
Inertial Sensing of the Abdominal Wall Kinematics during Diaphragmatic Breathing in Head Standing



Abstract
1. Introduction
2. Materials and Methods
2.1. Participants
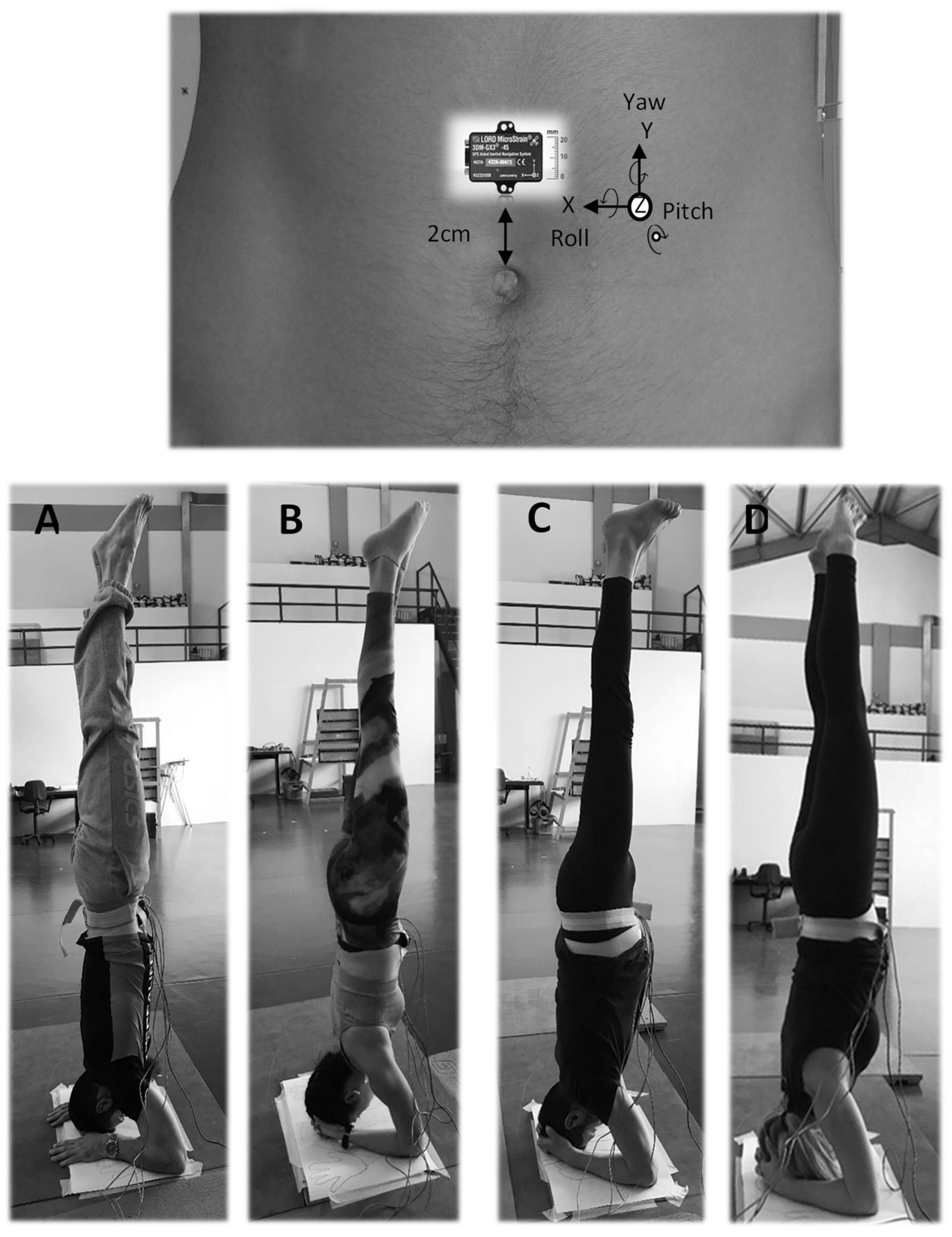
2.2. Experimental Procedure
2.2.1. Verification of Diaphragmatic Breathing Pattern
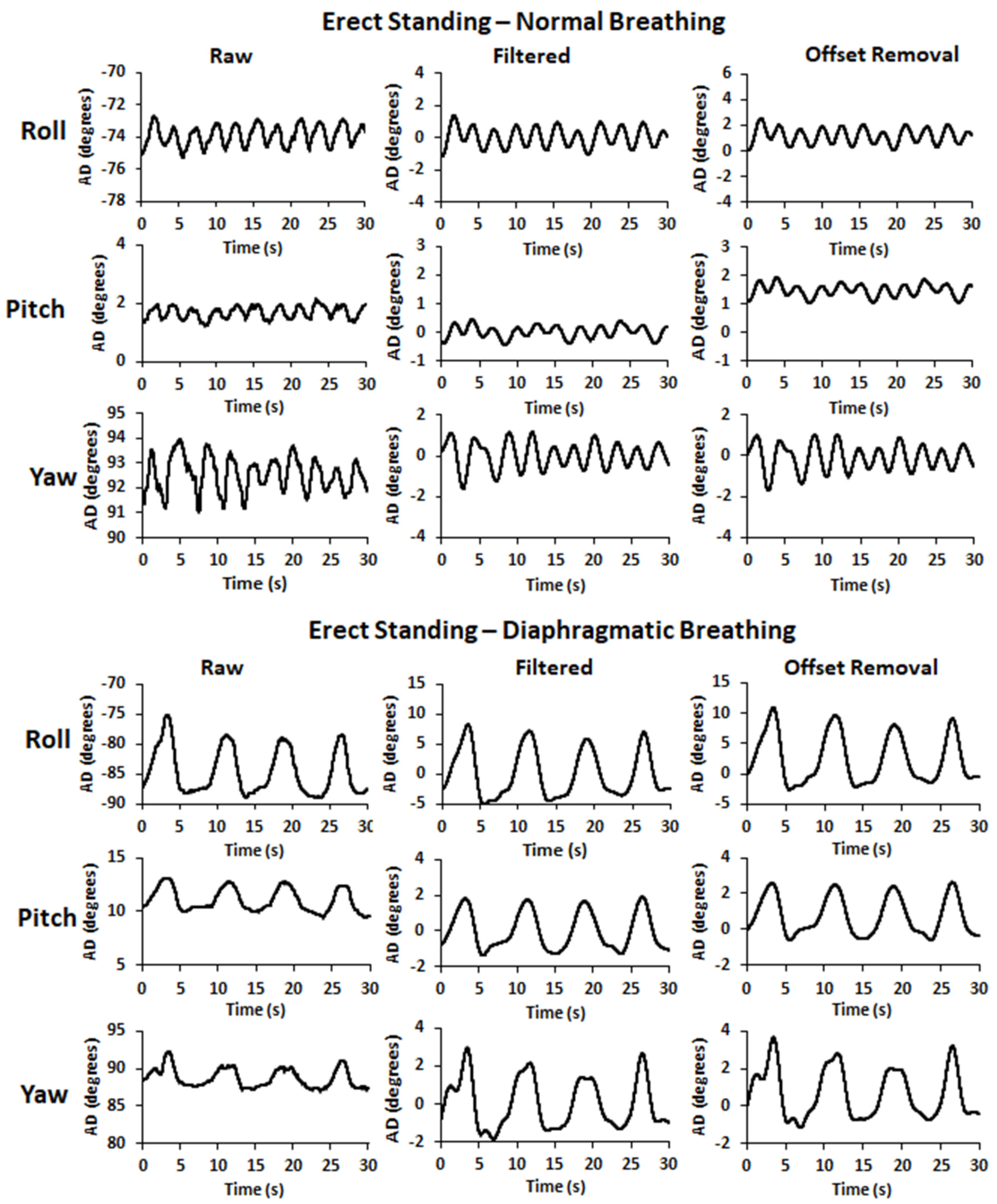
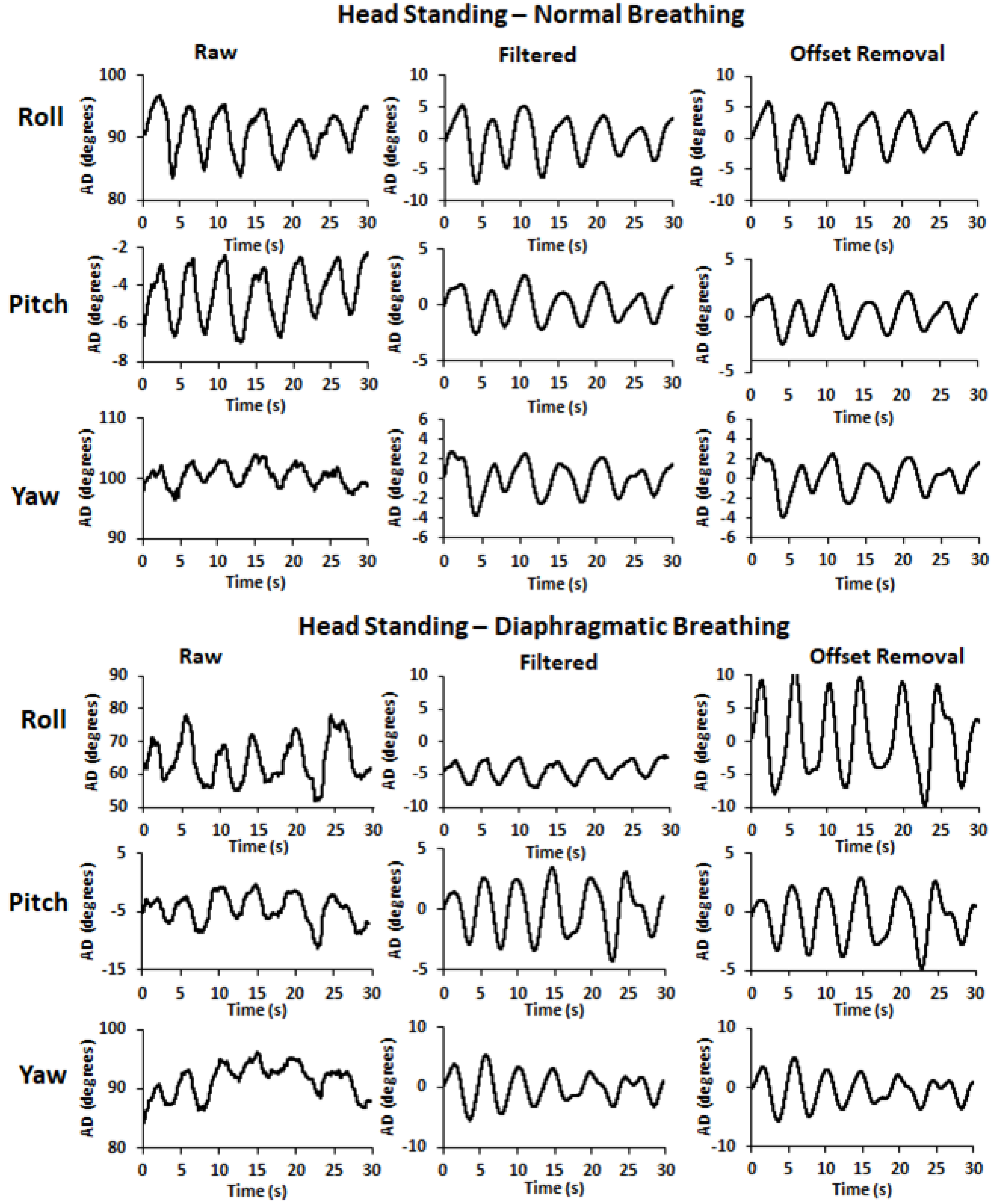
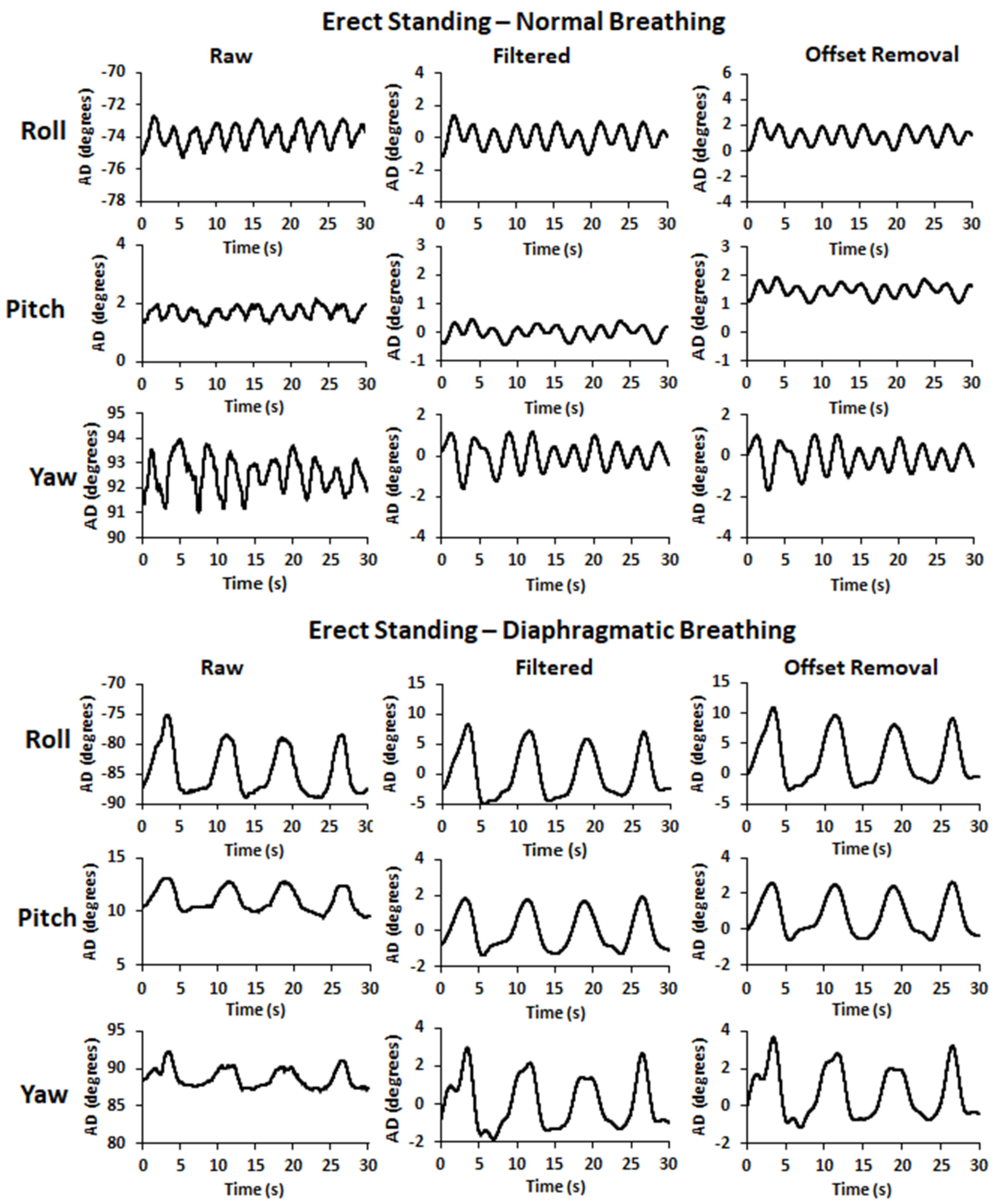
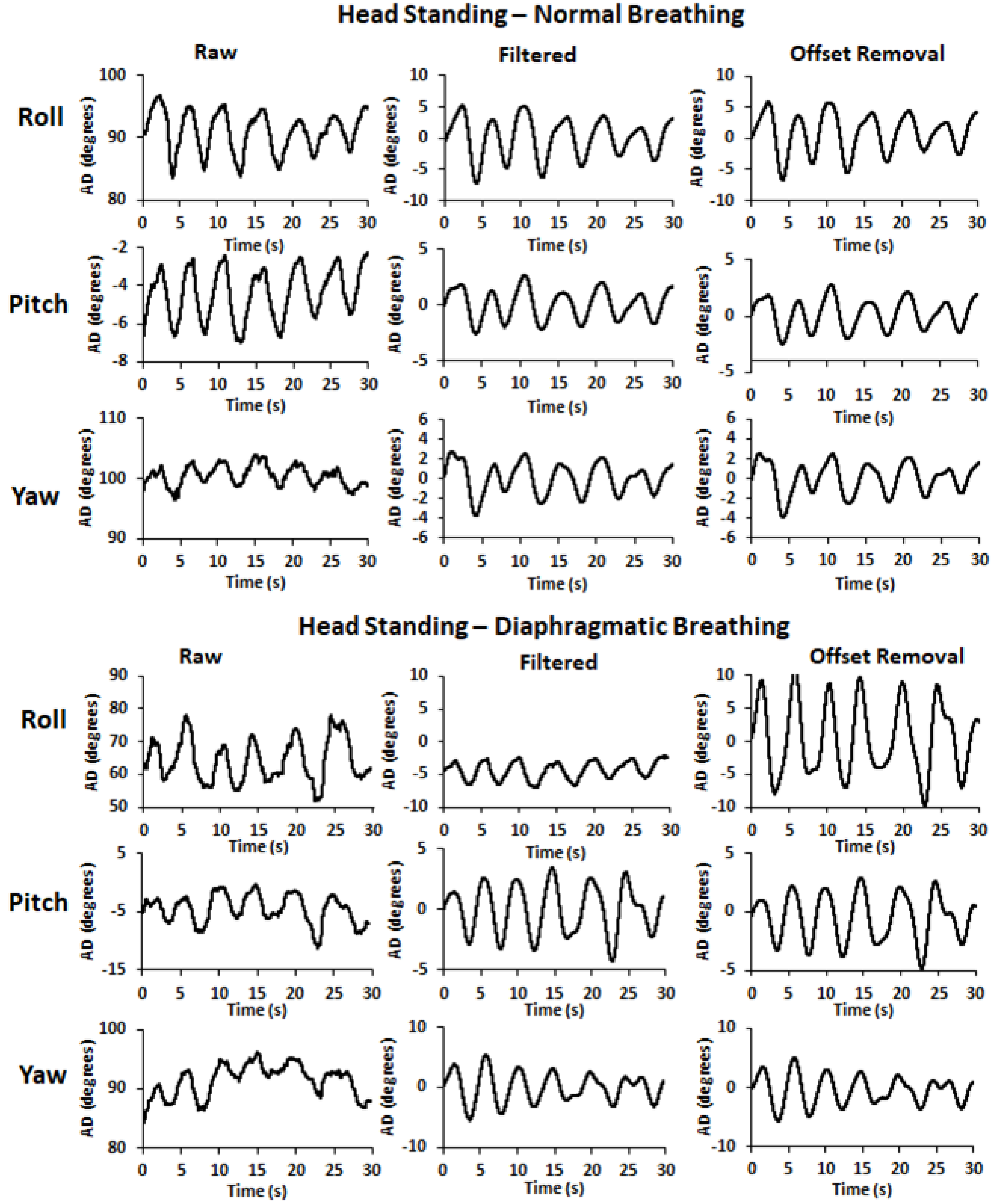
2.2.2. Data Collection
2.2.3. Data Procession
2.2.4. Estimation of Angular Displacement (AD) Variables
2.2.5. Cross-Correlation, Relative Reliability, Standard Error of Measurement, and Minimal Detectable Change
2.3. Statistical Analysis
3. Results
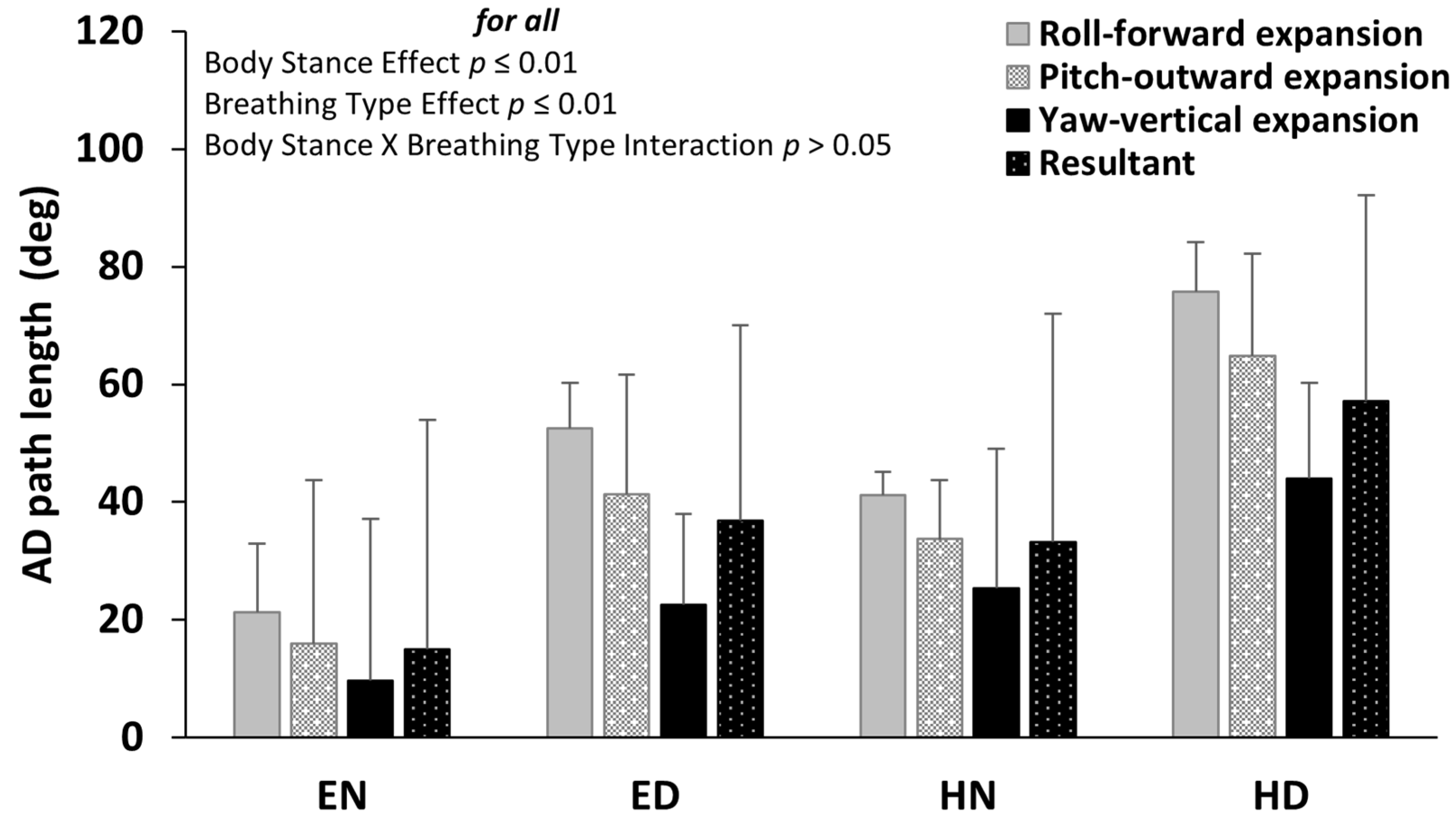
3.1. Angular Displacement Path Length
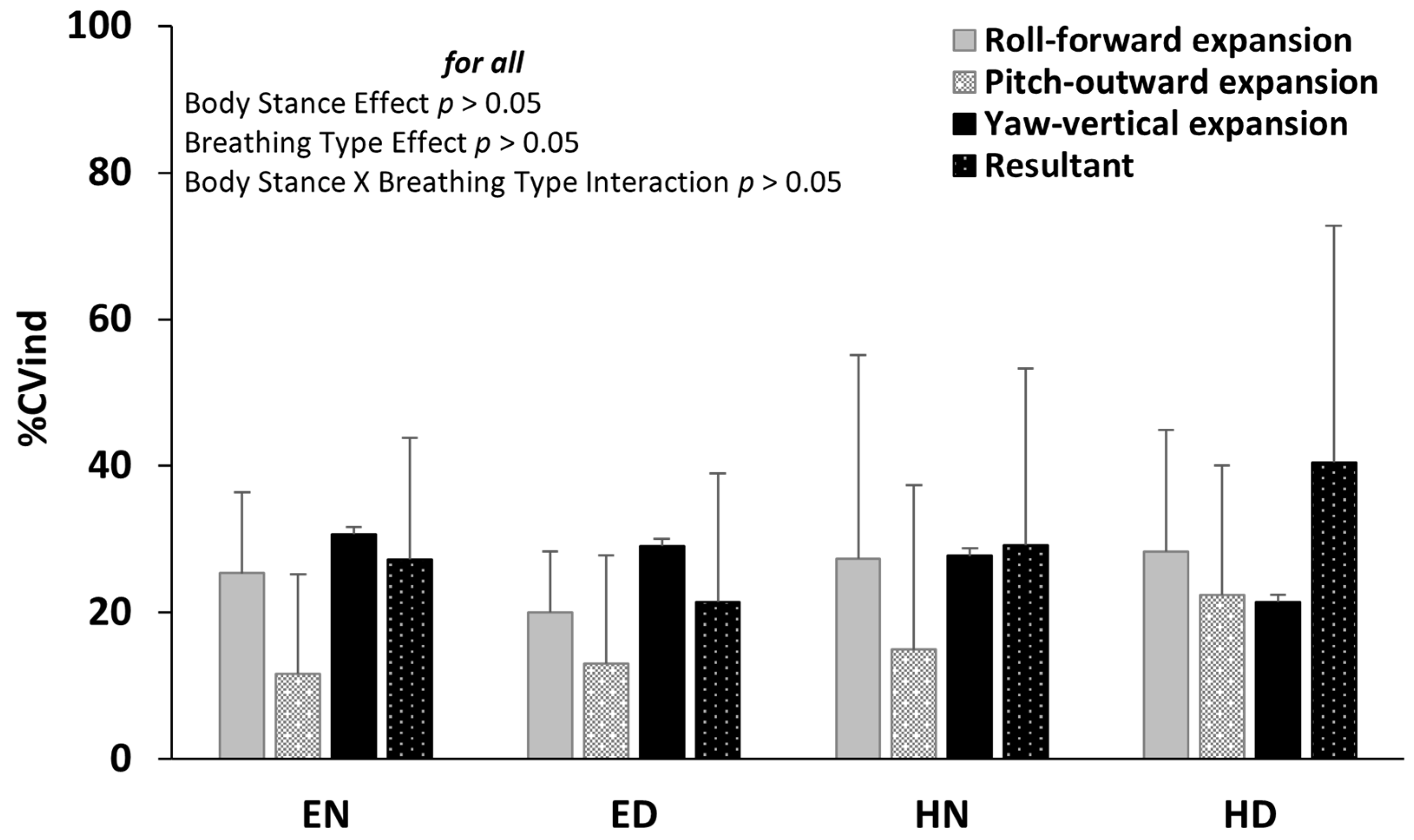
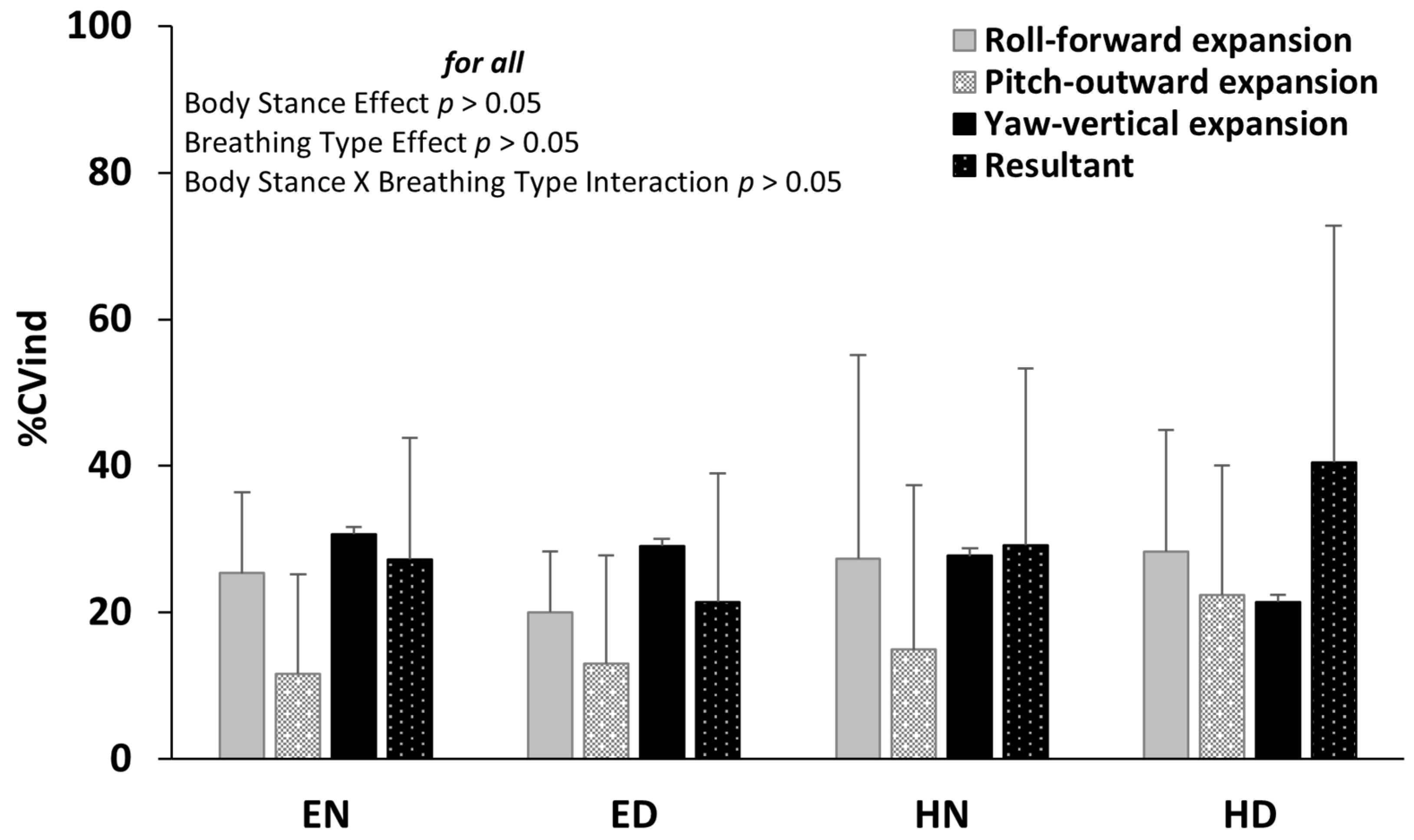
3.2. Individual Variability of AD Path
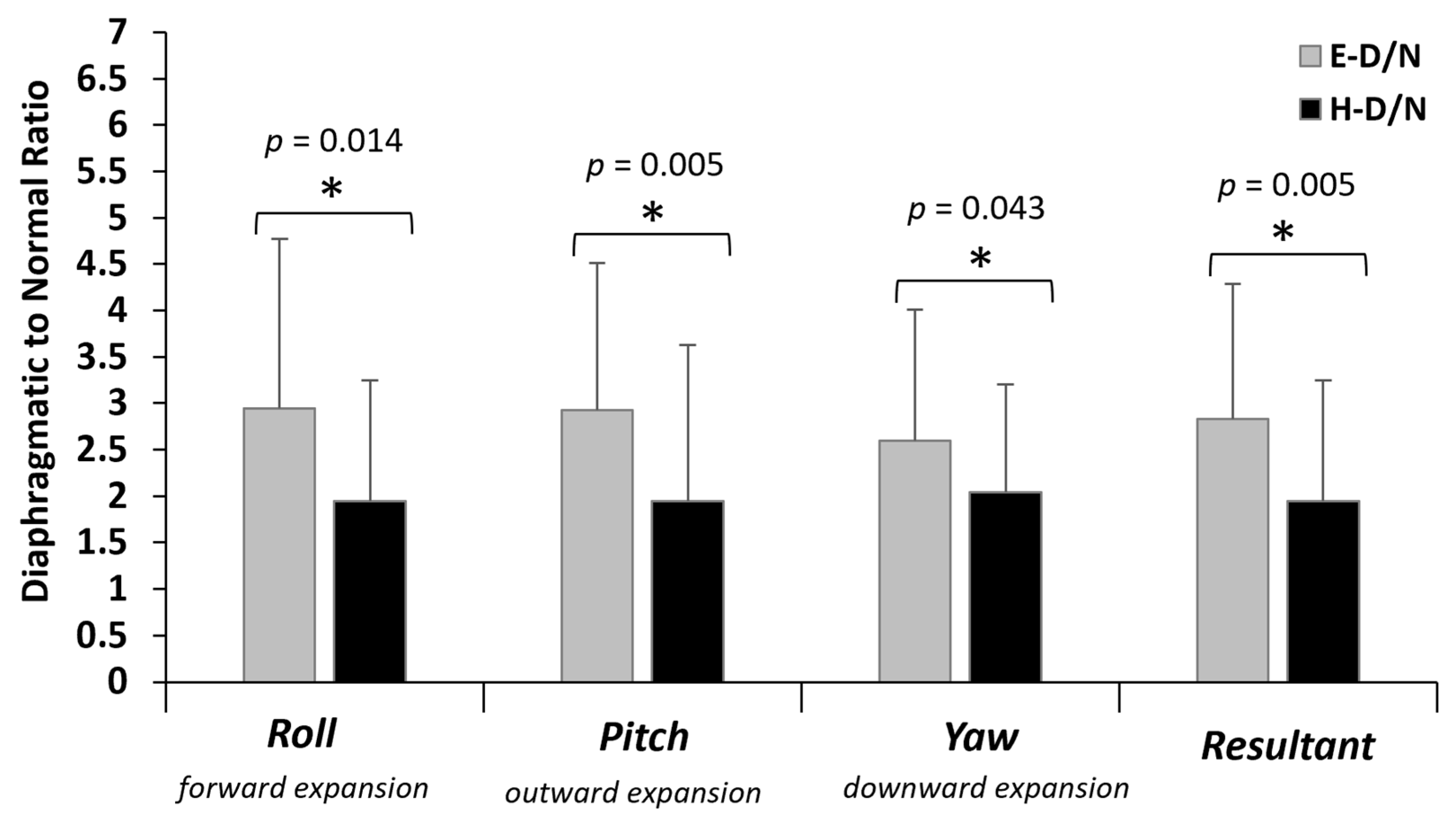
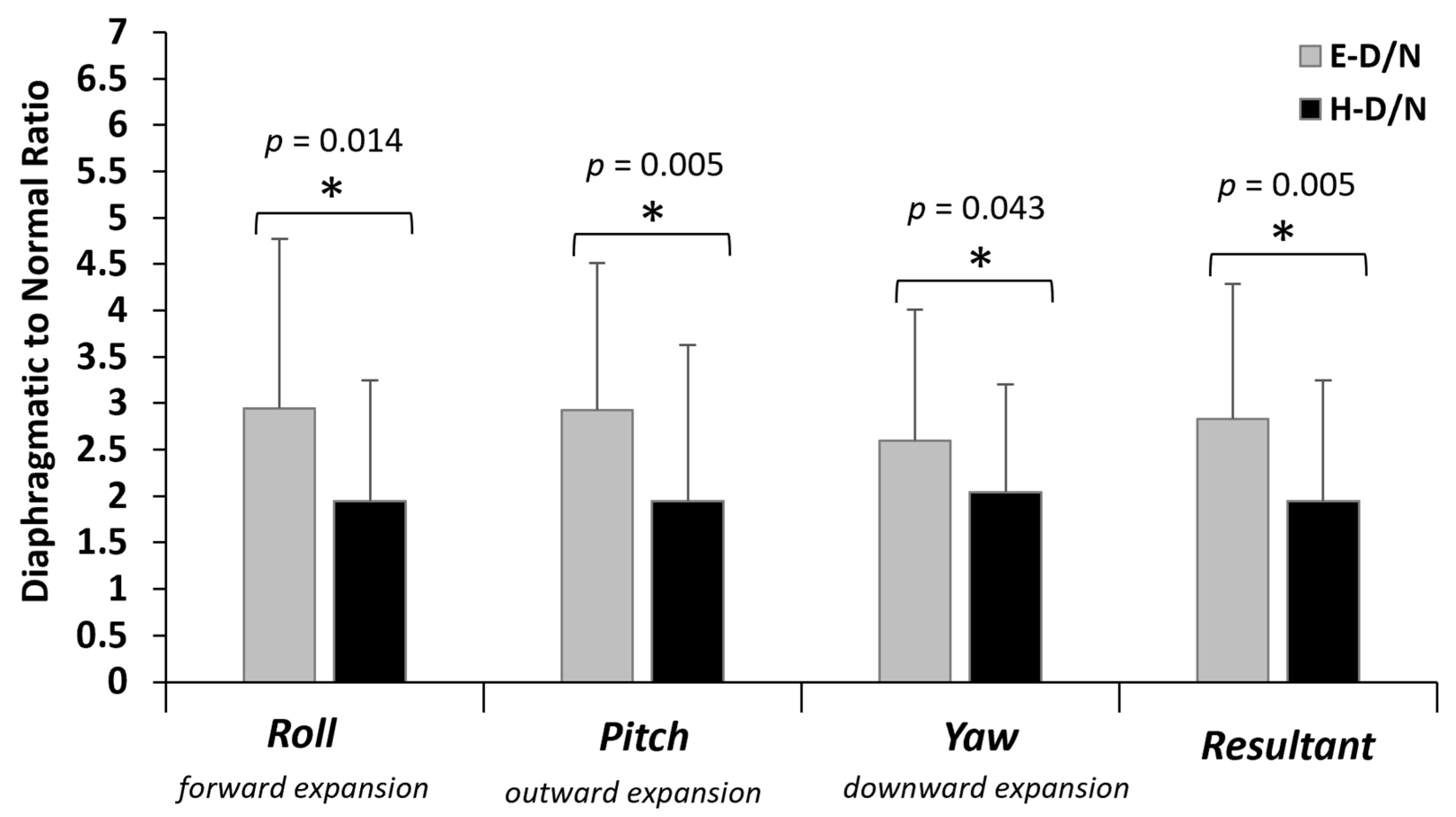
3.3. Diaphragmatic to Normal Breathing Ratio of AD Path
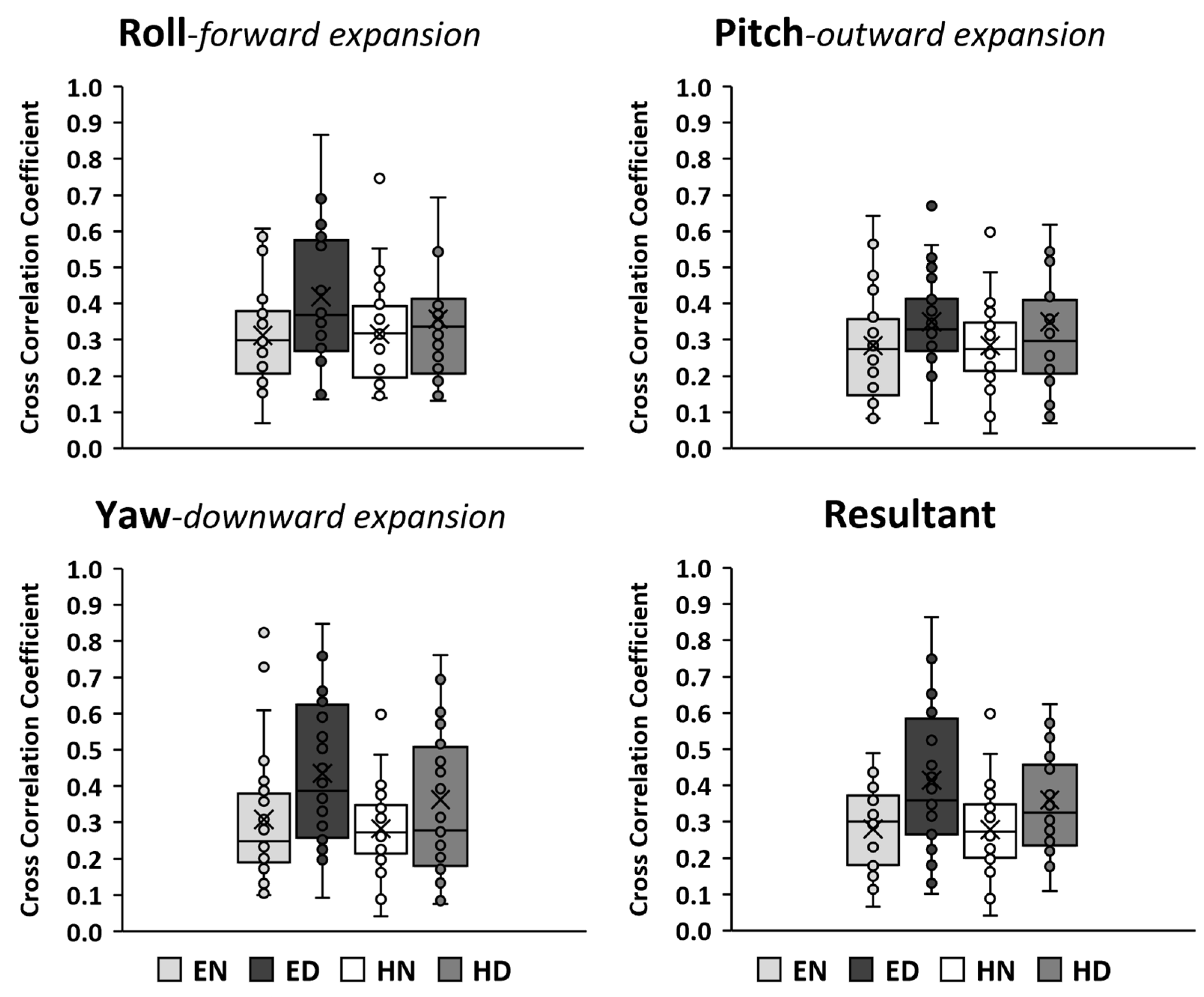
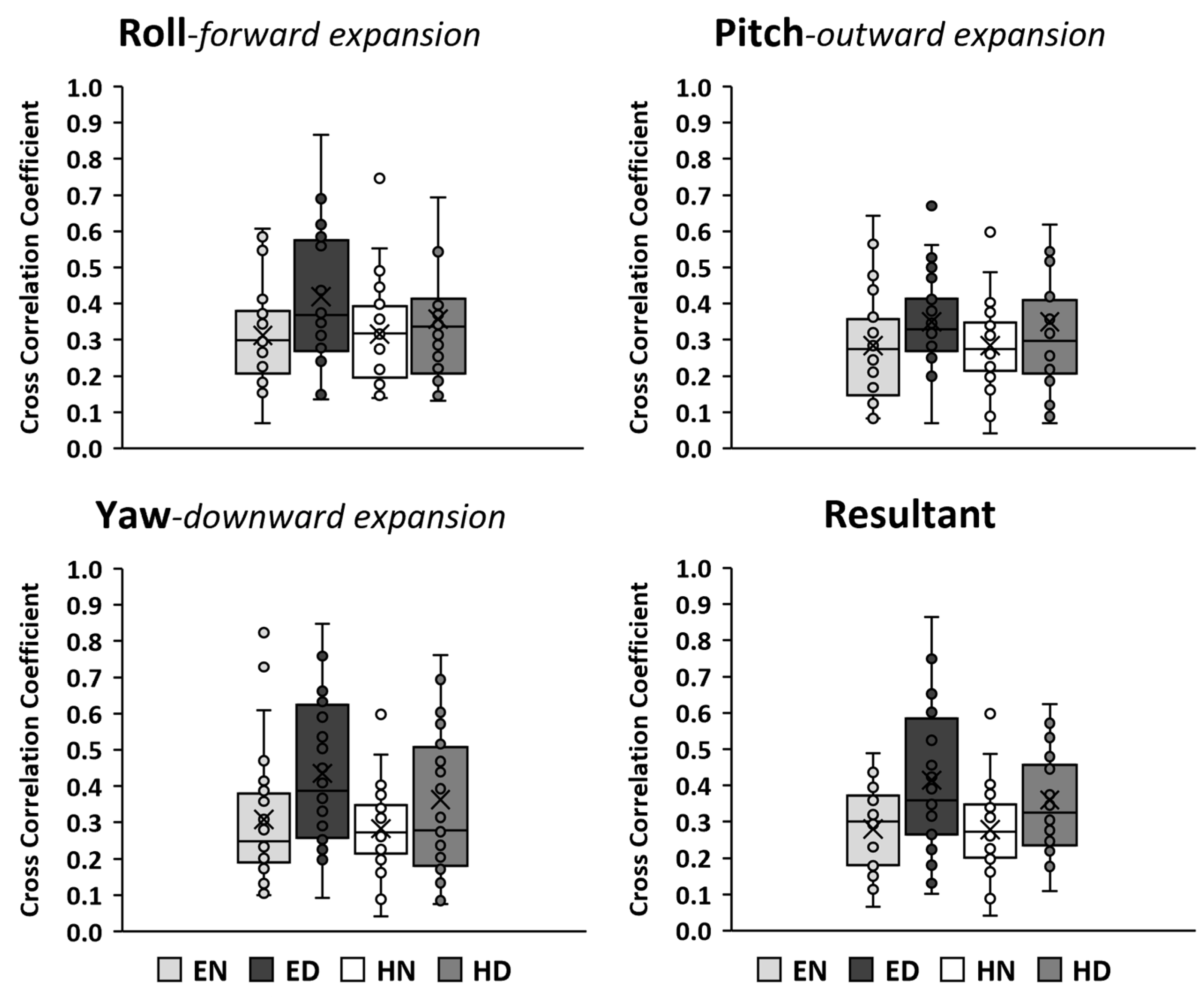
3.4. Cross-Correlation of AD Time Series Signals
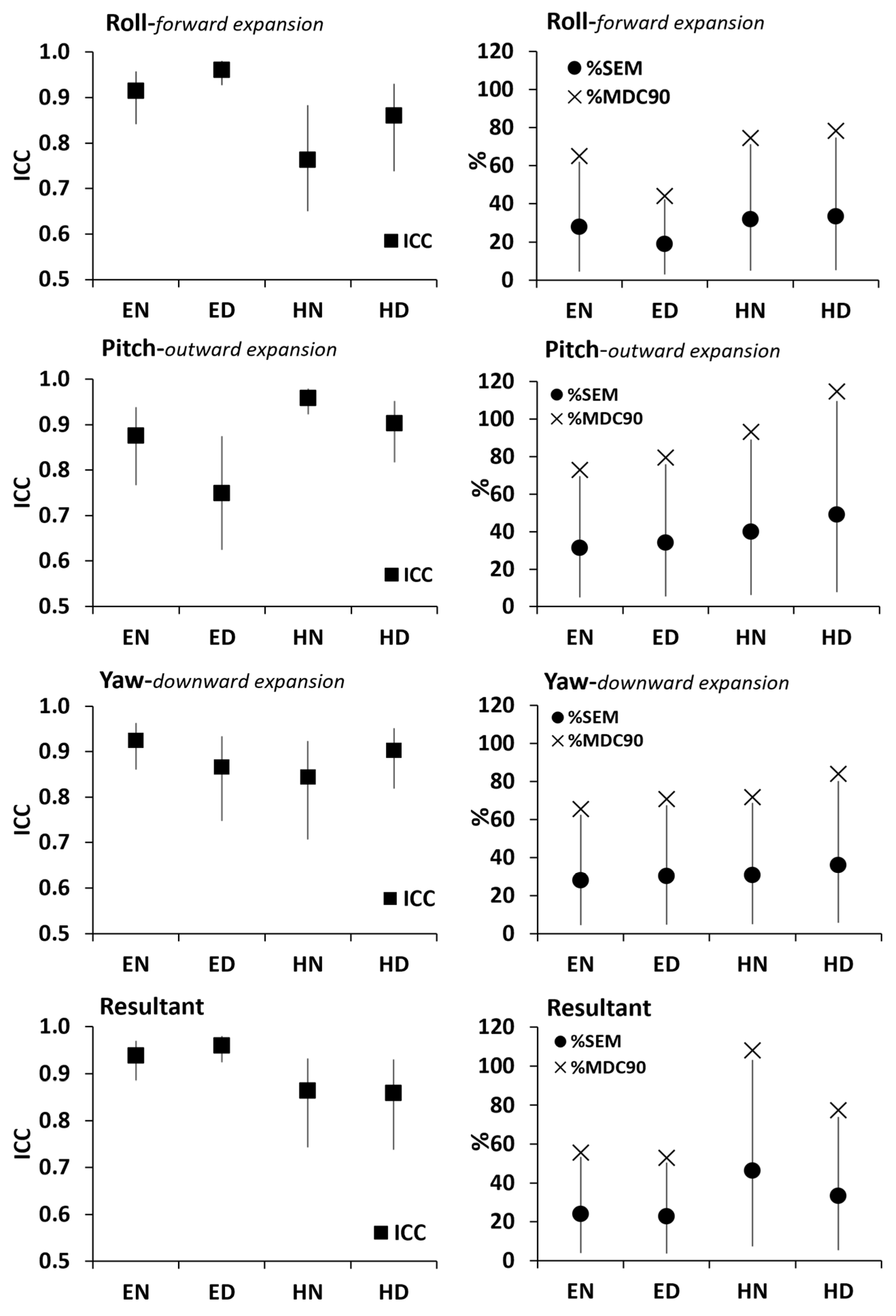
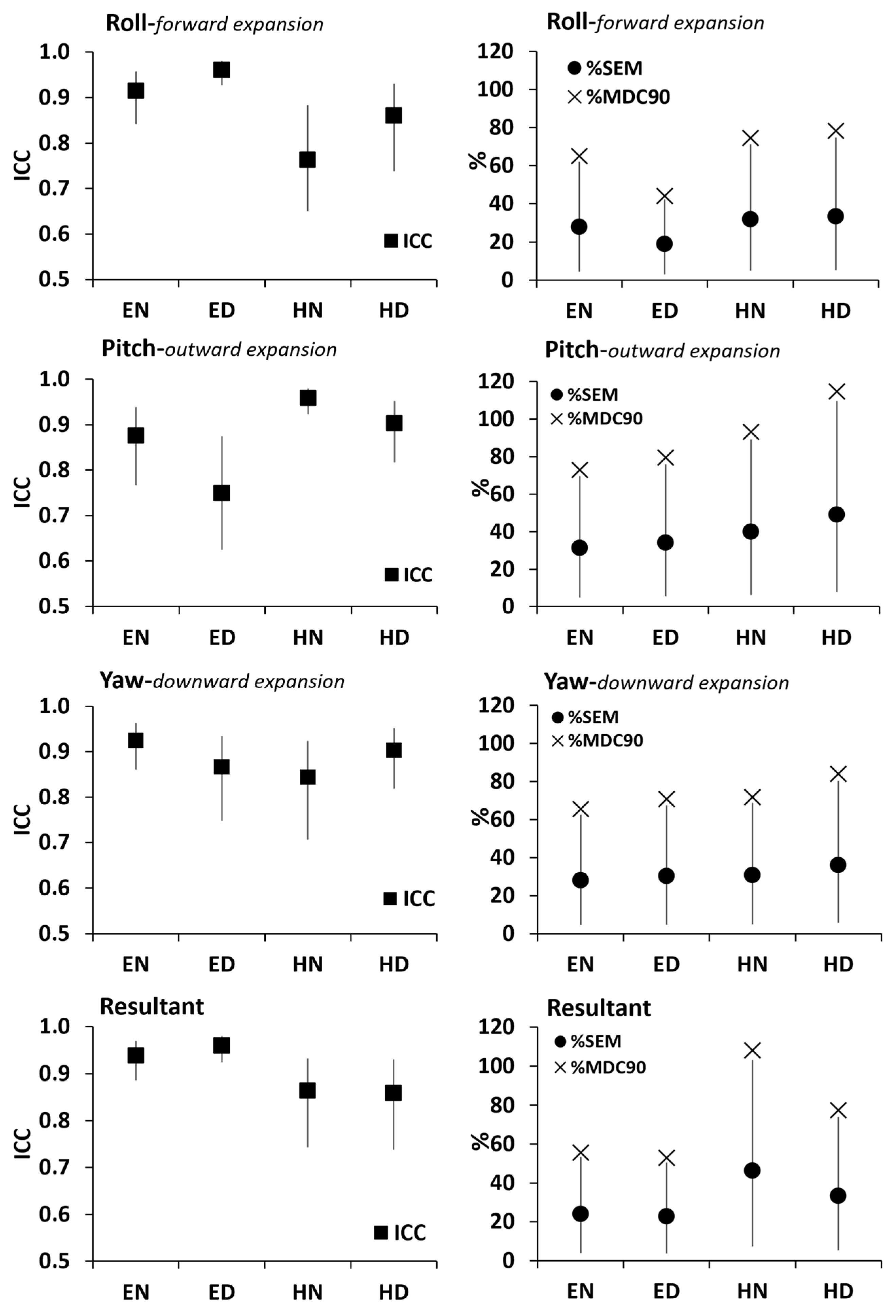
3.5. Relative Reliability–Intraclass Correlation Coefficient (ICC) of AD Path
3.6. Standard Error of Measurement and Minimal Detectable Change in AD Path
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| F | Significance p Value | Partial Eta Squared | Cohen’s d Effect Size | Observed Power | ||
|---|---|---|---|---|---|---|
| Body Stance Main Effect | ||||||
| AD path length | Roll | 21.60 | 0.000 * | 0.444 | 1.79 | 0.99 |
| Pich | 23.82 | 0.000 * | 0.469 | 1.88 | 1.00 | |
| Yaw | 14.35 | 0.001 * | 0.347 | 1.46 | 0.95 | |
| Resultant | 22.52 | 0.000 * | 0.455 | 1.83 | 1.00 | |
| %CVind | Roll | 3.75 | 0.063 ns | 0.122 | 0.75 | 0.46 |
| Pich | 2.88 | 0.101 ns | 0.097 | 0.65 | 0.37 | |
| Yaw | 1.48 | 0.234 ns | 0.052 | 0.47 | 0.22 | |
| Resultant | 4.76 | 0.038 ns | 0.150 | 0.84 | 0.56 | |
| Breathing Type Main Effect | ||||||
| AD path length | Roll | 39.70 | 0.000 * | 0.595 | 2.43 | 1.00 |
| Pich | 64.23 | 0.000 * | 0.704 | 3.09 | 1.00 | |
