
Autologous Adipose-Derived Mesenchymal Stem Cells Combined with Shockwave Therapy Synergistically Ameliorates the Osteoarthritic Pathological Factors in Knee Joint

 ,
, 
 ,
, {kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
1. Introduction
2. Results
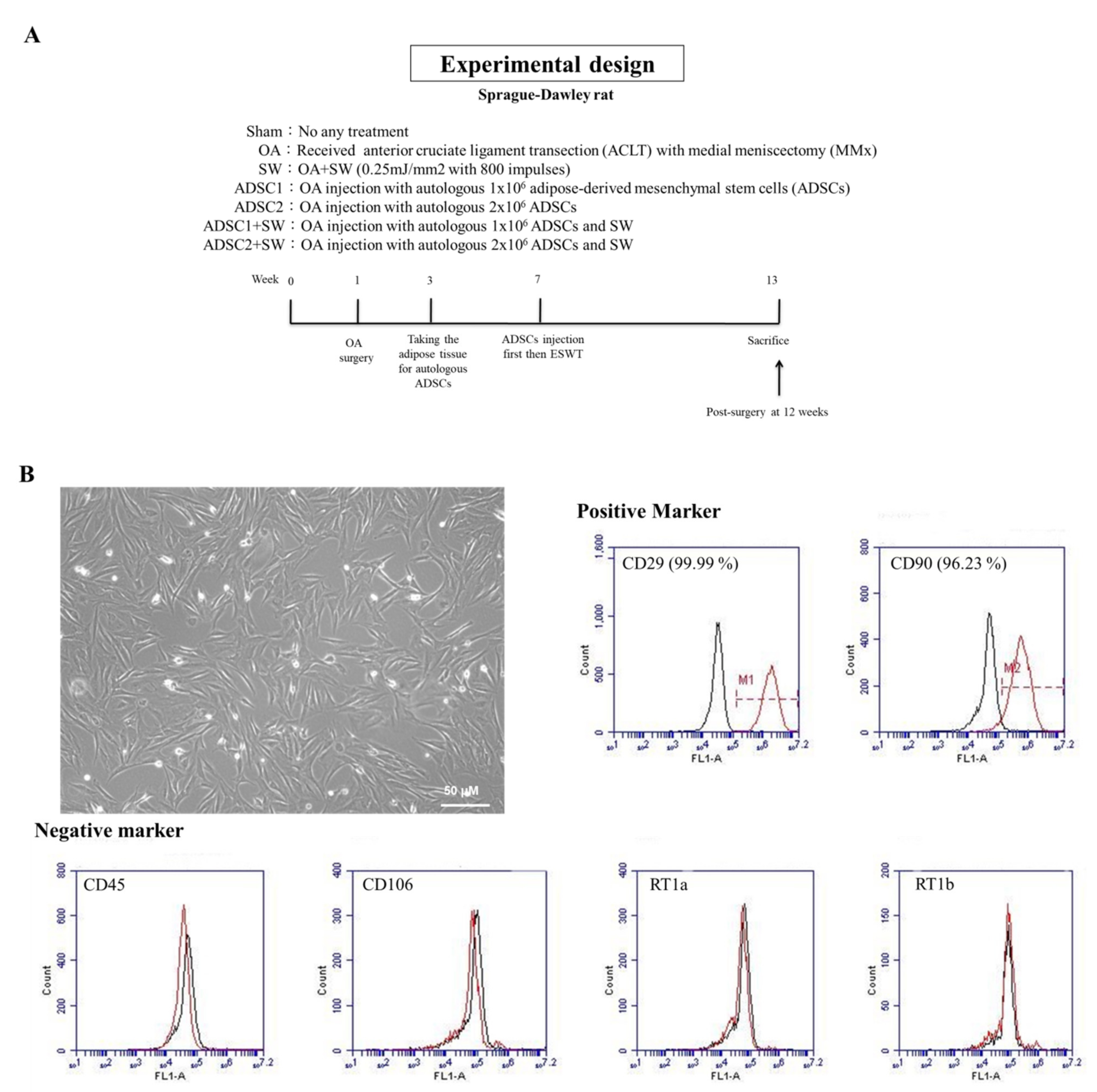
2.1. Study Design and Identification of Autologous Rat ADSCs
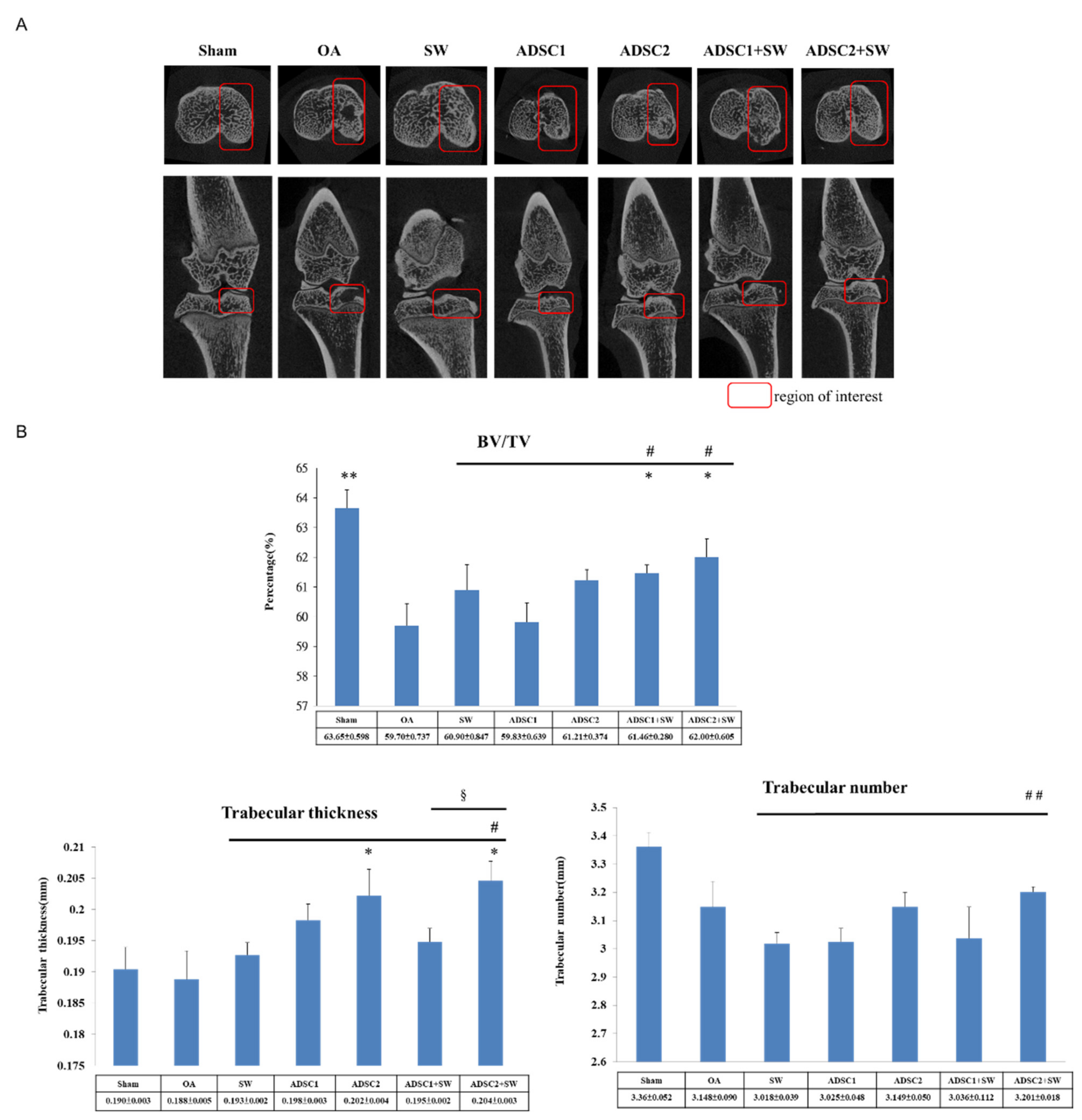
2.2. Dose-Dependent of Autologous ADSCs and SW Combination Therapy Improved Bone Remodeling in the Treatment of Knee OA
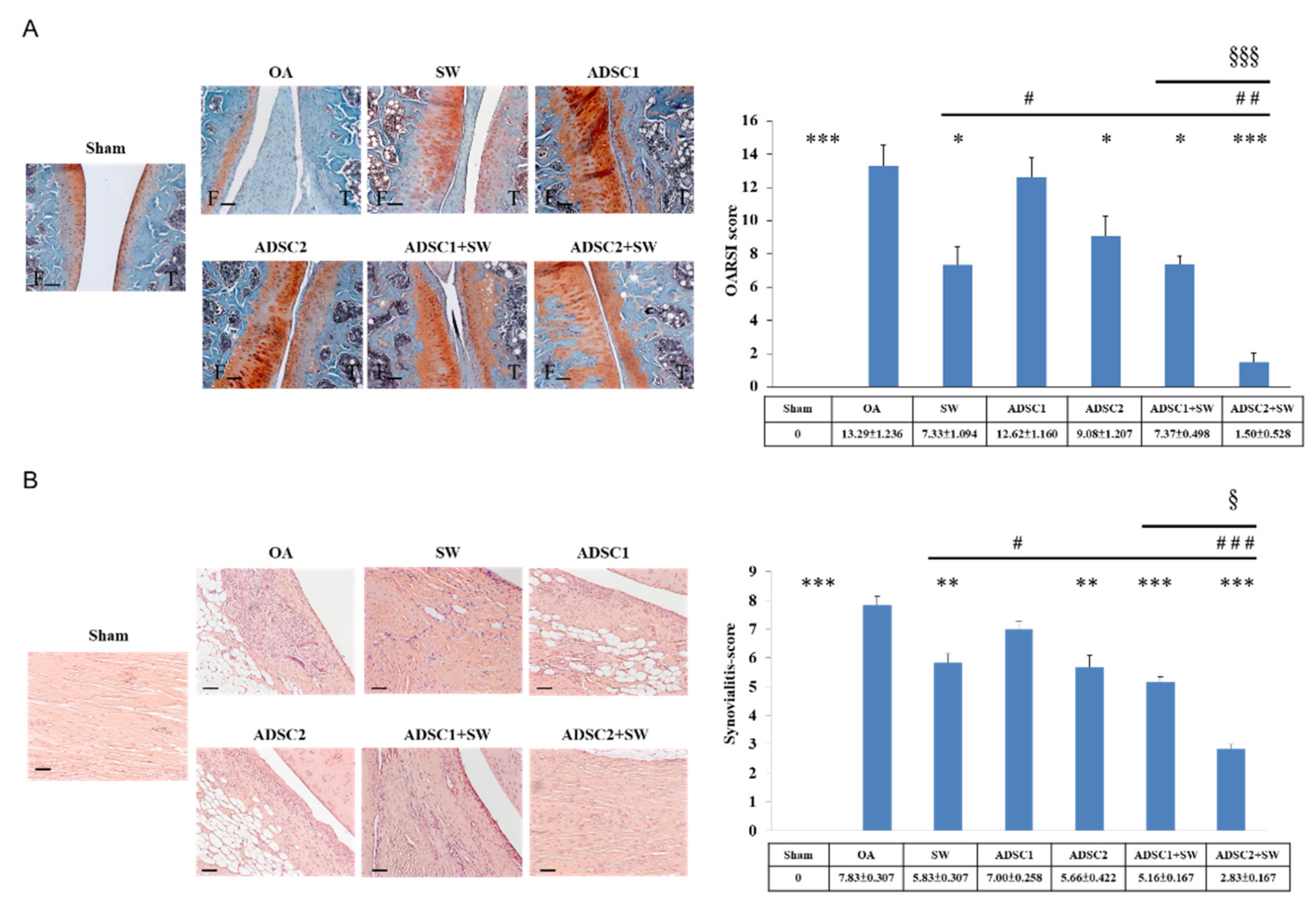
2.3. Autologous ADSCs Combined with SW Therapy Significantly Reduced the Destruction of Articular Cartilage and Synovitis in Knee OA
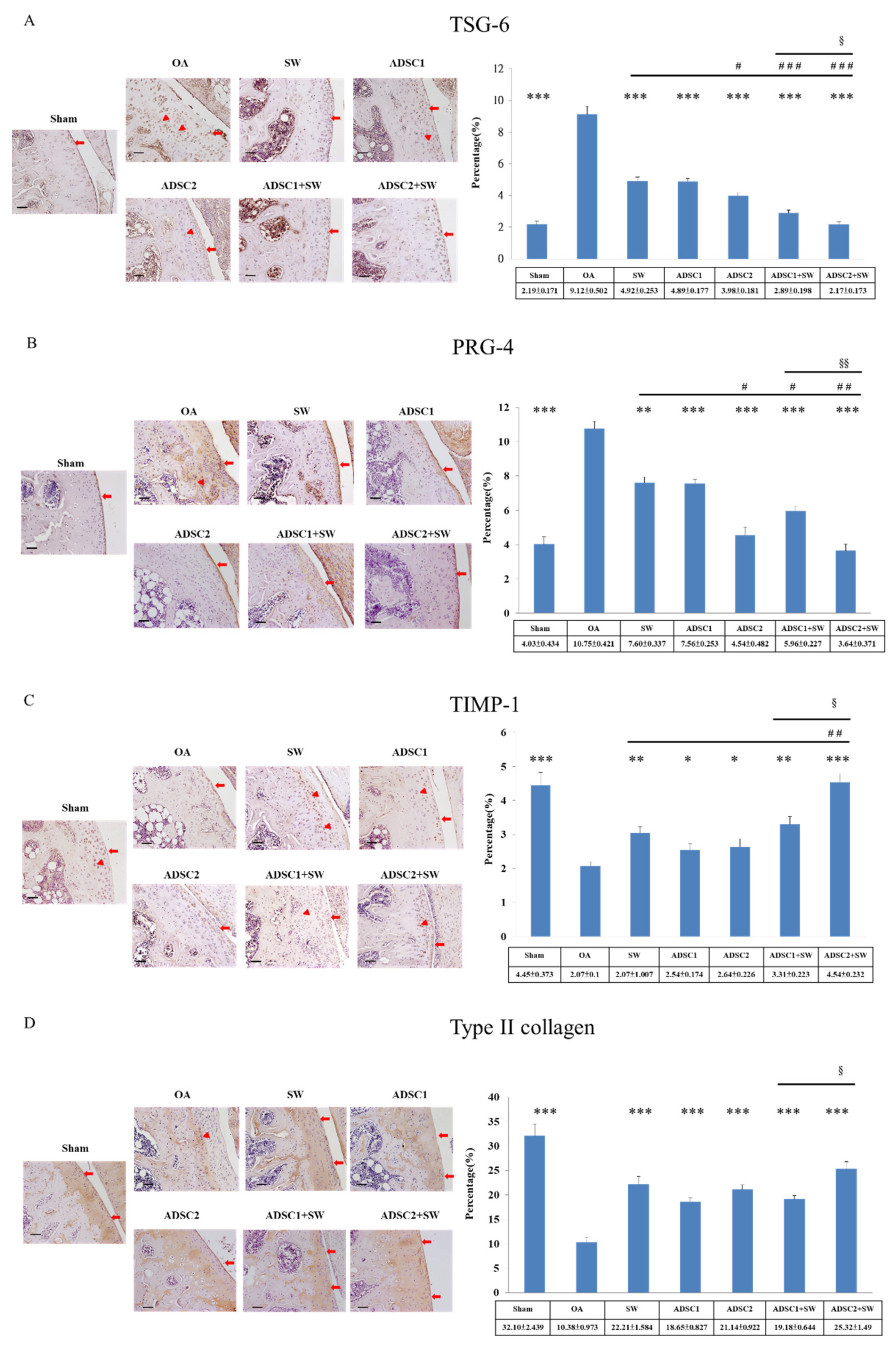
2.4. Specific Extracellular Matrix Factors Were Modulated after Autologous ADSCs and Combination Treatments in the Inflammatory Knee OA
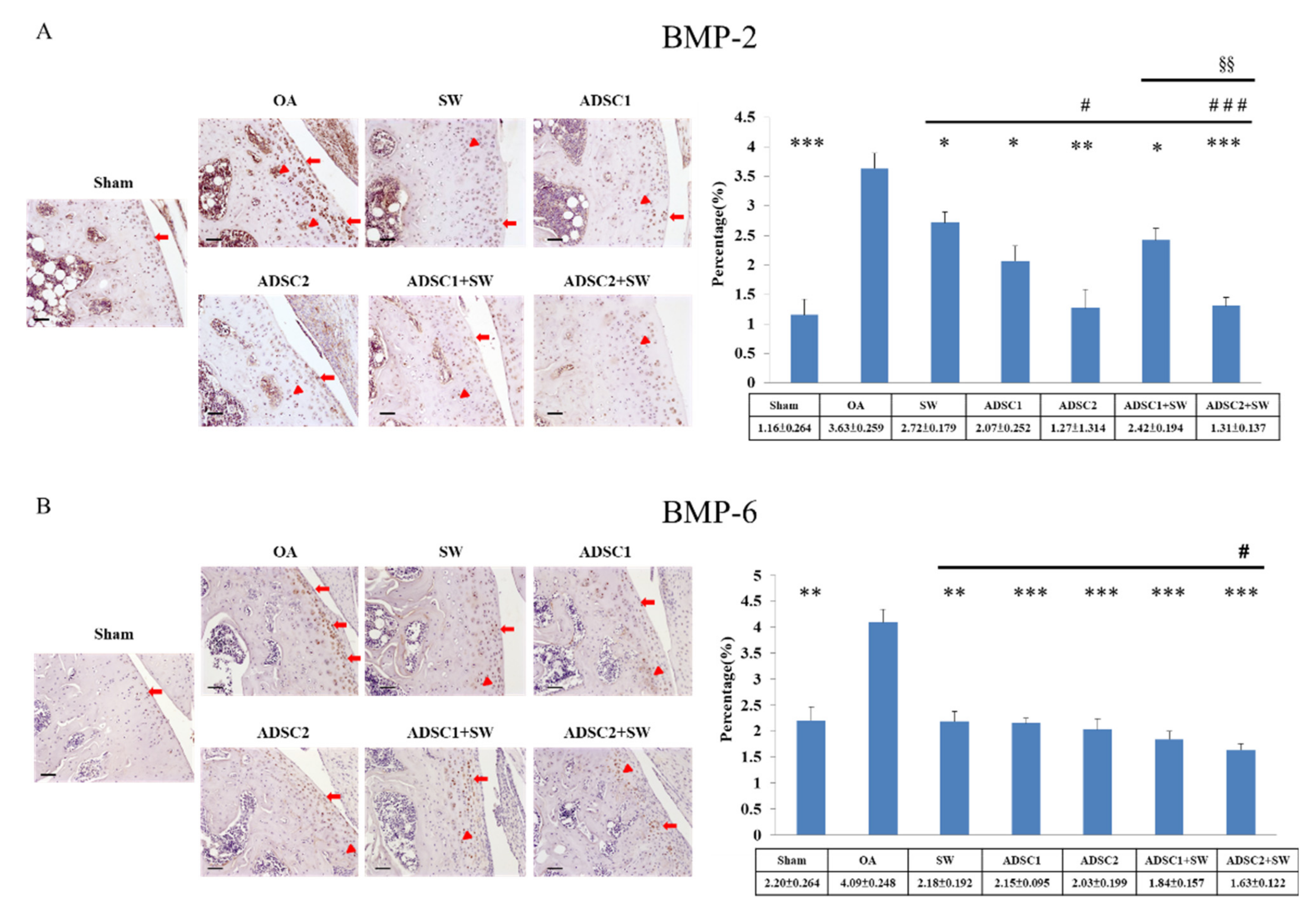
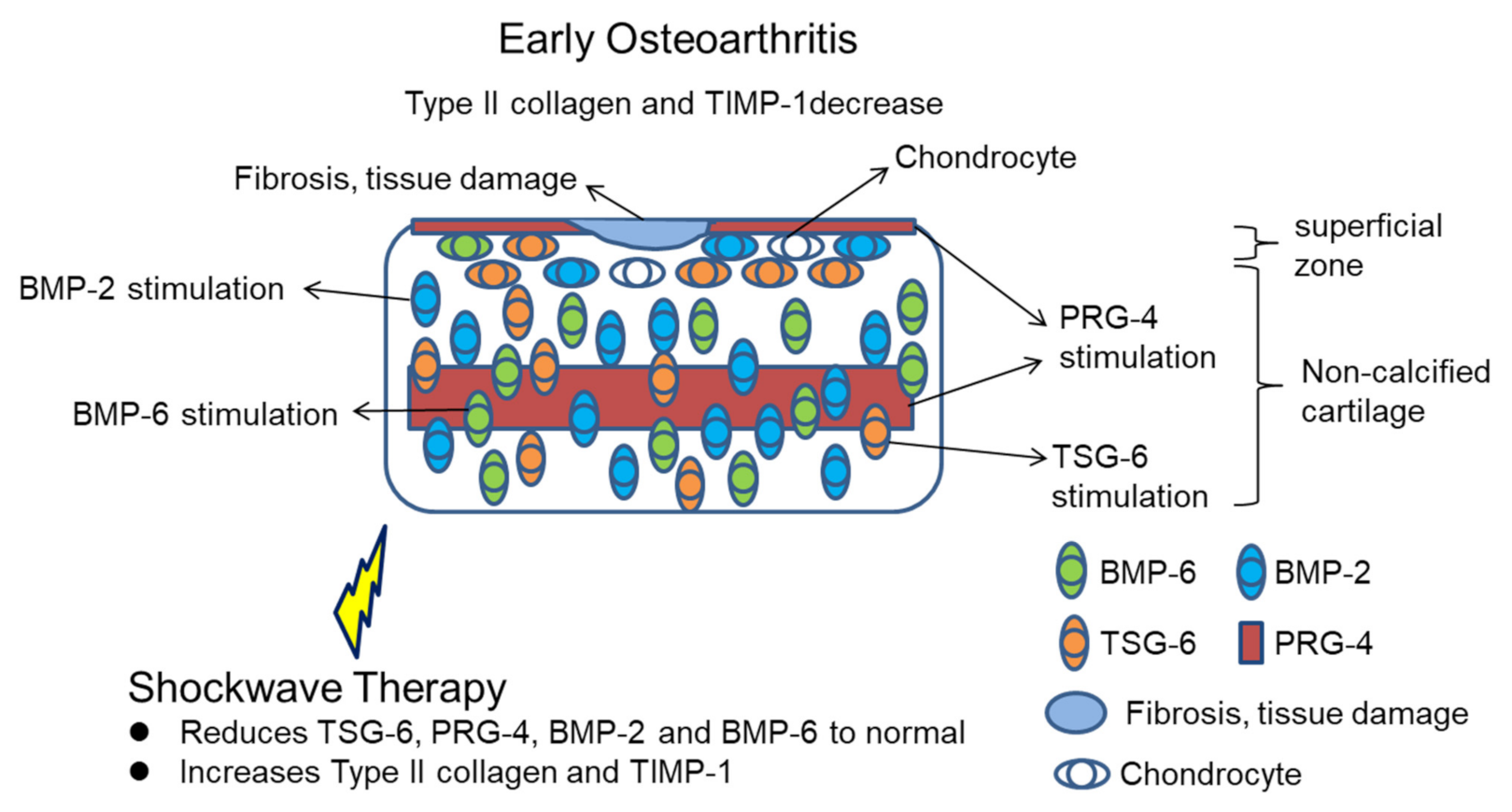
2.5. Effect of Autologous ADSCs Combined with SW Therapy in Regulation Inflammation-Induced BMP-2 and BMP-6 in the Treatment of Knee OA
3. Discussion
4. Materials and Methods
4.1. Experimental Rats
4.2. OA Rat Model
4.3. Shockwave Therapy
4.4. Isolation of Rat Autologous Adipose-Derived Mesenchymal Stem Cells
4.5. ADSCs Cell Morphology, Phenotype Identification, and Intra-Articular Injection
4.6. Micro-CT Analysis
4.7. Histopathological Examination and OARSI Score
4.8. Synovitis Scoring
4.9. Immunohistochemical Analysis
4.10. Statistical Analysis
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Tsuji, W.; Rubin, J.P.; Marra, K.G. Adipose-derived stem cells: Implications in tissue regeneration. World J. Stem Cells 2014, 6, 312–321. [Google Scholar] [CrossRef]
