Rehabilitative Support for Persons with Dementia and Their Families to Acquire Self-Management Attitude and Improve Social Cognition and Sense of Cognitive Empathy


{kind=link}
Abstract
:1. Dementia and Social Interaction
1.1. Social Cognition in Dementia
1.2. Difficulties in Social Interaction Due to Decline in Social Cognition and Other Cognitive Function
2. Rehabilitation for Person with Dementia to Improve Social Health
2.1. Social Health in Dementia
2.2. Dementia Rehabilitation from the Perspective of International Classification of Functioning, Disability and Health
2.3. Occupational Therapy for People with Dementia
3. Proposal of Rehabilitation Support Using Communication via Activities: Co-Beneficial Relationship-Based Rehabilitation
3.1. Rehabilitation Support for People with Dementia: Social Reserves
3.2. Rehabilitation Support for the Family Members of People with Dementia: Cognitive Empathy
3.3. Role of the Practitioners
3.4. Characteristics of the Rehabilitation Program
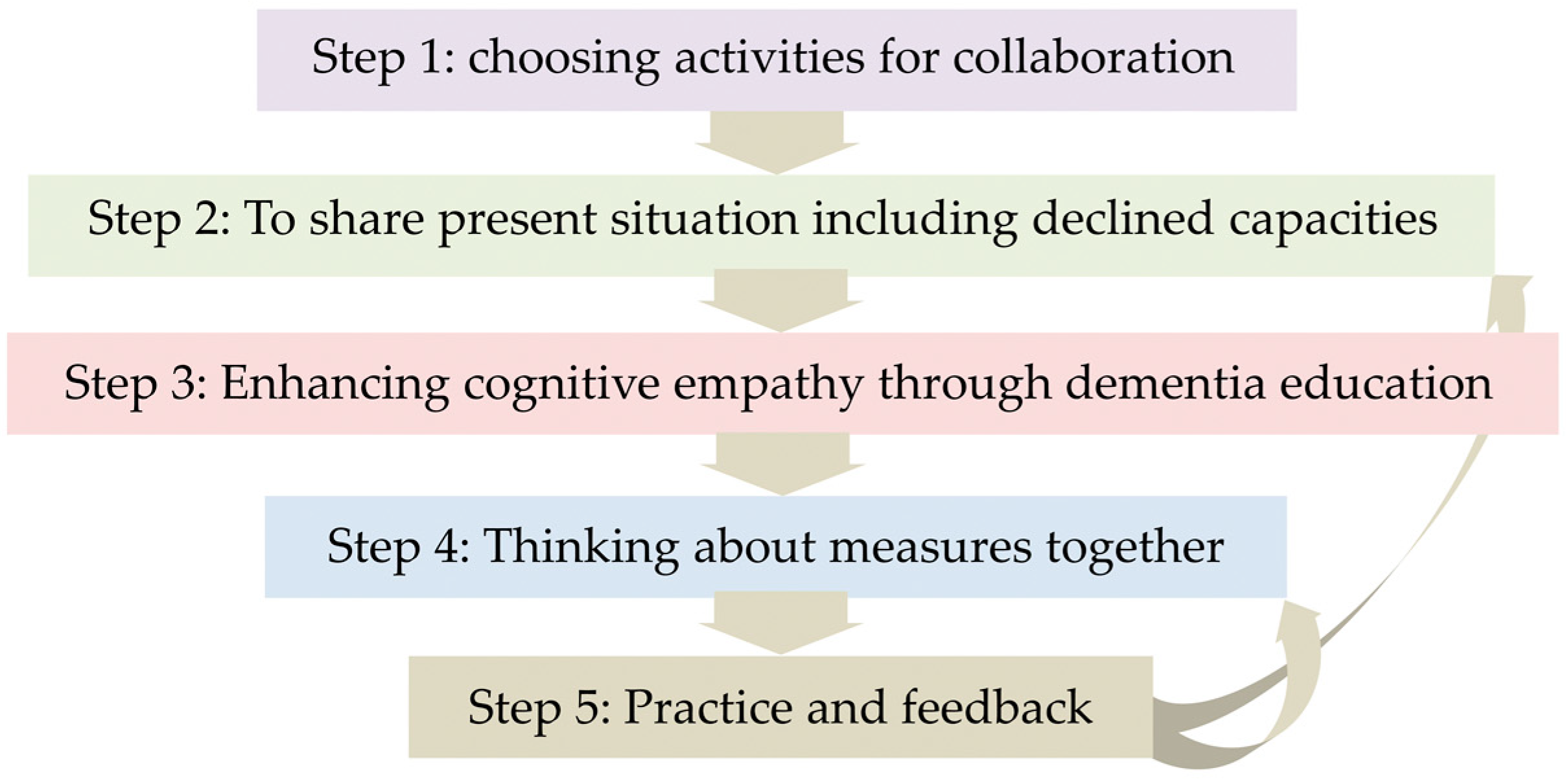
4. Intervention Process
- First, listen without interrupting.
