
Self-Inflicted Foreign Bodies in the Lower Urinary Tract Associated with Sexual Activities—A Case Series

 , , , ,
, , , ,
Abstract
1. Introduction
2. Materials and Methods
3. Results
3.1. Case Overview
3.2. Results Summary
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| KUB | kidney, ureter, and bladder |
| UTI | urinary tract infection |
| LUTS | lower urinary tract symptoms |
| SUR | acute urinary retention |
References
- Angulo-Lozano, J.C.; Gonzaga-Carlos, N.; Virgen-Rivera, M.F.; Sanchez-Musi, L.F.; Acosta-Falomir, M.J.; De la Cruz-Galvan, R.; Toro, I.A.C.-D.; Maga, J.E.; Virgen-Gutierrez, F.; Gastelum, J.L. Should Psychiatry Be Consulted When Facing a Self-Inflicted Foreign Bo dy in the Urinary Tract? Cureus 2022, 14, e23400. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Z.; Zhu, X.; Wang, Y.; Chen, D.; Fan, J.; Deng, C.; Liu, G.; Yang, L.; Feloney, M.; Wang, X.; et al. Sexual dysfunction associated with chronic retention of foreign bodies in the low urinary tract. Andrologia 2021, 54, e14346. [Google Scholar] [CrossRef]
- Tuncer, H.; Karacam, H.; Cam, B.; Huber, H. A Self-Inserted Foreign Body in the Urinary Bladder and Urethra. Cureus 2021, 13, e16322. [Google Scholar] [CrossRef]
- Boyle, A.; Martinez, D.R.; Mennie, P.A.; Rafiei, A.; Carrion, R. The time-less urologic question, “Now why would you do that?” A case series and literature review of self-inserted urethral foreign bodies. J. Clin. Urol. 2013, 7, 165–169. [Google Scholar] [CrossRef]
