
Involvement Theory with Market Segmentation: Effect of False Functional Food Advertising on Purchase Intention



Abstract
:1. Introduction
2. Literature Review
2.1. Involvement Theory and Possible Construct
2.2. Current Market for Functional Foods and Consumption Intention
3. Methods
- Product involvement scale: Based on Roe and Bruwer [22], Te’eni-Hararis and Lehman-Wilzig [47], and Zaichkowsky [48], this scale consisted of eight items. Representative items of nutrition claims include ‘Foods with nutrition claims are important to me’, ‘Foods with nutrition claims are valuable to me’, and ‘Foods with nutrition claims are attractive to me’.
- Advertising involvement scale: In reference to the literature [21,23,24,48], this scale had a total of six items. Representative items of nutrition claims include ‘Advertisements claiming certain foods are nutritious catch my attention’, ‘Advertisements claiming certain foods are nutritious appeal to me’, and ‘To understand the value of food, I spend time researching the nutritional benefits stated in the advertisements’.
- Situational involvement scale: In accordance with the suggestions of other studies [25,49], this scale comprised six items. Representative items of nutrition claims include ‘When purchasing foods claiming to have nutritional benefits, I believe I am making the right choice’, ‘I enjoy the process of purchasing foods claiming to have nutritional benefits’, and ‘Spending time shopping for foods claiming to have nutritional benefits is worthwhile’.
- False advertisements and penalties: A false advertisement with a particular health-related claim and the issued penalty was displayed directly after the situational involvement scale. The participants were asked to read the advertisement and penalty before completing the subsequent purchase intention scale. The false advertisement with nutrition claims focused on a high-protein, low-fat product; that with health-related claims centred on weight loss and weight loss function; and that with disease risk reduction claims focused on anticancer effects. The false advertisements used were drawn from the penalty list issued regularly by the Taiwanese government.
- Purchase intention scale: Based on the suggestions of Spears and Singh [50] and Te’eni-Hararis and Lehman-Wilzig [47], this scale comprised four items. Representative items of nutrition claims include ‘I will consider purchasing food with nutrition claims’, ‘I will continue purchasing food with nutrition claims’, and ‘I will recommend that my friends buy food with nutrition claims’.
- Demographic variables: This part contained basic information on gender, age, education level, and residential regions.
4. Analyses
4.1. Descriptive Statistics
4.2. Confirmatory Factor Analysis
4.3. SEM
5. Results
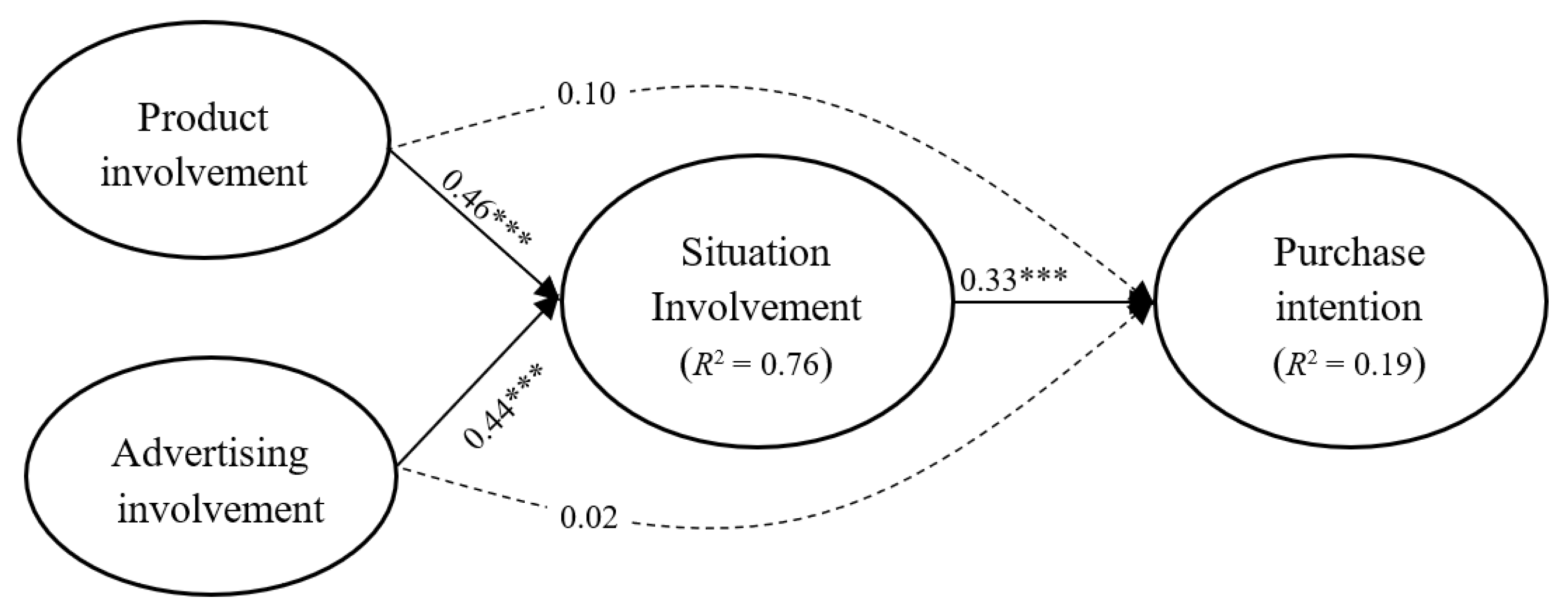
5.1. Mediating Model for H1, H2, and H3
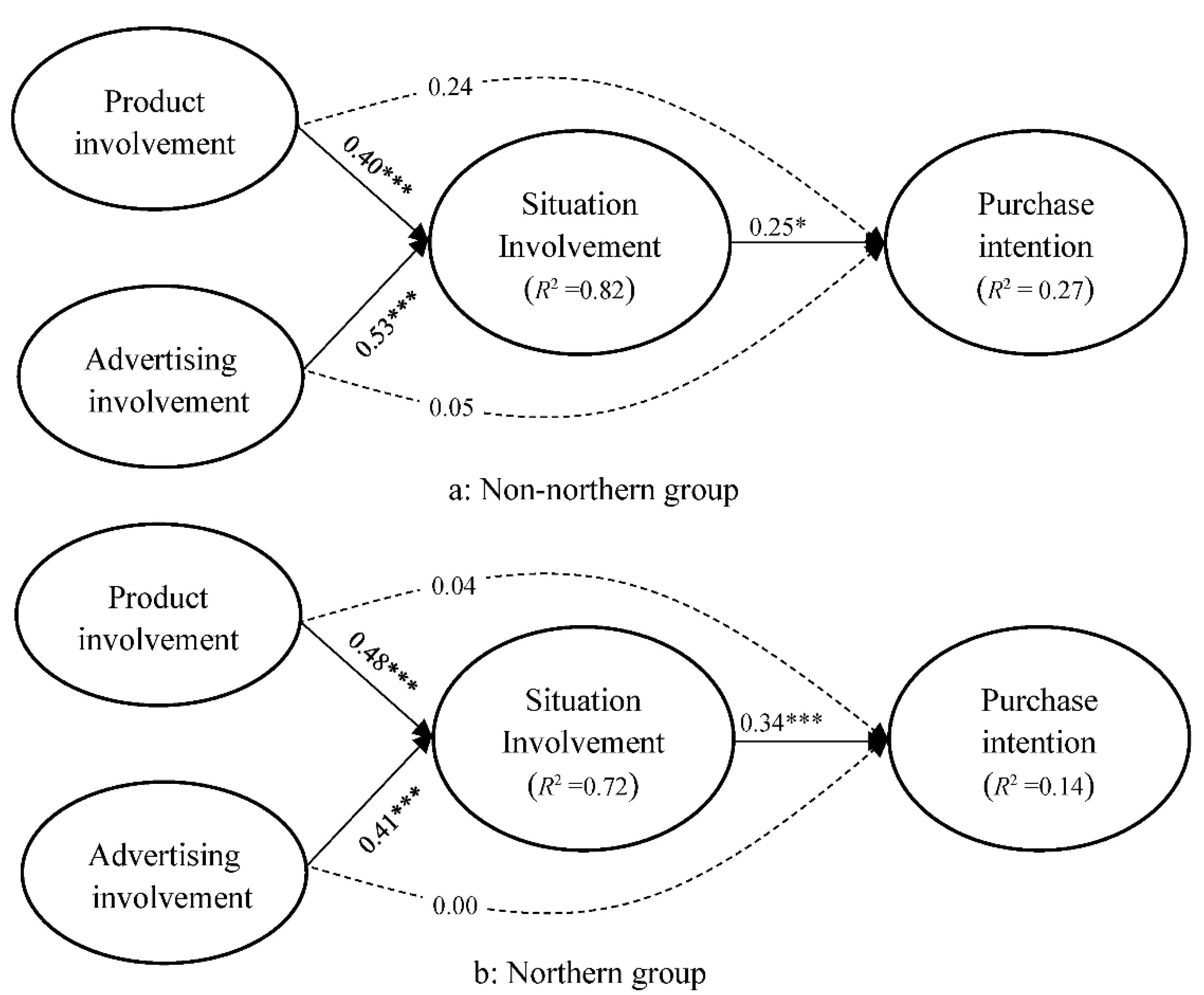
