
A Computational Study on Temperature Variations in MRgFUS Treatments Using PRF Thermometry Techniques and Optical Probes

 ,
,  ,
,  and
and 
Abstract
1. Introduction
2. Materials and Methods
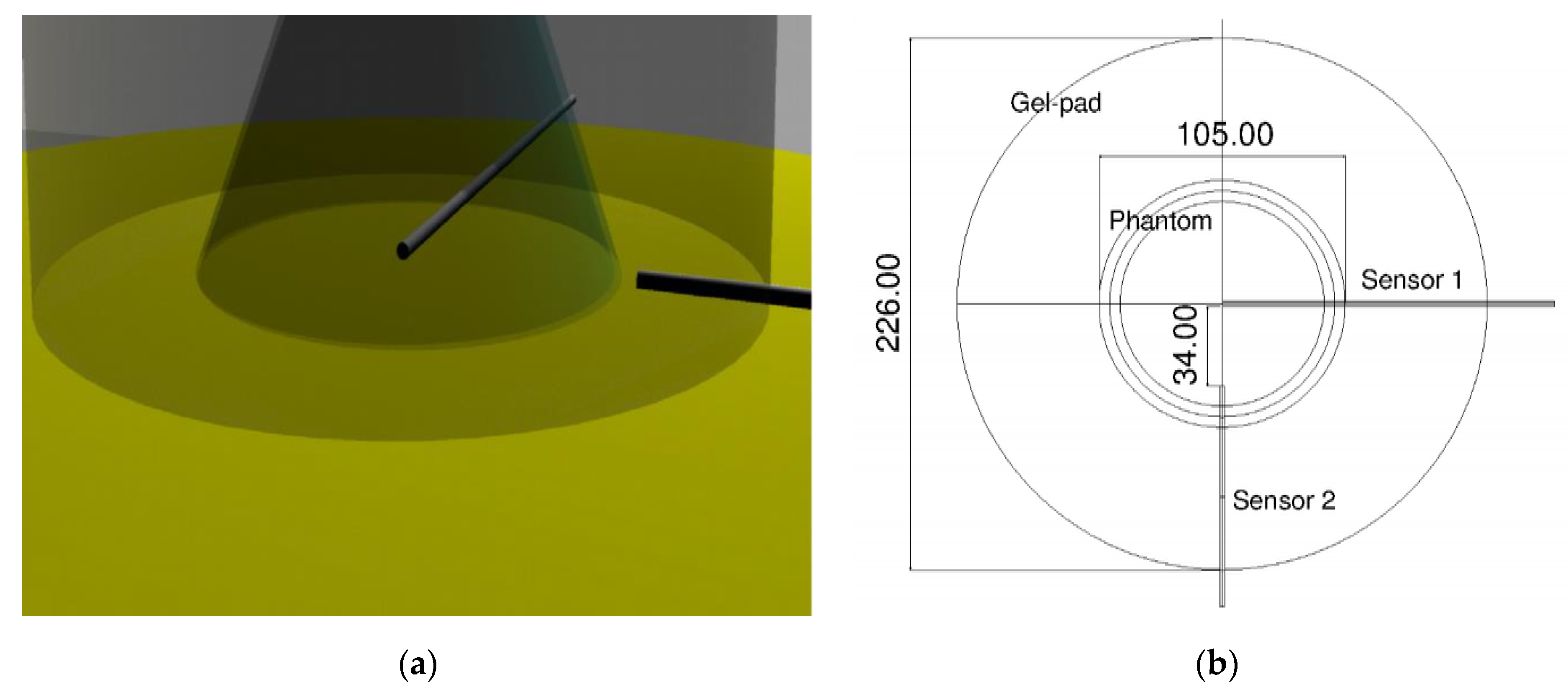
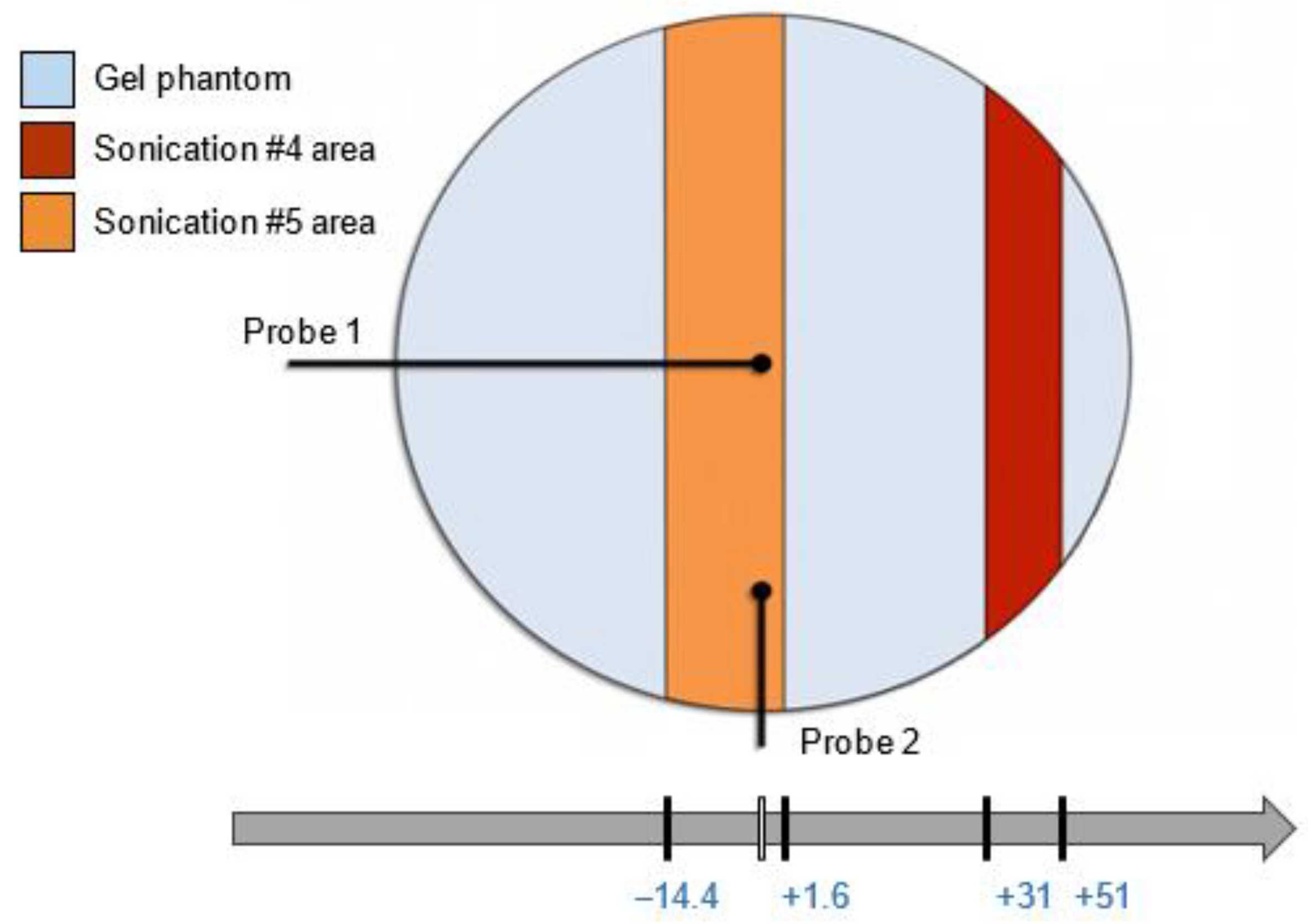
2.1. MRgFUS Treatments
2.2. Optical Thermometry
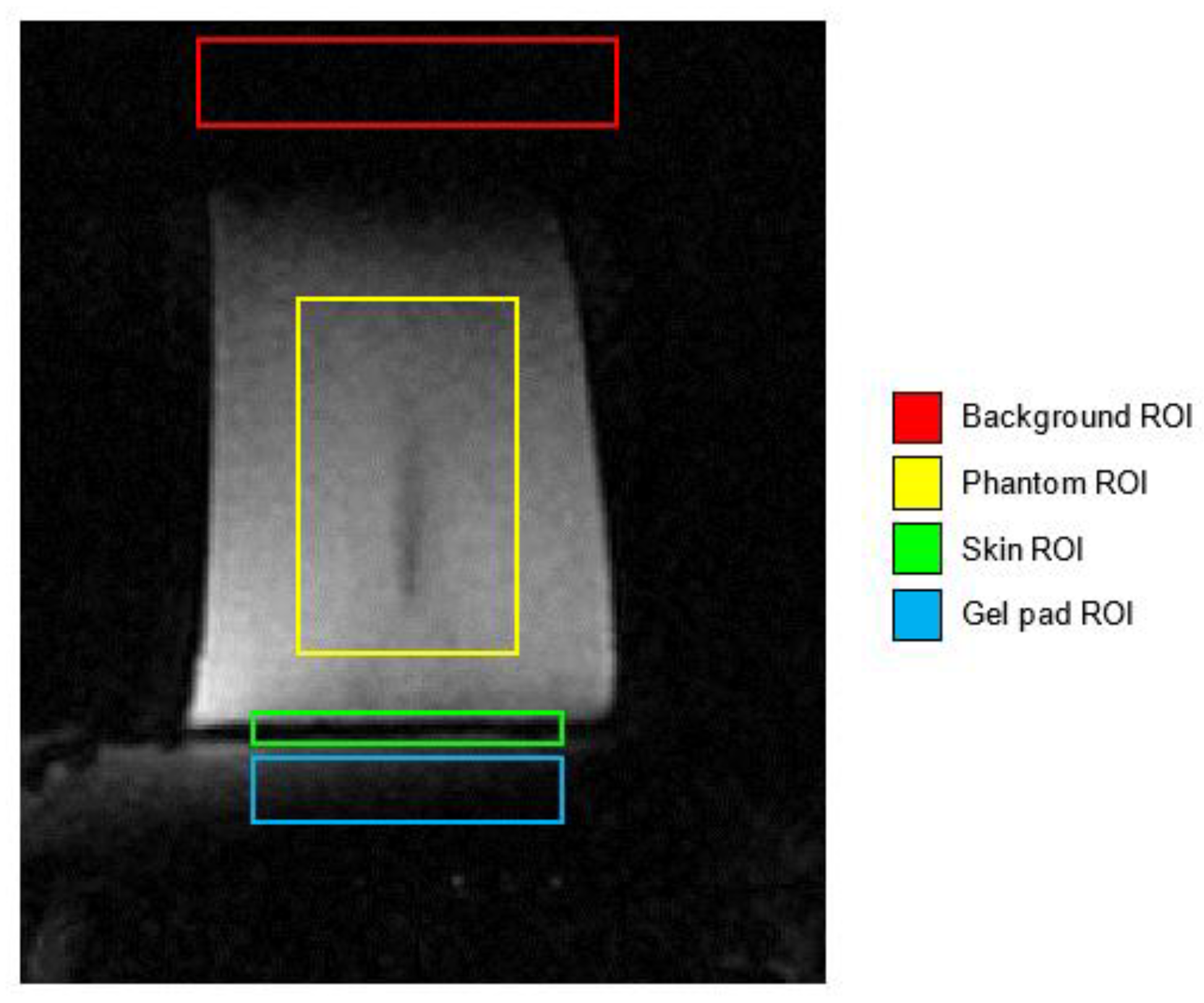
2.3. Signal-to-Noise-Ratio Estimation
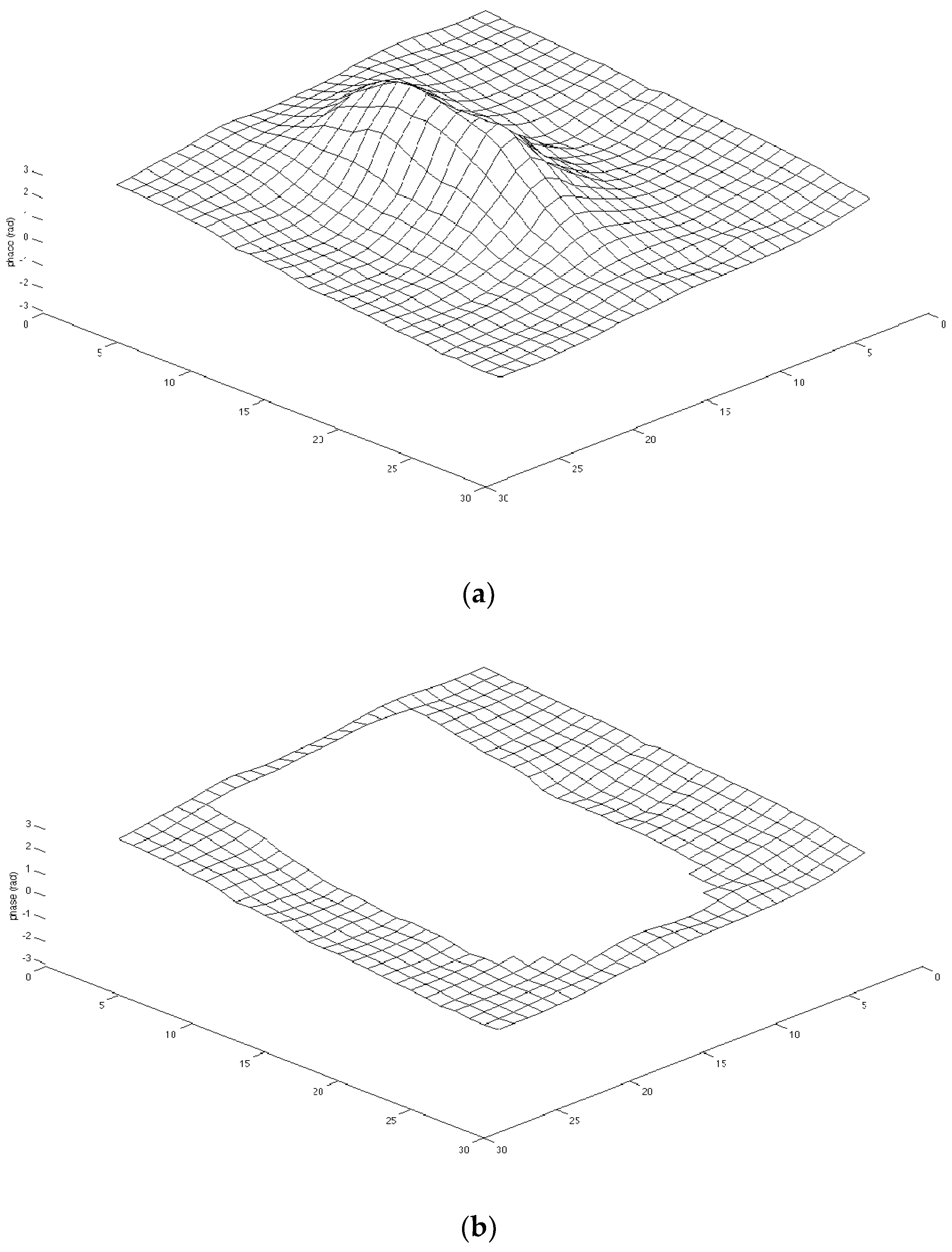
2.4. Referenceless Thermometry
Radial Basis Function Theory
3. Results
4. Discussion
5. Conclusions and Future Work
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Mauri, G.; Nicosia, L.; Varano, G.M.; Bonomo, G.; Della Vigna, P.; Monfardini, L.; Orsi, F. Tips and tricks for a safe and effective image-guided percutaneous renal tumour ablation. Insights Imaging 2017, 8, 357–363. [Google Scholar] [CrossRef]
- Mainini, A.P.; Monaco, C.; Pescatori, L.C.; De Angelis, C.; Sardanelli, F.; Sconfienza, L.M.; Mauri, G. Image-guided thermal ablation of benign thyroid nodules. J. Ultrasound 2017, 20, 11–22. [Google Scholar] [CrossRef]
- Seifabadi, R.; Li, M.; Xu, S.; Chen, Y.; Squires, A.; Negussie, A.H.; Bakhutashvili, I.; Choyke, P.; Turkbey, I.B.; Tse, Z.T.H.; et al. MRI Robot for Prostate Focal Laser Ablation: An Ex Vivo Study in Human Prostate. J. Imaging 2018, 4, 140. [Google Scholar] [CrossRef]
- Ning, G.; Zhang, X.; Zhang, Q.; Wang, Z.; Liao, H. Real-time and multimodality image-guided intelligent HIFU therapy for uterine fibroid. Theranostics 2020, 10, 4676–4693. [Google Scholar] [CrossRef] [PubMed]
- Lynn, J.G.; Zwemer, R.L.; Chick, A.J.; Miller, A.E. A new method for the generation and use of focused ultrasound in experimental biology. J. Gen. Physiol. 1942, 26, 179–193. [Google Scholar] [CrossRef] [PubMed]
- Doan, V.H.M.; Nguyen, V.T.; Choi, J.; Park, S.; Oh, J. Fuzzy Logic Control-Based HIFU System Integrated with Photoacoustic Imaging Module for Ex Vivo Artificial Tumor Treatment. Appl. Sci. 2020, 10, 7888. [Google Scholar] [CrossRef]
