


Mimicking an Asymmetrically Walking Visual Cue Alters Gait Symmetry in Healthy Adults


Abstract
1. Introduction
2. Materials and Methods
2.1. Participants
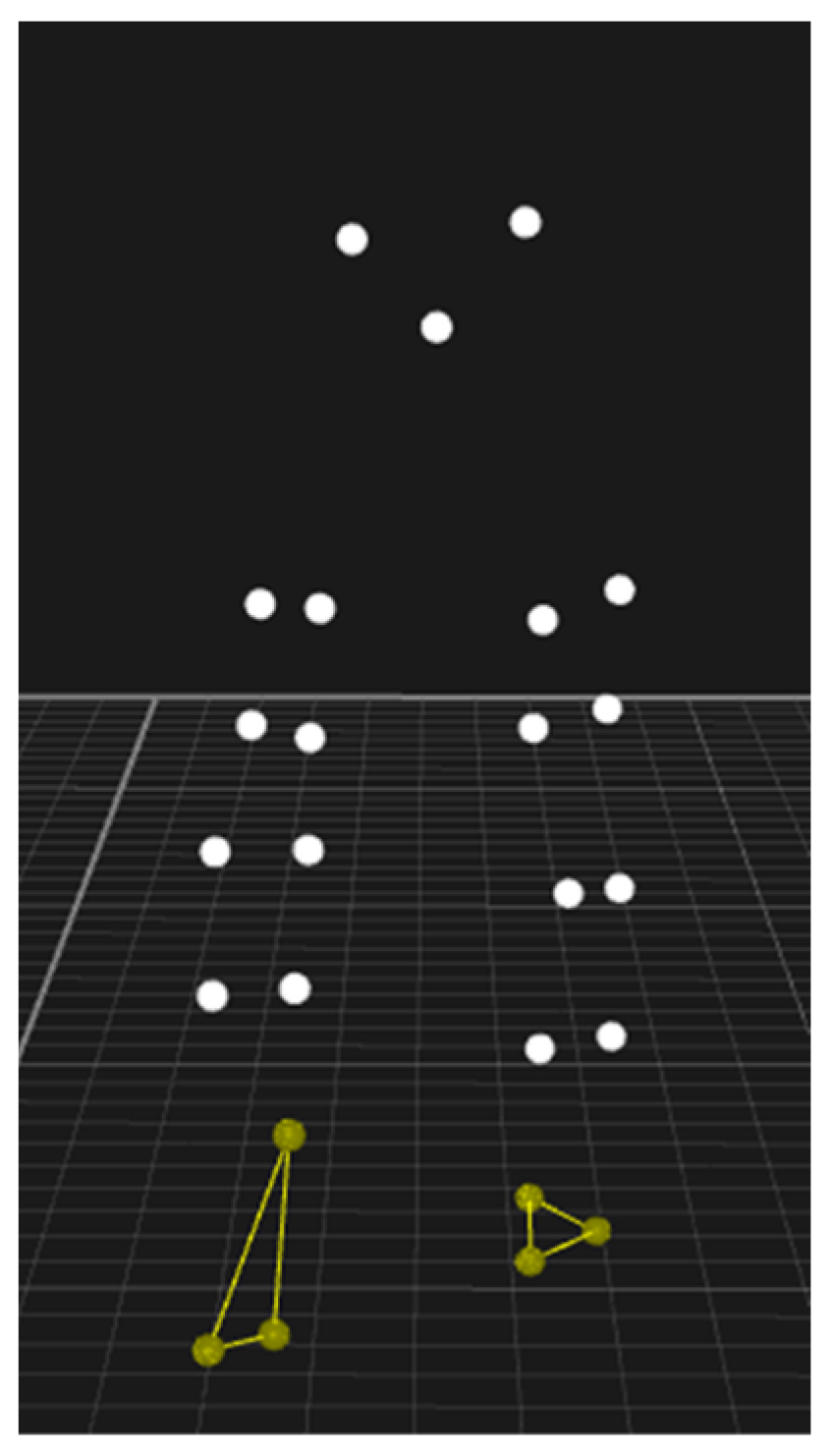
2.2. Procedures
2.3. Statistical Analysis
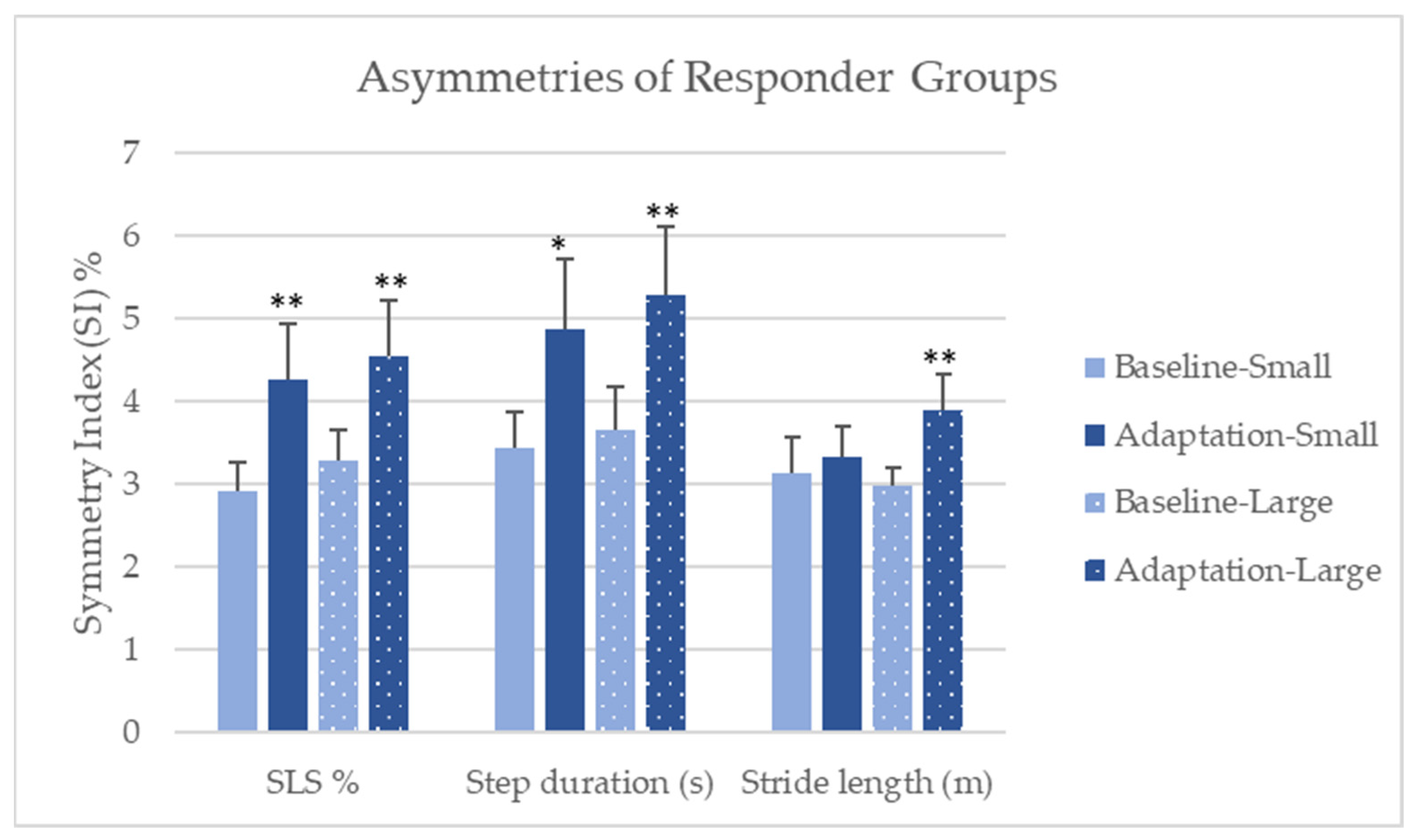
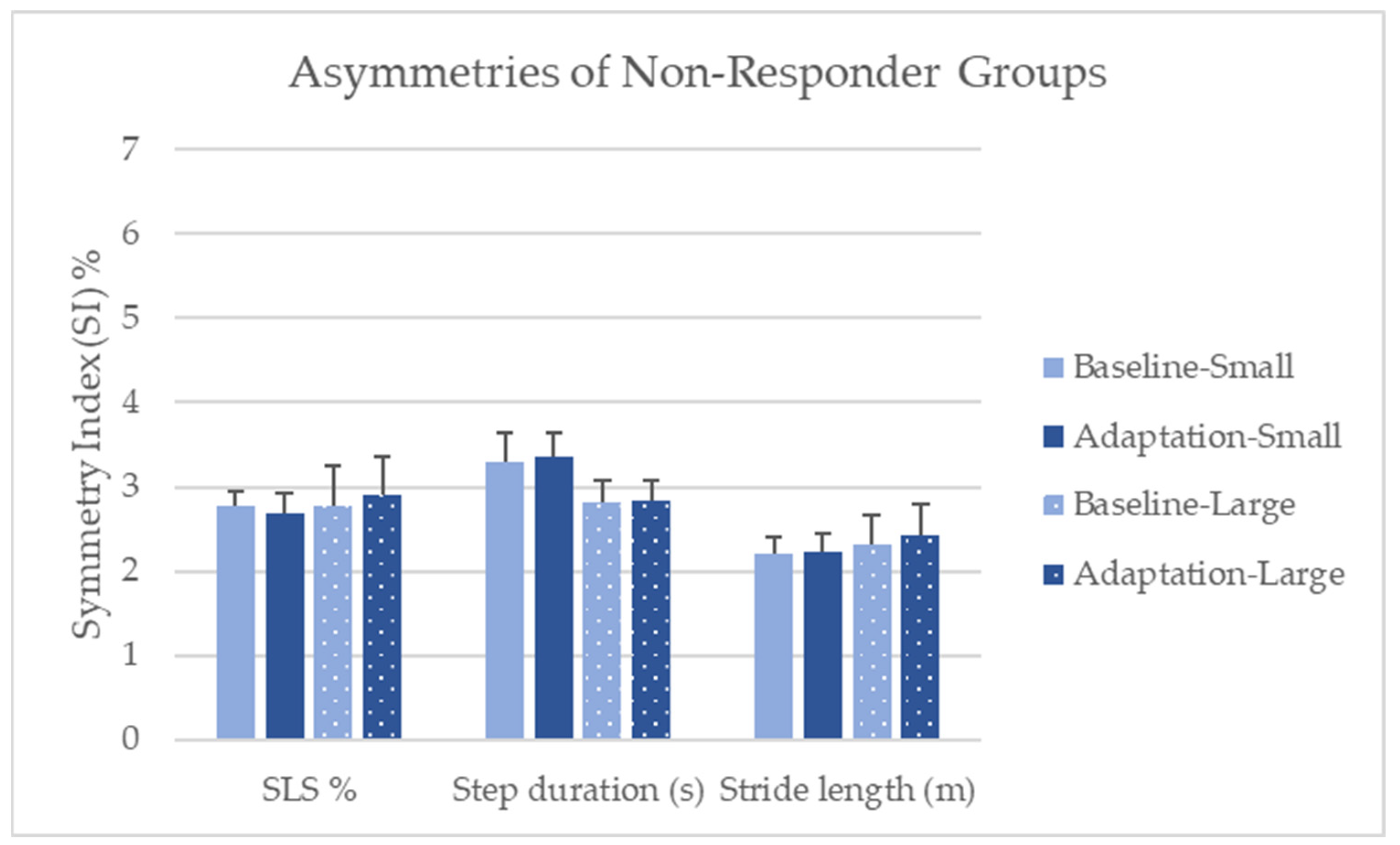
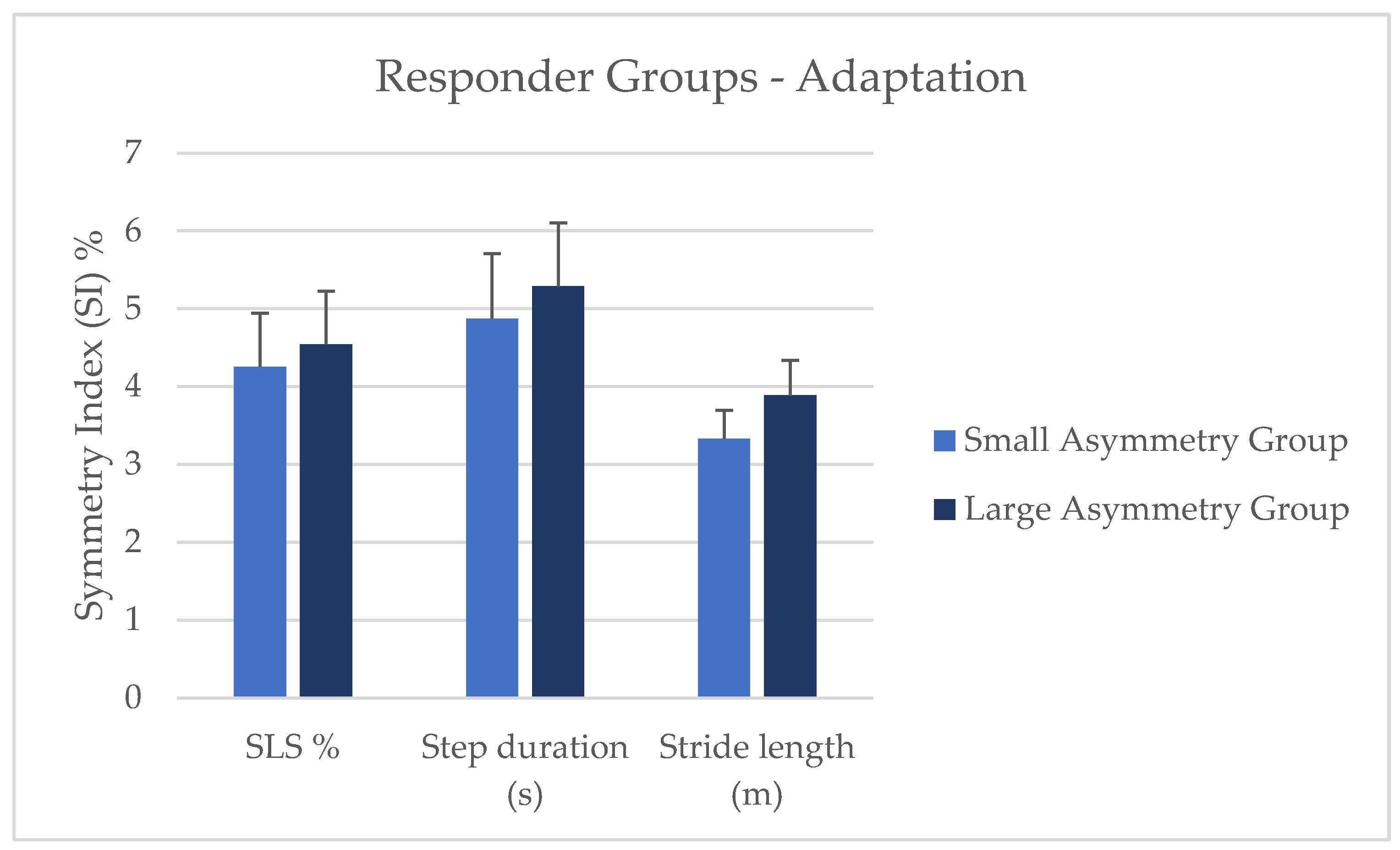
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Jørgensen, L.; Crabtree, N.J.; Reeve, J.; Jacobsen, B.K. Ambulatory Level and Asymmetrical Weight Bearing after Stroke Affects Bone Loss in the Upper and Lower Part of the Femoral Neck Differently: Bone Adaptation after Decreased Mechanical Loading. Bone 2000, 27, 701–707. [Google Scholar] [CrossRef]
- Patterson, K.K.; Parafianowicz, I.; Danells, C.J.; Closson, V.; Verrier, M.C.; Staines, W.R.; Black, S.E.; McIlroy, W.E. Gait Asymmetry in Community-Ambulating Stroke Survivors. Arch. Phys. Med. Rehabil. 2008, 89, 304–310. [Google Scholar] [CrossRef]
- Yogev, G.; Plotnik, M.; Peretz, C.; Giladi, N.; Hausdorff, J.M. Gait Asymmetry in Patients with Parkinson’s Disease and Elderly Fallers: When Does the Bilateral Coordination of Gait Require Attention? Exp. Brain Res. 2007, 177, 336–346. [Google Scholar] [CrossRef]
- Awad, L.N.; Palmer, J.A.; Pohlig, R.T.; Binder-Macleod, S.A.; Reisman, D.S. Walking Speed and Step Length Asymmetry Modify the Energy Cost of Walking After Stroke. Neurorehabilit. Neural Repair 2015, 29, 416–423. [Google Scholar] [CrossRef]
