Older Australians Can Achieve High Adherence to the Mediterranean Diet during a 6 Month Randomised Intervention; Results from the Medley Study


 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. The Mediterranean Diet
2.2. Intervention Strategy
2.3. Three-Day Weighed Food Records
2.4. Weekly Checklists
2.5. Serum Carotenoids, Erythrocyte Fatty Acids and 24-h Urinary Metabolites
2.6. Exit Survey
| Did you… | Yes all of the time | Yes most of the time | Yes some of the time | None of the time |
| (1) Enjoy the yoghurt? | ||||
| (2) Enjoy the legumes? | ||||
| (3) Enjoy the tuna? | ||||
| (4) Enjoy the olive oil? | ||||
| (5) Enjoy the nuts? | ||||
| (6) Manage the red meat restrictions? | ||||
| (7) Manage the “extras” restrictions? | ||||
| (8) Manage with the milk restrictions? |
2.7. Statistics
3. Results
3.1. A Priori Adherence Score and Checklists
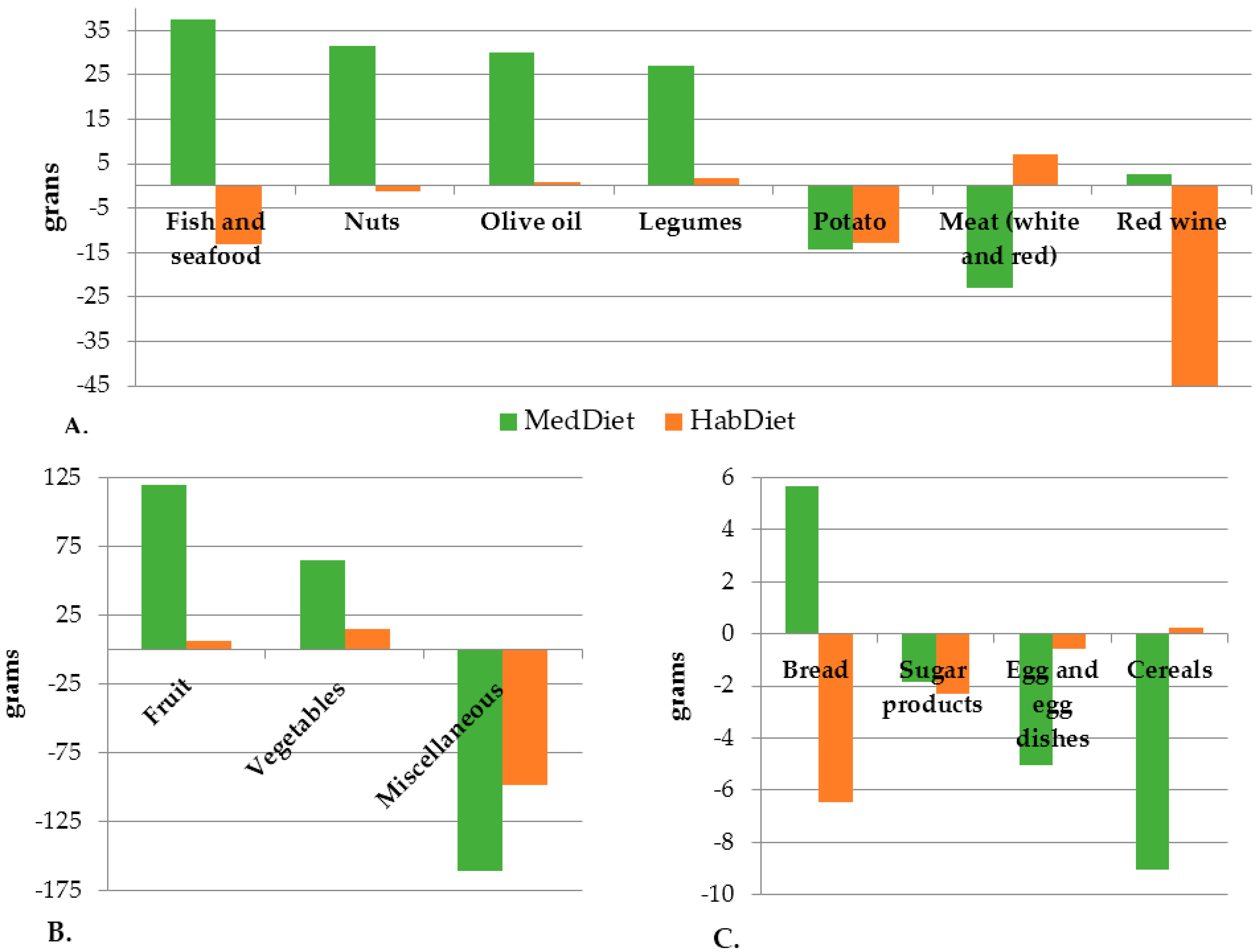
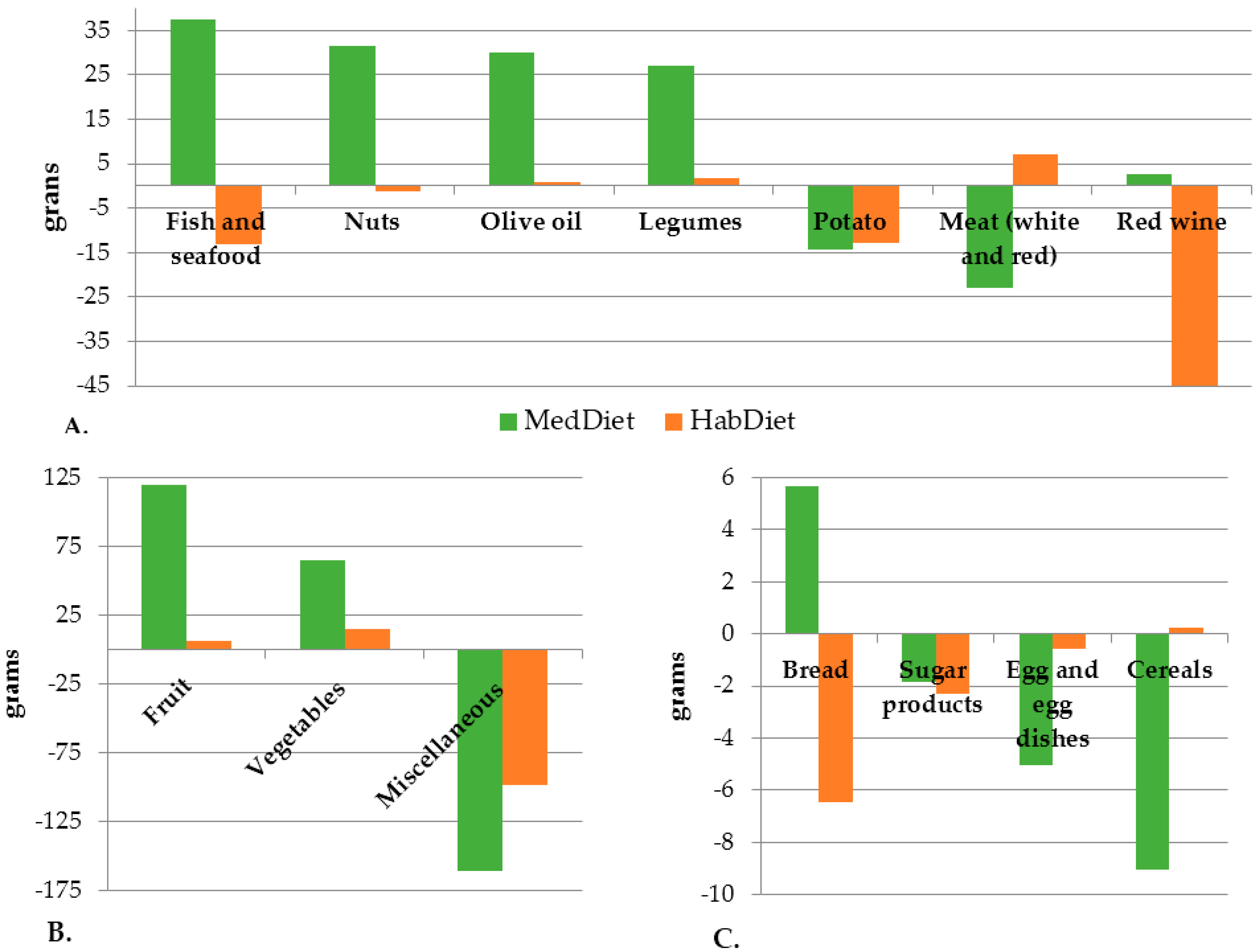
3.2. Food and Nutrient Intake
3.3. Serum Carotenoids, Erythrocyte Fatty Acids and 24-h Urinary Metabolites
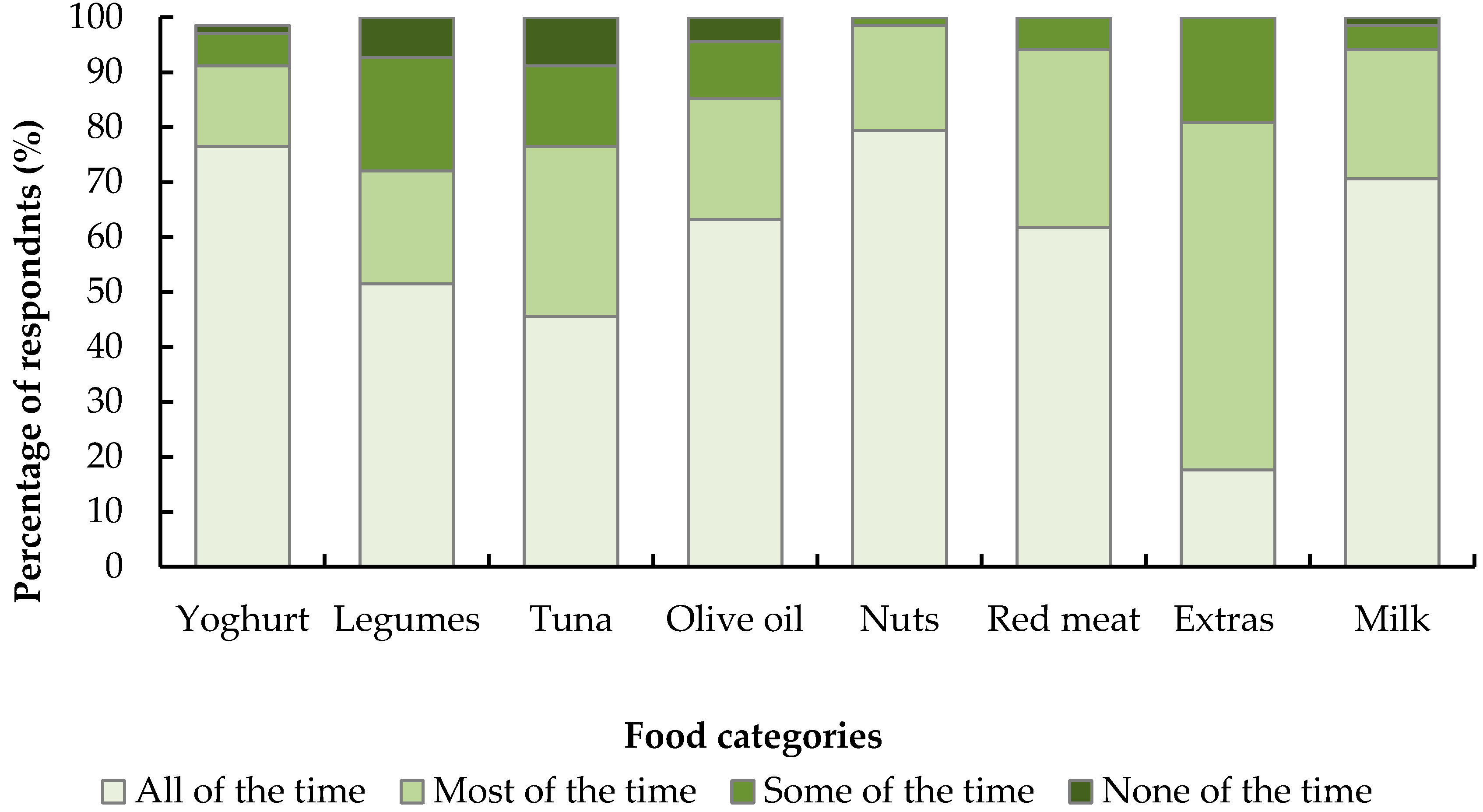
3.4. Exit Survey
4. Discussion
5. Conclusions
Supplementary Materials
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Keys, A.; Mienotti, A.; Karvonene, M.J.; Aravanis, C.; Blackburn, H.; Buzina, R.; Djordjevic, B.; Dontas, A.; Fidanza, F.; Keys, M.H.; et al. The diet and 15-year death rate in the Seven Countries Study. Am. J. Epidemiol. 1986, 124, 903–915. [Google Scholar] [CrossRef] [PubMed]
- Kromhout, D.; Menotti, A.; Bloemberg, B.; Aravanis, C.; Blackburn, H.; Buzina, R.; Dontas, A.S.; Fidanza, F.; Giampaoli, S.; Jansen, A.; et al. Dietary saturated and trans fatty acids and cholesterol and 25-year mortality from coronary heart disease: The Seven Countries Study. Prev. Med. 1995, 24, 308–315. [Google Scholar] [CrossRef] [PubMed]