- Then, confirm the person’s intended meaning by conversing with them.
- Supplement the missing parts, if necessary and in such situations, use the words that the person with dementia has used, without paraphrasing.
- Confirm the comprehended meaning step by step and reiterate the understood idea (this is the attitude of cognitive empathy).
- Present alternatives, as open questions are difficult for them to configure answers.
- Questions should be divided into small steps and the session should proceed after confirming the steps. Furthermore, it is desirable to obtain feedback and emphasize the good points.
Expected Effects
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders: DSM-5; Psychiatric Association Publishing: Arlington, TX, USA, 2013. [Google Scholar]
- Schaafsma, S.M.; Pfaff, D.W.; Spunt, R.P.; Adolphs, R. Deconstructing and reconstructing theory of mind. Trends Cogn. Sci. 2015, 19, 65–72. [Google Scholar] [CrossRef] [PubMed]
- Bora, E.; Walterfang, M.; Velakoulis, D. Theory of mind in behavioural-variant frontotemporal dementia and Alzheimer’s disease: A meta-analysis. J. Neurol. Neurosurg. Psychiatry 2015, 86, 714–719. [Google Scholar] [CrossRef] [PubMed]
- Sandoz, M.; Demonet, J.F.; Fossard, M. Theory of mind and cognitive processes in aging and Alzheimer type dementia: A systematic review. Aging Ment. Health 2014, 18, 815–827. [Google Scholar] [CrossRef] [PubMed]
- Yamaguchi, T.; Maki, Y.; Takatama, M.; Yamaguchi, H. Gullibility may be a warning sign of Alzheimer’s disease dementia. Int. Psychogeriatr. 2018, 25, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Yamaguchi, T.; Maki, Y.; Yamaguchi, H. Pitfall Intention Explanation Task with Clue Questions (Pitfall task): Assessment of comprehending other people’s behavioral intentions in Alzheimer’s disease. Int. Psychogeriatr. 2012, 24, 1919–1926. [Google Scholar] [CrossRef] [PubMed]
- Starkstein, S.E.; Jorge, R.; Mizrahi, R.; Robinson, R.G. A diagnostic formulation for anosognosia in Alzheimer’s disease. J. Neurol. Neurosurg. Psychiatry 2006, 77, 719–725. [Google Scholar] [CrossRef] [PubMed]
- Spalletta, G.; Girardi, P.; Caltagirone, C.; Orfei, M.D. Anosognosia and neuropsychiatric symptoms and disorders in mild Alzheimer disease and mild cognitive impairment. J. Alzheimers Dis. 2012, 29, 761–772. [Google Scholar] [CrossRef] [PubMed]
- Mograbi, D.C.; Brown, R.G.; Morris, R.G. Anosognosia in Alzheimer’s disease—The petrified self. Conscious Cogn. 2009, 18, 989–1003. [Google Scholar] [CrossRef] [PubMed]
- Huber, M.; Green, L.; Jadad, A.R.; Lorig, K.; Schnabel, P. How should we define health? BMJ 2011, 343, d4163. [Google Scholar] [CrossRef] [PubMed]
- Dröes, R.M.; Chattat, R.; Diaz, A.; Gove, D.; Graff, M.; Murphy, K.; Verbeek, H.; Vernooij-Dassen, M.; Clare, L.; Johannessen, A.; et al. Social health and dementia: A European consensus on the operationalization of the concept and directions for research and practice. Aging Ment. Health. 2017, 21, 4–17. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. International Classification of Functioning, Disability and Health (ICF). 2017. Available online: http://www.who.int/classifications/icf/en/ (accessed on 7 February 2019).
