Diagnosis and Management of Central Nervous System Cryptococcal Infections in HIV-Infected Adults


Abstract
1. Introduction
2. Diagnosis of Cryptococcal Meningitis
3. Management of Cryptococcal Meningitis
3.1. Induction Therapy
3.2. Consolidation Therapy
3.3. Maintenance Therapy
3.4. Management of Intracranial Pressure
3.5. Management of Amphotericin B-Related Toxicities
3.6. ART Initiation
4. Immune Reconstitution Inflammatory Syndrome versus Cryptococcal Meningitis Relapse
5. Special Situations
5.1. Pregnancy
5.2. Cryptococcus neoformans versus C. gattii
5.3. Unmasking Disease
5.4. Cerebral Cryptococcoma
5.5. Asymptomatic Antigenemia
6. Summary
Funding
Acknowledgments
Conflicts of Interest
References
- Lazera, M.S.; Cavalcanti, M.A.S.; Londero, A.T.; Trilles, L.; Nishikawa, M.M.; Wanke, B. Possible primary ecological niche of Cryptococcus neoformans. Med. Mycol. 2000, 38, 379–383. [Google Scholar] [CrossRef] [PubMed]
- Rajasingham, R.; Smith, R.M.; Park, B.J.; Jarvis, J.N.; Govender, N.P.; Chiller, T.M.; Denning, D.W.; Loyse, A.; Boulware, D.R. Global burden of disease of HIV-associated cryptococcal meningitis: An updated analysis. Lancet Infect. Dis. 2017, 17, 873–881. [Google Scholar] [CrossRef]
- Tugume, L.; Rhein, J.; Hullsiek, K.H.; Mpoza, E.; Kiggundu, R.; Ssebambulidde, K.; Schutz, C.; Taseera, K.; Williams, D.A.; Abassi, M.; et al. HIV-associated cryptococcal meningitis occurring at relatively higher CD4 counts. J. Infect. Dis. 2019, 219, 877–883. [Google Scholar] [CrossRef] [PubMed]
- Jarvis, J.N.; Boulle, A.; Loyse, A.; Bicanic, T.; Rebe, K.; Williams, A.; Harrison, T.S.; Meintjes, G. High ongoing burden of cryptococcal disease in Africa despite antiretroviral roll out. AIDS 2009, 23, 1182–1183. [Google Scholar] [CrossRef] [PubMed]
- Kambugu, A.; Meya, D.B.; Rhein, J.; O’Brien, M.; Janoff, E.N.; Ronald, A.R.; Kamya, M.R.; Mayanja-Kizza, H.; Sande, M.A.; Bohjanen, P.R.; et al. Outcomes of cryptococcal meningitis in Uganda before and after the availability of highly active antiretroviral therapy. Clin. Infect. Dis. 2008, 46, 1694–1701. [Google Scholar] [CrossRef]
- Boulware, D.R.; Meya, D.B.; Bergemann, T.L.; Wiesner, D.L.; Rhein, J.; Musubire, A.; Lee, S.J.; Kambugu, A.; Janoff, E.N.; Bohjanen, P.R. Clinical features and serum biomarkers in HIV immune reconstitution inflammatory syndrome after cryptococcal meningitis: A prospective cohort study. PLoS Med. 2010, 7, e1000384. [Google Scholar] [CrossRef]
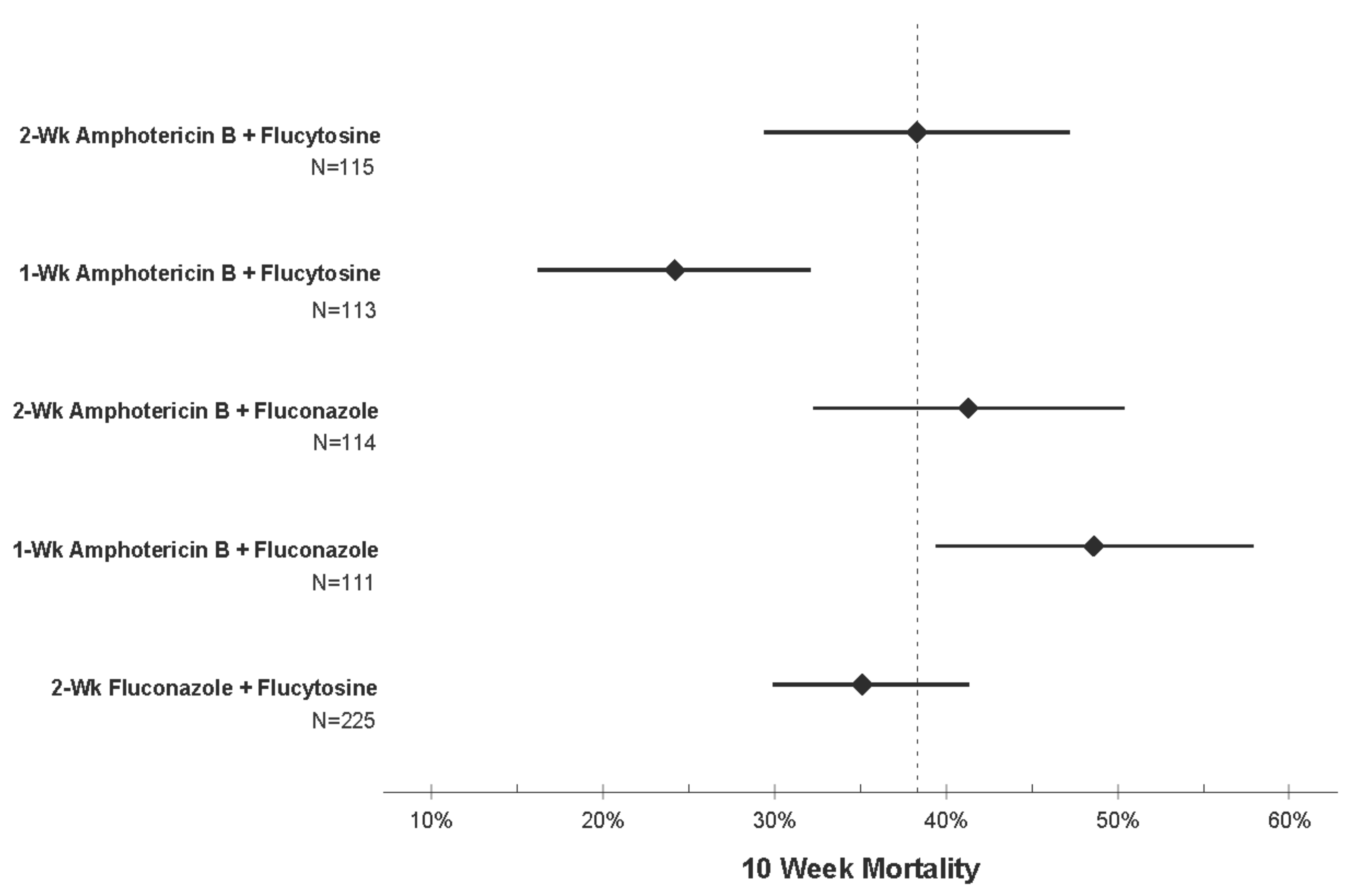
- Day, J.N.; Chau, T.T.H.; Wolbers, M.; Mai, P.P.; Dung, N.T.; Mai, N.H.; Phu, N.H.; Nghia, H.D.; Phong, N.D.; Thai, C.Q.; et al. Combination antifungal therapy for cryptococcal meningitis. N. Engl. J. Med. 2013, 368, 1291–1302. [Google Scholar] [CrossRef]
- Boulware, D.R.; Meya, D.B.; Muzoora, C.; Rolfes, M.A.; Huppler Hullsiek, K.; Musubire, A.; Taseera, K.; Nabeta, H.W.; Schutz, C.; Williams, D.A.; et al. Timing of antiretroviral therapy after diagnosis of cryptococcal meningitis. N. Engl. J. Med. 2014, 370, 2487–2498. [Google Scholar] [CrossRef]
- Montezuma-Rusca, J.M.; Powers, J.H.; Follmann, D.; Wang, J.; Sullivan, B.; Williamson, P.R. Early Fungicidal Activity as a Candidate Surrogate Endpoint for All-Cause Mortality in Cryptococcal Meningitis: A Systematic Review of the Evidence. PLoS ONE 2016, 11, e0159727. [Google Scholar] [CrossRef]
- Dominic, R.S.; Prashanth, H.; Shenoy, S.; Baliga, S. Diagnostic value of latex agglutination in cryptococcal meningitis. J. Lab. Physicians 2009, 1, 67–68. [Google Scholar] [CrossRef]
- Boulware, D.R.; Rolfes, M.A.; Rajasingham, R.; von Hohenberg, M.; Qin, Z.; Taseera, K.; Schutz, C.; Kwizera, R.; Butler, E.K.; Meintjes, G.; et al. Multisite validation of cryptococcal antigen lateral flow assay and quantification by laser thermal contrast. Emerg. Infect. Dis. 2014, 20, 45–53. [Google Scholar] [CrossRef] [PubMed]
