1. Introduction
When severe enough, a renal artery stenosis (RAS) leads to hypertension and impaired renal function. RAS may have different etiologies, e.g., fibromuscular dysplasia or being of atherosclerotic character (denoted as ARAS). In 90% of cases, RAS is caused by arteriosclerosis [
1]. Although much less common than other manifestations of atherosclerotic disease, the condition can be present in the range of 3–7% in a healthy population [
2]. Similar to atherosclerotic disease in general, the prevalence increases with age. For certain patient groups with severe heart disease, a prevalence of 54% has been observed. Conversely, patients with newly discovered RAS often have cardiovascular disease with widespread arteriosclerosis [
3]. The overall mortality is increased up to 6 times in patients with atherosclerotic RAS compared to healthy subjects of similar age [
2].
Arteriosclerotic changes are predominantly found in certain arteries (coronary, carotid, renal and femoral) at certain locations (bifurcations, branches and at strong curvatures). The impact of hemodynamics in atherogenesis (i.e., plaque formation) has been recognized for many decades [
4]. Moreover, it has been hypothesized that the process is related to the Wall Shear Stress (
WSS) [
5], claiming that both high
WSS [
6] as well as low and, in particular, oscillatory
WSS [
7] can play a role in the processes. The latter mechanism appears to be more frequently associated with intimal thickening. In recent years, the temporal- and spatial-gradients of the
WSS has been recognized as equally important factors as the magnitude of the
WSS itself [
6].
There is no consensus in the precise definition of RAS [
2]. However, according to the American Heart Association (AHA), RAS is defined as hemodynamically significant if one or more of the following criteria are fulfilled [
1]:
a narrowing of the vessels’ inner diameter between 50% to 70% by visual estimation with a peak translesional pressure gradient of at least 20 mmHg (2.67 kPa) or a mean gradient of at least 10 mmHg (measured with a 5 F (about 1.6 mm) or smaller catheter or pressure wire at conventional angiography),
a stenosis of at least 70% narrowing (inner diameter) measured on a conventional angiogram, and
a stenosis greater than 70% narrowing (inner diameter) by intravascular ultrasound measurement.
RAS shows subtle or no symptoms before the disease becomes severe [
2] and is usually presented with hypertension that is often resistant to drug therapy. Treatment options include antihypertensive medication and reduction of risk factors [
2]. In some cases, angioplasty with dilatation and stenting of the affected artery is an alternative. Although the patency of the renal artery is improved after revascularization therapy, the clinical outcome for the patient is not necessarily beneficial [
8,
9]. Hence, medical therapy is considered as a first option. The main issue with revascularization is the long-term effect as discussed by Lao et al. [
1] and the references therein. After having a progressive ARAS over a longer period of time, the damage to the kidneys can be irreversible [
10]. Moreover, as revascularization does not eliminate the underlying reasons for the disease, it is not surprising that a continuation of the atherosclerotic process is observed also postoperatively.
Numerical simulation of the flow in renal arteries and its relation to renal artery stenosis (RAS) was recently reported [
11,
12]. In the present study, four indicators are considered in order to assess the possibility of relapse of atherosclerosis/stenosis after revascularization. Three of these markers, namely time averaged wall shear stress (
TAWSS), relative residence time (RRT) and oscillatory shear index (
OSI) have been used in literature for stenosis identification in blood flow simulations in arteries, most commonly in the carotid artery [
13]. The relevance of these indicators has been questioned in the review of Peiffer et al. [
14]. The fourth marker has not previously been applied as an indicator for stenosis.
2. Materials and Methods
2.1. Patient Cases
For this study, three patients who had underwent Computed Tomography Angiography (CTA) were selected.
Two patients with a left sided ARAS (at common locations for the stenosis)
A previously healthy patient undergoing an acute CTA study of the aorta, where no pathological changes were found (except minor atherosclerotic changes that could be considered as a “normal” finding considering the patient’s age).
The patients having ARAS underwent conventional angiography and treatment with dilatation and/or stenting of the stenosis.
The CTA data was used to define the geometry of the abdominal aorta, also including the celiac trunk, the superior mesenteric and renal arteries. Siemens Somatom Flash Scanners, having a limit of 0.3 mm isotropic voxels, were used to carry out the CTA study with slice thicknesses of 1 mm and 0.75 mm. The reason for the difference is advances in imaging software improving the quality and noise reduction for the image rendering carried out in 2015 and 2017. For the image reconstruction, Siemens SAFIRE I30 (iterative reconstruction algorithm) was applied. Iodine contrast used for the CT angiography showed a concentration in the abdominal aorta of about 300–500 HU.
The shape of a sclerotic artery has randomly distributed irregularities, making it difficult to distinguish these from noise in the CTA data. Here, the software Mialab by Wang and Smedby [
15] is applied to perform the segmentations (i.e., the process of generating the three-dimensional shape of the aorta), utilizing threshold-based techniques. The effect of the segmentation approach on the arteriosclerotic indicators has recently been investigated by Berg et al. [
16]. The inside wall of the abdominal aorta was delineated from the level of the diaphragm down to right above its bifurcation, including the celiac trunk, the superior mesenteric artery and the renal arteries.
