Towards a New Paradigm of Federated Electronic Health Records in Palestine



{kind=link}
{kind=link}
{kind=link}
Abstract
1. Background
- a.
- The first strategic area is to strengthen and build resilience of the Palestinian health system and progress to universal health coverage. Currently, the Italian government and the WHO support capacity building and data analysis in health information management and health financing. The aim is to improve health service delivery using the family medicine approach. They are also advancing the integration of services at the primary and secondary levels. The WHO has supported the Ministry of Health (MOH) to strengthen the quality of health care and patient safety. According to the Palestinian National Institute of Public Health (2018), there are 743 primary health care centers in Palestine (583 in the West Bank and 160 in Gaza), and 81 hospitals (51 in the West Bank, including East Jerusalem, and 30 in Gaza) [7]. Jabari et al. [2] reported that there were more than 400 primary care centers (governmental sector) connected to the District of Health Information Systems (DHIS).
- b.
- The second strategy is to strengthen core capacities in the Palestinian territories to meet the International Health Regulations (2005) [1]. This strategy includes the development of guidelines that will manage communicable disease outbreaks among all heath care providers and agencies, estimate and integrate event-based surveillance, strengthen coordination mechanisms within the MOH, etc.
- c.
- Noncommunicable diseases are the leading cause of morbidity and mortality in the Palestinian territories [7]. The WHO has listed this as the third strategy whereby the Organization will work with the MOH to boost the capacity to prevent, manage, and control noncommunicable diseases.
- d.
- The fourth strategy is to strength the capacity of the MOH and other health care providers to protect the right to health, reduce barriers to access, and improve social determinants of health.
2. Federated Electronic Health Records
- The software application should run in any mobile device or desktop;
- The protocol should be open, human readable, and easy to integrate with legacy EHR or new systems;
- The protocol should be flexible and must have an easy integration process.
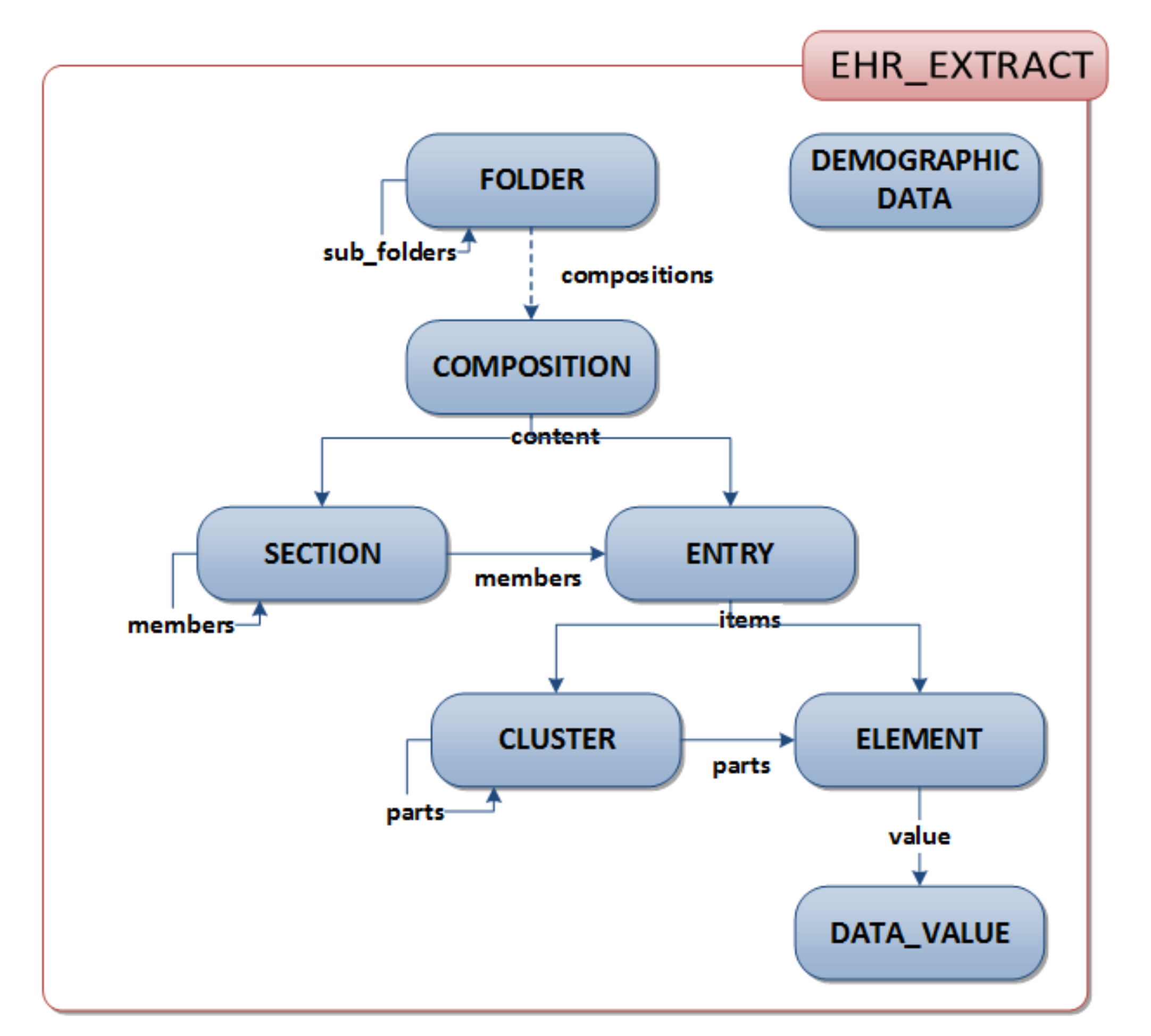
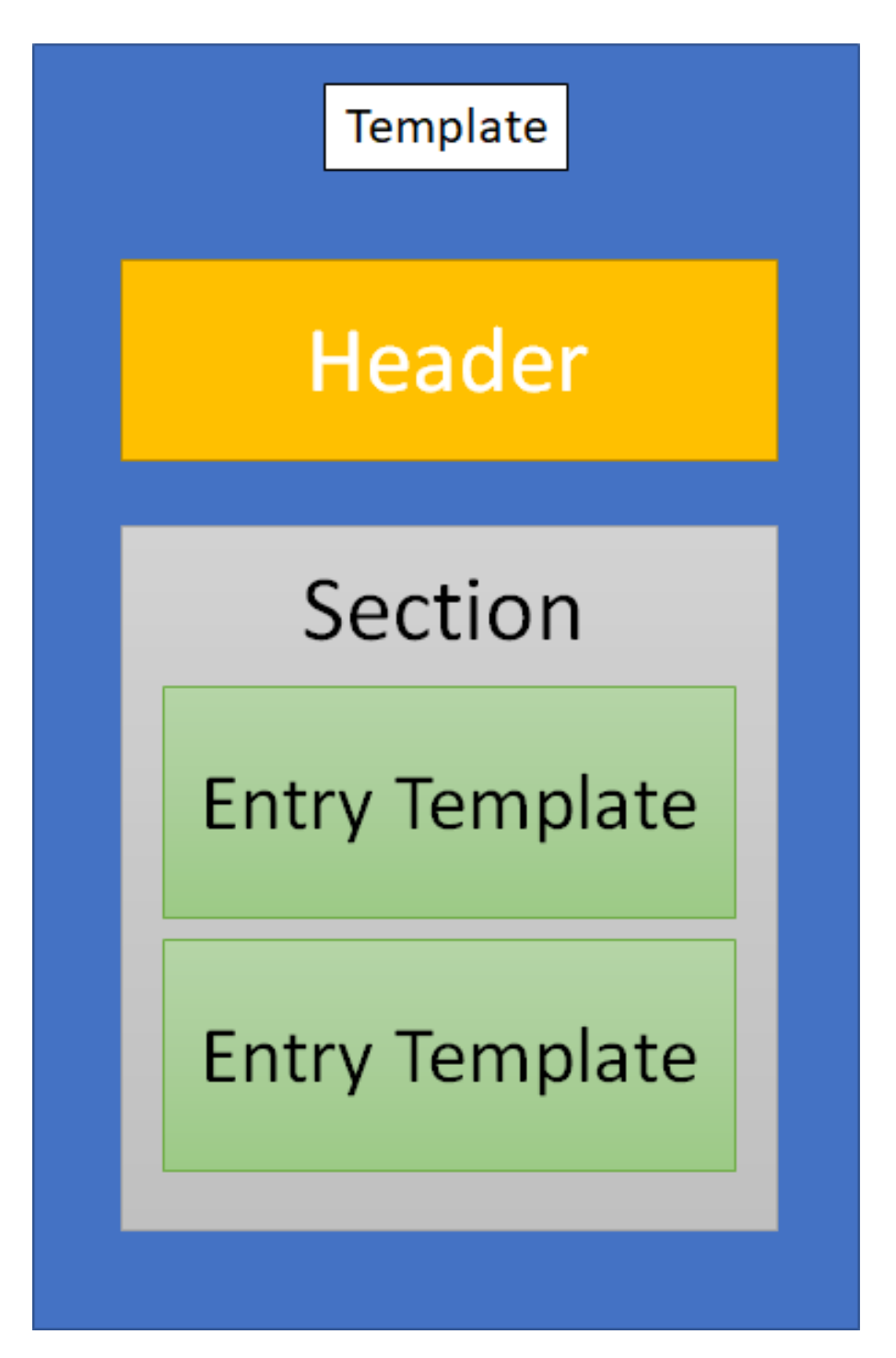
2.1. The Clinical Document Architecture (CDA)
- Persistence
- Stewardship
- Potential for authentication
- Context
- Wholeness
- Human readability
2.1.1. Advantages of CDA
- (1)
- Discharge summary note;
- (2)
- History and physical;
- (3)
- Progress note;
- (4)
- Consultation note;
- (5)
- Referral note;
- (6)
- Continuity of care document (CCD);
- (7)
- Unstructured document.
- Allergies
- Care team
- Encounters
- Family history
- Functional status
- Immunizations
- Medical equipment
- Medications
- Mental status
- Plan of treatment
- Problems
- Procedures
- Referrals—planned and completed
- Social history
- Vital signs
2.1.2. Compliance with Widely Accepted Ontologies and Technologies
2.1.3. Blockchain as a Solution
- EHR manager—this component is responsible for controlling all user EHR transactions;
- Admin— this component is responsible for deploying the smart contracts and manage the user permissions;
- Smart Contracts—this component is responsible for managing the Application Binary Interface;
- Decentralized Storage—this component is responsible for the storage of large amounts of data that cannot be shared with blockchain (e.g., clinical images, videos, or all multimedia data related with healthcare);
- Data block structure that defines the data organization and its contents.