| Yaw | 15.70 | 0.000 * | 0.368 | 1.53 | 0.97 | |
| Resultant | 35.75 | 0.000 * | 0.570 | 2.30 | 1.00 | |
| %CVind | Roll | 0.49 | 0.489 ns | 0.018 | 0.27 | 0.10 |
| Pich | 1.63 | 0.212 ns | 0.057 | 0.49 | 0.23 | |
| Yaw | 0.82 | 0.374 ns | 0.029 | 0.35 | 0.14 | |
| Resultant | 0.33 | 0.571 ns | 0.012 | 0.22 | 0.09 | |
| Body Stance * Breathing Type Interaction | ||||||
| AD path length | Roll | 0.10 | 0.754 ns | 0.004 | 0.12 | 0.06 |
| Pich | 0.85 | 0.364 ns | 0.031 | 0.36 | 0.15 | |
| Yaw | 0.72 | 0.404 ns | 0.026 | 0.33 | 0.13 | |
| Resultant | 0.12 | 0.734 ns | 0.004 | 0.13 | 0.06 | |
| %CVind | Roll | 1.22 | 0.279 ns | 0.043 | 0.43 | 0.19 |
| Pich | 0.51 | 0.483 ns | 0.018 | 0.27 | 0.11 | |
| Yaw | 0.22 | 0.640 ns | 0.008 | 0.18 | 0.07 | |
| Resultant | 5.74 | 0.024 ns | 0.175 | 0.92 | 0.64 | |
| F | Significance p Value | Partial Eta Squared | Cohen’s d Effect Size | Observed Power | |
|---|---|---|---|---|---|
| Roll | 6.83 | 0.014 * | 0.202 | 1.00 | 0.71 |
| Pitch | 9.18 | 0.005 * | 0.254 | 1.17 | 0.83 |
| Yaw | 4.50 | 0.043 * | 0.143 | 0.82 | 0.53 |
| Resultant | 9.50 | 0.005 * | 0.259 | 1.18 | 0.84 |
References
- Liu, H.; Xu, Q.; Xiang, X.; Liu, D.; Si, S.; Wang, L.; Lv, Y.; Liao, Y.; Yang, H. Case report: Passive handstand promotes cerebrovascular elasticity training and helps delay the signs of aging: A 40-year follow-up investigation. Front. Med. 2022, 9, 752076. [Google Scholar] [CrossRef] [PubMed]
- Manjunath, N.K.; Telles, S. Effects of sirsasana (headstand) practice on autonomic and respiratory variables. Indian J. Physiol. Pharmacol. 2003, 47, 34–42. Available online: https://ijpp.com/IJPP%20archives/2003_47_1/vol47_no1_orgn_artcl_2.htm (accessed on 10 August 2023). [PubMed]
- Rao, S. Metabolic cost of head-stand posture. J. Appl. Physiol. 1962, 17, 117–118. [Google Scholar] [CrossRef] [PubMed]
- Rao, S. Cardiovascular responses to head-stand posture. J. Appl. Physiol. 1963, 18, 987–990. [Google Scholar] [CrossRef] [PubMed]
- Rao, S. Respiratory responses to headstand posture. J. Appl. Physiol. 1968, 24, 697–699. [Google Scholar] [CrossRef] [PubMed]
- LeMarr, J.D.; Golding, A.L.; Kevin, D.; Crehan, K.D. Cardiorespiratory responses to inversion. Phys. Sportsmed. 1983, 11, 51–57. [Google Scholar] [CrossRef] [PubMed]