- Lewek, M.D.; Bradley, C.E.; Wutzke, C.J.; Zinder, S.M. The Relationship Between Spatiotemporal Gait Asymmetry and Balance in Individuals With Chronic Stroke. J. Appl. Biomech. 2014, 30, 31–36. [Google Scholar] [CrossRef]
- Wei, T.-S.; Liu, P.-T.; Chang, L.-W.; Liu, S.-Y. Gait Asymmetry, Ankle Spasticity, and Depression as Independent Predictors of Falls in Ambulatory Stroke Patients. PLoS ONE 2017, 12, e0177136. [Google Scholar] [CrossRef]
- Alexander, B.H.; Rivara, F.P.; Wolf, M.E. The Cost and Frequency of Hospitalization for Fall-Related Injuries in Older Adults. Am. J. Public Health 1992, 82, 1020–1023. [Google Scholar] [CrossRef]
- Axer, H.; Axer, M.; Sauer, H.; Witte, O.W.; Hagemann, G. Falls and Gait Disorders in Geriatric Neurology. Clin. Neurol. Neurosurg. 2010, 112, 265–274. [Google Scholar] [CrossRef]
- Contreras, A.; Grandas, F. Risk of Falls in Parkinson’s Disease: A Cross-Sectional Study of 160 Patients. Park. Dis. 2012, 2012, 362572. [Google Scholar] [CrossRef]
- Mahlknecht, P.; Kiechl, S.; Bloem, B.R.; Willeit, J.; Scherfler, C.; Gasperi, A.; Rungger, G.; Poewe, W.; Seppi, K. Prevalence and Burden of Gait Disorders in Elderly Men and Women Aged 60–97 Years: A Population-Based Study. PLoS ONE 2013, 8, e69627. [Google Scholar] [CrossRef]