- Aust, L.; Devlin, B.; Foster, S.J.; Halvorsen, Y.D.C.; Hicok, K.; du Laney, T.; Sen, A.; Willingmyre, G.D.; Gimble, J.M. Yield of human adipose-derived adult stem cells from liposuction aspirates. Cytotherapy 2004, 6, 7–14. [Google Scholar] [CrossRef] [PubMed]
- Liao, H.-T. Osteogenic potential: Comparison between bone marrow and adipose-derived mesenchymal stem cells. World J. Stem Cells 2014, 6, 288. [Google Scholar] [CrossRef] [PubMed]
- Strem, B.M.; Hicok, K.C.; Zhu, M.; Wulur, I.; Alfonso, Z.; Schreiber, R.E.; Fraser, J.K.; Hedrick, M.H. Multipotential differentiation of adipose tissue-derived stem cells. Keio J. Med. 2005, 54, 132–141. [Google Scholar] [CrossRef] [PubMed]
- Han, Y.; Li, X.; Zhang, Y.; Han, Y.; Chang, F.; Ding, J. Mesenchymal stem cells for regenerative medicine. Cells 2019, 8, 886. [Google Scholar] [CrossRef] [PubMed]
- Mazini, L.; Ezzoubi, M.; Malka, G. Overview of current adipose-derived stem cell (ADSCs) processing involved in therapeutic advancements: Flow chart and regulation updates before and after COVID-19. Stem Cell Res. Ther. 2021, 12, 250–252. [Google Scholar] [CrossRef]
- Pak, J.; Lee, J.H.; Lee, S.H. Regenerative repair of damaged meniscus with autologous adipose tissue-derived stem cells. BioMed Res. Int. 2014, 2014, 1–10. [Google Scholar] [CrossRef]
- Sánchez-Guijo, F.; García-Arranz, M.; López-Parra, M.; Monedero, P.; Mata-Martínez, C.; Santos, A.; Sagredo, V.; Álvarez-Avello, J.-M.; Guerrero, J.E.; Pérez-Calvo, C.; et al. Adipose-derived mesenchymal stromal cells for the treatment of patients with severe SARS-CoV-2 pneumonia requiring mechanical ventilation. A proof of concept study. EClinicalMedicine 2020, 25, 100454. [Google Scholar] [CrossRef]