- Oh, C.; Noll, D.; John, A.; Hong, M. Genitourethral foreign bodies: 20-year experience and outcomes from a single center. Asian J. Androl. 2024, 27, 185–188. [Google Scholar] [CrossRef]
- Palmer, C.J.; Houlihan, M.; Psutka, S.P.; Ellis, K.A.; Vidal, P.; Hollowell, C.M.P. Urethral Foreign Bodies: Clinical Presentation and Management. Urology 2016, 97, 257–260. [Google Scholar] [CrossRef] [PubMed]
- Reztsova, M.; Chien, K.S.; Post, K.T.; Canales, A.; Yokota, S. Bladder perforation as a rare complication of urethra sounding with a blunt marking pen. J. Surg. Case Rep. 2023, 2023, rjad032. [Google Scholar] [CrossRef] [PubMed]
- Elawdy, M.; El-Halwagy, S.; Mousa, E.; Maliakal, J. Self-insertion of an odd urethral foreign body that led to fournier’s gangrene. Urol. Ann. 2019, 11, 320. [Google Scholar] [CrossRef]
- Fatahajjad, H.H.; Ompusunggu, R.A.; Laksita, T.B.; Soebadi, M.A. Multiple lower urinary tract calculi induced by foreign bodies inserti on: A case report. Radiol. Case Rep. 2024, 19, 2443–2447. [Google Scholar] [CrossRef]
- Ahmed, M.M.; Ahmed, N.A.; Sharma, V. A Self Inserted Unusual Foreign Body “An Entire Pencil” in a Male Uret hra and Bladder: A Case Report. Cureus 2022, 14, e25198. [Google Scholar] [CrossRef]
- Naidu, K.; Chung, A.; Mulcahy, M. An unusual urethral foreign body. Int. J. Surg. Case Rep. 2013, 4, 1052–1054. [Google Scholar] [CrossRef] [PubMed]