- Wilt, T.J.; MacDonald, R.; Rutks, I.; Shamliyan, T.A.; Taylor, B.C.; Kane, R.L. Systematic review: Comparative effectiveness and harms of treatments for clinically localized prostate cancer. Ann. Intern. Med. 2008, 148, 435–448. [Google Scholar] [CrossRef]
- Napoli, A.; Mastantuono, M.; Marincola, B.C.; Anzidei, M.; Zaccagna, F.; Moreschini, O.; Passariello, R.; Catalano, C. Osteoid Osteoma: MR-guided Focused Ultrasound for Entirely Noninvasive Treatment. Radiology 2013, 267, 514–521. [Google Scholar] [CrossRef]
- Li, C.-X.; Xu, G.-L.; Jiang, Z.-Y.; Li, J.-J.; Luo, G.-Y.; Shan, H.-B.; Zhang, R.; Li, Y. Analysis of clinical effect of high-intensity focused ultrasound on liver cancer. World J. Gastroenterol. 2004, 10, 2201–2204. [Google Scholar] [CrossRef]
- Merckel, L.G.; Bartels, L.W.; Köhler, M.O.; van den Bongard, H.J.G.D.; Deckers, R.; Mali, W.P.T.M.; Binkert, C.A.; Moonen, C.T.; Gilhuijs, K.G.A.; van den Bosch, M.A.A.J. MR-Guided High-Intensity Focused Ultrasound Ablation of Breast Cancer with a Dedicated Breast Platform. Cardiovasc. Interv. Radiol. 2013, 36, 292–301. [Google Scholar] [CrossRef]
- Gharib, H.; Hegedüs, L.; Pacella, C.M.; Baek, J.H.; Papini, E. Nonsurgical, Image-Guided, Minimally Invasive Therapy for Thyroid Nodules. J. Clin. Endocrinol. Metab. 2013, 98, 3949–3957. [Google Scholar] [CrossRef]
- Hindley, J.; Gedroyc, W.M.; Regan, L.; Stewart, E.; Tempany, C.; Hynnen, K.; Macdanold, N.; Inbar, Y.; Itzchak, Y.; Rabinovici, J.; et al. MRI Guidance of Focused Ultrasound Therapy of Uterine Fibroids:Early Results. Am. J. Roentgenol. 2004, 183, 1713–1719. [Google Scholar] [CrossRef] [PubMed]
- Militello, C.; Rundo, L.; Gilardi, M.C. Applications of imaging processing to MRgFUS treatment for fibroids: A review. Transl. Cancer Res. 2014, 3, 472–482. [Google Scholar] [CrossRef]
- Zaccagna, F.; Anzidei, M.; Sandolo, F.; Marincola, B.C.; Palla, C.; Leonardi, A.; Caliolo, G.; Andreani, F.; De Soccio, V.; Catalano, C.; et al. MRgFUS for liver and pancreas cancer treatments: The Umberto I hospital experience. Transl. Cancer Res. 2014, 3. [Google Scholar] [CrossRef]