- Kromhout, D.; Keys, A.; Aravanis, C.; Buzina, R.; Fidanza, F.; Giampaoli, S.; Jansen, A.; Menotti, A.; Nedeljkovic, S.; Pekkarinen, M.; et al. Food consumption patterns in the 1960s in seven countries. Am. J. Clin. Nutr. 1989, 49, 889–894. [Google Scholar] [PubMed]
- Willett, W.C.; Sacks, F.; Trichopoulou, A.; Drescher, G.; Ferro-Luzzi, A.; Helsing, E.; Trichopoulos, D. Mediterranean diet pyramid: A cultural model for healthy eating. Am. J. Clin. Nutr. 1995, 61 (Suppl. S6), 1402S–1406S. [Google Scholar] [PubMed]
- Roman, B.; Carta, L.; Marinez-Gonzalez, M.A.; Serra-Majem, L. Effectiveness of the Mediterranean diet in the elderly. Clin. Interv. Aging 2008, 3, 97–109. [Google Scholar] [PubMed]
- Sofi, F.; Macchi, C.; Abbate, R.; Gensini, G.F.; Casini, A. Mediterranean diet and health status: An updated meta-analysis and a proposal for a literature-based adherence score. Public Health Nutr. 2014, 17, 2769–2782. [Google Scholar] [CrossRef] [PubMed]
- Guallar-Castillon, P.; Rodriguez-Artalejo, F.; Tormo, M.; Sanchez, M.; Rodriguez, L.; Quiros, J.R.; Navarro, C.; Molina, E.; Martinez, C.; Marin, P.; et al. Major dietary patterns and risk of coronary heart disease in middle-aged persons from a Mediterranean country: The EPIC-Spain cohort study. Nutr. Metab. Cardiovasc. Dis. 2012, 22, 192–199. [Google Scholar] [CrossRef] [PubMed]
- Dilis, V.; Katsoulis, M.; Lagiou, P.; Trichopoulos, D.; Naska, A.; Trichopoulou, A. Mediterranean diet and CHD: The Greek European Prospective Investigation into Cancer and Nutrition cohort. Br. J. Nutr. 2012, 108, 699–709. [Google Scholar] [CrossRef] [PubMed]
- Buckland, G.; González, C.A.; Agudo, A.; Vilardell, M.; Berenguer, A.; Amiano, P.; Ardanaz, E.; Arriola, L.; Barricarte, A.; Basterretxea, M.; et al. Adherence to the Mediterranean diet and risk of coronary heart disease in the Spanish EPIC cohort study. Am. J. Epidemiol. 2009, 170, 1518–1529. [Google Scholar] [CrossRef] [PubMed]
- Knoops, K.T.; de Groot, L.C.; Kromhout, D.; Perrin, A.-E.; Moreiras-Varela, O.; Menotti, A.; van Staveren, W.A. Mediterranean diet, lifestyle factors, and 10-year mortality in elderly European men and women. The HALE project. J. Am. Med. Assoc. 2004, 292, 1433–1439. [Google Scholar] [CrossRef] [PubMed]