- Iyengar, B.K. Light on Yoga; Schocken Books: New York, NY, USA, 1966. [Google Scholar]
- Ma, X.; Yue, Z.-Q.; Gong, Z.-Q.; Zhang, H.; Duan, N.-Y.; Shi, Y.-T.; Wei, G.-X.; Li, Y.-F. The effect of diaphragmatic breathing on attention, negative affect and stress in healthy adults. Front. Psychol. 2017, 8, 234806. [Google Scholar] [CrossRef] [PubMed]
- Martarelli, D.; Cocchioni, M.; Scuri, S.; Pompei, P. Diaphragmatic breathing reduces exercise-induced oxidative stress. Evid. Based. Complement. Altern. Med. 2011, 2011, 932430. [Google Scholar] [CrossRef]
- De Troyer, A.; Estenne, M. Functional anatomy of the respiratory muscles. Clin. Chest Med. 1988, 9, 175–193. [Google Scholar] [CrossRef]
- Hodges, P.W.; Gandevia, S.C. Activation of the human diaphragm during a repetitive postural task. J. Physiol. 2000, 522, 165–175. [Google Scholar] [CrossRef]
- Fogarty, M.J.; Mantilla, C.B.; Sieck, G.C. Breathing: Motor Control of Diaphragm Muscle. Physiol 2018, 33, 113–126. [Google Scholar] [CrossRef] [PubMed]
- Agostoni, E.; Hyatt, R.E. Static behavior of the respiratory system. In Comprehensive Physiology, Supplement 12 Handbook of Physiology, the Respiratory System, Mechanics of Breathing; Maclem, P.T., Mead, J., Eds.; American Physiological Society: Bethesda, MD, USA, 1986; pp. 113–130. [Google Scholar] [CrossRef]
- Foskolou, A.; Emmanouil, A.; Boudolos, K.; Rousanoglou, E. Abdominal breathing effect on postural stability and the respiratory muscles’ activation during body stances used in fitness modalities. Biomechanics 2022, 2, 478–493. [Google Scholar] [CrossRef]
- Perry, S.F.; Similowski, T.; Klein, W.; Codd, J.R. The evolutionary origin of the mammalian diaphragm. Respir. Physiol. Neurobiol. 2010, 171, 1–16. [Google Scholar] [CrossRef] [PubMed]
- Bates, A.; Ling, M.; Mann, J.; Arvind, D.K. Respiratory rate and flow waveform estimation from tri-axial accelerometer data. In Proceedings of the 2010 International Conference on Body Sensor Networks, Singapore, 7–9 June 2010; IEEE Computer Society: Singapore, 2010; pp. 144–150. [Google Scholar] [CrossRef]
- Beck, S.; Laufer, B.; Krueger-Ziolek, S.; Moeller, K. Measurement of respiratory rate with inertial measurement units. Curr. Dir. Biomed. Eng. 2020, 6, 237–240. [Google Scholar] [CrossRef]
