Abstract
Background/Objectives: Gait analysis, traditionally performed with lab-based optical motion capture systems, offers high accuracy but is costly and impractical for real-world use. Wearable technologies, especially inertial measurement units (IMUs), enable portable and accessible assessments outside the lab, though challenges with sensor placement, signal selection, and algorithm design can affect accuracy. This systematic review aims to bridge the benchmarking gap between IMU-based and traditional systems, validating the use of wearable inertial systems for gait analysis. Methods: This review examined English studies between 2012 and 2023, retrieved from the Scopus database, comparing wearable sensors to optical motion capture systems, focusing on IMU body placement, gait parameters, and validation metrics. Exclusion criteria for the search included conference papers, reviews, unavailable papers, studies without wearable inertial sensors for gait analysis, and those not involving agreement studies or optical motion capture systems. Results: From an initial pool of 479 articles, 32 were selected for full-text screening. Among them, the lower body resulted in the most common site for single IMU placement (in 22 studies), while the most frequently used multi-sensor configuration involved IMU positioning on the lower back, shanks, feet, and thighs (10 studies). Regarding gait parameters, 11 studies out of the 32 included studies focused on spatial-temporal parameters, 12 on joint kinematics, 2 on gait events, and the remainder on a combination of parameters. In terms of validation metrics, 24 studies employed correlation coefficients as the primary measure, while 7 studies used a combination of error metrics, correlation coefficients, and Bland–Altman analysis. Validation metrics revealed that IMUs exhibited good to moderate agreement with optical motion capture systems for kinematic measures. In contrast, spatiotemporal parameters demonstrated greater variability, with agreement ranging from moderate to poor. Conclusions: This review highlighted the transformative potential of wearable IMUs in advancing gait analysis beyond the constraints of traditional laboratory-based systems.
1. Introduction
Human locomotion is a sophisticated process requiring complex interplay between multiple systems, including skeletal alignment, joint mobility, neuromuscular regulation, and the biomechanical forces that direct movement [,]. Pathological conditions such as congenital deformities, developmental issues, traumatic injuries, or degenerative disorders can affect these systems, leading to decreased walking efficiency and reduced mobility [,,,]. Therefore, the possible comprehensive gait assessment using gait analysis (GA), which systematically examines human movement, is crucial in several fields, including sports, clinical diagnoses, physical ergonomics, and rehabilitation [,,,,]. In sports, GA helps in determining better athletic performance, preventing injuries, as well as developing tailored training programs [,]. From a clinical point of view, GA allows identifying abnormalities, monitoring recovery, and evaluating fall risk, especially among the elderly [,]. At the same time, for rehabilitation purposes, it provides therapists with critical data to track patient progress, enabling them to modify treatment plans based on mobility improvements [,].
Human walking consists of a cyclical motion divided into distinct gait phases: the stance phase (60% of the cycle), where the foot remains on the ground, and the swing phase (40% of the cycle), where the foot moves forward []. These phases, including heel strike, toe-off, and various stages of swing, form a coordinated cycle of leg and foot movements (Figure 1). Thus, to provide deeper insights into human movement, quantitative GA focuses on measuring, describing, and evaluating several parameters, including kinematic, kinetic, and spatiotemporal (ST) metrics [].
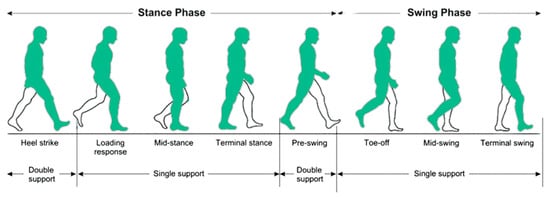
Figure 1.
Gait phases in a single gait cycle.
The origins of GA date back to the 19th century, with pioneers such as Étienne-Jules Marey and Eadweard Muybridge using sequential photography to study motion []. The 20th century marked a significant milestone in the integration of biomechanics with GA, highlighted by the introduction of force plates and multi-camera optical motion capture (OMC) systems [,,,]. These innovations enabled accurate measurements of forces and three-dimensional movement, establishing OMC systems as a practical gold standard in the GA field [,]. OMC systems offer high accuracy in motion capture, making them ideal for advanced biomechanical studies in various fields, from sports medicine and rehabilitation to scientific research [,]. In addition, OMC systems excel in controlled (with sufficient space and good lighting) and unobstructed environments, such as motion analysis labs, where precise tracking is essential []. However, conventional OMC systems are often more expensive and complex to install, resulting in lengthy set-up times, as well as space issues, requiring specialized structures, which may also hinder their ability to accurately reflect real-world walking scenarios [].
In recent years, the emergence of wearable technologies, including inertial measurement units (IMUs) which combine accelerometers, gyroscopes, and magnetometers, has revolutionized GA. These devices facilitate assessments outside traditional lab settings, providing more realistic evaluations of human movement and being very useful in the context of telemedicine for remote patient monitoring. Indeed, inertial systems are typically more portable and affordable than optical systems, enabling motion analysis in any environment—including outdoors or in confined spaces—without requiring cameras or specialized lighting. Therefore, advances in miniaturization and accessibility have fostered a shift in movement biomechanics, making wearable sensors a viable alternative to established OMC systems [,,]. The integration of these wearable inertial systems with advanced signal processing algorithms for gait events (GEs) detection holds significant promise for enhancing the extraction of kinematic parameters and transforming how movement is monitored [,,,,,]. The primary limitation of inertial systems is sensor drift, which causes error accumulation and progressively reduces tracking accuracy over time. Moreover, IMUs are highly sensitive to sensor placement, considering factors such as soft-tissue artefacts, muscle movement, and attachment to non-bony areas introducing significant noise and compromising data reliability. Furthermore, IMUs cannot directly measure kinetic variables (e.g., joint moments or power) and may be influenced by external magnetic or metallic interference, which can occasionally result in system failure. In contrast, OMC systems offer highly accurate and direct measurements of both kinematic and kinetic variables by tracking reflective markers in controlled environments. However, their substantial infrastructure requirements limit their feasibility in real-world settings. Additionally, IMUs are less accurate in capturing complex movements, as they may struggle to detect subtle changes or rotations as accurately as OMC systems.
Despite the growing adoption of wearable inertial sensors and specialized motion analysis algorithms, there is still a lack of systematic literature review studies validating their effectiveness. Possible inconsistencies in the adoption of different wearable inertial sensors may indeed lead to potential variability in gait parameter estimates, which may arise from differences in sensor placement and in the inertial signals used to calculate kinematic parameters [,,].
