
Two-Year Longitudinal Motor Performance of Very Preterm and/or Very-Low-Birth-Weight Infants in Suriname

 , , and
, , and
Abstract
1. Introduction
2. Materials and Methods
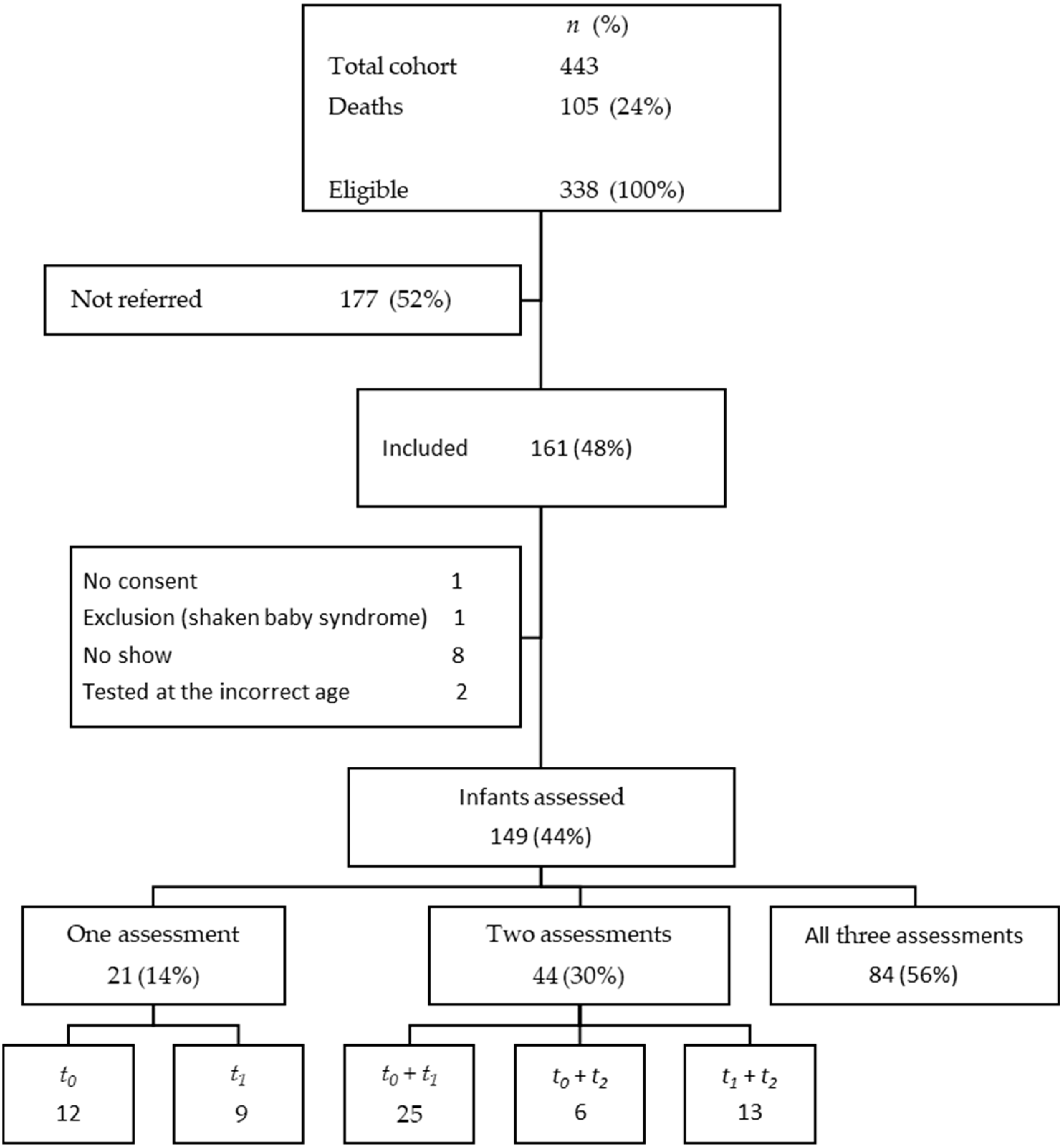
2.1. Design and Participants
2.2. Outcome Measures
2.2.1. Assessment of Motor Performance
2.2.2. Perinatal and Environmental Factors
2.2.3. Early Motor Intervention Program (EIP)
2.3. Statistical Analysis
3. Results
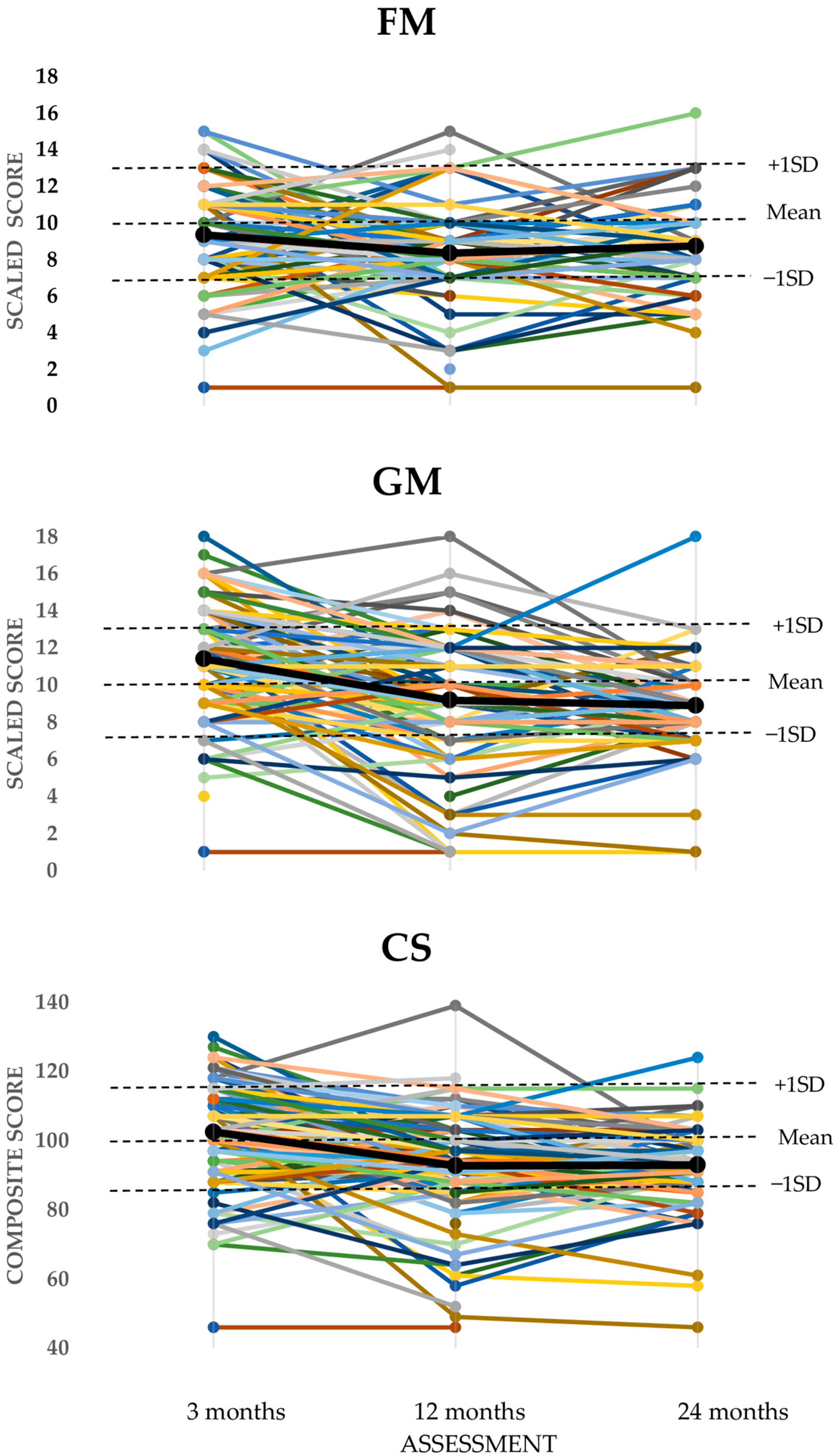
3.1. Longitudinal Motor Performance
3.2. Influence of Perinatal or Environmental Factors on Longitudinal Performance
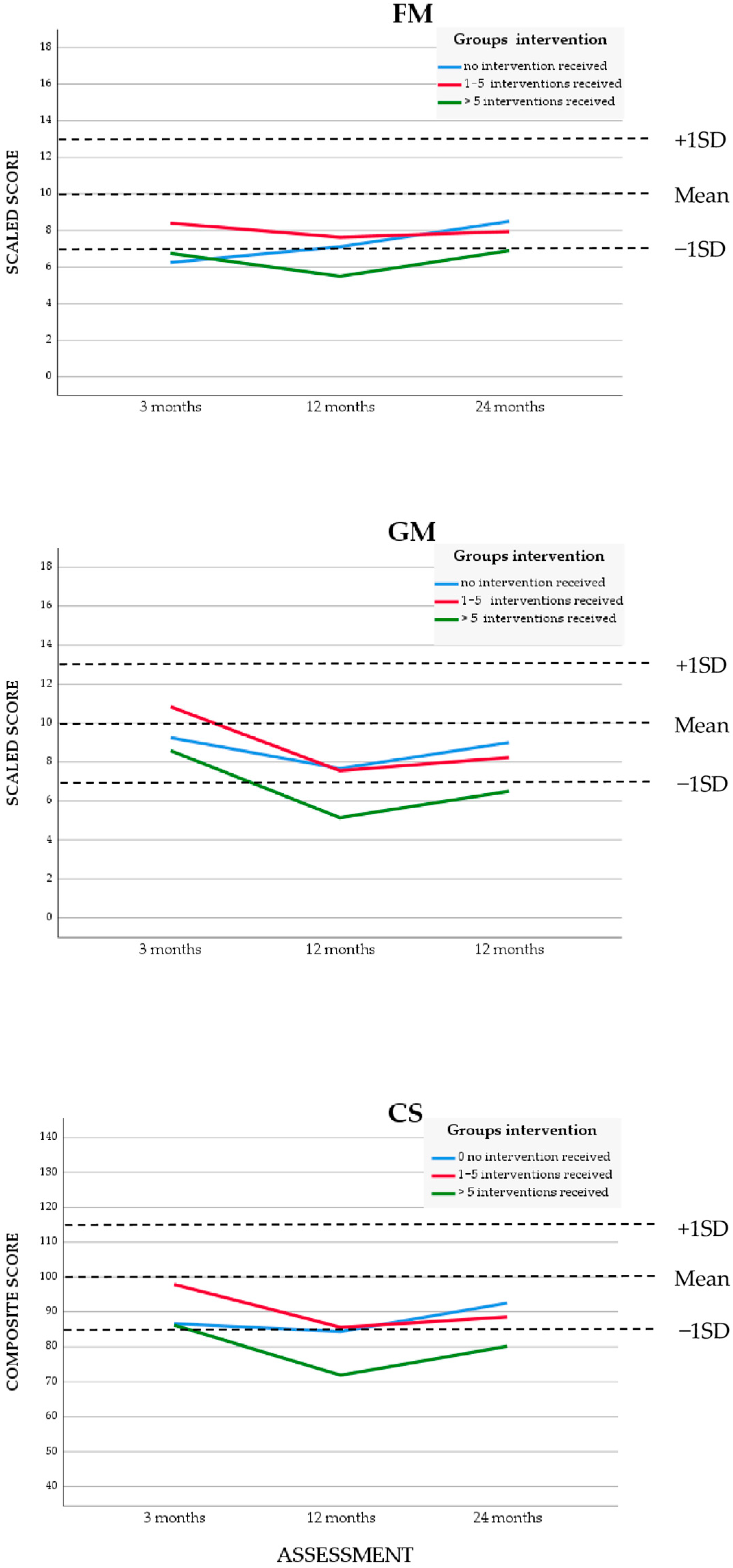
3.3. Influence of the Early Intervention Program