- Saputra, H.M.; Kloping, Y.P.; Renaldo, J.; Hakim, L. An earphone wire inside the urinary bladder: A case report and compreh ensive literature review of genitourinary polyembolokoilamania. Radiol. Case Rep. 2022, 17, 1457–1463. [Google Scholar] [CrossRef] [PubMed]
- Simangunsong, A.I.; Pramod, S.V. Intravesical foreign object: A case report of autoerotism. Int. J. Surg. Case Rep. 2020, 77, 515–518. [Google Scholar] [CrossRef] [PubMed]
- Gite, V.; Nikose, J.; Agrawal, M.; Sankapal, P. Self-inflicted urethral and vesical foreign bodies—Case report. Arch. Int. Surg. 2020, 10, 66. [Google Scholar] [CrossRef]
- Velten, J.; Margraf, J. Satisfaction guaranteed? How individual, partner, and relationship factors impact sexual satisfaction within partnerships. PLoS ONE 2017, 12, e0172855. [Google Scholar] [CrossRef]
- Rowland, D.; McMahon, C.G.; Abdo, C.; Chen, J.; Jannini, E.; Waldinger, M.D.; Ahn, T.Y. Disorders of Orgasm and Ejaculation in Men. J. Sex. Med. 2010, 7, 1668–1686. [Google Scholar] [CrossRef]
- Montorsi, F.; Adaikan, G.; Becher, E.; Giuliano, F.; Khoury, S.; Lue, T.F.; Christ, G.; Hatzichristou, D.; Hirsch, M.; Kimoto, Y.; et al. Summary of the recommendations on sexual dysfunctions in men. J. Sex. Med. 2010, 7, 3572–3588. [Google Scholar] [CrossRef]