- Erfianto, B.; Rizal, A. IMU-based respiratory signal processing using cascade complementary filter. J. Sens. 2022, 2022, 7987159. [Google Scholar] [CrossRef]
- Hung, P.D.; Bonnet, S.; Guillemaud, R.; Castelli, E.; Yen, P.T.N. Estimation of respiratory waveform using an accelerometer. In Proceedings of the 5th IEEE International Symposium on Biomedical Imaging: From Nano to Macro, Paris, France, 14–17 May 2008; pp. 1493–1496. Available online: https://ieeexplore.ieee.org/document/4541291 (accessed on 10 August 2023).
- Karacocuk, G.; Höflinger, F.; Zhang, R.; Reindl, L.M.; Laufer, B.; Möller, K.; Röell, M.; Zdzieblik, D. Inertial sensor-based respiration analysis. IEEE Trans. Instrum. Meas. 2019, 68, 4268–4275. [Google Scholar] [CrossRef]
- Siqueira, A.; Spirandeli, F.; Moraes, R.; Zarzoso, V. Respiratory waveform estimation from multiple accelerometers: An optimal sensor number and placement analysis. IEEE J. Biomed. Health Inform. 2018, 23, 1507–1515. [Google Scholar] [CrossRef]
- Gaidhani, A.; Moon, K.S.; Ozturk, Y.; Lee, S.Q.; Youm, W. Extraction and analysis of respiratory motion using wearable inertial sensor system during trunk motion. Sensors 2017, 17, 2932. [Google Scholar] [CrossRef]
- Hughes, S.; Liu, H.; Zheng, D. Influences of sensor placement site and subject posture on measurement of respiratory frequency using triaxial accelerometers. Front Physiol. 2020, 11, 823. [Google Scholar] [CrossRef]
- Chu, M.; Nguyen, T.; Pandey, V.; Zhou, Y.; Pham, H.N.; Bar-Yoseph, R.; Radom-Aizik, S.; Jain, R.; Cooper, D.M.; Khine, M. Respiration rate and volume measurements using wearable strain sensors. NPJ Digit. Med. 2019, 2, 8. [Google Scholar] [CrossRef]
- Presti, D.L.; Massaroni, C.; Caponero, M.; Formica, D.; Schena, E. Cardiorespiratory monitoring using a mechanical and an optical system. In Proceedings of the IEEE International Symposium on Medical Measurements and Applications (MeMeA), Lausanne, Switzerland, 23–25 June 2021; pp. 1–6. [Google Scholar] [CrossRef]
- Lee, H.-Y.; Cheon, S.-H.; Yong, M.-S. Effect of diaphragm breathing exercise applied on the basis of overload principle. J. Phys. Ther. Sci. 2017, 29, 1054–1056. [Google Scholar] [CrossRef] [PubMed]
