
Advances in Local Drug Delivery for Periodontal Treatment: Present Strategies and Future Directions

 ,
,  ,
,  and
and
Abstract
1. Introduction
2. Overview of DDSs in Periodontal Treatment
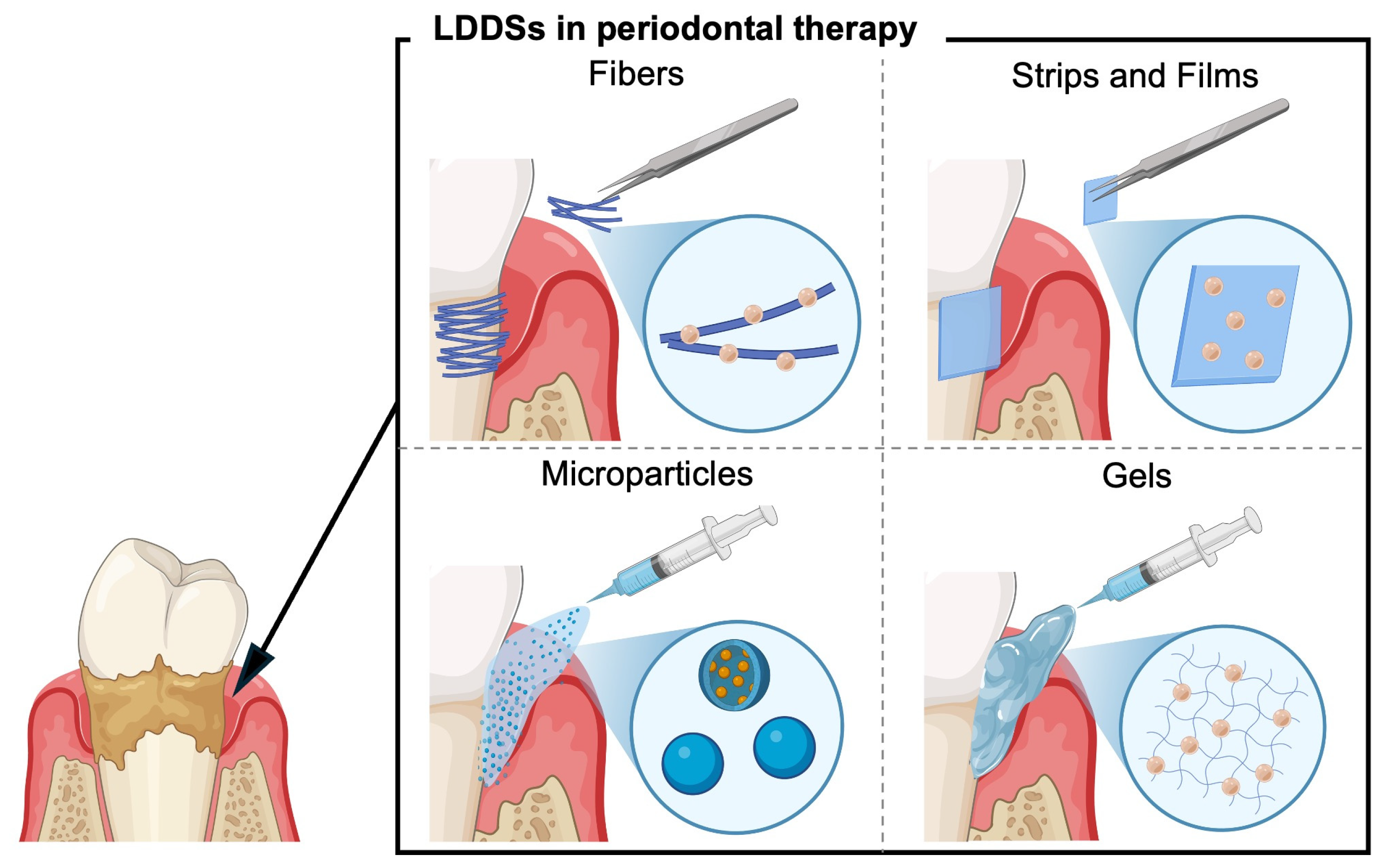
3. Current Status of LDDSs in Periodontal Therapy
3.1. Fibers
3.2. Strips and Films
3.3. Gels
3.4. Microparticles
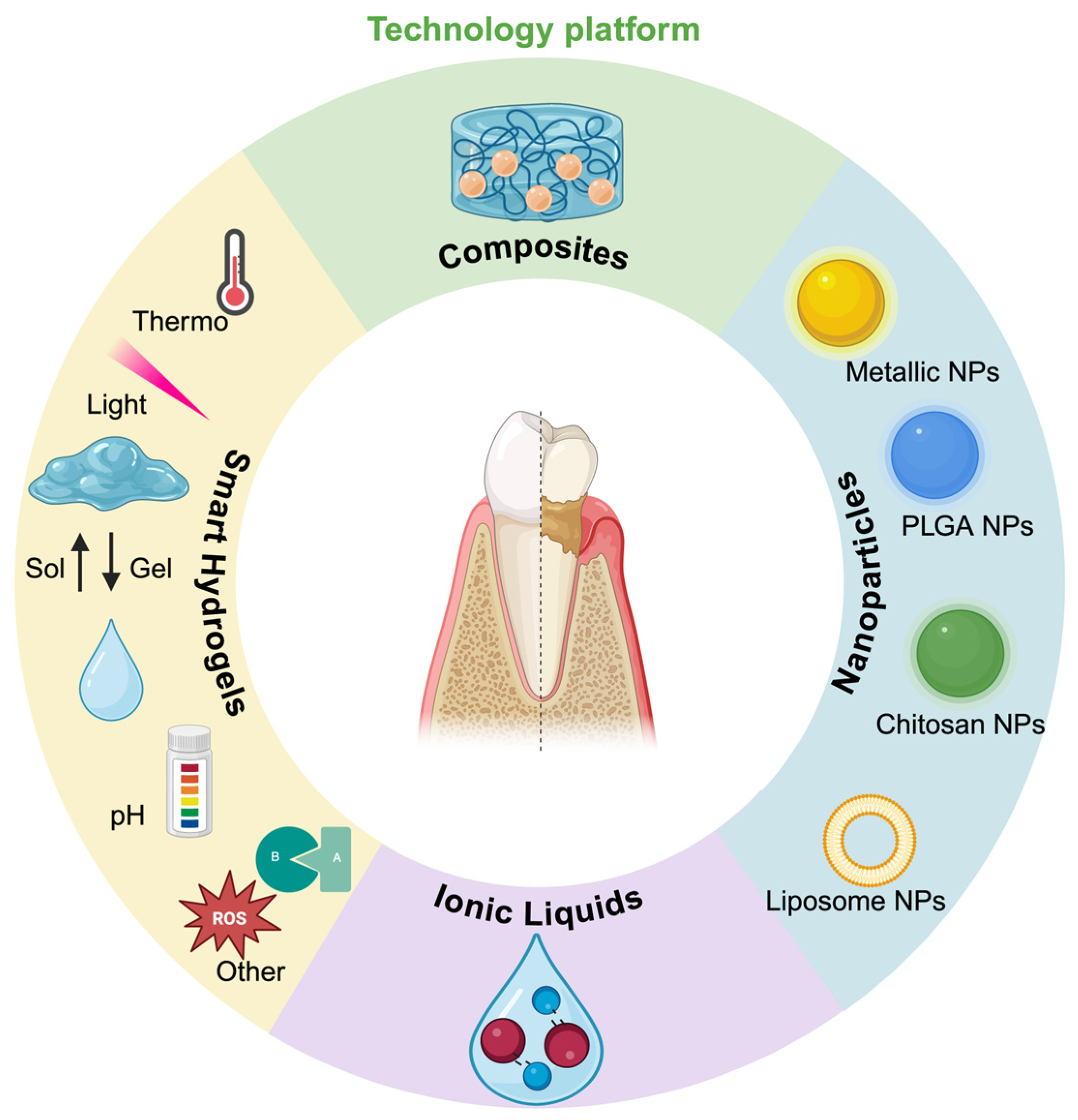
4. Future Perspectives of LDDSs in Periodontal Therapy
4.1. Overview
4.2. Gels
4.2.1. Enhanced Retention Capability
4.2.2. On-Demand Drug Release
4.2.3. Limitations of Gel-Based LDDSs and Future Directions

{kind=link}
{kind=link}
{kind=link}
| Hydrogel Matrix | Drug Incorporated | Study Design | Characteristic | Refs |
|---|---|---|---|---|
| Thermoresponsive hydrogels | ||||
| Chitosan/sodium ß-glycerophosphate | Minocycline | In vitro + in vivo (rat) |
| [49] |
| Thermo- and pH-responsive hydrogels | ||||
| Carboxymethyl–hexanoyl chitosan sodium ß-glycerophosphate | Naringin (flavonoid) | In vivo (mouse) |
| [47] |
| Chitosan Quaternized chitosan sodium α,ß-glycerophosphate | Ornidazole | In vitro |
| [54] |
| pH-responsive hydrogels | ||||
| Carboxymethyl chitosan Oxidized dextran | Embelin | In vitro + in vivo (rat) |
| [52] |
| Light-responsive hydrogels | ||||
| Gelatin methacrylate Gold nanobipyramids coated with mesoporous silica | Minocycline | In vitro |
| [55] |
| Polyvinyl alcohol Sodium alginate Carbon nanofiber | Icariin (flavonoid) | In vitro + in vivo (rat) |
| [56] |
| Poly(N-isopropyl-acrylamide-co-diethyl-aminoethyl methacrylate) Gold nanocages | Tetracycline | In vitro + in vivo (rat) |
| [53] |
| ROS-responsive hydrogels | ||||
| Phenylboronic acid–functionalized poly(ethylene imine) Oxidized dextran | Doxycycline Metformin | In vitro + in vivo (rat) |
| [57] |
| pH- and ROS-responsive hydrogels | ||||