Therefore, in the wake of the increasing use of wearable inertial sensors in the field of GA, this systematic review aims to address, possibly filling, gaps of inconsistency in the literature, proposing a systematic analysis of the validity of wearable sensors, both prototype and commercial ones, comparing the benchmarking with OMC systems, which can be considered the gold standard also for clinical applications.
2. Research Strategy
A systematic review involves the rigorous selection, evaluation, and synthesis of studies on a defined subject []. This review adheres to the guidelines set by the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) [] (the checklist is included in the Supplementary Materials).
Search Methodology and Study Selection
The literature search was conducted by searching for documents in the Scopus database and was limited to English documents published between 2012 and 2023. The database was queried using the following keyword structure: ((“agreement”) or (“benchmarking”) or (“validity”)) and ((“optoelectronic system”) or (“stereophotogrammetry”)) and ((“wearable sensor”) or (“imu”) or (“inertial measurement unit”) or (“accelerometer”)) and ((“gait analysis”) or (“gait”)).
In order to simplify our research, the exclusion criteria were:
- manuscripts not published in English;
- conference reviews, reviews, and book chapters;
- papers not available.
For the screening process involving titles, abstracts, and full texts, the following exclusion criteria were established:
- papers assessing gait parameters without utilizing wearable inertial sensors;
- papers comparing wearable inertial sensors with OMC systems for tasks not related to gait analysis;
- papers that do not include agreement studies;
- papers using wearable inertial sensors for gait assessment that do not compare results with OMC systems.
Documents were screened by first assessing the content of the titles and abstracts. If any documents did meet the inclusion criteria at this stage, a full-text evaluation was conducted. Following the completion of the initial search of electronic database, one reviewer (G.P.) examined the titles and abstracts of the identified articles to determine their eligibility for inclusion in the review. Full-text evaluations of potentially relevant articles were conducted independently by two reviewers (G.P. and M.A.P.).
The PRISMA workflow is illustrated in Figure 2, which also indicates the number of documents included in this systematic review.
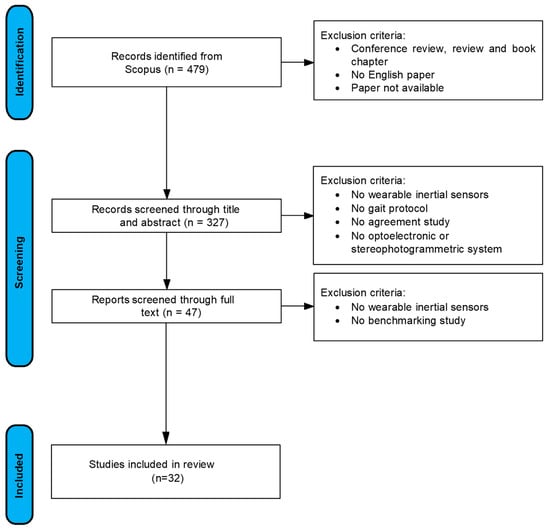
Figure 2.
Summary review workflow.
3. Main Findings and Argumentation
This systematic review encompasses 32 studies, published between 2014 and 2023. Publication activity reached its highest point in 2022, as depicted in Figure 3. This surge highlights the rising interest in applying IMUs for GA from both practical and scientific research perspectives. This demonstrates the growing role of IMUs in clinical practice, particularly in assessing gait parameters. Their portability and relatively low cost make them ideal for tracking rehabilitation progress or identifying motor impairments without relying on complex motion analysis labs.
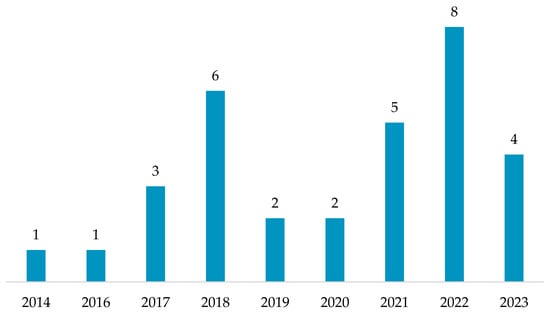
Figure 3.
Distribution of papers over time.
Data collection, organization of tabular information, and the creation of graphics and charts were conducted using Microsoft Excel 2021. The papers were examined across several key aspects: the aim of the study, the participants involved, and the tasks performed; the type of wearable inertial system used, including the number of the devices used and their placement on the body; the OMC system, including the number of cameras; the extracted kinematic and kinetic parameters; the statistical methodologies employed; and the results obtained for each study. Table 1 presents the studies, listed in chronological order by publication year.

Table 1.
Analysis of the studies included in this review.
4. Wearable Inertial Systems and Study Population
The development of wearable devices has rapidly advanced due to the introduction of novel sensors and technologies []. These innovations enable continuous monitoring of various physiological parameters, demonstrating versatility across a wide range of healthcare applications, including the management of chronic and degenerative diseases, as well as other medical conditions [,,,,,,]. The reviewed studies focused on wearable inertial systems and their placement on the human body to detect ST and kinematic gait parameters to establish a benchmark with gold-standard OMC systems.
Two categories of devices were considered: (1) prototypes, representing experimental configurations not commercially available, and (2) commercial devices, referring to those already widely available (Figure 4). Among the reviewed studies, 4 out of 32 papers utilized a prototype device. Pepa et al. [] investigated the accuracy of different spatial gait parameter estimation methods using the iPhone 4s accelerometer, positioned on the lumbar region, and compared the results with OMC data. Koska et al. [] assessed the accuracy of kinematic data related to human running obtained from brief sequences of shoe-mounted IMU sensors, comparing the results with those from an OMC system. Amitrano et al. [] evaluated a prototype system that combined e-textile sensor socks with ankle-mounted IMUs to assess both postural and ST gait parameters. Hellec et al. [] aimed to determine the concurrent validity of ST parameters captured by an IMU integrated into smart glasses, compared with an OMC system.
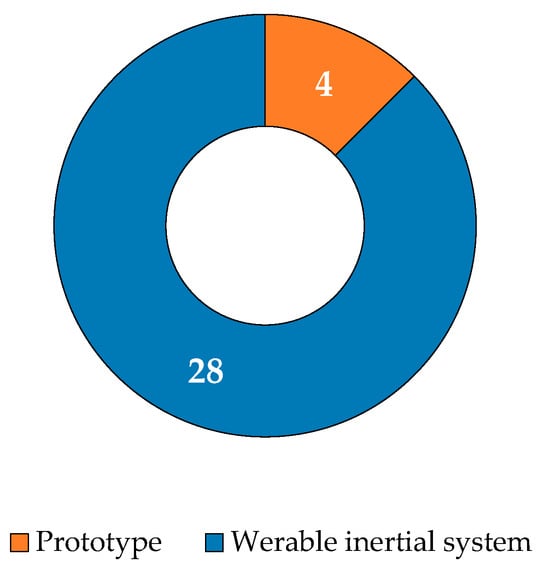
Figure 4.