- Durski, K.N.; Kuntz, K.M.; Yasukawa, K.; Virnig, B.A.; Meya, D.B.; Boulware, D.R. Cost-effective diagnostic checklists for meningitis in resource-limited settings. J. Acquir. Immune Defic. Syndr. 2013, 63, e101–e108. [Google Scholar] [CrossRef]
- Jongwutiwes, U.; Kiertiburanakul, S.; Sungkanuparph, S. Impact of antiretroviral therapy on the relapse of cryptococcosis and survival of HIV-infected patients with cryptococcal infection. Curr. HIV Res. 2007, 5, 355–360. [Google Scholar] [CrossRef] [PubMed]
- Kwizera, R.; Nguna, J.; Kiragga, A.; Nakavuma, J.; Rajasingham, R.; Boulware, D.R.; Meya, D.B. Performance of cryptococcal antigen lateral flow assay using saliva in Ugandans with CD4 < 100. PLoS ONE 2014, 9, e103156. [Google Scholar] [CrossRef]
- Lindsley, M.D.; Mekha, N.; Baggett, H.C.; Surinthong, Y.; Autthateinchai, R.; Sawatwong, P.; Harris, J.R.; Park, B.J.; Chiller, T.; Balajee, S.A.; et al. Evaluation of a newly developed lateral flow immunoassay for the diagnosis of cryptococcosis. Clin. Infect. Dis. 2011, 53, 321–325. [Google Scholar] [CrossRef] [PubMed]
- Wake, R.M.; Jarvis, J.N.; Harrison, T.S.; Govender, N.P. Brief Report: Point of Care Cryptococcal Antigen Screening: Pipetting Finger-Prick Blood Improves Performance of Immunomycologics Lateral Flow Assay. J. Acquir. Immune Defic. Syndr. 2018, 78, 574–578. [Google Scholar] [CrossRef] [PubMed]
- Williams, D.A.; Kiiza, T.; Kwizera, R.; Kiggundu, R.; Velamakanni, S.; Meya, D.B.; Rhein, J.; Boulware, D.R. Evaluation of Fingerstick Cryptococcal Antigen Lateral Flow Assay in HIV-Infected Persons: A Diagnostic Accuracy Study. Clin. Infect. Dis. 2015, 61, 464–467. [Google Scholar] [CrossRef]
- Mpoza, E.; Mukaremera, L.; Kundura, D.A.; Akampurira, A.; Luggya, T.; Tadeo, K.K.; Pastick, K.A.; Bridge, S.C.; Tugume, L.; Kiggundu, R.; et al. Evaluation of a point-of-care immunoassay test kit ‘StrongStep’ for cryptococcal antigen detection. PLoS ONE 2018, 13, e0190652. [Google Scholar] [CrossRef]
- Kabanda, T.; Siedner, M.J.; Klausner, J.D.; Muzoora, C.; Boulware, D.R. Point-of-care diagnosis and prognostication of cryptococcal meningitis with the cryptococcal antigen lateral flow assay on cerebrospinal fluid. Clin. Infect. Dis. 2014, 58, 113–116. [Google Scholar] [CrossRef]
- Rajasingham, R.; Boulware, D.R. Cryptococcal antigen screening and preemptive treatment—How can we improve survival? Clin. Infect. Dis. 2019. [Google Scholar] [CrossRef]
- Rhein, J.; Bahr, N.C.; Morawski, B.M.; Schutz, C.; Zhang, Y.; Finkelman, M.; Meya, D.B.; Meintjes, G.; Boulware, D.R. Detection of High Cerebrospinal Fluid Levels of (1-->3)-beta-d-Glucan in Cryptococcal Meningitis. Open Forum Infect. Dis. 2014, 1, ofu105. [Google Scholar] [CrossRef] [PubMed]
- Rhein, J.; Bahr, N.C.; Hemmert, A.C.; Cloud, J.L.; Bellamkonda, S.; Oswald, C.; Lo, E.; Nabeta, H.; Kiggundu, R.; Akampurira, A.; et al. Diagnostic performance of a multiplex PCR assay for meningitis in an HIV-infected population in Uganda. Diagn. Microbiol. Infect. Dis. 2016, 84, 268–273. [Google Scholar] [CrossRef] [PubMed]
- Tarumoto, N.; Sakai, J.; Kodana, M.; Kawamura, T.; Ohno, H.; Maesaki, S. Identification of Disseminated Cryptococcosis Using MALDI-TOF MS and Clinical Evaluation. Med. Mycol. J. 2016, 57, E41–E46. [Google Scholar] [CrossRef] [PubMed][Green Version]
- World Health Organization. Rapid Advice: Diagnosis, Prevention and Management of Cryptococcal Disease in HIV-Infected Adults, Adolescents and Children. Available online: www.who.int/hiv/pub/cryptococcal_disease2011 (accessed on 1 January 2019).
