Short- and Long-Term Outcomes of Patients with Postoperative Arrhythmia after Liver Surgery

 , ,
, ,
Abstract
1. Introduction
2. Materials and Methods
2.1. Patient Cohort
- Respiratory frequency: ≥22/min;
- Systolic blood pressure: <100 mmHg;
- CNS: reduced vigilance or altered mental status (GCS score);
2.2. Statistical Analysis
3. Results
3.1. Demographic Data
3.2. Incidence, Time Point, and Type of PA
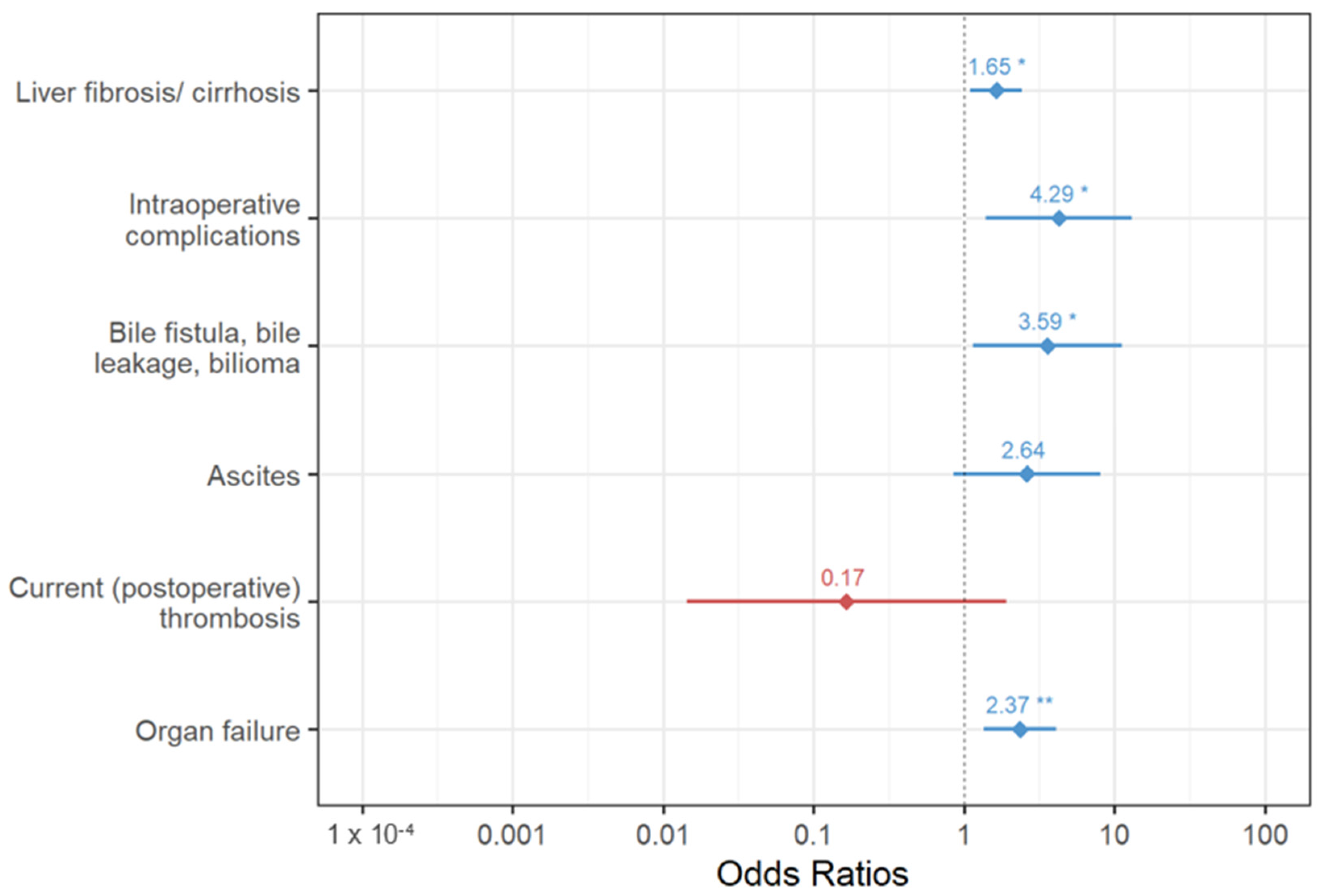
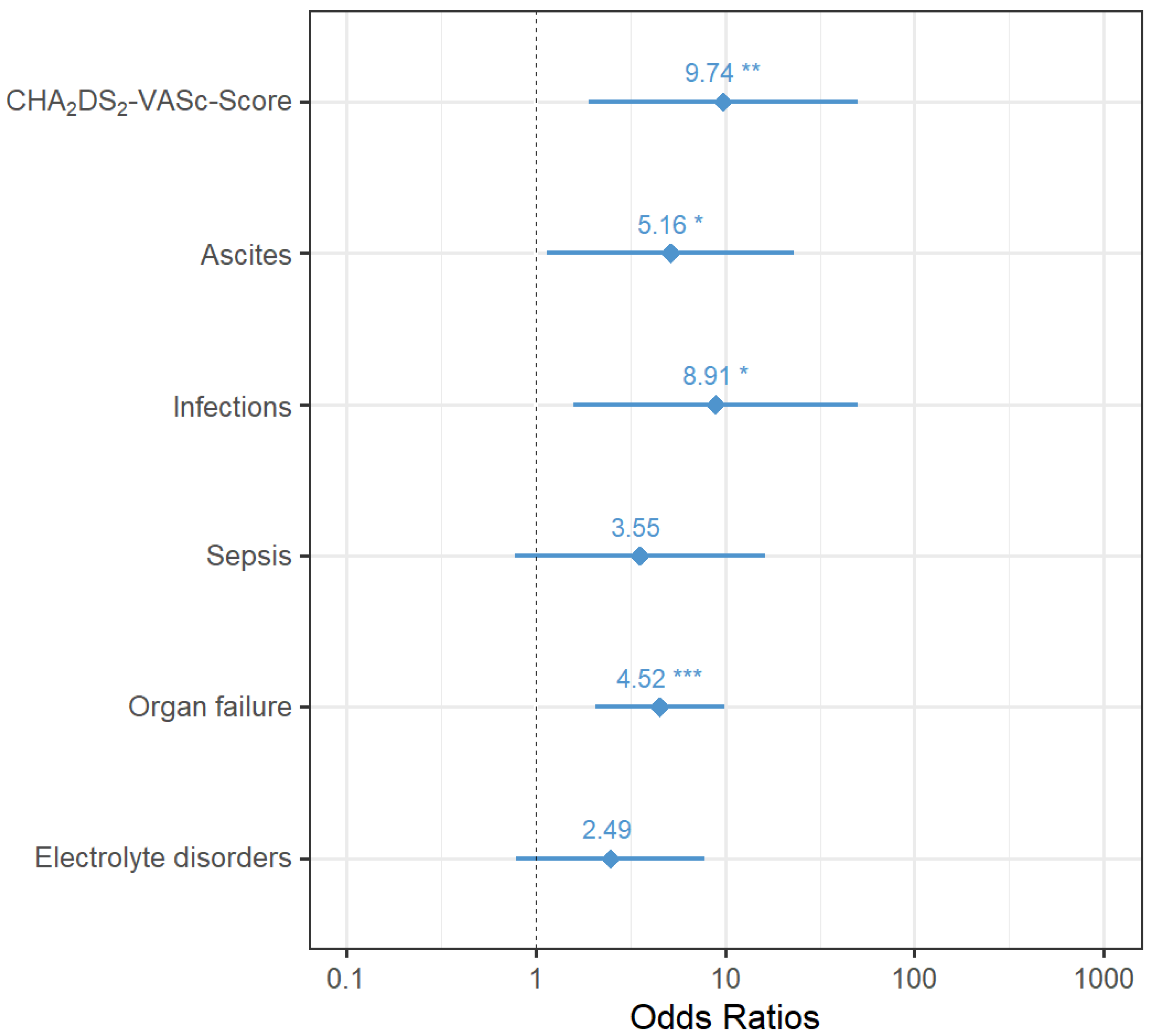
3.3. PA and Associated Factors
3.4. PA and In-House Mortality
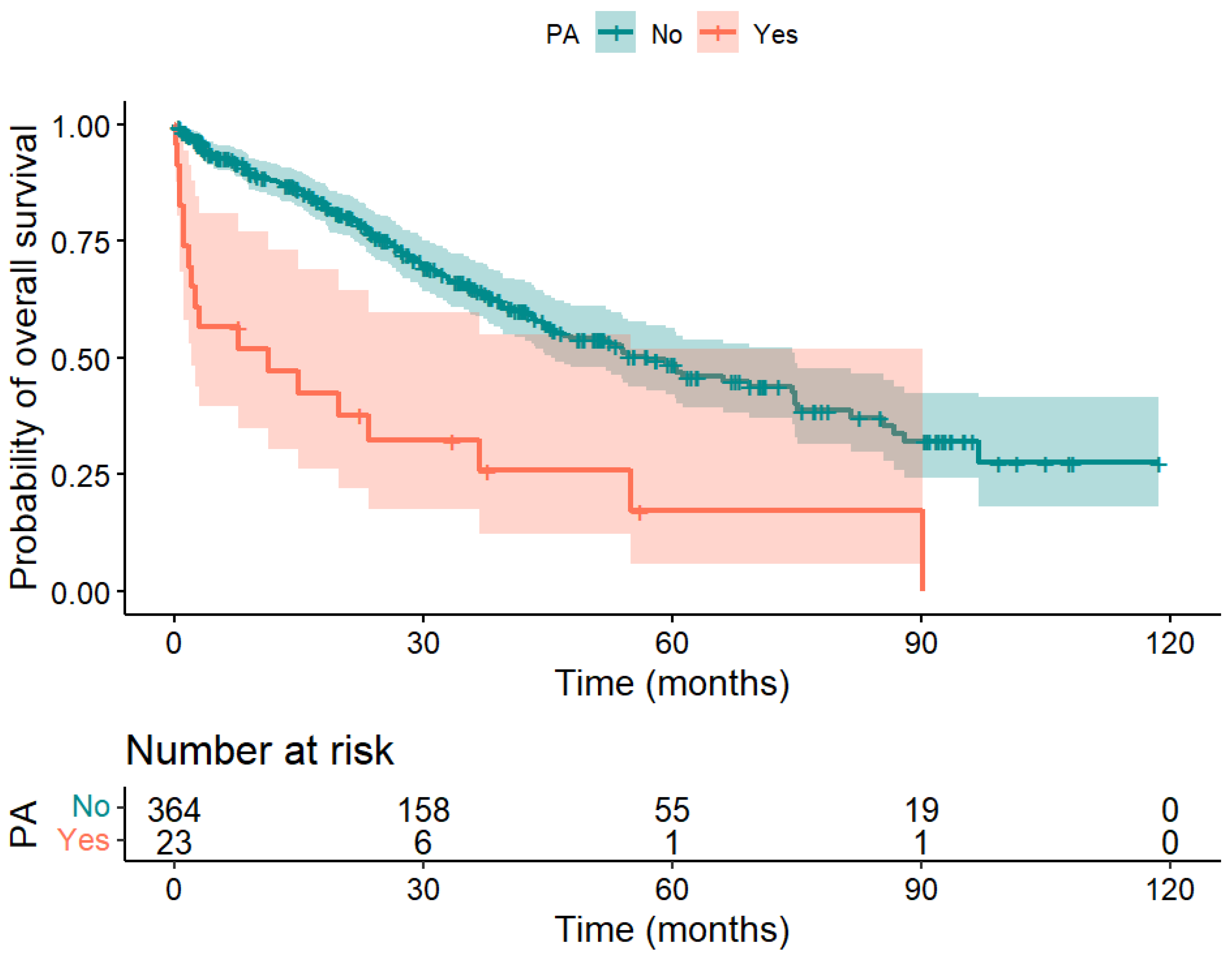
3.5. Long-Term Overall Survival (OS)
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Ruhlmann, F.; Tichelbacker, T.; Mackert, A.F.; Engelhardt, D.; Leha, A.; Bernhardt, M.; Ghadimi, M.; Perl, T.; Azizian, A.; Gaedcke, J. Incidence, Associated Risk Factors, and Outcomes of Postoperative Arrhythmia after Upper Gastrointestinal Surgery. JAMA Netw. Open 2022, 5, e2223225. [Google Scholar] [CrossRef]
- Ruhlmann, F.; Hedicke, M.S.; Engelhardt, D.; Mackert, A.F.; Tichelbacker, T.; Leha, A.; Bernhardt, M.; Ghadimi, M.; Perl, T.; Azizian, A.; et al. Incidence and impact of new-onset postoperative arrhythmia after surgery of the lower gastrointestinal tract. Sci. Rep. 2023, 13, 1284. [Google Scholar] [CrossRef]
- Chebbout, R.; Heywood, E.G.; Drake, T.M.; Wild, J.R.L.; Lee, J.; Wilson, M.; Lee, M.J. A systematic review of the incidence of and risk factors for postoperative atrial fibrillation following general surgery. Anaesthesia 2018, 73, 490–498. [Google Scholar] [CrossRef]
- Bender, J.S. Supraventricular tachyarrhythmias in the surgical intensive care unit: An under-recognized event. Am. Surg. 1996, 62, 73–75. [Google Scholar]
- Rao, V.P.; Addae-Boateng, E.; Barua, A.; Martin-Ucar, A.E.; Duffy, J.P. Age and neo-adjuvant chemotherapy increase the risk of atrial fibrillation following oesophagectomy. Eur. J. Cardiothorac. Surg. 2012, 42, 438–443. [Google Scholar] [CrossRef]
- Mc Cormack, O.; Zaborowski, A.; King, S.; Healy, L.; Daly, C.; O’Farrell, N.; Donohoe, C.L.; Ravi, N.; Reynolds, J.V. New-onset atrial fibrillation post-surgery for esophageal and junctional cancer: Incidence, management, and impact on short- and long-term outcomes. Ann. Surg. 2014, 260, 772–778; discussion 778. [Google Scholar] [CrossRef]