- McCabe, M.P.; Sharlip, I.D.; Atalla, E.; Balon, R.; Fisher, A.D.; Laumann, E.; Lee, S.W.; Lewis, R.; Segraves, R.T. Definitions of Sexual Dysfunctions in Women and Men: A Consensus Statement from the Fourth International Consultation on Sexual Medicine 2015. J. Sex. Med. 2016, 13, 135–143. [Google Scholar] [CrossRef]
- Alwaal, A.; Breyer, B.N.; Lue, T.F. Normal male sexual function: Emphasis on orgasm and ejaculation. Fertil. Steril. 2015, 104, 1051–1060. [Google Scholar] [CrossRef]
- Brijawi, O.; Hartman, E.; Wright, S.; Schneegurt, N.R. Batteries Included: A Case of Multiple Self-Inflicted Foreign Bodies i n the Lower Genitourinary Tract. Cureus 2024, 16, e73048. [Google Scholar] [CrossRef]
- Zeng, S.X.; Li, H.Z.; Zhang, Z.S.; Lu, X.; Yu, X.W.; Yang, Q.S.; Ma, C.; Xu, C.L.; Sun, Y.H. Removal of Numerous Vesical Magnetic Beads with a Self-Made Magnetic S heath. J. Sex. Med. 2015, 12, 567–571. [Google Scholar] [CrossRef] [PubMed]
- Rahman, M.; Bari, A.K.M.A.; Khatoon, S.N. An Unusual Self-Inflicted Foreign Body in the Urinary Bladder and Uret hra: A Case Report. Bangladesh J. Urol. 2020, 18, 94–97. [Google Scholar] [CrossRef]
- Porav-Hodade, D.; Gherasim, R.; Todea-Moga, C.; Reman, T.; Feciche, B.O.; Hunor, K.; Guliciuc, M.; Ilona, M.O.K.; Coman, I.; Crisan, N. Electric Wire in the Urinary Bladder: Surgical Challenges and Comprehe nsive Literature Insights. Diagnostics 2024, 14, 2825. [Google Scholar] [CrossRef]