- Boiko, A.; Gaiduk, M.; Scherz, W.D.; Gentili, A.; Conti, M.; Orcioni, S.; Martínez Madrid, N.; Seepold, R. Monitoring of cardiorespiratory parameters during sleep using a special holder for the accelerometer sensor. Sensors 2023, 23, 5351. [Google Scholar] [CrossRef] [PubMed]
- Phan, D.H.; Bonnet, S.; Guillemaud, R.; Castelli, E.; Pham Thi, N.Y. Estimation of respiratory waveform and heart rate using an accelerometer. In Proceedings of the 30th Annual International Conference of the IEEE Engineering in Medicine and Biology Society, Vancouver, BC, Canada, 20–25 August 2008; pp. 4916–4919. [Google Scholar] [CrossRef]
- Droitcour, A.D.; Boric-Lubecke, O.; Kovacs, G.T.A. Signal-to-noise ratio in doppler radar system for heart and respiratory rate measurements. IEEE Trans. Microw. Theory Tech. 2009, 57, 2498–2507. [Google Scholar] [CrossRef]
- Heinz, C.; Reiner, M.; Belka, C.; Walter, F.; Söhn, M. Technical evaluation of different respiratory monitoring systems used for 4D CT acquisition under free breathing. J. Appl. Clin. Med. Phys. 2015, 16, 334–349. [Google Scholar] [CrossRef] [PubMed]
- Corbishley, P.; Rodriguez-Villegas, E. Breathing detection: Towards a miniaturized, wearable, battery-operated monitoring system. IEEE. Trans. Biomed. Eng. 2008, 55, 196–204. [Google Scholar] [CrossRef] [PubMed]
- Beaton, D.E.; Bombardier, C.; Katz, J.N.; Wright, J.G. A taxonomy for responsiveness. J. Clin. Epidemiol. 2001, 54, 1204–1217. [Google Scholar] [CrossRef] [PubMed]
- Dontje, M.L.; Dall, P.M.; Skelton, D.A.; Gill, J.M.R.; Chastin, S.F.M.; Seniors USP Team. Reliability, minimal detectable change and responsiveness to change: Indicators to select the best method to measure sedentary behaviour in older adults in different study designs. PLoS ONE 2018, 13, e0195424. [Google Scholar] [CrossRef] [PubMed]
- Derrick, T.R.; Thomas, J.M. Time-series analysis: The cross-correlation function. In Innovative Analyses of Human Movement, 1st ed.; Stergiou, N., Ed.; Human Kinetics Publishers: Champaign, IL, USA, 2004; pp. 189–205. [Google Scholar]
- McGraw, K.O.; Wong, S.P. Forming inferences about some intraclass correlation coefficients. Psychol. Methods 1996, 1, 30–46. [Google Scholar] [CrossRef]
