1. Introduction
According to the South China Morning Post, the first case of coronavirus was reported in China’s Hubei County in December 2019, about a month before the case was reported in Wuhan, China. The novel Coronavirus SARS-CoV-2 was named COVID-19 by the World Health Organization in the month of February, 2020. The virus is a zoonotic disease because it began in animals and then spread to humans. The coronavirus originated in China and quickly spread throughout the world due to migration. This virus has spread to around 210 countries [
1]. Coronavirus can affect people of any age, according to the World Health Organization, but people over the age of 60 are particularly vulnerable. Common symptoms of the disease include a cold, cough, ache, fever, and other symptoms that appear after a 14-day incubation period. The disease was declared a pandemic on 11 March 2020, due to its alarming spread [
2]. A study conducted in Wuhan, China in January 2020 confirmed about 41 patients with COVID-19 [
3]. The patients’ symptoms were similar to severe respiratory problems such as fever and cough, with less common symptoms including diarrhoea and headache. People with a history of diseases, like hypertension and diabetes, made up nearly half of the infected population [
3]. Severe Acute Respiratory Syndrome Coronavirus (SARS-CoV) and Middle East Respiratory Syndrome Coronavirus (MERS-CoV) have been found to be similar to this novel COVID-19 disease [
4]. Unlike SARS, which is caused by SARS-CoV, and MERS, which is caused by MERS-CoV, COVID-19 is caused by the SARS-CoV-2 virus. Simulation of Covid-19 pandemic in United Arab Emirates is performed using SIR model in [
5]. A study on the hepatitis B virus (HBV) using nonlinear incidence rate for developing the epidemic model was also studied [
6].
Many authors have worked on mathematical modelling of COVID-19 pandemic. For example, Yousefpour et al. [
7] use a genetic algorithm to investigate optimal control strategies on COVID-19. Singh et al. [
8] estimated the number of coronavirus-related deaths in various countries around the world. To study SARS-COVID 19 transmission, an agent-based model is created and parameterized with US demographics. Initially, high-risk individuals and healthcare professionals were given priority for vaccination, while children were not taken into consideration [
9].
In 2020, the team of [
10] investigated the characteristics of the novel coronavirus disease and provides an explanatory analysis. A report is prepared, addressing the cases through 11 February 2020 in China. The virus spread outward from Hubei to almost every country in a short span of time. It is concluded that in a period of 30 days, the entire land of China got infected with the disease. The number of coronavirus-infected patients in mainland China has been studied. The number of confirmed coronavirus infected cases peaked between 31 January and 4 February 2020, but dropped significantly between 5 February and 9 February 2020. The precautionary control measures taken by the government at state levels and at many other levels have shown a decline in the number of confirmed cases [
11]. The disease outbreak caused by the new coronavirus shook the entire world, with 73 million confirmed cases and 1.5 million deaths as of 14 December 2020 [
12]. In comparison to the management of an isolated population, it has been discovered that managing a quarantined population has a significant impact on disease declination. Quarantined, isolated, and transmission rate modification factors were investigated and found to be an effective strategy for disease control [
12]. Both types of disease controls, namely control at the basic level and control in reproduction numbers, are discussed in the paper [
12] for the COVID-19 model. A statistical study of the countries most affected by the new COVID-19 infection was conducted. The data regarding the infected persons were collected and fitted with various growth models of different countries. Following that, a comparative study was conducted in order to lower the infection rate and take preventative measures to address the various factors affecting the epidemic [
13]. A study is conducted for investigating the potential transmission from the infectious source (bats) to humans by the formation of Bats–Hosts–Reservoir–People transmission network system [
14]. In addition, the basic reproduction number is calculated for the system to examine the transmission of COVID-19 [
14]. The model was created to investigate the relationship between the infection source (bats), hosts, and the human population. A simplified version of the model is discussed in [
14], which focuses on the host–human interaction. The reproduction number is calculated to investigate the transmission process.
Natsuko et al. [
15] investigated that human transmission was the only possible cause of disease outbreak in Wuhan, China. Control measures have the potential to prevent up to 60 percent of disease transmission. It is quite clear from the earlier outbreaks of SARS-CoV and MERS-CoV that the number of infections transmitted by a single patient with COVID-19 is variable in nature. In some cases, there may be multiple secondary infections, while in others, there may be fewer. Adam et al. [
16] conducted research to predict the early transmission of the novel coronavirus outside of Wuhan, China. A mathematical model has been developed to better understand the dynamics of human-to-human transmission and the impact of various control measures. The model is formed while taking into consideration the four dataries from China and estimated to assess the transmission outside China. Various vaccination strategies and an SEIR (Susceptible–Exposed–Infected–Recovered) model for different populations have been investigated. To help the system in overcoming the infection, various threshold parameters have been calculated [
17]. In [
18], it has been demonstrated that in the case of deadly diseases such as COVID-19, migration can slow the spread of the epidemic; however, this is at the cost of contaminating nearby areas.
This worldwide pandemic hit the Kerala state of India on 30 January 2020, when the first case was detected. The capital then reported the first COVID-19 positive person on 2 February 2020, as a result of an Italian visitor [
19]. Various control measures have been implemented in India, beginning with the lockdown on 24 March 2020, but the number of active cases continues to rise, particularly in the Delhi and Maharashtra regions of the country. As of 5 March 2020, around 29 cases were reported in India [
20]. Although the virus is deadly and spreads quickly, it has a low fatality rate when compared to the previous two viruses. So far, it is noticed that children are the least affected with the virus [
21]. The future of the virus is still uncertain and remains to be predicted. COVID-19 has spread throughout the globe, and billions of people are attempting to combat this serious issue. As a result, an attempt is being made to study and test this disease using mathematical modelling. The proposed model is interpretable from a human point of view and heuristically justifiable. The proposed system has six compartments and is extremely useful in applied epidemiology.
The current paper is divided into the following sections, with
Section 2 dealing with the creation of mathematical models. The model basic preliminaries, basic reproduction number and sensitivity analysis are also discussed in
Section 2. Numerical discussions and simulations are used to validate the theory in
Section 3. The article concludes with key points as a conclusion in
Section 4.