- Malone, L.A.; Bastian, A.J. Spatial and Temporal Asymmetries in Gait Predict Split-Belt Adaptation Behavior in Stroke. Neurorehabilit. Neural Repair 2014, 28, 230–240. [Google Scholar] [CrossRef]
- Sterling, D.A.; O’Connor, J.A.; Bonadies, J. Geriatric Falls: Injury Severity Is High and Disproportionate to Mechanism. J. Trauma Acute Care Surg. 2001, 50, 116–119. [Google Scholar] [CrossRef]
- Wagner, L.M.; Phillips, V.L.; Hunsaker, A.E.; Forducey, P.G. Falls among Community-Residing Stroke Survivors Following Inpatient Rehabilitation: A Descriptive Analysis of Longitudinal Data. BMC Geriatr. 2009, 9, 46. [Google Scholar] [CrossRef]
- Brandstater, M.E.; de Bruin, H.; Gowland, C.; Clark, B.M. Hemiplegic Gait: Analysis of Temporal Variables. Arch. Phys. Med. Rehabil. 1983, 64, 583–587. [Google Scholar]
- Nanhoe-Mahabier, W.; Snijders, A.H.; Delval, A.; Weerdesteyn, V.; Duysens, J.; Overeem, S.; Bloem, B.R. Split-Belt Locomotion in Parkinson’s Disease with and without Freezing of Gait. Neuroscience 2013, 236, 110–116. [Google Scholar] [CrossRef]
- Reisman, D.S.; Wityk, R.; Silver, K.; Bastian, A.J. Locomotor Adaptation on a Split-Belt Treadmill Can Improve Walking Symmetry Post-Stroke. Brain 2007, 130, 1861–1872. [Google Scholar] [CrossRef]
- Reisman, D.S.; McLean, H.; Keller, J.; Danks, K.A.; Bastian, A.J. Repeated Split-BeltTreadmill Training Improves Poststroke Step Length Asymmetry. Neurorehabilit. Neural Repair 2013, 27, 460–468. [Google Scholar] [CrossRef]