- Fung, T.T.; Rexrode, K.M.; Mantzoros, C.S.; Manson, J.E.; Willett, W.C.; Hu, F.B. Mediterranean diet and incidence of and mortality from coronary heart disease and stroke in women. Circulation 2009, 119, 1093–1100. [Google Scholar] [CrossRef] [PubMed]
- Estruch, R.; Ros, E.; Salas-Salvadó, J.; Covas, M.-I.; Corella, D.; Arós, F.; Gómez-Gracia, E.; Ruiz-Gutiérrez, V.; Fiol, M.; Lapetra, J.; et al. Primary prevention of cardiovascualr disease with a Mediterranean diet. N. Engl. J. Med. 2013, 368, 1279–1290. [Google Scholar] [CrossRef] [PubMed]
- Salas-Salvadó, J.; Bullo, M.; Babio, N.; Martinez-Gonzalez, M.A.; Ibarrola-Jurado, N.; Basora, J.; Estruch, R.; Covas, M.-I.; Corella, D.; Aros, F.; et al. Reduction in the incidence of type 2 diabetes with the Mediterranean diet. Diabetes Care 2011, 34, 14–19. [Google Scholar] [CrossRef] [PubMed]
- U.S. Department of Health and Human Services; U.S. Department of Agriculture. 2015–2020 Dietary Guidelines for Americans, 8th ed.; 2015; US Government. Available online: http://health.gov/dietaryguidelines/2015/guidelines/ (accessed on 8 February 2016).
- Australian Bureau of Statistics. Australian Health Survey: Consumption of Food Groups from the Australian Dietary Guidelines, 2011-12. 2016. Available online: http://www.abs.gov.au/ausstats/abs@.nsf/Lookup/4364.0.55.012main+features12011–12 (accessed on 19 October 2016).
- Australian Institute of Health and Welfare (AIHW). Australia’s Health 2014, 14th ed.; AIHW: Canberra, Australia, 2014. Available online: http://www.aihw.gov.au/publication-detail/?id=60129547205 (accessed on 31 July 2014).
- Australian Institute of Health and Welfare (AIHW). Australia’s Health 2016, 15th ed.; AIHW: Canberra, Australia, 2016. Available online: http://www.aihw.gov.au/publication-detail/?id=60129555544 (accessed on 14 November 2016).
