1. Introduction
Coffee is one of the most consumed beverages worldwide. Global coffee consumption is estimated to increase, particularly in non-traditional coffee drinking countries in Africa, Asia, and Oceania (+4.1%). Demand in traditional markets is estimated to grow by 1% in Europe and by 2.5% in North America [
1]. Leading drivers for coffee market growth are innovations in out-of-home consumption, online commerce opportunities, and innovative brewed coffee beverage types [
2]. Consumers are interested in coffee product quality and origin, as well as social, environmental, and economic sustainability [
3].
Innovative coffee attributes related to the health properties of coffee could be a driver for coffee consumption [
4]. Some researchers suggest that coffee might have the potential of a functional food thanks to its biochemical properties and the possible health benefits [
5,
6]. In particular, there is evidence that coffee consumption may have beneficial effects on non-communicable diseases (NCDs) [
7]. This may contribute to the World Health Organization’s objective of reducing the relative risk of premature mortality from NCDs by 25% by 2025, by improving the modifiable risk factor of an unhealthy diet [
8].
Consumers’ beliefs in the health benefits of coffee are unclear. Only 16% of U.S. consumers know about coffee’s health benefits, and 66% are prone to limiting their caffeine consumption [
9]. Many European consumers are also confused about coffee’s impact on health, with 49% believing coffee has negative health effects [
10]. On the other hand, consumption of green coffee-based beverages has become popular in recent years due to the belief in its beneficial antioxidant properties (e.g., chlorogenic acids, polyphenols) [
5,
11,
12].
Coffee contributes to the daily intake of dietary antioxidants, more than tea, fruit, and vegetables [
13]. A screening of the most consumed beverages for their bioactive non-nutrient contents identified instant coffee as the beverage with the highest total biophenol content [
14]. Two other studies observed coffee to be the beverage with the highest total antioxidant capacity as compared to others like green and black tea and herbal infusions [
15,
16]. The biochemical composition of a cup of coffee depends on the degree of roasting, the type of bean (Arabica versus Robusta), and the coffee brewing method, including grind type [
17,
18,
19]
There is little scientific knowledge on consumers’ attitude towards coffee health benefits. The perception of coffee’s health effects in consumers’ minds is unclear and has not been thoroughly researched. Past research studied consumer preferences and attitudes towards coffee attributes including sustainability, brands, coffee types, and motives for consumption like taste, energy, pleasure, socialization [
20]. The paper aims to fill this gap in the literature and analyze the link between consumers’ coffee consumption behavior and their perception of coffee’s health benefits and risks. The research adds value to existing literature by analyzing what consumers perceive about coffee’s health effects. If coffee has positive effects on human health it would be important to educate consumers about the possible health benefits and the correct consumption of coffee. Therefore, it is important to first study the status of consumers’ perceptions about coffee’s health effects. Furthermore, this will allow for an exploration into whether there are marketing possibilities for coffee with health benefits considering the increasing consumption trend of healthy food.
In evaluating the healthiness of a cup of coffee it is important to consider that coffee drinking is a complex consumption behavior and that preferences and preparation methods are influenced by culture and tradition. To fully exploit coffee’s capability to impact on consumer food dietary lifestyle and health, there is need to better understand consumers’ coffee consumption habits, motives, and perception of coffee’s health benefits. Therefore, the objective of the research is to analyze consumers’ perception of coffee’s health benefits, consumption and purchasing motives of coffee consumers with positive perception of coffee health benefits, and willingness to pay for coffee with associated health claims.
Data was collected through a direct face-to-face survey with consumers using questionnaires with closed-ended questions. The structure of the paper is as follows.
Section 2 provides a literature review of coffee consumption and purchasing motives and coffee and health, with a detailed review of the relevant literature on coffee’s effect on single health conditions.
Section 3 describes data gathering and elaboration, and the data sample. Results are presented in
Section 4. This section first discusses the results regarding consumers’ characteristics and perception of health effects of coffee, followed by insights on consumers’ perception of coffee health effects and motives for coffee consumption and purchasing, and concludes with analyzing consumers’ willingness to pay a price premium for coffee with associated health claims. Finally, the paper provides a discussion and conclusions on consumers’ perceptions of coffee’s health effects, profiling consumers according to their attitudes towards health coffee benefits.
