Abstract
Knee osteoarthritis (KOA) is a progressive joint disease and a leading source of chronic pain and disability. OA-bone marrow lesions (BMLs) are a recognised aetiopathological feature of KOA. Several intra-articular injectable therapies are recommended and used for management of KOA. This systematic review assessed the efficacy and safety of intra-articular therapies for improving OA-BMLs and reducing pain in adults with KOA. The study was conducted following registered review protocol (PROSPERO CRD42020189461) and six bibliographic databases, and two clinical trial registries were searched. We included eight randomised clinical trials involving 1294 participants, reported in 12 publications from 2016 to 2021. Two studies of sprifermin, one of autologous protein solution (APS) and one of high-dose TissueGene-C, reported a positive effect on OA-BMLs under 1-year follow-up. Two studies with corticosteroids reported mixed findings with no beneficial effect beyond 14 weeks of follow-up. One study assessing platelet-rich plasma found no significant improvement in OA-BMLs at 12 months follow-up. Knee pain was improved in two studies evaluating TissueGene-C and one study assessing APS; the remaining studies found no improvement in knee pain. Overall, we found mixed evidence on the efficacy of intra-articular therapy for improving OA-BMLs in KOA. Additional studies with long-term follow-up are needed to confirm the effect of various intra-articular therapies on OA-BMLs in KOA.
1. Introduction
Osteoarthritis (OA) is a chronic, progressive, and painful condition that affects many joints, including the knee. Knee OA (KOA) is the most common form of OA and is characterised by an inflammatory-degenerative process of all joint structures, which involves reduced physical activity and social and occupational functioning, mainly due to pain, the primary symptom [1]. It is the leading cause of disability in OA patients worldwide and the predominant condition leading to total knee replacement (TKR) surgery from a global perspective [2].
Despite the substantial global burden of KOA, no disease-modifying osteoarthritis drugs (DMOADS) are available to treat OA [3]. The reasons are multifactorial and include multiple heterogeneous causes of OA, which are difficult to target given the multiple pathways of causality [3]. Furthermore, dry biomarkers, such as traditional radiography, are relatively insensitive to early KOA changes [3,4]. The initial treatment of KOA is conservative and includes targeted exercise programs, such as Good Life with osteoArthritis: Denmark (GLA:D®) [2,5], in conjunction with pharmacological interventions such as paracetamol and, in selective cases, nonsteroidal anti-inflammatory drugs (NSAIDs) [2]. With regard to conservative treatments, the use of non-pharmacological interventions such as knee rehabilitation exercises, including the combination of aerobic exercise, strengthening, neuromuscular training, isometric exercises, and pharmacological interventions such as intra-articular therapies (corticosteroids and hyaluronic acid) are commonly recommended by the guidelines. [2] For patients with chronic knee pain and functional loss, TKR is an effective option for many individuals. However, it is expensive and may be prevented or delayed if KOA is well managed conservatively.
KOA is a disease of the whole joint [6], and the role of subchondral bone in the pathogenesis of KOA has attracted increasing attention [7]. Bone marrow lesions (BMLs), referred to previously as bone marrow oedema, are recognised as important features of KOA [8]. However, BMLs are not exclusive to KOA and not all BMLs in patients with KOA are OA-BMLs [9]. OA-BMLs are those that are adjacent to articular cartilage and without any visible fracture line [9]. Magnetic resonance imaging (MRI) is the most sensitive modality for detecting OA-BMLs [4,10]. Several studies in patients with KOA have found knee pain to be positively associated with MRI-detected OA-BMLs. For example, Zhang et al. found that changes in OA-BMLs are associated with knee pain and that the decrease in OA-BML size is associated with a reduction in knee pain in patients with KOA [11]. Given that OA-BMLs occur early in subchondral bone and reverse earlier than cartilage degradation [12], treatments focused on targeting bone, shrinking OA-BMLs, and reducing focal contact stress across the joint can have a profound impact on reducing pain and progression to surgery [11].
Several interventions delivered through the intra-articular route are recommended by guidelines for the management of KOA [2]. Researchers have evaluated intra-articular treatments such as hyaluronic acid, glucocorticoids [13], autologous protein solution injections [14], platelet-rich plasma [15], human bone marrow mesenchymal stem cells [16], gene therapies [17], and human recombinant fibroblast growth factor (sprifermin) in patients with KOA [7]. Intra-articular therapies can be administered by direct injection into the knee in the clinic, for example, platelet-rich plasma [15], or by a surgical procedure involving a general anaesthetic such as bone marrow aspirate concentrate [16]. Surgical procedures are costly and more complex, with the potential for significant side effects and can only be used for certain cartilage defects [17]. Therapies administered in a clinical setting offer many patients a more convenient and accessible option.