- Schizas, D.; Kosmopoulos, M.; Giannopoulos, S.; Giannopoulos, S.; Kokkinidis, D.G.; Karampetsou, N.; Papanastasiou, C.A.; Rouvelas, I.; Liakakos, T. Meta-analysis of risk factors and complications associated with atrial fibrillation after oesophagectomy. Br. J. Surg. 2019, 106, 534–547. [Google Scholar] [CrossRef] [PubMed]
- Koshy, A.N.; Enyati, A.; Weinberg, L.; Han, H.C.; Horrigan, M.; Gow, P.J.; Ko, J.; Thijs, V.; Testro, A.; Lim, H.S.; et al. Postoperative Atrial Fibrillation and Long-Term Risk of Stroke in Patients Undergoing Liver Transplantation. Stroke 2021, 52, 111–120. [Google Scholar] [CrossRef] [PubMed]
- Xia, V.W.; Worapot, A.; Huang, S.; Dhillon, A.; Gudzenko, V.; Backon, A.; Agopian, V.G.; Aksoy, O.; Vorobiof, G.; Busuttil, R.W.; et al. Postoperative atrial fibrillation in liver transplantation. Am. J. Transplant. 2015, 15, 687–694. [Google Scholar] [CrossRef] [PubMed]
- Rachwan, R.J.; Kutkut, I.; Hathaway, T.J.; Timsina, L.R.; Kubal, C.A.; Lacerda, M.A.; Ghabril, M.S.; Bourdillon, P.D.; Mangus, R.S. Postoperative Atrial Fibrillation and Flutter in Liver Transplantation: An Important Predictor of Early and Late Morbidity and Mortality. Liver Transpl. 2020, 26, 34–44. [Google Scholar] [CrossRef] [PubMed]
- Reddy, S.K.; Barbas, A.S.; Turley, R.S.; Steel, J.L.; Tsung, A.; Marsh, J.W.; Geller, D.A.; Clary, B.M. A standard definition of major hepatectomy: Resection of four or more liver segments. Hpb 2011, 13, 494–502. [Google Scholar] [CrossRef] [PubMed]
- Balzan, S.; Belghiti, J.; Farges, O.; Ogata, S.; Sauvanet, A.; Delefosse, D.; Durand, F. The “50-50 criteria” on postoperative day 5: An accurate predictor of liver failure and death after hepatectomy. Ann. Surg. 2005, 242, 824–828; discussion 828–829. [Google Scholar] [CrossRef] [PubMed]
- Ranieri, V.M.; Rubenfeld, G.D.; Thompson, B.T.; Ferguson, N.D.; Caldwell, E.; Fan, E.; Camporota, L.; Slutsky, A.S. Acute respiratory distress syndrome: The Berlin Definition. JAMA 2012, 307, 2526–2533. [Google Scholar] [CrossRef] [PubMed]
- Lamb, E.J.; Levey, A.S.; Stevens, P.E. The Kidney Disease Improving Global Outcomes (KDIGO) guideline update for chronic kidney disease: Evolution not revolution. Clin. Chem. 2013, 59, 462–465. [Google Scholar] [CrossRef] [PubMed]
- Singer, M.; Deutschman, C.S.; Seymour, C.W.; Shankar-Hari, M.; Annane, D.; Bauer, M.; Bellomo, R.; Bernard, G.R.; Chiche, J.D.; Coopersmith, C.M.; et al. The Third International Consensus Definitions for Sepsis and Septic Shock (Sepsis-3). JAMA 2016, 315, 801–810. [Google Scholar] [CrossRef] [PubMed]