- Roemmich, R.T.; Nocera, J.R.; Stegemöller, E.L.; Hassan, A.; Okun, M.S.; Hass, C.J. Locomotor Adaptation and Locomotor Adaptive Learning in Parkinson’s Disease and Normal Aging. Clin. Neurophysiol. 2014, 125, 313–319. [Google Scholar] [CrossRef]
- Meder, K.G.; LoJacono, C.T.; Rhea, C.K. A Systematic Review of Non-Pharmacological Interventions to Improve Gait Asymmetries in Neurological Populations. Symmetry 2022, 14, 281. [Google Scholar] [CrossRef]
- Reisman, D.S.; Block, H.J.; Bastian, A.J. Interlimb Coordination During Locomotion: What Can Be Adapted and Stored? J. Neurophysiol. 2005, 94, 2403–2415. [Google Scholar] [CrossRef]
- Lewek, M.D.; Braun, C.H.; Wutzke, C.; Giuliani, C. The Role of Movement Errors in Modifying Spatiotemporal Gait Asymmetry Post Stroke: A Randomized Controlled Trial. Clin. Rehabil. 2018, 32, 161–172. [Google Scholar] [CrossRef]
- Maidan, I.; Patashov, D.; Shustak, S.; Fahoum, F.; Gazit, E.; Shapiro, B.; Levy, A.; Sosnik, R.; Giladi, N.; Hausdorff, J.M.; et al. A New Approach to Quantifying the EEG during Walking: Initial Evidence of Gait Related Potentials and Their Changes with Aging and Dual Tasking. Exp. Gerontol. 2019, 126, 110709. [Google Scholar] [CrossRef]