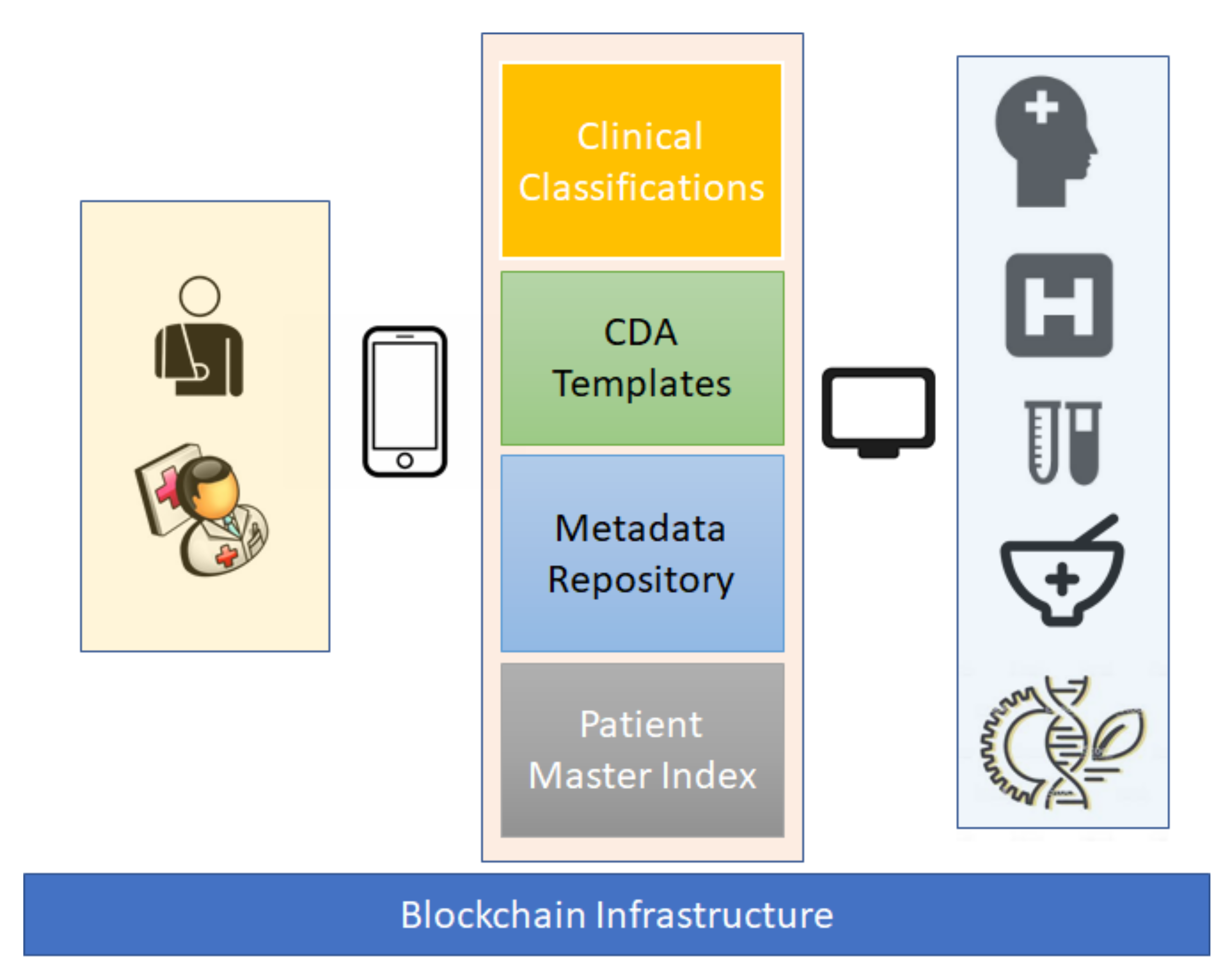
2.2. Detailed Architecture of the Proposed Model
- A decentralized and flexible format of electronic clinical messages should be used.
- The semantic alignment of the messages should be compliant with international standards but must also be adaptable to local culture.
- It should be possible to aggregate each piece of clinical data in a clinical episode and each episode in the EHR.
- The clinical data should be open to clinical research, but the patient’s identification should be secure.
- W3 PROV [18] (p. 3) to promote the information about data structures about the relationships among data elements, actors and activities;
- Repositories with clinical classifications aligned with the Value Set Authority Center [16];
- CDA infrastructure to promote the flexibility and dynamics of clinical charts.