Currently, intra-articular injectable therapies as treatments for KOA are in widespread use worldwide. The autologous blood product platelet-rich plasma (PRP), for example, produces high concentrations of growth factors and has been shown to have favourable pain and functional outcomes in KOA [15,18,19]. From a patient well-being perspective, since OA-BMLs are shown to be associated with pain and pain is one of the main reasons individuals progress to TKR, there is a need for a better understanding of how effective intra-articular injectable treatment options are for improving OA-BMLs and knee symptoms in patients with KOA. The purpose of this systematic review was to synthesise the evidence on the efficacy and safety of available non-surgical intra-articular injectable treatments. The research question for this review was “How effective are non-operative intra-articular injectable treatments for the improvement of OA-BMLs and reducing pain in adults with KOA?”.
2. Materials and Methods
This systematic review was performed following our a priori registered protocol on PROSPERO (registration number CRD42020189461) [20] and reported according to the Preferred Reporting Items for Systematic Review and Meta-Analyses (PRISMA) statement [21].
2.1. Criteria for Study Inclusion
Studies were included if they compared intra-articular injectable non-operative interventions with placebo or other active treatments for KOA in an adult population with at least one OA-BML on MRI. Eligible study designs included randomised, quasi-randomised, or non-randomised controlled clinical trials. Sub-group analysis and post hoc analysis were also eligible. No restrictions were placed on the type of publication (full-text papers or conference abstracts), provided they had reported measuring the required outcomes.
2.2. Criteria for Study Exclusion
We excluded studies with no comparison group and those published in a language other than English.
2.3. Population, Intervention, Comparator and Outcomes
A detailed account of the Population, Intervention, Comparator, and Outcomes (PICO) is provided in the published protocol [20]. Briefly, the population constituted adult (≥18 years) humans with KOA; the intervention group for this review was intra-articular injectable non-operative therapy, and the comparator group was a placebo or any active intra-articular pharmacological intervention.
The primary outcomes of interest included structural changes (maximal area/volume) of OA-BMLs, determined at baseline and treatment intervals measured by quantitative or semi-quantitative measurements from MRI. The secondary outcomes of interest included changes in knee pain intensity determined at baseline and at treatment intervals measured by validated patient-reported outcome measures (PROMS) such as the Knee Injury and Osteoarthritis Outcome Score (KOOS); Western Ontario and McMaster University Arthritis Index (WOMAC); and changes in health-related quality-of-life (HRQoL) were assessed using the Assessment of Quality of Life-8 Dimension score (AQoL-8D) and the 36-Item Short Form Health Survey score (SF-36).
2.4. Search Strategy and Study Selection
Systematic and comprehensive searches were conducted from database inception to 16 May 2022 in the bibliographic databases Ovid MEDLINE®, Embase, CENTRAL, CINAHL, SPORTDiscus and pEDro. Additionally, ClinicalTrials.gov and the Australian New Zealand Clinical Trials Registry (ANZCTR) were also searched. The search strategy was first optimised for MEDLINE and then adapted for other databases. The search strategy for MEDLINE is shown in Supplement Table S1. The complete search strategy, including MeSH terms, was developed and validated by the first author (A.K.) with assistance from a Medical Librarian. Bibliographic database searches were supplemented by hand-searching the reference lists of included articles and by contacting study authors.
Search results were imported into Covidence (Veritas Health Innovation, Melbourne, Australia), and two reviewers (A.K. and A.W.S.) screened the titles and abstracts of all articles against the eligibility criteria. Full-text copies of studies identified by the title/abstract screen as having met the inclusion criteria were obtained. Any disagreements or conflicting decisions were resolved through discussion and consensus with the other authors. Reasons for excluding studies were documented.
2.5. Data Extraction and Risk of Bias Assessment
Relevant data were extracted independently for each included study by two authors using a prespecified MS Excel-based data extraction template. The data extracted included publication details, study design, follow-up duration, population, intervention details, key outcomes, conclusion, etc.
Two reviewers (S.H. and A.S.) independently assessed the risk of bias in the included studies according to the Cochrane Handbook 5.0.1 RCT risk of bias assessment (RoB-I) tool [22]. As per the Cochrane RoB-I tool, the bias was assessed for items such as sequence generation, allocation concealment, blinding of participants, study personnel, outcome assessors, incomplete outcome data, selective outcome reporting, and other potential sources of bias.
2.6. Data Synthesis and Statistical Analysis
Due to the heterogeneity among included studies in terms of intervention, doses, duration of follow-up, and outcome reporting (OA-BMLs reported as a continuous outcome as well as categorical outcome), a meta-analysis was not deemed appropriate. Hence, we analysed the data qualitatively and presented it in the form of a narrative synthesis.
3. Results
Following database searches, hand-searching references, and trial registry screening, 1245 records were identified (Figure 1). After removing duplicates, 740 records had titles and abstracts screened, and 97 full-text articles were screened for eligibility. After the full-text screening, eight studies reported in 12 publications met the eligibility criteria and were included in the review (Supplement Figure S1: PRISMA 2020 flow diagram).
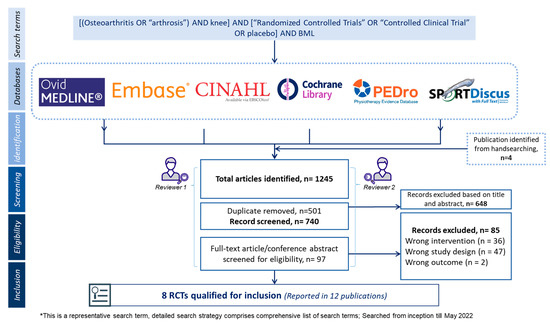
Figure 1.