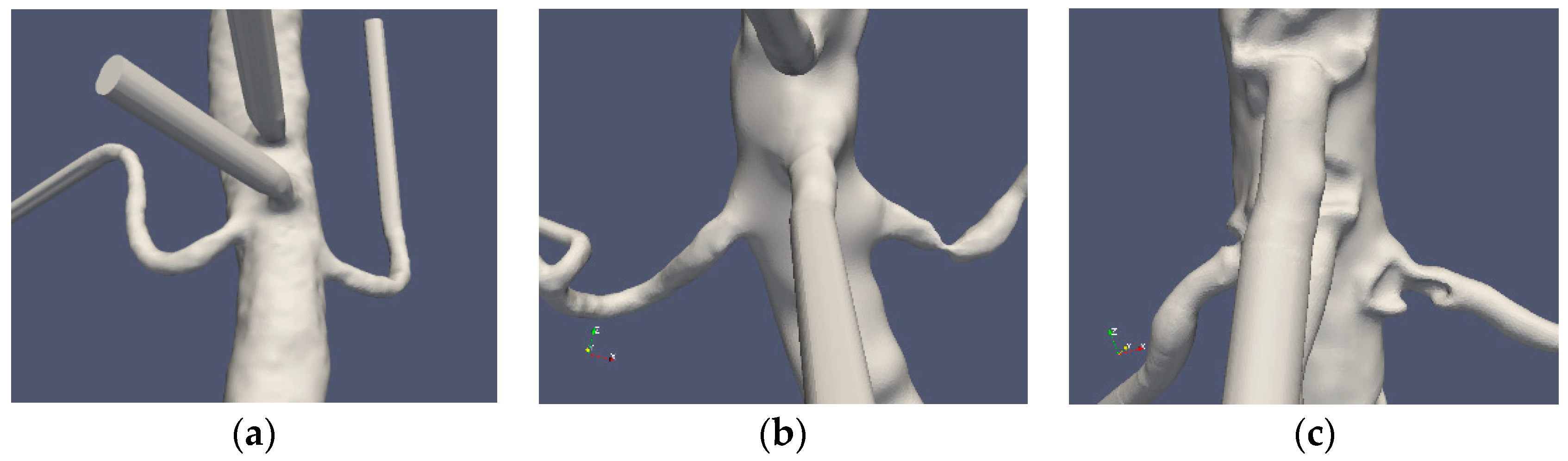
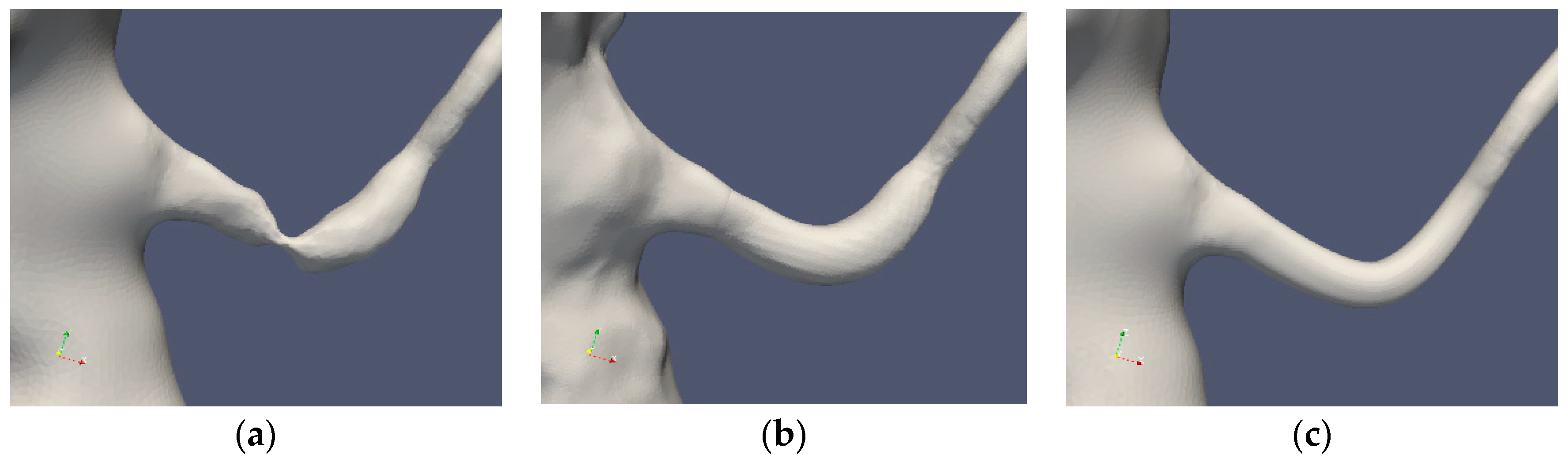
In patients 1 and 2 (termed as Case1 and Case2 in the following), the affected renal artery was reconstructed. In Case1 reconstruction was made using two different computational methods. For Case2, computational reconstruction was unfeasible due the stenosis location close to the vessel ostium. Therefore, reconstructions were created manually by removing the stenosis and, in a second step, by post-stenotic dilatation, using the graphics software Blender [
17]. Further smoothing of the surface geometry was applied to mimic the smoother shape commonly obtained in a revasculated and stented artery. Moreover, no attempt was made to reshape the artery into a circular cross section. The reconstructed arteries were used to assess the applicability of the abovementioned indicators.
The computational domain (including the abdominal artery and the main arteries bifurcating from it, namely the celiac trunk, superior and inferior mesenteric arteries and the renal arteries) was used for the blood flow simulations presented here.
