Fire in the Operating Room: Use of Mixed Reality Simulation with Nurse Anesthesia Students


 ,
,  and
and
Abstract
1. Introduction
1.1. Use of Simulation
1.2. Non-Technical Skills
1.3. Use of Checklists
1.4. Mixed Reality in Nursing Education
1.5. Research Aims
- (1)
- Assess SRNAs’ technical skills while managing a simulated OR fire using mixed reality.
- (2)
- Assess SRNA’ non-technical skills while managing a simulated OR fire using mixed reality.
2. Materials and Methods
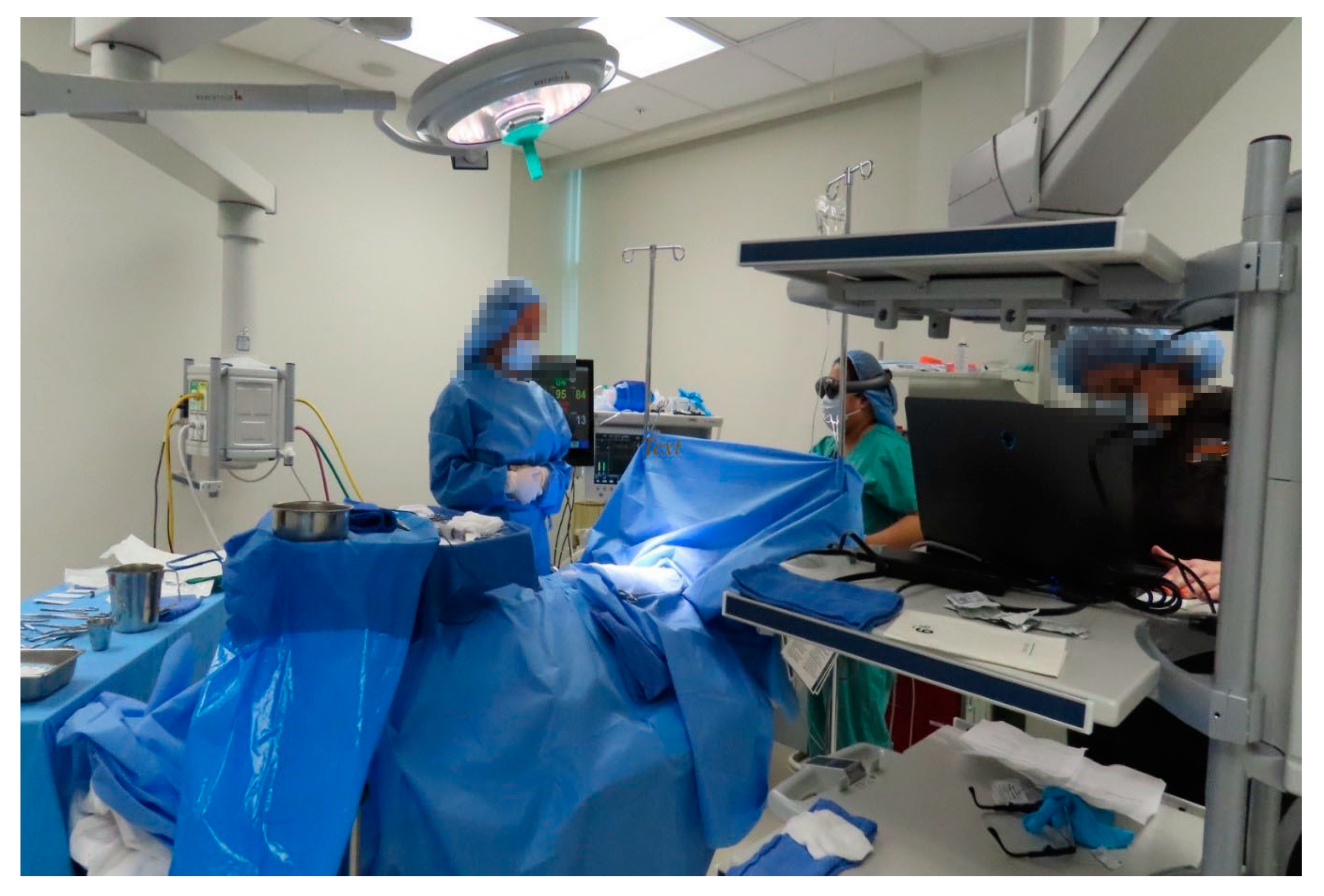
2.1. Methods
- Student is able to understands fire risks in the OR and the fire triangle.