- Kouris-Blazos, A.; Gnardellis, C.; Wahlqvist, M.L.; Trichopoulos, D.; Lukito, W.; Trichopoulou, A. Are the advantages of the Mediterranean diet transferable to other populations? A cohort study in Melbourne, Australia. Br. J. Nutr. 1999, 82, 57–61. [Google Scholar] [PubMed]
- Lara, J.; Turbett, E.; Mckevic, A.; Rudgard, K.; Hearth, H.; Mathers, J.C. The Mediterranean diet among British older adults: Its understanding, acceptability and the feasibility of a randomised brief intervention with two levels of dietary advice. Maturitas 2015, 82, 387–393. [Google Scholar] [CrossRef] [PubMed]
- Lopez-Garcia, E.; Rodriguez-Artalejo, F.; Li, T.Y.; Fung, T.T.; Li, S.; Willett, W.C.; Rimm, E.B.; Hu, F.B. The Mediterranean-style dietary pattern and mortalty among men and women with cardiovascular disease. Am. J. Clin. Nutr. 2014, 4, 172–180. [Google Scholar] [CrossRef] [PubMed]
- Trichopoulou, A.; Lagiou, P. Healthy traditional Mediterranean diet: An expression of culture, history, and lifestyle. Nutr. Rev. 1997, 55, 383–389. [Google Scholar] [CrossRef] [PubMed]
- Trichopoulou, A.; Costacou, T.; Bamia, C.; Trichopoulos, D. Adherence to a Mediterranean diet and survivial in a Greek population. N. Engl. J. Med. 2003, 348, 2599–2608. [Google Scholar] [CrossRef] [PubMed]
- Davis, C.R.; Bryan, J.; Hodgson, J.; Wilson, C.; Dhillon, V.; Murphy, K.J. A randomised controlled intervention trial evaluating the efficacy of an Australianised Mediterranean diet compared to the habitual Australian diet on cognitive function, psychological wellbeing and cardiovascular health in healthy older adults (MedLey study): Protocol paper. BMC Nutr. 2015, 1. [Google Scholar] [CrossRef]
- Knight, A.; Bryan, J.; Wilson, C.; Hodgson, J.; Murphy, K.J. A randomised controlled intervention trial evaluating the efficacy of a Mediterranean dietary pattern on cognitive function and psychological wellbeing in healthy older adults: The MedLey study. BMC Geriatr. 2015, 15. [Google Scholar] [CrossRef] [PubMed]
- Australian New Zealand Clinical Trials Registry. Available online: https://www.anzctr.org.au/Trial/Registration/TrialReview.aspx?id=363860 (accessed on 23 May 2017).
- Davis, C.R.; Bryan, J.; Hodgson, J.; Murphy, K.J. Definition of the Mediterranean diet: A literature review. Nutrients 2015, 7, 9139–9153. [Google Scholar] [CrossRef] [PubMed]
- Davis, C.R.; Bryan, J.; Hodgson, J.M.; Wilson, C.; Murphy, K.J. Older Australians can adhere to a traditional Mediterranean style diet over two weeks: A pilot dietary intervention study. BMC Nutr. 2015, 1. [Google Scholar] [CrossRef]
- Bamia, C.; Trichopoulos, D.; Ferrari, P.; Overvad, K.; Bjerregaard, L.; Tjønneland, A.; Halkjær, J.; Clavel-Chapelon, F.; Kesse, E.; Boutron-Ruault, M.-C.; et al. Dietary patterns and survival of older Europeans: The EPIC-Eldely study (European Prospective Investigation into Cancer and Nutrition). Public Health Nutr. 2007, 10, 590–598. [Google Scholar] [CrossRef] [PubMed]
- Tu, W.; Mühlhäusler, B.; Yelland, L.; Gibson, R. Correlations between blood and tissue omega-3 LCPUFA staus following dietary ALA intervention in rats. Prostaglandins Leukot. Essent. Fat. Acids 2013, 88, 53–60. [Google Scholar] [CrossRef] [PubMed]
- Barua, A.B.; Kostic, D.; Olson, J.A. New simplified procedures for the extraction and simultaneous high-performance liquid chromatographic analysis of retinol, tocopherols and carotenoids in human serum. J Chromatogr. B Biomed. Sci. Appl. 1993, 617, 257–264. [Google Scholar] [CrossRef]
- Davis, C.R.; Hodgson, J.; Woodman, R.; Bryan, J.; Wilson, C.; Murphy, K.J. A Mediterranean diet lowers blood pressure and improves endothelial function: Results from the MedLey randomized intervention trial. Am. J. Clin. Nutr. 2017, in press. [Google Scholar] [CrossRef] [PubMed]
- National Health and Medical Research Council Department of Health and Ageing. Australian Dietary Guidelines: Summary. 2013. Available online: https://www.nhmrc.gov.au/guidelines-publications/n55 (accessed on 24 October 2016).
- Carlsen, M.H.; Karslen, A.; Lillegaard, I.T.L.; Gran, J.M.; Drevon, C.A.; Blomhoff, R.; Andersen, L.F. Relative validity of fruit and vegetable intake estimated from an FFQ, using carotenoid and flavonoid biomarkers and the method of triads. Br. J. Nutr. 2011, 105, 1530–1538. [Google Scholar] [CrossRef] [PubMed]
- Al-Delaimy, W.; Slimani, N.; Ferrari, P.; Key, T.; Spencer, E.; Johansson, I.; Johansson, G.; Mattisson, I.; Wirfält, E.; Sieri, S.; et al. Plasma carotenoids as biomarkers of intake of fruits and vegetables: Ecological-level correlations in the European Prospective Investigation into Cancer and Nutrition (EPIC). Eur. J. Clin. Nutr. 2005, 59, 1397–1408. [Google Scholar] [CrossRef] [PubMed]
- Kappel, A.L.V.; Steghens, J.-P.; Zeleniuch-Jacquotte, A.; Chajés, V.; Toniolo, P.; Riboli, E. Serum carotenoids as biomarkers of fruit and vegetable consumption in the New York Women’s Health Study. Public Health Nutr. 2000, 4, 829–835. [Google Scholar] [CrossRef]
- Campbell, D.R.; Gross, M.D.; Martini, M.C.; Grandits, G.A.; Slavin, J.L.; Potter, J.D. Plasma carotenoids as biomarkers of vegetable and fruit intake. Cancer Epidemiol. Biomark. Prev. 1994, 3, 493–500. [Google Scholar]
- De Lorgeril, M.; Salen, P.; Martin, J.-L.; Monjaud, I.; Delaye, J.; Mamelle, N. Mediterranean diet, traditional risk factors, and the rate of cardiovascular complications after myocardial infarction: Final report of the Lyon Diet Heart Study. Circulation 1999, 99, 779–785. [Google Scholar] [CrossRef] [PubMed]
- Speed, C. The transposability of the Mediterranean-type diet in non-Mediterranean regions: Application to the physician/allied health team. Eur. J. Cancer Prev. 2004, 13, 529–534. [Google Scholar] [CrossRef] [PubMed]
- O’Donnell, M.; Mente, A.; Rangarajan, S.; McQueen, M.; Wang, X.; Liu, L.; Yan, H.; Lee, S.F.; Mony, P.; Devanath, A.; et al. Urinary sodium and potassium excretion, mortality and cardiovascular events. N. Engl. J. Med. 2014, 371, 612–623. [Google Scholar] [CrossRef] [PubMed]
- Schachter, J.; Harper, P.H.; Radin, M.E.; Caggiula, A.W.; McDonald, R.H.; Diven, W.F. Comparison of sodium and potassium intake with excretion. Hypertension 1980, 2, 695–699. [Google Scholar] [CrossRef] [PubMed]
- Mercado, C.I.; Cogswell, M.E.; Valderrama, A.L.; Wang, C.-Y.; Loria, C.M.; Moshfegh, A.J.; Rhodes, D.G.; Carriquiry, A.L. Difference between 24-h diet recall and urine excretion for assessing population sodium and potassium intake in adults aged 18–39 year. Am. J. Clin. Nutr. 2015, 101, 376–386. [Google Scholar] [CrossRef] [PubMed]
- Serra-Majem, L.; Nissensohn, M.; Øverby, N.C.; Fekete, K. Dietary methods and biomarkers of omega-3 fatty acids: A systematic review. Br. J. Nutr. 2012, 107 (Suppl. S2), S64–S76. [Google Scholar] [CrossRef] [PubMed]
- National Health and Medical Research Council. Nutrient Reference Values for Australia and New Zealand; Including Recommended Dietary Intakes. 2006. Available online: https://www.nrv.gov.au/ (accessed on 23 November 2016).