- American Occupational Therapy Association. Occupational Therapy Practice Framework: Domain and Process, 3rd Ed. Am. J. Occup. Ther. 2017, 68, S1–S48. [Google Scholar] [CrossRef]
- De Coninck, L.; Bekkering, G.E.; Bouckaert, L.; Declercq, A.; Graff, M.J.L.; Aertgeerts, B. Home- and community-based occupational therapy improves functioning in frail older people: A systematic review. J. Am. Geriatr. Soc. 2017, 65, 1863–1869. [Google Scholar] [CrossRef] [PubMed]
- Mallfield, S.; Molitor, W.L. Occupational therapy interventions supporting social participation and leisure engagement for community-dwelling older adults: A systematic review. Am. J. Occup. Ther. 2018, 72, 7204190020p1–7204190020p8. [Google Scholar] [CrossRef] [PubMed]
- Maki, Y.; Sakurai, T.; Okochi, J.; Yamaguchi, H.; Toba, K. Rehabilitation to live better with dementia. Geriatr. Gerontol. Int. 2018, 18, 1529–1536. [Google Scholar] [CrossRef] [PubMed]
- American Occupational Therapy Association. Productive Aging. Available online: https://www.aota.org/Practice/Productive-Aging.aspx (accessed on 7 February 2019).
- Gitlin, L.N.; Arthur, P.; Piersol, C.; Hessels, V.; Wu, S.S.; Dai, Y.; Mann, W.C. Targeting behavioral symptoms and functional decline in dementia: A randomized clinical trial. J. Am. Geriatr. Soc. 2018, 66, 339–345. [Google Scholar] [CrossRef] [PubMed]
- Gitlin, L.N.; Marx, K.A.; Alonzi, D.; Kvedar, T.; Moody, J.; Trahan, M.; Van Haitsma, K. Feasibility of the Tailored Activity Program for Hospitalized (TAP-H) Patients with Behavioral Symptoms. Gerontologist 2017, 57, 575–584. [Google Scholar] [CrossRef] [PubMed]
- Gitlin, L.N.; Winter, L.; Vause Earland, T.; Adel Herge, E.; Chernett, N.L.; Piersol, C.V.; Burke, J.P. The Tailored Activity Program to reduce behavioral symptoms in individuals with dementia: Feasibility, acceptability and replication potential. Gerontologist 2009, 49, 428–439. [Google Scholar] [CrossRef] [PubMed]
- Gitlin, L.N.; Winter, L.; Burke, J.; Chernett, N.; Dennis, M.P.; Hauck, W.W. Tailored activities to manage neuropsychiatric behaviors in persons with dementia and reduce caregiver burden: A randomized pilot study. Am. J. Geriatr. Psychiatry 2008, 6, 229–239. [Google Scholar] [CrossRef]
- Fliss, R.; Le Gall, D.; Etcharry-Bouyx, F.; Chauviré, V.; Desgranges, B.; Allain, P. Theory of Mind and social reserve: Alternative hypothesis of progressive Theory of Mind decay during different stages of Alzheimer’s disease. Soc. Neurosci. 2016, 11, 409–423. [Google Scholar] [CrossRef] [PubMed]
- Decety, J.; Yoder, K.J. Empathy and motivation for justice: Cognitive empathy and concern but not emotional empathy, predict sensitivity to injustice for others. Soc. Neurosci. 2016, 11, 1–14. [Google Scholar] [CrossRef] [PubMed]
- Kitwood, T. Dementia Reconsidered: The Person Comes First (Rethinking Ageing Series); Open University Press: London, UK, 1997. [Google Scholar]
- Alzheimer’s Society. Person-Centered Care. Available online: https://www.alzheimers.org.uk/about-dementia/treatments/person-centred-care (accessed on 7 February 2019).