2.2. Governing Equations
The blood was considered to be an incompressible non-Newtonian fluid and modeled as a mixture of Red Blood Cells (RBC) and plasma (solution of proteins, electrolytes and other small molecules in water). The volume fraction of RBCs (hematocrit) is denoted by
α. The density of RBCs and plasma were
ρα = 1100 kg/m
3 and
ρp = 1025 kg/m
3, respectively. The mixture density
ρ =
ρα·
α +
ρp (1 −
α) varied in space and time. However, the density of the RBCs and plasma being similar allowed for the mixture to be approximated as being incompressible. Thus, the Navier–Stokes equations for the conservation of mass and momentum can be expressed as
where
ui is the mixture velocity in the
ith direction,
p is the pressure and
ν is the kinematic viscosity of the mixture. The RBC phase, and thereby the blood, is assumed to behave as a continuum. This assumption is based on the large difference in scales concerning the diameters of the arteries and the RBC (6 ×∙10
−3 m and 6 ×∙10
−6 m, respectively). Thus, the RBCs were assumed to be transported by the mixture (advection) and diffusion:
where
D represents the diffusivity of the RBC phase. In the following, the RBC diffusivity is assumed to be constant with
D = 10
−8 m
2/s, corresponding to the largest diffusivity value as presented by Casa and Ku [
18].
The conservation of mass and momentum (Equations (1) and (2)) are so-called incompletely parabolic. In the steady state, the system is elliptic and requires three conditions on all boundaries. Similar boundary conditions are assumed to be needed in the time-dependent case. A wide range of boundary conditions may be applied, provided that the normal to the inflow and outflow surfaces are such that the total mass conservation is satisfied.
2.3. Rheological Model
There exist several models for blood viscosity dependence on
α and the shear rate,
γ [
19]. In the following, the Quemada model is used [
20]. The Quemada model has been adjusted for a wide range of hematocrit as well as shear rates and has been described as well-suited for modeling blood rheology in a range relevant to clinical situations [
21]. The apparent viscosity of the blood is modeled by the following expression:
where the plasma viscosity
μp = 1.32 × 10
−3 Pa s,
γ is the magnitude of the shear-rate tensor
and
The coefficients k0(α), k∞ (α) and γc(α) are given by
The model accounts for the shear thinning property of the blood; hence μ decreases with an increasing γ, consistent with experimental observations. When the diffusivity of α is small (as used in the cases herein) and the inlet condition of the RBC concentration is uniform, α remains constant throughout the computational domain and over time.
2.4. Centerline and Geometrical Parameters
The centerline of the artery is useful to characterize vessel geometry as well as for post-processing. Simply, the centerline can be defined as the path inside the vessel, between two points (at the vessels inlet and outlet), maximizing the total distance to the boundary [
22]. In this study, the centerlines were computed using the Vascular Modeling Tool Kit, VMTK [
23], computing all lines from the aortic inlet to the outlets. To evaluate the effects of the vessel geometry, the surface curvature was calculated using VTMK. From the two principal curvatures
k1 and
k2, also known as maximum and minimum, the Gaussian curvature,
K = k1·k2 and the mean curvature
M = (k1 + k2)/2 was obtained.
2.5. Wall Shear Stress and Wall Indicators
From the shear stress tensor τij = μ·γij on the wall of the vessel and the unit normal to the wall (nj), the wall shear vector WSSi = τij·nj can be defined. This vector defines the force per unit area acting on the endothelium. The component of the wall shear stress vector, normal the wall, is denoted by WSSNi = (WSSj nj) ni. If ni is normal to the wall, the planar components (WSSpi) are given by WSSpi = εijk WSSj nk or WSSi − WSSNi ni. As the WSS is commonly accepted as a crucial parameter for the formation of atherosclerosis, several WSS-based indicators for the presence of stenosis has been presented. To directly measure WSS in vivo and even in mock-loops using water is difficult. Hence, time-averaged values of the components of the WSS that are parallel to the surface under consideration (i.e., WSSi) is most commonly found in literature. The following four indicators were used to assess the flow data.
2.5.1. Time Averaged Wall Shear Stress (TAWSS) [24,25]
TAWSS is the time-averaged value of WSS vector magnitude. TAWSS is a local value and does not contain information regarding the temporal or spatial WSS variations. TAWSS cannot be lower than 0 but has no definitive upper bound. Computed values of TAWSS may be compared to the measured data for the few and simple cases for which such data exists. It has empirically been observed that oscillatory WSS promotes atherosclerosis. However, this information is not included in TAWSS. To at least partially account for such an effect, the following indicator was introduced:
2.5.2. Oscillatory Shear Index (OSI) [25,26]
OSI varies between 0 and 0.5. When
WSSi is strictly positive (oscillatory or non-oscillatory),
OSI = 0. When
WSSi changes signs such that the integral of the positive and negative sequences are the same,
OSI obtains the value 0.5. Values of 0 <
OSI < 0.5 indicate an oscillatory
WSS field, but the indicator does not indicate the amplitude nor frequency of the oscillations. The time during which extreme
WSS (high or low) exists appears to be essential for the development of atherosclerosis. Low
TAWSS (< 4 dynes/cm
2) and significant
OSI (>0.15) are risk factors for the incidence and progression of atherosclerosis [
27,
28].
2.5.3. Relative Residence Time (RRT) [29]
RRT includes both OSI and TAWSS. From Equation (11), it can be noted that RRT is related to the time-mean of the shear-rate and not the residence time of a fluid or a real particle. For OSI = 0, the time scale is proportional to the viscosity and inversely proportional to TAWSS.