4. Discussion
4.1. Exploration of Influence of Perinatal or Environmental Factors
4.2. Exploration of the Influence of an Early Intervention Program
4.3. Strengths and Limitations
4.4. Implications for Future Studies
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| VPT | Very preterm |
| VLBW | Very low birth weight |
| HIC | High income country |
| LMIC | Low- or middle-income country |
| MIC | Middle-income country |
| GA | Gestational age |
| NICU | Neonatal intensive care unit |
| BW | Birth weight |
| EIP | Early intervention program |
| BSID-III | Bayley scales of infant and toddler development, third version |
| FM | Fine motor |
| GM | Gross motor |
| CS | Composite score |
| PPT | Pediatric physical therapist |
| CA | Corrected age |
| SS | Scales scores |
| SGA | Small for gestational age |
| AS | Apgar score |
Appendix A. Early Intervention Program (EIP)
- First session: explanation motor delay and recommendations for home to parents/caregivers. (±45 min)
- First 4 weeks: once a week feedback and if necessary, adjusting recommendations. (±30 min)
- Second and third month: once per month feedback and if necessary, adjusting recommendations. (±30 min)
- After 3 months: repeat BSID III. (depending on age 30 to 45 min)
- If score below average:
- check once a month with feedback and if necessary, adjusting recommendations.