- Student identifies fuel, ignition, and oxidizer sources in the perioperative setting.
- Student is able to utilize new innovation to appropriately treat an OR/Airway fire.
2.2. Instrument
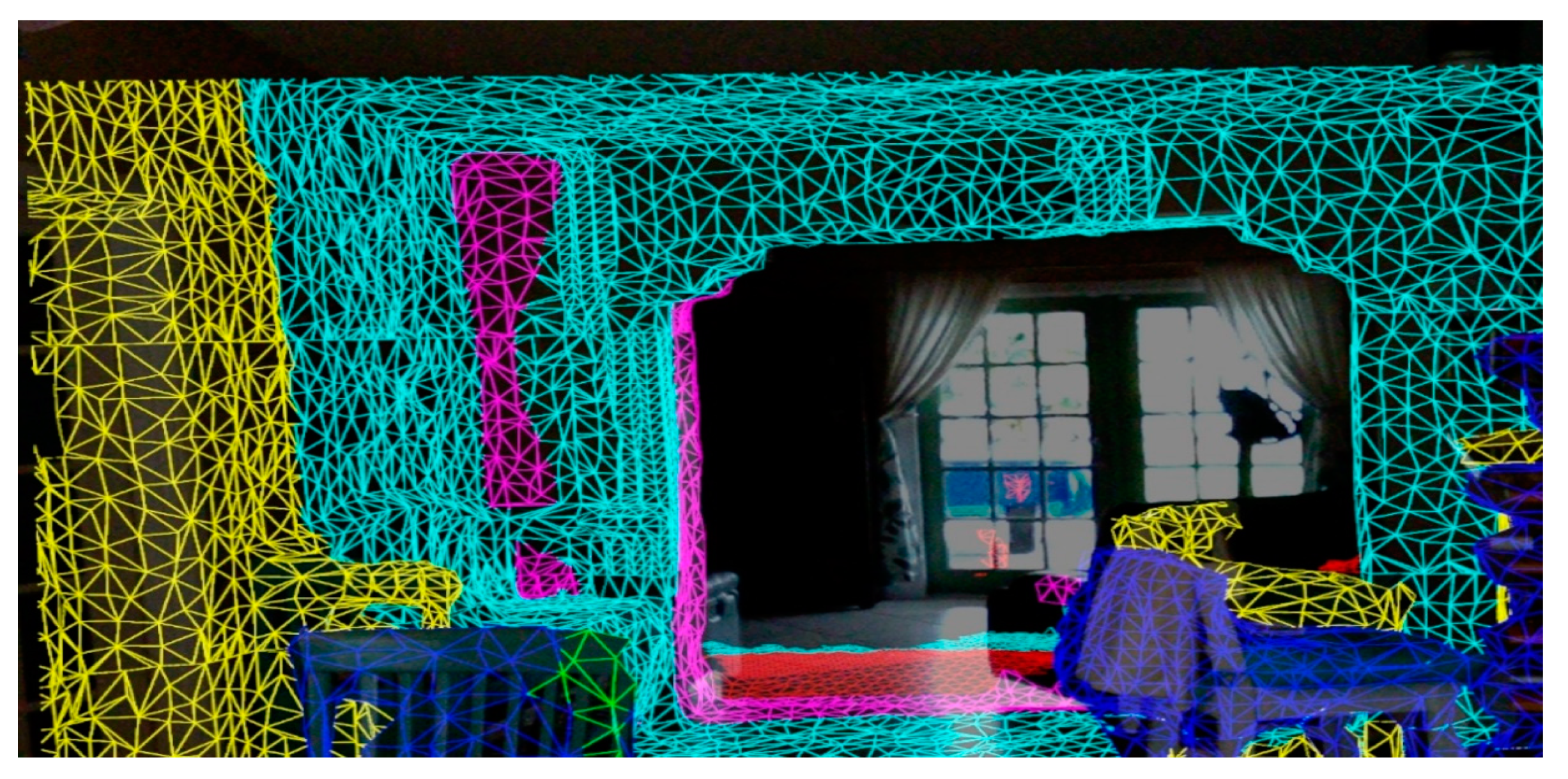
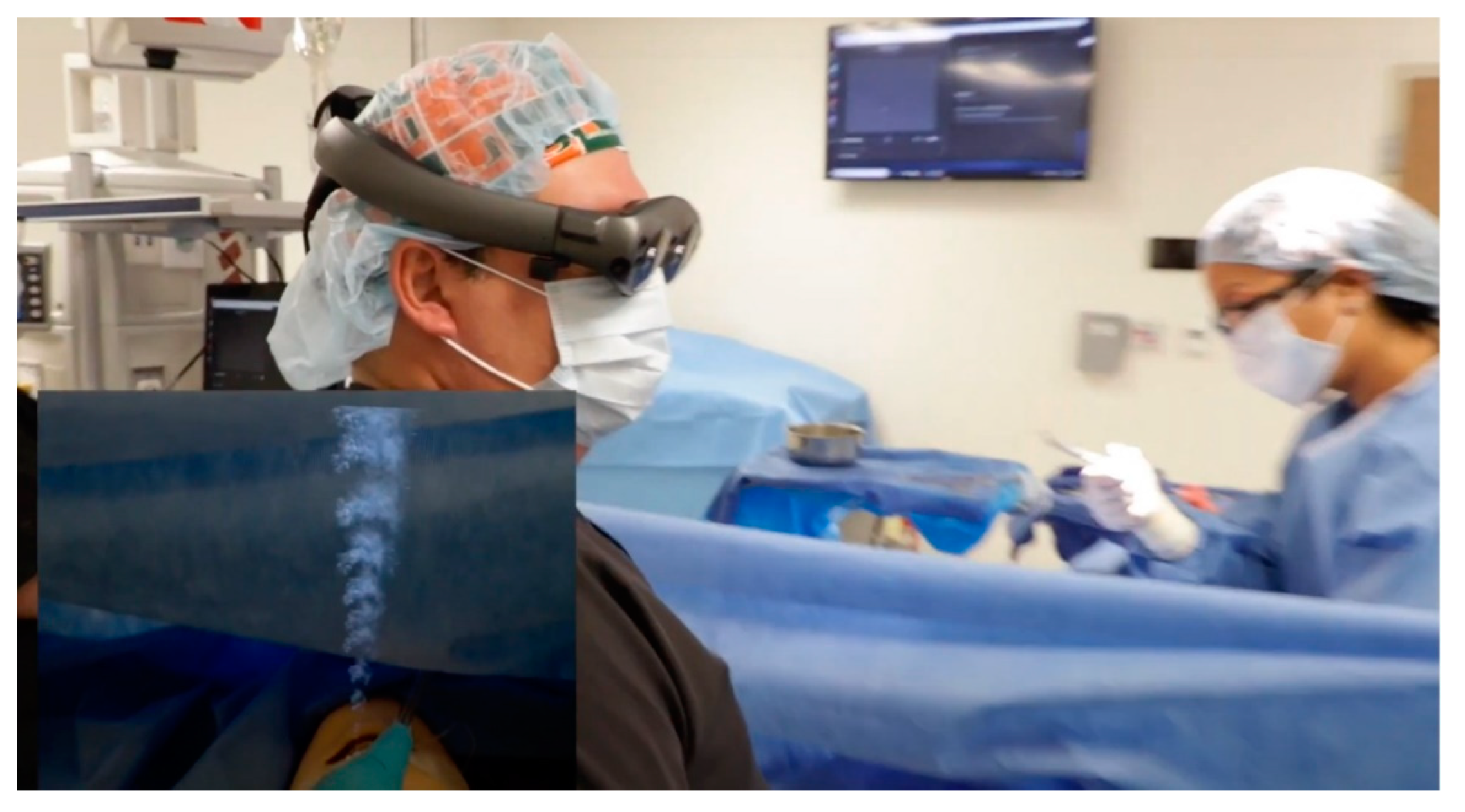
2.3. Augmented Reality Headset
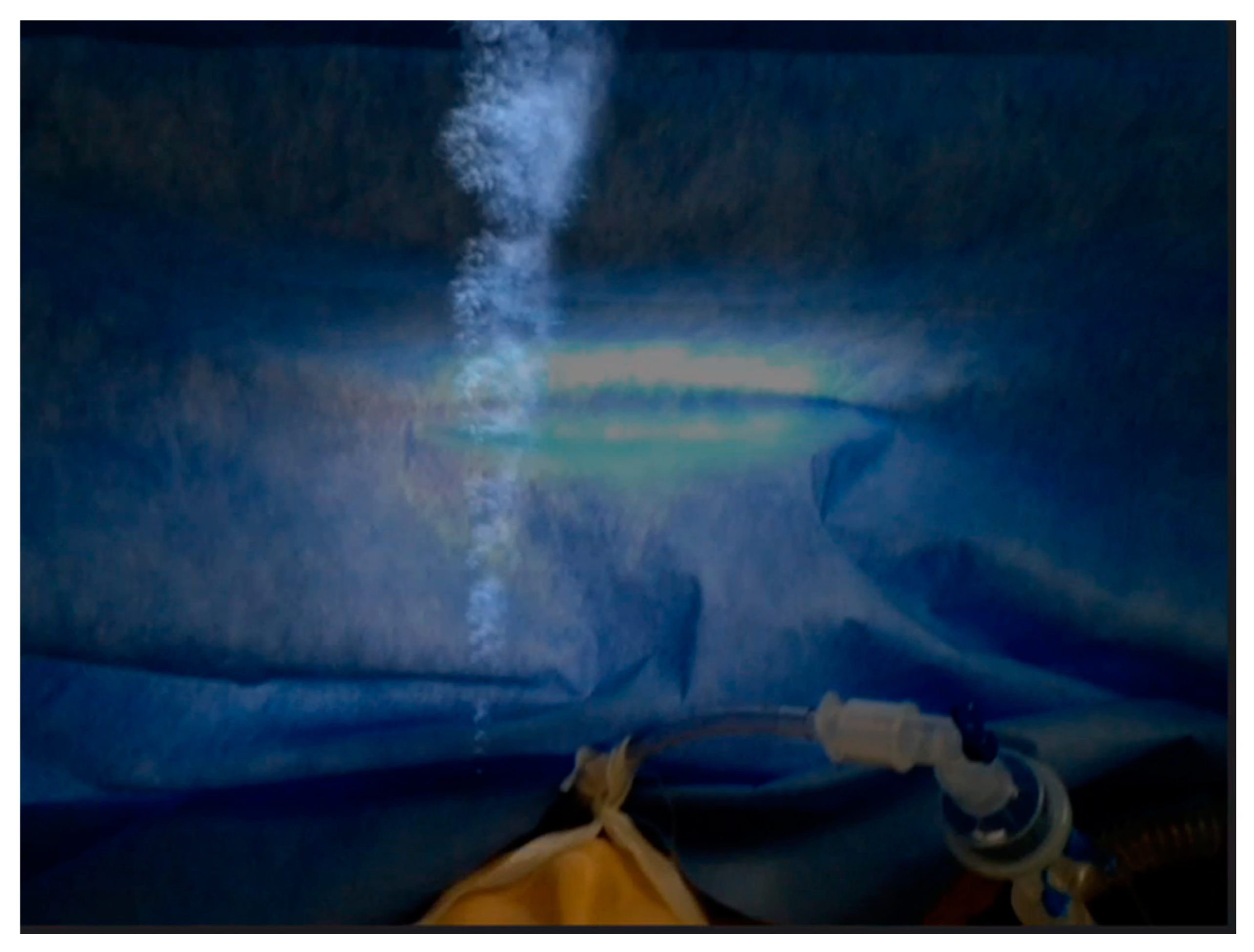
2.4. Airway Fire Application
2.5. Data Collection
2.6. Data Analysis
3. Results
3.1. Sample
3.2. Performance
4. Discussion
4.1. Students’ Simulation Performance
4.2. Limitations
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Jones, T.S.; Black, I.H.; Robinson, T.N.; Jones, E.L. Operating room fires. Anesthesiology 2019, 130, 492–501. [Google Scholar] [CrossRef]
- McDougall, E.M. Simulation in education for health care professionals. BCMJ 2015, 57, 444–448. [Google Scholar]
- Howard, S.K.; Gaba, D.M.; Fish, K.J.; Yang, G.; Sarnquist, F.H. Anesthesia crisis resource management training: Teaching anesthesiologist to handle critical incident. Aviat. Space Environ. Med. 1992, 63, 763–770. [Google Scholar]
- Gonzalez, J.E. The Effects of an ACLS Simulation-Based Educational Intervention on Performance, Self-efficacy, and General Knowledge in a Group of First-Year Nurse Anesthetist Students. Ph.D. Thesis, Barry University, Miami Shores, FL, USA, 2009. [Google Scholar]
- Kolb, D.A. The process of experiential learning. In Experiential Learning: Experience as the Source of Learning and Development; Prentice-Hall: Englewood Cliffs, NJ, USA, 1984; pp. 20–38. [Google Scholar]