- Lofgren, S.; Abassi, M.; Rhein, J.; Boulware, D.R. Recent advances in AIDS-related cryptococcal meningitis treatment with an emphasis on resource limited settings. Expert Rev. Anti-Infect. Ther. 2017, 15, 331–340. [Google Scholar] [CrossRef] [PubMed]
- Veltman, J.A.; Bristow, C.C.; Klausner, J.D. Meningitis in HIV-positive patients in sub-Saharan Africa: A review. J. Int AIDS Soc. 2014, 17, 19184. [Google Scholar] [CrossRef] [PubMed]
- Pappas, P.G.; Chetchotisakd, P.; Larsen, R.A.; Manosuthi, W.; Morris, M.I.; Anekthananon, T.; Sungkanuparph, S.; Supparatpinyo, K.; Nolen, T.L.; Zimmer, L.O.; et al. A phase II randomized trial of amphotericin B alone or combined with fluconazole in the treatment of HIV-associated cryptococcal meningitis. Clin. Infect. Dis. 2009, 48, 1775–1783. [Google Scholar] [CrossRef]
- World Health Organization. Guidelines for the Diagnosis, Prevention and Management of Cryptococcal Disease in HIV-Infected Adults, Adolescents and Children. Available online: http://www.who.int/hiv/pub/guidelines/cryptococcal-disease/en/ (accessed on 1 April 2018).
- Molloy, S.F.; Kanyama, C.; Heyderman, R.S.; Loyse, A.; Kouanfack, C.; Chanda, D.; Mfinanga, S.; Temfack, E.; Lakhi, S.; Lesikari, S.; et al. Antifungal combinations for treatment of cryptococcal meningitis in Africa. N. Engl. J. Med. 2018, 378, 1004–1017. [Google Scholar] [CrossRef]
- Merry, M.; Boulware, D.R. Cryptococcal meningitis treatment strategies affected by the explosive cost of flucytosine in the United States: A cost-effectiveness analysis. Clin. Infect. Dis. 2016, 62, 1564–1568. [Google Scholar] [CrossRef]
- Zhai, B.; Wu, C.; Wang, L.; Sachs, M.S.; Lin, X. The antidepressant sertraline provides a promising therapeutic option for neurotropic cryptococcal infections. Antimicrob. Agents Chemother. 2012, 56, 3758–3766. [Google Scholar] [CrossRef]
- Lewis, R.J.; Angier, M.K.; Williamson, K.S.; Johnson, R.D. Analysis of Sertraline in Postmortem Fluids and Tissues in 11 Aviation Accident Victims. J. Anal. Toxicol. 2013, 37, 208–216. [Google Scholar] [CrossRef]
- Rhein, J.; Hullsiek, K.H.; Tugume, L.; Nuwagira, E.; Mpoza, E.; Evans, E.E.; Kiggundu, R.; Pastick, K.A.; Ssebambulidde, K.; Akampurira, A.; et al. Adjunctive sertraline in HIV-associated cryptococcal meningitis: A randomised, placebo-controlled, double-blind phase 3 trial. Lancet Infect. Dis. 2019, 19. in press. [Google Scholar]
- Hai, T.P.; Van, A.D.; Ngan, N.T.T.; Nhat, L.T.H.; Lan, N.P.H.; Vinh Chau, N.V.; Thwaites, G.E.; Krysan, D.; Day, J.N. The combination of tamoxifen with amphotericin B, but not with fluconazole, has synergistic activity against the majority of clinical isolates of Cryptococcus neoformans. Mycoses 2019. [Google Scholar] [CrossRef] [PubMed]
- Herring, A.C.; Lee, J.; McDonald, R.A.; Toews, G.B.; Huffnagle, G.B. Induction of interleukin-12 and gamma interferon requires tumor necrosis factor alpha for protective T1-cell-mediated immunity to pulmonary Cryptococcus neoformans infection. Infect. Immun. 2002, 70, 2959–2964. [Google Scholar] [CrossRef] [PubMed]
- Huffnagle, G.B.; Toews, G.B.; Burdick, M.D.; Boyd, M.B.; McAllister, K.S.; McDonald, R.A.; Kunkel, S.L.; Strieter, R.M. Afferent phase production of TNF-alpha is required for the development of protective T cell immunity to Cryptococcus neoformans. J. Immunol. 1996, 157, 4529–4536. [Google Scholar] [PubMed]
- Decken, K.; Kohler, G.; Palmer-Lehmann, K.; Wunderlin, A.; Mattner, F.; Magram, J.; Gately, M.K.; Alber, G. Interleukin-12 is essential for a protective Th1 response in mice infected with Cryptococcus neoformans. Infect. Immun. 1998, 66, 4994–5000. [Google Scholar] [PubMed]