- Bhave, P.D.; Goldman, L.E.; Vittinghoff, E.; Maselli, J.; Auerbach, A. Incidence, predictors, and outcomes associated with postoperative atrial fibrillation after major noncardiac surgery. Am. Heart J. 2012, 164, 918–924. [Google Scholar] [CrossRef] [PubMed]
- Chung, M.K.; Martin, D.O.; Sprecher, D.; Wazni, O.; Kanderian, A.; Carnes, C.A.; Bauer, J.A.; Tchou, P.J.; Niebauer, M.J.; Natale, A.; et al. C-reactive protein elevation in patients with atrial arrhythmias: Inflammatory mechanisms and persistence of atrial fibrillation. Circulation 2001, 104, 2886–2891. [Google Scholar] [CrossRef] [PubMed]
- Subramani, Y.; El Tohamy, O.; Jalali, D.; Nagappa, M.; Yang, H.; Fayad, A. Incidence, Risk Factors, and Outcomes of Perioperative Atrial Fibrillation following Noncardiothoracic Surgery: A Systematic Review and Meta-Regression Analysis of Observational Studies. Anesthesiol. Res. Pract. 2021, 2021, 5527199. [Google Scholar] [CrossRef]
- Aghaulor, B.; VanWagner, L.B. Cardiac and Pulmonary Vascular Risk Stratification in Liver Transplantation. Clin. Liver Dis. 2021, 25, 157–177. [Google Scholar] [CrossRef]
- Patel, S.S.; Lin, F.P.; Rodriguez, V.A.; Bhati, C.; John, B.V.; Pence, T.; Siddiqui, M.B.; Sima, A.P.; Abbate, A.; Reichman, T.; et al. The relationship between coronary artery disease and cardiovascular events early after liver transplantation. Liver Int. 2019, 39, 1363–1371. [Google Scholar] [CrossRef]
- Dangl, M.; Grant, J.K.; Vincent, L.; Ebner, B.; Maning, J.; Olorunfemi, O.; Zablah, G.; Sancassani, R.; Colombo, R. The association of pre-transplant atrial fibrillation with in-hospital outcomes in patients undergoing orthotopic liver transplantation: A propensity score matching analysis. J. Card. Surg. 2022, 37, 4762–4773. [Google Scholar] [CrossRef] [PubMed]
- Chokesuwattanaskul, R.; Thongprayoon, C.; Bathini, T.; Ungprasert, P.; Sharma, K.; Wijarnpreecha, K.; Pachariyanon, P.; Cheungpasitporn, W. Liver transplantation and atrial fibrillation: A meta-analysis. World J. Hepatol. 2018, 10, 761–771. [Google Scholar] [CrossRef] [PubMed]
- Rivas, E.; Sasaki, K.; Liang, C.; Wang, J.; Quintini, C.; Maheshwari, K.; Turan, A.; Fares, M.; Cywinski, J.B. New-Onset Atrial Fibrillation in Patients Undergoing Liver Transplantation: Retrospective Analysis of Risk Factors and Outcomes. J. Cardiothorac. Vasc. Anesth. 2022, 36, 4100–4107. [Google Scholar] [CrossRef] [PubMed]