- Smith, P.M.; Harbias, A.; Robinson, R.; Palmer, A.; Grey, B.R. Isiris: A Novel Method of Removing Foreign Bodies from the Lower Urina ry Tract to Avoid Unnecessary Hospitalization and Anesthesia. J. Endourol. Case Rep. 2016, 2, 144–147. [Google Scholar] [CrossRef]











{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Case No. | Age | Sex | Foreign Body | Localization | Cause | Indwelling Time | Clinical Presentation | Treatment |
|---|---|---|---|---|---|---|---|---|
| (Years) | ||||||||
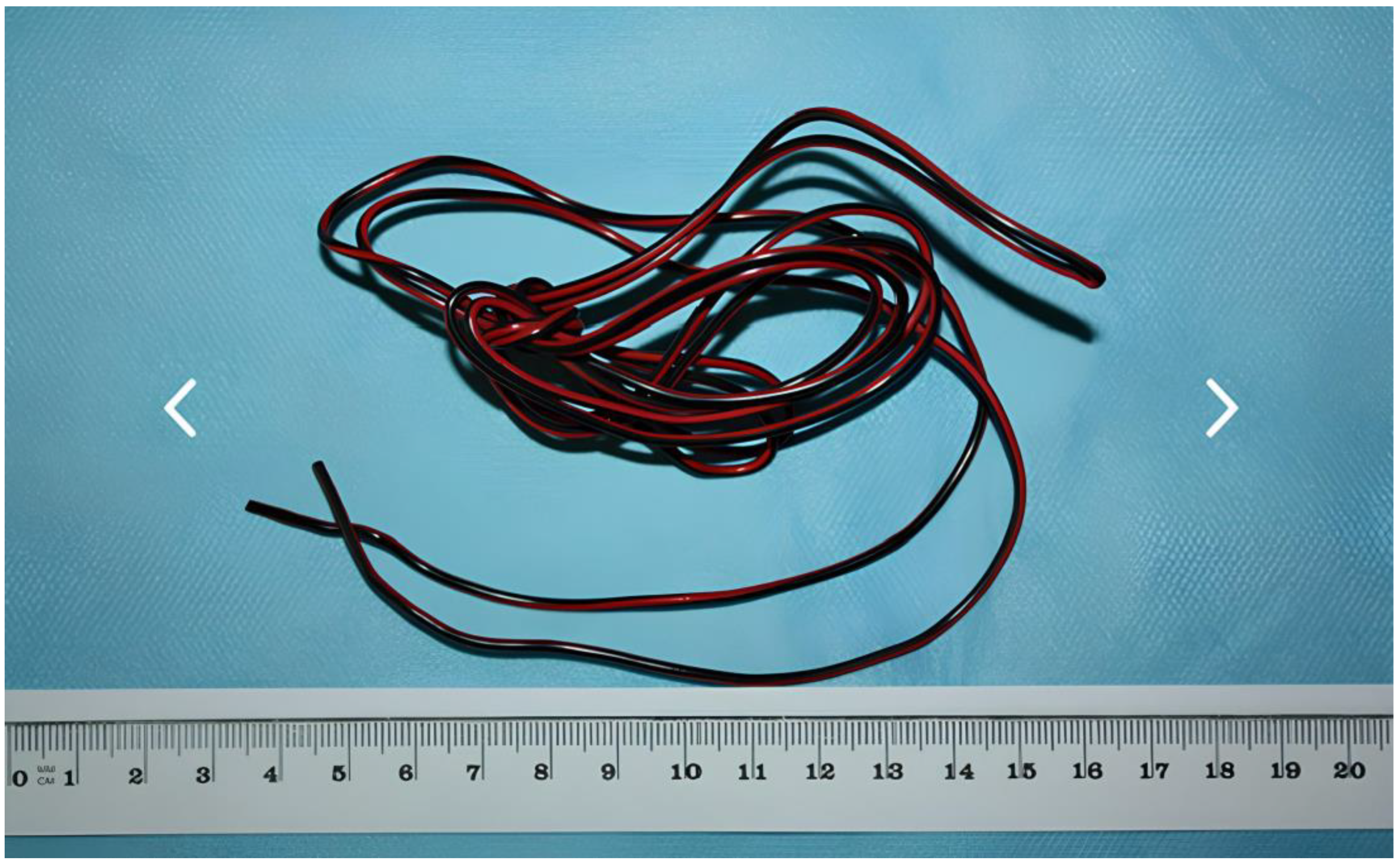
| 1 | 34 | M | wire | urinary bladder | unknown | unknown | hematuria | cystotomy |
| 2 | 25 | F | pencil | urinary bladder | sexual stimulation | 5 weeks | UTI, LUTS | cystoscopy |
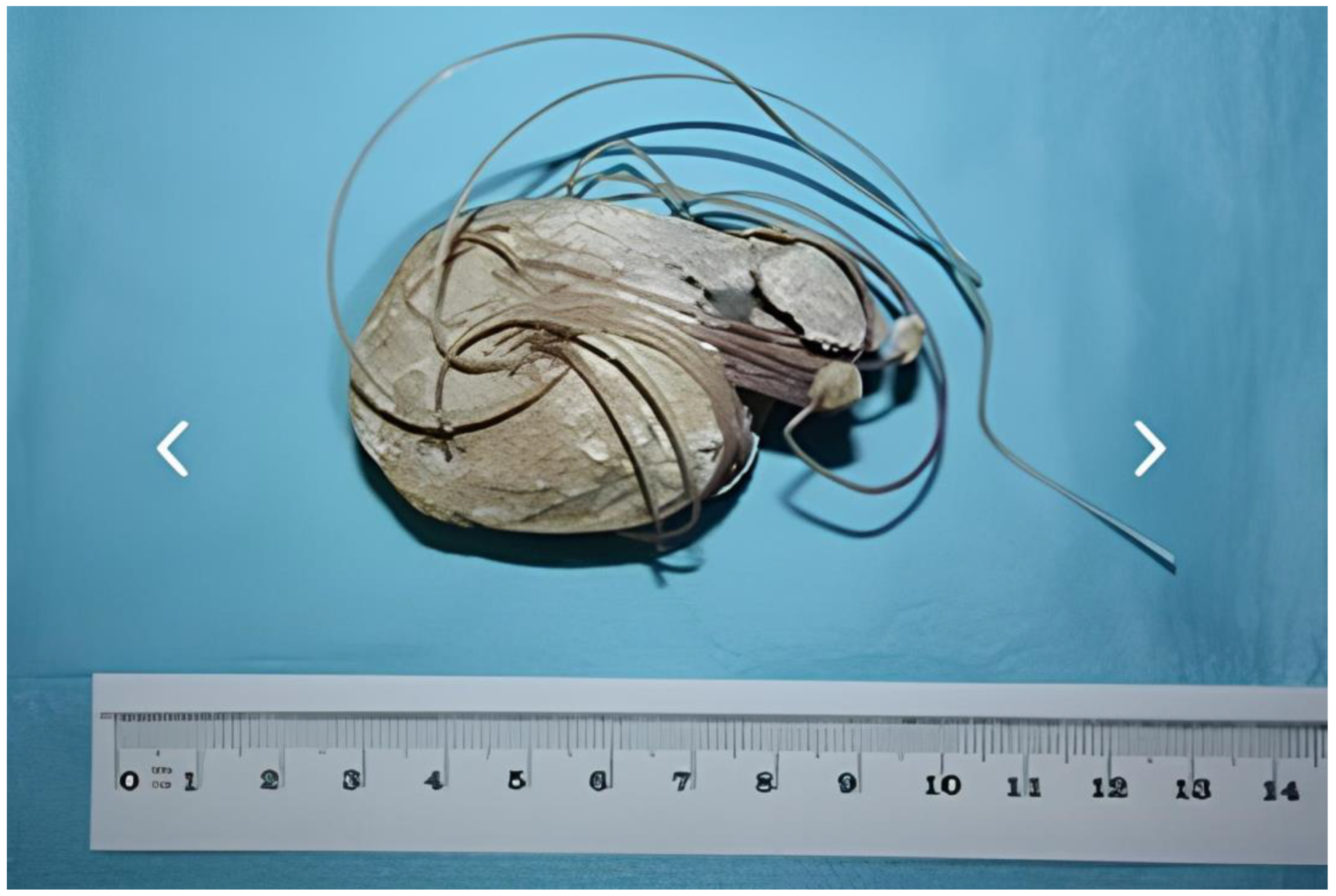
| 3 | 32 | M | string | urinary bladder | alcohol | 3 years | hematuria | cystotomy |
| intoxication | ||||||||
| 4 | 63 | M | hairpin | urinary bladder | sexual stimulation | <24 h | none | cystotomy |
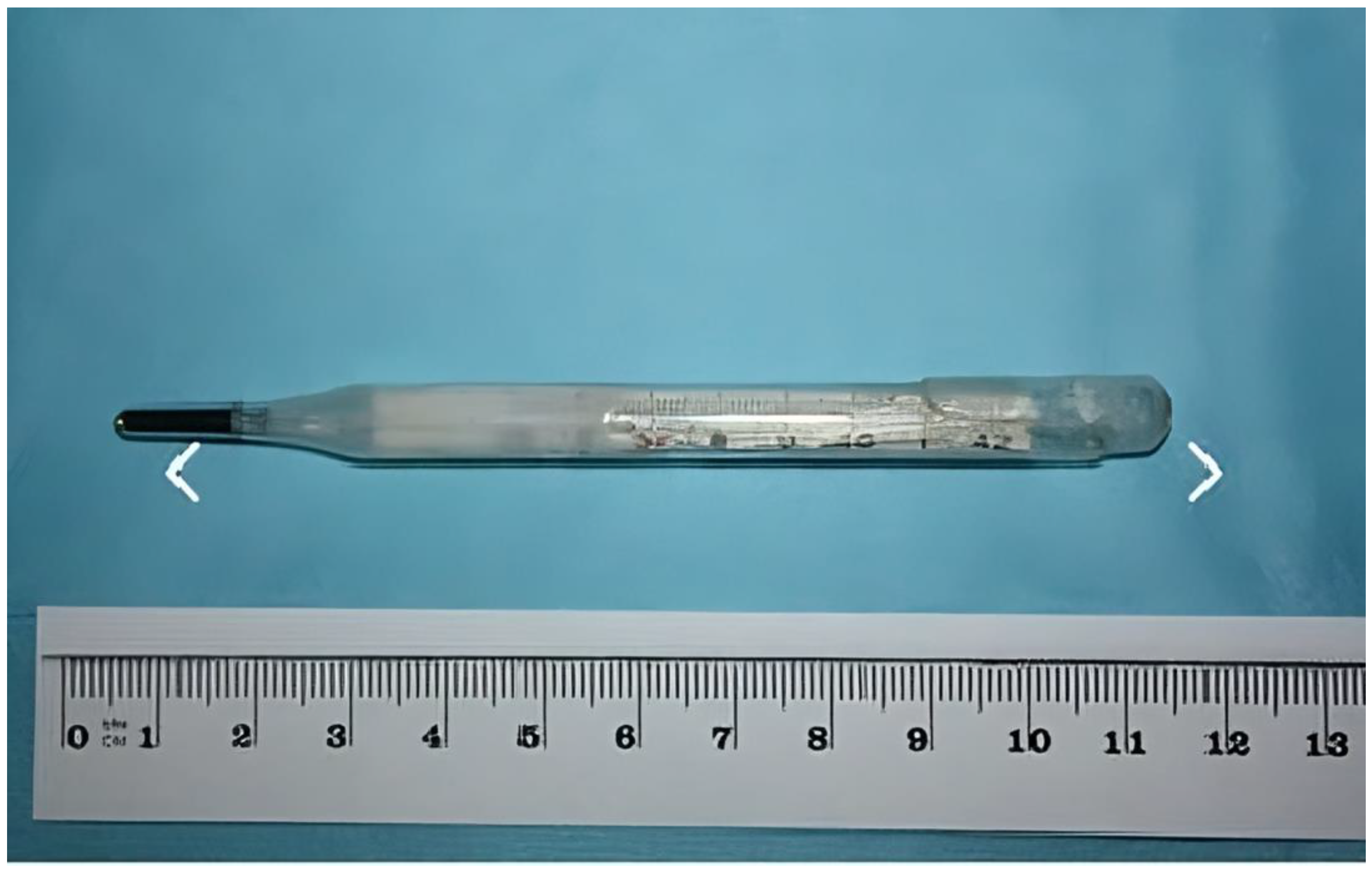
| 5 | 46 | F | thermometer | urinary bladder | alcohol | unknown | none | cystoscopy |
| intoxication | ||||||||
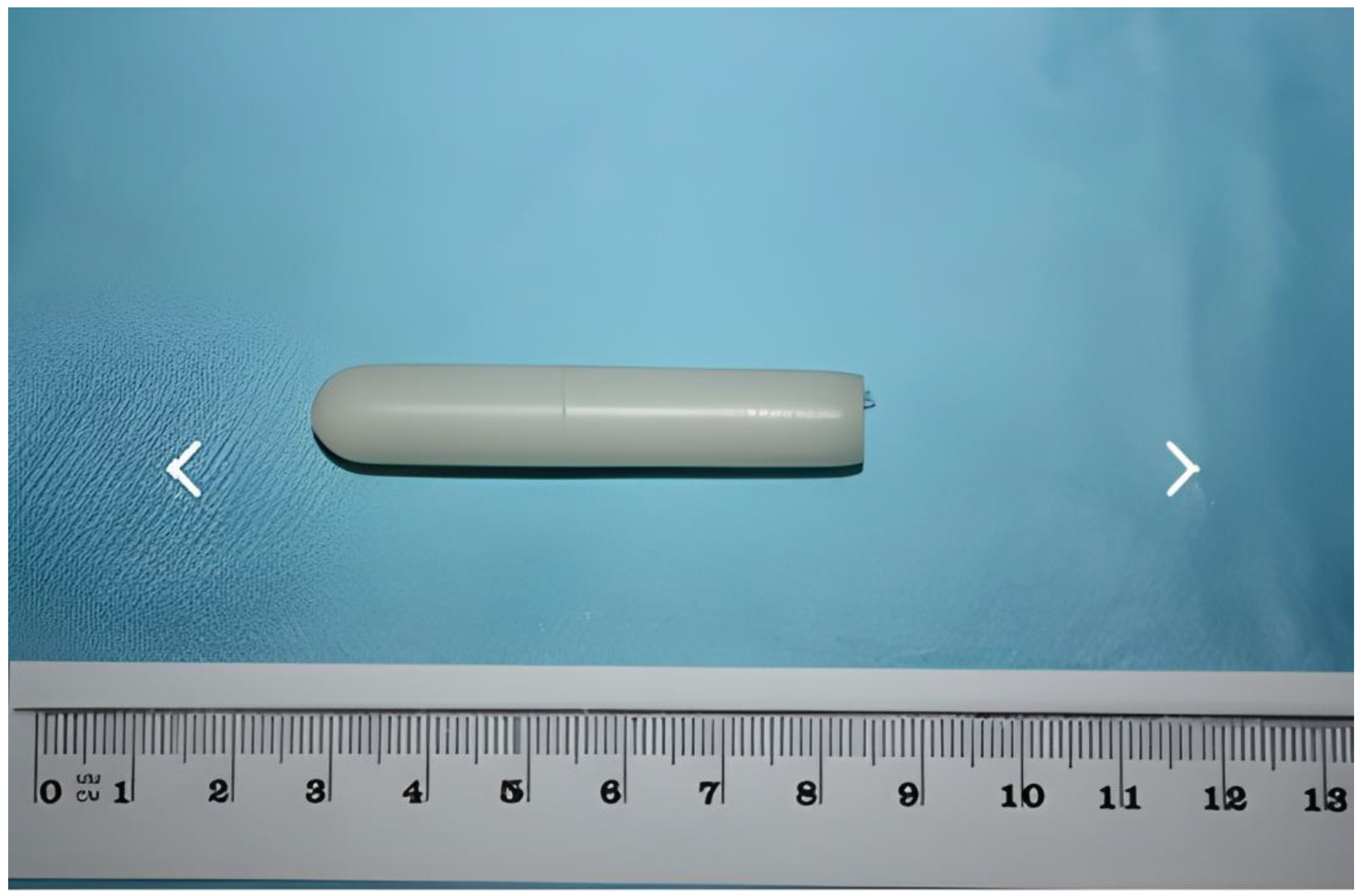
| 6 | 43 | F | plastic | urinary bladder | sexual stimulation | <24 h | none | cystoscopy |
| 7 | 16 | F | pen | urinary bladder | sexual stimulation | 1 year | abdominal pain, pyuria | cystoscopy |
| 8 | 61 | M | pen cartridge | urethra | unknown | unknown | LUTS | cystoscopy |
| 9 | 24 | F | pencil | urinary bladder | unknown | unknown | pyuria | cystotomy |