- Pozzi, N.G.; Canessa, A.; Palmisano, C.; Brumberg, J.; Steigerwald, F.; Reich, M.M.; Minafra, B.; Pacchetti, C.; Pezzoli, G.; Volkmann, J.; et al. Freezing of Gait in Parkinson’s Disease Reflects a Sudden Derangement of Locomotor Network Dynamics. Brain 2019, 142, 2037–2050. [Google Scholar] [CrossRef]
- Hasegawa, N.; Shah, V.V.; Carlson-Kuhta, P.; Nutt, J.G.; Horak, F.B.; Mancini, M. How to Select Balance Measures Sensitive to Parkinson’s Disease from Body-Worn Inertial Sensors-Separating the Trees from the Forest. Sensors 2019, 19, 3320. [Google Scholar] [CrossRef]
- Cano Porras, D.; Siemonsma, P.; Inzelberg, R.; Zeilig, G.; Plotnik, M. Advantages of Virtual Reality in the Rehabilitation of Balance and Gait: Systematic Review. Neurology 2018, 90, 1017–1025. [Google Scholar] [CrossRef]
- Janeh, O.; Fründt, O.; Schönwald, B.; Gulberti, A.; Buhmann, C.; Gerloff, C.; Steinicke, F.; Pötter-Nerger, M. Gait Training in Virtual Reality: Short-Term Effects of Different Virtual Manipulation Techniques in Parkinson’s Disease. Cells 2019, 8, 419. [Google Scholar] [CrossRef]
- Keshner, E.A.; Lamontagne, A. The Untapped Potential of Virtual Reality in Rehabilitation of Balance and Gait in Neurological Disorders. Front. Virtual Real. 2021, 2, 6. [Google Scholar] [CrossRef]