2.5.4. A Fourth Indicator of Atherosclerosis is Proposed Herein
As endothelial activation is associated with the activation of other cells, similar activation models could possibly be applied also for endothelial cells. Here, the power law model of Nobili et al. [
30] for platelet activation is applied. Analogous models have been used for RBC destruction due to elevated shear. In the platelet activation model, the target variable, the Platelet Activation State (PAS), was defined as the fraction of platelets that have become activated relative to all platelets in the tested blood. The model has three empirically determined parameters:
a,
b and
c [
31]. In our study, the target variable is denoted endothelial activation index (EAI), using the same numerical values for the model parameters as suggested by the original model for platelets.
τ is the so-called scalar stress, corresponding to the length of the
WSS vector. The following values of the parameters were used:
a = 1.3198,
b = 0.6256 and
c = 10
−5 [
30]. The dose term,
H, contains the accumulated stress whereas the instantaneous effect of stress enters through the scalar stress. It can be noted that the stress effect is computed as the scalar stress to the power of b/a = 0.474. This numerical value has no real physical meaning; it is rather the result of fitting the model parameters to the experimental data (PAS). Moreover, it is noted that EAI, as PAS, is a dimensionless number, interpreted as the probability of activation of an endothelial cell. The meaning of
H and
τb/a is less clear as these entities contain dimensional variables to some power.
The PAS-based indicator differs in essence from the former three as it indicates the time evolution of the activation level. TAWSS, OSI and RRT are, on the other hand, time-averaged quantities that do not attempt to indicate the temporal effect of the WSS.
2.6. Numerical Methods
The meshes for all cases were generated using STAR-CCM+ (v12.04.11, Siemens, Alameda, CA, USA). The flow simulations were carried out using the open software package OpenFOAM (v5.0, CFD Direct Ltd, Reading, UK) [
32]. A formally second-order finite volume discretization was used to approximate Equations (1)–(3). The diffusive fluxes were computed using central differences while the convective fluxes were computed with limited central differences. The time derivatives were approximated to second order with an implicit backward time stepping scheme. The time step was adapted to allow for stability (Courant number restriction) and speed. Thus, the time step was in the range of 10
−4 s and 2 ∙ 10