- Damia, E.; Chicharro, D.; Lopez, S.; Cuervo, B.; Rubio, M.; Sopena, J.; Vilar, J.; Carrillo, J. Adipose-derived mesenchymal stem cells: Are they a good therapeutic strategy for osteoarthritis? Int. J. Mol. Sci. 2018, 19, 1926. [Google Scholar] [CrossRef]
- Hunter, D.J.; Bierma-Zeinstra, S. Osteoarthritis. Lancet 2019, 393, 1745–1759. [Google Scholar] [CrossRef]
- Musumeci, G.; Aiello, F.; Szychlinska, M.; Di Rosa, M.; Castrogiovanni, P.; Mobasheri, A. Osteoarthritis in the 21st century: Risk factors and behaviours that influence disease onset and progression. Int. J. Mol. Sci. 2015, 16, 6093–6112. [Google Scholar] [CrossRef]
- Szekanecz, Z.; Koch, A.E. Update on synovitis. Curr. Rheum. Rep. 2001, 3, 53–63. [Google Scholar] [CrossRef]
- Pelletier, J.-P.; Martel-Pelletier, J.; Abramson, S.B. Osteoarthritis, an inflammatory disease: Potential implication for the selection of new therapeutic targets. Arthritis Rheum. 2001, 44, 1237–1247. [Google Scholar] [CrossRef]
- Chen, D.; Shen, J.; Zhao, W.; Wang, T.; Han, L.; Hamilton, J.L.; Im, H.-J. Osteoarthritis: Toward a comprehensive understanding of pathological mechanism. Bone Res. 2017, 5, 44. [Google Scholar] [CrossRef]
- Fukui, N.; Zhu, Y.; Maloney, W.J.; Clohisy, J.; Sandell, L.J. Stimulation of bmp-2 expression by pro-inflammatory cytokines Il-1 and Tnf-α in normal and osteoarthritic chondrocytes. J. Bone Jt. Surg. Am. Vol. 2003, 85, 59–66. [Google Scholar] [CrossRef]
- Pester, J.K.; Stumpfe, S.; Steinert, S.; Marintschev, I.; Aurich, M.; Hofmann, G.O. BMP-2 shows characteristic extracellular patterns in osteoarthritic cartilage: A preliminary report. GMS Interdiscip. Plast. Reconstr. Surg. DGPW 2013, 2, Doc09. [Google Scholar] [CrossRef]