Flow chart describing method and inclusion of studies.
3.1. Study Characteristics
The characteristics of included studies are summarised in Table 1. Of the eight included studies, two each used intra-articular injectable sprifermin [7,23,24,25], corticosteroids [13,26] and TissueGene-C [17,27,28,29], and one each used platelet-rich plasma [15] and APS [14]. All included studies were registered in clinical trial registries and were published between 2016 and 2021. Two studies were multicentre, multinational trials [7,25], two studies were from the US [26,29], and the remaining studies were conducted in Italy [14], South Korea [17], Australia [15], and Denmark [13]. The follow-up period ranged between 14 weeks to 24 months [7,13,26]; the largest trial consisted of 549 patients with KOA [7].

Table 1.
Study design characteristics.
Four studies used the American College of Rheumatology (ACR) classification criteria for the diagnosis of KOA [7,13,25,26], and one study used the International Cartilage Repair Society (ICRS) criteria [17]. Additionally, seven studies [7,14,15,17,25,26,29] used Kellgren and Lawrence (KL) grade, and one study [13] reported using the Ahlback grading system to grade the severity of KOA and to classify the participants. The majority of the studies included participants with KL grade 2 to 3 KOA [7,14,15,25,26,29].
3.2. Risk of Bias
The overall risk of bias in included studies was low, with five trials assessed as having a low risk of bias according to the Cochrane RoB-1 tool. Three studies were considered at risk of bias due to one or more RoB-1 tool domains (High risk: random sequence generation, blinding; Unclear risk: random sequence generation, selective reporting allocation concealment) being at high or unclear risk of bias (Figure 2).
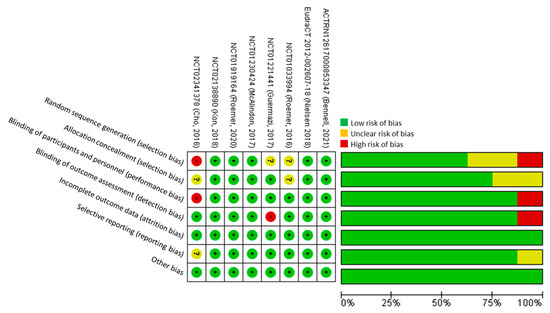
Figure 2.
Cochrane risk of bias assessment.
3.3. Primary Outcome—Effect of Intra-Articular Treatments on MRI-Assessed OA-BMLs
In all included studies that used MRI to assess the outcomes of OA-BMLs, four of those studies assessed change in OA-BML size using a modified Whole-Organ Magnetic Resonance Imaging Score (WORMS) system [7,17,25,29], while one study used MRI Osteoarthritis Knee Score (MOAKS) to assess BMLs [14]. The remaining studies did not specify using any specific type of MRI scoring tool (Table 1 and Table 2). None of the studies assessed change in OA-BMLs as a primary outcome.
Table 2.
Changes in MRI-measured OA-BMLs after treatment at longest reported follow-up.
3.4. Sprifermin
Among the two studies that used intra-articular injectable sprifermin [7,25], Roemer et al. (2020) reported a positive effect of sprifermin in OA-BML on the patellofemoral joint (PFJ); however, there was no significant difference observed in OA-BML changes when accounted for the entire knee at 24 months of follow-up (p > 0.05) [7]. In an earlier study by Roemer et al. (2016), the OA-BMLs analysed for the whole knee showed significant (p = 0.042) improvement from 6 to 12 months but not from baseline to 6 months or 12 months (p = 0.237) [25].
3.5. Corticosteroids
Two studies evaluating corticosteroids [13,26] observed similar findings and reported no significant improvement in OA-BMLs. While Nielsen et al. observed a significant improvement in OA-BML volume at 14 weeks (mean difference: −3.8; 95% CI: −7, −0.5; p = 0.03), the difference in OA-BML volume levelled out at the 26 week follow-up (mean difference: −0.8; 95% CI: −4.4, 2.8; p = 0.65) [13]. Similarly, in a study evaluating triamcinolone, McAlindon et al. reported no significant improvement (p = 0.80) in OA-BMLs between the triamcinolone and saline groups at 24 months follow-up [26].
3.6. TissueGene-C
Two studies assessing TissueGene-C (TissueGene Inc., Rockville, MD), a 3:1 mixture of non-transduced allogeneic human chondrocytes and allogeneic human chondrocytes transduced to express transforming growth factor (TGF)-β1, reported mixed findings [17,29]. Cho et al. compared high-dose TissueGene-C with low-dose TissueGene-C and reported an improvement in OA-BMLs in the high-dose group (25% vs. 22%) at 12 months follow-up [17,28]. In contrast, Guermazi et al. found no significant difference (p = 0.237) in OA-BML progression between TissueGene-C and placebo at a similar follow-up duration [27,29].