| Carboxymethyl chitosan Dextran 4-Formylphenylboronic acid | Metal–organic framework of magnesium and gallic acid | In vitro + in vivo (rat) |
| [58] |
| Enzyme-responsive hydrogels | ||||
| Polyethylene glycol–diacrylate MMP-8-sensitive peptide (CGPQG↓IWGQC *) | Minocycline Antibacterial peptide KSL (KKVVFKVKFK) | In vitro |
| [59] |
| Hydrogel Matrix | Drug Incorporated | Study Design | Characteristic | Refs |
|---|---|---|---|---|
| Thermoresponsive hydrogels | ||||
| Poloxamer 407 (Pluronic F127) | Green tea catechin extract | RCT (n = 30) Groups: Control: SRP + placebo gel Test: SRP + green tea catechin gel (once at baseline) Time: baseline and 1 month | Both groups showed improvements. However, the treatment group significantly outperformed the control group in all parameters (GI, PPD, and CAL) | [50] |
| Thermo- and pH-responsive hydrogels | ||||
| Pluronic F127 Carbopol P934 | Curcumin | RCT (n = 20) Groups: Control: SRP Test: SRP + 2% curcumin in situ gel (once weekly for 3 weeks) Time: baseline and 1 month | Significant improvements in PPD and BOP were observed in the test group | [51] |
4.3. Nanoparticles
4.3.1. Metallic NPs
4.3.2. PLGA NPs
4.3.3. Chitosan NPs
4.3.4. Nanoliposomes
4.3.5. NP Composites: Association Between NPs and Scaffolds
4.3.6. Limitations of NP-Based LDDSs and Future Directions
| NPs | Drug Incorporated | Study Design | Characteristic | Refs |
|---|---|---|---|---|
| AgNPs | Ebselen | In vitro + in vivo (rat) |
| [88] |
| AuNPs | Epigallocatechin gallate (photosensitizer) | In vitro + in vivo (rat) |
| [68] |
| PtNPs | - | In vitro |
| [66] |
| ZIF-8 NPs | Cerium ions | In vitro |
| [89] |
| ZIF-8 NPs | Minocycline | In vitro + in vivo (rat) |
| [90] |
| PLGA NPs | Minocycline | In vitro + in vivo (rat) |
| [69] |
| PLGA NPs | Peptide (BAR) | In vitro + in vivo (mouse) |