- Trabulsi, J.; Schoeller, D.A. Evaluation of dietary assessment instruments against doubly labeled water, a biomarker of habitual energy intake. Am. J. Physiol. Endocrinol. Metab. 2001, 281, E891–E899. [Google Scholar] [PubMed]
- Tresserra-Rimbau, A.; Rimm, E.B.; Medina-Remón, A.; Martínez-González, M.Á.; López-Sabater, C.M.; Arós, F.; Fiol, M.; Ros, E.; Serra-Majem, L.; Pintó, X.; et al. Polyphenol intake and mortality risk: A re-analysis of the PREDIMED trial. BMC Med. 2014, 12. [Google Scholar] [CrossRef] [PubMed]
- Australian Bureau of Statistics. Australian Health Survey: Nutrition First Results—Foods and Nutrients, 2011-12—Australia; Table 1.1 Mean Daily Energy and Nutrient Intake; Australian Bureau of Statistics: Canberra, Australia, 2014.
- Hoffman, R.; Gerber, M. Evaluating and adapting the Mediterranean diet for non-Mediterranean populations: A critical appraisal. Nutr. Rev. 2013, 71, 573–584. [Google Scholar] [CrossRef] [PubMed]
- Zazpe, I.; Sanchez-Tainta, A.; Martinez-Gonzalez, M.A.; Lamuela-Raventos, R.M.; Schröder, H.; Estruch, R.; Salas-Salvado, J.; Corella, D.; Fiol, M.; Gomez-Gracia, E.; et al. A large randomized individual and group intervention conduction by registered dietitians increased adherence to Mediterranean-type diets: The PREDIMED study. J. Am. Diet. Assoc. 2008, 108, 1134–1144. [Google Scholar] [CrossRef] [PubMed]
- Saulle, R.; Semyonov, L.; La Torre, G. Cost and cost-effectiveness of the Mediterranean diet: Results of a systematic review. Nutrients 2013, 5, 4566–4586. [Google Scholar] [CrossRef] [PubMed]
- Opie, R.S.; Segal, L.; Jacka, F.N.; Nicholls, L.; Dash, S.; Pizzinga, J.; Itsiopoulos, C. Assessing healthy diet affordability in a cohort with major depressive disorders. J. Public Health Epidemiol. 2015, 7, 159–169. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
| Serum Carotenoids | MedDiet (n = 80) | HabDiet (n = 72) |
|---|---|---|
| β-cryptoxanthin (ng/mL) | 57.5 ± 55.8 | 52.7 ± 42.7 |
| Lycopene (ng/mL) | 192.1 ± 133.0 | 191.2 ± 228.9 |
| α-carotene (ng/mL) | 92.0 ± 145.8 | 74.2 ± 128.7 |
| β-carotene (ng/mL) | 1287.4 ± 1489.7 | 1028.3 ± 1785.9 |
| Lutein:zeaxanthin | 505.2 ± 376.0 | 513.2 ± 238.2 |
| Erythrocyte fatty acids | n = 80 | n = 72 |
| Total SFA (%tot) | 43.3 ± 0.9 | 43.6 ± 1.1 |
| Total trans fatty acids (%tot) | 0.4 ± 0.1 | 0.4 ± 0.1 |
| Total MUFA (%tot) | 18.4 ± 0.9 | 18.5 ± 1.2 |
| Total PUFA (%tot) | 37.8 ± 1.1 | 37.2 ± 3.2 |
| Total omega-3 fatty acids (%tot) | 10.7 ± 2.6 | 10.4 ± 2.7 |
| Total omega-6 fatty acids (%tot) | 27.1 ± 2.7 | 27.1 ± 2.8 |
| Omega-6:omega-3 | 2.7 ± 0.8 | 2.8 ± 0.8 |
| Omega-3 index | 7.4 ± 2.5 | 7.1 ± 2.5 |
| Urinary metabolites | n = 80 | n = 70 |
| Sodium (mmol/24 h) | 115.2 ± 51.0 | 119.6 ± 78.3 |
| Potassium (mmol/24 h) | 79.4 ± 24.4 | 78.3 ± 23.8 |
| Calcium (mmol/24 h) | 3.6 ± 1.8 | 4.1 ± 2.0 |
| Magnesium (mmol/24 h) | 4.6 ± 2.2 | 4.3 ± 1.5 |
| Adherence Score | Adherence Scores | p for Interaction | |||||
|---|---|---|---|---|---|---|---|
| Baseline | 2 Months | 4 Months | |||||
| MedDiet | HabDiet | MedDiet | HabDiet | MedDiet | HabDiet | ||
| 15-point score | 7.1 ± 1.9 | 7.4 ± 2.4 | 9.7 ± 2.4 | 7.7 ± 2.2 | 10.6 ± 1.7 | 7.9 ± 2.5 | <0.001 |
| 10-point MDS 1 | 4.2 ± 1.7 | 4.2 ± 1.6 | 5.9 ± 1.6 | 4.1 ± 1.7 | 6.2 ± 1.4 | 4.4 ± 1.5 | <0.001 |
| 10-point MDS 2 | 2.8 ± 1.4 | 2.8 ± 1.5 | 3.7 ± 2.1 | 2.6 ± 1.5 | 4.7 ± 1.3 | 3.0 ± 1.3 | <0.001 |