Section 6 puts the topic into the broader context of consumers’ increasing interest in healthy food and eating behavior, and reflects on marketing possibilities for coffee focusing on specific health benefits.
4. Results
4.1. Consumers Characteristics and Perception of Health Effects of Coffee
A relevant minority of consumers (25%) thought that drinking coffee could have positive effects on health (
Table 4). The average value of the perception on coffee health benefits of the positively inclined consumers was fairly high (3.7). The analysis of consumers’ socio-economic characteristics, coffee consumption, and purchasing habits of the positively versus the negatively inclined consumers showed interesting elements (
Table 4). A higher percentage of men (31%), of younger (30.4%), and of working (27.2%) consumers had a positive perception of the health effects of coffee consumption compared to female, older, and not working consumers. The level of education was not an explanatory characteristic for the perception of health effect of coffee consumption. There were more consumers that tended to drink non-espresso based coffee (36.2%), that consumed from one to two cups of coffee per day (32.5%), that never or rarely drank coffee for breakfast (34.3%), and that bought coffee in big retailer chains (27.9%) that had a positive perception of coffee health benefits. A chi-squared
p-value confirmed the results. Other data support that positively inclined consumers tended to drink coffee with other people (28.5%), and that they did not to have coffee as a break (29.4%) or after lunch (28.1%).
These results suggest that consumers positively inclined towards coffee health benefits are more likely to be male, young, and working, tending to appreciate non espresso-based coffee, consume in limited amounts and in social settings, and not usually consuming in the morning. They are more likely to purchase it in common outlets, probably with other food items.
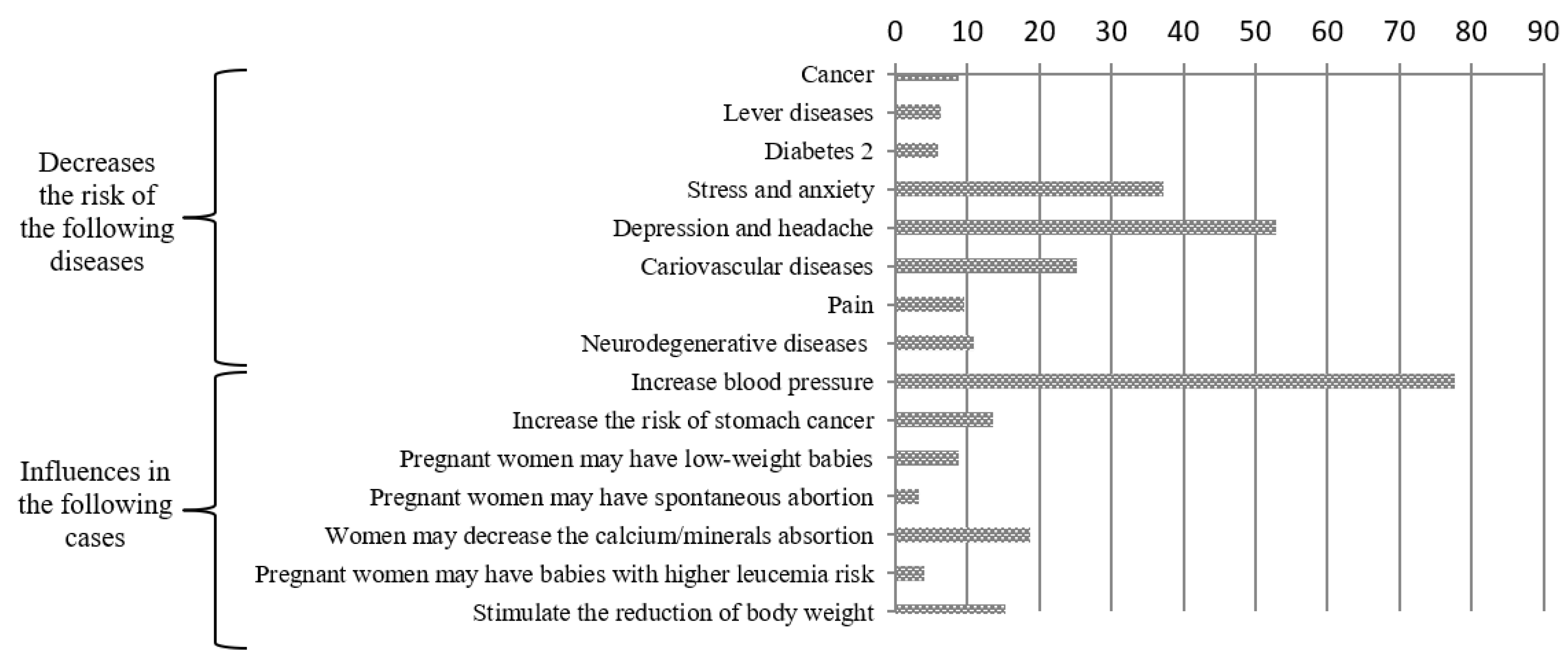
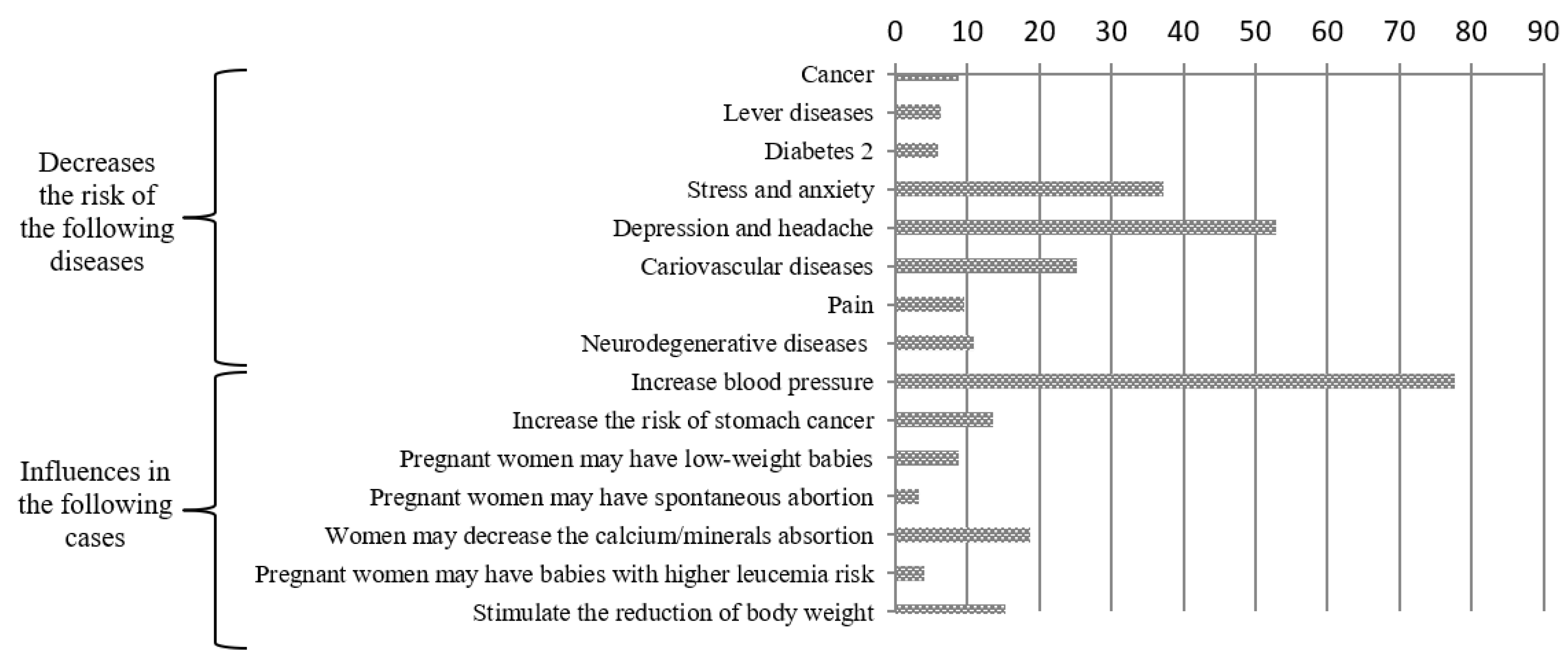
Consumers are better inclined towards a limited number of benefits of coffee consumption (
Figure 1). In particular, almost 80% of consumers believe that drinking coffee increases blood pressure, more than half think that it decreases depression and headache, one-third that it decreases the risk of stress and anxiety, one-fourth that it decreases the risk of cardiovascular diseases, and one-fifth that it impacts on women’s capability to absorb calcium and minerals and stimulates the reduction of body weight. Consumers do not acknowledge other medically tested effects on pregnant women, diabetes, liver, cancer, neurodegenerative diseases, and pain.