5.2. Mediating Model for H4
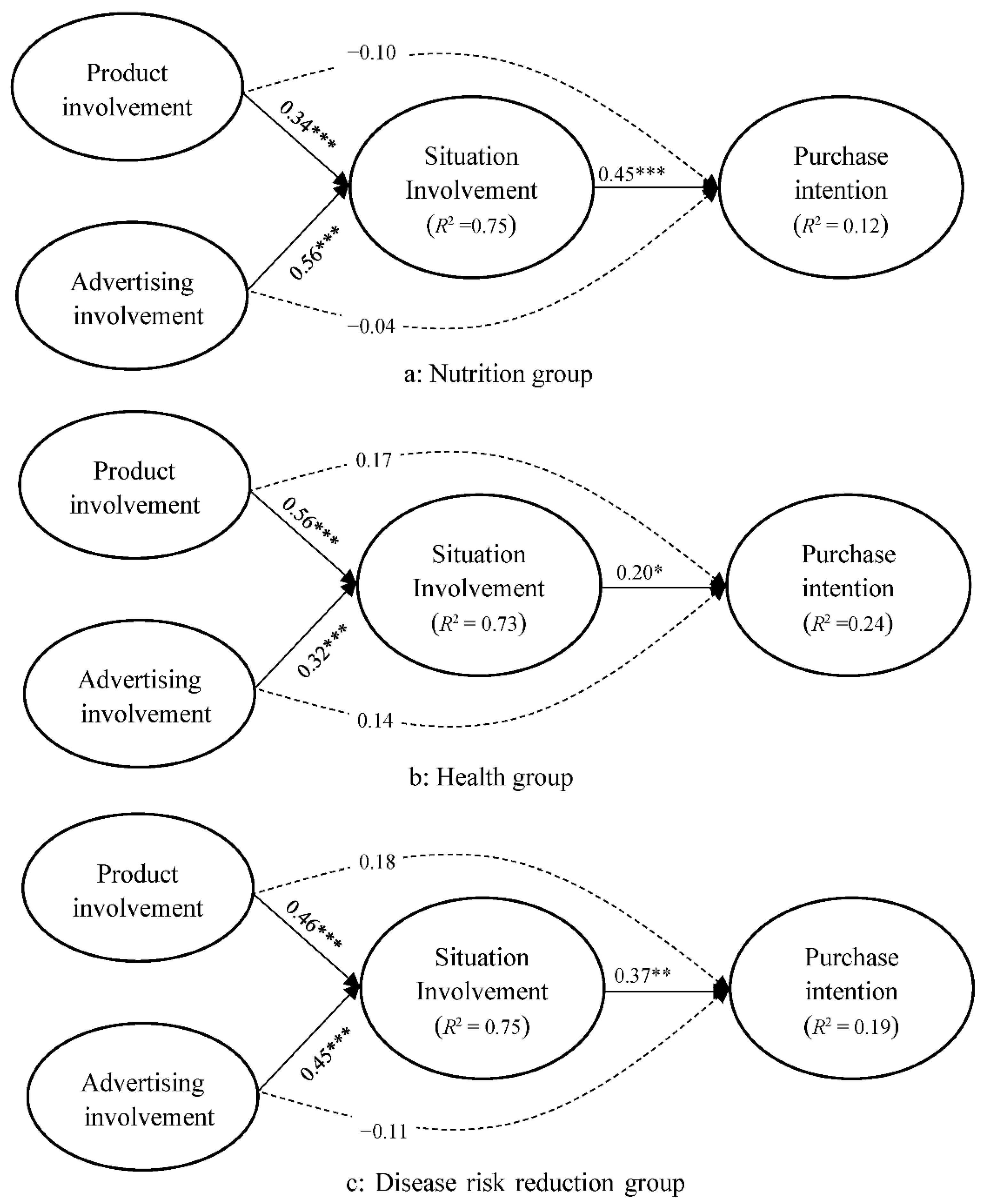
5.3. Mediating Model for H5
6. Discussion
6.1. Effects of Involvement on Purchase Intention
6.2. Effect of Residential Regions and Health-Related Claims on Purchase Intention
7. Conclusions and Suggestions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Product involvement (a) |
| Foods that are claimed to be nutritious or healthy are important to me. |
| Foods that are claimed to be nutritious or healthy are closely related to my life. |
| Foods that are claimed to be nutritious or healthy can provide me with much health information. |
| Foods that are claimed to be nutritious or healthy are valuable to me. |
| Foods that are claimed to be nutritious or healthy are attractive to me. |
| Foods that are claimed to be nutritious or healthy are related to my health. |
| I am interested in foods that are claimed to be nutritious or healthy. |
| I need foods that are claimed to be nutritious or healthy. |
| Advertisement involvement (b) |
| Food advertisements that claim a particular food is nutritious or healthy appeal more to me. |
| Food advertisements that claim a particular food is nutritious or healthy catch my attention in my daily life. |
| I have a keen interest in food advertisements that claim a certain food has nutritional or health benefits. |
| The nutritional or health benefits communicated in food advertisements are often the focus of my attention. |
| Before purchasing foods, gaining an understanding of the nutritional or health benefits claimed in the advertisements is important to me. |
| To understand the value of foods, I spend time gaining an understanding of the nutritional or health benefits stated in the advertisements. |
| Situational involvement (c) |
| The process of purchasing foods that are claimed to have nutritional or health benefits is interesting. |
| When purchasing foods that are claimed to be nutritious or healthy, I feel more confident in myself. |
| When purchasing foods that are claimed to have nutritional or health benefits, I believe I am making the right choice. |
| I enjoy the process of purchasing foods that are claimed to have nutritional or health benefits. |
| Spending time shopping for foods that are claimed to have nutritional or health benefits is worthwhile. |
| I feel upset if I do not purchase foods that are claimed to have nutritional or health benefits. |
| The false advertisement with nutrition claims |
| In 2017, the direct seller of a certain food company (XXX) declared that their particular product was ‘high in protein, low in fat, is suitable for ages 0 to 99 years, and can be drunk by both mothers and babies’. Believing the content of this advertisement, a mother in Kaohsiung purchased the product to replace general infant milk powder. She fed her 4-month-old baby six meals per day. After 3 months, the baby exhibited the symptoms of loss of appetite, diarrhoea, and generalized paralysis. The mother took her baby to the hospital for medical emergency treatment. The local government health bureau determined that the nutritional labelling of this product was incorrect and advertising information was false, which violated Articles 22 and 28 of the Food Safety and Hygiene Management Law. |