- Brems, J.J.; Takiff, H.; McHutchison, J.; Collins, D.; Biermann, L.A.; Pockros, P. Systemic versus nonsystemic reperfusion of the transplanted liver. Transplantation 1993, 55, 527–529. [Google Scholar] [CrossRef]
- Raval, Z.; Harinstein, M.E.; Skaro, A.I.; Erdogan, A.; DeWolf, A.M.; Shah, S.J.; Fix, O.K.; Kay, N.; Abecassis, M.I.; Gheorghiade, M.; et al. Cardiovascular risk assessment of the liver transplant candidate. J. Am. Coll. Cardiol. 2011, 58, 223–231. [Google Scholar] [CrossRef]
- Shi, X.Y.; Xu, Z.D.; Xu, H.T.; Jiang, J.J.; Liu, G. Cardiac arrest after graft reperfusion during liver transplantation. Hepatobiliary Pancreat. Dis. Int. 2006, 5, 185–189. [Google Scholar]

{kind=link}
{kind=link}
{kind=link}
| Parameter | Level | All Patients n (%) | Patients without PA n (%) | Patients with PA n (%) | p |
|---|---|---|---|---|---|
| n | 460 (100) | 435 (94.6) | 25 (5.4) | ||
| Sex | Male Female | 239 (52.0) 221 (48.0) | 225 (94.1) 210 (95.0) | 14 (5.9) 11 (5.0) | 0.838 |
| Age | Mean ± sd | 60.9 ± 13.6 | 60.7 ± 13.8 | 65.3 ± 9.9 | 0.033 |
| Median (min; max) | 63.6 (19.2; 87.1) | 63.6 (19.2; 87.1) | 64.0 (35.9; 80.9) | ||
| Surgery | n.s. | ||||
| (Extended) right hemihepatectomy | 163 (35.4) | 152 (93.3) | 11 (6.7) | ||
| (Extended) left hemihepatectomy | 64 (13.9) | 62 (96.9) | 2 (3.1) | ||
| Segmentectomy | 43 (9.3) | 42 (97.7) | 1 (2.3) | ||
| Right trisegmentectomy | 41 (8.9) | 38 (92.7) | 3 (7.3) | ||
| Multivisceral resection | 41 (8.9) | 39 (95.1) | 2 (4.9) | ||
| Cytoreductive surgery with HIPEC | 5 (1.1) | 4 (80.0) | 1 (20.0) | ||
| Bisegmentectomy (e.g., left lateral and right posterior sectionectomy) | 47 (10.2) | 45 (95.7) | 2 (4.3) | ||
| Resection of other segment combinations | 31 (6.7) | 29 (93.5) | 2 (6.5) | ||
| Atypical liver resections, wedge resections | 12 (2.6) | 12 (100.0) | 0 (0.0) | ||
| ALLPS | 11 (2.4) | 11 (100.0) | 0 (0.0) | ||
| Left trisegmentectomy | 2 (0.4) | 1 (50.0) | 1 (50.0) | ||
| Major resection | No Yes | 193 (42.0) 267 (58.0) | 185 (95.9) 250 (93.6) | 8 (4.1) 17 (6.4) | 0.407 |
| Diagnosis | Benign disease | 73 (16.0) | 71 (97.3) | 2 (2.7) | 0.400 |
| Malignant disease | 387 (84.0) | 364 (94.1) | 23 (5.9) | ||
| 200 (43.5) | 196 (98.0) | 4 (2.0) | ||
| 29 (6.3) | 29 (100.0) | 0 (0.0) | ||
| 5 (1.1) | 5 (100.0) | 0 (0.0) | ||