Distribution of wearable sensors: prototypes and commercial wearable inertial systems.
Other studies utilized commercial inertial systems, enrolling both healthy subjects and patients suffering from specific impairments. Of these studies, 10 out of 32 works tested the wearable inertial systems during gait tasks on participants with specific impairments. The distribution of subject impairments considered across the studies is presented in Table 2. Cimolin et al. [] validated ST parameter estimates during level walking using a single IMU positioned on the lower trunk of both obese and normal-weight adolescents. Pham et al. [] assessed an algorithm for step detection in 11 participants with Parkinson’s disease (PD) during turning and non-turning episodes, utilizing an IMU placed on the lumbar region. Kleiner et al. [] compared total times from the timed up and go (TUG) test in 30 PD participants, measuring outcomes with a wearable tri-axial IMU against an OMC system. Zago et al. [] evaluated the validity of two systems for measuring ST gait parameters (BTS® G-Sensor vs. BTS SMART System) in 22 PD participants. Berner et al. [] investigated the validity of an IMU system in measuring lower limb kinematics and ST gait parameters with eight HIV-positive and eight HIV-negative participants. Simonetti et al. [] validated a wearable framework for estimating the center of mass (CoM) acceleration and velocity using one participant with transfemoral amputation. Romijnders et al. [] assessed GE detection using a shank-mounted IMU in 14 PD participants and 9 stroke (STR) participants. In a subsequent study, the same authors [] examined the effectiveness of a deep learning approach for detecting GEs from an IMU on the lower leg in 93 participants with various conditions. Ricciardi et al. [] evaluated the agreement between two systems for measuring ST gait parameters (Opal System vs. BTS SMART System) in 15 participants with progressive supranuclear palsy (PSP). Finally, Brasiliano et al. [] validated three IMU-based algorithms (shank and foot set-ups) in identifying GEs among children with idiopathic toe walking (ITW).
Table 2.
Distribution of subject impairments as reported in the studies included in this systematic review.
5. Sensor Placement
The placement of IMUs offers multiple options, and researchers explored different configurations in gait-related studies, applying sensors to various body segments or combinations of segments. This distribution is highlighted in Figure 5 (one study was excluded from the figure as the sensor was not placed directly on the body but was instead embedded in a pair of eyeglasses []). Among the studies analyzed, the lower back was the most frequently used site for lower-body IMU placement in GA (22 studies), followed closely by the feet and shanks (20 studies each). Additionally, 10 out of 32 studies used a single sensor, while the remaining studies employed multiple sensors. The most common multi-sensor set-up involved placing IMUs on the low back, shanks, feet, and thighs (used by ten studies). While these statistics provided insight into current research preferences, it should be noted that they did not necessarily indicate whether these segments delivered the most informative data or simplified the identification of key GEs. Some researchers sought to clarify these considerations further. For instance, Micó-Amigo et al. [] compared two IMU configurations (placed on the low back and feet) for estimating step time and validated their results against an OMC system. In both configurations, the anteroposterior (AP) acceleration signal was used to identify GEs and calculate step time. The study concluded that step time can be estimated with acceptable accuracy using either a single sensor on the low back or two sensors positioned on the heels, demonstrating flexibility in sensor placement without compromising accuracy. Additionally, Digo et al. [] conducted a comparative study evaluating three distinct IMU set-ups (ankle, shank, and trunk-mounted IMUs) against a gold-standard OMC system for assessing ST gait parameters in a healthy elderly population. The algorithms for the shank and ankle IMUs focused on identifying GEs from mediolateral (ML) angular velocity signals, while the trunk IMU algorithm analyzed AP acceleration signals. Despite all IMU configurations demonstrating good accuracy, the authors concluded that the trunk-IMU system outperformed both the ankle and shank set-ups in terms of precision in detecting GEs. Moreover, Brasiliano et al. [] evaluated the effectiveness of three IMU-based algorithms in detecting GEs in children with ITW. The study compared two setups: one where the IMUs were placed on the shanks and another where they were mounted on the feet. All algorithms were applied to the ML angular velocity signals. The authors concluded that the IMU-foot algorithm was the best for identifying heel strikes and estimating ST parameters, while the IMU-shank algorithm excelled at identifying GEs. Finally, Pepa et al. [] evaluated three algorithms for detecting GEs using a smartphone placed on the low back to assess the potential of smartphones in estimating gait parameters. All methods relied on AP acceleration signals, with results compared against the gold-standard OMC system. The sensor placement on the low back did not negatively impact the precision of ST parameter estimations. The results indicated a high accuracy in estimating GEs using the smartphone, confirming its suitability for gait monitoring. Unlike all the other items, only one involved the use of an IMU placed on the glasses []. The authors developed a methodology based on the vertical acceleration signal acquired by an IMU placed on the subject’s glasses for the detection of ST parameters. Good agreement was observed between the measures extracted by IMU embedded in the glasses and the ones obtained from the OMC system. However, a challenge was the variability in IMU positioning. Each time the IMU was attached, its location or orientation within the same body segment could differ, leading to inconsistent datasets and results across subjects. This intra-segment placement variability could be mitigated by employing a fixed mount or holder, ensuring consistent sensor positioning for more reliable measurements.
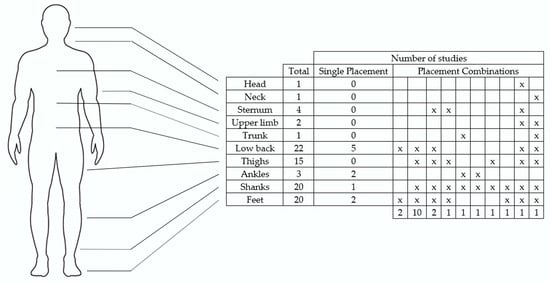
Figure 5.
The number of studies that positioned IMUs on specific anatomical locations. The “Single Placement” column represents studies where sensors were located at only one anatomical site. The “Placement Combinations” columns represent studies where sensors were positioned at multiple anatomical locations. Each relevant location is marked with an “x”, and the number of studies utilizing that specific combination is noted at the bottom of each column. The “Total” reflects the cumulative number of studies that placed sensors at the respective anatomical location.