Moreover, 61% of consumers believe that the correct number of cups of coffee per day is between three and four. According to scientific studies, this is the recommended quantity (equivalent to 300–400 milligrams of caffeine per day) [
7,
26,
32]. Therefore, the vast majority has an adequate knowledge of the daily quantity of coffee to be consumed. Around 35% of consumers think that between one and two cups is adequate, values lower than the threshold set by scientists, thereby showing some skepticism towards coffee impact on health. Moreover, 84% of consumers think that the effect is similar in men and women, and 80% that decaffeinated coffee has a similar impact to caffeinated coffee on human health. These results support that consumers have adequate knowledge on the quantity to be consumed, the effects on gender, and the types of coffee, fairly in line with scientific evidence [
7,
26,
32]. There is no evident misconception of the effects of coffee on health.
4.2. Consumers’ Perception of Coffee Health Effect and Motives for Coffee Consumption and Purchasing
The two factor analyses on consumers’ coffee consumption and purchasing motives identified seven main components (
Table 5 and
Table 6). Four components derive from the factor analysis on the initial 12 items on coffee consumption motives, and three components derive from the factor analysis on the initial 13 items on purchasing motives. The second factor analysis was tested until all identified components had satisfactory internal consistency values. This lead to delete three items. In both factor analyses items were loaded into single factors, with factor loadings above 0.585. The Kaiser–Meyer–Olkin measure of sampling adequacy and Bartlett’s test of sphericity were calculated to assess the appropriateness of the data for factor analysis. The Kaiser–Meyer–Olkin index was 0.649 in the coffee consumption motives PCA and 0.660 in the coffee purchasing motives PCA. Bartlett’s tests of sphericity were highly significant (0.000). The cumulated variance values explained by the factors were respectively 66.2 and 66.3. Elaboration results confirmed the data appropriateness. The values of the factors were calculated based on the mean of the items loading into the single factors.
The internal consistency and convergent and discriminant validity of each component was verified (
Table 5 and
Table 6). The internal consistency of each set of items was measured using Cronbach’s alpha and composite reliability (CR). Alpha component values were from 0.633 to 0.771, and CR values were from 0.77 to 0.88 in the first factor analysis. In the second factor analysis, alpha component values were from 0.675 to 0.836 and CR values were from 0.81 to 0.94. Values were satisfactory and acceptable [
93,
94]. The average variance extracted (AVE) provides a measure of convergent validity, and ranged from 0.504 to 0.696 in the first factor analysis and from 0.510 and 0.776 in the second factor analysis. These were satisfactory as above the 0.50 threshold [
95]. To confirm discriminant validity, the square root of each construct’s AVE was calculated to ensure it was greater than its bivariate correlation with other constructs in the model. This led to adequate outcomes. The results confirm the reliability and validity of the research components.