3. Numerical Results and Discussion
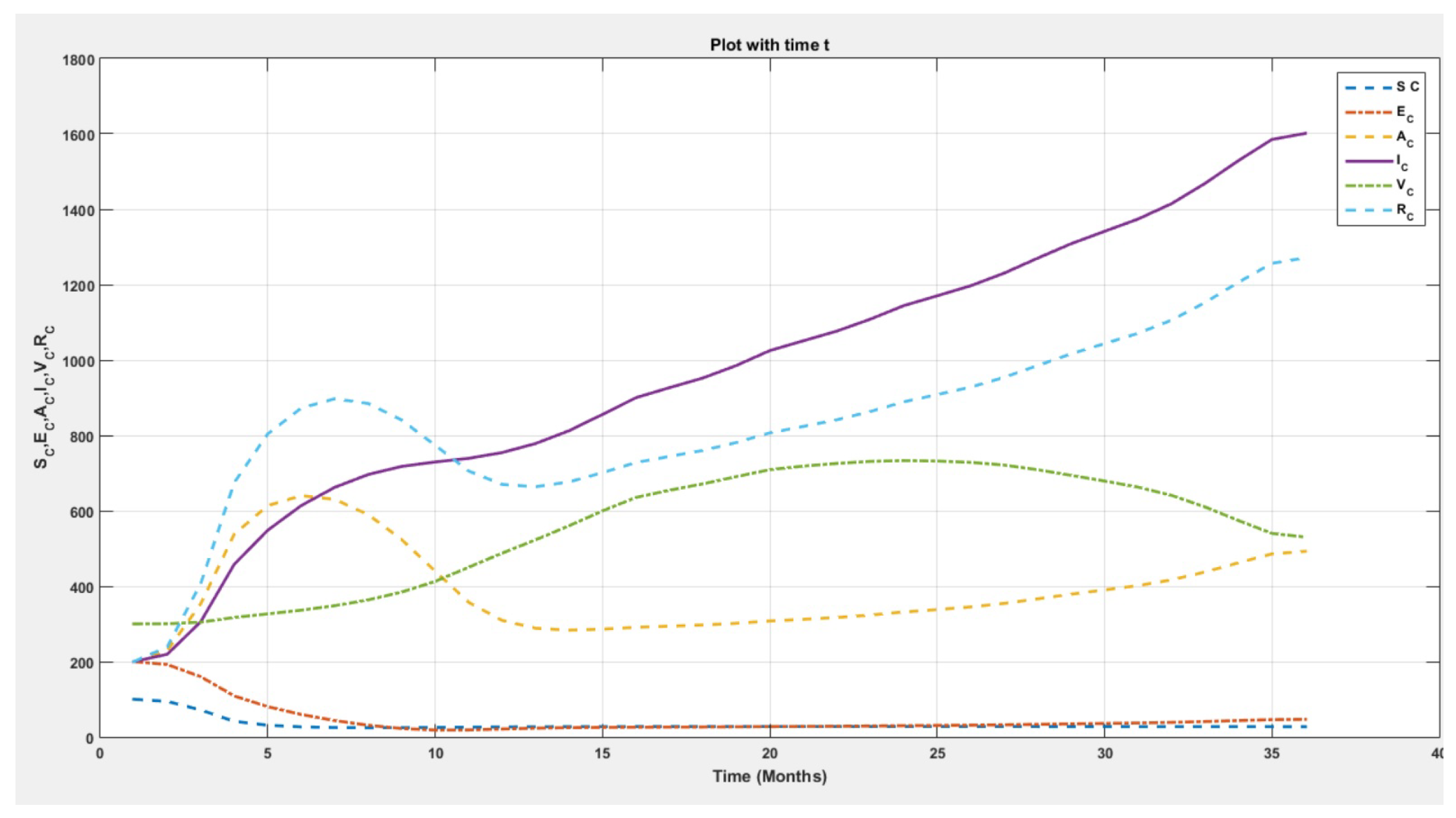
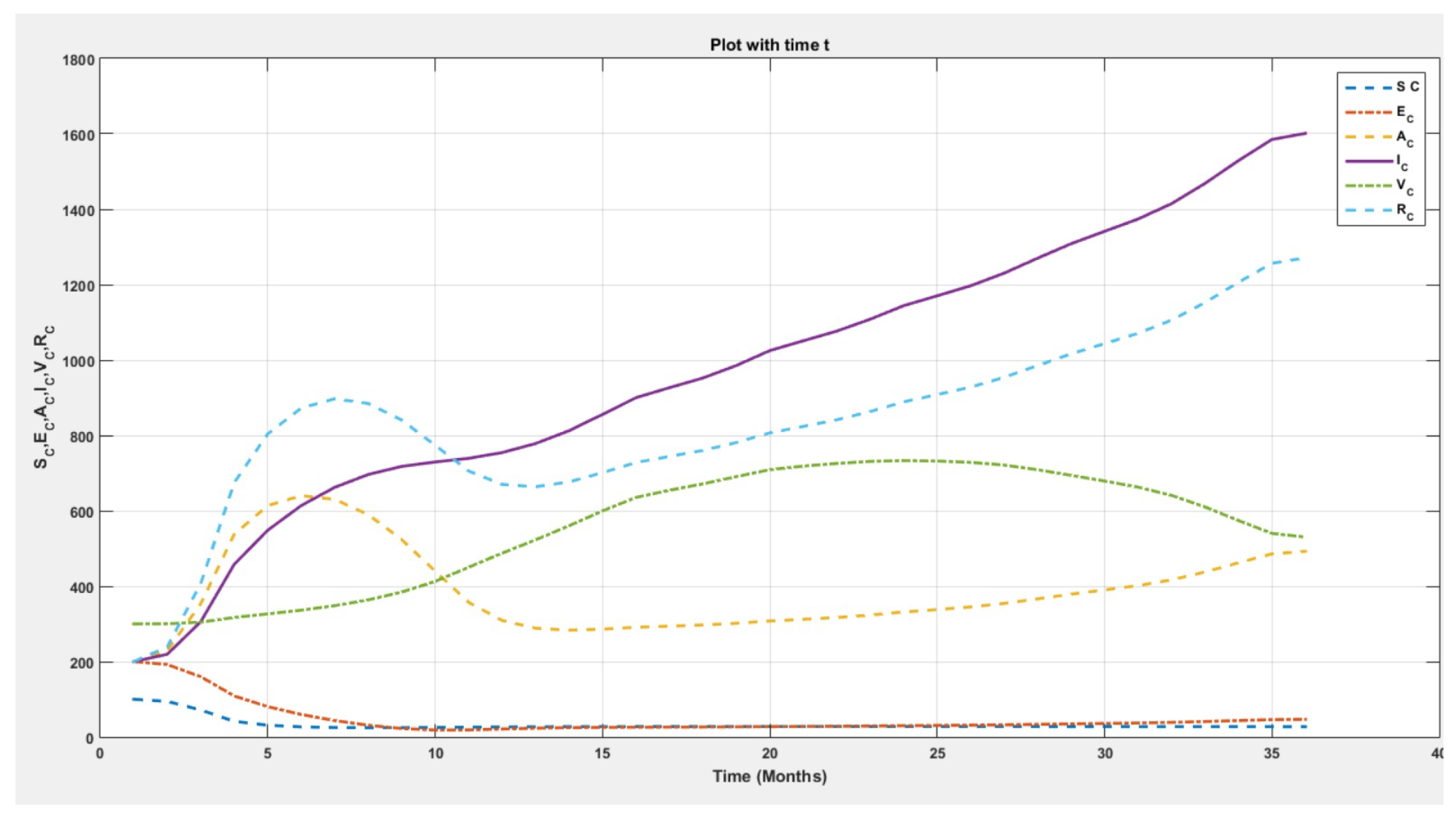
Dynamics of the system are depicted in
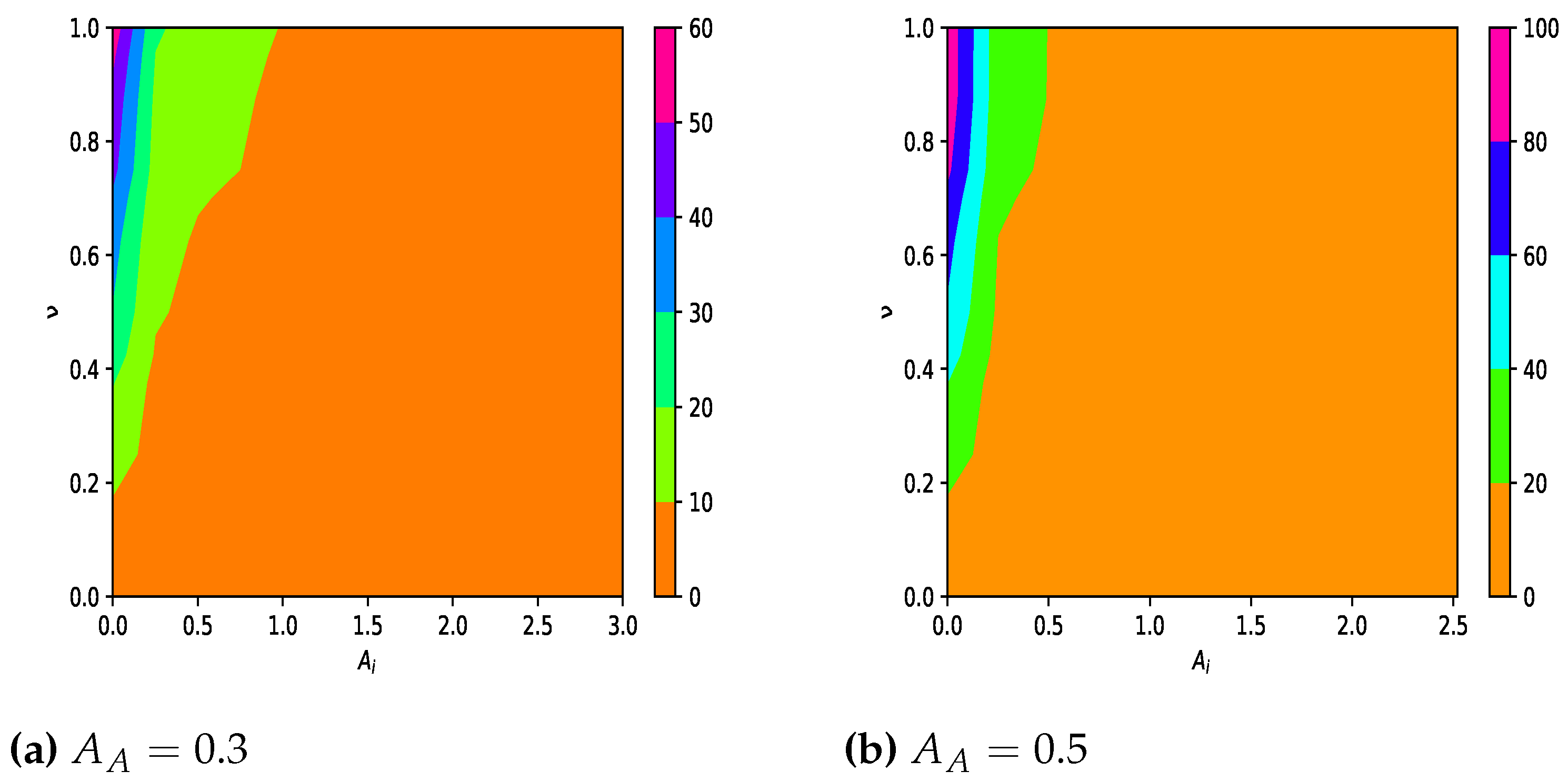
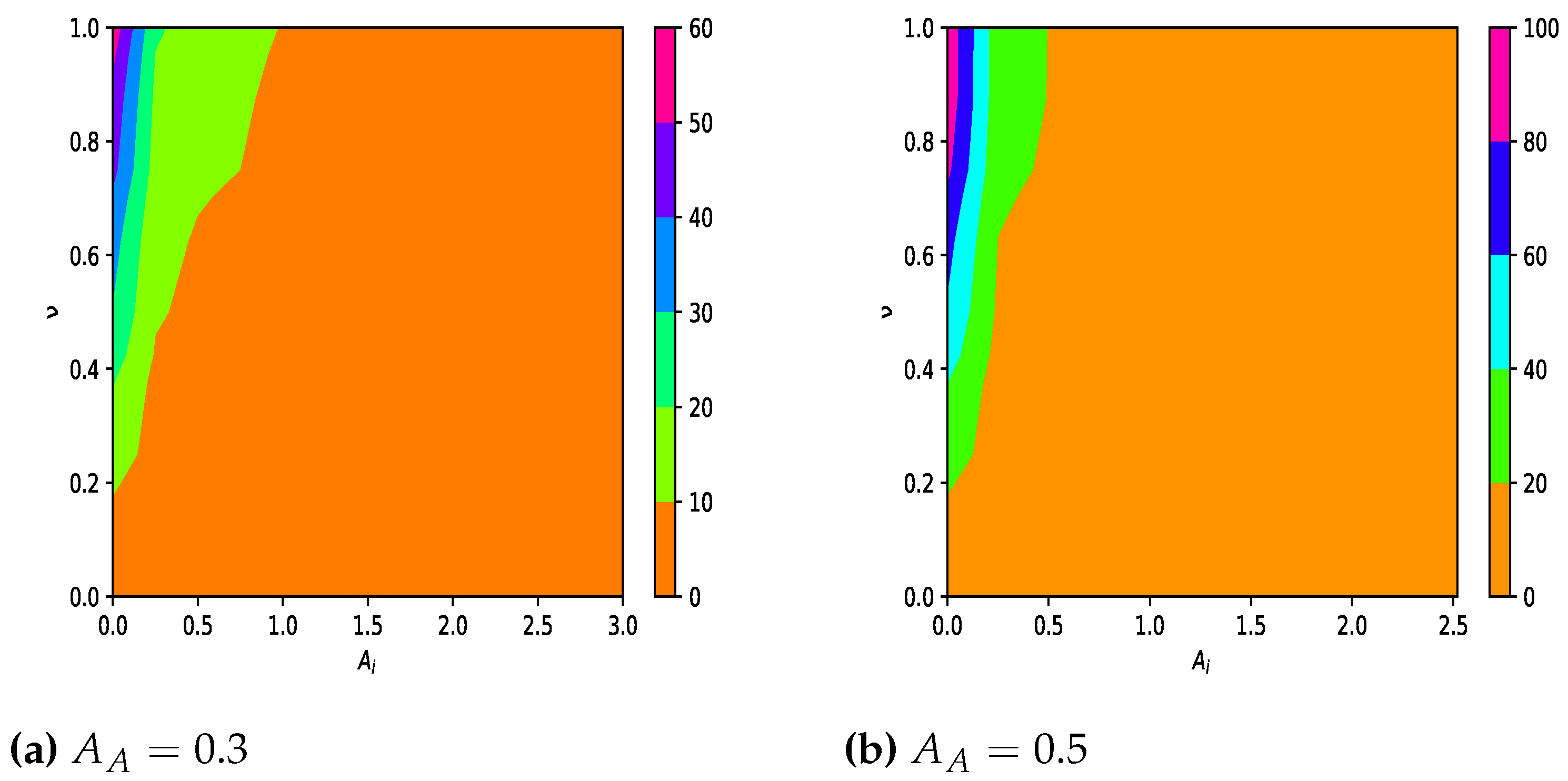
Figure 1. It shows the steady state behaviour of all the class of populations over the period of time. The contour plots in
Figure 2 of reproduction number show that
lies between 0 and 20, as the maximum region of the graph is under that shade. Relationship of
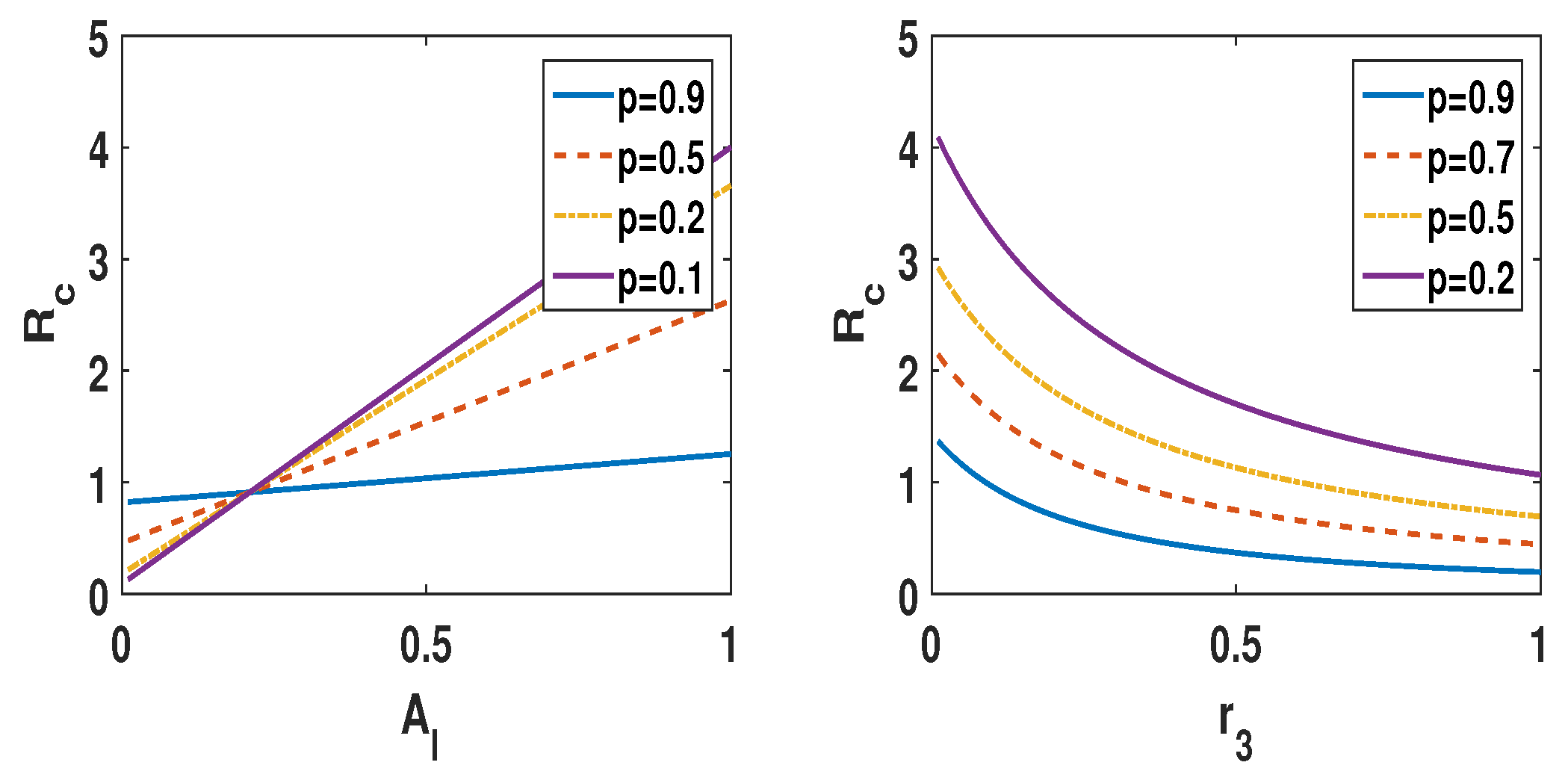
is depicted in
Figure 3 for different values of p. In order to study the effect of the efficacy of vaccine (
) and the percentage of population being vaccinated on the spread of the COVID-19 epidemic/pandemic, a regular network with size
was generated by using the Runge–Kutta method. The effect of efficacy of the vaccination developed for pandemic is simulated in this work. The effect of vaccinated population is also simulated in this study. Overall, the process of spreading the pandemic is simulated in the paper. The impact of vaccination in the spread of the pandemic is shown and demonstrated through simulation with various percentages of efficacy of vaccine and percentage of population vaccinated in a closed region. Initially, the parameters are set as
,
,
, and
.