- Yamaguchi, H.; Maki, Y.; Yamagami, T. Overview of non-pharmacological intervention for dementia and principles of brain-activating rehabilitation. Psychogeriatrics 2010, 10, 206–213. [Google Scholar] [CrossRef] [PubMed]
- Woods, B.; Aguirre, E.; Spector, A.E.; Orrell, M. Cognitive stimulation to improve cognitive functioning in people with dementia. Cochrane Database Syst. Rev. 2012, 2, CD001120. [Google Scholar] [CrossRef] [PubMed]
- Clare, L.; Woods, R.T.; Moniz Cook, E.D.; Orrell, M.; Spector, A. Cognitive rehabilitation and cognitive training for early-stage Alzheimer’s disease and vascular dementia. Cochrane Database Syst. Rev. 2013, 6, CD003260. [Google Scholar]
- van der Steen, J.T.; Smaling, H.J.; van der Wouden, J.C.; Bruinsma, M.S.; Scholten, R.J.; Vink, A.C. Music-based therapeutic interventions for people with dementia. Cochrane Database Syst. Rev. 2018, 23, CD003477. [Google Scholar] [CrossRef] [PubMed]
- Woods, B.; O’Philbin, L.; Farrell, E.M.; Spector, A.E.; Orrell, M. Reminiscence therapy for dementia. Cochrane Database Syst. Rev. 2018, 3, CD001120. [Google Scholar] [CrossRef] [PubMed]
- Maki, Y. A reappraisal of the evidence of non-pharmacological intervention for people with dementia. J. Geriatr. Care Res. 2018, 5, 41–42. [Google Scholar]
- Clare, L. Rehabilitation for people living with dementia: A practical framework of positive support. PLoS Med. 2017, 14, e1002245. [Google Scholar] [CrossRef] [PubMed]
- van Paasschen, J.; Clare, L.; Yuen, K.S.; Woods, R.T.; Evans, S.J.; Parkinson, C.H.; Rugg, M.D.; Linden, D.E.J. Cognitive rehabilitation changes memory-related brain activity in people with Alzheimer disease. Neurorehabil. Neural Repair 2013, 27, 448–459. [Google Scholar] [CrossRef] [PubMed]
- Clare, L.; Linden, D.E.; Woods, R.T.; Whitaker, R.; Evans, S.J.; Parkinson, C.H.; van Paasschen, J.; Nelis, S.M.; Hoare, Z.; Yuen, K.S.; et al. Goal-oriented cognitive rehabilitation for people with early-stage Alzheimer disease: A single-blind randomized controlled trial of clinical efficacy. Am. J. Geriatr. Psychiatry 2010, 18, 928–939. [Google Scholar] [CrossRef] [PubMed]
- Clare, L.; van Paasschen, J.; Evans, S.J.; Parkinson, C.; Woods, R.T.; Linden, D.E. Goal-oriented cognitive rehabilitation for an individual with Mild Cognitive Impairment: Behavioural and neuroimaging outcomes. Neurocase 2009, 15, 318–331. [Google Scholar] [CrossRef] [PubMed]
- Mountain, G.A.; Craig, C.L. What should be in a self-management programme for people with early dementia? Aging Ment. Health 2012, 16, 576–583. [Google Scholar] [CrossRef] [PubMed]
- Sprange, K.; Mountain, G.A.; Shortland, K.; Craig, C.; Blackburn, D.; Bowie, P.; Harkness, K.; Spencer, M. Journeying through Dementia, a community-based self-management intervention for people aged 65 years and over: A feasibility study to inform a future trial. Pilot Feasibility Stud. 2015, 1, 42. [Google Scholar] [CrossRef] [PubMed]
- Alzheimer’s Disease International. Importance of Early Diagnosis. Available online: https://www.alz.co.uk/info/importance-of-early-diagnosis (accessed on 7 February 2019).
- Alzheimer’s Society. Tips: Communicating with Someone with Dementia. Available online: https://www.alzheimers.org.uk/about-dementia/symptoms-and-diagnosis/symptoms/tips-for-communicating-dementia (accessed on 7 February 2019).
- Antonovsky, A. Unraveling the Mystery of Health. How People Manage Stress and Stay Well; Jossey-Bass: San Francisco, CA, USA; London, UK, 1987; p. 19. [Google Scholar]
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Maki, Y.; Hattori, H. Rehabilitative Support for Persons with Dementia and Their Families to Acquire Self-Management Attitude and Improve Social Cognition and Sense of Cognitive Empathy. Geriatrics 2019, 4, 26. https://doi.org/10.3390/geriatrics4010026
Maki Y, Hattori H. Rehabilitative Support for Persons with Dementia and Their Families to Acquire Self-Management Attitude and Improve Social Cognition and Sense of Cognitive Empathy. Geriatrics. 2019; 4(1):26. https://doi.org/10.3390/geriatrics4010026
Chicago/Turabian StyleMaki, Yohko, and Hideyuki Hattori. 2019. "Rehabilitative Support for Persons with Dementia and Their Families to Acquire Self-Management Attitude and Improve Social Cognition and Sense of Cognitive Empathy" Geriatrics 4, no. 1: 26. https://doi.org/10.3390/geriatrics4010026
APA StyleMaki, Y., & Hattori, H. (2019). Rehabilitative Support for Persons with Dementia and Their Families to Acquire Self-Management Attitude and Improve Social Cognition and Sense of Cognitive Empathy. Geriatrics, 4(1), 26. https://doi.org/10.3390/geriatrics4010026