−6 s where the smallest time steps were applied during peak systole for the stenoted artery cases where the mesh size and the high flow speed dictates the smallest time steps. The discretized equations were solved sequentially, starting with the RBC transport (Equation (3)) coupled to the flow equations through the density and viscosity fields. The momentum equation was solved component by component, after which three pressure correction steps with the PISO algorithm were carried out to ensure that velocity field satisfies continuity (Equation (2)).
5. Discussion
This work implicitly assumes that renal arteries developing stenosis and that are “revascularized" shall develop a new stenosis over time. This “assumption” has clinically been confirmed and is expected as the surgical treatment does not remedy the underlying atherosclerotic disease [
10]. Therefore, the stenosis indicators are assessed in terms of their detection ability of the location of the stenosis in the reconstructed artery. Such an indicator could be used to determine the possible benefit of arterial revascularization. However, reaching this goal requires more cases to be considered, yet the results are useful in order to develop appropriate indicators that shall be predictive in the sense stated above.
The close connection between the endothelial activation and the activation of inflammatory cells as well as coagulation system is now well-established [
36]. It is also reasonable that the response of different cells to external stress is similar to each other (through evolution). Thus, it is natural that similar models can be applied for the activation of endothelial cells, platelets and leukocytes.
The four indicators investigated do locate the stenosis in the affected artery. However, the level of success in predicting the potential risk for restenosis is less clear. The different indictors heavily rely on the
WSS, well-motivated by the literature in the field. A major problem associated with the commonly used indicators is that
WSS is a tensor and the variable called
WSS by the indicators is a scalar. Different expressions of a tensor could be used that leads to a scalar expressing some property of the tensor. The different in vitro measurements of the effect of
WSS on endothelial cells were assessed in a unidirectional flow [
35]. The expression for
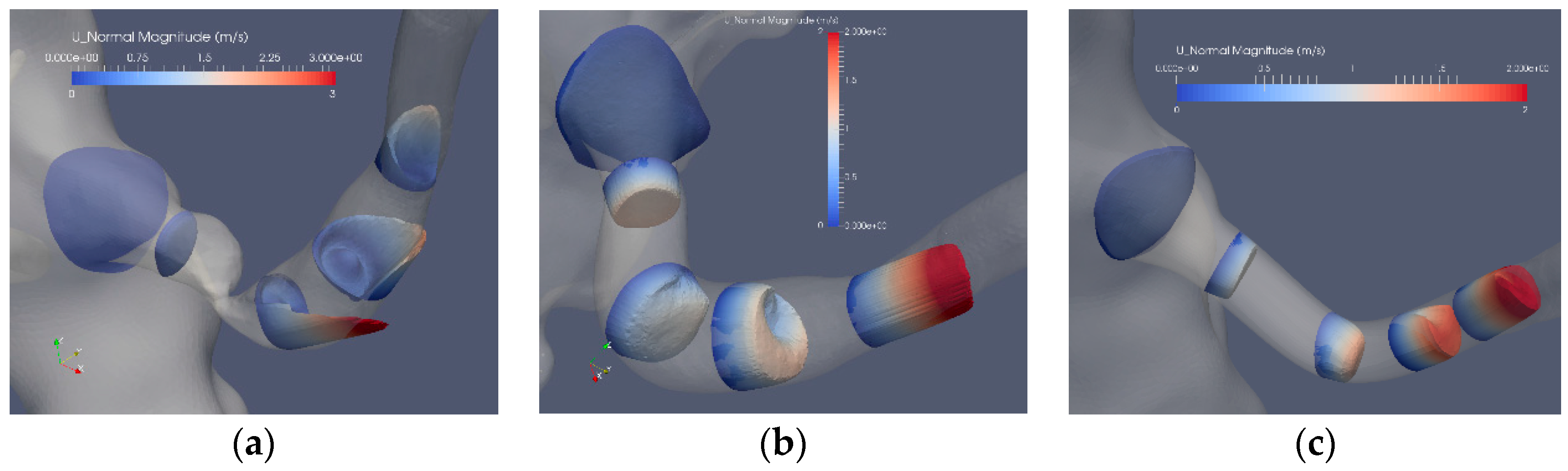
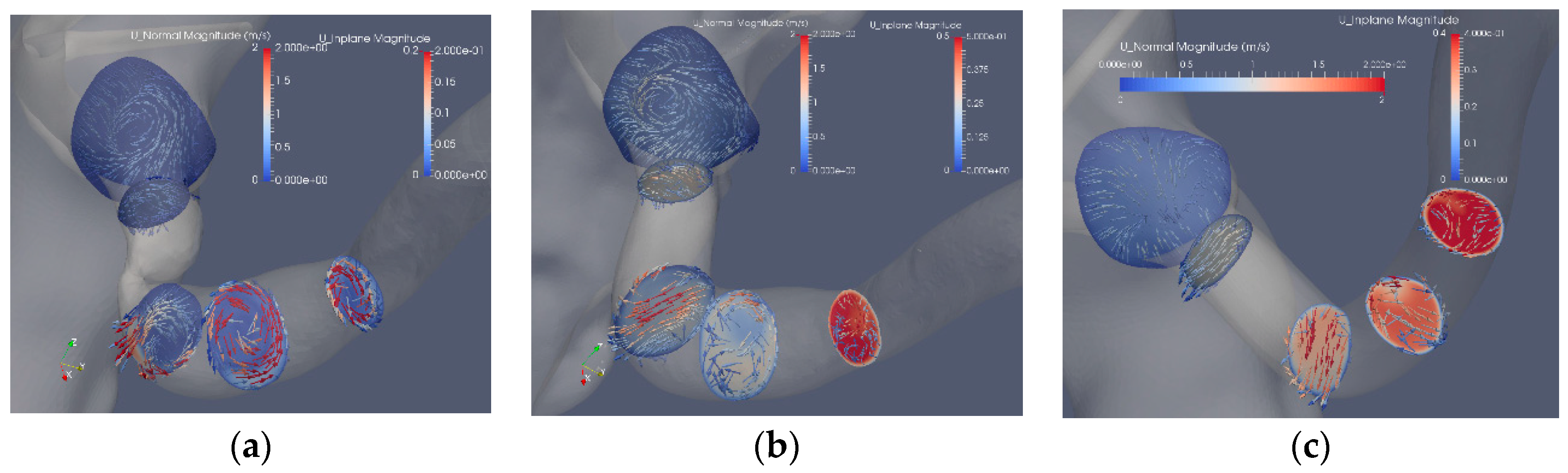
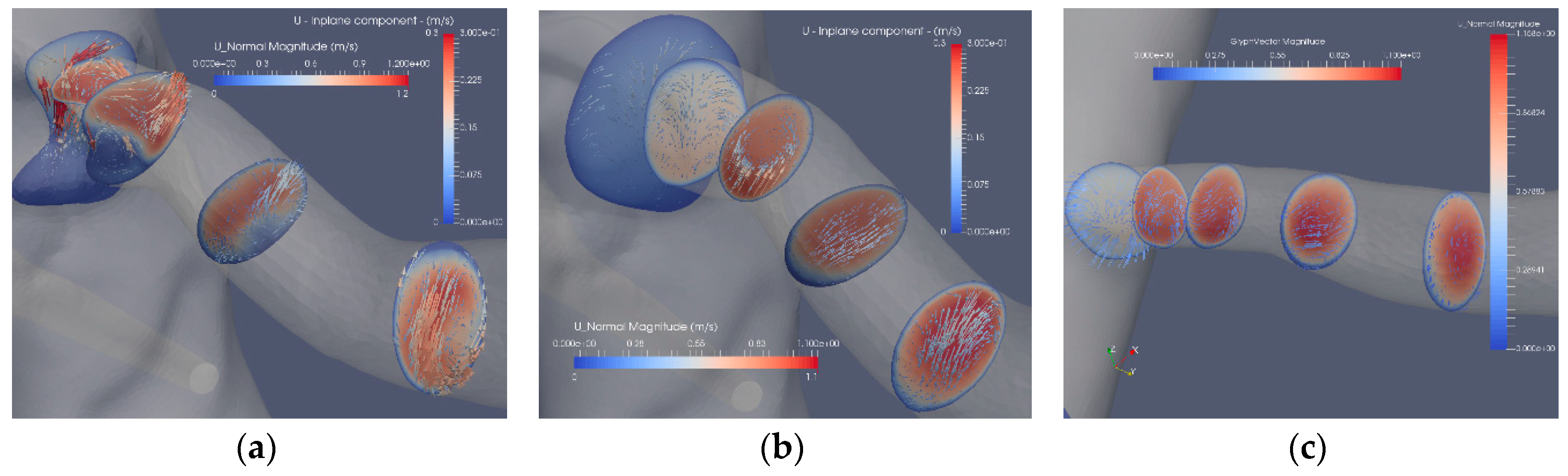
WSS in such simple cases is a scalar. The flow in the renal artery is much more complex. As shown in
Figure 6,
Figure 7 and
Figure 8, the flow is not always aligned with the centerline of the artery. Swirling flow leads to a
WSS that has a component along the axis of the artery as well as another component along the circumference of the artery. This issue has been discussed in relation to platelet activation where all the components of the stress tensor may be important.