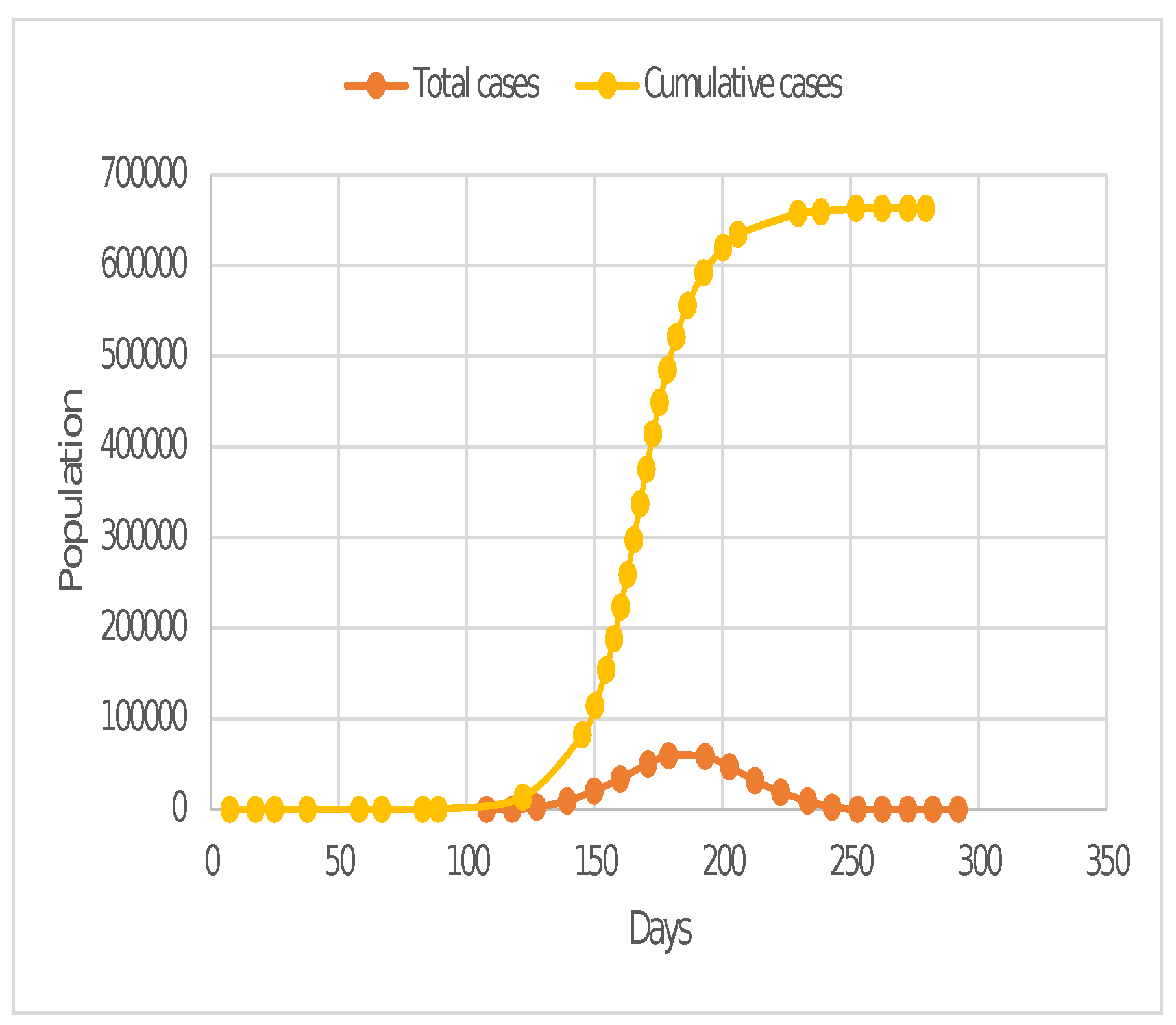
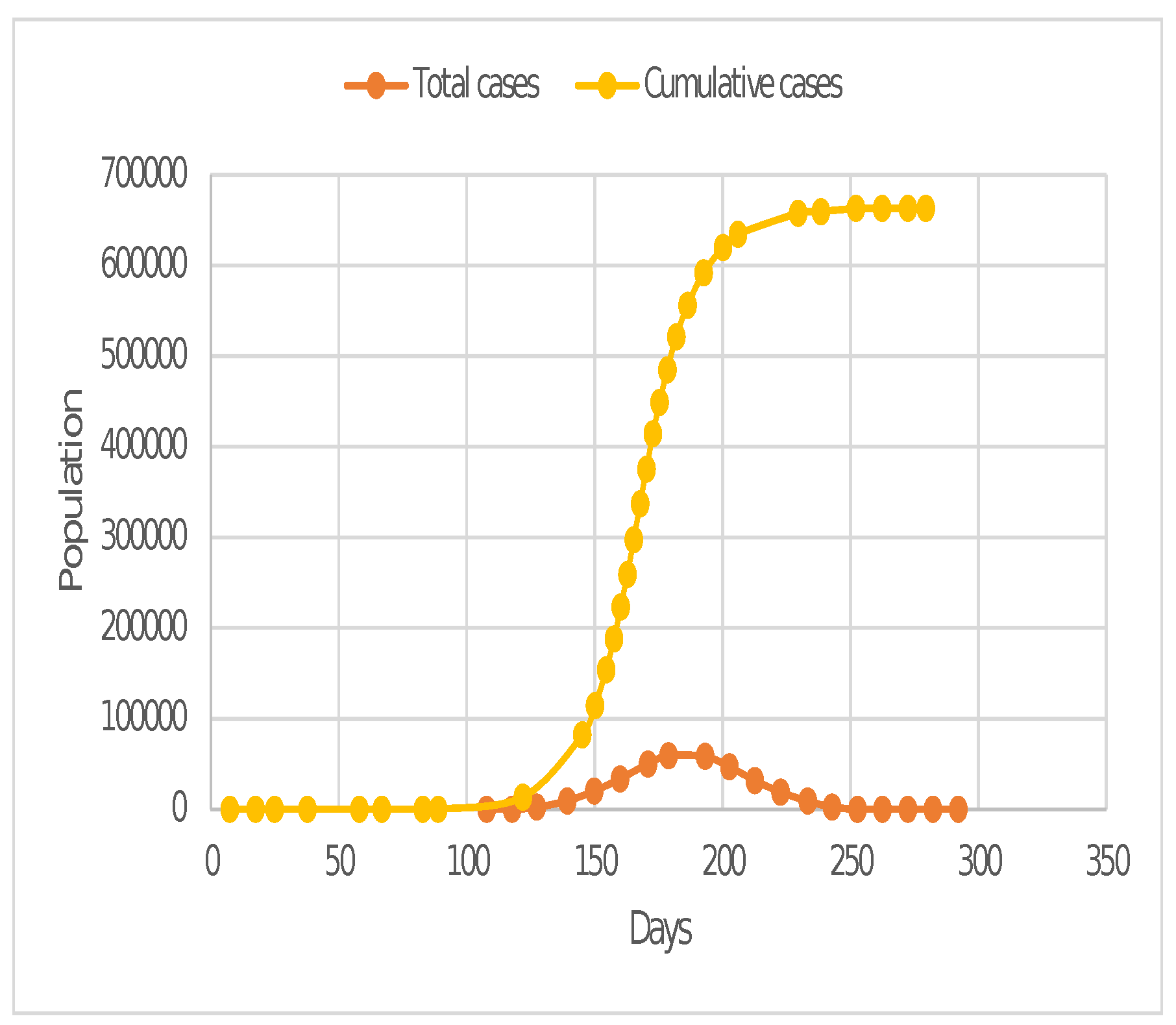
Case I. The transmission rate is () = 0.5, the rate of infected people is () = 0.25, the efficacy of vaccine is () = 0, and the percentage of initially vaccinated population is .
In this case, when there is initially no vaccinated population, this could be considered as the case when the vaccination is not being used for countering any pandemic/COVID-19. As shown in
Figure 4, epidemics with large
reach their peak quickly, with the total number of cases reaching a maximum of 640,000.
Figure 4 shows that the total number of cases reached a maximum of 80,000. (approx.). The pandemic starts to rise rapidly after 100 days.