- Jain, A.V.; Zhang, Y.; Fields, W.B.; McNamara, D.A.; Choe, M.Y.; Chen, G.H.; Erb-Downward, J.; Osterholzer, J.J.; Toews, G.B.; Huffnagle, G.B.; et al. Th2 but not Th1 immune bias results in altered lung functions in a murine model of pulmonary Cryptococcus neoformans infection. Infect. Immun. 2009, 77, 5389–5399. [Google Scholar] [CrossRef] [PubMed]
- Wiesner, D.L.; Smith, K.D.; Kotov, D.I.; Nielsen, J.N.; Bohjanen, P.R.; Nielsen, K. Regulatory T Cell Induction and Retention in the Lungs Drives Suppression of Detrimental Type 2 Th Cells During Pulmonary Cryptococcal Infection. J. Immunol. 2016, 196, 365–374. [Google Scholar] [CrossRef]
- Wiesner, D.L.; Specht, C.A.; Lee, C.K.; Smith, K.D.; Mukaremera, L.; Lee, S.T.; Lee, C.G.; Elias, J.A.; Nielsen, J.N.; Boulware, D.R.; et al. Chitin recognition via chitotriosidase promotes pathologic type-2 helper T cell responses to cryptococcal infection. PLoS Pathog. 2015, 11, e1004701. [Google Scholar] [CrossRef]
- Jarvis, J.N.; Casazza, J.P.; Stone, H.H.; Meintjes, G.; Lawn, S.D.; Levitz, S.M.; Harrison, T.S.; Koup, R.A. The phenotype of the Cryptococcus-specific CD4+ memory T-cell response is associated with disease severity and outcome in HIV-associated cryptococcal meningitis. J. Infect. Dis. 2013, 207, 1817–1828. [Google Scholar] [CrossRef]
- Jarvis, J.N.; Meintjes, G.; Rebe, K.; Williams, G.N.; Bicanic, T.; Williams, A.; Schutz, C.; Bekker, L.G.; Wood, R.; Harrison, T.S. Adjunctive interferon-gamma immunotherapy for the treatment of HIV-associated cryptococcal meningitis: A randomized controlled trial. AIDS 2012, 26, 1105–1113. [Google Scholar] [CrossRef]
- Brouwer, M.C.; McIntyre, P.; Prasad, K.; van de Beek, D. Corticosteroids for acute bacterial meningitis. Cochrane Database Syst. Rev. 2015. [Google Scholar] [CrossRef] [PubMed]
- Prasad, K.; Singh, M.B.; Ryan, H. Corticosteroids for managing tuberculous meningitis. Cochrane Database Syst Rev. 2016, 4, Cd002244. [Google Scholar] [CrossRef] [PubMed]
- Beardsley, J.; Wolbers, M.; Kibengo, F.M.; Ggayi, A.B.; Kamali, A.; Cuc, N.T.; Binh, T.Q.; Chau, N.V.; Farrar, J.; Merson, L.; et al. Adjunctive Dexamethasone in HIV-Associated Cryptococcal Meningitis. N. Engl. J. Med. 2016, 374, 542–554. [Google Scholar] [CrossRef] [PubMed]
- Bahr, N.; Boulware, D.R.; Marais, S.; Scriven, J.; Wilkinson, R.J.; Meintjes, G. Central nervous system immune reconstitution inflammatory syndrome. Curr. Infect. Dis. Rep. 2013, 15, 583–593. [Google Scholar] [CrossRef] [PubMed]
- Perfect, J.R.; Dismukes, W.E.; Dromer, F.; Goldman, D.L.; Graybill, J.R.; Hamill, R.J.; Harrison, T.S.; Larsen, R.A.; Lortholary, O.; Nguyen, M.H.; et al. Clinical practice guidelines for the management of cryptococcal disease: 2010 update by the infectious diseases society of america. Clin. Infect. Dis. 2010, 50, 291–322. [Google Scholar] [CrossRef] [PubMed]
- Bicanic, T.; Meintjes, G.; Wood, R.; Hayes, M.; Rebe, K.; Bekker, L.G.; Harrison, T. Fungal burden, early fungicidal activity, and outcome in cryptococcal meningitis in antiretroviral-naive or antiretroviral-experienced patients treated with amphotericin B or fluconazole. Clin. Infect. Dis. 2007, 45, 76–80. [Google Scholar] [CrossRef] [PubMed]
- van der Horst, C.M.; Saag, M.S.; Cloud, G.A.; Hamill, R.J.; Graybill, J.R.; Sobel, J.D.; Johnson, P.C.; Tuazon, C.U.; Kerkering, T.; Moskovitz, B.L.; et al. Treatment of cryptococcal meningitis associated with the acquired immunodeficiency syndrome. National Institute of Allergy and Infectious Diseases Mycoses Study Group and AIDS Clinical Trials Group. N. Engl. J. Med. 1997, 337, 15–21. [Google Scholar] [CrossRef] [PubMed]
- Rolfes, M.A.; Rhein, J.; Schutz, C.; Taseera, K.; Nabeta, H.W.; Huppler Hullsiek, K.; Akampuira, A.; Rajasingham, R.; Musubire, A.; Williams, D.A.; et al. Cerebrospinal Fluid Culture Positivity and Clinical Outcomes After Amphotericin-Based Induction Therapy for Cryptococcal Meningitis. Open Forum Infect. Dis. 2015, 2, ofv157. [Google Scholar] [CrossRef]