- Houard, X.; Goldring, M.B.; Berenbaum, F. Homeostatic mechanisms in articular cartilage and role of inflammation in osteoarthritis. Curr. Rheum. Rep. 2013, 15. [Google Scholar] [CrossRef]
- Jevotovsky, D.S.; Alfonso, A.R.; Einhorn, T.A.; Chiu, E.S. Osteoarthritis and stem cell therapy in humans: A systematic review. Osteoarthr. Cartil. 2018, 26, 711–729. [Google Scholar] [CrossRef]
- Chen, L.; Ye, L.; Liu, H.; Yang, P.; Yang, B. Extracorporeal shock wave therapy for the treatment of osteoarthritis: A systematic review and meta-analysis. BioMed Res. Int. 2020, 2020, 1–15. [Google Scholar] [CrossRef]
- Moya, D.; Ramón, S.; Schaden, W.; Wang, C.-J.; Guiloff, L.; Cheng, J.-H. The role of extracorporeal shockwave treatment in musculoskeletal disorders. J. Bone Jt. Surg. 2018, 100, 251–263. [Google Scholar] [CrossRef]
- Leu, S.; Huang, T.-H.; Chen, Y.-L.; Yip, H.-K. Effect of extracorporeal shockwave on angiogenesis and anti-inflammation: Molecular-cellular signaling pathways. Am. J. Cardiol. 2018, 6, 109–116. [Google Scholar] [CrossRef]
- Carmignano, M.S. Extracorporeal shock wave therapy in chronic wound care. IntechOpen 2020. [Google Scholar] [CrossRef]
- Liu, T.; Shindel, A.W.; Lin, G.; Lue, T.F. Cellular signaling pathways modulated by low-intensity extracorporeal shock wave therapy. Int. J. Impot. Res. 2019, 31, 170–176. [Google Scholar] [CrossRef] [PubMed]
- d’Agostino, M.C.; Craig, K.; Tibalt, E.; Respizzi, S. Shock wave as biological therapeutic tool: From mechanical stimulation to recovery and healing, through mechanotransduction. Int. J. Surg. 2015, 24, 147–153. [Google Scholar] [CrossRef]