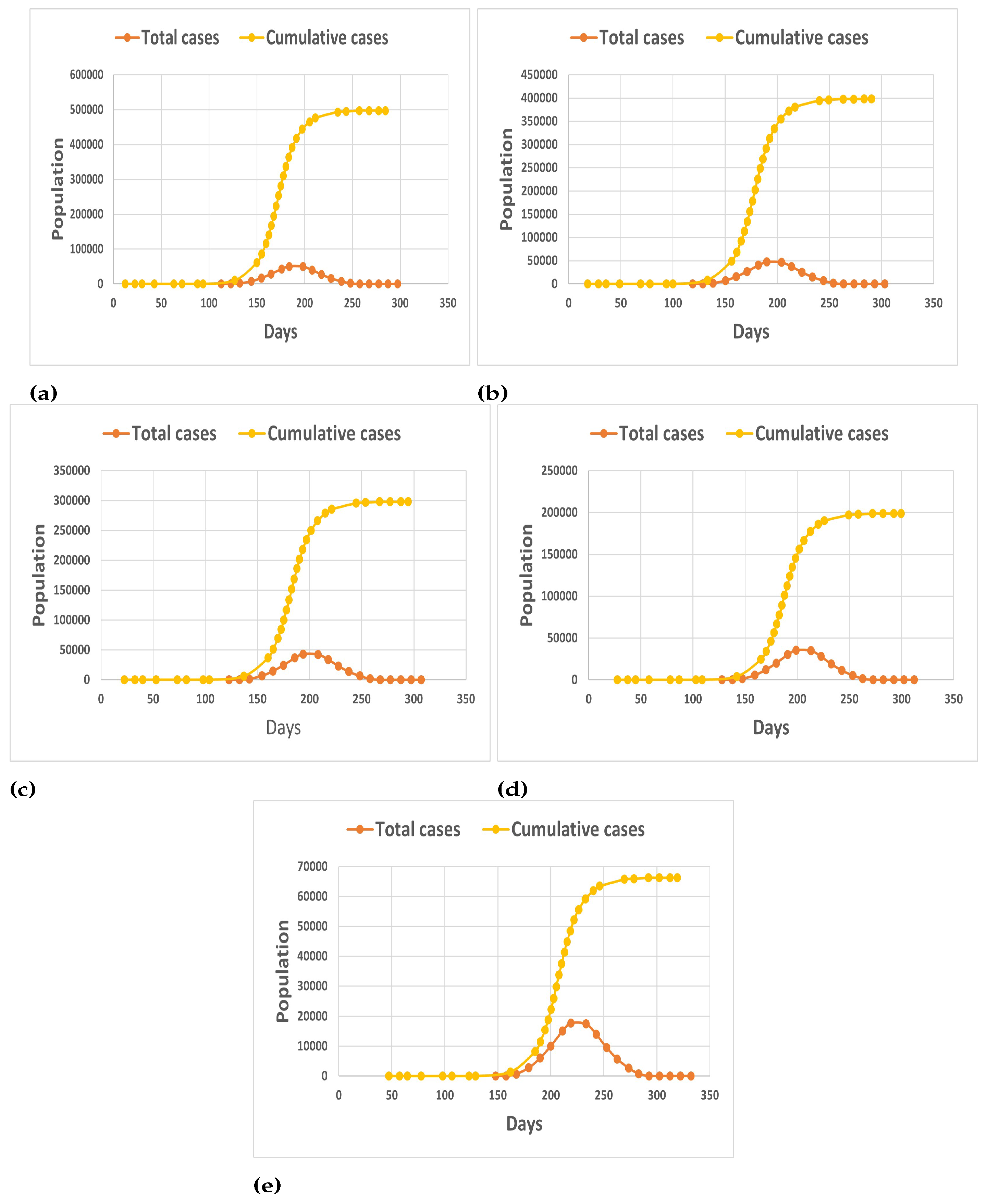
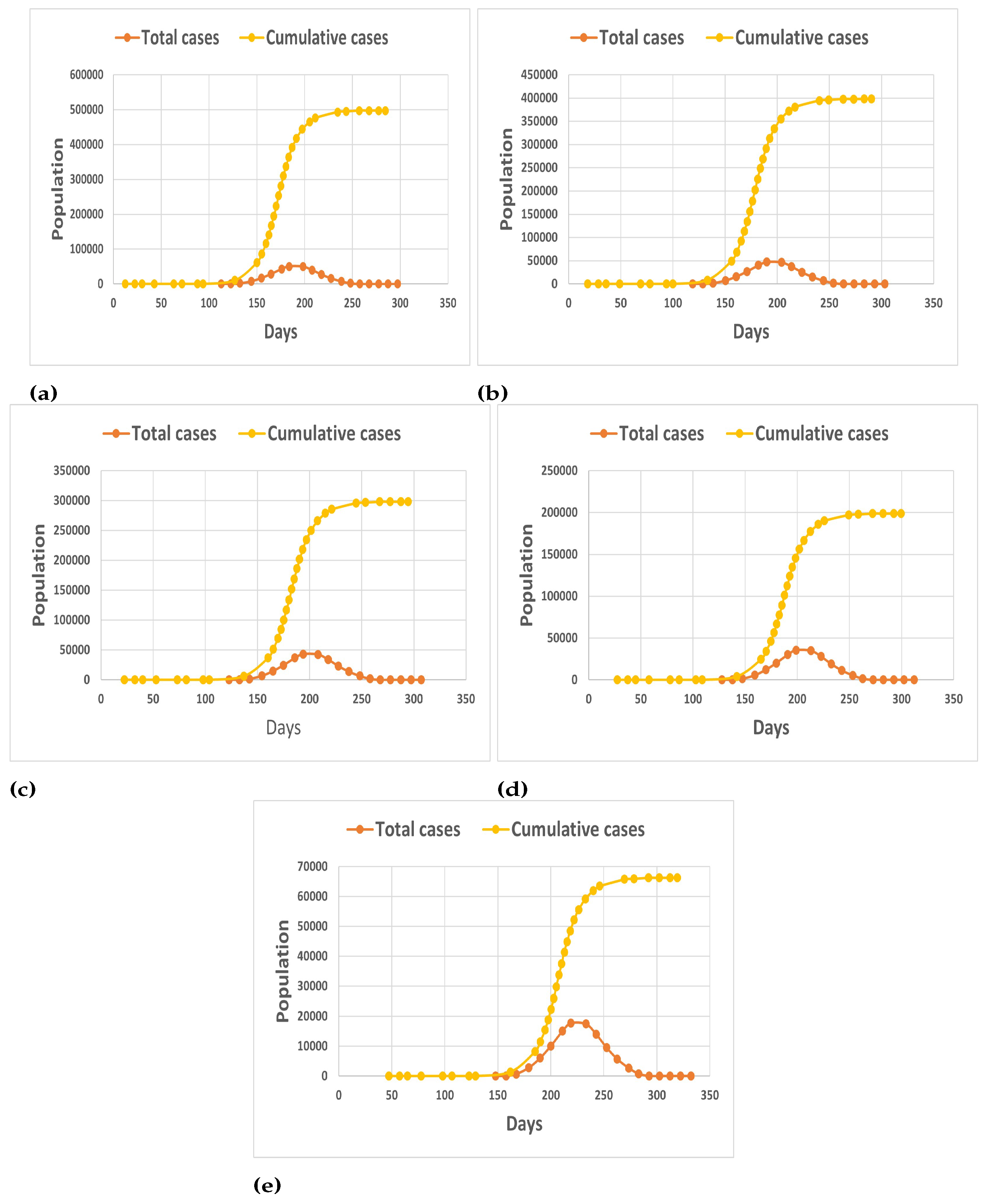
Case II. The transmission rate is () = 0.5, the rate of infected people is () = 0.25, the efficacy of vaccine is () = 0.6, and the percentage of initially vaccinated population is .
This represents the case, when 0 percent of the population is initially vaccinated and the efficacy of the vaccination considered to be 60 percent. It is observed from
Figure 5a that there is a slight delay of approximately 5 days in the rise of pandemic, there is a reduction of approximately 25 percent in the cumulative number of cases, and reduction of 15 percent in the total number of current cases.
Case III. The transmission rate is () = 0.5, the rate of infected people is () = 0.25, the efficacy of vaccine is () = 0.6, and the percentage of initially vaccinated population is .
In this case, the population that is initially vaccinated is considered to be about 30 percent of the total population and the efficacy of the vaccination used is 60 percent.
Figure 5b shows that, compared to
Figure 5a of case two, the delay in the onset of the pandemic has increased to 11 days from 5 days. In addition, compared to case one, when the vaccination is not used, the number of cumulative cases is reduced by 40 percent and the total number of cases is reduced by 20 percent.