The factors were labeled according to coffee consumption and purchasing motives associated with the statements. Coffee consumption is driven by four main factors. The most important factor is the habit and pleasure of drinking it (3.1). This connects to the organoleptic characteristics that are coffee smell and taste, family traditions and habits, and the emotions and moods created by coffee. The energetic physical and mental awakening power of coffee is as important as its role in having a break during the day and socializing at work (2.7). The fourth motive for drinking coffee is its therapeutic impact, that is, the capability of coffee to help digestion, increase blood pressure, and alleviate headaches (1.7). Coffee purchasing is driven by three main motives. The main driving element is the price, that is promotion and value for money (3.3). Another key aspect is the declared aroma, recipe, level of roasting, and intensity (3.2). The coffee sustainability (1.8) does not strongly influence consumers’ coffee purchasing. In synthesis, consumers have a hedonistic approach towards coffee, focused on its taste, smell, and family habits and culture. Their consumer behavior is also driven by utilitarian reasoning, focused on price. In addition, coffee is drunk for its relevant socializing and energetic power.
There is a statistically significant relationship between consumers’ perception of coffee health benefits and motives for coffee consumption and purchasing (
Table 7 and
Table 8). The VIF values were between 1.020 and 1.401, and the lowest tolerance value was 0.714. Therefore, there was no multicollinearity between variables. The significant relation is between the perception that coffee can have health benefits, and the following motives of coffee experience: habit and pleasure (0.017), aroma (0.048), and price (0.058). The significant relation is in some cases an unpredicted direction. If the consumers believe in the coffee health benefits, they tend not to drink it as a habit or for pleasure or consume coffee for its aroma. Moreover, the positively inclined consumers believe price is a motive of coffee purchasing. Results are confirmed by
p-values.
These results suggest that if consumers drink coffee for the pleasure of it, out of family and traditional habits, and because of the taste and coffee roasting/recipes, then they are distant from the idea that coffee may have a positive health impact. If their coffee purchasing experience is influenced by the product price, then they are sensitive to coffee’s health impact. If coffee purchasing and consumption are not driven by hedonism and traditional routine and are not emotional, then their perception is better inclined towards new features of coffee.
4.3. Consumers’ Willingness to Pay a Price Premium for Coffee Health Benefits
The vast majority of consumers (74%) is willing to pay a price premium for coffee with health benefits (
Table 9). Given that the average price is around €2.75/brick pack, a €1.03 average price premium is equivalent to +37% (average price is €2.78/250 g brick pack, equivalent to €11/kg) [
96]. The price premium is significant. There are variations among the different socio-economic groups of consumers. The highest price premium (between €1.00 and €1.50) would be paid mostly by older (62.9%) and higher income consumers (17.5%). A higher percentage of women (70.4%) are favorable towards fairly high coffee price premiums (between €0.51 and €1.00).
5. Discussion
The debate over coffee’s effects on the human body has gone through various stages, with recommendations aimed at promoting or avoiding coffee consumption. The history of coffee started in the 15th century [
97]. Its consumption first grew in Arabic countries and then expanded to Persia, Egypt, Syria, and Turkey. It was known as “wine of Araby”, and drunk as a substitute for alcohol, which was prohibited according to the Islamic religion. In the 17th century coffee arrived in Europe (e.g., Italy, England, France, Austria). Consumers increasingly drank it in coffee houses that become competitors for pubs, with coffee becoming a substitute for beer and wine. During the 18th century it became common in North America, and then, thanks to the optimal weather, it was cultivated in South America. Brazil is currently the most significant coffee-exporting country. During its long history, coffee has been criticized for various reasons: because it was considered to stimulate critical thinking (Mecca), because it was considered Satanic (Italy), because it was considered as a toxic substance used to bring about death (unsuccessfully) (Sweden), and because it threatened beer consumption and therefore local agricultural production (Prussia) [
97,
98]. As history shows, coffee consumption and the beliefs in its nutritional properties have always been intertwined. Coffee properties perceptions have often shaped coffee consumption and purchasing habits, including preparation methods, favorite types of coffee, and places of consumption and purchasing.
The present research paper provides valuable insights on consumers’ perception over coffee health effects, and profiles coffee consumers’ characteristics based on their positive or negative attitudes towards coffee health effects. There are a number of results that highlight consumers’ socio-economic characteristics and coffee consumption habits, consumers’ motives for coffee consumption and purchasing, and consumers’ interest in coffee with associated health claims.