Another factor contributing to variability in results was the choice of signal (acceleration or angular velocity). Gyroscopes, which measure angular velocity, are unaffected by positional translation because the angular velocity of a rigid body remains consistent across any point on the body, assuming the sensor’s orientation relative to the body segment remains stable. Additionally, gyroscopes are not influenced by gravity and are less prone to noise. In contrast, accelerometers tend to be noisier, sensitive to both position and orientation, and susceptible to gravitational effects. Consequently, despite numerous studies, disagreements persist regarding the optimal sensor positioning, orientation, and signal type.
6. Gait Task
Most of the studies (22 out of 32) involved a gait task where participants walked at either a self-selected pace or at three different speeds over a predetermined distance. Five additional studies required participants to walk on a treadmill. Two studies, conducted by Kleiner et al. [] and El Fezazi et al. [], used the TUG test. The TUG test measures the time taken for an individual to rise from a seated position, walk three meters, turn around, walk back, and sit down. This test is commonly used to assess mobility issues, particularly in individuals with PD, stroke, or other conditions affecting balance and gait []. Jordan et al. [] chose the acceleration–deceleration ability (ADA) test, which consists of a 20 m sprint, followed by rapid linear deceleration after crossing the 20 m line, and then backpedaling to the same line. Romijnders et al. [] asked participants to complete three distinct tasks: walking at a self-selected speed over a 5 m path, a slalom task (covering 5 m with a cone placed every meter, at a preferred speed), and a Stroop-and-walk trial (walking back and forth along the 5 m path while performing a numerical Stroop test on a handheld mobile device, at a self-selected pace, until the Stroop test was completed) []. Finally, Bartoszek et al. [] enrolled a single participant who performed a 12 m walk at their preferred speed for the Nordic walking gait style.
7. Gait Parameters
Gait parameters are essential metrics that characterize human locomotion, offering valuable insights into mobility, efficiency, and injury risk. These parameters are typically classified into three categories: ST, kinematic, and kinetic. ST parameters focus on timing and distances, relying on critical GEs such as heel strike, toe-off, and mid-swing. Kinematic parameters capture the movement of joints and limbs without accounting for forces, while kinetic parameters assess the forces and moments exerted on the body during movement. Notably, no kinetic parameters were reported in the reviewed works. Table 3 presents a detailed breakdown of the parameters measured across the selected studies, while Figure 6 reports the distribution of gait parameters. Joint kinematic angles were recorded 117 times, ST parameters 91 times, center-of-mass parameters 3 times, and gait events 9 times, totaling 233 parameters across 32 studies. Hip flexion was the most frequently measured parameter (ten occurrences), followed by knee flexion (nine occurrences). Hip abduction, hip rotation, ankle flexion, stride length, and speed were each recorded eight times. This is related to the different set-ups (number and positions of sensors that were used).
Table 3.
Gait parameters computed in the studies included in this systematic review. The parameters are categorized based on their type, with the total number of parameters measured per category indicated in parentheses. The “Articles” column provides the reference for each measurement, while the “Total” column displays the overall count for each individual parameter.
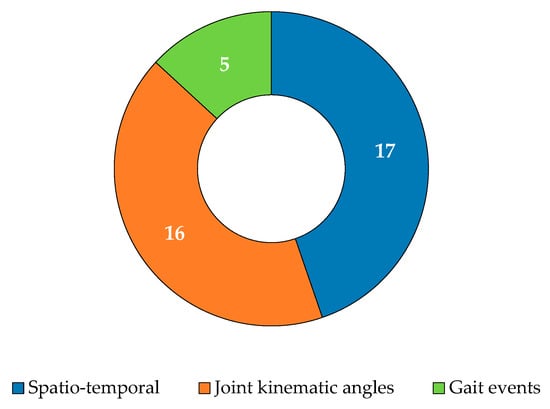
Figure 6.
Distribution of gait parameters: spatiotemporal, joint kinematic angles, and gait events.
Of the 32 studies reviewed, 17 focused on calculating ST parameters, while 2 concentrated only on extracting GEs such as heel strike and toe-off, as shown in Figure 6. Pham et al. [] developed an algorithm that uses an AP acceleration signal from a single IMU placed on the lumbar region to detect GEs. Romijnders et al. [] designed an algorithm based on angular velocity signals along the ML axis, using two IMUs mounted on the shanks. Both studies were validated by comparing their results with those from two commercial OMC systems, with Pham et al. [] achieving 90% accuracy and Romijnders et al. [] achieving 100% accuracy in detecting GEs during non-rotational phases of step detection.
Twelve articles focused exclusively on kinematic parameter estimation, while four studies focused on kinematic parameters coupled with ST parameters. Only one study, Bartoszek et al. [], investigated the validation of joint kinematic measures for both the lower and upper limbs during the Nordic walking gait. The study found a consistent systematic error across all joint kinematic measurements. Finally, Simonetti et al. [] focused on two CoM parameters related to gait—CoM velocity and acceleration—to validate a wearable framework in a person with a transfemoral amputation. Strong agreement was obtained by the authors when comparing a network of five IMUs with a gold-standard OMC system.
8. Validation Metrics
The present systematic review identified several benchmarking validation metrics, which can be grouped into five categories: correlation coefficients (CC), Bland–Altman (BA) analyses, error metrics (ER), statistical tests (ST), and Passing–Bablok (PB) linear regression.
As reported in Figure 7, in the CC category, the most frequently reported metrics across 24 papers included the Pearson correlation coefficient (PCC), Lin’s concordance correlation (LCC), coefficient of determination (R2), Spearman’s rank correlation coefficient (ρ), intraclass correlation coefficient (ICC), and the coefficient of multiple correlation (CMC). The BA approach was the second most widely used, appearing in 20 studies. The ER category was identified in 18 papers and included measures such as mean difference (MD), typical error of estimate (TEE), root mean square deviation (RMSD), root mean square error (RMSE), mean absolute error (MAE), absolute error (ε), absolute percentage error (ε%), absolute difference in range of motion (ΔROM), standardized typical error (SEE), range of motion error (ROME), and non-parametric effect size (ES). The ST category, used in 13 papers, included the paired t-Test, Wilcoxon test, ANOVA, and likelihood ratio (LR) test. Finally, the PB linear regression method was reported in four studies.