- Pinsault, N.; Vuillerme, N. Test-retest reliability of centre of foot pressure measures to assess postural control during unperturbed stance. Med. Eng. Phys. 2009, 31, 276–286. [Google Scholar] [CrossRef]
- Fleiss, J.L. Reliability of measurement. In The Design and Analysis of Clinical Experiments; Fleiss, J.L., Ed.; Wiley: New York, NY, USA, 1986; pp. 1–32. [Google Scholar]
- Weir, J.P. Quantifying test-retest reliability using the intraclass correlation coefficient and the SEM. J. Strength Cond. Res. 2005, 19, 231–240. [Google Scholar] [CrossRef]
- Campos, M.H.; Giraldi, N.M.; Gentil, P.; de Lira, C.A.; Vieira, C.A.; de Paula, M.C. The geometric curvature of the spine during the sirshasana, the yoga’s headstand. J. Sports Sci. 2017, 35, 1134–1141. [Google Scholar] [CrossRef]
- Hopkins, W.G. Measures of reliability in sports medicine and science. Sports Med. 2000, 30, 1–15. [Google Scholar] [CrossRef]
- Furlan, L.; Sterr, A. The applicability of standard error of measurement and minimal detectable change to motor learning research-A behavioral study. Front. Hum. Neurosci. 2018, 12, 95. [Google Scholar] [CrossRef] [PubMed]
- Atkinson, G.; Nevill, A.M. Statistical methods for assessing measurement error (reliability) in variables relevant to sports medicine. Sports Med. 1998, 26, 217–238. [Google Scholar] [CrossRef]
- Jaworski, J.; Ambroży, T.; Lech, G.; Spieszny, M.; Bujas, P.; Żak, M.; ChwaŁa, W. Absolute and relative reliability of several measures of static postural stability calculated using a GYKO inertial sensor system. Acta Bioeng. Biomech. 2020, 22, 94–99. [Google Scholar] [CrossRef] [PubMed]
- Pooranawatthanakul, K.; Siriphorn, A. Comparisons of the validity and reliability of two smartphone placements for balance assessment using an accelerometer based application. Eur. J. Physiother. 2020, 22, 236–242. [Google Scholar] [CrossRef]
- Konno, K.; Mead, J. Measurement of the separate volume changes of rib cage and abdomen during breathing. J. Appl. Physiol. 1967, 22, 407–422. [Google Scholar] [CrossRef] [PubMed]
- LoMauro, A.; Aliverti, A. Sex differences in respiratory function. Breathe 2018, 14, 131–140. [Google Scholar] [CrossRef]