- After 3 months: BSID III (repeat from point 4).
- If score average or higher:
- repeat BSID III after 3 months.
- When BSID III on two consecutively assessments is average or higher: continue standard follow-up program.
- Instructions and recommendations are given on positioning (e.g., tummy time when infant is awake), and how to elicit movements in a playful way.
- Instructions and recommendations are given verbally and are demonstrated.
- Parents/caregivers are encouraged to film the therapy sessions with their smartphone, If that was not possible it was filmed by the pediatric physical therapy department and supplied on CD/DVD.
- The parents/caregivers are then asked to practice themselves during the therapy session and coaching and feedback was given.
References
- Evensen, K.A.I.; Ustad, T.; Tikanmaki, M.; Haaramo, P.; Kajantie, E. Long-term motor outcomes of very preterm and/or very low birth weight individuals without cerebral palsy: A review of the current evidence. Semin. Fetal Neonatal. Med. 2020, 25, 101116. [Google Scholar] [CrossRef] [PubMed]
- Pascal, A.; Govaert, P.; Oostra, A.; Naulaers, G.; Ortibus, E.; Van den Broeck, C. Neurodevelopmental outcome in very preterm and very-low-birthweight infants born over the past decade: A meta-analytic review. Dev. Med. Child. Neurol. 2018, 60, 342–355. [Google Scholar] [CrossRef] [PubMed]
- Boonzaaijer, M.; Suir, I.; Mollema, J.; Nuysink, J.; Volman, M.; Jongmans, M. Factors associated with gross motor development from birth to independent walking: A systematic review of longitudinal research. Child. Care Health Dev. 2021, 47, 525–561. [Google Scholar] [CrossRef] [PubMed]
- Valentini, N.C.; de Borba, L.S.; Panceri, C.; Smith, B.A.; Procianoy, R.S.; Silveira, R.C. Early Detection of Cognitive, Language, and Motor Delays for Low-Income Preterm Infants: A Brazilian Cohort Longitudinal Study on Infant Neurodevelopment and Maternal Practice. Front. Psychol. 2021, 12, 753551. [Google Scholar] [CrossRef]
- Namazzi, G.; Tumwine, J.K.; Hildenwall, H.; Ndeezi, G.; Mubiri, P.; Hanson, C.; Kakooza-Mwesige, A.; Waiswa, P. Neurodevelopmental outcomes of preterm babies during infancy in Eastern Uganda: A prospective cohort study. Glob. Health Action 2020, 13, 1820714. [Google Scholar] [CrossRef]
- Ballot, D.E.; Potterton, J.; Chirwa, T.; Hilburn, N.; Cooper, P.A. Developmental outcome of very low birth weight infants in a developing country. BMC Pediatr. 2012, 12, 11. [Google Scholar] [CrossRef]
- Pieris, L.; Sigera, P.C.; De Silva, A.P.; Munasinghe, S.; Rashan, A.; Athapattu, P.L.; Jayasinghe, K.S.A.; Samarasinghe, K.; Beane, A.; Dondorp, A.M.; et al. Experiences of ICU survivors in a low middle income country—A multicenter study. BMC Anesthesiol. 2018, 18, 30. [Google Scholar] [CrossRef]
- Sefidkar, R.; Zayeri, F.; Kazemi, E.; Salehi, M.; Dehnad, A.; Hafizi, M. A Trend Study of Preterm Infant Mortality Rate in Developed and Developing Countries over 1990 to 2017. Iran. J. Public Health 2021, 50, 369–375. [Google Scholar] [CrossRef]