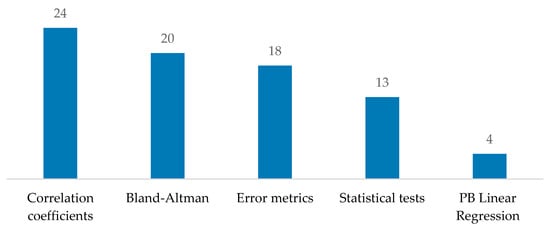
Figure 7.
Employed statistical tool distributions.
Overall, CC was the most frequently used metric, followed by BA, ER, ST, and PB linear regression (Figure 7).
While these validation metrics offer insights into current research preferences, individually, they fall short of providing a comprehensive picture of agreement levels. Therefore, combining multiple metrics is essential to achieve more robust and reliable results. Some researchers have explored this approach further to enhance interpretability in validation. For example, Amitrano et al. [] evaluated the validity of gait parameters measured by the SWEET Sock, a novel wearable device designed for remote health monitoring, using four validation metrics: the paired test (either t-Test or Wilcoxon test), PCC, PB linear regression, and BA analysis. The authors found strong agreement for temporal parameters, such as gait cycle time and cadence, but limited agreement for spatial parameters, especially step length. Similarly, El Fezazi et al. [] developed and validated a method for estimating knee kinematics during the TUG test using IMU devices, comparing it to an optical system through metrics including the paired test, RMSE, PCC, and BA. They concluded that no significant differences were found in the kinematic parameters compared to the reference system, indicating strong agreement between the two methodologies. Ricciardi et al. [] assessed the agreement between two systems for measuring spatial-temporal gait parameters in patients with PSP by comparing the Opal System and BTS SMART System using the paired test, PB, and BA analyses. They found that while the systems showed general agreement, they were not fully interchangeable due to two types of error: a constant systematic error affecting cadence and gait cycle time, and a proportional error affecting stance phase, swing phase, and stride length. Digo et al. [] compared three different IMU set-ups—placed on the trunk, shank, and ankle—with an OMC system to evaluate ST parameters in a healthy elderly population. Using metrics such as the PCC, RMSE, and BA analysis, they concluded that all IMU configurations demonstrated good performance in assessing gait. However, the trunk-mounted IMU system showed superior accuracy compared to the shank- and ankle-mounted configurations.
Overall, the combination of validation metrics most frequently used is ER, CC, and BA with seven papers [,,,,,,].
9. Conclusions
This systematic review highlights the transformative potential of wearable IMUs in advancing gait analysis beyond the constraints of traditional laboratory-based systems. This review synthesized findings from studies up to 2023, evaluating the validity of wearable sensors by assessing their benchmarking with gold-standard OMC systems.
The analysis of IMU configurations in the reviewed studies revealed that lower-body placement on the lower back, feet, and shanks is the most common setup, with these sites appearing collectively in over two-thirds of studies. Single-sensor configurations on the lower back proved effective for estimating ST parameters (such as step time and cadence), while multi-sensor setups on the lower back, shanks, feet, and thighs demonstrated superior accuracy for a broader range of gait metrics. Overall, kinematic parameters demonstrated consistently reliable levels of agreement, independently of sensor placement, the number of sensors used, or the validation metrics applied. Among ST parameters, metrics such as cadence, stride time, and stride cycle time demonstrated stronger agreement compared to those describing specific stride cycle phases, such as swing, stance, and double support. Despite high levels of agreement between IMU- and OMC-derived data, several limitations remain in the benchmarking evaluation of the aforementioned systems, especially in confirming the validity of wearable inertial sensors, which would promote their diffusion in clinical practice in the near future.
In conclusion, this review confirmed the promising role of wearable IMUs as viable alternatives to the gold-standard systems (OMCs), particularly in settings where portability and ease of use are paramount. IMUs demonstrated strong agreement with OMC systems in estimating gait parameters. Specifically, kinematic parameters showed good to moderate agreement, while ST parameters exhibited varied results: good agreement for parameters such as cadence and gait cycle time but moderate to poor agreement for parameters associated with gait cycle phases. Therefore, as IMU technology continues to evolve, standardization in positioning, refined signal processing algorithms, and improved validation protocols will be essential to fully realize the potential of IMU-based GA.
Our systematic review identified a key limitation in the heterogeneity of the included studies, particularly in sensor configurations, data processing methods, and validation metrics. This variability hindered direct comparisons and resulted in inconsistent findings. To address these challenges, future research could incorporate meta-analytic approaches to quantitatively synthesize agreement metrics, offering clearer insights into IMU performance trends.
Supplementary Materials
The following supporting information can be downloaded at: https://www.mdpi.com/article/10.3390/diagnostics15010036/s1, PRISMA 2020 Main Checklist. Reference [] is cited in the Supplementary Materials.
Author Contributions
Conceptualization, G.P. and L.D.; methodology, G.P., M.A.P. and L.D.; software, G.P. and L.D.; validation, G.P., M.A.P. and L.D.; formal analysis, G.P. and L.D.; investigation, G.P. and L.D.; resources, L.D.; data curation, G.P., M.A.P. and L.D.; writing—original draft preparation, G.P., M.A.P. and L.D.; writing—review and editing, A.S., F.E., M.C., F.A. and L.D.; visualization, G.P., M.A.P. and L.D.; supervision, L.D.; project administration, L.D.; funding acquisition, L.D. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Not applicable.
Acknowledgments
Work by G.P. was supported by the Intesa Sanpaolo Onlus Foundation under the initiative “Doctorates in the Humanities—38th Cycle”. Work by M.A.P, F.E. and L.D. was supported by #NEXTGENERATIONEU (NGEU) and funded by the Ministry of University and Research (MUR), National Recovery and Resilience Plan (NRRP), project MNESYS (PE0000006)—a multiscale integrated approach to the study of the nervous system in health and disease (DN. 1553 11.10.2022).