Case IV. The transmission rate is () = 0.5, the rate of infected people is () = 0.25, the efficacy of vaccine is () = 0.6, and the percentage of initially vaccinated population is .
In this case, when the initially vaccinated population has reached around 50 percent of the total population, it means that 50 percent of the population has been vaccinated before any pandemic/ensuing wave of COVID-19 exists in the closed state/territory. In this case, it is observed through
Figure 5c that there is a delay of about 15 days in the rapid rise of pandemic cases as compared to Case I, where 0 percent of the population is vaccinated. Additionally, compared to Case I, where the maximum cumulative cases reached around 640,000 and the total number of cases reached a maximum peak of around 50,000 cases on the 200th day of the pandemic, the maximum cumulative cases reached around 300,000 cases. This clearly indicates that if even half of the population is fully vaccinated before the start of any upcoming pandemic wave, there may be a significant reduction of around or greater than 50 percent of cases, compared to when there is no vaccination.
Case V. The transmission rate is () = 0.5, the rate of infected people is () = 0.25, the efficacy of vaccine is () = 0.6, and the percentage of initially vaccinated population is .
This is the case when the initially vaccinated population before the pandemic is approximately 80 percent of the total population of the closed state/area. In comparison to Case I, there is a reduction of about 70 percent in cumulative cases and around 40 percent of total cases, as shown in
Figure 5d. It is also observed that, in comparison to Case I, the rapid rise of the pandemic/COVID-19 is approximately shifted by 20 days.
Case VI. The transmission rate is () = 0.5, the rate of infected people is () = 0.25, the efficacy of vaccine is () = 0.6, and the percentage of initially vaccinated population is .
Now, we consider an ideal case when the complete population of the closed state is vaccinated before the uprising of the further wave of pandemic, and the efficacy of the vaccination is 60 percent. It could be seen from
Figure 5e that there is a huge reduction in the number of cumulative and total infected cases as compared to Case I. It can be seen that cumulative cases have decreased by around 90 percent, demonstrating the importance of vaccination in the eradication of certain diseases.
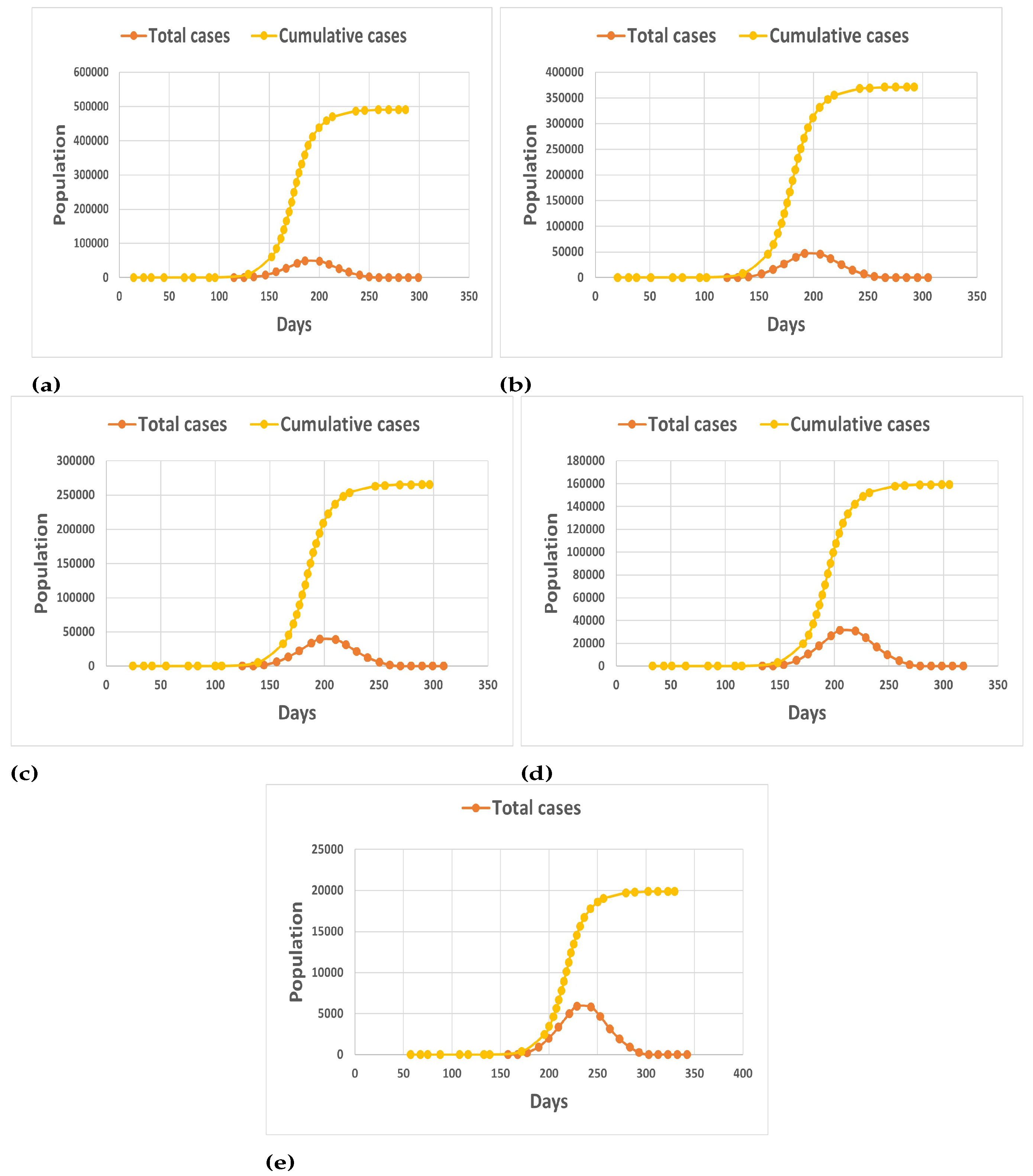
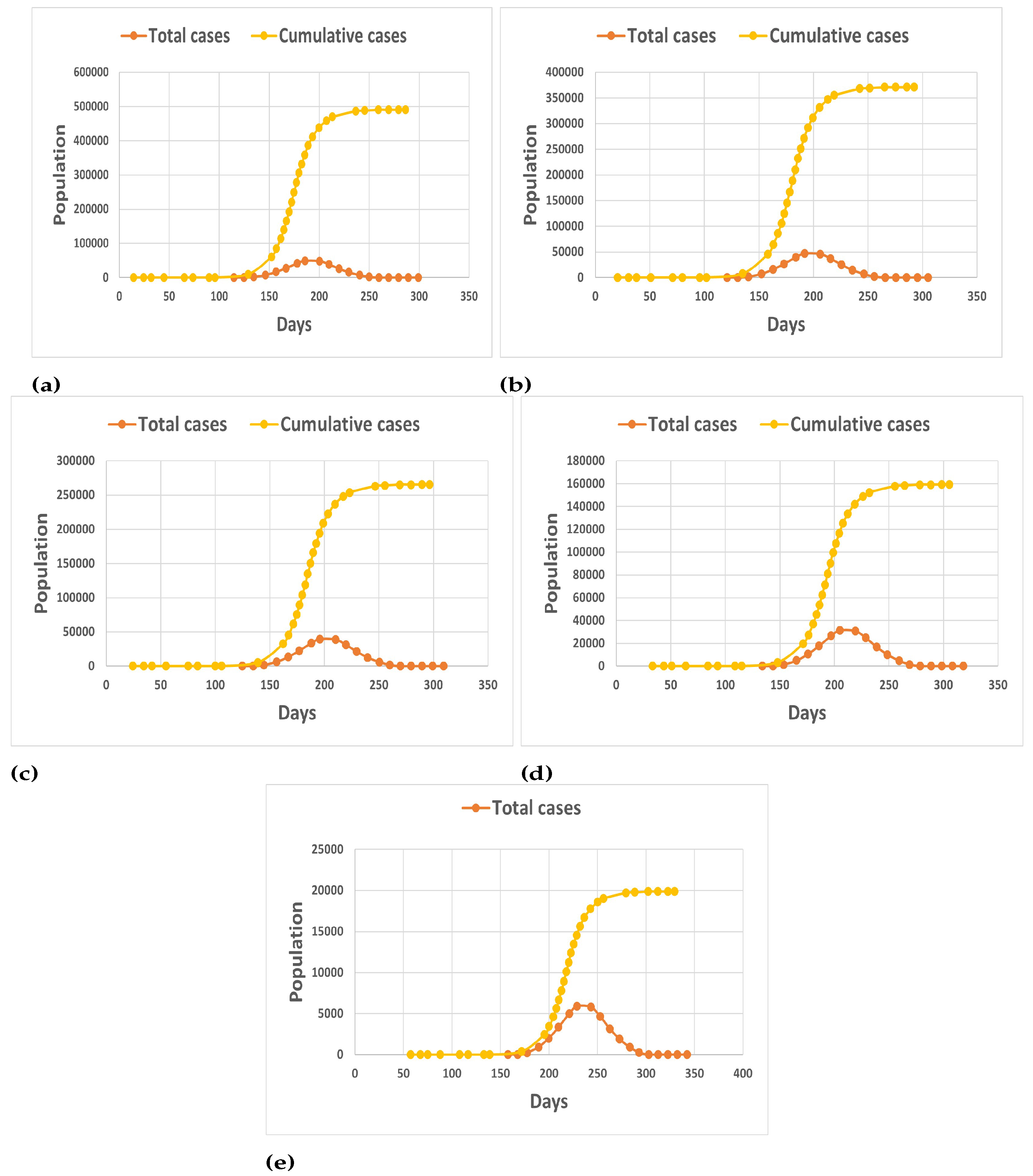
Case VII. The transmission rate is () = 0.5, the rate of infected people is () = 0.25, the efficacy of vaccine is () = 0.7, and the percentage of initially vaccinated population is .