- Mactier, H.; Bates, S.E.; Johnston, T.; Lee-Davey, C.; Marlow, N.; Mulley, K.; Smith, L.K.; To, M.; Wilkinson, D.; Grp, B.W. Perinatal management of extreme preterm birth before 27 weeks of gestation: A framework for practice. Arch. Dis. Child-Fetal 2020, 105, F232–F239. [Google Scholar] [CrossRef]
- Sansavini, A.; Savini, S.; Guarini, A.; Broccoli, S.; Alessandroni, R.; Faldella, G. The effect of gestational age on developmental outcomes: A longitudinal study in the first 2 years of life. Child Care Health Dev. 2011, 37, 26–36. [Google Scholar] [CrossRef]
- Karasik, L.B.; Adolph, K.E.; Tamis-Lemonda, C.S.; Bornstein, M.H. WEIRD walking: Cross-cultural research on motor development. Behav. Brain Sci. 2010, 33, 95–96. [Google Scholar] [CrossRef]
- Oudgenoeg-Paz, O.; Atun-Einy, O.; van Schaik, S.D.M. Two Cultural Models on Infant Motor Development: Middle Class Parents in Israel and the Netherlands. Front. Psychol. 2020, 11, 119. [Google Scholar] [CrossRef]
- Jeon, M.; Dimitriou, D.; Halstead, E.J. A Systematic Review on Cross-Cultural Comparative Studies of Sleep in Young Populations: The Roles of Cultural Factors. Int. J. Environ. Res. Public Health 2021, 18, 2005. [Google Scholar] [CrossRef] [PubMed]
- Karasik, L.B.; Robinson, S.R. Milestones or Millstones: How Standard Assessments Mask Cultural Variation and Misinform Policies Aimed at Early Childhood Development. Policy Insights Behav. Brain Sci. 2022, 9, 57–64. [Google Scholar] [CrossRef]
- Pan American Health Organization, World Health Organization. Health in de Americas, Suriname—Country Profile 17 October, 2024. Available online: https://hia.paho.org/en/country-profiles/suriname (accessed on 16 March 2025).
- Worldometer. Countries in the World by Population 2022. Available online: https://www.worldometers.info/world-population/population-by-country/ (accessed on 4 May 2022).
- Verschueren, K.J.C.; Prust, Z.D.; Paidin, R.R.; Kodan, L.R.; Bloemenkamp, K.W.M.; Rijken, M.J.; Browne, J.L. Childbirth outcomes and ethnic disparities in Suriname: A nationwide registry-based study in a middle-income country. Reprod. Health 2020, 17, 62. [Google Scholar] [CrossRef]
- Janssen, A.J.; Akkermans, R.P.; Steiner, K.; de Haes, O.A.; Oostendorp, R.A.; Kollee, L.A.; Nijhuis-van der Sanden, M.W. Unstable longitudinal motor performance in preterm infants from 6 to 24 months on the Bayley Scales of Infant Development--Second edition. Res. Dev. Disabil. 2011, 32, 1902–1909. [Google Scholar] [CrossRef]
- Khurana, S.; Kane, A.E.; Brown, S.E.; Tarver, T.; Dusing, S.C. Effect of neonatal therapy on the motor, cognitive, and behavioral development of infants born preterm: A systematic review. Dev. Med. Child Neurol. 2020, 62, 684–692. [Google Scholar] [CrossRef]
- Mobbs, C.; Spittle, A.; Johnston, L. PreEMPT (Preterm infant Early intervention for Movement and Participation Trial): Feasibility outcomes of a randomised controlled trial. Early Hum. Dev. 2022, 166, 105551. [Google Scholar] [CrossRef]
- Orton, J.; Doyle, L.W.; Tripathi, T.; Boyd, R.; Anderson, P.J.; Spittle, A. Early developmental intervention programmes provided post hospital discharge to prevent motor and cognitive impairment in preterm infants. Cochrane Database Syst. Rev. 2024, 2, CD005495. [Google Scholar] [CrossRef]