- Hsu, C.-C.; Cheng, J.-H.; Wang, C.-J.; Ko, J.-Y.; Hsu, S.-L.; Hsu, T.-C. Shockwave therapy combined with autologous adipose-derived mesenchymal stem cells is better than with human umbilical cord Wharton’s jelly-derived mesenchymal stem cells on knee osteoarthritis. Int. J. Mol. Sci. 2020, 21, 1217. [Google Scholar] [CrossRef] [PubMed]
- Chen, K.-H.; Hsiao, H.-Y.; Wallace, G.C.; Lin, K.-C.; Li, Y.-C.; Huang, T.-H.; Huang, C.-R.; Chen, Y.-L.; Luo, C.-W.; Lee, F.-Y.; et al. Combined adipose-derived mesenchymal stem cells and low-energy extracorporeal shock wave therapy protect the brain from brain death-induced injury in rat. J. Neuropathol. Exp. Neurol. 2019, 78, 65–77. [Google Scholar] [CrossRef]
- Zhang, W.; Ouyang, H.; Dass, C.R.; Xu, J. Current research on pharmacologic and regenerative therapies for osteoarthritis. Bone Res. 2016, 4, 40. [Google Scholar] [CrossRef] [PubMed]
- Najman, S.; Najdanović, J.; Cvetković, V. Application of adipose-derived stem cells in treatment of bone tissue defects. IntechOpen 2021. [Google Scholar] [CrossRef]
- Petrisor, B.A.; Lisson, S.; Sprague, S. Extracorporeal shockwave therapy: A systematic review of its use in fracture management. Indian J. Orthop. 2009, 43, 161. [Google Scholar] [CrossRef]
- Cheng, J.-H.; Wang, C.-J. Biological mechanism of shockwave in bone. Int. J. Surg. 2015, 24, 143–146. [Google Scholar] [CrossRef]
- Zhang, H.; Li, Z.-L.; Yang, F.; Zhang, Q.; Su, X.-Z.; Li, J.; Zhang, N.; Liu, C.-H.; Mao, N.; Zhu, H. Radial shockwave treatment promotes human mesenchymal stem cell self-renewal and enhances cartilage healing. Stem Cell Res. Ther. 2018, 9, 414–416. [Google Scholar] [CrossRef]
- Lee, T.H.; Lee, G.W.; Ziff, E.B.; Vilcek, J. Isolation and characterization of eight tumor necrosis factor-induced gene sequences from human fibroblasts. Mol. Cell. Biol. 1990, 10, 1982–1988. [Google Scholar] [CrossRef]