In a new scenario, a case is being considered in which vaccine effectiveness has improved from 60 percent to 70 percent and the population that was initially vaccinated is zero.
Figure 6a shows that there is a small variation from Case II, when the efficacy of vaccine was 60 percent. The reduction in the cumulative cases, as compared to Case I, is around 26 percent, the total cases is around 18 percent, and there is a delay of 7 days in the fast rising of the pandemic wave.
Case VIII. The transmission rate is () = 0.5, the rate of infected people is () = 0.25, the efficacy of vaccine is () = 0.7, and the percentage of initially vaccinated population is .
In this case, the effect of the previously vaccinated population and the vaccine’s efficacy have been clearly visible and depicted in
Figure 6b. Since the pandemic’s initial rapid rise is shifted 13 days ahead, there is a reduction of around 44 percent in the number of cumulative cases and 21 percent in total cases when compared to Case I. In comparison to Case III, where the initial vaccination population is around 30 percent and vaccination efficacy is 60 percent, it is clear that a modest increase of vaccine effectiveness of about 10 percent (from 60 percent to 70 percent) results in a (cumulative) case reduction of approximately 25,000. It shows that increasing vaccine effectiveness while also increasing the number of people who have been vaccinated has a positive impact on epidemic control.
Case IX. The transmission rate is () = 0.5, the rate of infected people is () = 0.25, the efficacy of vaccine is () = 0.7, and the percentage of initially vaccinated population is .
Figure 6c shows that, when the initially vaccinated population is covered up to the total population of the closed state, the cumulative cases are reduced by around 60 percent, as compared to around 55 percent in Case IV. In addition, compared to Case IV, the pandemic rise is delayed by two days, demonstrating the importance of vaccine efficacy in pandemic coverage.
Case X. The transmission rate is () = 0.5, the rate of infected people is () = 0.25, the efficacy of vaccine is () = 0.7, and the percentage of initially vaccinated population is .
In comparison to Case I, a very good result is obtained, indicating the significant effect of vaccination and the importance of vaccination during pandemics for human survival.
Figure 6d shows a 76 percent reduction in cumulative cases and a 26-day delay in the rapid spread of the pandemic when compared to Case I. In comparison to Case V, when the vaccine’s efficacy was 60 percent and all other factors remained the same, the vaccine’s efficacy has improved dramatically, resulting in a massive reduction of around 40,000 cases.
Case XI. The transmission rate is () = 0.5, the rate of infected people is () = 0.25, the efficacy of vaccine is () = 0.7, and the percentage of initially vaccinated population is .
Figure 6e shows that, if 100 percent of the population is vaccinated, there is a 97 percent reduction in cumulative cases compared to Case I. The maximum cumulative case reaches 20,000. In comparison to Case I, there is a 50-day delay in the rapid spread of pandemic. It is evident that having a highly vaccinated population can become a major factor in controlling and declining a pandemic wave.
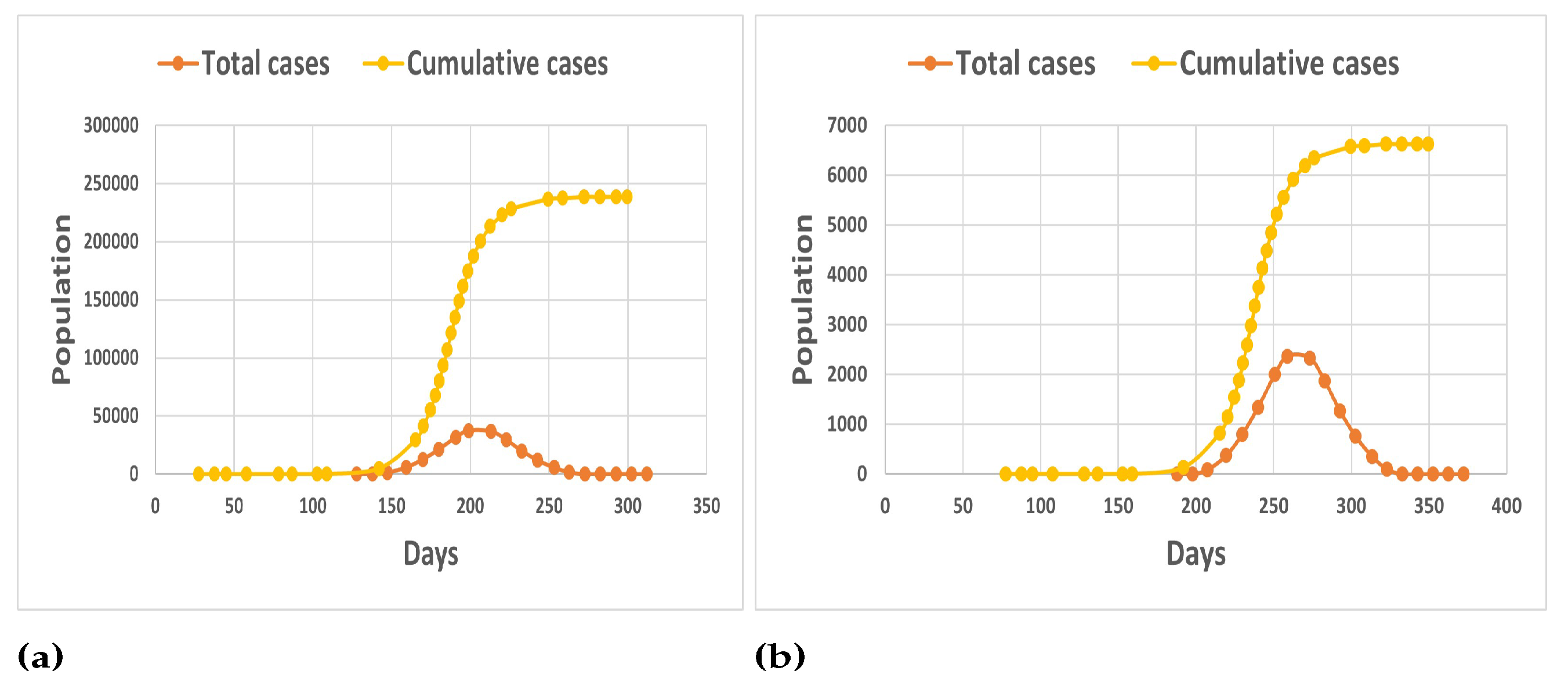
Case XII. The transmission rate is () = 0.5, the rate of infected people is () = 0.25, the efficacy of vaccine is () = 0.8, and the percentage of initially vaccinated population .
In this case, it is considered that 50 percent of total population is being vaccinated and the efficacy of vaccination has reached up to 80 percent. We can conclude, from
Figure 7a, that a reduction of around 65 percent in cumulative cases is obtained as compared to Case I. In addition, in comparison to Case IV, where vaccine efficacy is 60 percent while all other factors remain constant, cumulative cases show a reduction of around 10 percent, indicating the effect of vaccine efficacy on pandemic control.
Case XIII. The transmission rate is () = 0.5, the rate of infected people is () = 0.25, the efficacy of vaccine is () = 0.8, and the percentage of initially vaccinated population is .