- Jiang, L.; Lee Him, R.; Sihota, D.; Muralidharan, O.; Dominguez, G.; Harrison, L.; Vaivada, T.; Bhutta, Z.A. Supportive Care for Common Conditions in Small Vulnerable Newborns and Term Infants: The Evidence. Neonatology 2025, 122, 129–151. [Google Scholar] [CrossRef]
- Bayley, N. Bayley Scales of Infant and Toddler Development Third Edition Manual; Pearson PsychCop: San Antonio, TX, USA, 2005. [Google Scholar]
- Pendergast, L.L.; Schaefer, B.A.; Murray-Kolb, L.E.; Svensen, E.; Shrestha, R.; Rasheed, M.A.; Scharf, R.J.; Kosek, M.; Vasquez, A.O.; Maphula, A.; et al. Assessing development across cultures: Invariance of the Bayley-III Scales Across Seven International MAL-ED sites. Sch. Psychol. Q. 2018, 33, 604–614. [Google Scholar] [CrossRef] [PubMed]
- McLester-Davis, L.W.Y.; Shankar, A.; Kataria, L.A.; Hidalgo, A.G.; van Eer, E.D.; Koendjbiharie, A.P.; Ramjatan, R.; Hatch, V.I.; Middleton, M.A.; Zijlmans, C.W.R.; et al. Validity, reliability, and transcultural adaptations of the Bayley Scales of Infant and Toddler Development (BSID-III-NL) for children in Suriname. Early Hum. Dev. 2021, 160, 105416. [Google Scholar] [CrossRef] [PubMed]
- Fleurkens-Peeters, M.J.; Zijlmans, W.C.; Akkermans, R.P.; Sanden, M.W.N.; Janssen, A.J. The United States reference values of the Bayley III motor scale are suitable in Suriname. Infant Behav. Dev. 2024, 74, 101922. [Google Scholar] [CrossRef] [PubMed]
- Fenton, T.R.; Kim, J.H. A systematic review and meta-analysis to revise the Fenton growth chart for preterm infants. BMC Pediatr. 2013, 13, 59. [Google Scholar] [CrossRef]
- Bersaoui, M.; Bisai, A.; Baldew, S.M.; Toelsie, J.; Goessler, K.; Cornelissen, V.A. Can postexercise hypotension also be observed in African and Asian populations: A systematic review and meta-analysis of randomized controlled trials. J. Hum. Hypertens. 2023, 37, 1076–1085. [Google Scholar] [CrossRef]
- Heemskerk, M.D.C. Suriname Migration Profile. A Study on Emigration from, and Immigration into Suriname. Available online: https://publications.iom.int/system/files/pdf/mp_suriname2015.pdf (accessed on 11 July 2022).
- Selvanathan, T.; Guo, T.; Ufkes, S.; Chau, V.; Branson, H.; Synnes, A.; Ly, L.G.; Kelly, E.N.; Grunau, R.E.; Miller, S.P. Size and Location of Preterm Brain Injury and Associations With Neurodevelopmental Outcomes. Neurology 2024, 102, e209264. [Google Scholar] [CrossRef]
- Walani, S.R. Global burden of preterm birth. Int. J. Gynaecol. Obstet. 2020, 150, 31–33. [Google Scholar] [CrossRef]
- Cao, G.; Liu, J.; Liu, M. Global, Regional, and National Incidence and Mortality of Neonatal Preterm Birth, 1990–2019. JAMA Pediatr. 2022, 176, 787–796. [Google Scholar] [CrossRef]
- Coletti, M.F.; Caravale, B.; Gasparini, C.; Franco, F.; Campi, F.; Dotta, A. One-year neurodevelopmental outcome of very and late preterm infants: Risk factors and correlation with maternal stress. Infant Behav. Dev. 2015, 39, 11–20. [Google Scholar] [CrossRef]
- Do, C.H.T.; Kruse, A.Y.; Wills, B.; Sabanathan, S.; Clapham, H.; Pedersen, F.K.; Pham, T.N.; Vu, P.M.; Borresen, M.L. Neurodevelopment at 2 years corrected age among Vietnamese preterm infants. Arch. Dis. Child. 2020, 105, 134–140. [Google Scholar] [CrossRef]