2.3. Advantages of the Blockchain Infrastructure
2.4. Security, Privacy, and Confidentiality of the Proposed Model
3. Conclusions and Future Work
Funding
Conflicts of Interest
Abbreviations
| ATC | Anatomical Therapeutic Chemical Classification System |
| CDA | Clinical document architecture |
| DIACOM | Digital Imaging and Communications in Medicine |
| DHIS | District of health information systems |
| FEHR | Federated electronic health records |
| HIS | Hospital information system |
| ICD | International Classification of Disease |
| ICF | International Classification of Functioning, Disability and Health |
| ISO | International Organization of Standardization |
| MOH | Ministry of Health |
| SNOMED | Systematized Nomenclature of Medicine |
| UNRWA | United Nations Relief and Works Agency |
| WHO | World Health Organization |
| XML | Extended Markup Language |
References
- WHO. Global Health Observatory (GHO) Data. Available online: https://www.who.int/gho/goe/electronic_health_records/en/ (accessed on 22 August 2020).
- Jabari, C.; Adwan, L. Health informatics in the Arab world. In Handbook of Healthcare in the Arab World; Laher, I., Ed.; Springer: Cham, Switzerland, 2019; pp. 1–12. [Google Scholar] [CrossRef]
- Purkayastha, S.; Allam, R.; Maity, P.; Gichoya, J.W. Comparison of Open-Source Electronic Health Record Systems Based on Functional and User Performance Criteria. Heal. Informatics Res. 2019, 25, 89–98. [Google Scholar] [CrossRef] [PubMed]
- World Health Assembly. Health Conditions in the Occupied Palestinian Territory, Including East Jerusalem, and in the Occupied Syrian Golan: Report by the Director-General; World Health Organization: Geneva, Switzerland, 2019; Available online: https://apps.who.int/iris/handle/10665/328758 (accessed on 25 July 2020).
- Palestinian National Institute of Public Health. Overview of Public Health in Palestine. 2018. Available online: https://www.pniph.org/en/about/overview-of-public-health-in-palestine (accessed on 25 July 2020).
- Keelan, E. Medical Care in Palestine: Working in a Conflict Zone. Ulst. Med J. 2016, 85, 3–7. [Google Scholar]
- Palestinian Health Information Center. Health Annual Report: Palestine 2018; Palestinian Health Information Center: Ramallah, Palestine, 2019; Available online: http://healthclusteropt.org/admin/file_manager/uploads/files/1/Health%20Annual%20Report%20Palestine%202018.pdf (accessed on 28 June 2020).
- Shawahna, R. Merits, features, and desiderata to be considered when developing electronic health records with embedded clinical decision support systems in Palestinian hospitals: A consensus study. BMC Med Informatics Decis. Mak. 2019, 19, 216. [Google Scholar] [CrossRef] [PubMed]
- Ballout, G.; Al-Shorbaji, N.; Abu-Kishk, N.; Turki, Y.; Zeidan, W.; Seita, A. UNRWA’s innovative e-Health for 5 million Palestine refugees in the Near East. BMJ Innov. 2018. [Google Scholar] [CrossRef]
- Claerhout, B.; Kalra, D.; Mueller, C.; Singh, G.; Ammour, N.; Meloni, L.; Blomster, J.; Hopley, M.; Kafatos, G.; Garvey, A.; et al. Federated electronic health records research technology to support clinical trial protocol optimization: Evidence from EHR4CR and the InSite platform. J. Biomed. Informatics 2019, 90, 10–30. [Google Scholar] [CrossRef] [PubMed]
- Katehakis, D.; Sfakianakis, S.; Tsiknakis, M.; Orphanoudakis, S.C. Fundamental components for the realization of a federated Integrated Electronic Health Record environment. In Proceedings of the 23rd Annual International Conference of the IEEE, Engineering in Medicine and Biology, Istanbul, Turkey, 25–28 October 2001. [Google Scholar] [CrossRef]
- Dewri, R.; Ong, T.C.; Thurimella, R. Linking Health Records for Federated Query Processing. Proc. Priv. Enhanc. Technol. 2016, 2016, 4–23. [Google Scholar] [CrossRef]
- Alhaqbani, B.; Fidge, C. Access control requirements for processing electronic health records. In Business Process Management Workshops. BPM 2007. Lecture Notes in Computer Science; Hofstede, A., Benatallah, B., Paik, H.Y., Eds.; Springer: Berlin/Heidelberg, Germany, 2008; Volume 4928. [Google Scholar] [CrossRef]
- Keith, W.B. The CDA TM Book; Springer-Verlag: London, UK, 2011. [Google Scholar]
- HL7 Searchable Project Index—Consolidated CDA STU 2019 Update (PSS in Confluence); HL7 International. Available online: https://www.hl7.org/special/Committees/projman/searchableProjectIndex.cfm?action=edit&ProjectNumber%20=1520 (accessed on 13 June 2020).