Figure 7b shows that, in this ideal special case, where the entire population is vaccinated and the vaccine efficacy is around 80 percent, the maximum pandemic (cumulative, Case I) is reduced by 99 percent and the pandemic rise is delayed by more than 2 months.The maximum number of cumulative cases has fallen below 7000, indicating the critical importance of vaccination for human survival, as compared to Case VI and Case XI, where the efficacy of vaccine is 60 and 70 percent, respectively. It can be seen that the maximum cumulative cases for both cases are around 70,000 and 20,000, respectively. With 100 percent of population vaccinated, the importance of quality of vaccination also matters.
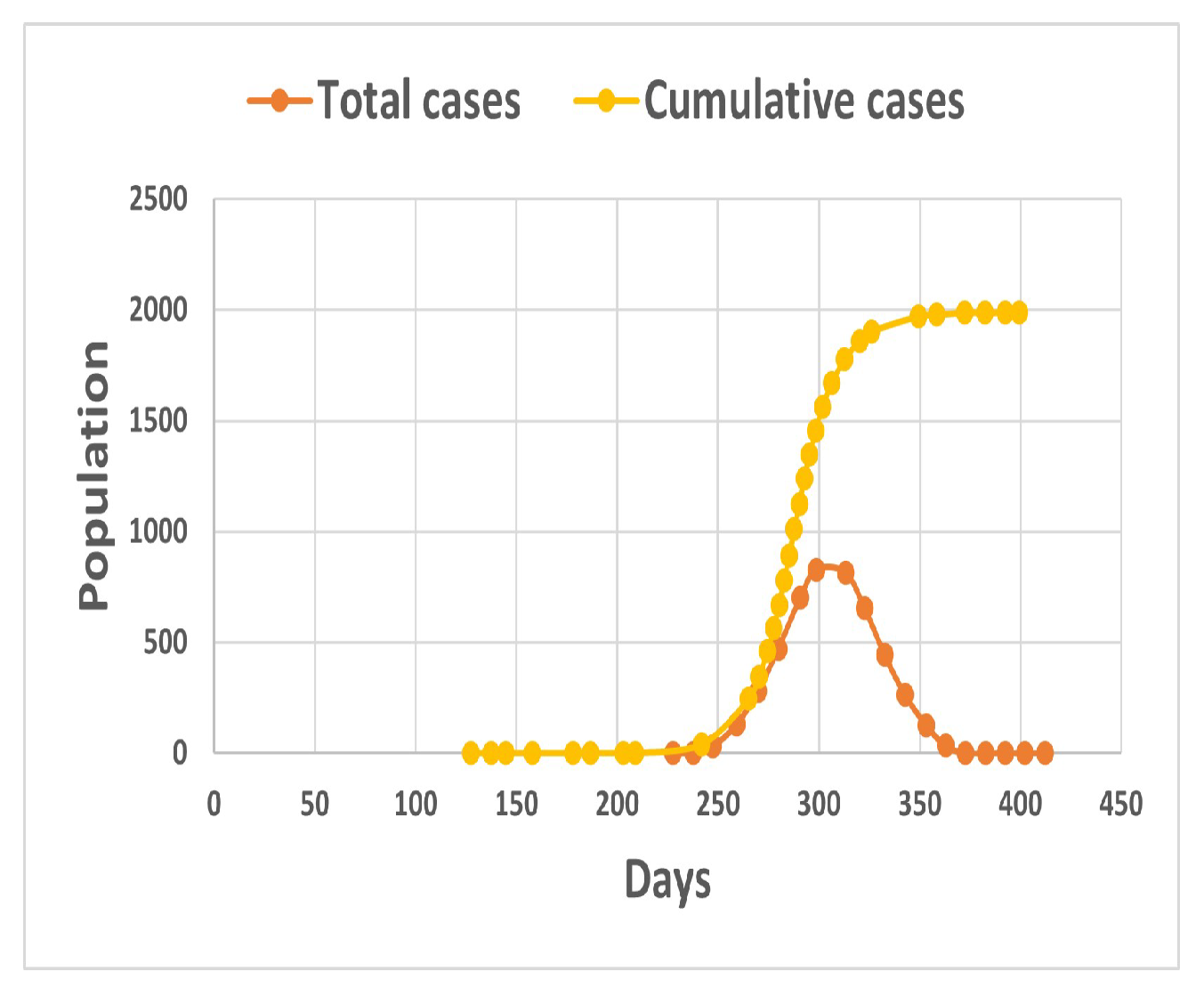
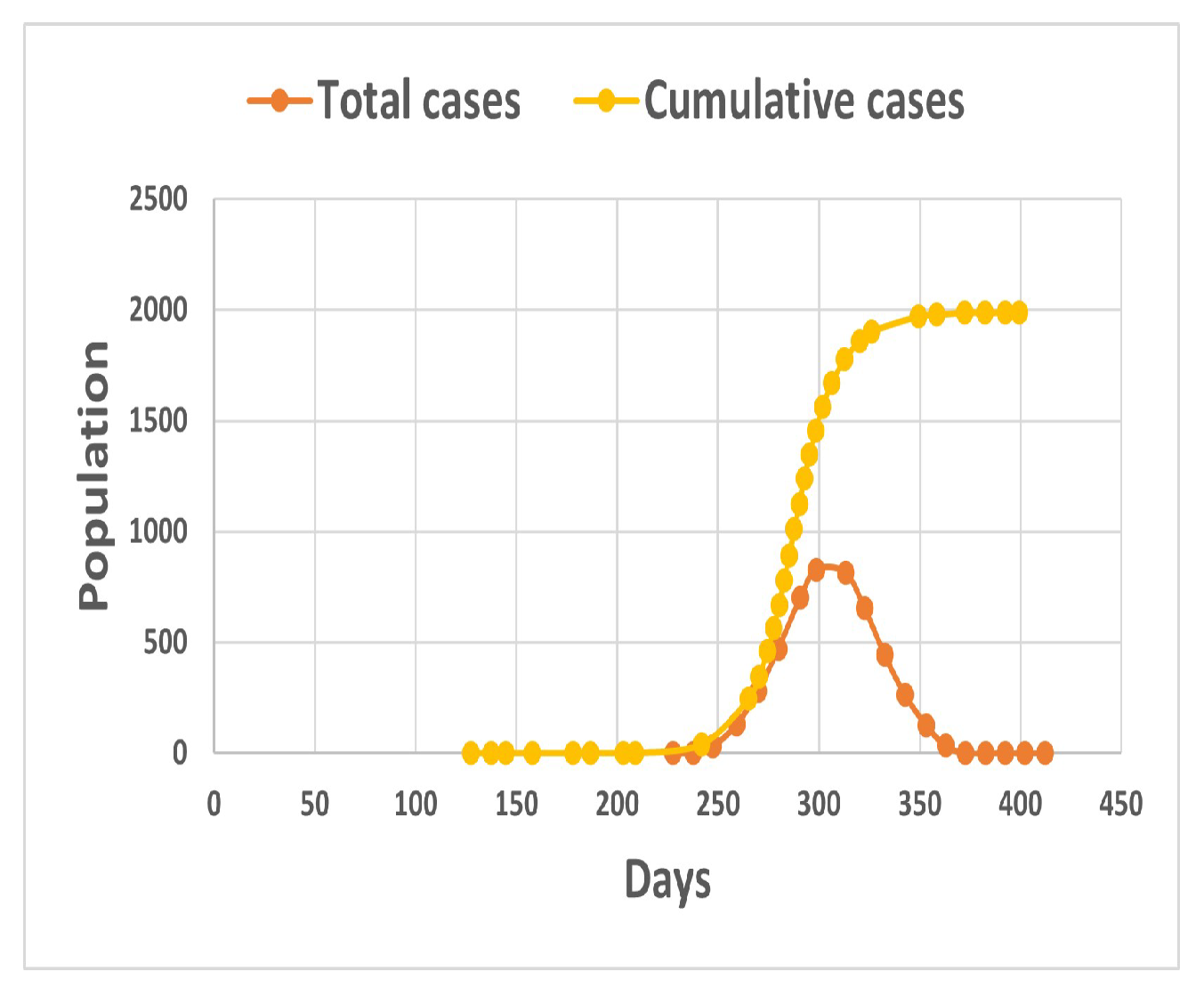
Case XIV. The transmission rate is () = 0.5, the rate of infected people is () = 0.25, the efficacy of vaccine is () = 0.9, and the percentage of initially vaccinated population is .
In this case, when 100 percent of the total closed population is vaccinated with a vaccination with 90 percent efficacy,
Figure 8 clearly shows that the maximum number of cumulative cases has reached 2000 cases. A delay of around 4 months in the rise of pandemic wave is obtained, clearly indicating that a vaccine with very good efficacy and percentage of vaccinated population are both important to curb the fatal pandemic waves and save thousands of lives.


 and
and 

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}