- Ertem, I.O.; Krishnamurthy, V.; Mulaudzi, M.C.; Sguassero, Y.; Balta, H.; Gulumser, O.; Bilik, B.; Srinivasan, R.; Johnson, B.; Gan, G.L.; et al. Similarities and differences in child development from birth to age 3 years by sex and across four countries: A cross-sectional, observational study. Lancet Glob. Health 2018, 6, E279–E291. [Google Scholar] [CrossRef] [PubMed]
- Koshy, B.; Srinivasan, M.; Bose, A.; John, S.; Mohan, V.R.; Roshan, R.; Ramanujam, K.; Kang, G. Developmental trends in early childhood and their predictors from an Indian birth cohort. BMC Public Health 2021, 21, 1083. [Google Scholar] [CrossRef] [PubMed]
- Pires, C.D.S.; Marba, S.T.M.; Caldas, J.P.S.; Stopiglia, M.C.S. Predictive Value of the General Movements Assessment in Preterm Infants: A Meta-Analysis. Rev. Paul. Pediatr. 2020, 38, e2018286. [Google Scholar] [CrossRef]
- Kadam, A.S.; Nayyar, S.A.; Kadam, S.S.; Patni, B.C.; Khole, M.C.; Pandit, A.N.; Kabra, N.S. General Movement Assessment in Babies Born Preterm: Motor Optimality Score-Revised (MOS-R), Trajectory, and Neurodevelopmental Outcomes at 1 Year. J. Pediatr. X 2023, 8, 100084. [Google Scholar] [CrossRef] [PubMed]
- Panceri, C.; Silveira, R.C.; Procianoy, R.S.; Valentini, N.C. Motor development in the first year of life predicts impairments in cognition and language at 3 years old in a Brazilian preterm cohort of low-income families. Front. Neurosci. 2022, 16, 1034616. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
| Total Group (n = 149) | No EIP (n = 95) | Referred for EIP (n = 54) | ||||
|---|---|---|---|---|---|---|
| Mean | SD (Range) | Mean | SD (Range) | Mean | SD (Range) | |
| GA (weeks) | 29+6 | 2.13 (25+6–36+3) | 30+1 | 2.02 (25+6–36+0) | 29+5 | 2.20 (26+0–36+3) |
| BW (grams) | 1271 | 303.9 (640–1990) | 1310 | 311.0 (640–1990) | 1201 | 280.1 (730–1920) * |
| z-score BW * | −0.58 | 1.17 (−3.8–3.3) | −0.50 | 1.23 (−3.8–3.3) | −0.72 | 1.06 (−3.5–1.0) |
| Age mother (years) | 27.2 | (14–41) | 27.3 | (15–41) | 27.1 | (14–40) |
| Median | (Range) | Median | (Range) | Median | (Range) | |
| Apgar Score | 9 | (1–10) | 9 | (1–10) | 8.5 | (1–9) |
| n | (%) | n | (%) | n | (%) | |
| Apgar score < 7 | 18 | (12.1) | 9 | (9.5) | 9 | (16.7) |
| Gender | ||||||
| Boys | 74 | (49.7) | 45 | (47.4) | 29 | (53.7) |
| Girls | 75 | (50.3) | 50 | (52.6) | 25 | (46.3) |
| Z-score BW * | ||||||
| SGA z-score < −1.28 | 40 | (26.8) | 29 | (30.5) | 14 | (26.9) |
| AGA z-score | 100 | (67.2) | 62 | (65.3) | 38 | (73.1) |
| LGA z-score > 1.28 | 3 | (2.0) | 4 | (4.2) | 0 | (0.0) |
| missing | 6 | (4.0) | – | – | – | – |
| Multiple birth | ||||||
| Singleton | 124 | (83.2) | 85 | (89.5) | 39 | (72.2) |
| Twin | 21 | (14.1) | 8 | (8.4) | 13 | (24.1) |
| Triplet | 4 | (2.7) | 2 | (2.1) | 2 | (3.7) |
| Ethnicity infant | ||||||
| African: | 53 | (35.6) | 38 | (40.0) | 18 | (33.3) |
| Creole | 25 | (16.8) | ||||
| Tribal | 28 | (18.8) | ||||
| Asian: | 45 | (30.2) | 28 | (29.5) | 17 | (31.5) |
| Chinese | 1 | (0.7) | ||||
| Hindustani | 32 | (21.5) | ||||
| Javanese | 12 | (8.1) | ||||