- Lakens, D. Calculating and reporting effect sizes to facilitate cumulative science: A practical primer for t-tests and ANOVAs. Front Psychol. 2013, 4, 863. [Google Scholar] [CrossRef]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences, 2nd ed.; Lawrence Erlbaum Associates Inc.: Mahwah, NJ, USA, 1988; pp. 24–27. [Google Scholar] [CrossRef]

| a/a | Gender | Age (y) | Body Mass (kg) | Body Height (m) | Body Mass Index (kg/m2) | * BMI Classification | Headstand History Experience | Headstand Practice Experience | Diaphragmatic Breathing Experience |
|---|---|---|---|---|---|---|---|---|---|
| S01 | F | 26 | 63.0 | 1.61 | 24.3 | Normal | 1–2 years | Personal Practice | <6 months |
| S02 | F | 25 | 57.5 | 1.68 | 20.4 | Normal | >8 years | Artistic Gymnastics | <1 year |
| S03 | M | 29 | 79.0 | 1.78 | 24.9 | Normal | >8 years | Artistic Gymnastics | <6 months |
| S04 | F | 21 | 55.0 | 1.60 | 21.5 | Normal | 5–7 years | Artistic Gymnastics | <6 months |
| S05 | F | 25 | 51.0 | 1.67 | 18.3 | Underweight | 5–7 years | Artistic Swimming | <1 year |
| S06 | M | 27 | 80.7 | 1.80 | 24.9 | Normal | <1 years | Personal Practice | <6 months |
| S07 | M | 34 | 68.3 | 1.67 | 24.5 | Normal | >8 years | Artistic Gymnastics | <6 months |
| S08 | F | 33 | 52.0 | 1.58 | 20.8 | Normal | 1–2 years | Yoga | 2–4 years |
| S09 | M | 41 | 72.0 | 1.82 | 21.7 | Normal | 2–4 years | Yoga | >8 years |
| S10 | F | 21 | 54.0 | 1.67 | 19.4 | Normal | 1–2 years | Yoga | 1–2 years |
| S11 | F | 37 | 64.0 | 1.67 | 22.9 | Normal | >8 years | Yoga | >8 years |
| S12 | F | 22 | 72.5 | 1.72 | 24.5 | Normal | >8 years | Rhythmic Gymnastics | <6 months |
| S13 | F | 18 | 60.0 | 1.60 | 23.4 | Normal | 2–4 years | Yoga | 2–4 years |
| S14 | M | 51 | 64.0 | 1.80 | 19.8 | Normal | 5–4 years | Yoga | 5–7 years |
| S15 | F | 22 | 65.0 | 1.70 | 22.5 | Normal | <1 years | Yoga | <1 year |
| S16 | F | 20 | 63.0 | 1.73 | 21.0 | Normal | 2–4 years | Yoga | 2–4 years |
| S17 | F | 20 | 54.0 | 1.64 | 20.1 | Normal | 2–4 years | Rhythmic Gymnastics | <6 months |
| S18 | F | 19 | 67.0 | 1.69 | 23.5 | Normal | >8 years | Rhythmic Gymnastics | <6 months |
| S19 | F | 19 | 62.0 | 1.72 | 21.0 | Normal | 5–7 years | Artistic Gymnastics | <6 months |