- Fewster-Thuente, L.; Batterson, T.J. Kolb’s Experienctial Learning Theory as a theoretical underpinning for interprofessional education. J. Allied Health 2018, 47, 3–8. [Google Scholar]
- Institute of Medicine. To Err Is Human: Building a Safer Health System; The National Academies Press: Washington, DC, USA, 2000. [Google Scholar] [CrossRef]
- Reason, J. Safety in the operating room theatre-Part 2 human error an organizational failure. Qual. Saf. Health Care 2005, 14, 56–61. [Google Scholar]
- Flin, R.; Martin, L.; Goeters, K.M.; Hörmann, H.J.; Amalberti, R.; Valot, C.; Nijhuis, H. Development of the NOTECH(non-technical skills) system for assessing pilots’ CRM skills. Hum. Factors Aerosp. Saf. 2003, 3, 97–120. [Google Scholar]
- Flin, R.; Patey, R.; Glavin, R.; Maran, M. Anaesthetists’ non-technical skills. BJA 2010, 105, 38–44. [Google Scholar] [CrossRef]
- Jackson, K.S. The importance of non-technical skills and risk reduction in the operating room theatre, royal college of obstetricians. TOG Obstet. Gynocol. 2016, 18, 309–314. [Google Scholar] [CrossRef]
- Wunder, L. The effect of a nontechnical skills intervention on first-year student registered nurse anesthetists’ skills during crisis simulation. AANA 2016, 84, 46–51. [Google Scholar]
- Pronovost, P.; Needham, D.; Berenholtz, S.; Sinopoli, D.; Chu, H.; Cosgrove, S.; Sexton, B.; Hyzy, R.; Welsh, R.; Roth, G.; et al. An intervention to decrease catheter-related bloodstream infections in the ICU. N. Engl. J. Med. 2006, 355, 2725–2732. [Google Scholar] [CrossRef]