- Mootsikapun, P.; Chetchotisakd, P.; Anunnatsiri, S.; Choksawadphinyo, K. The efficacy of fluconazole 600 mg/day versus itraconazole 600 mg/day as consolidation therapy of cryptococcal meningitis in AIDS patients. J. Med. Assoc. Thail. 2003, 86, 293–298. [Google Scholar]
- Bozzette, S.A.; Larsen, R.A.; Chiu, J.; Leal, M.A.; Jacobsen, J.; Rothman, P.; Robinson, P.; Gilbert, G.; McCutchan, J.A.; Tilles, J.; et al. A placebo-controlled trial of maintenance therapy with fluconazole after treatment of cryptococcal meningitis in the acquired immunodeficiency syndrome. California Collaborative Treatment Group. N. Engl. J. Med. 1991, 324, 580–584. [Google Scholar] [CrossRef]
- Powderly, W.G.; Saag, M.S.; Cloud, G.A.; Robinson, P.; Meyer, R.D.; Jacobson, J.M.; Graybill, J.R.; Sugar, A.M.; McAuliffe, V.J.; Follansbee, S.E.; et al. A controlled trial of fluconazole or amphotericin B to prevent relapse of cryptococcal meningitis in patients with the acquired immunodeficiency syndrome. The NIAID AIDS Clinical Trials Group and Mycoses Study Group. N. Engl. J. Med. 1992, 326, 793–798. [Google Scholar] [CrossRef]
- Saag, M.S.; Cloud, G.A.; Graybill, J.R.; Sobel, J.D.; Tuazon, C.U.; Johnson, P.C.; Fessel, W.J.; Moskovitz, B.L.; Wiesinger, B.; Cosmatos, D.; et al. A comparison of itraconazole versus fluconazole as maintenance therapy for AIDS-associated cryptococcal meningitis. National Institute of Allergy and Infectious Diseases Mycoses Study Group. Clin. Infect. Dis. 1999, 28, 291–296. [Google Scholar] [CrossRef] [PubMed]
- Loyse, A.; Wainwright, H.; Jarvis, J.N.; Bicanic, T.; Rebe, K.; Meintjes, G.; Harrison, T.S. Histopathology of the arachnoid granulations and brain in HIV-associated cryptococcal meningitis: Correlation with cerebrospinal fluid pressure. AIDS 2010, 24, 405–410. [Google Scholar] [CrossRef] [PubMed]
- Moodley, A.; Rae, W.; Bhigjee, A. Visual loss in HIV-associated cryptococcal meningitis: A case series and review of the mechanisms involved. S. Afr. J. HIV Med. 2015, 16, 305. [Google Scholar] [CrossRef]
- Loyse, A.; Moodley, A.; Rich, P.; Molloy, S.F.; Bicanic, T.; Bishop, L.; Rae, W.I.; Bhigjee, A.I.; Loubser, N.D.; Michowicz, A.J.; et al. Neurological, visual, and MRI brain scan findings in 87 South African patients with HIV-associated cryptococcal meningoencephalitis. J. Infect. 2015, 70, 668–675. [Google Scholar] [CrossRef] [PubMed]
- Johnston, S.R.; Corbett, E.L.; Foster, O.; Ash, S.; Cohen, J. Raised intracranial pressure and visual complications in AIDS patients with cryptococcal meningitis. J. Infect. 1992, 24, 185–189. [Google Scholar] [CrossRef]
- Graybill, J.R.; Sobel, J.; Saag, M.; van Der Horst, C.; Powderly, W.; Cloud, G.; Riser, L.; Hamill, R.; Dismukes, W. Diagnosis and management of increased intracranial pressure in patients with AIDS and cryptococcal meningitis. The NIAID Mycoses Study Group and AIDS Cooperative Treatment Groups. Clin. Infect. Dis. 2000, 30, 47–54. [Google Scholar] [CrossRef] [PubMed]
- Bicanic, T.; Brouwer, A.E.; Meintjes, G.; Rebe, K.; Limmathurotsakul, D.; Chierakul, W.; Teparrakkul, P.; Loyse, A.; White, N.J.; Wood, R.; et al. Relationship of cerebrospinal fluid pressure, fungal burden and outcome in patients with cryptococcal meningitis undergoing serial lumbar punctures. AIDS 2009, 23, 701–706. [Google Scholar] [CrossRef]
- Jarvis, J.N.; Bicanic, T.; Loyse, A.; Namarika, D.; Jackson, A.; Nussbaum, J.C.; Longley, N.; Muzoora, C.; Phulusa, J.; Taseera, K.; et al. Determinants of mortality in a combined cohort of 501 patients with HIV-associated Cryptococcal meningitis: Implications for improving outcomes. Clin. Infect. Dis. 2014, 58, 736–745. [Google Scholar] [CrossRef]