3.7. Platelet-Rich Plasma and Autologous Protein Solution
Bennell et al. compared platelet-rich plasma against placebo in patients with symptomatic medial KOA (KL grade 2–3). The study found no significant (p = 0.31) benefit of platelet-rich plasma at 12 months follow-up for the reduction in OA-BML progression (24.3% vs. 18.9%) [15].
Kon et al. compared APS with placebo and reported a beneficial effect of APS on OA-BMLs in patients with KOA. At 12 months follow-up, the study found a significant (p = 0.041) reduction in progression in OA-BMLs grade favouring APS [14].
3.8. Secondary Outcomes
3.8.1. Knee Pain
All studies assessed pain using PROMs such as visual analogue scales (VAS) [14,17,25,26,29], KOOS [13,14,15,29], or WOMAC [7,14,17,26].
A significant improvement in WOMAC pain subscale scores (p = 0.02) was observed in the study evaluating APS, compared to placebo, over 12 months of follow-up [14]. Similarly, the study comparing TissueGene-C with placebo reported a significant improvement in pain in the TissueGene-C group compared to placebo at 52 weeks follow-up [27,29]. Another study evaluating high-dose TissueGene-C with low-dose TissueGene-C found a significant improvement in pain within both groups (p < 0.001); the between-group difference, however, was not significant (p > 0.05) [17,28].
Two studies evaluating corticosteroids reported no significant benefit compared to placebo in pain reduction at 14 and 26 weeks of follow-up [13], or at 24 months [26]. Similarly, studies evaluating PRP [15] and sprifermin [7,23,25] reported no benefit, compared to placebo, in pain reduction over a follow-up period of 12 and 24 months. However, Lohmander et al. reported statistically significantly lower improvement in pain compared to placebo at 12 months follow-up (p = 0.0013) (Table 3) [24,25].
Table 3.
Changes in knee pain after treatment at longest reported follow-up.
3.8.2. Health-Related Quality-of-Life
Three studies reported HRQoL using a 36-Item Short Form Health Survey (SF-36) [14,26,27,29], and one study used the Assessment of Quality of Life–8 Dimension (AQoL-8D) tool [15]. None of the studies found a significant improvement in HRQoL assessed at 12 months or 24 months (Table 4) [14,15,26,27,29].
Table 4.
Quality of life outcomes at longest reported follow-up.
3.8.3. Safety Outcomes
The overall safety profile of intra-articular therapies was acceptable, with no noticeable concerns (Table 5). No serious adverse events (SAEs) were reported with PRP, although the PRP group experienced more commonly encountered adverse events (AEs), such as knee joint pain, swelling, and stiffness after injections compared to the placebo [15]. Kon et al. demonstrated a favourable safety profile of APS at 12 months follow-up with no significant difference in the frequency and severity of AEs between groups with SAEs unrelated to the treatment [14].
Table 5.
Safety Outcomes.
Two studies evaluating sprifermin reported an acceptable safety profile with no treatment-related SAEs or AEs reported in both trials [7,23,25]. The typical local treatment-emergent AEs were arthralgia, joint swelling, and injection-site pain [7,23,25]. Similarly, TissueGene-C trialled in two studies showed no noticeable safety concerns. One study reported no significant difference in AEs [17,28], and the second reported joint inflammation, arthralgia, and effusion to be commonly experienced AEs in the TissueGene-C arm [27,29]. Both studies reported no SAEs related to treatment [17,27,28,29]. Likewise, corticosteroids assessed in two studies were reported to have no noticeable safety concerns [13,26]. While one study reported no SAEs [13], another found no significant difference in SAEs in the two arms (p = 0.06) [26].
4. Discussion
To the best of our knowledge, this is the first study to systematically review the efficacy and safety of intra-articular therapies for the treatment of KOA with a primary focus on structural changes assessed using OA-BMLs and symptomatic improvement assessed using knee pain.
This systematic review found mixed evidence from the included primary studies. High-quality evidence from the RCTs demonstrated improvement in the whole knee MRI-assessed OA-BMLs with high dose sprifermin at 6 to 12 months [25] and in PFJ OA-BMLs up to 12 months [7]. A significant reduction in OA-BML grade was seen with APS at 12 months of follow-up [14], and OA-BMLs improved in the high-dose cohort with TissueGene-C over the same follow-up period [17]. Similarly, a statistically significant reduction in OA-BML volume in the short term (14 weeks) was observed with intra-articular corticosteroids [13]. On the other hand, the beneficial effect of sprifermin on OA-BMLs was not significant when assessed from baseline to 12 months [25] and when accounted for the entire knee region at a longer follow-up (24 months) [7]. Another study assessing TissueGene-C found no differences in the progression of OA-BMLs when compared with placebo at 12 months [29]. The study that reported a positive effect of corticosteroids at 14 weeks found the difference in OA-BMLs levelled out at 26 weeks follow-up [13], whereas another study found no benefit of triamcinolone compared to placebo over 24 months [26]. The only study assessing PRP found no significant difference in OA-BML progression at 12 months of follow-up [15]. The improvement in knee pain outcome was reported in two studies evaluating TissueGene-C [17,29] and one study assessing APS. The remaining studies found no improvement in knee pain. The HRQoL outcomes assessed using the SF-36 and AQoL-8D in four studies found no significant improvement in scores with any of the intra-articular therapies compared with placebo [14,15,26,29].