| 53 (11.5) | 47 (88.7) | 6 (11.3) | ||
| 46 (10.0) | 41 (89.1) | 5 (10.9) | ||
| 26 (5.7) | 22 (84.6) | 4 (15.4) | ||
| 4 (1.0) | 3 (75.0) | 1 (25.0) | ||
| 24 (5.2) | 21 (87.5) | 3 (12.5) | ||
| Dyslipidemia | No Yes | 408 (88.7) 52 (11.3) | 386 (94.6) 49 (94.2) | 22 (5.4) 3 (5.8) | 0.754 |
| Hypertension | No Yes | 223 (48.5) 237 (51.5) | 214 (96.0) 221 (93.2) | 9 (4.0) 16 (6.8) | 0.281 |
| Diabetes mellitus | No Yes (Type I/II) | 382 (83.0) 78 (17.0) | 364 (95.3) 71 (91.0) | 18 (4.7) 7 (9.0) | 0.165 |
| Venous thrombosis | No Yes (current) Yes (in past) | 405 (88.0) 23 (5.0) 32 (7.0) | 384 (94.8) 19 (82.6) 32 (100.0) | 21 (5.2) 4 (17.4) 0 (0.0) | 0.030 |
| Embolic event | No Yes (apoplex/ transient ischemic attack in past) | 441 (95.9) 19 (4.1) | 417 (94.6) 18 (94.7) | 24 (5.4) 1 (5.3) | 0.662 |
| Preexisting cardiac illness | No Yes | 397 (86.3) 63 (13.7) | 377 (95.0) 58 (92.1) | 20 (5.0) 5 (7.9) | 0.37 |
| Multiple (≥2) cardiovascular diseases | No Yes | 304 (66.1) 156 (33.9) | 293 (96.4) 142 (91.0) | 11 (3.6) 14 (9.0) | 0.029 |
| Kidney diseases | No Yes | 420 (91.3) 40 (8.7) | 398 (94.8) 37 (92.5) | 22 (5.2) 3 (7.5) | 0.469 |
| Intraoperative complications | No Yes | 363 (78.9) 97 (21.1) | 349 (96.1) 86 (88.7) | 14 (3.9) 11 (11.3) | 0.009 |
| Anastomosis insufficiency | No Yes | 447 (97.2) 13 (2.8) | 422 (94.4) 13 (100.0) | 25 (5.6) 0 (0.0) | 1 |
| Wound healing deficit | No Yes | 391 (85.0) 69 (15.0) | 373 (95.4) 62 (89.9) | 18 (4.6) 7 (10.1) | 0.079 |
| Bile fistula, bile leakage, bilioma | No Yes | 369 (80.2) 91 (19.8) | 354 (95.9) 81 (89.0) | 15 (4.1) 10 (11.0) | 0.017 |
| Liver parenchyma | Normal | 163 (35.4) | 158 (96.9) | 5 (3.1) | 0.004 |
| Steatosis | 145 (31.5) | 141 (97.2) | 4 (2.8) | ||
| Fibrosis | 43 (9.3) | 38 (88.4) | 5 (11.6) | ||
| Cirrhosis | 26 (5.7) | 21 (80.8) | 5 (19.2) | ||
| Not classified | 83 (18.0) | 77 (92.8) | 6 (7.2) | ||
| Ascites (500 > mL/24 h drainage after the third postoperative day) | No Yes | 355 (77.2) 105 (22.8) | 344 (96.9) 91 (86.7) | 11 (3.1) 14 (13.3) | <0.001 |
| Pleural effusion | No Yes | 361 (78.5) 99 (21.5) | 350 (97.0) 85 (85.9) | 11 (3.0) 14 (14.1) | <0.001 |
| Revision surgery | No Yes | 415 (90.2) 45 (9.8) | 398 (95.9) 37 (82.2) | 17 (4.1) 8 (17.8) | 0.002 |
| Organic failure | No Yes | 317 (68.9) 143 (31.1) | 309 (97.5) 126 (88.1) | 8 (2.5) 17 (11.9) | <0.001 |
| Electrolyte disorders | No Yes | 254 (55.2) 206 (44.8) | 248 (97.6) 187 (90.8) | 6 (2.4) 19 (9.2) | <0.001 |