- Coluccia, D.; Figueiredo, C.A.; Wu, M.Y.; Riemenschneider, A.N.; Diaz, R.; Luck, A.; Smith, C.; Das, S.; Ackerley, C.; O’Reilly, M.; et al. Enhancing glioblastoma treatment using cisplatin-gold-nanoparticle conjugates and targeted delivery with magnetic resonance-guided focused ultrasound. Nanomed. Nanotechnol. Biol. Med. 2018, 14, 1137–1148. [Google Scholar] [CrossRef] [PubMed]
- Davidson, B.; Hamani, C.; Huang, Y.; Jones, R.M.; Meng, Y.; Giacobbe, P.; Lipsman, N. Magnetic Resonance-Guided Focused Ultrasound Capsulotomy for Treatment-Resistant Psychiatric Disorders. Oper. Neurosurg. 2020. [Google Scholar] [CrossRef] [PubMed]
- Kapadia, A.N.; Elias, G.J.B.; Boutet, A.; Germann, J.; Pancholi, A.; Chu, P.; Zhong, J.; Fasano, A.; Munhoz, R.; Chow, C.; et al. Multimodal MRI for MRgFUS in essential tremor: Post-treatment radiological markers of clinical outcome. J. Neurol. Neurosurg. Psychiatry 2020, 91, 921–927. [Google Scholar] [CrossRef]
- Bruno, F.; Catalucci, A.; Arrigoni, F.; Sucapane, P.; Cerone, D.; Cerrone, P.; Ricci, A.; Marini, C.; Masciocchi, C. An experience-based review of HIFU in functional interventional neuroradiology: Transcranial MRgFUS thalamotomy for treatment of tremor. Radiol. Med. 2020, 125, 877–886. [Google Scholar] [CrossRef]
- Abel, M.; Ahmed, H.; Leen, E.; Park, E.; Chen, M.; Wasan, H.; Price, P.; Monzon, L.; Gedroyc, W.; Abel, P. Ultrasound-guided trans-rectal high-intensity focused ultrasound (HIFU) for advanced cervical cancer ablation is feasible: A case report. J. Ther. Ultrasound 2015, 3, 1–4. [Google Scholar] [CrossRef]
- Gross, D.; Coutier, C.; Legros, M.; Bouakaz, A.; Certon, D. A CMUT Probe for Ultrasound-Guided Focused Ultrasound Targeted Therapy. IEEE Trans. Ultrason. Ferroelectr. Freq. Control 2015, 62, 1145–1160. [Google Scholar] [CrossRef]
- Ye, G.; Smith, P.P.; Noble, A.; Mayia, F. A Model Based Approach to Monitor Temperature During HIFU Thermal Therapy. In AIP Conference Proceedings; American Institute of Physics: College Park, MD, USA, 2007. [Google Scholar]