| MedDiet (n = 80) | HabDiet (n = 70) | Between Group Difference at 4 Months 1 | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Nutrients 2 | Baseline | 4 Months | p Value | Baseline | 4 Months | p Value | Diet*Visit Interaction | Difference (95% CI) | p Value |
| Energy (kJ) | 8847.2 ± 229.7 | 8777.8 ± 245.5 | 1.00 | 8773.9 ± 229.7 | 8380.1 ± 252.1 | 0.377 | 0.41 | 384.3 (−1070.6, 302.2) | 0.27 |
| kJ from protein (%) | 19.3 ± 0.37 | 19.5 ± 0.4 | 1.00 | 19.3 ± 0.4 | 19.3 ± 0.4 | 1.00 | 0.96 | 0.2 (−0.9, 1.3) | 0.74 |
| kJ from fat (%) | 33.5 ± 0.7 | 38.7 ± 0.8 | <0.001 | 34.4 ± 0.7 | 35.6 ± 0.8 | 0.65 | <0.001 | 3.1 (1.1, 5.2) | <0.01 |
| kJ from saturated fat (%) | 12.1 ± 0.3 | 9.1 ± 0.3 | <0.001 | 12.9 ± 0.3 | 13.1 ± 0.3 | 1.00 | <0.01 | −4.0 (−4.9, −3.1) | <0.001 |
| kJ from monounsaturated fat (%) | 13.2 ± 0.4 | 19.7 ± 0.5 | <0.001 | 13.2 ± 0.4 | 14.3 ± 0.5 | 0.24 | <0.001 | 5.5 (4.2, 6.8) | <0.001 |
| kJ from carbohydrate (%) | 42.3 ± 0.7 | 37.8 ± 0.8 | <0.001 | 41.3 ± 0.8 | 40.3 ± 0.8 | 0.77 | <0.001 | −2.5 (−4.7, −0.3) | 0.03 |
| kJ from alcohol (%) | 4.5 ± 1.1 | 2.7 ± 1.2 | 0.40 | 2.9 ± 1.2 | 3.4 ± 0.4 | 1.00 | 0.47 | −0.6 (−3.2, 2.0,) | 0.67 |
| Fat as mono (%) | 42.5 ± 0.7 | 54.3 ± 0.7 | <0.001 | 41.3 ± 0.7 | 43.1 ± 0.7 | 0.09 | <0.001 | 11.2 (9.3, 13.7) | <0.001 |
| Fat as saturated (%) | 39.6 ± 0.8 | 25.3 ± 0.9 | <0.001 | 41.0 ± 0.9 | 40.0 ± 0.9 | 1.00 | <0.001 | −14.7 (−17.1, −12.3) | <0.001 |
| Cholesterol (mg/MJ) | 33.3 ± 1.4 | 25.5 ± 1.5 | <0.001 | 34.7 ± 1.5 | 36.1 ± 1.5 | 1.00 | <0.001 | −10.5 (−14.7, −6.3) | <0.001 |
| Sugars (g/MJ) | 12.5 ± 0.38 | 11.3 ± 0.36 | <0.01 | 12.1 ± 0.4 | 11.6 ± 0.38 | 0.56 | 0.51 | −0.3 (−1.3, 0.8) | 0.62 |
| MUFA:SFA | 1.2 ± 0.1 | 2.2 ± 0.1 | <0.001 | 1.1 ± 0.1 | 1.2 ± 0.1 | 0.50 | <0.001 | 1.0 (0.9, 1.2) | <0.001 |
| Fibre (g/MJ) | 3.4 ± 0.1 | 3.8 ± 0.1 | <0.01 | 3.2 ± 0.1 | 3.1 ± 0.1 | 0.80 | <0.01 | 0.7 (0.4, 1.0) | <0.001 |
| Vitamin C (mg/MJ) | 17.6 ± 1.1 | 18.9 ± 0.97 | 1.00 | 15.9 ± 1.2 | 14.2 ± 1.0 | 0.53 | 0.21 | 4.7 (1.9, 7.5) | <0.01 |
| Vitamin E (mg/MJ) | 1.2 ± 0.5 | 1.9 ± 0.6 | <0.001 | 1.2 ± 0.6 | 1.3 ± 0.6 | 0.74 | <0.001 | 0.6 (0.5, 0.8) | <0.001 |
| Total folate (µg/MJ) | 54.4 ± 2.1 | 56.1 ± 1.2 | 1.00 | 49.8 ± 2.3 | 47.3 ± 2.0 | 1.00 | 0.51 | 8.8 (3.3, 14.4) | <0.01 |
| Total vitamin A equivalents (µg/MJ) | 130.4 ± 6.8 | 140.0 ± 15.4 | 1.00 | 121.3 ± 7.3 | 131.4 ± 16.0 | 1.00 | 0.37 | 8.6 (−35.5, 52.6) | 0.70 |
| B-carotene equivalents (µg/MJ) | 588.7 ± 40.4 | 687.4 ± 53.6 | 0.33 | 473.4 ± 43.2 | 467.4 ± 55.6 | 1.00 | 0.31 | 220.0 (67.4, 372.7) | <0.01 |
| Sodium (mg/MJ) | 264.5 ± 8.8 | 202.3 ± 6.8 | <0.001 | 267.7 ± 9.4 | 259.5 ± 7.0 | 1.00 | <0.01 | −57.2 (−76.6, −37.9) | <0.001 |
| Potassium (mg/MJ) | 447.1 ± 10.6 | 442.5 ± 9.0 | 1.00 | 421.6 ± 11.3 | 403.1 ± 9.3 | 0.48 | 0.71 | 39.3 (13.8, 64.9) | <0.01 |
| Calcium (mg/MJ) | 109.3 ± 4.0 | 105.5 ± 3.2 | 1.00 | 107.1 ± 4.3 | 103.9 ± 3.4 | 1.00 | 0.62 | 1.6 (−7.7, 10.8) | 0.74 |
| Magnesium (mg/MJ) | 50.2 ± 1.3 | 44.2 ± 2.0 | 0.01 | 46.4 ± 1.4 | 41.8 ± 2.1 | 0.09 | 0.48 | 2.4 (−3.2, 8.1) | 0.39 |
| Iron (mg/MJ) | 1.61 ± 0.4 | 1.57 ± 0.4 | 1.00 | 1.5 ± 0.4 | 1.5 ± 0.4 | 1.00 | 0.53 | 0.1 (−0.1, 2.1) | 0.07 |
| Zinc (mg/MJ) | 1.4 ± 0.4 | 1.2 ± 0.5 | <0.01 | 1.4 ± 0.4 | 1.5 ± 0.5 | 0.09 | <0.001 | −0.2 (−0.4, −0.1) | <0.01 |
| Total long-chain n3 (mg/MJ) | 50.4 ± 6.6 | 89.0 ± 7.1 | <0.001 | 52.9 ± 7.0 | 35.9 ± 7.3 | 0.27 | <0.001 | 53.1 (32.9, 73.2) | <0.001 |
| Linoleic acid (g/MJ) | 1.3 ± 0.6 | 1.7 ± 0.6 | <0.001 | 1.3 ± 0.6 | 1.3 ± 0.6 | 1.00 | <0.01 | 0.4 (0.2, 0.6) | <0.001 |
