6.43 | 62.50 | ||||
| LT/D 5 | 5.11 | 44.44 |
| Model Summery | Parameter Estimates | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Variable | Equation | R2 | F | df1 | df2 | sig | Constant | b1 | b2 | b3 |
| M-AgNOR-N and ANPCT | Linear | 0.491 | 17.335 | 1 | 18 | 0.001 | −1.135 | 2.626 | ||
| Log | 0.540 | 21.120 | 1 | 18 | 0.000 | 0.805 | 5.240 | |||
| Cubic | 0.612 | 8.419 | 3 | 16 | 0.001 | −16.973 | 23.016 | −7.378 | 0.731 | |
| M-AgNOR-N and PAT | Linear | 0.255 | 6.162 | 1 | 18 | 0.023 | 5.953 | 14.277 | ||
| Log | 0.318 | 8.385 | 1 | 18 | 0.010 | 15.506 | 30.314 | |||
| Cubic | 0.568 | 7.009 | 3 | 16 | 0.003 | −104.265 | 133.132 | −26.750 | −0.807 | |
| TAA/TNA and ANPCT | Linear | 0.632 | 30.926 | 1 | 18 | 0.000 | 0.317 | 48.638 | ||
| Log | 0.631 | 30.803 | 1 | 18 | 0.000 | 12.153 | 2.959 | |||
| Cubic | 0.632 | 14.609 | 2 | 17 | 0.000 | 0.052 | 59.827 | −80.823 | 0.000 | |
| TAA/TNA and PAT | Linear | 0.511 | 18.810 | 1 | 18 | 0.000 | 9.351 | 329.732 | ||
| Log | 0.510 | 18.705 | 1 | 18 | 0.000 | 89.558 | 20.050 | |||
| Cubic | 0.511 | 8.885 | 2 | 17 | 0.002 | 10.496 | 289.733 | 0.000 | 2509.205 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kabaklıoğlu, M.; Eroz, R.; Kaya, M. May Argyrophilic Nucleolar Organizer Regions Be Used as a Biomarker for the Detection of the Degree of Ischemic Damage Instead of Tunel in Testicular Torsion? Medicina 2021, 57, 1177. https://doi.org/10.3390/medicina57111177
Kabaklıoğlu M, Eroz R, Kaya M. May Argyrophilic Nucleolar Organizer Regions Be Used as a Biomarker for the Detection of the Degree of Ischemic Damage Instead of Tunel in Testicular Torsion? Medicina. 2021; 57(11):1177. https://doi.org/10.3390/medicina57111177
Chicago/Turabian StyleKabaklıoğlu, Murat, Recep Eroz, and Murat Kaya. 2021. "May Argyrophilic Nucleolar Organizer Regions Be Used as a Biomarker for the Detection of the Degree of Ischemic Damage Instead of Tunel in Testicular Torsion?" Medicina 57, no. 11: 1177. https://doi.org/10.3390/medicina57111177
APA StyleKabaklıoğlu, M., Eroz, R., & Kaya, M. (2021). May Argyrophilic Nucleolar Organizer Regions Be Used as a Biomarker for the Detection of the Degree of Ischemic Damage Instead of Tunel in Testicular Torsion? Medicina, 57(11), 1177. https://doi.org/10.3390/medicina57111177