| Postoperative delirium | No Yes | 411 (89.4) 49 (10.6) | 391 (95.1) 44 (89.8) | 20 (4.9) 5 (10.2) | 0.170 |
| Infections | No Yes | 337 (73.3) 123 (26.7) | 324 (96.1) 111 (90.2) | 13 (3.9) 12 (9.8) | 0.025 |
| Sepsis | No Yes | 433 (94.1) 27 (5.9) | 417 (96.3) 18 (66.7) | 16 (3.7) 9 (33.3) | <0.001 |
| CHA2DS2-VASc-Score ≥4 | No Yes | 376 (81.7) 84 (18.3) | 358 (95.2) 77 (91.7) | 18 (4.8) 7 (8.3) | 0.190 |
| Betablocker preoperatively | No Yes | 325 (70.7) 135 (29.3) | 311 (95.7) 124 (91.9) | 14 (4.3) 11 (8.1) | 0.160 |
| Diagnosis Groups | PA Incidence | p | |
|---|---|---|---|
| Median Difference (in %) | 95% CI (in %) | ||
| Patients with primary liver cancer vs. patients with liver metastases | −9.9 (11.6 vs. 1.7) | −3.2–(−16.7) | <0.001 *** |
| Patients with primary liver cancer vs. patients with benign lesions | −8.9 (11.6 vs. 2.7) | −0.1–(−17.7) | 0.04 * |
| Patients with liver-infiltrating malignant tumors vs. patients with benign lesions | −11.3 (14.0 vs. 2.7) | −0.7–(−21.8) | 0.03 * |
| Patients with liver-infiltrating malignant tumors vs. patients with liver metastases | −12.3 (14.0 vs. 1.7) | −3.4–(−21.2) | 0.002 ** |
| Parameter | Level | All Patients n (%) | Patients Who Did Not Die during Their Stay n (%) | Patients Who Died during Their Stay n (%) | p |
|---|---|---|---|---|---|
| n | 460 (100) | 440 (95.7) | 20 (4.3) | ||
| Sex | Male Female | 239 (52.0) 221 (48.0) | 227 (95.0) 213 (96.0) | 12 (5.0) 8 (4.0) | 0.503 |
| Age | Mean ± sd | 60.9 ± 13.6 | 60.7 ± 13.7 | 66.8 ± 10.1 | 0.015 |
| Median (min; max) | 63.6 (19.2; 87.1) | 63.5 (52.4; 70.6) | 67.8 (59.1; 73.4) | ||
| Surgery | |||||
| (Extended) right hemihepatectomy | 163 (35.4) | 152 (93.3) | 11 (6.7) | ||
| (Extended) left hemihepatectomy | 64 (13.9) | 61 (95.3) | 3 (4.7) | ||
| Segmentectomy | 43 (9.3) | 43 (100.0) | 0 (0.0) | ||
| Right trisegmentectomy | 41 (8.9) | 40 (97.6) | 1 (2.4) | ||
| Multivisceral resection | 41 (8.9) | 38 (92.7) | 3 (7.3) | ||
| Cytoreductive surgery with HIPEC | 5 (1.1) | 5 (100.0) | 0 (0.0) | ||
| Bisegmentectomy (e.g., left lateral and right posterior sectionectomy) | 47 (10.2) | 47 (100.0) | 0 (0.0) | ||
| Resection of other segment combinations | 31 (6.7) | 31 (100.0) | 0 (0.0) | ||
| Atypical liver resections, wedge resections | 12 (2.6) | 12 (100.0) | 0 (0.0) | ||