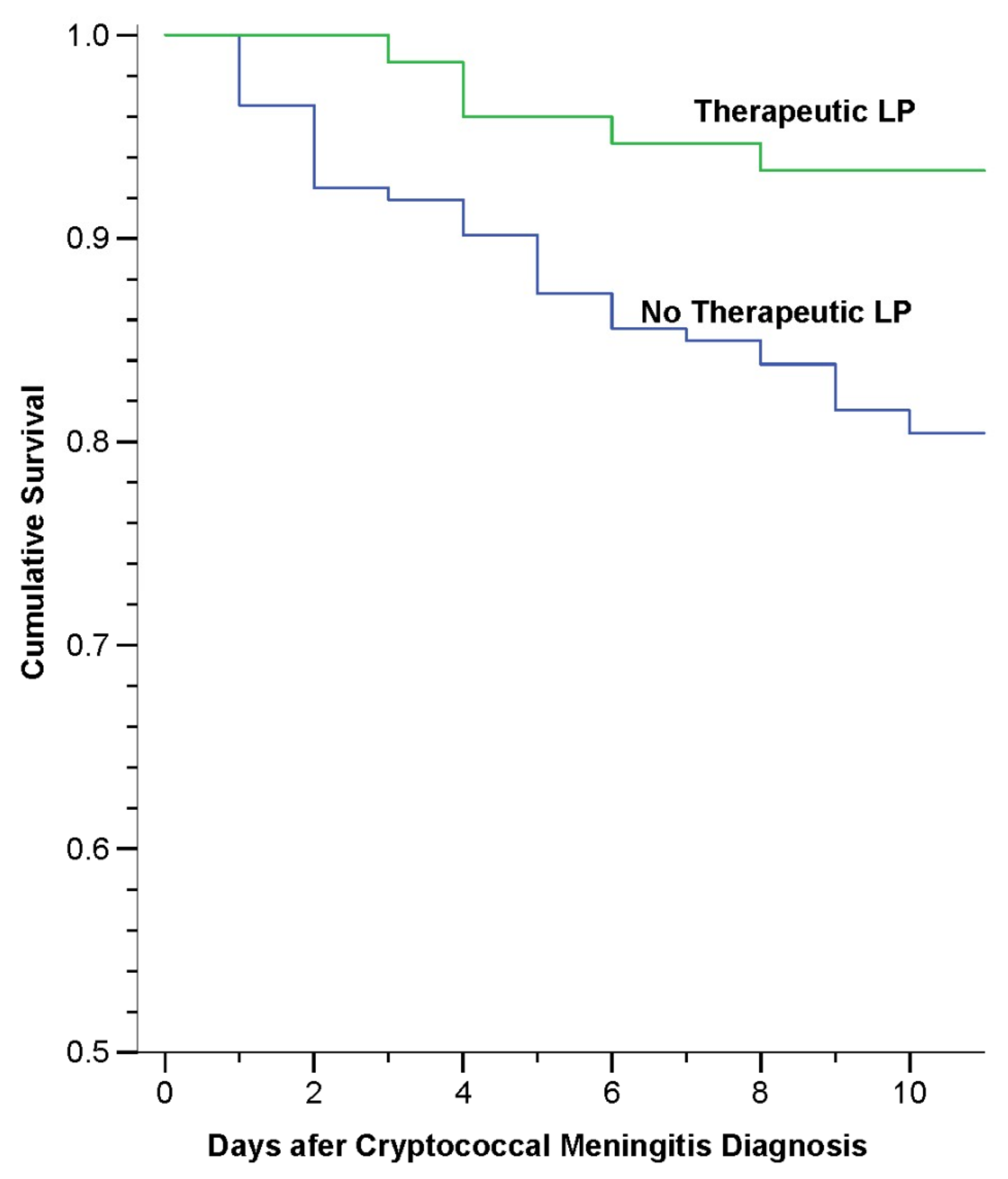
- Rolfes, M.A.; Hullsiek, K.H.; Rhein, J.; Nabeta, H.W.; Taseera, K.; Schutz, C.; Musubire, A.; Rajasingham, R.; Williams, D.A.; Thienemann, F.; et al. The effect of therapeutic lumbar punctures on acute mortality from cryptococcal meningitis. Clin. Infect. Dis. 2014, 59, 1607–1614. [Google Scholar] [CrossRef]
- Orem, J.; Tindyebwa, L.; Twinoweitu, O.; Mukasa, B.; Tomberland, M.; Mbidde, E.K. Feasibility study of serial lumbar puncture and acetazolamide combination in the management of elevated cerebrospinal fluid pressure in AIDS patients with cryptococcal meningitis in Uganda. Trop. Dr. 2005, 35, 19–21. [Google Scholar] [CrossRef] [PubMed]
- Newton, P.N.; Thai le, H.; Tip, N.Q.; Short, J.M.; Chierakul, W.; Rajanuwong, A.; Pitisuttithum, P.; Chasombat, S.; Phonrat, B.; Maek, A.N.W.; et al. A randomized, double-blind, placebo-controlled trial of acetazolamide for the treatment of elevated intracranial pressure in cryptococcal meningitis. Clin. Infect. Dis. 2002, 35, 769–772. [Google Scholar] [CrossRef] [PubMed]
- Siberry, G.K.; Tessema, S. Immune reconstitution syndrome precipitated by bacille Calmette Guerin after initiation of antiretroviral therapy. Pediatr. Infect. Dis. J. 2006, 25, 648–649. [Google Scholar] [CrossRef] [PubMed]
- Bahr, N.C.; Rolfes, M.A.; Musubire, A.; Nabeta, H.; Williams, D.A.; Rhein, J.; Kambugu, A.; Meya, D.B.; Boulware, D.R. Standardized electrolyte supplementation and fluid management improves survival during amphotericin therapy for cryptococcal meningitis in resource-limited settings. Open Forum Infect. Dis. 2014, 1, ofu070. [Google Scholar] [CrossRef] [PubMed]
- Masur, H.; Brooks, J.T.; Benson, C.A.; Holmes, K.K.; Pau, A.K.; Kaplan, J.E. Prevention and treatment of opportunistic infections in HIV-infected adults and adolescents: Updated Guidelines from the Centers for Disease Control and Prevention, National Institutes of Health, and HIV Medicine Association of the Infectious Diseases Society of America. Clin. Infect. Dis. 2014, 58, 1308–1311. [Google Scholar] [CrossRef] [PubMed]
- Hamill, R.J. Amphotericin B formulations: A comparative review of efficacy and toxicity. Drugs 2013, 73, 919–934. [Google Scholar] [CrossRef]
- Khoo, S.H.; Bond, J.; Denning, D.W. Administering amphotericin B—A practical approach. J. Antimicrob. Chemother. 1994, 33, 203–213. [Google Scholar] [CrossRef]
- Sawaya, B.P.; Briggs, J.P.; Schnermann, J. Amphotericin B nephrotoxicity: The adverse consequences of altered membrane properties. J. Am. Soc. Nephrol. 1995, 6, 154–164. [Google Scholar]
- Yeo, E.J.; Ryu, J.H.; Cho, Y.S.; Chun, Y.S.; Huang, L.E.; Kim, M.S.; Park, J.W. Amphotericin B blunts erythropoietin response to hypoxia by reinforcing FIH-mediated repression of HIF-1. Blood 2006, 107, 916–923. [Google Scholar] [CrossRef]
- Bicanic, T.; Bottomley, C.; Loyse, A.; Brouwer, A.E.; Muzoora, C.; Taseera, K.; Jackson, A.; Phulusa, J.; Hosseinipour, M.C.; van der Horst, C.; et al. Toxicity of Amphotericin B Deoxycholate-Based Induction Therapy in Patients with HIV-Associated Cryptococcal Meningitis. Antimicrob. Agents Chemother. 2015, 59, 7224–7231. [Google Scholar] [CrossRef]
- Tugume, L.; Morawski, B.M.; Abassi, M.; Bahr, N.C.; Kiggundu, R.; Nabeta, H.W.; Hullsiek, K.H.; Taseera, K.; Musubire, A.K.; Schutz, C.; et al. Prognostic implications of baseline anaemia and changes in haemoglobin concentrations with amphotericin B therapy for cryptococcal meningitis. HIV Med. 2017, 18, 13–20. [Google Scholar] [CrossRef]