- Napoli, A.; Anzidei, M.; Ciolina, F.; Marotta, E.; Marincola, B.C.; Brachetti, G.; Di Mare, L.; Cartocci, G.; Boni, F.; Noce, V.; et al. MR-Guided High-Intensity Focused Ultrasound: Current Status of an Emerging Technology. Cardiovasc. Interv. Radiol. 2013, 36, 1190–1203. [Google Scholar] [CrossRef] [PubMed]
- Jolesz, F.A.; Hynynen, K.H. MRI-Guided Focused Ultrasound Surgery; CRC Press: Boca Raton, FL, USA, 2007; ISBN 9781420019933. [Google Scholar]
- Chen, J.; Chen, W.; Zhang, L.; Li, K.; Peng, S.; He, M.; Hu, L. Safety of ultrasound-guided ultrasound ablation for uterine fibroids and adenomyosis: A review of 9988 cases. Ultrason. Sonochem. 2015, 27, 671–676. [Google Scholar] [CrossRef] [PubMed]
- Joo, B.; Park, M.-S.; Lee, S.H.; Choi, H.J.; Lim, S.T.; Rha, S.Y.; Rachmilevitch, I.; Lee, Y.H.; Suh, J.-S. Pain Palliation in Patients with Bone Metastases Using Magnetic Resonance-Guided Focused Ultrasound with Conformal Bone System: A Preliminary Report. Yonsei Med. J. 2015, 56, 503–509. [Google Scholar] [CrossRef]
- Kim, S.J.; Kim, K.A. Safety issues and updates under MR environments. Eur. J. Radiol. 2017, 89, 7–13. [Google Scholar] [CrossRef]
- Epistatou, A.C.; Tsalafoutas, I.A.; Delibasis, K.K. An Automated Method for Quality Control in MRI Systems: Methods and Considerations. J. Imaging 2020, 6, 111. [Google Scholar] [CrossRef]
- Antila, K.; Nieminen, H.J.; Sequeiros, R.B.; Ehnholm, G. Automatic segmentation for detecting uterine fibroid regions treated with MR-guided high intensity focused ultrasound (MR-HIFU). Med. Phys. 2014, 41, 73502. [Google Scholar] [CrossRef]
- Rundo, L.; Militello, C.; Vitabile, S.; Casarino, C.; Russo, G.L.; Midiri, M.; Gilardi, M.C. Combining split-and-merge and multi-seed region growing algorithms for uterine fibroid segmentation in MRgFUS treatments. Med. Biol. Eng. Comput. 2016, 54, 1071–1084. [Google Scholar] [CrossRef]
- Militello, C.; Vitabile, S.; Rundo, L.; Russo, G.; Midiri, M.; Gilardi, M.C. A fully automatic 2D segmentation method for uterine fibroid in MRgFUS treatment evaluation. Comput. Biol. Med. 2015, 62, 277–292. [Google Scholar] [CrossRef]