- Chelsom, J.; Pande, I.; Gaywood, I.; Granja, C.; Bolle, S. Document-driven care pathways using HL7 CDA. In Proceedings of the eTELEMED 2015, The Seventh International Conference on eHealth, Telemedicine and Social Medicine, Lisbon, Portugal, 27 February 2015. [Google Scholar]
- Lantana Consulting Group. Trifolia-on-FHIR. Transforming Healthcare through Health Information. Available online: http://www.lantanagroup.com/our-software-products/trifolia-on-fhir/ (accessed on 21 June 2020).
- PROV-Overview. Available online: https://www.w3.org/TR/prov-overview/ (accessed on 21 June 2020).
- Missier, P.; Belhajjame, K.; Cheney, J. The W3C PROV family of specifications for modelling provenance metadata. In Proceedings of the 16th International Conference on Extending Database Technology, Genoa, Italy, 18–22 March 2013; pp. 773–776. [Google Scholar] [CrossRef]
- Cross-Enterprise Document Sharing—IHE Wiki. Available online: https://wiki.ihe.net/index.php/Cross-Enterprise_Document_Sharing (accessed on 21 June 2020).
- Margheri, A.; Masi, M.; Miladi, A.; Sassone, V.; Rosenzweig, J. Decentralised provenance for healthcare data. Int. J. Med Inform. 2020, 141. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, D.C.; Pathirana, P.N.; Ding, M.; Seneviratne, A. Blockchain for Secure EHRs Sharing of Mobile Cloud Based E-Health Systems. IEEE Access 2019, 7, 66792–66806. [Google Scholar] [CrossRef]
- Anastasiia, L. Blockchain Architecture Explained: How It Works & How to Build. Available online: https://mlsdev.com/blog/156-how-to-build-your-own-blockchain-architecture (accessed on 3 July 2020).
- Inupakutika, D.; Kaghyan, S.; Akopian, D.; Chalela, P.; Ramirez, A.G. Facilitating the development of cross-platform mHealth applications for chronic supportive care and a case study. J. Biomed. Inform. 2020, 105, 103420. [Google Scholar] [CrossRef] [PubMed]



© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
El Jabari, C.; Macedo, M.; Al-jabari, M.O. Towards a New Paradigm of Federated Electronic Health Records in Palestine. Informatics 2020, 7, 41. https://doi.org/10.3390/informatics7040041
El Jabari C, Macedo M, Al-jabari MO. Towards a New Paradigm of Federated Electronic Health Records in Palestine. Informatics. 2020; 7(4):41. https://doi.org/10.3390/informatics7040041
Chicago/Turabian StyleEl Jabari, Carol, Mario Macedo, and Mohanad O. Al-jabari. 2020. "Towards a New Paradigm of Federated Electronic Health Records in Palestine" Informatics 7, no. 4: 41. https://doi.org/10.3390/informatics7040041
APA StyleEl Jabari, C., Macedo, M., & Al-jabari, M. O. (2020). Towards a New Paradigm of Federated Electronic Health Records in Palestine. Informatics, 7(4), 41. https://doi.org/10.3390/informatics7040041