- Diehl, J.W.; Hullsiek, K.H.; Okirwoth, M.; Stephens, N.; Abassi, M.; Rhein, J.; Meya, D.B.; Boulware, D.R.; Musubire, A.K. Cerebral Oximetry for Detecting High-mortality Risk Patients with Cryptococcal Meningitis. Open Forum Infect. Dis. 2018, 5, ofy105. [Google Scholar] [CrossRef] [PubMed]
- Burgess, K.; Price, P.; James, I.R.; Stone, S.F.; Keane, N.M.; Lim, A.Y.; Warmington, J.R.; French, M.A. Interferon-gamma responses to Candida recover slowly or remain low in immunodeficient HIV patients responding to ART. J. Clin. Immunol. 2006, 26, 160–167. [Google Scholar] [CrossRef] [PubMed]
- Mateo-Urdiales, A.; Johnson, S.; Smith, R.; Nachega, J.B.; Eshun-Wilson, I. Rapid initiation of antiretroviral therapy for people living with HIV. Cochrane Database Syst. Rev. 2019, 6, Cd012962. [Google Scholar] [CrossRef] [PubMed]
- Haddow, L.J.; Colebunders, R.; Meintjes, G.; Lawn, S.D.; Elliott, J.H.; Manabe, Y.C.; Bohjanen, P.R.; Sungkanuparph, S.; Easterbrook, P.J.; French, M.A.; et al. Cryptococcal immune reconstitution inflammatory syndrome in HIV-1-infected individuals: Proposed clinical case definitions. Lancet Infect. Dis. 2010, 10, 791–802. [Google Scholar] [CrossRef]
- Longley, N.; Harrison, T.S.; Jarvis, J.N. Cryptococcal immune reconstitution inflammatory syndrome. Curr. Opin. Infect. Dis. 2013, 26, 26–34. [Google Scholar] [CrossRef] [PubMed]
- Katchanov, J.; Blechschmidt, C.; Nielsen, K.; Branding, G.; Arasteh, K.; Tintelnot, K.; Meintjes, G.; Boulware, D.R.; Stocker, H. Cryptococcal meningoencephalitis relapse after an eight-year delay: An interplay of infection and immune reconstitution. Int. J. STD AIDS 2015, 26, 912–914. [Google Scholar] [CrossRef] [PubMed]
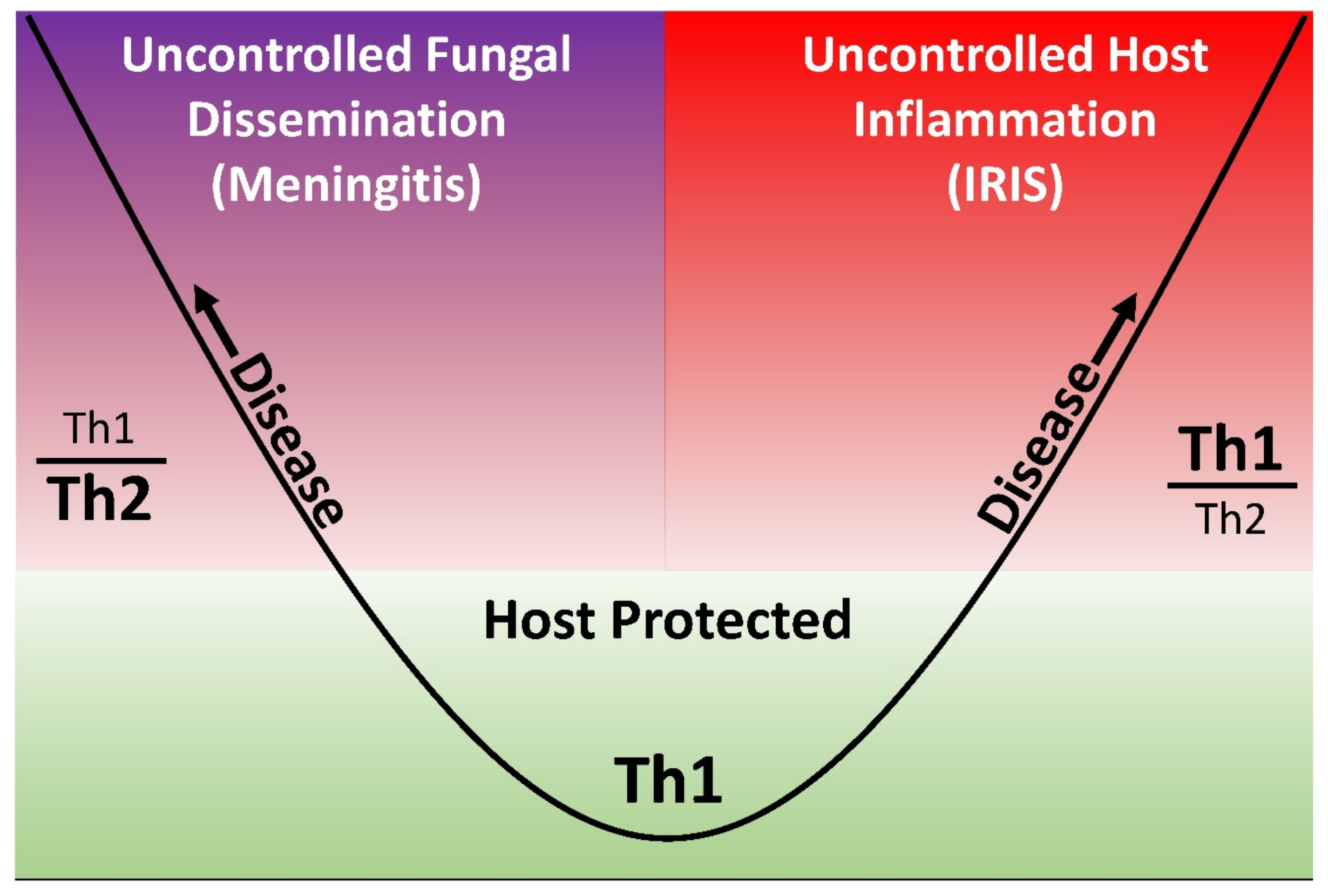
- Pirofski, L.-A.; Casadevall, A. Immune-Mediated Damage Completes the Parabola: Cryptococcus neoformans Pathogenesis Can Reflect the Outcome of a Weak or Strong Immune Response. mBio 2017, 8, e02063–e02017. [Google Scholar] [CrossRef]
- Boulware, D.R.; Bonham, S.C.; Meya, D.B.; Wiesner, D.L.; Park, G.S.; Kambugu, A.; Janoff, E.N.; Bohjanen, P.R. Paucity of initial cerebrospinal fluid inflammation in cryptococcal meningitis is associated with subsequent immune reconstitution inflammatory syndrome. J. Infect. Dis. 2010, 202, 962–970. [Google Scholar] [CrossRef]
- Gamaletsou, M.N.; Sipsas, N.V.; Kontoyiannis, D.P.; Tsiakalos, A.; Kontos, A.N.; Stefanou, I.; Kordossis, T. Successful salvage therapy of refractory HIV-related cryptococcal meningitis with the combination of liposomal amphotericin B, voriconazole, and recombinant interferon-gamma. Diagn. Microbiol. Infect. Dis. 2012, 74, 409–411. [Google Scholar] [CrossRef]
- Shelburne, S.A., 3rd; Darcourt, J.; White, A.C., Jr.; Greenberg, S.B.; Hamill, R.J.; Atmar, R.L.; Visnegarwala, F. The role of immune reconstitution inflammatory syndrome in AIDS-related Cryptococcus neoformans disease in the era of highly active antiretroviral therapy. Clin. Infect. Dis. 2005, 40, 1049–1052. [Google Scholar] [CrossRef]
- Brunel, A.S.; Reynes, J.; Tuaillon, E.; Rubbo, P.A.; Lortholary, O.; Montes, B.; Le Moing, V.; Makinson, A. Thalidomide for steroid-dependent immune reconstitution inflammatory syndromes during AIDS. AIDS 2012, 26, 2110–2112. [Google Scholar] [CrossRef]
- Sitapati, A.M.; Kao, C.L.; Cachay, E.R.; Masoumi, H.; Wallis, R.S.; Mathews, W.C. Treatment of HIV-related inflammatory cerebral cryptococcoma with adalimumab. Clin. Infect. Dis. 2010, 50, e7–e10. [Google Scholar] [CrossRef]
- Molgaard-Nielsen, D.; Pasternak, B.; Hviid, A. Use of oral fluconazole during pregnancy and the risk of birth defects. N. Engl. J. Med. 2013, 369, 830–839. [Google Scholar] [CrossRef]
- Moudgal, V.V.; Sobel, J.D. Antifungal drugs in pregnancy: A review. Expert Opin. Drug Saf. 2003, 2, 475–483. [Google Scholar] [CrossRef]