Previous studies have found a discrepancy in the association between structural changes and pain in patients with OA [9]. However, OA-BMLs correlate with pain and changes in pain [30] in patients with KOA [9,11]. Furthermore, OA-BMLs are thought to drive OA-associated pain and may help predict treatment outcomes and prognosis [9,31]. Hence, researchers have argued that OA-BMLs could be the appropriate target for novel interventions that might reduce symptoms and improve the structural progression of KOA [9,31].
Two studies that evaluated sprifermin reported positive findings for improvements in OA-BMLs when considered for PFJ [7] or at a shorter follow-up [25]. Morphologically, positive findings in the PFJ can be attributed to its indirect effect on cartilage thickness [23] and the different loading patterns compared to the more load-bearing tibiofemoral joint (TFJ). Furthermore, less worsening of cartilage surface morphology in the PFJ may lead to an improvement in OA-BMLs at the PFJ [7]. However, an improvement in the whole knee region from 6 to 12 months and not from baseline to 12 months is not easily explained, and the exact causes are still to be understood [25]. The study evaluating APS showed the beneficial effect of APS, improving OA-BMLs with a significant improvement in knee pain, compared with placebo at 12 months [14]. However, the authors noted no improvement in cartilage and suggested future studies to confirm whether OA-BML improvements could be attributed to APS or if the observed improvements were the result of other unexplained factors [14].
TissueGene-C was evaluated in two studies that reported mixed findings. Cho et al.’s. study was constrained by a smaller sample size (n = 27), shorter follow-up duration, and no placebo control [17]. Guermazi et al. found no difference in OA-BMLs with TissueGene-C when compared to placebo, however an improvement in KOA structural features and other MRI markers such as Hoffa-synovitis and effusion-synovitis was observed [29]. Furthermore, the study found no improvement in meniscal damage or hypertrophic osteophyte formation [29]. Future studies of TissueGene-C in KOA should use a sufficient sample size and use a placebo-controlled study design.
The two studies evaluating corticosteroids uniformly demonstrated no benefit in OA-BML reduction in KOA [13,26] and found no association between OA-BMLs and knee pain [13]. Although Nielsen et al. found a significant positive effect at 14 weeks of follow-up, the effect levelled out at 26 weeks. The study concluded that there was no relation between corticosteroids and OA-BML volume [13]. This finding was consistent with the McAlindon et al. study that reported significantly greater cartilage volume loss and no improvements in OA-BMLs with triamcinolone compared with saline placebo. To be noted, earlier KOA trials have reported a strong placebo response to intra-articular injection, and a higher placebo effect has been a known phenomenon in OA studies [13,32]. Bennell et al. found no benefit of PRP compared to placebo for improvements in OA-BMLs, cartilage volume loss, or pain reduction and did not support the use of PRP for treating KOA [15]. The findings were inconsistent with earlier studies reporting the beneficial effects of PRP in pain reduction [33]. This inconsistency could be attributed to discrepancies in preparing PRP, injection regimens, outcome measures, and patient characteristics. Furthermore, the lack of blinding in the earlier trials may have influenced the positive outcome with PRP [15,33].
Additionally, although intra-articular therapies involving surgery were out of the scope of this paper, we note that studies using stem cell therapy, such as bone marrow aspirate concentrate (BMAC) or mesenchymal stem cells (MSCs), showed some promise by demonstrating regression of subchondral OA-BMLs, improvement in pain and subsequent reduction in progression to TKR [12,16]. However, further studies are warranted in this area as well. Additionally, given that poor knee alignment and resultant dynamic load are known to impact significantly on the natural history of KOA, this may contribute to the heterogenous OA-BML outcomes seen in our study [9,14]. Furthermore, variability among studies was observed in terms of MRI scoring tools used to assess OA-BMLs. While the majority of studies used tools such as WORMS and MOAKS, other studies, such as Nielsen et al., used computer-assisted segmentation (CAS) for OA-BML scoring, reflecting the heterogeneity of BML measurement [13]. Future studies should use validated tools (WORMS and MOAKS) to standardise the reporting of structural changes in KOA (OA-BMLs) to allow effective comparison across studies [34,35].
The safety of intra-articular therapies across the included studies was favourable, with no notable AEs or SAEs reported. The implication of these findings is of particular interest as it confirms the absence of any harmful effect of intra-articular therapies delivered in a clinical setting. Given that the intra-articular therapies in this review are safe in a controlled environment, we suggest further studies investigate their use in the clinic over a more extended period.
Notable strengths of this systematic review include a registered protocol-based method, exhaustive database and hand-searching, and a transparent risk of bias assessment. However, this study has certain limitations. Of note, we included only the RCTs that assessed intra-articular therapy delivered in a clinic setting through a non-operative procedure for treating KOA and reported OA-BMLs as an outcome. Considerable variability existed in reporting the OA-BML outcomes across the studies, limiting the possibility of a meta-analysis. Additional work could be done to assess the effect of intra-articular therapies on structural changes associated with pain in KOA. Future work should aim to incorporate outcomes such as osteophytes, effusion, synovitis, cartilage thickness, cartilage defect, and meniscal damage. Nonetheless, our study sets the priority for future systematic reviews to focus on structural outcomes and their association with symptom improvement in patients with KOA in this rapidly evolving research area.