| A-linolenic acid (g/MJ) | 0.16 ± 0.01 | 0.18 ± 0.01 | 0.68 | 0.17 ± 0.1 | 0.14 ± 0.1 | 0.17 | 0.07 | 0.0 (0.0, 0.1) | 0.03 |
| Total flavonoids (mg/MJ) | 59.7 ± 5.7 | 64.9 ± 5.8 | 0.35 | 68.1 ± 6.0 | 63.0 ± 6.0 | 0.04 | 0.94 | 3.4 (−16.0, 22.8) | 0.73 |
| Anthocyanidins (mg/MJ) | 7.8 ± 1.0 | 10.0 ± 1.0 | 0.02 | 7.8 ± 1.1 | 6.6 ± 1.1 | 0.20 | 0.01 | 3.3 (0.03, 6.66) | 0.05 |
| Flavan-3-ols (mg/MJ) | 45.0 ± 4.7 | 47.3 ± 4.8 | 0.51 | 52.6 ± 5.0 | 51.7 ± 5.0 | 0.83 | 0.82 | −2.1 (−16.3, 20.5) | 0.82 |
| Flavanones (mg/MJ) | 3.0 ± 0.4 | 2.3 ± 0.3 | 0.05 | 2.6 ± 0.4 | 1.4 ± 0.3 | <0.01 | 0.59 | 0.9 (−0.1, 1.8) | 0.06 |
| Flavones (mg/MJ) | 0.3 ± 0.1 | 0.6 ± 0.1 | 0.10 | 0.4 ± 0.1 | 0.3 ± 0.1 | 0.50 | 0.36 | 0.6 (−0.2, 1.4) | 0.14 |
| Flavonols (mg/MJ) | 3.3 ± 0.3 | 3.6 ± 0.3 | 0.16 | 3.2 ± 0.3 | 3.1 ± 0.3 | 0.56 | 0.18 | 0.5 (−0.2, 1.3) | 0.18 |
| Isoflavones (mg/MJ) | 0.1 ± 0.0 | 0.2 ± 0.1 | 0.26 | 0.1 ± 0.0 | 0.1 ± 0.1 | 0.82 | 0.48 | 0.2 (−0.1, 0.4) | 0.25 |
| Carotenoids (mg/MJ) | 1.6 ± 0.1 | 2.0 ± 0.1 | 0.03 | 1.4 ± 0.1 | 1.3 ± 0.2 | 0.46 | 0.03 | 0.8 (0.5 1.2) | <0.001 |
| MedDiet (n = 80) | HabDiet (n = 70) | Between Group Difference at 4 Months | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Foods 1 (g/mJ/Day) | Baseline 2 | 4 Months | p Value | Baseline 2 | 4 Months | p Value | Diet*Visit Interaction | Difference (95% CI) | p Value |
| Extra virgin olive oil | 0.3 ± 0.1 | 3.6 ± 0.2 | <0.001 | 0.6 ± 0.1 | 0.8 ± 0.2 | 1.00 | <0.001 | 2.9 (2.3, 3.4) | <0.001 |
| Vegetables | 18.2 ± 1.4 | 25.7 ± 1.6 | <0.001 | 19.0 ± 21.8 | 21.9 ± 1.6 | 0.40 | 0.02 | 3.8 (−0.6, 8.2) | 0.09 |
| White potato | 4.8 ± 0.6 | 3.2 ± 0.6 | 0.09 | 5.5 ± 0.7 | 3.9 ± 0.6 | 0.09 | 0.09 | −0.7 (−2.4, 0.9) | 0.37 |
| Fruits | 30.6 ± 2.0 | 42.4 ± 2.3 | <0.001 | 31.1 ± 2.1 | 35.6 ± 2.4 | 0.47 | 0.04 | 6.8 (0.2, 13.4) | 0.05 |
| Nuts | 1.9 ± 0.3 | 5.6 ± 0.7 | <0.001 | 1.7 ± 0.3 | 1.9 ± 0.7 | 1.00 | <0.01 | 3.8 (1.9, 5.6) | <0.001 |
| Legumes | 2.1 ± 0.5 | 5.2 ± 0.6 | <0.001 | 1.7 ± 0.5 | 2.2 ± 0.6 | 1.00 | <0.01 | 3.0 (1.3, 4.7) | <0.01 |
| Bread | 8.3 ± 0.5 | 9.1 ± 0.6 | 0.26 | 9.5 ± 0.6 | 9.0 ± 0.6 | 1.00 | 0.22 | 0.05 (−1.6, 1.7) | 0.95 |
| Cereals | 8.2 ± 0.8 | 7.4 ± 0.8 | 1.00 | 7.7 ± 0.9 | 8.3 ± 0.8 | 1.00 | 0.40 | −0.8 (−3.1, 1.4) | 0.46 |
| Dairy (all types) | 30.4 ± 2.5 | 37.5 ± 2.2 | <0.01 | 32.2 ± 2.7 | 29.8 ± 2.2 | 0.94 | 0.01 | 7.7 (1.6, 13.8) | 0.01 |
| Fish and seafood | 4.2 ± 0.7 | 9.2 ± 0.7 | <0.001 | 6.5 ± 0.7 | 4..8 ± 0.7 | 0.17 | <0.001 | 4.5 (2.4, 6.5) | <0.001 |
| Eggs | 2.5 ± 0.4 | 2.2 ± 0.4 | 1.00 | 2.9 ± 0.4 | 3.2 ± 0.4 | 1.00 | 0.76 | −1.0 (−2.1, 0.2) | 0.09 |
| Meats | 8.0 ± 0.8 | 5.3 ± 0.8 | 0.03 | 8.8 ± 0.9 | 10.7 ± 0.9 | <0.01 | 0.43 | −5.4 (−7.8, −3.1) | <0.001 |
| Red wine | 8.7 ± 1.8 | 10.7 ± 1.5 | 0.62 | 11.9 ± 1.9 | 7.5 ± 1.6 | 0.03 | 0.02 | 3.2 (−1.2, 7.5) | 0.15 |
| Sugars | 1.3 ± 0.2 | 1.1 ± 0.2 | 0.9 | 1.3 ± 0.2 | 1.2 ± 0.2 | 1.00 | 0.01 | −0.1 (−0.7, 0.5) | 0.70 |
| Miscellaneous | 32.1 ± 2.1 | 15.6 ± 1.8 | <0.001 | 34.5 ± 2.2 | 23.9 ± 1.8 | <0.001 | 0.10 | −8.2 (−13.3, −3.2) | <0.01 |
| MedDiet Group (n = 82) | HabDiet Group (n = 70) | Between Group Difference 6 Months | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Baseline | 6 Months | p Value | Baseline | 6 Months | p Value | DietxVisit Interaction | Difference (95% CI) | p Value | |
| β-cryptoxanthin (ng/mL) | 56.8 ± 5.6 | 52.7 ± 6.6 | 1.00 | 51.3 ± 5.9 | 49.5 ± 7.0 | 1.00 | 0.77 | 0.1 (−0.1, 0.2) | 0.44 |
| Lycopene (ng/mL) | 184.0 ± 13.8 | 197.4 ± 13.4 | 1.00 | 162.1 ± 14.8 | 135.6 ± 13.7 | 1.00 | <0.01 | 0.2 (0.1, 0.3) | <0.01 |