| The false advertisement with health claims |
| In 2019, the local government health bureau announced the results of their investigation into illegal advertisements in 2018. The highest number of regulation violations was related to the product advertisements of a certain company (YYY) claiming ‘weight loss’; the company was issued a fine of USD 65,000. The content of the advertisement stated that the product ‘suppresses fat absorption by 87%, suppresses fat accumulation by 92%, and promotes fat burning by up to 97%’, which violated Article 28 of the Food Safety and Hygiene Management Law. The local government health bureau emphasized that food advertising involving false, exaggerated, or misunderstood claims of medical efficacy is in violation of Article 28 of the Food Safety and Hygiene Management Law. A fine of USD 1500 to USD 180,000 can be imposed. |
| The false advertisement with disease risk reduction claims |
| In 2018, the distributor of ZZZ organic farm produce claimed that a particular food had ‘anticancer’ properties. A woman who participated in a ‘Lotus Tea Party’ believed the false advertisement and spent nearly USD 35,000 purchasing the product, hoping to cure her breast cancer. Consequently, her medical treatment was delayed, and the woman unfortunately died. After an investigation was launched by the local government health bureau, the advertisement was declared to contain false, exaggerated, or misunderstood claims of medical efficacy, according to Article 28 of the Food Safety and Sanitation Management Law. A fine of USD 1500 to USD 180,000 can be imposed. |
| After reading this message, (Purchase intention) |
| I would still consider purchasing this food that is claimed to have nutritional or health benefits. |
| I would continue purchasing this food with nutritional or health benefits. |
| I would recommend that my relatives and friends purchase this food that is claimed to have nutritional or health benefits. |
| I would like to receive information about this food that is claimed to have nutritional or health benefits. |
References
- Rezai, G.; Teng, P.K.; Shamsudin, M.N.; Mohamed, Z.; Stanton, J.L. Effect of perceptual differences on consumer purchase intention of natural functional food. J. Agribus. Dev. Emerg. Econ. 2017, 7, 153–173. [Google Scholar] [CrossRef]
- Domínguez Díaz, L.; Fernández-Ruiz, V.; Cámara, M. The frontier between nutrition and pharma: The international regulatory framework of functional foods, food supplements and nutraceuticals. Food Sci. Nutr. 2020, 60, 1738–1746. [Google Scholar] [CrossRef] [PubMed]