5. Conclusions
This systematic review found mixed evidence on the efficacy of intra-articular therapies for improving OA-BMLs in patients with KOA. While high-dose sprifermin, TissueGene-C, and APS showed some promise for improving OA-BMLs, corticosteroids and PRP showed no improvement in OA-BMLs. In addition, no intra-articular therapy, except TissueGene-C and APS, showed any improvements in knee pain. Overall, although some of the studies were promising, the data is heterogenous, and more research is needed over a longer follow-up to support the use of intra-articular therapies for improvement in OA-BMLs in KOA.
Supplementary Materials
The following supporting information can be downloaded at: https://www.mdpi.com/article/10.3390/ph15121555/s1, Supplementary Figure S1: PRISMA 2020 flow diagram. Table S1: Ovid Medline search strategy. Table S2: Search terms used for Clinicaltrial.gov and ANZCTR. Table S3: List of ongoing trials of intra-articular injectables for the treatment of knee OA. Table S4: OMERACT-OARSI response. Table S5: PRISMA 2020 checklist.
Author Contributions
Conceptualisation, A.C.K.; methodology, A.C.K., A.S., S.H., A.W.S. and G.A.L.; investigation, A.C.K., A.S. and S.H.; resources, A.C.K. and A.S.; data curation, A.C.K., S.H. and A.S.; writing—original draft preparation, A.C.K. and A.S.; writing—review and editing, A.C.K., A.S., S.H., A.W.S. and G.A.L.; visualisation, A.C.K. and A.S.; supervision, A.C.K. and A.S.; and project administration, A.C.K. and A.S. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Not applicable.
Acknowledgments
Authors would like to thank Nikki May and Caroline Litster for their contributions to this project. A.S. is supported by the International Graduate Research Scholarship, University of Tasmania. SH was supported from Operational Programme Research, Development and Education–Project, Postdoc2MUNI “(No.CZ.02.2.69/0.0/0.0/18_053/0016952)”.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Vos, T.; Lim, S.S.; Abbafati, C.; Abbas, K.M.; Abbasi, M.; Abbasifard, M.; Abbasi-Kangevari, M.; Abbastabar, H.; Abd-Allah, F.; Abdelalim, A. Global burden of 369 diseases and injuries in 204 countries and territories, 1990–2019: A systematic analysis for the Global Burden of Disease Study 2019. Lancet 2020, 396, 1204–1222. [Google Scholar] [CrossRef] [PubMed]
- Katz, J.N.; Arant, K.R.; Loeser, R.F. Diagnosis and treatment of hip and knee osteoarthritis: A review. JAMA 2021, 325, 568–578. [Google Scholar] [CrossRef] [PubMed]
- Katz, J.N.; Neogi, T.; Callahan, L.F.; Block, J.A.; Conaghan, P.G.; Simon, L.S.; Kraus, V.B.; Hochberg, M.C. Disease modification in osteoarthritis; pathways to drug approval. Osteoarthr. Cartil. Open 2020, 2, 100059. [Google Scholar] [CrossRef] [PubMed]
- Antony, B.; Singh, A. Imaging and Biochemical Markers for Osteoarthritis; Diagnostics: Basel, Switzerland, 2021; Volume 11, p. 1205. [Google Scholar]
- Skou, S.T.; Roos, E.M. Good Life with osteoArthritis in Denmark (GLA: D™): Evidence-based education and supervised neuromuscular exercise delivered by certified physiotherapists nationwide. BMC Musculoskelet. Disord. 2017, 18, 72. [Google Scholar] [CrossRef]
- Martel-Pelletier, J.; Barr, A.J.; Cicuttini, F.M.; Conaghan, P.G.; Cooper, C.; Goldring, M.B.; Goldring, S.R.; Jones, G.; Teichtahl, A.J.; Pelletier, J.-P. Osteoarthritis. Nat. Rev. Dis. Prim. 2016, 2, 16072. [Google Scholar] [CrossRef]
- Roemer, F.W.; Kraines, J.; Aydemir, A.; Wax, S.; Hochberg, M.C.; Crema, M.D.; Guermazi, A. Evaluating the structural effects of intra-articular sprifermin on cartilage and non-cartilaginous tissue alterations, based on sqMRI assessment over 2 years. Osteoarthr. Cartil. 2020, 28, 1229–1234. [Google Scholar] [CrossRef]