- Chou, C.H.; Attarian, D.E.; Wisniewski, H.G.; Band, P.A.; Kraus, V.B. TSG-6—A double-edged sword for osteoarthritis (OA). Osteoarthr. Cartil. 2018, 26, 245–254. [Google Scholar] [CrossRef]
- Bayliss, M.T.; Howat, S.L.T.; Dudhia, J.; Murphy, J.M.; Barry, F.P.; Edwards, J.C.W.; Day, A.J. Up-regulation and differential expression of the hyaluronan-binding protein TSG-6 in cartilage and synovium in rheumatoid arthritis and osteoarthritis. Osteoarthr. Cartil. 2001, 9, 42–48. [Google Scholar] [CrossRef]
- Zhu, L.; Lympany, S.; Zarebska, J.M.; Burleigh, A.; Vincent, T.L. TNF alpha-stimulated gene 6 (TSG6) is chondroprotective in vivo but overexpression cannot compensate for loss of FGF2. Osteoarthr. Cartil. 2020, 28, S107–S108. [Google Scholar] [CrossRef]
- Sayegh, S.; El Atat, O.; Diallo, K.; Rauwel, B.; Degboé, Y.; Cavaignac, E.; Constantin, A.; Cantagrel, A.; Trak-Smayra, V.; Alaaeddine, N.; et al. Rheumatoid synovial fluids regulate the immunomodulatory potential of adipose-derived mesenchymal stem cells through a TNF/NF-κB-dependent mechanism. Front. Immunol. 2019, 10, 1482. [Google Scholar] [CrossRef]
- Colón, E.; Shytuhina, A.; Cowman, M.K.; Band, P.A.; Sanggaard, K.W.; Enghild, J.J.; Wisniewski, H.-G. Transfer of inter-α-inhibitor heavy chains to hyaluronan by surface-linked hyaluronan-TSG-6 complexes. J. Biol. Chem. 2009, 284, 2320–2331. [Google Scholar] [CrossRef] [PubMed]
- Rhee, D.K.; Marcelino, J.; Baker, M.; Gong, Y.; Smits, P.; Lefebvre, V.; Jay, G.D.; Stewart, M.; Wang, H.; Warman, M.L.; et al. The secreted glycoprotein lubricin protects cartilage surfaces and inhibits synovial cell overgrowth. J. Clin. Investig. 2005, 115, 622–631. [Google Scholar] [CrossRef]