- Huang, L.; Bai, L.; Gong, S. The effects of carrier, benefit, and perceived trust in information channel on functional food purchase intention among Chinese consumers. Food Qual. Prefer. 2020, 81, 103854. [Google Scholar] [CrossRef]
- Domínguez Díaz, L.; Fernández-Ruiz, V.; Cámara, M. An international regulatory review of food health-related claims in functional food products labeling. J. Funct. Foods 2020, 68, 103896. [Google Scholar] [CrossRef]
- Hieke, S.; Cascanette, T.; Pravst, I.; Kaur, A.; Van Trijp, H.C.M.; Verbeke, W.; Grunert, K.G. The role of health-related claims and health-related symbols in consumer behaviour: The CLYMBOL project. Agro Food Ind Hi-Tech 2016, 27, 26–29. [Google Scholar]
- González-Díaz, C.; Vilaplana-Aparicio, M.J.; Iglesias-García, M. How is functional food advertising understood? An approximation in university students. Nutrients 2020, 12, 3312. [Google Scholar] [CrossRef]
- Mohammadi-Nasrabadi, F.; Salmani, Y.; Banihashemi, S.M.; Roudsari, A.H.; Zargaraan, A.; Esfarjani, F. Policy challenges of food advertisements from the viewpoints of stakeholders: A qualitative study. Food Sci. Nutr. 2020, 8, 1949–1956. [Google Scholar] [CrossRef]
- Muela-Molina, C.; Perelló-Oliver, S.; García-Arranz, A. Health-related claims in food supplements endorsements: A content analysis from the perspective of EU regulation. Public Health 2021, 190, 168–172. [Google Scholar] [CrossRef]
- Holden, A.C. Testimonials within health advertising in Australia: An analysis of current policy. Aust. Health Rev. 2019, 43, 712–716. [Google Scholar] [CrossRef]
- Leyva-Flores, R.; Kageyama, M.L.; Erviti-Ericeb, J. How people respond to illness in Mexico: Self-care or medical care? Health Policy 2001, 57, 15–26. [Google Scholar] [CrossRef]
- Chang, C.-J.; Tung, H.-J. Factors of Dietary Supplements Usage by Elderly in Taiwan. Taiwan J. Gerontol. Health Res. 2011, 7, 33–54. [Google Scholar] [CrossRef]
- Kendilci, E.A.; Kendilci, K.; Gunes, G. Assessment of awareness, knowledge levels and consumer perception of students of health high school towards functional foods. Med. Sci. 2018, 7, 194–202. [Google Scholar] [CrossRef] [Green Version]
- Kim, D.; Ji, I.; Han, K.; Ng’ombe, J.N. Effects of consumer characteristics on the intake of health functional foods: Implications for national health expenditure savings. Food Suppl. Biomater. Health 2021, 1, e3. [Google Scholar] [CrossRef]
- Kljusurić, J.G.; Cacic, J.; Misir, A.; Čačić, D. Geographical region as a factor influencing consumers’ perception of functional food: Case of Croatia. Br. Food J. 2015, 117, 1017–1031. [Google Scholar] [CrossRef]
- Food Industry Research and Development Institute. 2018 Food Industry. 2018. Available online: https://www.itis.org.tw/PubReport/PubReport_Detail.aspx?rpno=69169900&industry (accessed on 1 December 2021).