| S20 | M | 33 | 72.0 | 1.70 | 24.9 | Normal | 5–7 years | Yoga | >8 years |
| S21 | F | 18 | 66.0 | 1.79 | 20.6 | Normal | >8 years | Artistic Gymnastics | <6 months |
| S22 | F | 20 | 68.0 | 1.78 | 21.5 | Normal | >8 years | Rhythmic Gymnastics | 2–4 years |
| S23 | F | 20 | 49.5 | 1.59 | 19.6 | Normal | 2–4 years | Artistic Gymnastics | <6 months |
| S24 | M | 26 | 55.0 | 1.53 | 23.5 | Normal | >8 years | Artistic Gymnastics | >8 years |
| S25 | F | 18 | 57.0 | 1.62 | 21.7 | Normal | 2–4 years | Breakdance | <6 months |
| S26 | F | 23 | 49.7 | 1.64 | 18.5 | Underweight | >8 years | Artistic Gymnastics | <6 months |
| S27 | F | 22 | 58.4 | 1.65 | 21.5 | Normal | >8 years | Artistic Gymnastics | <6 months |
| S28 | M | 20 | 76.5 | 1.80 | 23.6 | Normal | 5–7 years | Personal Practice | <6 months |
| Filtering Condition | Experimental Condition | Signal to Noise Ratio (dB) | |||
|---|---|---|---|---|---|
| Roll | Pitch | Yaw | Resultant | ||
| Pre-Filtering | EN | 13 | 14 | 10 | 12 |
| ED | 19 | 18 | 19 | 16 | |
| HN | 6 | 6 | 5 | 6 | |
| HD | 7 | 6 | 7 | 6 | |
| Post-Filtering | ED | 93 | 110 | 101 | 96 |
| HN | 47 | 41 | 38 | 36 | |
| HD | 44 | 39 | 44 | 37 | |
| EN | 79 | 81 | 69 | 64 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rousanoglou, E.; Foskolou, A.; Emmanouil, A.; Boudolos, K. Inertial Sensing of the Abdominal Wall Kinematics during Diaphragmatic Breathing in Head Standing. Biomechanics 2024, 4, 63-83. https://doi.org/10.3390/biomechanics4010005
Rousanoglou E, Foskolou A, Emmanouil A, Boudolos K. Inertial Sensing of the Abdominal Wall Kinematics during Diaphragmatic Breathing in Head Standing. Biomechanics. 2024; 4(1):63-83. https://doi.org/10.3390/biomechanics4010005
Chicago/Turabian StyleRousanoglou, Elissavet, Apostolina Foskolou, Analina Emmanouil, and Konstantinos Boudolos. 2024. "Inertial Sensing of the Abdominal Wall Kinematics during Diaphragmatic Breathing in Head Standing" Biomechanics 4, no. 1: 63-83. https://doi.org/10.3390/biomechanics4010005
APA StyleRousanoglou, E., Foskolou, A., Emmanouil, A., & Boudolos, K. (2024). Inertial Sensing of the Abdominal Wall Kinematics during Diaphragmatic Breathing in Head Standing. Biomechanics, 4(1), 63-83. https://doi.org/10.3390/biomechanics4010005