| 10 | 35 | F | pen | urinary bladder | unknown | unknow | abdominal pain, pyuria | cystotomy |
| 11 | 26 | M | silicone | urethra | alcohol intoxication | 1 week | abdominal pain, dysuria | cystoscopy |
| 12 | 51 | M | silicone | urethra | unknown | <24 h | AUR | cystoscopy |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Godzisz, M.; Kuliniec, I.; Mitura, P.; Młynarczyk, G.; Bar, M.; Płaza, P.; Sudoł, D.; Pogoda, M.; Bar, K. Self-Inflicted Foreign Bodies in the Lower Urinary Tract Associated with Sexual Activities—A Case Series. Sexes 2025, 6, 15. https://doi.org/10.3390/sexes6020015
Godzisz M, Kuliniec I, Mitura P, Młynarczyk G, Bar M, Płaza P, Sudoł D, Pogoda M, Bar K. Self-Inflicted Foreign Bodies in the Lower Urinary Tract Associated with Sexual Activities—A Case Series. Sexes. 2025; 6(2):15. https://doi.org/10.3390/sexes6020015
Chicago/Turabian StyleGodzisz, Michał, Iga Kuliniec, Przemysław Mitura, Grzegorz Młynarczyk, Marek Bar, Paweł Płaza, Damian Sudoł, Marcel Pogoda, and Krzysztof Bar. 2025. "Self-Inflicted Foreign Bodies in the Lower Urinary Tract Associated with Sexual Activities—A Case Series" Sexes 6, no. 2: 15. https://doi.org/10.3390/sexes6020015
APA StyleGodzisz, M., Kuliniec, I., Mitura, P., Młynarczyk, G., Bar, M., Płaza, P., Sudoł, D., Pogoda, M., & Bar, K. (2025). Self-Inflicted Foreign Bodies in the Lower Urinary Tract Associated with Sexual Activities—A Case Series. Sexes, 6(2), 15. https://doi.org/10.3390/sexes6020015