- Rundo, L.; Tangherloni, A.; Cazzaniga, P.; Nobile, M.S.; Russo, G.; Gilardi, M.C.; Vitabile, S.; Mauri, G.; Besozzi, D.; Militello, C. A novel framework for MR image segmentation and quantification by using MedGA. Comput. Methods Programs Biomed. 2019, 176, 159–172. [Google Scholar] [CrossRef]
- Ikink, M.E.; Van Breugel, J.M.M.; Schubert, G.; Nijenhuis, R.J.; Bartels, L.W.; Moonen, C.T.W.; van den Bosch, M.A.A.J. Volumetric MR-Guided High-Intensity Focused Ultrasound with Direct Skin Cooling for the Treatment of Symptomatic Uterine Fibroids: Proof-of-Concept Study. BioMed Res. Int. 2015, 2015, 1–10. [Google Scholar] [CrossRef][Green Version]
- Ishihara, Y.; Calderon, A.; Watanabe, H.; Okamoto, K.; Suzuki, Y.; Kuroda, K.; Suzuki, Y. A precise and fast temperature mapping using water proton chemical shift. Magn. Reson. Med. 1995, 34, 814–823. [Google Scholar] [CrossRef]
- Sapareto, S.A.; Dewey, W.C. Thermal dose determination in cancer therapy. Int. J. Radiat. Oncol. Biol. Phys. 1984, 10, 787–800. [Google Scholar] [CrossRef]
- O’Neill, D.P.; Peng, T.; Stiegler, P.; Mayrhauser, U.; Koestenbauer, S.; Tscheliessnigg, K.; Payne, S.J. A Three-State Mathematical Model of Hyperthermic Cell Death. Ann. Biomed. Eng. 2010, 39, 570–579. [Google Scholar] [CrossRef]
- Yung, J.P.; Shetty, A.; Elliott, A.; Weinberg, J.S.; McNichols, R.J.; Gowda, A.; Hazle, J.D.; Stafford, R.J. Quantitative comparison of thermal dose models in normal canine brain. Med. Phys. 2010, 37, 5313–5321. [Google Scholar] [CrossRef]
- Wu, F.; Wang, Z.-B.; Chen, W.-Z.; Zou, J.-Z.; Bai, J.; Zhu, H.; Li, K.-Q.; Jin, C.-B.; Xie, F.-L.; Su, H.-B. Advanced Hepatocellular Carcinoma: Treatment with High-Intensity Focused Ultrasound Ablation Combined with Transcatheter Arterial Embolization. Radiology 2005, 235, 659–667. [Google Scholar] [CrossRef] [PubMed]
- Li, J.-J.; Xu, G.-L.; Gu, M.-F.; Luo, G.-Y.; Rong, Z.; Wu, P.-H.; Xia, J.-C. Complications of high intensity focused ultrasound in patients with recurrent and metastatic abdominal tumors. World J. Gastroenterol. 2007, 13, 2747–2751. [Google Scholar] [CrossRef] [PubMed]