- Agarwala, A.V.; McRichards, L.K.; Rao, V.; Kurzweil, V.; Goldhaber-Fiebert, S.N. Bringing perioperative emergency manuals to your institution: A “How to” from concept to implementation in 10 steps. Jt. Comm. J. Qual. Saf. 2019, 45, 170–179. [Google Scholar] [CrossRef] [PubMed]
- Alidina, S.; Goldhaber-Fiebert, S.N.; Hannenberg, A.A.; Hepner, D.L.; Singer, S.J.; Neville, B.A.; Sachetta, J.R.; Lipsitz, S.R.; Berry, W.R. Factors associated with the use of cognitive aids in operating room crises: A cross-sectional study of US hospitals and ambulatory surgical centers. Implement. Sci. 2018, 13, 50. [Google Scholar] [CrossRef]
- Hepner, D.L.; Arriaga, A.F.; Cooper, J.B.; Goldhaber-Fiebert, S.N.; Gaba, D.M.; Berry, W.R.; Boorman, D.J.; Bader, A.M. Operating room crisis checklists and emergency manuals. Anesthesiology 2017, 127, 384–392. [Google Scholar] [CrossRef] [PubMed]
- Everett, T.C.; Morgan, P.J.; Brydges, R.; Kurrek, M.; Tregunno, D.; Cunningham, L.; Chan, A.; Forde, D.; Tarshis, J. The impact of critical event checklists on medical management and teamwork during simulated crises in a surgical daycare facility. Anaesthesia 2016, 72, 350–358. [Google Scholar] [CrossRef] [PubMed]
- Arriaga, A.F.; Bader, A.M.; Wong, J.M.; Lipsitz, S.R.; Berry, W.R.; Ziewacz, J.E.; Hepner, D.L.; Boorman, D.J.; Pozner, C.N.; Smink, D.S.; et al. Simulation-based trial of surgical-crisis checklists. Obstet. Gynecol. Surv. 2013, 68, 336–338. [Google Scholar] [CrossRef]
- Foronda, C.; Alfes, C.M.; Dev, P.; Kleinheksel, A.J.; Nelson, D.A.; O’Donnell, J.M.; Samosky, J.T. Virtually nursing: Emerging technologies in nursing education. Nurse Educ. 2017, 42, 14–17. [Google Scholar] [CrossRef]