| α-carotene (ng/mL) | 77.6 ± 10.2 | 125.1 ± 15.6 | <0.01 | 61.6 ± 10.8 | 55.0 ± 16.1 | 0.50 | <0.01 | 0.2 (−0.0, 0.4) | 0.12 |
| β-carotene (ng/mL) | 1287.4 ± 141.4 | 1543.8 ± 136.1 | 0.10 | 858.7 ± 150.8 | 851.8 ± 136.3 | 1.00 | <0.001 | 0.2 (0.1, 0.3) | <0.001 |
| Lutein:zeaxanthin | 489.5 ± 30.6 | 524.6 ± 33.6 | 0.40 | 511.3 ± 32.2 | 521.8 ± 34.9 | 1.00 | 0.30 | −0.0 (−0.1, −0.1) | 0.65 |
| Total erythrocyte saturated fat (%) | 43.3 ± 0.1 | 42.8 ± 0.1 | <0.001 | 43.5 ± 0.1 | 43.5 ± 0.1 | 1.00 | <0.001 | −0.7 (−1.0, −0.5) | <0.001 |
| Total erythrocyte trans−fat (%) | 0.44 ± 0.02 | 0.37 ± 0.02 | <0.001 | 0.4 ± 0.02 | 0.4 ± 0.02 | 0.34 | <0.001 | −0.0 (−0.1, 0.0) | 0.08 |
| Total erythrocyte MUFA (%) | 18.4 ± 0.1 | 19.3 ± 0.1 | <0.001 | 18.5 ± 0.1 | 18.6 ± 0.1 | 1.00 | <0.001 | 0.8 (0.4, 1.1) | <0.001 |
| Total erythrocyte omega-3 (%) | 10.8 ± 0.3 | 10.9 ± 0.3 | 1.00 | 10.5 ± 0.3 | 10.7 ± 0.3 | 0.30 | 0.24 | 0.2 (−0.6, 1.1) | 0.62 |
| Docosahexaenoic acid (22:6 n3) (%) | 5.8 ± 0.14 | 6.1 ± 0.13 | 0.01 | 5.6 ± 0.14 | 5.7 ± 0.14 | 0.29 | 0.03 | 0.31 (−0.06, 0.68) | 0.10 |
| Eicosapentaenoic acid (20:5 n3) (%) | 1.8 ± 0.13 | 1.8 ± 0.13 | 1.00 | 1.7 ± 0.14 | 1.8 ± 0.14 | 0.38 | 0.58 | 0.01 (−0.37, 0.38) | 0.98 |
| Docosapentaenoic acid (22:5 n3) (%) | 3.0 ± 0.06 | 2.9 ± 0.06 | <0.001 | 3.0 ± 0.07 | 3.0 ± 0.06 | 1.00 | <0.001 | −0.11 (−0.29, 0.06) | 0.19 |
| Total erythrocyte omega 6 (%) | 27.1 ± 0.3 | 26.7 ± 0.3 | 0.07 | 27.2 ± 0.3 | 27.0 ± 0.3 | 1.00 | 0.50 | −0.3 (−1.2, 0.5) | 0.44 |
| Omega-6:omega-3 from erythrocytes | 2.7 ± 0.1 | 2.6 ± 0.1 | 0.05 | 2.8 ± 0.1 | 2.7 ± 0.1 | 0.15 | 0.12 | −0.1 (−0.4, 0.1) | 0.35 |
| Omega 3 index | 1.99 ± 0.3 | 2.0 ± 0.3 | 0.02 | 1.9 ± 0.3 | 2.0 ± 0.3 | 0.28 | 0.03 | 0.7 (−0.0, 0.2) | 0.13 |
| Sodium (mmol/24 h) | 113.9 ± 5.4 | 107.8 ± 4.9 | 0.85 | 118.3 ± 5.7 | 111.5 ± 5.1 | 0.73 | 0.30 | −5.5 (−20.4, 9.4) | 0.47 |
| Potassium (mmol/24 h) | 79.7 ± 2.7 | 80.7 ± 3.0 | 1.00 | 77.9 ± 2.9 | 74.9 ± 3.1 | 1.00 | 0.63 | 5.0 (−3.2, 13.2) | 0.24 |
| Calcium (mmol/24 h) | 3.6 ± 0.2 | 4.0 ± 0.2 | 0.16 | 4.1 ± 0.2 | 3.9 ± 0.2 | 0.99 | 0.13 | −0.0 (−0.7, 0.6) | 0.90 |
| Magnesium (mmol/24 h) | 4.4 ± 0.2 | 4.7 ± 0.2 | 0.17 | 4.3 ± 0.2 | 4.2 ± 0.2 | 1.00 | 0.12 | 0.6 (0.0, 1.1) | 0.04 |
© 2017 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Davis, C.; Hodgson, J.; Bryan, J.; Garg, M.; Woodman, R.; Murphy, K. Older Australians Can Achieve High Adherence to the Mediterranean Diet during a 6 Month Randomised Intervention; Results from the Medley Study. Nutrients 2017, 9, 534. https://doi.org/10.3390/nu9060534
Davis C, Hodgson J, Bryan J, Garg M, Woodman R, Murphy K. Older Australians Can Achieve High Adherence to the Mediterranean Diet during a 6 Month Randomised Intervention; Results from the Medley Study. Nutrients. 2017; 9(6):534. https://doi.org/10.3390/nu9060534
Chicago/Turabian StyleDavis, Courtney, Jonathan Hodgson, Janet Bryan, Manohar Garg, Richard Woodman, and Karen Murphy. 2017. "Older Australians Can Achieve High Adherence to the Mediterranean Diet during a 6 Month Randomised Intervention; Results from the Medley Study" Nutrients 9, no. 6: 534. https://doi.org/10.3390/nu9060534
APA StyleDavis, C., Hodgson, J., Bryan, J., Garg, M., Woodman, R., & Murphy, K. (2017). Older Australians Can Achieve High Adherence to the Mediterranean Diet during a 6 Month Randomised Intervention; Results from the Medley Study. Nutrients, 9(6), 534. https://doi.org/10.3390/nu9060534