- Allied Market Research Functinal Food Market. 2022. Available online: https://www.alliedmarketresearch.com/functional-food-market (accessed on 10 December 2021).
- Hong, Y.-C.; Lin, C.-H. Exploring the relationship between medical resources and health status: An empirical study of crude and accidental death rates in 23 counties in Taiwan. Taiwan J. Public Health 2010, 29, 347–359. [Google Scholar] [CrossRef]
- Wang, L.-F.; Wu, T.-Y.; Wu, W.-H. A geographic information system study on the accessibility to emergency medical resources for new hospitals: A case of Hsinchu district. J. Health Manag. 2018, 16, 69–84. [Google Scholar]
- Hanzaee, K.H.; Taghipourian, M.J. The effects of brand credibility and prestige on consumers purchase intention in low and high product involvement. J. Basic Appl. Sci. Res. 2012, 2, 1281–1291. [Google Scholar]
- Wu, I.-H.; Liang, C. Purchase Intention after Learning of False Advertising: The Effect of Food Consumers’ Involvement. In Proceedings of the International Conference on Science Communication and Literacy, Taipei, Taiwan, 25 June 2021. [Google Scholar]
- Karpińska-Krakowiak, M. Conceptualizing and measuring consumer engagement in social media: Implications for personal involvement. Int. J. Contemp. Hospit. Manag. 2014, 13, 49–65. [Google Scholar]
- Roe, D.; Bruwer, J. Self-concept, product involvement and consumption occasions: Exploring fine wine consumer behaviour. Br. Food J. 2017, 119, 1362–1377. [Google Scholar] [CrossRef]
- Heath, R. Low involvement processing: A new model of brands and advertising. Int. J. Advert. 2000, 19, 287–298. [Google Scholar] [CrossRef]
- Li, L.Q.; Gao, J.; Shi, Z.; Song, W. The influence of self-construal on frequency of user activities and advertisement involvement in MsgSN. Behav. Inf. Technol. 2020, 1–12. [Google Scholar] [CrossRef]
- Havitz, M.E.; Mannell, R.C. Enduring involvement, situational involvement, and flow in leisure and non-leisure activities. J. Leis. Res. 2005, 37, 152–177. [Google Scholar] [CrossRef]
- Mou, J.; Zhu, W.; Benyoucef, M. Impact of product description and involvement on purchase intention in cross-border e-commerce. Ind. Manag. Data Syst. 2019, 120, 567–586. [Google Scholar] [CrossRef]
- Lee, W.-I.; Cheng, S.-Y.; Shih, Y.-T. Effects among product attributes, involvement, word-of-mouth, and purchase intention in online shopping. Asia Pac. Manag. Rev. 2017, 22, 223–229. [Google Scholar] [CrossRef]
- Conlin, R.; Labban, A. Clustering attitudes and behaviors of high/low involvement grocery shopper. J. Food Prod. Mark. 2019, 25, 647–667. [Google Scholar] [CrossRef]
- Tarkiainen, A.; Sundqvist, S. Product involvement in organic food consumption: Does ideology meet practice? Psychol. Mark. 2009, 26, 844–863. [Google Scholar] [CrossRef]
- Kamrath, C.; Bidkar, S.; Bröring, S. Is food involvement in purchasing decisions always low? A consumer study from Germany. PharmaNutrition 2019, 9, 100157. [Google Scholar] [CrossRef]
- Bornkessel, S.; Bröringa, S.; Omta, S.W.F.; van Trijp, H. What determines ingredient awareness of consumers? A study on ten functional food ingredients. Food Qual. Prefer. 2014, 32, 330–339. [Google Scholar] [CrossRef]
- Im, H.; Ha, Y. The effect of perceptual fluency and enduring involvement on situational involvement in an online apparel shopping context. J. Fash. Mark. Manag. 2011, 15, 345–362. [Google Scholar] [CrossRef]
- Lindgaard, G.; Fernandes, G.J.; Dudek, C.; Brown, J. Attention, web designers: You have 50 milliseconds to make a good first impression. Behav. Inf. Technol. 2006, 25, 115–126. [Google Scholar] [CrossRef]
- Beatty, S.E.; Homer, P.; Kahle, L.R. The involvement-model: Theory and implications. J. Bus. Res. 1988, 16, 149–167. [Google Scholar] [CrossRef]
- Starr, R.R. Too little, too late: Ineffective regulation of dietary supplements in the United States. Am. J. Public Health 2015, 105, 478–485. [Google Scholar] [CrossRef] [PubMed]