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Miller, F. Gait. In Cerebral Palsy, 1st ed.; Springer: New York, NY, USA, 2005; Volume 16, pp. 251–386. [Google Scholar]
- Ghoussayni, S.; Stevens, C. Assessment and validation of a simple automated method for the detection of gait events and intervals. Gait Posture 2004, 20, 266–272. [Google Scholar] [CrossRef] [PubMed]
- Viswanathan, A.; Sudarsky, L. Balance and gait problems in the elderly. Handb. Clin. Neurol. 2012, 103, 623–634. [Google Scholar]
- Baker, J.M. Gait disorders. Am. J. Med. 2018, 131, 602–607. [Google Scholar] [CrossRef] [PubMed]
- Axer, H.; Axer, M. Falls and gait disorders in geriatric neurology. Clin. Neurol. Neurosurg. 2010, 112, 265–274. [Google Scholar] [CrossRef] [PubMed]
- Salzman, B. Gait and balance disorders in older adults. Am. Fam. Physician 2010, 82, 61–68. [Google Scholar] [PubMed]
- Houmanfar, R.; Karg, M. Movement analysis of rehabilitation exercises: Distance metrics for measuring patient progress. IEEE Syst. J. 2014, 10, 1014–1025. [Google Scholar] [CrossRef]
- Bartlett, R. Movement patterns—the essence of sports biomechanics. In Introduction to Sports Biomechanics: Analysing Human Movement Patterns, 3rd ed.; Routledge: London, UK, 2021; pp. 1–57. [Google Scholar]
- Winter, D.A. Biomechanics as an Interdiscipline. In Biomechanics and Motor Control of Human Movement, 4th ed.; John Wiley & Sons: Hoboken, NJ, USA, 2009; pp. 1–14. [Google Scholar]
- Donisi, L.; Cesarelli, G. A logistic regression model for biomechanical risk classification in lifting tasks. Diagnostics 2022, 12, 2624. [Google Scholar] [CrossRef]
- Prisco, G.; Donisi, L.; Jacob, D. Binary Risk vs No-Risk Classification of Load Lifting Activities Using Features Extracted from sEMG Trapezius Muscle. In Proceedings of the International Conference on E-Health and Bioengineering, Iasi, Romania, 9–10 November 2023. [Google Scholar]
- Wahab, Y.; Bakar, N.A. Gait analysis measurement for sport application based on ultrasonic system. In Proceedings of the 2011 IEEE 15th International Symposium on Consumer Electronics (ISCE), Singapore, 11–17 June 2011. [Google Scholar]
- Watanabe, K.; Hokari, M. Kinematical analysis and measurement of sports form. IEEE Trans. Syst. Man Cybern. Part A Syst. Hum. 2006, 36, 549–557. [Google Scholar] [CrossRef]
- Di Biase, L.; Di Santo, A. Gait analysis in Parkinson’s disease: An overview of the most accurate markers for diagnosis and symptoms monitoring. Sensors 2020, 20, 3529. [Google Scholar] [CrossRef]
- Picillo, M.; Ricciardi, C. Gait analysis in progressive supranuclear palsy phenotypes. Front. Neurol. 2021, 12, 674495. [Google Scholar] [CrossRef]
- Steultjens, M.P.M.; Dekker, J.V. Range of joint motion and disability in patients with osteoarthritis of the knee or hip. Rheumatology 2000, 39, 955–961. [Google Scholar] [CrossRef] [PubMed]
- Baker, R. Gait analysis methods in rehabilitation. J. Neuroeng. Rehabil. 2006, 3, 4. [Google Scholar] [CrossRef]
- Kharb, A.; Saini, V. A review of gait cycle and its parameters. IJCEM Int. J. Comput. Eng. Manag. 2011, 13, 2230–7893. [Google Scholar]
- Whittle, M.W. Clinical gait analysis: A review. Hum. Mov. Sci. 1996, 15, 369–387. [Google Scholar] [CrossRef]
- Baker, R. The history of gait analysis before the advent of modern computers. Gait Posture 2007, 26, 331–342. [Google Scholar] [CrossRef]
- Furnee, E.H. Real-time motion capture systems. In Three-Dimensional Analysis of Human Locomotion; Allard, A.C.P., Lundberg, A., Vaughan, C.L., Eds.; John Wiley & Sons: West Sussex, UK, 1997; pp. 85–108. [Google Scholar]
- Gavrila, D.M.; Davis, L.S. 3-D model-based tracking of humans in action: A multi-view approach. In Proceedings of the IEEE Computer Vision and Pattern Recognition, San Francisco, CA, USA, 18–20 June 1996. [Google Scholar]
- Cappozzo, A.; Della Croce, U. Human movement analysis using stereophotogrammetry: Part 1: Theoretical background. Gait Posture 2005, 21, 186–196. [Google Scholar] [PubMed]
- Wang, Y.; Mukaino, M. Gait characteristics of post-stroke hemiparetic patients with different walking speeds. Int. J. Rehabil. Res. 2020, 43, 69–75. [Google Scholar] [CrossRef] [PubMed]
- Muro-De-La-Herran, A.; Garcia-Zapirain, B. Gait analysis methods: An overview of wearable and non-wearable systems, highlighting clinical applications. Sensors 2014, 14, 3362–3394. [Google Scholar] [CrossRef]
- Harris, G.F.; Wertsch, J.J. Procedures for gait analysis. Arch. Phys. Med. Rehabil. 1994, 75, 216–225. [Google Scholar] [CrossRef] [PubMed]
- Cloete, T.; Scheffer, C. Benchmarking of a full-body inertial motion capture system for clinical gait analysis. In Proceedings of the 2008 30th Annual International Conference of the IEEE Engineering in Medicine and Biology Society, Vancouver, BC, Canada, 20–24 August 2008. [Google Scholar]
- Mihradi, S.; Dirgantara, T.; Mahyuddin, A.I. Development of an optical motion-capture system for 3D gait analysis. In Proceedings of the 2011 2nd International Conference on Instrumentation, Communications, Information Technology, and Biomedical Engineering, Bandung, Indonesia, 8–9 November 2011. [Google Scholar]
- Yu, P.; Cen, X. Differences in intra-foot movement strategies during locomotive tasks among chronic ankle instability, copers and healthy individuals. J. Biomech. 2024, 162, 111865. [Google Scholar] [CrossRef] [PubMed]
- Akhtaruzzaman, M.D.; Shafie, A.A. Gait analysis: Systems, technologies, and importance. J. Mech. Med. Biol. 2016, 16, 1630003. [Google Scholar] [CrossRef]
- Mayagoitia, R.E.; Nene, A.V. Accelerometer and rate gyroscope measurement of kinematics: An inexpensive alternative to optical motion analysis systems. J. Biomech. 2002, 35, 537–542. [Google Scholar] [CrossRef] [PubMed]
- Hanlon, M.; Anderson, R. Real-time gait event detection using wearable sensors. Gait Posture 2006, 24, S127–S128. [Google Scholar] [CrossRef]