| [71] |
| PLGA NPs | MB (photosensitizer) | In vitro (human sample) |
| [91] |
| Chitosan-modified PLGA NPs | Paclitaxel | In vitro |
| [78] |
| Nanoliposomes | Minocycline | In vivo (mouse) |
| [79] |
| Chitosan-modified nanoliposomes | Doxycycline | In vitro + in vivo (rat) |
| [80] |
| Composite | ||||
| Polydopamine NPs + chitosan/ß-glycerol phosphate gel | Antimicrobial peptides(Nal-P-113) | In vitro + in vivo (rat) |
| [85] |
| Chitosan NPs + Pluronic F127/hyaluronic acid gel | Opuntia ficus-indica extract | In vitro |
| [86] |
| NPs | Drug Incorporated | Treatment | Clinical Effectiveness | Refs |
|---|---|---|---|---|
| AgNPs | - | RCT (n = 30) Groups: Control: 0.2% CHX mouthwash Test: AgNPs mouthwash Time: baseline and 15 days | The AgNP mouthwash efficiently reduced PI, GI, and CRP levels in the GCF. However, it was not equivalent to the CHX mouthwash | [92] |
| PLGA NPs | Curcumin | RCT (n = 20) Groups: Control: SRP + empty NPs Test: SRP + PLGA/PLA NPs loaded with 50 μg of curcumin (once at baseline) Time: baseline, 3, 7, and 15 days | Both groups showed similar improvements in PPD, CAL, and BOP, with no additional benefit in bacterial elimination observed in the test group compared with the control group | [70] |
| PLGA NPs | 20% doxycycline | RCT (n = 40) Groups: Control: FMUD + placebo NPs Test: FMUD + doxycycline NPs (once at baseline) Time: baseline, 1, 3, and 6 months | In deep pockets, test NPs significantly improved BOP at 3 and 6 months, PPD at 3 months, and CAL at 1 and 3 months. A higher percentage of sites with ≥2 mm PPD reduction and CAL gain was observed in the test group at 3 months | [93] |
| PLGA NPs | Methylene blue (photosensitizer) | RCT (n = 10) Groups: Control: US + SRP Test: US + SRP + aPDT with the NP (once at baseline) Time: baseline, 1 week, 1 month, and 3 months | The test group showed significantly greater improvement in the gingival bleeding index than the control group at 3 months | [74] |