| In situ split with subsequent trisegmentectomy or (extended) hemi-hepatectomy on the right | 11 (2.4) | 10 (90.9) | 1 (9.1) | ||
| Left trisegmentectomy | 2 (0.4) | 1 (50.0) | 1 (50.0) | ||
| Major resection | No Yes | 193 (42.0) 267 (58.0) | 190 (98.4) 250 (93.6) | 3 (1.6) 17 (6.4) | 0.018 |
| Diagnosis | Benign disease | 73 (16.0) | 71 (97.3) | 2 (2.7) | 0.754 |
| Malignant disease | 387 (84.0) | 364 (95.3) | 18 (4.7) | ||
| 200 (43.5) | 199 (99.5) | 1 (0.5) | ||
| 29 (6.3) | 28 (96.6) | 1 (3.4) | ||
| 5 (1.1) | 5 (100.0) | 0 (0.0) | ||
| 53 (11.5) | 51 (96.2) | 2 (3.8) | ||
| 46 (10.0) | 43 (93.5) | 3 (6.5) | ||
| 26 (5.7) | 20 (76.9) | 6 (23.1) | ||
| 4 (1.0) | 4 (100.0) | 0 (0.0) | ||
| 24 (5.2) | 19 (79.2) | 5 (20.8) | ||
| Dyslipidemia | No Yes | 408 (88.7) 52 (11.3) | 389 (95.3) 51 (98.1) | 19 (4.7) 1 (1.9) | 0.714 |
| Hypertension | No Yes | 223 (48.5) 237 (51.5) | 216 (96.9) 224 (94.5) | 7 (3.1) 13 (5.5) | 0.315 |
| Diabetes mellitus | No Yes (type I/II) | 382 (83.0) 78 (17.0) | 367 (96.1) 73 (93.6) | 15 (3.9) 5 (6.4) | 0.357 |
| Venous thrombosis | No Yes (current) Yes (in past) | 405 (88.0) 23 (5.0) 32 (7.0) | 389 (96.0) 19 (82.6) 32 (100.0) | 16 (4.0) 4 (17.4) 0 (0.0) | 0.014 |
| Embolic event | No Yes (apoplex/ transient ischemic attack in past) | 441 (95.9) 19 (4.1) | 422 (95.7) 18 (94.7) | 19 (4.3) 1 (5.3) | 0.578 |
| Preexisting cardiac illness | No Yes | 397 (86.3) 63 (13.7) | 379 (95.5) 61 (96.8) | 18 (4.5) 2 (3.2) | 1 |
| Multiple (≥2) cardiovascular diseases | No Yes | 304 (66.1) 156 (33.9) | 295 (97.0) 145 (92.9) | 9 (3.0) 11 (7.1) | 0.073 |
| Kidney diseases | No Yes | 420 (91.3) 40 (8.7) | 402 (95.7) 38 (95.0) | 18 (4.3) 2 (5.0) | 0.689 |
| Intraoperative complications | No Yes | 363 (78.9) 97 (21.1) | 352 (97.0) 88 (90.7) | 11 (3.0) 9 (9.3) | 0.020 |
| Anastomosis insufficiency | No Yes | 447 (97.2) 13 (2.8) | 430 (96.2) 10 (76.9) | 17 (3.8) 3 (23.1) | 0.015 |
| Wound healing deficit | No Yes | 391 (85.0) 69 (15.0) | 376 (96.2) 64 (92.8) | 15 (3.8) 5 (7.2) | 0.202 |
| Bile fistula, bile leakage, bilioma | No Yes | 369 (80.2) 91 (19.8) | 359 (97.3) 81 (89.0) | 10 (2.7) 10 (11.0) | 0.002 |
| Liver parenchyma | Normal | 163 (35.4) | 156 (95.7) | 7 (4.3) | 0.167 |
| Steatosis | 145 (31.5) | 142 (97.9) | 3 (2.1) | ||
| Fibrosis | 43 (9.3) | 42 (97.7) | 1 (2.3) | ||
| Cirrhosis | 26 (5.7) | 24 (92.3) | 2 (7.7) | ||
| Not classified | 83 (18.0) | 80 (96.4) | 3 (3.6) | ||