- Jung, S.E.; Cho, S.H.; Jang, J.H.; Han, J.-Y. High-intensity focused ultrasound ablation in hepatic and pancreatic cancer: Complications. Abdom. Imaging 2011, 36, 185–195. [Google Scholar] [CrossRef]
- Zucconi, F.; Colombo, P.E.; Pasetto, S.; Lascialfari, A.; Ticca, C.; Torresin, A. Analysis and reduction of thermal dose errors in MRgFUS treatment. Phys. Med. 2014, 30, 111–116. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Kinsler, L.E.; Frey, A.R.; Coppens, A.B.; Sanders, J.V. Fundamentals of Acoustics, 4th ed.; Wiley India Private Ltd.: New Delhi, India, 2009; ISBN 9788126521999. [Google Scholar]
- National Council on Radiation. Protection and Measurements Biological Effects of Ultrasound: Mechanisms and Clinical Implications; National Council on Radiation: Bethesda, MD, USA, 1983. [Google Scholar]
- Gorny, K.R.; Hangiandreou, N.J.; Ward, H.A.; Hesley, G.K.; Brown, D.L.; Felmlee, J.P. The utility of pelvic coil SNR testing in the quality assurance of a clinical MRgFUS system. Phys. Med. Biol. 2009, 54, N83–N91. [Google Scholar] [CrossRef]
- Firbank, M.J.; Harrison, R.M.; Williams, E.D.; Coulthard, A. Quality assurance for MRI: Practical experience. Br. J. Radiol. 2000, 73, 376–383. [Google Scholar] [CrossRef]
- Ross, J.C.; Tranquebar, R.; Shanbhag, D. Real-Time Liver Motion Compensation for MRgFUS. Comput. Vis. 2008, 11, 806–813. [Google Scholar] [CrossRef]
- Jenne, J.W.; Tretbar, S.H.; Hewener, H.J.; Speicher, D.; Barthscherer, T.; Sarti, C.; Bongers, A.; Schwaab, J.; Günther, M. Ul-trasonography-based motion tracking for MRgFUS. In AIP Conference Proceedings; AIP Publishing LLC: Melville, NY, USA, 2017. [Google Scholar]
- Agnello, L.; Militello, C.; Gagliardo, C.; Vitabile, S. Referenceless thermometry using radial basis function interpolation. In Proceedings of the 2014 World Symposium on Computer Applications & Research (WSCAR), Sousse, Tunisia, 18–20 January 2014. [Google Scholar]
- Agnello, L.; Militello, C.; Gagliardo, C.; Vitabile, S. Radial Basis Function Interpolation for Referenceless Thermometry En-hancement. In Advances in Neural Networks: Computational and Theoretical Issues; Springer: Cham, Switzerland, 2015; pp. 195–206. [Google Scholar]