- Dore, D.; Quinn, S.; Ding, C.; Winzenberg, T.; Zhai, G.; Cicuttini, F.; Jones, G. Natural history and clinical significance of MRI-detected bone marrow lesions at the knee: A prospective study in community dwelling older adults. Arthritis Res. Ther. 2010, 12, R223. [Google Scholar] [CrossRef]
- Walsh, D.A.; Sofat, N.; Guermazi, A.; Hunter, D.J. Osteoarthritis Bone Marrow Lesions. Osteoarthr. Cartil. 2022. [Google Scholar] [CrossRef]
- Eriksen, E.F. Treatment of bone marrow lesions (bone marrow edema). BoneKEy Rep. 2015, 4, 755. [Google Scholar] [CrossRef]
- Zhang, Y.; Nevitt, M.; Niu, J.; Lewis, C.; Torner, J.; Guermazi, A.; Roemer, F.; McCulloch, C.; Felson, D.T. Fluctuation of Knee Pain and Changes in Bone Marrow Lesions, Effusions, and Synovitis on Magnetic Resonance Imaging. Arthritis Rheum. 2011, 63, 691–699. [Google Scholar] [CrossRef]
- Hernigou, P.; Bouthors, C.; Bastard, C.; Flouzat Lachaniette, C.H.; Rouard, H.; Dubory, A. Subchondral bone or intra-articular injection of bone marrow concentrate mesenchymal stem cells in bilateral knee osteoarthritis: What better postpone knee arthroplasty at fifteen years? A randomized study. Int. Orthop. 2021, 45, 391–399. [Google Scholar] [CrossRef] [PubMed]
- Nielsen, F.; Boesen, M.; Jurik, A.; Bliddal, H.; Nybing, J.; Ellegaard, K.; Bartholdy, C.; Bandak, E.; Henriksen, M. The effect of intra-articular glucocorticosteroids and exercise on symptoms and bone marrow lesions in knee osteoarthritis: A secondary analysis of results from a randomized controlled trial. Osteoarthr. Cartil. 2018, 26, 895–902. [Google Scholar] [CrossRef] [PubMed]
- Kon, E.; Engebretsen, L.; Verdonk, P.; Nehrer, S.; Filardo, G. Clinical outcomes of knee osteoarthritis treated With an autologous protein solution injection: A 1-Year pilot double-blinded randomized controlled trial. Am. J. Sport. Med. 2018, 46, 171–180. [Google Scholar] [CrossRef] [PubMed]
- Bennell, K.L.; Paterson, K.L.; Metcalf, B.R.; Duong, V.; Eyles, J.; Kasza, J.; Wang, Y.; Cicuttini, F.; Buchbinder, R.; Forbes, A.; et al. Effect of Intra-articular Platelet-Rich Plasma vs. Placebo Injection on Pain and Medial Tibial Cartilage Volume in Patients With Knee Osteoarthritis: The RESTORE Randomized Clinical Trial. JAMA 2021, 326, 2021–2030. [Google Scholar] [CrossRef] [PubMed]
- Hernigou, P.; Delambre, J.; Quiennec, S.; Poignard, A. Human bone marrow mesenchymal stem cell injection in subchondral lesions of knee osteoarthritis: A prospective randomized study versus contralateral arthroplasty at a mean fifteen year follow-up. Int. Orthop. 2021, 45, 365–373. [Google Scholar] [CrossRef] [PubMed]
- Cho, J.J.; Totterman, S.; Elmallah, R.K.; Kim, T.W.; Lee, B.; Mont, M.A. An MRI evaluation of patients who underwent treatment with a cell-mediated gene therapy for degenerative knee arthritis: A phase IIa clinical trial. J. Knee Surg. 2017, 30, 694–703. [Google Scholar] [CrossRef]
- Shen, L.; Yuan, T.; Chen, S.; Xie, X.; Zhang, C. The temporal effect of platelet-rich plasma on pain and physical function in the treatment of knee osteoarthritis: Systematic review and meta-analysis of randomized controlled trials. J. Orthop. Surg. Res. 2017, 12, 16. [Google Scholar] [CrossRef]
- Hohmann, E.; Tetsworth, K.; Glatt, V. Is platelet-rich plasma effective for the treatment of knee osteoarthritis? A systematic review and meta-analysis of level 1 and 2 randomized controlled trials. Eur. J. Orthop. Surg. Traumatol. 2020, 30, 955–967. [Google Scholar] [CrossRef]
- Kleinschmidt, A.S.A.; Wong; Hussain, K.; Ambrish, S.; Gregory, L. How effective are non-operative treatments for bone marrow lesions in knee osteoarthritis in adults. Prospero 2020. Available online: https://www.crd.york.ac.uk/prospero/display_record.php?RecordID=189461 (accessed on 20 November 2022).