- Apfelbaum, J.L.; Caplan, R.A.; Barker, S.J.; Connis, R.T.; Cowles, C.; Ehrenwerth, J.; Nickinovich, D.G.; Pritchard, D.; Roberson, D.W.; Caplan, R.A.; et al. American Society of Anesthesiologist Task Force on Operating Room Fires: Practice advisory for the prevention and management of operating room fires: An updated report by the American Society of Anesthesiologist Task Force on Operation Room Fires. Anesthesiology 2013, 118, 271–290. [Google Scholar] [CrossRef]
- INACSL Standards Committee. December 2016. INACSL Standards of Best Practice: SimulationSM: Simulation Design. Clin. Simul. Nurs. 2016, 12, S5–S12. [Google Scholar] [CrossRef]
- Zhu, E.; Hadadgar, A.; Masiello, I.; Zary, N. Augmented reality in healthcare education: An integrative review. PeerJ 2014, 2, 469. [Google Scholar] [CrossRef]
- Eppich, W.; Cheng, A. Promoting excellence and reflective learning in simulation (PEARLS). Development and rationale for a blended approach to health care simulation debriefing. Simul. Healthc. 2015, 10, 106–115. [Google Scholar] [CrossRef]
- Dorozhkin, D.; Olasky, J.; Jones, D.B.; Schwaitzberg, S.D.; Jones, S.B.; Cao, C.G.L.; Molina, M.; Henriques, S.; Wang, J.; Flinn, J.; et al. OR fire virtual training simulator: Design and face validity. Surg. Endosc. 2017, 31, 3527–3533. [Google Scholar] [CrossRef] [PubMed]
- Haulk, L. Vitural reality may prove useful for surgical fire education and training. AORN 2018, 108, 4. [Google Scholar] [CrossRef]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Technical Skills Scores | Mean | SD | % | Range |
|---|---|---|---|---|
| Overall | 18.16 | ±1.44 | 91 | 15–20 |