- Liu, L.Y.; Sangani, S.; Patterson, K.K.; Fung, J.; Lamontagne, A. Real-Time Avatar-Based Feedback to Enhance the Symmetry of Spatiotemporal Parameters After Stroke: Instantaneous Effects of Different Avatar Views. IEEE Trans. Neural Syst. Rehabil. Eng. 2020, 28, 878–887. [Google Scholar] [CrossRef]
- Meerhoff, L.A.; De Poel, H.J.; Jowett, T.W.D.; Button, C. Walking with Avatars: Gait-Related Visual Information for Following a Virtual Leader. Hum. Mov. Sci. 2019, 66, 173–185. [Google Scholar] [CrossRef]
- Rhea, C.K.; Kiefer, A.W.; D’Andrea, S.E.; Warren, W.H.; Aaron, R.K. Entrainment to a Real Time Fractal Visual Stimulus Modulates Fractal Gait Dynamics. Hum. Mov. Sci. 2014, 36, 20–34. [Google Scholar] [CrossRef]
- Soczawa-Stronczyk, A.A.; Bocian, M. Gait Coordination in Overground Walking with a Virtual Reality Avatar. R. Soc. Open Sci. 2020, 7, 200622. [Google Scholar] [CrossRef] [PubMed]
- Felsberg, D.T.; Rhea, C.K. Spontaneous Interpersonal Synchronization of Gait: A Systematic Review. Arch. Rehabil. Res. Clin. Transl. 2021, 3, 100097. [Google Scholar] [CrossRef] [PubMed]
- Kaufman, K.R.; Miller, L.S.; Sutherland, D.H. Gait Asymmetry in Patients with Limb-Length Inequality. J. Pediatr. Orthop. 1996, 16, 144–150. [Google Scholar] [CrossRef] [PubMed]
- Khamis, S.; Carmeli, E. Relationship and Significance of Gait Deviations Associated with Limb Length Discrepancy: A Systematic Review. Gait Posture 2017, 57, 115–123. [Google Scholar] [CrossRef] [PubMed]