The present research shows that men are more positively inclined towards coffee health benefits as compared to women. Women appear more skeptical, whereas a higher percentage of men already believe that drinking coffee benefits their health. Considering women’s general strong propensity towards healthy food [
99], coffee with certified health claims may lead women to have a more positive inclination towards it. Moreover, the consumer with a positive attitude towards coffee health benefits is fairly young, works, and has a habit of drinking coffee in social occasions, in limited quantity, and in various preparations, not necessarily espresso. This approach to coffee drinking is in line with the most recent coffee consumption trends. Recent studies support that there is an increasing number of people drinking coffee, with interest in gourmet coffee, new types of coffee (e.g., frozen blended coffee drinks, nitro coffee, and cold brew), out-of-home consumption, and lower appreciation for cafe moka [
9]. Moreover consumers believe coffee has some effects on the human body (e.g., blood pressure, depression, headache, stress and anxiety, body weight). This suggests that there are no specific misconceptions over coffee, but consumers are still not fully aware of coffee’s nutritional potential and health impacts.
Results on the motives for coffee consumption support that the energy coffee provides is the key health effect consumers aim for. Coffee drinkers expect improved alertness and higher physical and mental performance [
24,
25,
77,
78]. There are motives for coffee consumption that differ among the positively and negatively inclined consumers with respect to coffee’s health benefits. The positively inclined consumer to a certain extent values coffee for its aroma, pleasure, habits, and socialization. This is a relevant difference compared to past studies that supported taste as the main motive for coffee drinking [
25,
77,
78,
79]. In consumers, coffee evokes feelings of pleasure and comfort during the drinking experience [
77,
78,
79]. The wide audience of coffee consumers gives particular importance to coffee habit and family traditions that influence preferred occasions, locations, and types of coffee consumption [
24,
25,
82]
Despite the fact that positively inclined consumers drink coffee with others to have a break, socialization is not a key motive. This approach brings a distinguishing interpretation with respect to past studies. These studies suggest that drinking coffee is a way to socialize and be part of a group [
25,
77,
79,
82]. In synthesis, the energizing effect is what the consumer aims for. The consumer aims for a functional drink with a clear mental- and body-stimulating function. This is the same consumer objective for soft drinks and energy drinks.
Results on the motives of coffee purchasing support that for the positively inclined consumer, price is a significant attribute. The consumer is influenced by extrinsic coffee attributes. Coffee purchasing is to a certain degree driven by aroma, coffee recipe, brand, information, and emotions, but rather by rational and economic elements. Therefore, for these consumers messages focused on health claims that give value to the money spent may be important for coffee consumption and purchasing. Past studies found that the use of texts, brands, and metaphorical images on coffee packaging moderately influenced product expectations, intrinsic quality perception, and purchase intention [
89]. Brand identification is especially important in the coffeehouse market [
87,
88,
89,
90]. Drinking a specific coffee brand (e.g., Starbucks) represents a status symbol and way of life for consumers [
87,
88].
Sustainability is one of the most studied subjects in consumer purchasing research on coffee [
20]. Present and past research results suggest that aroma, price, and promotions are more important factors as compared to sustainability [
85]. Only consumers with a strong attitude towards sustainability gave more importance to the sustainability claims over hedonic attributes and were willing to pay more for sustainably produced coffee [
84,
86,
100].
The present research on consumers’ interest in the economic investment over coffee products with health claims further highlights the importance of price in coffee purchasing. Results show that price is an important element for all consumers and that coffee is mostly purchased from large retailers. The importance of price in coffee purchasing shows that coffee is still a rather undifferentiated commodity. Consumers with positive attitudes towards coffee’s health benefits give particular importance to price. Moreover, consumers are generally willing to pay higher prices for coffee with health claims. This is suggested for both positively and negatively coffee health-oriented consumers. In particular, women and consumers with higher monetary resources are more favorable towards healthy food. This is consistent with past research results [
101,
102,
103].