| FP | 5.81 | ±0.46 | 97 | 4–6 |
| FM | 3.20 | ±1.00 | 80 | 0–4 |
| AFM | 6.28 | ±0.82 | 90 | 4–7 |
| NAFM | 2.86 | ±0.35 | 95 | 2–3 |
| Non-Technical Skills Scores | Mean | SD | % | Range |
|---|---|---|---|---|
| TM | 11.67 | ±1.10 | 90 | 9–13 |
| TW | 3.80 | ±0.44 | 95 | 2–4 |
| SA | 7.30 | ±0.70 | 91 | 6–8 |
| DM | 8.94 | ±1.03 | 89 | 7–10 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wunder, L.; Gomez, N.A.G.; Gonzalez, J.E.; Mitzova-Vladinov, G.; Cacchione, M.; Mato, J.; Foronda, C.L.; Groom, J.A. Fire in the Operating Room: Use of Mixed Reality Simulation with Nurse Anesthesia Students. Informatics 2020, 7, 40. https://doi.org/10.3390/informatics7040040
Wunder L, Gomez NAG, Gonzalez JE, Mitzova-Vladinov G, Cacchione M, Mato J, Foronda CL, Groom JA. Fire in the Operating Room: Use of Mixed Reality Simulation with Nurse Anesthesia Students. Informatics. 2020; 7(4):40. https://doi.org/10.3390/informatics7040040
Chicago/Turabian StyleWunder, Linda, Nicole A. Gonzaga Gomez, Juan E. Gonzalez, Greta Mitzova-Vladinov, Max Cacchione, Jampierre Mato, Cynthia L. Foronda, and Jeffrey A. Groom. 2020. "Fire in the Operating Room: Use of Mixed Reality Simulation with Nurse Anesthesia Students" Informatics 7, no. 4: 40. https://doi.org/10.3390/informatics7040040
APA StyleWunder, L., Gomez, N. A. G., Gonzalez, J. E., Mitzova-Vladinov, G., Cacchione, M., Mato, J., Foronda, C. L., & Groom, J. A. (2020). Fire in the Operating Room: Use of Mixed Reality Simulation with Nurse Anesthesia Students. Informatics, 7(4), 40. https://doi.org/10.3390/informatics7040040