- Dingwell, J.B.; Marin, L.C. Kinematic Variability and Local Dynamic Stability of Upper Body Motions When Walking at Different Speeds. J. Biomech. 2006, 39, 444–452. [Google Scholar] [CrossRef] [PubMed]
- Reisman, D.S.; Wityk, R.; Silver, K.; Bastian, A.J. Split-Belt Treadmill Adaptation Transfers to Overground Walking in Persons Poststroke. Neurorehabilit. Neural Repair 2009, 23, 735–744. [Google Scholar] [CrossRef] [PubMed]
- Morris, R.; Stuart, S.; McBarron, G.; Fino, P.C.; Mancini, M.; Curtze, C. Validity of MobilityLab (Version 2) for Gait Assessment in Young Adults, Older Adults and Parkinson’s Disease. Physiol. Meas. 2019, 40, 095003. [Google Scholar] [CrossRef] [PubMed]
- Faul, F.; Erdfelder, E.; Lang, A.-G.; Buchner, A. G*Power 3: A Flexible Statistical Power Analysis Program for the Social, Behavioral, and Biomedical Sciences. Behav. Res. Methods 2007, 39, 175–191. [Google Scholar] [CrossRef] [PubMed]
- R Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2023. [Google Scholar]
- Błażkiewicz, M.; Wiszomirska, I.; Wit, A. Comparison of Four Methods of Calculating the Symmetry of Spatial-Temporal Parameters of Gait. Acta Bioeng. Biomech. 2014, 16, 29–35. [Google Scholar] [CrossRef]
- Kassambara, A. rstatix: Pipe-Friendly Framework for Basic Statistical Tests. R Package Version 0.7.2, 2023. Available online: https://cran.r-project.org/web/packages/rstatix/index.html (accessed on 10 May 2024).