| Ascites | No Yes | 355 (77.2) 105 (22.8) | 349 (98.3) 91 (86.7) | 6 (1.7) 14 (13.3) | <0.001 |
| Pleural effusion | No Yes | 361 (78.5) 99 (21.5) | 353 (97.8) 87 (87.9) | 8 (2.2) 12 (12.1) | <0.001 |
| Revision surgery | No Yes | 415 (90.2) 45 (9.8) | 404 (97.3) 36 (80.0) | 11 (2.7) 9 (20.0) | <0.001 |
| Organic failure | No Yes | 317 (68.9) 143 (31.1) | 314 (99.0) 126 (88.1) | 3 (1.0) 17 (11.9) | <0.001 |
| Electrolyte disorders | No Yes | 254 (55.2) 206 (44.8) | 253 (99.6) 187 (90.8) | 1 (0.4) 19 (9.2) | <0.001 |
| Postoperative delirium | No Yes | 411 (89.4) 49 (10.6) | 394 (95.9) 46 (93.9) | 17 (4.1) 3 (6.1) | 0.460 |
| Infections | No Yes | 337 (73.3) 123 (26.7) | 333 (98.8) 107 (87.0) | 4 (1.2) 16 (13.0) | <0.001 |
| Sepsis | No Yes | 433 (94.1) 27 (5.9) | 424 (97.9) 16 (59.3) | 9 (2.1) 11 (40.7) | <0.001 |
| CHA2DS2-VASc-Score ≥ 4 | No Yes | 376 (81.7) 84 (18.3) | 365 (97.1) 75 (89.3) | 11 (2.9) 9 (10.7) | 0.004 |
| New-onset PA | No Yes | 435 (94.6) 25 (5.4) | 422 (97.0) 18 (72.0) | 13 (3.0) 7 (28.0) | <0.001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rühlmann, F.; Engelhardt, D.; Mackert, A.F.; Hedicke, M.S.; Tichelbäcker, T.; Leha, A.; Bernhardt, M.; Ghadimi, M.; Perl, T.; Azizian, A.; et al. Short- and Long-Term Outcomes of Patients with Postoperative Arrhythmia after Liver Surgery. Biomedicines 2024, 12, 271. https://doi.org/10.3390/biomedicines12020271
Rühlmann F, Engelhardt D, Mackert AF, Hedicke MS, Tichelbäcker T, Leha A, Bernhardt M, Ghadimi M, Perl T, Azizian A, et al. Short- and Long-Term Outcomes of Patients with Postoperative Arrhythmia after Liver Surgery. Biomedicines. 2024; 12(2):271. https://doi.org/10.3390/biomedicines12020271
Chicago/Turabian StyleRühlmann, Felix, Deborah Engelhardt, Alma Franziska Mackert, Mara Sophie Hedicke, Tobias Tichelbäcker, Andreas Leha, Markus Bernhardt, Michael Ghadimi, Thorsten Perl, Azadeh Azizian, and et al. 2024. "Short- and Long-Term Outcomes of Patients with Postoperative Arrhythmia after Liver Surgery" Biomedicines 12, no. 2: 271. https://doi.org/10.3390/biomedicines12020271
APA StyleRühlmann, F., Engelhardt, D., Mackert, A. F., Hedicke, M. S., Tichelbäcker, T., Leha, A., Bernhardt, M., Ghadimi, M., Perl, T., Azizian, A., & Gaedcke, J. (2024). Short- and Long-Term Outcomes of Patients with Postoperative Arrhythmia after Liver Surgery. Biomedicines, 12(2), 271. https://doi.org/10.3390/biomedicines12020271