- Mansfield, A.; Lyons, G.M. The use of accelerometry to detect heel contact events for use as a sensor in FES assisted walking. Med. Eng. Phys. 2003, 25, 879–885. [Google Scholar] [CrossRef]
- Pappas, I.P.I.; Popovic, M.R. A reliable gait phase detection system. IEEE Trans. Neural Syst. Rehabil. Eng. 2001, 9, 113–125. [Google Scholar] [CrossRef]
- Li, Q.; Young, M. Walking speed estimation using a shank-mounted inertial measurement unit. J. Biomech. 2010, 43, 1640–1643. [Google Scholar] [CrossRef]
- Lau, H.; Tong, K. The reliability of using accelerometer and gyroscope for gait event identification on persons with dropped foot. Gait Posture 2008, 27, 248–257. [Google Scholar] [CrossRef] [PubMed]
- González, R.C.; López, A.M. Real-time gait event detection for normal subjects from lower trunk accelerations. Gait Posture 2010, 31, 322–325. [Google Scholar] [CrossRef]
- Bugané, F.; Benedetti, M.G. Estimation of spatial-temporal gait parameters in level walking based on a single accelerometer: Validation on normal subjects by standard gait analysis. Comput. Methods Programs Biomed. 2012, 108, 129–137. [Google Scholar] [CrossRef] [PubMed]
- Zijlstra, W.; Hof, A.L. Assessment of spatio-temporal gait parameters from trunk accelerations during human walking. Gait Posture 2003, 18, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Panebianco, G.P.; Bisi, M.C. Analysis of the performance of 17 algorithms from a systematic review: Influence of sensor position, analyzed variable and computational approach in gait timing estimation from IMU measurements. Gait Posture 2018, 66, 76–82. [Google Scholar] [CrossRef] [PubMed]
- Celik, Y.; Stuart, S. Wearable inertial gait algorithms: Impact of wear location and environment in healthy and Parkinson’s populations. Sensors 2021, 21, 6476. [Google Scholar] [CrossRef] [PubMed]
- Renggli, D.; Graf, C. Wearable inertial measurement units for assessing gait in real-world environments. Front. Physiol. 2020, 11, 90. [Google Scholar] [CrossRef]
- Higgins, J.P.; Green, S. Cochrane Handbook for Systematic Reviews of Interventions, 1st ed.; The Cochrane Collaboration: London, UK, 2011; pp. 1–78. [Google Scholar]
- Liberati, A.; Altman, D.G. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: Explanation and elaboration. Ann. Intern. Med. 2009, 151, W-65. [Google Scholar] [CrossRef] [PubMed]
- Buganè, F.; Benedetti, M.G. Estimation of pelvis kinematics in level walking based on a single inertial sensor positioned close to the sacrum: Validation on healthy subjects with stereophotogrammetric system. Biomed. Eng. Online 2014, 13, 146. [Google Scholar] [CrossRef]
- Micó-Amigo, M.E.; Kingma, I. A novel accelerometry-based algorithm for the detection of step durations over short episodes of gait in healthy elderly. J. Neuroeng. Rehabil. 2016, 13, 38. [Google Scholar] [CrossRef]
- Pepa, L.; Verdini, F. Gait parameter and event estimation using smartphones. Gait Posture 2017, 57, 217–223. [Google Scholar] [CrossRef] [PubMed]
- Cimolin, V.; Capodaglio, P. Computation of spatio-temporal parameters in level walking using a single inertial system in lean and obese adolescents. Biomed. Eng./Biomed. Tech. 2017, 62, 505–511. [Google Scholar] [CrossRef] [PubMed]
- Pham, M.H.; Elshehabi, M. Validation of a step detection algorithm during straight walking and turning in patients with Parkinson’s disease and older adults using an inertial measurement unit at the lower back. Front. Neurol. 2017, 8, 457. [Google Scholar] [CrossRef] [PubMed]
- Koska, D.; Gaudel, J.; Hein, T. Validation of an inertial measurement unit for the quantification of rearfoot kinematics during running. Gait Posture 2018, 64, 135–140. [Google Scholar] [CrossRef] [PubMed]
- Kleiner, A.F.R.; Pacifici, I. Timed Up and Go evaluation with wearable devices: Validation in Parkinson’s disease. J. Bodyw. Mov. Ther. 2018, 22, 390–395. [Google Scholar] [CrossRef] [PubMed]
- Al-Amri, M.; Nicholas, K. Inertial measurement units for clinical movement analysis: Reliability and concurrent validity. Sensors 2018, 18, 719. [Google Scholar] [CrossRef] [PubMed]
- Zago, M.; Sforza, C. Gait evaluation using inertial measurement units in subjects with Parkinson’s disease. J. Electromyogr. Kinesiol. 2018, 42, 44–48. [Google Scholar] [CrossRef]
- Teufl, W.; Lorenz, M. Towards inertial sensor based mobile gait analysis: Event-detection and spatio-temporal parameters. Sensors 2018, 19, 38. [Google Scholar] [CrossRef] [PubMed]
- Teufl, W.; Miezal, M. Validity, test-retest reliability and long-term stability of magnetometer free inertial sensor based 3D joint kinematics. Sensors 2018, 18, 1980. [Google Scholar] [CrossRef]
- Fleron, M.K.; Ubbesen, N.C.H. Accuracy between optical and inertial motion capture systems for assessing trunk speed during preferred gait and transition periods. Sports Biomech. 2019, 18, 366–377. [Google Scholar] [CrossRef] [PubMed]
- Adamowicz, L.; Gurchiek, R.D. Validation of novel relative orientation and inertial sensor-to-segment alignment algorithms for estimating 3D hip joint angles. Sensors 2019, 19, 5143. [Google Scholar] [CrossRef] [PubMed]
- Amitrano, F.; Coccia, A. Design and validation of an e-textile-based wearable sock for remote gait and postural assessment. Sensors 2020, 20, 6691. [Google Scholar] [CrossRef]
- Berner, K.; Cockcroft, J. Kinematics and temporospatial parameters during gait from inertial motion capture in adults with and without HIV: A validity and reliability study. BioMed. Eng. OnLine 2020, 19, 57. [Google Scholar] [CrossRef] [PubMed]
- Jordan, A.; Carson, H.J. Validity of an inertial measurement unit system to assess lower-limb kinematics during a maximal linear deceleration. Cent. Eur. J. Sport Sci. Med. 2021, 33, 5–16. [Google Scholar] [CrossRef]
- Ziagkas, E.; Loukovitis, A. A novel tool for gait analysis: Validation study of the smart insole podosmart®. Sensors 2021, 21, 5972. [Google Scholar] [CrossRef]