- Neu, C.P.; Reddi, A.H.; Komvopoulos, K.; Schmid, T.M.; Di Cesare, P.E. Increased friction coefficient and superficial zone protein expression in patients with advanced osteoarthritis. Arthritis Rheum. 2010, 62, 2680–2687. [Google Scholar] [CrossRef]
- Ruan, M.Z.C.; Erez, A.; Guse, K.; Dawson, B.; Bertin, T.; Chen, Y.; Jiang, M.M.; Yustein, J.; Gannon, F.; Lee, B.H.L. Proteoglycan 4 expression protects against the development of osteoarthritis. Sci. Transl. Med. 2013, 5, 176ra34. [Google Scholar] [CrossRef]
- Reesink, H.L.; Watts, A.E.; Mohammed, H.O.; Jay, G.D.; Nixon, A.J. Lubricin/proteoglycan 4 increases in both experimental and naturally occurring equine osteoarthritis. Osteoarthr. Cartil. 2017, 25, 128–137. [Google Scholar] [CrossRef] [PubMed]
- van der Kraan, P.M.; Blaney Davidson, E.N.; van den Berg, W.B. Bone morphogenetic proteins and articular cartilage. Osteoarthr. Cartil. 2010, 18, 735–741. [Google Scholar] [CrossRef] [PubMed]
- Nakase, T.; Miyaji, T.; Tomita, T.; Kaneko, M.; Kuriyama, K.; Myoui, A.; Sugamoto, K.; Ochi, T.; Yoshikawa, H. Localization of bone morphogenetic protein-2 in human osteoarthritic cartilage and osteophyte. Osteoarthr. Cartil. 2003, 11, 278–284. [Google Scholar] [CrossRef]
- Deng, Z.H.; Li, Y.S.; Gao, X.; Lei, G.H.; Huard, J. Bone morphogenetic proteins for articular cartilage regeneration. Osteoarthr. Cartil. 2018, 26, 1153–1161. [Google Scholar] [CrossRef]
- Bobacz, K.; Gruber, R.; Soleiman, A.; Erlacher, L.; Smolen, J.S.; Graninger, W.B. Expression of bone morphogenetic protein 6 in healthy and osteoarthritic human articular chondrocytes and stimulation of matrix synthesis in vitro. Arthritis Rheum. 2003, 48, 2501–2508. [Google Scholar] [CrossRef]