- Kuroda, K.; Kokuryo, D.; Kumamoto, E.; Suzuki, K.; Matsuoka, Y.; Keserci, B. Optimization of self-reference thermometry using complex field estimation. Magn. Reson. Med. 2006, 56, 835–843. [Google Scholar] [CrossRef] [PubMed]
- Rieke, V.; Vigen, K.K.; Sommer, G.; Daniel, B.L.; Pauly, J.M.; Butts, K. Referenceless PRF shift thermometry. Magn. Reson. Med. 2004, 51, 1223–1231. [Google Scholar] [CrossRef]
- Beatson, R.; Newsam, G. Fast evaluation of radial basis functions: I. Comput. Math. Appl. 1992, 24, 7–19. [Google Scholar] [CrossRef]
- Carr, J.C.; Fright, W.R.; Beatson, R.K. Surface interpolation with radial basis functions for medical imaging. IEEE Trans. Med Imaging 1997, 16, 96–107. [Google Scholar] [CrossRef]
- Powell, M.J.D.; Light, W.A. Advances in Numerical Analysis III Wavelets Subdivision Algorithms and Radial Basis Functions. The Theory of Radial Basis Function; Oxford University Press on Demand: Oxford, UK, 1992. [Google Scholar]
- Light, W.A. Some Aspects of Radial Basis Function Approximation. Approx. Theory Spline Funct. Appl. 1992, 163–190. [Google Scholar] [CrossRef]
- Rieke, V.; Pauly, K.B. MR thermometry. J. Magn. Reson. Imaging 2008, 27, 376–390. [Google Scholar] [CrossRef] [PubMed]
- Kuroda, K.; Oshio, K.; Mulkern, R.V.; Jolesz, F.A. Optimization of chemical shift selective suppression of fat. Magn. Reson. Med. 1998, 40, 505–510. [Google Scholar] [CrossRef]
- Wilcoxon, F. Individual Comparisons by Ranking Methods. Biom. Bull. 1945, 1, 80. [Google Scholar] [CrossRef]
- Moritz, A.R.; Henriques, F.C. Studies of Thermal Injury: II. The Relative Importance of Time and Surface Temperature in the Causation of Cutaneous Burns. Am. J. Pathol. 1947, 23, 695–720. [Google Scholar]
- Viglianti, B.L.; Dewhirst, M.W.; Abraham, J.P.; Gorman, J.M.; Sparrow, E.M. Rationalization of thermal injury quantification methods: Application to skin burns. Burns 2014, 40, 896–902. [Google Scholar] [CrossRef] [PubMed]