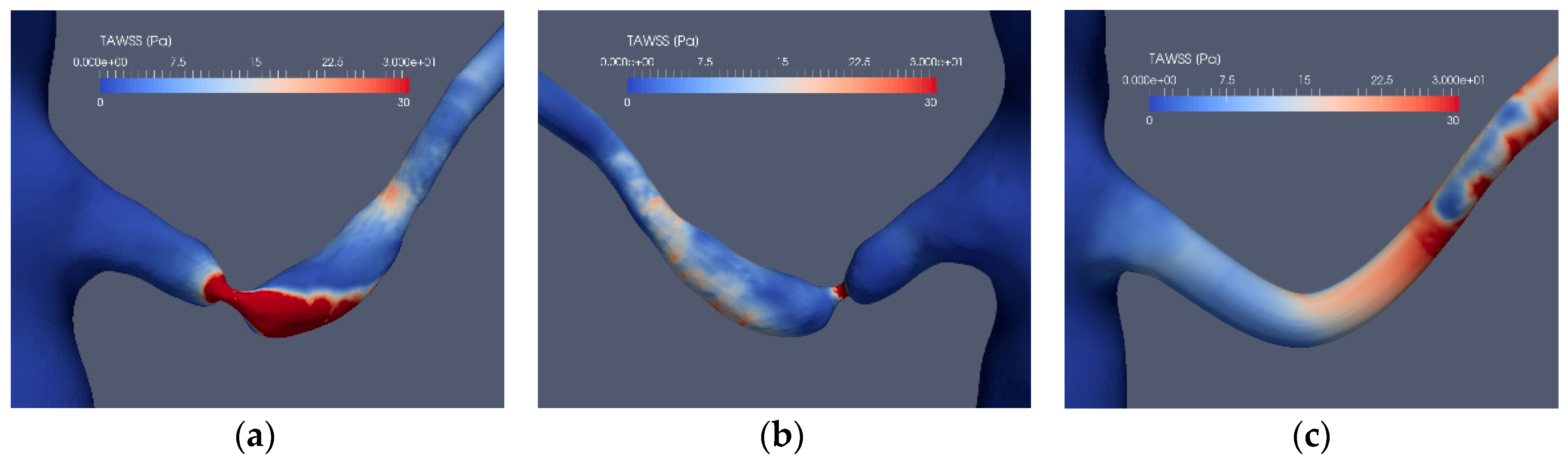
TAWSS was introduced as an indicator since the role of WSS for atherosclerosis was recognized for decades. TAWSS has a meaning when compared to a reference value. To this end, it has to be noted that it has experimentally been found that atherosclerosis may occur in low WSS as well as at high WSS regions. Therefore, to interpret TAWSS, threshold values for the “non-pathological” range have to be set. Hence, TAWSS can be used quantitatively only if empirical data can be relied upon, which appears to be case-dependent. TAWSS does not contain any impact of WSS transients on the endothelium. This poses an additional drawback as transients are known to play a role in low WSS cases. Despite these shortcomings, TAWSS did produce an elevated level in the reconstructed artery at the location of the stenosis in the non-reconstructed artery.
In contrast to
TAWSS,
OSI is sensitive to oscillatory
WSS. However, this is the case
only when the flow changes sign.