- Saggio, G.; Tombolini, F. Technology-based complex motor tasks assessment: A 6-DOF inertial-based system versus a gold-standard optoelectronic-based one. IEEE Sens. J. 2021, 21, 1616–1624. [Google Scholar] [CrossRef]
- Simonetti, E.; Bergamini, E. Estimation of 3D body center of mass acceleration and instantaneous velocity from a wearable inertial sensor network in transfemoral amputee gait: A case study. Sensors 2021, 21, 3129. [Google Scholar] [CrossRef]
- Romijnders, R.; Warmerdam, E. Validation of IMU-based gait event detection during curved walking and turning in older adults and Parkinson’s Disease patients. J. Neuroeng. Rehabil. 2021, 18, 28. [Google Scholar] [CrossRef] [PubMed]
- Piche, E.; Guilbot, M. Validity and repeatability of a new inertial measurement unit system for gait analysis on kinematic parameters: Comparison with an optoelectronic system. Measurement 2022, 198, 111442. [Google Scholar] [CrossRef]
- Rekant, J.; Rothenberger, S. Inertial measurement unit-based motion capture to replace camera-based systems for assessing gait in healthy young adults: Proceed with caution. Meas. Sens. 2022, 23, 100396. [Google Scholar] [CrossRef] [PubMed]
- Bartoszek, A.; Struzik, A. Comparison of the optoelectronic BTS Smart system and IMU-based MyoMotion system for the assessment of gait variables. Acta Bioeng. Biomech. 2022, 24. [Google Scholar] [CrossRef]
- Choo, C.Z.Y.; Chow, J.Y. Validation of the Perception Neuron system for full-body motion capture. PLoS ONE 2022, 17, e0262730. [Google Scholar] [CrossRef] [PubMed]
- Digo, E.; Panero, E. Comparison of IMU set-ups for the estimation of gait spatio-temporal parameters in an elderly population. Proc. Inst. Mech. Eng. Part H J. Eng. Med. 2022, 237, 61–73. [Google Scholar] [CrossRef]
- Carcreff, L.; Payen, G. Three-dimensional lower-limb kinematics from accelerometers and gyroscopes with simple and minimal functional calibration tasks: Validation on asymptomatic participants. Sensors 2022, 22, 5657. [Google Scholar] [CrossRef] [PubMed]
- Hellec, J.; Chorin, F. Smart eyeglasses: A valid and reliable device to assess spatiotemporal parameters during gait. Sensors 2022, 22, 1196. [Google Scholar] [CrossRef]
- Romijnders, R.; Warmerdam, E. A deep learning approach for gait event detection from a single Shank-Worn IMU: Validation in healthy and neurological cohorts. Sensors 2022, 22, 3859. [Google Scholar] [CrossRef] [PubMed]
- Ricciardi, C.; Pisani, N. Agreement between Optoelectronic System and Wearable Sensors for the Evaluation of Gait Spatiotemporal Parameters in Progressive Supranuclear Palsy. Sensors 2023, 23, 9859. [Google Scholar] [CrossRef] [PubMed]
- El Fezazi, M.; Achmamad, A. A convenient approach for knee kinematics assessment using wearable inertial sensors during home-based rehabilitation: Validation with an optoelectronic system. Sci. Afr. 2023, 20, e01676. [Google Scholar] [CrossRef]
- Brasiliano, P.; Mascia, G. Impact of Gait Events Identification through Wearable Inertial Sensors on Clinical Gait Analysis of Children with Idiopathic Toe Walking. Micromachines 2023, 14, 277. [Google Scholar] [CrossRef]
- Pacher, L.; Vignais, N. The contribution of multibody optimization when using inertial measurement units to compute lower-body kinematics. Med. Eng. Phys. 2023, 111, 103927. [Google Scholar] [CrossRef]
- Motti, V.G.; Caine, K. Human factors considerations in the design of wearable devices. In Proceedings of the Human Factors and Ergonomics Society Annual Meeting, Los Angeles, CA, USA, 1 September 2014. [Google Scholar]
- Donisi, L.; Jacob, D. sEMG Spectral Analysis and Machine Learning Algorithms Are Able to Discriminate Biomechanical Risk Classes Associated with Manual Material Liftings. Bioengineering 2023, 10, 1103. [Google Scholar] [CrossRef] [PubMed]
- Prisco, G.; Romano, M. Capability of Machine Learning Algorithms to Classify Safe and Unsafe Postures during Weight Lifting Tasks Using Inertial Sensors. Diagnostics 2024, 14, 576. [Google Scholar] [CrossRef]
- D’Addio, G.; Donisi, L.; Pagano, G. Agreement between opal and G-walk wearable inertial systems in gait analysis on normal and pathological subjects. In Proceedings of the 2019 41st Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC), Berlin, Germany, 23–27 July 2019. [Google Scholar]
- Donisi, L.; Pagano, G. Benchmarking between two wearable inertial systems for gait analysis based on a different sensor placement using several statistical approaches. Measurement 2021, 173, 108642. [Google Scholar] [CrossRef]
- Russo, M.; Amboni, M. Kinematic and Kinetic Gait Features Associated with Mild Cognitive Impairment in Parkinson’s Disease. IEEE Trans. Neural Syst. Rehabil. Eng. 2024, 32, 2676–2687. [Google Scholar] [CrossRef]
- Franco, A.; Russo, M. The Role of Deep Learning and Gait Analysis in Parkinson’s Disease: A Systematic Review. Sensors 2024, 24, 5957. [Google Scholar] [CrossRef]
- Prisco, G.; Romano, M.; Esposito, F. Feasibility of Tree-Based Machine Learning Models to Discriminate Safe and Unsafe Posture During Weight Lifting. In Proceedings of the 2023 IEEE International Conference on Metrology for eXtended Reality, Artificial Intelligence and Neural Engineering (MetroXRAINE), Milan, Italy, 25–27 October 2023. [Google Scholar]
- Kear, B.M.; Guck, T.P. Timed up and go (TUG) test: Normative reference values for ages 20 to 59 years and relationships with physical and mental health risk factors. J. Prim. Care Community Health 2017, 8, 9–13. [Google Scholar] [CrossRef] [PubMed]
- Henik, A.; Tzelgov, J. Is three greater than five: The relation between physical and semantic size in comparison tasks. Mem. Cogn. 1982, 10, 389–395. [Google Scholar] [CrossRef] [PubMed]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. MetaArXiv 2020. [Google Scholar] [CrossRef]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).