| Chitosan-modified PLGA NPs | Indocyanine green (photosensitizer) | RCT (n = 40) Groups: Control: PDT Test: PDT with the NPs Time: immediately after treatment and at 1 week | No significant differences in PPD and BOP between the groups. However, the bacterial colony counts were significantly lower immediately after treatment in the test group | [94] |
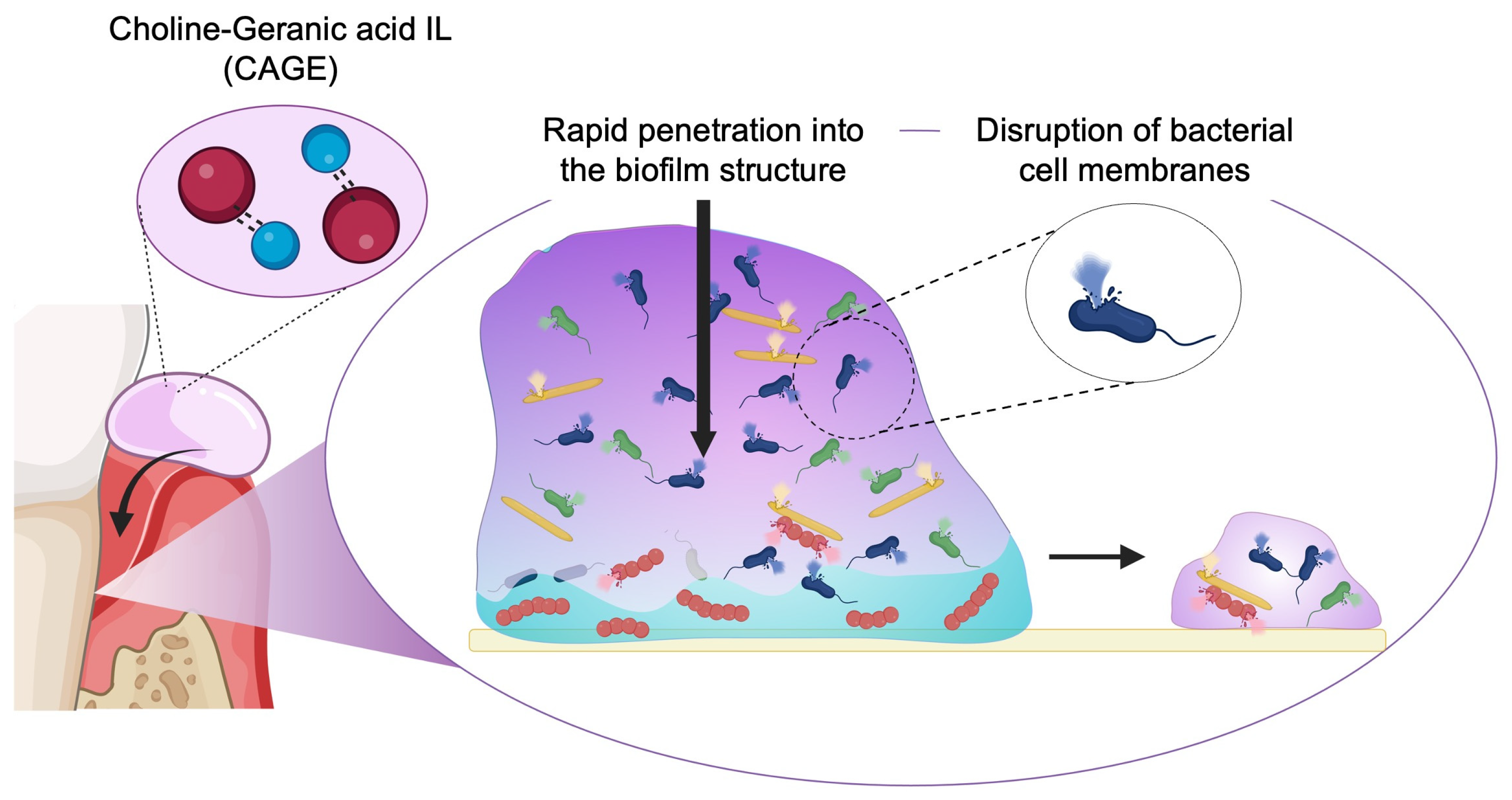
4.4. Ionic Liquids
4.5. LDDSs for Alveolar Bone Regeneration
| LDDSs | Drug incorporated | Study design | Characteristic | Refs |
|---|---|---|---|---|
| Nap-Phe-Phe-Tyr-OH-based hydrogel |
| In vitro + in vivo (rat) |
| [102] |
| Chitosan-modified PLGA NPs + gelatin |
| In vitro + in vivo (dog) |
| [103] |
| Asymmetric membrane Aspirin-PLGA-NP/curcumin + collagen nanofibers |
| In vitro + in vivo (dog) |
| [104] |
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| BOP | Bleeding on probing |
| CAL | Clinical attachment levels |
| DDS | Drug delivery systems |
| GCF | Gingival crevicular fluid |
| GI | Gingival index |
| IL | Ionic liquids |
| LDDS | Local DDSs |
| PDT | Photodynamic therapy |
| PPD | Probing pocket depth |
| SF | Strips and films |
| SRP | Scaling and root planning |
| USFDA | United States Food and Drug Administration |
References
- Ferreira, M.C.; Dias-Pereira, A.C.; Branco-de-Almeida, L.S.; Martins, C.C.; Paiva, S.M. Impact of periodontal disease on quality of life: A systematic review. J. Periodontal Res. 2017, 52, 651–665. [Google Scholar] [CrossRef] [PubMed]
- Nibali, L.; D’Aiuto, F.; Griffiths, G.; Patel, K.; Suvan, J.; Tonetti, M.S. Severe periodontitis is associated with systemic inflammation and a dysmetabolic status: A case-control study. J. Clin. Periodontol. 2007, 34, 931–937. [Google Scholar] [CrossRef] [PubMed]