OSI has a value of 0 for all oscillatory flows in which the flow is unidirectional, independent to the magnitude or the frequency of the oscillations. Thus,
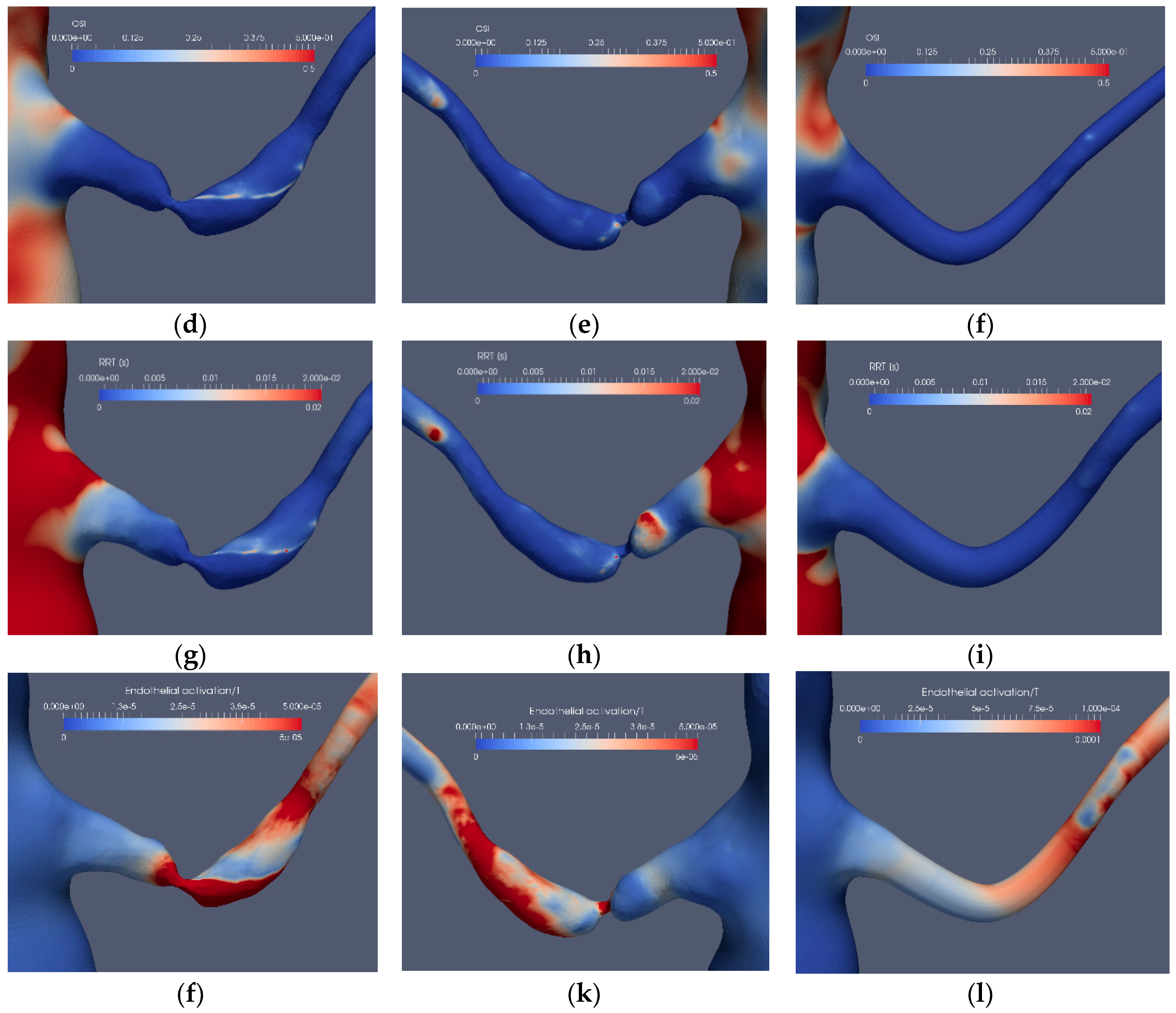
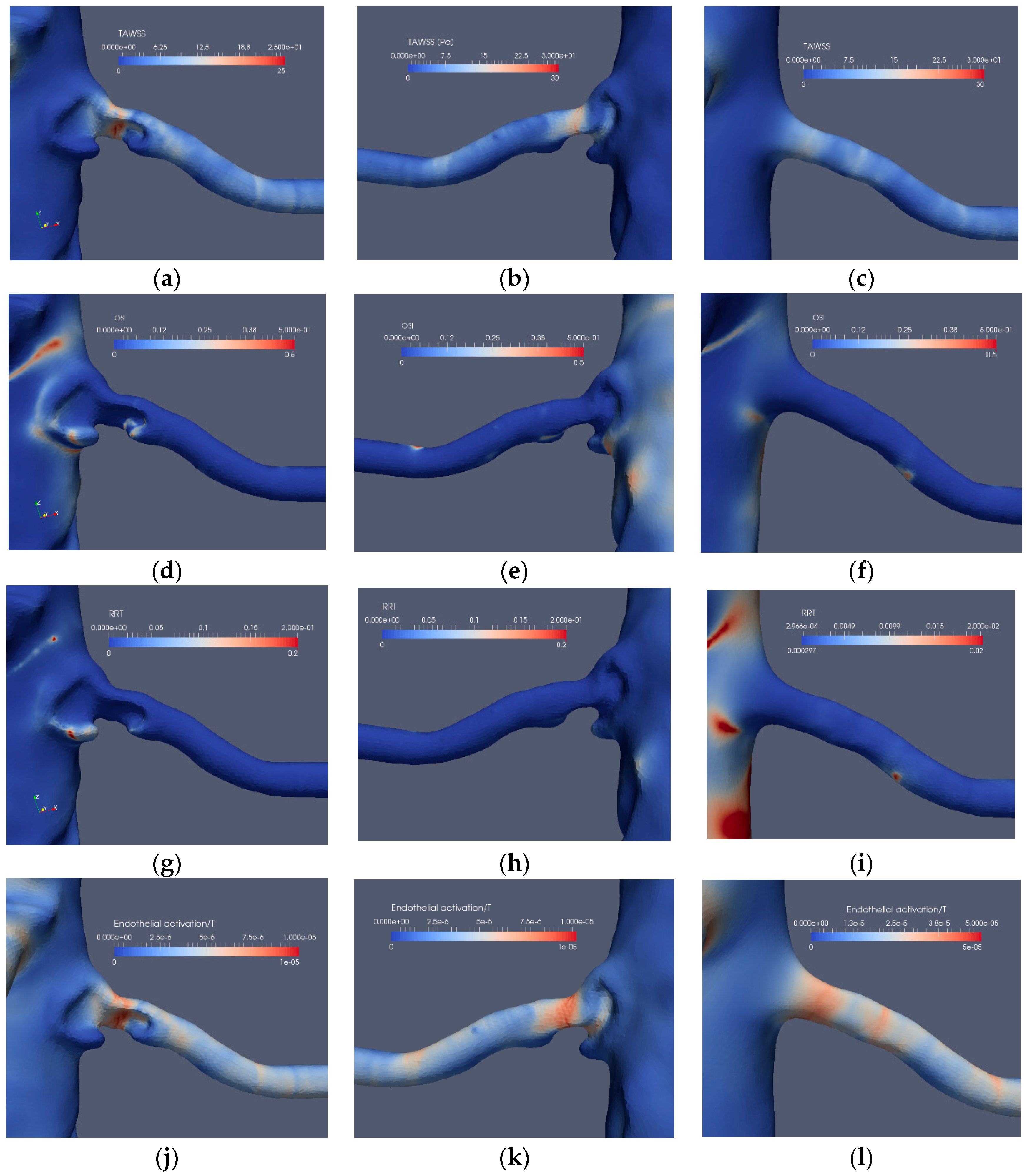
OSI may solely detect the edge of an oscillating separation bubble, independent of the frequency of the oscillation. This effect can be observed in
Figure 9d and
Figure 10d. The separation bubbles formed due to the post-stenotic dilatation were also located by
OSI (
Figure 9e and
Figure 10e). Due to its construction,
OSI has limited value in cases with significant oscillatory
WSS, and it should not be used for assessing future risks for stenosis in revascularized arteries.