- Pritzker, K.P.H.; Gay, S.; Jimenez, S.A.; Ostergaard, K.; Pelletier, J.P.; Revell, P.A.; Salter, D.; van den Berg, W.B. Osteoarthritis cartilage histopathology: Grading and staging. Osteoarthr. Cartil. 2006, 14, 13–29. [Google Scholar] [CrossRef]






Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cheng, J.-H.; Yen, K.-T.; Chou, W.-Y.; Jhan, S.-W.; Hsu, S.-L.; Ko, J.-Y.; Wang, C.-J.; Kuo, C.-E.A.; Wu, S.-Y.; Hsu, T.-C.; et al. Autologous Adipose-Derived Mesenchymal Stem Cells Combined with Shockwave Therapy Synergistically Ameliorates the Osteoarthritic Pathological Factors in Knee Joint. Pharmaceuticals 2021, 14, 318. https://doi.org/10.3390/ph14040318
Cheng J-H, Yen K-T, Chou W-Y, Jhan S-W, Hsu S-L, Ko J-Y, Wang C-J, Kuo C-EA, Wu S-Y, Hsu T-C, et al. Autologous Adipose-Derived Mesenchymal Stem Cells Combined with Shockwave Therapy Synergistically Ameliorates the Osteoarthritic Pathological Factors in Knee Joint. Pharmaceuticals. 2021; 14(4):318. https://doi.org/10.3390/ph14040318
Chicago/Turabian StyleCheng, Jai-Hong, Ke-Tien Yen, Wen-Yi Chou, Shun-Wun Jhan, Shan-Ling Hsu, Jih-Yang Ko, Ching-Jen Wang, Chun-En Aurea Kuo, Szu-Ying Wu, Tsai-Chin Hsu, and et al. 2021. "Autologous Adipose-Derived Mesenchymal Stem Cells Combined with Shockwave Therapy Synergistically Ameliorates the Osteoarthritic Pathological Factors in Knee Joint" Pharmaceuticals 14, no. 4: 318. https://doi.org/10.3390/ph14040318
APA StyleCheng, J.-H., Yen, K.-T., Chou, W.-Y., Jhan, S.-W., Hsu, S.-L., Ko, J.-Y., Wang, C.-J., Kuo, C.-E. A., Wu, S.-Y., Hsu, T.-C., & Hsu, C.-C. (2021). Autologous Adipose-Derived Mesenchymal Stem Cells Combined with Shockwave Therapy Synergistically Ameliorates the Osteoarthritic Pathological Factors in Knee Joint. Pharmaceuticals, 14(4), 318. https://doi.org/10.3390/ph14040318