- Mougenot, C.; Köhler, M.O.; Enholm, J.; Quesson, B.; Moonen, C. Quantification of near-field heating during volumetric MR-HIFU ablation. Med. Phys. 2010, 38, 272–282. [Google Scholar] [CrossRef] [PubMed]












{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristic | Value |
|---|---|
| Temperature operating range | 0 °C to 85 °C |
| Specific calibrated range | 20 °C to 45 °C standard (other ranges available) |
| Resolution | 0.01 °C |
| Accuracy (specific calibrated range) | ±0.15 °C @ ±3.3 σ limit (99.9% confidence level) |
| Response time | <1 s |
| Operating humidity range | 0–100% |
| Function Type | Spatial Dimension | Polynomial Degree | Restriction on Nodes |
|---|---|---|---|
| linear RBF | any | 1 | not coplanar |
| thin-plate spline | 2 | 1 | not coplanar |
| Gaussian | any | absent | none |
| multiquadratic RBF | any | absent | none |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Militello, C.; Rundo, L.; Vicari, F.; Agnello, L.; Borasi, G.; Vitabile, S.; Russo, G. A Computational Study on Temperature Variations in MRgFUS Treatments Using PRF Thermometry Techniques and Optical Probes. J. Imaging 2021, 7, 63. https://doi.org/10.3390/jimaging7040063
Militello C, Rundo L, Vicari F, Agnello L, Borasi G, Vitabile S, Russo G. A Computational Study on Temperature Variations in MRgFUS Treatments Using PRF Thermometry Techniques and Optical Probes. Journal of Imaging. 2021; 7(4):63. https://doi.org/10.3390/jimaging7040063
Chicago/Turabian StyleMilitello, Carmelo, Leonardo Rundo, Fabrizio Vicari, Luca Agnello, Giovanni Borasi, Salvatore Vitabile, and Giorgio Russo. 2021. "A Computational Study on Temperature Variations in MRgFUS Treatments Using PRF Thermometry Techniques and Optical Probes" Journal of Imaging 7, no. 4: 63. https://doi.org/10.3390/jimaging7040063
APA StyleMilitello, C., Rundo, L., Vicari, F., Agnello, L., Borasi, G., Vitabile, S., & Russo, G. (2021). A Computational Study on Temperature Variations in MRgFUS Treatments Using PRF Thermometry Techniques and Optical Probes. Journal of Imaging, 7(4), 63. https://doi.org/10.3390/jimaging7040063