- Wilcox, R. A Robust Nonparametric Measure of Effect Size Based on an Analog of Cohen’s d, Plus Inferences About the Median of the Typical Difference. J. Mod. Appl. Stat. Methods 2019, 17, eP2726. [Google Scholar] [CrossRef]
- Prokop, T.; Berger, W.; Zijlstra, W.; Dietz, V. Adaptational and Learning Processes during Human Split-Belt Locomotion: Interaction between Central Mechanisms and Afferent Input. Exp. Brain Res. 1995, 106, 449–456. [Google Scholar] [CrossRef] [PubMed]
- Bruijn, S.M.; Van Impe, A.; Duysens, J.; Swinnen, S.P. Split-Belt Walking: Adaptation Differences between Young and Older Adults. J. Neurophysiol. 2012, 108, 1149–1157. [Google Scholar] [CrossRef] [PubMed]
- Leitner, Y.; Barak, R.; Giladi, N.; Peretz, C.; Eshel, R.; Gruendlinger, L.; Hausdorff, J.M. Gait in Attention Deficit Hyperactivity Disorder. J. Neurol. 2007, 254, 1330–1338. [Google Scholar] [CrossRef]
- Schmidt, R.A.; Lee, T.D.; Winstein, C.J.; Wulf, G.; Zelaznik, H.N. Motor Control and Learning: A Behavioral Emphasis; Human Kinetics: Champaign, IL, USA, 2019; ISBN 978-1-4925-4775-4. [Google Scholar]
- Bootsma, J.M.; Hortobágyi, T.; Rothwell, J.C.; Caljouw, S.R. The Role of Task Difficulty in Learning a Visuomotor Skill. Med. Sci. Sports Exerc. 2018, 50, 1842. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | Small Res (n = 20) | Small Non-R (n = 12) | Large Res (n = 22) | Large Non-R (n = 10) | Control (n = 8) | p |
|---|---|---|---|---|---|---|
| Age (years) | 24.09 (6.29) | 22.62 (7.30) | 23.57 (4.33) | 23.93 (6.98) | 26.16 (2.37) | 0.520 |
| Height (cm) | 168.29 (10.50) | 166.32 (8.93) | 167.97 (8.90) | 169.20 (5.79) | 168.20 (3.77) | 0.822 |
| Weight (kg) | 70.22 (15.45) | 68.00 (17.40) | 71.07 (16.68) | 75.89 (9.98) | 69.97 (2.79) | 0.564 |
| Preferred walking speed (m/s) | 0.88 (0.16) | 0.93 (0.18) | 0.84 (0.16) | 0.96 (0.15) | 1.14 (0.09) | 0.011 * |
| Left leg length (cm) | 88.40 (6.67) | 88.31 (5.22) | 87.69 (5.96) | 89.32 (3.35) | 88.60 (2.10) | 0.860 |
| Right leg length (cm) | 88.37 (6.91) | 88.75 (5.38) | 87.72 (6.26) | 89.12 (3.31) | 88.68 (2.13) | 0.906 |
| Leg length difference (cm) | 0.51 (0.30) | 0.56 (0.44) | 0.39 (0.30) | 0.50 (0.28) | 0.30 (0.07) | 0.128 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Clark, K.G.; Raisbeck, L.D.; Ross, S.E.; Rhea, C.K. Mimicking an Asymmetrically Walking Visual Cue Alters Gait Symmetry in Healthy Adults. Biomechanics 2024, 4, 346-356. https://doi.org/10.3390/biomechanics4020024
Clark KG, Raisbeck LD, Ross SE, Rhea CK. Mimicking an Asymmetrically Walking Visual Cue Alters Gait Symmetry in Healthy Adults. Biomechanics. 2024; 4(2):346-356. https://doi.org/10.3390/biomechanics4020024
Chicago/Turabian StyleClark, Krista G., Louisa D. Raisbeck, Scott E. Ross, and Christopher K. Rhea. 2024. "Mimicking an Asymmetrically Walking Visual Cue Alters Gait Symmetry in Healthy Adults" Biomechanics 4, no. 2: 346-356. https://doi.org/10.3390/biomechanics4020024
APA StyleClark, K. G., Raisbeck, L. D., Ross, S. E., & Rhea, C. K. (2024). Mimicking an Asymmetrically Walking Visual Cue Alters Gait Symmetry in Healthy Adults. Biomechanics, 4(2), 346-356. https://doi.org/10.3390/biomechanics4020024