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. Ann. Intern. Med. 2009, 151, 264–269. [Google Scholar] [CrossRef]
- Higgins, J.P.; Savović, J.; Page, M.J.; Elbers, R.G.; Sterne, J.A. Assessing risk of bias in a randomized trial. Cochrane Handb. Syst. Rev. Interv. 2019, 205–228. [Google Scholar]
- Hochberg, M.C.; Guermazi, A.; Guehring, H.; Aydemir, A.; Wax, S.; Fleuranceau-Morel, P.; Bihlet, A.R.; Byrjalsen, I.; Ragnar Andersen, J.; Eckstein, F. Effect of Intra-Articular Sprifermin vs. Placebo on Femorotibial Joint Cartilage Thickness in Patients With Osteoarthritis: The FORWARD Randomized Clinical Trial. JAMA 2019, 322, 1360–1370. [Google Scholar] [CrossRef] [PubMed]
- Lohmander, L.S.; Hellot, S.; Dreher, D.; Krantz, E.F.; Kruger, D.S.; Guermazi, A.; Eckstein, F. Intraarticular sprifermin (recombinant human fibroblast growth factor 18) in knee osteoarthritis: A randomized, double-blind, placebo-controlled trial. Arthritis Rheumatol. 2014, 66, 1820–1831. [Google Scholar] [CrossRef] [PubMed]
- Roemer, F.W.; Aydemir, A.; Lohmander, S.; Crema, M.D.; Marra, M.D.; Muurahainen, N.; Felson, D.T.; Eckstein, F.; Guermazi, A. Structural effects of sprifermin in knee osteoarthritis: A post-hoc analysis on cartilage and non-cartilaginous tissue alterations in a randomized controlled trial. BMC Musculoskelet. Disord. 2016, 17, 267. [Google Scholar] [CrossRef] [PubMed]
- McAlindon, T.E.; LaValley, M.P.; Harvey, W.F.; Price, L.L.; Driban, J.B.; Zhang, M.; Ward, R.J. Effect of Intra-articular Triamcinolone vs. Saline on Knee Cartilage Volume and Pain in Patients With Knee Osteoarthritis: A Randomized Clinical Trial. JAMA 2017, 317, 1967–1975. [Google Scholar] [CrossRef] [PubMed]
- Cherian, J.J.; Parvizi, J.; Bramlet, D.; Lee, K.H.; Romness, D.W.; Mont, M.A. Preliminary results of a phase II randomized study to determine the efficacy and safety of genetically engineered allogeneic human chondrocytes expressing TGF-β1 in patients with grade 3 chronic degenerative joint disease of the knee. Osteoarthr. Cartil. 2015, 23, 2109–2118. [Google Scholar] [CrossRef]
- Ha, C.W.; Cho, J.J.; Elmallah, R.K.; Cherian, J.J.; Kim, T.W.; Lee, M.C.; Mont, M.A. A Multicenter, Single-Blind, Phase IIa Clinical Trial to Evaluate the Efficacy and Safety of a Cell-Mediated Gene Therapy in Degenerative Knee Arthritis Patients. Hum. Gene. Clin. Dev. 2015, 26, 125–130. [Google Scholar] [CrossRef]
- Guermazi, A.; Kalsi, G.; Niu, J.; Crema, M.D.; Copeland, R.O.; Orlando, A.; Noh, M.J.; Roemer, F.W. Structural effects of intra-articular TGF-β1 in moderate to advanced knee osteoarthritis: MRI-based assessment in a randomized controlled trial. BMC Musculoskelet. Disord. 2017, 18, 461. [Google Scholar] [CrossRef]
- Roemer, F.; Collins, J.; Neogi, T.; Crema, M.; Guermazi, A. Association of knee OA structural phenotypes to risk for progression: A secondary analysis from the Foundation for National Institutes of Health Osteoarthritis Biomarkers study (FNIH). Osteoarthr. Cartil. 2020, 28, 1220–1228. [Google Scholar] [CrossRef]
- Klement, M.R.; Sharkey, P.F. The Significance of Osteoarthritis-associated Bone Marrow Lesions in the Knee. J. Am. Acad. Orthop. Surg. 2019, 27, 752–759. [Google Scholar] [CrossRef]
- Singh, A.; Kotlo, A.; Wang, Z.; Dissanayaka, T.; Das, S.; Antony, B. Efficacy and safety of hydroxychloroquine in osteoarthritis: A systematic review and meta-analysis of randomized controlled trials. Korean J. Intern. Med. 2022, 37, 210. [Google Scholar] [CrossRef] [PubMed]
- Hong, M.; Cheng, C.; Sun, X.; Yan, Y.; Zhang, Q.; Wang, W.; Guo, W. Efficacy and Safety of Intra-Articular Platelet-Rich Plasma in Osteoarthritis Knee: A Systematic Review and Meta-Analysis. Biomed Res. Int. 2021, 2021, 2191926. [Google Scholar] [CrossRef] [PubMed]
- Peterfy, C.G.; Guermazi, A.; Zaim, S.; Tirman, P.F.; Miaux, Y.; White, D.; Kothari, M.; Lu, Y.; Fye, K.; Zhao, S.; et al. Whole-Organ Magnetic Resonance Imaging Score (WORMS) of the knee in osteoarthritis. Osteoarthr. Cartil. 2004, 12, 177–190. [Google Scholar] [CrossRef] [PubMed]
- Hunter, D.J.; Guermazi, A.; Lo, G.H.; Grainger, A.J.; Conaghan, P.G.; Boudreau, R.M.; Roemer, F.W. Evolution of semi-quantitative whole joint assessment of knee OA: MOAKS (MRI Osteoarthritis Knee Score). Osteoarthr. Cartil. 2011, 19, 990–1002. [Google Scholar] [CrossRef] [PubMed]
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).