| Mixed and other: | 38 | (25.5) | 21 | (22.1) | 17 | (31.5) |
| Indigenous | 1 | (0.7) | ||||
| Mixed | 37 | (24.8) | ||||
| Missing | 13 | (8.7) | 8 | (8.4) | 2 | (3.7) |
| Highest maternal educational level | ||||||
| Low a | 40 | (28.8) | 24 | (25.3) | 22 | (40.7) |
| Low average b | 39 | (28) | 27 | (28.4) | 11 | (20.4) |
| Average c | 36 | (25.9) | 27 | (28.4) | 13 | (24.1) |
| High d | 7 | (5) | 5 | (5.3) | 2 | (3.7) |
| Missing | 17 | (12.2) | 12 | (12.6) | 6 | (11.1) |
| Overall Scores | Corrected for EIP a | |||||
|---|---|---|---|---|---|---|
| Mean | 95% CI | Estimate of Change from t0 | p Value | Estimate of Change from t0 | p Value | |
| FM | <0.001 * | 0.015 * | ||||
| t0 | 9.32 | 8.91–9.73 | ||||
| t1 | 8.36 | 7.95–8.77 | −0.96 | <0.001 | −0.76 | 0.004 |
| t2 | 8.66 | 8.21–9.12 | −0.66 | 0.014 | −0.42 | 0.134 |
| GM | <0.001 * | <0.001 * | ||||
| t0 | 11.39 | 10.90–11.87 | ||||
| t1 | 9.18 | 8.70–9.65 | −2.20 | <0.001 | −1.94 | <0.001 |
| t2 | 8.78 | 8.25–9.31 | −2.60 | <0.001 | −2.29 | <0.001 |
| CS | <0.001 * | <0.001 * | ||||
| t0 | 102.25 | 99.92–104.57 | ||||
| t1 | 92.74 | 90.44–95.04 | −9.50 | <0.001 | −8.31 | <0.001 |
| t2 | 92.24 | 89.73–94.76 | −10.0 | <0.001 | −8.55 | <0.001 |
| FM p Value | GM p Value | CS p Value | |
|---|---|---|---|
| Gender | 0.442 | 0.164 | 0.179 |
| Teenaged mother | 0.630 | 0.292 | 0.304 |
| Ethnicity infant | 0.209 | 0.773 | 0.352 |
| Maternal educational level | 0.206 | 0.421 | 0.283 |
| GA | 0.497 | 0.394 | 0.304 |
| BW (z-score) | 0.013 * | 0.097 | 0.009 * |
| Apgar score (dichotomized) | 0.560 | 0.075 | 0.173 |
| Multiple birth | 0.065 | 0.935 | 0.300 |
| Ventilation | 0.999 | 0.768 | 0.892 |
| Sepsis | 0.402 | 0.095 | 0.102 |
| Indication for EIP | 0.293 | 0.718 | 0.340 |
| EIP frequency | 0.406 | 0.775 | 0.452 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Janssen, A.J.W.M.; Fleurkens-Peeters, M.J.A.J.; Akkermans, R.P.; Baldew, S.-S.M.; Nijhuis-van der Sanden, M.W.G.; Zijlmans, W.C.W.R. Two-Year Longitudinal Motor Performance of Very Preterm and/or Very-Low-Birth-Weight Infants in Suriname. Children 2025, 12, 414. https://doi.org/10.3390/children12040414
Janssen AJWM, Fleurkens-Peeters MJAJ, Akkermans RP, Baldew S-SM, Nijhuis-van der Sanden MWG, Zijlmans WCWR. Two-Year Longitudinal Motor Performance of Very Preterm and/or Very-Low-Birth-Weight Infants in Suriname. Children. 2025; 12(4):414. https://doi.org/10.3390/children12040414
Chicago/Turabian StyleJanssen, Anjo J. W. M., Maria J. A. J. Fleurkens-Peeters, Reinier P. Akkermans, Se-Sergio M. Baldew, Maria W. G. Nijhuis-van der Sanden, and Wilco C. W. R. Zijlmans. 2025. "Two-Year Longitudinal Motor Performance of Very Preterm and/or Very-Low-Birth-Weight Infants in Suriname" Children 12, no. 4: 414. https://doi.org/10.3390/children12040414
APA StyleJanssen, A. J. W. M., Fleurkens-Peeters, M. J. A. J., Akkermans, R. P., Baldew, S.-S. M., Nijhuis-van der Sanden, M. W. G., & Zijlmans, W. C. W. R. (2025). Two-Year Longitudinal Motor Performance of Very Preterm and/or Very-Low-Birth-Weight Infants in Suriname. Children, 12(4), 414. https://doi.org/10.3390/children12040414