- Matos, J.; Cardoso, C.; Bandarra, N.M.; Afonso, C. Microalgae as healthy ingredients for functional food: A review. Food Funct. 2017, 8, 2672–2685. [Google Scholar] [CrossRef] [PubMed]
- Chen, M.-F. The joint moderating effect of health consciousness and healthy lifestyle on consumers’ willingness to use functional foods in Taiwan. Appetite 2011, 57, 253–262. [Google Scholar] [CrossRef]
- Watanabe, E.A.M.; Alfinito, S.; Curvelo, I.C.G.; Hamza, K.M. Perceived value, trust and purchase intention of organic food: A study with Brazilian consumers. Br. Food J. 2020, 122, 1070–1184. [Google Scholar] [CrossRef]
- Rutkow, L.; Vernick, J.S.; Edwards, D.M.; Rodman, S.O.; Barry, C.L. Legal action against health claims on foods and beverages marketed to youth. Am. J. Public Health 2015, 105, 450–456. [Google Scholar] [CrossRef] [PubMed]
- The Codex Alimentarius Commission. Guidelines for Use of Nutrition and Health Claims. 2013. Available online: http://www.fao.org/fao-who-codexalimentarius/sh-proxy/en/?lnk=1&url=https%253A%252F%252Fworkspace.fao.org%252Fsites%252Fcodex%252FStandards%252FCXG%2B23-1997%252FCXG_023e.pdf (accessed on 15 December 2021).
- Rebouças, M.C.; Rodrigues, M.C.P.; Ferreira, B.B.A.; Freitas, S.M. Evaluation of the effect of label attributes over the purchase intention of a cashew nut functional beverage using conjoint analysis. Food Sci. Technol. Int. 2020, 27, 164–171. [Google Scholar] [CrossRef]
- Schoenberg, N.E.; Traywick, L.S.; Jacobs-Lawson, J.; Kart, C.S. Diabetes self-care among a multiethnic sample of older adults. J. Cross Cult. Gerontol. 2008, 23, 361–376. [Google Scholar] [CrossRef] [Green Version]
- Li, J.; Shi, L.; Liang, H.; Ding, G.; Xu, L. Urban-rural disparities in health care utilization among Chinese adults from 1993 to 2011. BMC Health Serv. Res. 2018, 157, 102–110. [Google Scholar] [CrossRef] [Green Version]
- Rahmatullah, M.; Mollik, M.A.H.; Islam, M.K.; Islam, M.R.; Jahan, F.I.; Khatun, Z.; Seraj, S.; Chowdhury, M.H.; Islam, F.; Miajee, Z.U.M.; et al. A survey of medicinal and functional food plants used by the folk medicinal practitioners of three villages in Sreepur Upazilla, Magura district, Bangladesh. Am. Eurasian J. Sustain. Agric. 2010, 4, 363–373. [Google Scholar]
- Ong, F.S.; Kassim, N.; Peng, O.S.; Singh, T. Purchase behaviour of consumers of functional foods in Malaysia: An analysis of selected demographic variables, attitude and health status. Asia Pac. Manag. Rev. 2013, 19, 81–98. [Google Scholar] [CrossRef]
- Vorage, L.; Wiseman, N.; Graca, J.; Harris, N. The association of demographic characteristics and food choice motives with the consumption of functional foods in emerging adults. Nutrients 2020, 12, 2582. [Google Scholar] [CrossRef] [PubMed]
- Te’eni-Hararis, T.; Lehman-Wilzig, S.N. The importance of product involvement for predicting advertising effectiveness among young people. Int. J. Advert. 2009, 28, 203–229. [Google Scholar] [CrossRef] [Green Version]
- Zaichkowsky, J.L. The personal involvement inventory: Revision and application to advertising. J. Advert. 1994, 23, 59–70. [Google Scholar] [CrossRef]
- Zaichkowsky, J.L. Measuring the involvement construct. J. Consum. Res. 1985, 12, 341–352. [Google Scholar] [CrossRef]
- Spears, N.; Singh, S.N. Measuring attitude toward the brand and purchase intentions. J. Curr. Issues Res. Advert. 2004, 26, 53–66. [Google Scholar] [CrossRef]
- Grant, T.; Clark, U.; Reershemius, G.; Pollard, D.; Hayes, S.; Plappert, G. Quantitative Research Methods for Linguists: A Questions and Answers Approach for Students; Routledge: London, UK, 2017. [Google Scholar] [CrossRef]
- Dogan, I.S.; Yildiz, O.; Eyduran, E.; Kose, S. A study on determination of functional food consumption habits and awareness of consumers in Turkey. Bulgarian J. Agric. Sci. 2011, 17, 246–257. [Google Scholar]
- Schultz, M.; Baranchi, A.; Thurston, L.; Yu, Y.C.; Wang, L.; Chen, J.; Sapsford, M.; Chung, J.; BinSadiq, M.; Craig, L.; et al. Consumer demographics and expectations of probiotic therapy in New Zealand: Results of a large telephone survey. N. Z. Med. J. 2011, 124, 36–43. [Google Scholar]