The relative residence time, RRT, has its basis in the observation that low flow and low shear regions are prone to the formation of thrombosis and become atherosclerotic (parts of Virchow’s triad). By this concept, prolonged residence time is a good indicator for a low flow region. The definition of RRT (Equation (11)) contains explicitly the viscosity as a parameter. This may lead to possible misinterpretation as RRT is not representing a diffusion process but rather the effect of vorticity. It would probably be more appropriate to replace the TAWSS term by the time average of the near wall vorticity as this would reflect a mechanism for prolonged residence time. In the cases investigated here, it was noted that RRT is largest at separated (high vorticity) regions. The indicator fails for the revascularized arteries as the near wall flow is smoother. For a more detailed prediction of the atherosclerotic process, the concentrations and residence times of cells and molecules would be needed. One possible option to achieve this is to use a Lagrangian Particle Tracking (LPT) approach, directly computing the residence time, instead of using RRT. Additionally, when using LPT, the details of mixing, cell/particle size and weight effects could also be accounted for.
Power law-based models such as Nobili et al. [
30] are phenomenological in character and not designed to reflect the details of the process modeled. The model parameters are adjusted so that the target variable, in our case, the Endothelial Activation Index (EAI), is well-represented. The model does include the history effects of
WSS on the endothelium, which is reasonable. In this sense, EAI differs from the other three indicators as EAI takes
WSS history into account. However, the
WSS history is considered in an unweighted manner. That is, the impact of a large
WSS value is the same, independent of when it occurred. Thereby, cellular response and possibilities of cell repair known to occur are neglected. For the two cases considered here, the EAI model is performing well, both for the stenoted and the smoothed revascularized arteries. However, due to the inherent limitations of the power law approach, we suggest introducing another approach in partial analogy proposed more recently for platelet activation (Soares et al. (2013) and Consolo et al. (2017)). The idea is to add the contribution of various parameters such that the indicator remains bounded and by using dimensionless variables, so that each term has a functional and physical meaning. Such an indicator could, in addition to the local effect of
WSS and the time-limited (or time-weighted) history effect of
WSS, also include the effects of temporal- and spatial-variations of
WSS. In this way, the low and oscillatory
WSS contribution to endothelial activation and atherosclerosis enter explicitly into the expression for the indicator. Platelet activation models lack a repair and/or cellular response mechanism. Such a mechanism could possibly be more important in modeling the endothelial response. Since atherosclerosis is a slow process, it is reasonable to assume that the endothelial cells respond to
WSS, strengthening their ability to withstand the elevated stress. The same applies to the response of the subendothelial matrix to the variability in the
WSS.
In addition to the modeling of the atherosclerotic process on a macroscopic level, there are several other issues related to the models used in the present simulations. As already noted, the RBC transport should account for diffusion due to the lift effect on the cells in the presence of a velocity gradient. The RBC concentration becomes nonuniform that may affect the local viscosity and the WSS by a factor of up to two under the same flow conditions.
Another issue that has to be addressed is the setting of appropriate boundary conditions. As in practically all clinical situations, there is no available data on the flow conditions. To a large extent, such data is less useful since the flow conditions in the aorta vary considerably, depending on the activities of the patient. Thus, the flow in the aorta cannot be set to a single value or percentage of the cardiac output. One could remedy the need for a large number of simulations by including the boundary conditions in the governing equations and use that as a parameter. It is not only the flow but also its redistribution from the aorta that varies. Such a redistribution changes the phase angle between the pressure and flow and also in the renal arteries. Therefore, defining the four outflow conditions, needed by the numerical procedure, is a real problem. The effect of errors in boundary conditions on the global flow behavior may not be pronounced in global terms [
37]. However, the effects of the flow details do enter in a pronounced manner in the
WSS and thereby in the stenosis indicators. Thus, developing clinically appropriate boundary conditions is essential.
















{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}