- Rhein, J.; Hullsiek, K.H.; Evans, E.E.; Tugume, L.; Nuwagira, E.; Ssebambulidde, K.; Kiggundu, R.; Mpoza, E.; Musubire, A.K.; Bangdiwala, A.S.; et al. Detrimental Outcomes of Unmasking Cryptococcal Meningitis With Recent ART Initiation. Open Forum Infect. Dis. 2018, 5, ofy122. [Google Scholar] [CrossRef]
- Speed, B.; Dunt, D. Clinical and host differences between infections with the two varieties of Cryptococcus neoformans. Clin. Infect. Dis. 1995, 21, 28–34. [Google Scholar] [CrossRef]
- Hongsakul, K.; Laothamatas, J. Computer tomographic findings of the brain in HIV-patients at Ramathibodi Hospital. J. Med. Assoc. Thail. 2008, 91, 895–907. [Google Scholar]
- Meya, D.B.; Manabe, Y.C.; Castelnuovo, B.; Cook, B.A.; Elbireer, A.M.; Kambugu, A.; Kamya, M.R.; Bohjanen, P.R.; Boulware, D.R. Cost-effectiveness of serum cryptococcal antigen screening to prevent deaths among HIV-infected persons with a CD4 + cell count < or = 100 cells/microL who start HIV therapy in resource-limited settings. Clin. Infect. Dis. 2010, 51, 448–455. [Google Scholar] [CrossRef]
- Musubire, A.K.; Boulware, D.R.; Meya, D.B.; Rhein, J. Diagnosis and Management of Cryptococcal Relapse. J. AIDS Clin. Res. 2013, (Suppl. 3). pii:S3-003. [Google Scholar] [CrossRef]
- Nalintya, E.; Meya, D.B.; Lofgren, S.; Huppler Hullsiek, K.; Boulware, D.R.; Rajasingham, R. A Prospective Evaluation of a Multisite Cryptococcal Screening and Treatment Program in HIV Clinics in Uganda. J. Acquir. Immune Defic. Syndr. 2018, 78, 231–238. [Google Scholar] [CrossRef]
- Butler, E.K.; Boulware, D.R.; Bohjanen, P.R.; Meya, D.B. Long term 5-year survival of persons with cryptococcal meningitis or asymptomatic subclinical antigenemia in Uganda. PLoS ONE 2012, 7, e51291. [Google Scholar] [CrossRef]
- Mfinanga, S.; Chanda, D.; Kivuyo, S.L.; Guinness, L.; Bottomley, C.; Simms, V.; Chijoka, C.; Masasi, A.; Kimaro, G.; Ngowi, B.; et al. Cryptococcal meningitis screening and community-based early adherence support in people with advanced HIV infection starting antiretroviral therapy in Tanzania and Zambia: An open-label, randomised controlled trial. Lancet 2015, 385, 2173–2182. [Google Scholar] [CrossRef]
- Letang, E.; Muller, M.C.; Ntamatungiro, A.J.; Kimera, N.; Faini, D.; Furrer, H.; Battegay, M.; Tanner, M.; Hatz, C.; Boulware, D.R.; et al. Cryptococcal Antigenemia in Immunocompromised Human Immunodeficiency Virus Patients in Rural Tanzania: A Preventable Cause of Early Mortality. Open Forum Infect. Dis. 2015, 2, ofv046. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Medication and Dose | Week 1 | Week 2 | Week 3–10 | Week > 10 |
|---|---|---|---|---|
| Amphotericin B (1.0 mg/kg/day) + flucytosine 100 mg/kg/day | X a | |||
| Fluconazole 1200 mg daily | X | |||
| Fluconazole 800 mg daily | X | |||
| Fluconazole 200 mg daily | Through 12 months | |||
| Treatment Phase | Induction Therapy | Consolidation | Maintenance | |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Skipper, C.; Abassi, M.; Boulware, D.R. Diagnosis and Management of Central Nervous System Cryptococcal Infections in HIV-Infected Adults. J. Fungi 2019, 5, 65. https://doi.org/10.3390/jof5030065
Skipper C, Abassi M, Boulware DR. Diagnosis and Management of Central Nervous System Cryptococcal Infections in HIV-Infected Adults. Journal of Fungi. 2019; 5(3):65. https://doi.org/10.3390/jof5030065
Chicago/Turabian StyleSkipper, Caleb, Mahsa Abassi, and David R Boulware. 2019. "Diagnosis and Management of Central Nervous System Cryptococcal Infections in HIV-Infected Adults" Journal of Fungi 5, no. 3: 65. https://doi.org/10.3390/jof5030065
APA StyleSkipper, C., Abassi, M., & Boulware, D. R. (2019). Diagnosis and Management of Central Nervous System Cryptococcal Infections in HIV-Infected Adults. Journal of Fungi, 5(3), 65. https://doi.org/10.3390/jof5030065