- Kolbina, A.Y.; Ulrikh, E.V.; Voroshilin, R.A. Analysis of consumer motivations of the Kemerovo city residents in relation to functional food products. Eurasian J. Biosci. 2020, 14, 6365–6369. [Google Scholar]
- Yilmaz-Ersan, L.; Ozcan, T.; Akpinar-Bayizit, A. Assessment of socio-demographic factors, health status and the knowledge on probiotic dairy products. Food Sci. Hum. Wellness 2020, 9, 272–279. [Google Scholar] [CrossRef]
- Brečić, R.; Gorton, M.; Barjolle, D. Understanding variations in the consumption of functional foods: Evidence from Croatia. Br. Food J. 2014, 116, 662–675. [Google Scholar] [CrossRef]
- Szakály, Z.; Kovács, S.; Pető, K.; Huszka, P.; Kiss, M. A modified model of the willingness to pay for functional foods. Appetite 2019, 138, 94–101. [Google Scholar] [CrossRef] [PubMed]
- Hu, L.-T.; Bentler, P.M. Cutoff criteria for fit indexes in covariance structure analysis: Conventional criteria versus new alternatives. Struct. Equ. Modeling 1999, 6, 1–55. [Google Scholar] [CrossRef]
- Henseler, J.; Ringle, C.M.; Sarstedt, M. A new criterion for assessing discriminant validity in variance-based structural equation modeling. J. Acad. Mark. Sci. 2015, 43, 115–135. [Google Scholar] [CrossRef] [Green Version]
- Voorhees, C.M.; Brady, M.K.; Calantone, R.; Ramirez, E. Discriminant validity testing in marketing: An analysis, causes for concern and proposed remedies. J. Acad. Mark. Sci. 2016, 44, 119–134. [Google Scholar] [CrossRef]
- Franke, G.; Sarstedt, M. Heuristics versus statistics in discriminant validity testing: A comparison of four procedures. Internet Res. 2019, 29, 430–447. [Google Scholar] [CrossRef]
- Nystrand, B.T.; Olsen, S.O. Consumers’ attitudes and intentions toward consuming functional foods in Norway. Food Qual. Prefer. 2020, 80, 103827. [Google Scholar] [CrossRef]
- Chang, C.-C. Exploring mobile application customer loyalty: The moderating effect of use contexts. Telecomm. Policy 2015, 39, 678–690. [Google Scholar] [CrossRef]
- Khuong, M.N.; Tram, V.N.B. The effects of emotional marketing on consumer product perception, brand awareness and purchase decision: A study in Ho Chi Minh City, Vietnam. J. Econ. Bus. Manag. 2015, 3, 524–530. [Google Scholar] [CrossRef] [Green Version]
- Hong, I.B. Understanding the consumer’s online merchant selection process: The roles of product involvement, perceived risk, and trust expectation. Int. J. Inf. Manag. 2015, 35, 322–336. [Google Scholar] [CrossRef]
- Hollebeek, L.D.; Jaeger, S.R.; Brodie, R.J.; Balemi, A. The influence of involvement on purchase intention for new world wine. Food Qual. Prefer. 2007, 18, 1033–1049. [Google Scholar] [CrossRef]
- Shaouf, A.; Lü, K.; Li, X. The effect of web advertising visual design on online purchase intention: An examination across gender. Comput. Hum. Behav. 2016, 60, 622–634. [Google Scholar] [CrossRef]
- Andrews, J.C.; Netemeyer, R.G.; Burton, S. Consumer generalization of nutrient content claims in advertising. J. Mark. 1998, 62, 62–75. [Google Scholar] [CrossRef]
- Venn, D.; Dixon, J.; Banwell, C.; Strazdins, L. Social determinants of household food expenditure in Australia: The role of education, income, geography and time. Public Health Nutr. 2017, 21, 902–911. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Verbeke, W.; Scholderer, J.; Lähteenmäki, L. Consumer appeal of nutrition and health claims in three existing product concepts. Appetite 2009, 52, 684–692. [Google Scholar] [CrossRef] [PubMed]
- Shi, H.-J.; Nakamura, K.; Takano, T. Health values and health-information-seeking in relation to positive change of health practice among middle-aged urban men. Prev. Med. 2004, 39, 1164–1171. [Google Scholar] [CrossRef]


| Demographic Variables | National Census (above 15 years/old) | Percentage (Frequency) | ||
|---|---|---|---|---|