- Li, X.; Kolltveit, K.M.; Tronstad, L.; Olsen, I. Systemic diseases caused by oral infection. Clin. Microbiol. Rev. 2000, 13, 547–558. [Google Scholar] [CrossRef] [PubMed]
- Kassebaum, N.J.; Smith, A.G.C.; Bernabé, E.; Fleming, T.D.; Reynolds, A.E.; Vos, T.; Murray, C.J.L.; Marcenes, W.; GBD 2015 Oral Health Collaborators. Global, regional, and national prevalence, incidence, and disability-adjusted life years for oral conditions for 195 countries, 1990–2015: A systematic analysis for the Global Burden of diseases, injuries, and risk factors. J Dent. Res. 2017, 96, 380–387. [Google Scholar] [CrossRef]
- Mira, A.; Simon-Soro, A.; Curtis, M.A. Role of microbial communities in the pathogenesis of periodontal diseases and caries. J. Clin. Periodontol. 2017, 44 (Suppl. 18), S23–S38. [Google Scholar] [CrossRef]
- Velsko, I.M.; Shaddox, L.M. Consistent and reproducible long-term in vitro growth of health and disease-associated oral subgingival biofilms. BMC Microbiol. 2018, 18, 70. [Google Scholar] [CrossRef]
- Polizzi, A.; Donzella, M.; Nicolosi, G.; Santonocito, S.; Pesce, P.; Isola, G. Drugs for the Quorum Sensing Inhibition of Oral Biofilm: New Frontiers and Insights in the Treatment of Periodontitis. Pharmaceutics 2022, 14, 2740. [Google Scholar] [CrossRef]
- Addy, M.; Martin, M.V. Systemic antimicrobials in the treatment of chronic periodontal diseases: A dilemma. Oral Dis. 2003, 9 (Suppl. 1), 38–44. [Google Scholar] [CrossRef]
- Karmakar, S.; Shanmugasundaram, S.; Modak, B. Oleogel-based drug delivery for the treatment of periodontitis: Current strategies and future perspectives. F1000Research 2023, 12, 1228. [Google Scholar] [CrossRef]
- Joshi, D.; Garg, T.; Goyal, A.K.; Rath, G. Advanced drug delivery approaches against periodontitis. Drug Deliv. 2016, 23, 363–377. [Google Scholar] [CrossRef]