The willingness to pay for coffee with innovative attributes is confirmed by the market expansion of coffee capsules. Capsules have been successful thanks to the low cost of machines, the ease of use, the practicality of packaging, and effective marketing communication campaigns [
96,
104]. This success was achieved despite the high price, with consumers willing to pay up to five times more than coffee powder brick (around €55/kg for coffee capsules). This market phenomenon has been disruptive for the coffee market. It contributed to stopping the price competition that excessively lowered the price of the powder coffee brick, coffee quality, and the capability for investing in coffee research and development as well as innovations.
6. Conclusions
Consumer attitudes toward food products determine consumption behavior more than knowledge. Attitudes and perceptions influence dietary behavior intentions [
105]. Results from the current study on coffee consumers’ consumption and purchasing habits can contribute to a better understanding of food lifestyle decisions. The integration of knowledge of nutritional qualities with knowledge of consumers’ expectations and perceived food qualities allows for addressing possible misconceptions and more effectively defining food consumption and purchasing behavior recommendations.
There is an expanding consumers’ interest for healthy food. Consumers are increasingly aware of the impact food has on body functions [
69,
71,
106]. Coffee consumption has often been negatively criticized for its health effect. Recent studies show that coffee can have positive health effects, but consumers are still cautious on drinking coffee. The coffee image is of a drink with a health impact, but not necessarily positive, and not based on the latest science-based outcomes. Coffee is used for its energetic and therapeutic effects. Together with other energy drinks, it is increasingly used as a substitute for soft drinks. Coffee is a drink with some advantages. It is naturally low in calories if drunk “black”, and it is a drink good for socializing. Coffee chains are expanding. Soft drinks companies are increasingly interested in developing their business to include coffee shop chains [
107].
The coffee market is very dynamic, and consumers are increasingly interested in artisanal coffee and small coffee breweries. Drinking coffee is already acknowledged as a pleasure. The aspects of aroma, taste, smell, and occasions of consumption are still crucial. However, there is space to improve perceptions of scientifically-based health benefits. To increase awareness and improve knowledge among consumers, coffee marketing strategies could focus more on health benefits and nutritional values of coffee [
4,
66,
108] in addition to the other positive characteristics consumers already associate with coffee. As a result, coffee consumption could be marketed as being pleasant and healthy at the same time.
There are already examples for market trends and innovations focusing on the functional and health aspects of coffee. Ready-to-drink (RTD) coffee (packaged liquid coffee designed to be consumed when opened without any additional steps) is interpreted as a clean functional beverage category and a healthier alternative to soft drinks. The RTD coffee segment is expected to grow due to global trends in the coffee sector: worldwide coffee culture growth, active on-the-go-lifestyle, and investments by major players [
109]. Some coffee brands already use health focused strategies for coffee marketing (RTD and ground coffee). RTD cold brew coffee is marketed as a sugar and fat-free alternative to traditional energy drinks [
110] or as a probiotic cold brewed coffee supporting digestive and immune health [
111]. There are examples for a prebiotic fiber-enriched ground coffees with digestive health benefits [
112] and for antioxidant-enriched ground coffees [
113].
The discussion whether coffee can be claimed as an actual functional food is ongoing and there is not enough long-term evidence that coffee can prevent disease. Therefore coffee consumption for health reasons requires further scientific evidence before being recommended and promoted [
7,
28,
114].
Limitations and Future Research
There are some study limitations. Results come from a convenience sample, focused on Italian consumers. Future studies may aim for samples with statistical representativeness and compare perceptions of consumers living in different countries. Coffee consumption behavior is related to various countries’ consumption traditions and habits, and cross-country analysis may bring a more comprehensive perspective. Furthermore, considering the fast development in coffee consumption habits, future studies may focus the analysis on consumers that specifically favor coffee consumption out-of-home or specific coffee types preparations, such as filter, capsules, and powder. Future studies may also test consumers’ WTP for different combinations of coffees with associated health claims such as disease reduction and health-promoting effects. Finally, future studies may explore coffee consumption motives within the dietary lifestyle, so as to provide sound information on the food behavior of coffee consumers for nutritionists and doctors.



{kind=link}