| Claims | Nutrition | Health | Disease risk reduction | |
| 21,597,840 | 33.5% (350) | 33.5% (350) | 33.1% (346) | |
| Gender | ||||
| Male | 10,134,705 | 30.6% (107) | 34.0% (119) | 28.3% (98) |
| Female | 10,463,135 | 69.4% (243) | 66.0% (231) | 71.7% (248) |
| Age | ||||
| 15–35 years old | 5,830,865 | 38.6% (135) | 36.3% (127) | 33.2% (115) |
| 36–49 years old | 5,671,100 | 38.3% (134) | 36.7% (128) | 44.3% (153) |
| 50 years old and above | 9,095,875 | 23.1% (81) | 27.0% (95) | 22.5% (78) |
| Education Levels | ||||
| Senior high school and lower | 13,436,711 | 6.0% (21) | 3.4% (12) | 6.1% (21) |
| University or junior college | 6,913,223 | 50.3% (176) | 47.1% (165) | 56.6% (196) |
| Graduate school and higher | 1,247,906 | 43.7% (153) | 49.5% (173) | 37.3% (129) |
| Residential Regions | ||||
| Northern Regions | 9,327,807 | 67.1% (235) | 62.6% (219) | 60.1% (208) |
| Nonnorthern Regions | 12,270,033 | 32.9% (115) | 37.4% (131) | 39.9% (138) |
| Item/Variable | Product Involvement | Advertisement Involvement | Situational Involvement | Purchase Intention |
|---|---|---|---|---|
| Factor loadings | ||||
| Item 1 | 0.83 | 0.85 | 0.81 | 0.91 |
| Item 2 | 0.82 | 0.86 | 0.85 | 0.97 |
| Item 3 | 0.82 | 0.90 | 0.84 | 0.89 |
| Item 4 | 0.88 | 0.83 | 0.89 | 0.81 |
| Item 5 | 0.89 | 0.70 | 0.81 | |
| Item 6 | 0.86 | 0.62 | 0.61 | |
| Item 7 | 0.87 | |||
| Item 8 | 0.86 | |||
| α | 0.96 | 0.91 | 0.91 | 0.94 |
| Composite reliability | 0.96 | 0.91 | 0.92 | 0.94 |
| AVE | 0.73 | 0.64 | 0.65 | 0.80 |
| Item/Variable | Product Involvement | Advertisement Involvement | Situational Involvement | Purchase Intention |
|---|---|---|---|---|
| Product involvement | (0.85) | |||
| Advertisement involvement | 0.86 | (0.80) | ||
| Situational involvement | 0.85 | 0.85 | (0.81) | |
| Purchase intention | 0.41 | 0.38 | 0.46 | (0.90) |
| Test Results/Advertising Claims | Nutrition | Health | Disease Risk Reduction |
|---|---|---|---|
| Configural invariance | Appropriate fit (χ2/df = 2.24, RMSEA = 0.06, SRMR = 0.04, CFI = 0.92, TLI = 0.91) | Appropriate fit (χ2/df = 2.38, RMSEA = 0.07, SRMR = 0.06, CFI = 0.92, TLI = 0.91) | Appropriate fit (χ2/df = 2.15, RMSEA = 0.06, SRMR = 0.04, CFI = 0.93, TLI = 0.92) |
| Metric invariance | Insignificant difference (Δχ2 = 18.70, Δdf = 20, p > 0.05) | Insignificant difference (Δχ2 = 19.97, Δdf = 20, p > 0.05) | Insignificant difference (Δχ2 = 28.00, Δdf = 20, p > 0.05) |
| Invariance results | Full invariance | Full invariance | Full invariance |
| Multigroup analysis | Significant change in χ2 (Δχ2 = 6.68, Δdf = 1, p < 0.05) | Significant change in χ2 (Δχ2 = 4.56, Δdf = 1, p < 0.05) | Significant change in χ2 (Δχ2 = 0.33, Δdf = 1, p > 0.05) |
| Nonnorthern group (situational involvement → purchase intention) | β = 0.68, p < 0.001, f2 = 0.09 | β = 0.21, p < 0.001, f2 = 0.02 | β = 0.29, p < 0.001, f2 = 0.02 |
| Northern group (situational involvement → purchase intention) | β = 0.34, p < 0.001, f2 = 0.03 | β = 0.36, p < 0.001, f2 = 0.04 | β = 0.47, p < 0.001, f2 = 0.07 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wu, I.-H.; Liang, C.; Ip, C.Y. Involvement Theory with Market Segmentation: Effect of False Functional Food Advertising on Purchase Intention. Foods 2022, 11, 978. https://doi.org/10.3390/foods11070978
Wu I-H, Liang C, Ip CY. Involvement Theory with Market Segmentation: Effect of False Functional Food Advertising on Purchase Intention. Foods. 2022; 11(7):978. https://doi.org/10.3390/foods11070978
Chicago/Turabian StyleWu, I-Hsuan, Chaoyun Liang, and Ching Yin Ip. 2022. "Involvement Theory with Market Segmentation: Effect of False Functional Food Advertising on Purchase Intention" Foods 11, no. 7: 978. https://doi.org/10.3390/foods11070978
APA StyleWu, I.-H., Liang, C., & Ip, C. Y. (2022). Involvement Theory with Market Segmentation: Effect of False Functional Food Advertising on Purchase Intention. Foods, 11(7), 978. https://doi.org/10.3390/foods11070978