- Larsson, L.; Decker, A.M.; Nibali, L.; Pilipchuk, S.P.; Berglundh, T.; Giannobile, W.V. Regenerative medicine for periodontal and Peri-implant diseases. J. Dent. Res. 2016, 95, 255–266. [Google Scholar] [CrossRef] [PubMed]
- Wang, D.; Li, Q.; Xiao, C.; Wang, H.; Dong, S. Nanoparticles in periodontitis therapy: A review of the current situation. Int. J. Nanomed. 2024, 19, 6857–6893. [Google Scholar] [CrossRef] [PubMed]
- Kornman, K.S. Controlled-release local delivery antimicrobials in periodontics: Prospects for the future. J. Periodontol. 1993, 64, 782–791. [Google Scholar] [CrossRef] [PubMed]
- Wei, Y.; Deng, Y.; Ma, S.; Ran, M.; Jia, Y.; Meng, J.; Han, F.; Gou, J.; Yin, T.; He, H.; et al. Local drug delivery systems as therapeutic strategies against periodontitis: A systematic review. J. Control. Release 2021, 333, 269–282. [Google Scholar] [CrossRef]
- Jain, N.; Jain, G.K.; Javed, S.; Iqbal, Z.; Talegaonkar, S.; Ahmad, F.J.; Khar, R.K. Recent approaches for the treatment of periodontitis. Drug Discov. Today 2008, 13, 932–943. [Google Scholar] [CrossRef]
- Liu, G.; Gu, Z.; Hong, Y.; Cheng, L.; Li, C. Electrospun starch nanofibers: Recent advances, challenges, and strategies for potential pharmaceutical applications. J. Control. Release 2017, 252, 95–107. [Google Scholar] [CrossRef]
- Han, D.; Steckl, A.J. Triaxial electrospun nanofiber membranes for controlled dual release of functional molecules. ACS Appl. Mater. Interfaces 2013, 5, 8241–8245. [Google Scholar] [CrossRef]
- Litch, J.M.; Encarnacion, M.; Chen, S.; Leonard, J.; Burkoth, T.L. Use of the polymeric matrix as internal standard for quantitation of in vivo delivery of tetracycline HCl from Actisite tetracycline fiber during periodontal treatment. J. Periodontal Res. 1996, 31, 540–544. [Google Scholar] [CrossRef]
- Goodson, J.M.; Haffajee, A.; Socransky, S.S. Periodontal therapy by local delivery of tetracycline. J. Clin. Periodontol 1979, 6, 83–92. [Google Scholar] [CrossRef]
- Luo, D.; Zhang, X.; Shahid, S.; Cattell, M.J.; Gould, D.J.; Sukhorukov, G.B. Electrospun poly(lactic acid) fibers containing novel chlorhexidine particles with sustained antibacterial activity. Biomater. Sci. 2016, 5, 111–119. [Google Scholar] [CrossRef]
- Reise, M.; Wyrwa, R.; Müller, U.; Zylinski, M.; Völpel, A.; Schnabelrauch, M.; Berg, A.; Jandt, K.D.; Watts, D.C.; Sigusch, B.W. Release of metronidazole from electrospun poly(L-lactide-co-D/L-lactide) fibers for local periodontitis treatment. Dent. Mater. 2012, 28, 179–188. [Google Scholar] [CrossRef] [PubMed]
- Sachdeva, S.; Agarwal, V. Evaluation of commercially available biodegradable tetracycline fiber therapy in chronic periodontitis. J. Indian Soc. Periodontol. 2011, 15, 130–134. [Google Scholar] [PubMed]
- Langer, R.; Peppas, N.A. Advances in biomaterials, drug delivery, and bionanotechnology. AIChE J. 2003, 49, 2990–3006. [Google Scholar] [CrossRef]
- Larsen, T. In vitro release of doxycycline from bioabsorbable materials and acrylic strips. J. Periodontol. 1990, 61, 30–34. [Google Scholar] [CrossRef]
- Steinberg, D.; Friedman, M.; Soskolne, A.; Sela, M.N. A new degradable controlled release device for treatment of periodontal disease: In vitro release study. J. Periodontol. 1990, 61, 393–398. [Google Scholar] [CrossRef]
- El-Kamel, A.H.; Ashri, L.Y.; Alsarra, I.A. Micromatricial metronidazole benzoate film as a local mucoadhesive delivery system for treatment of periodontal diseases. AAPS PharmSciTech 2007, 8, E75. [Google Scholar] [CrossRef]
- Schwach-Abdellaoui, K.; Vivien-Castioni, N.; Gurny, R. Local delivery of antimicrobial agents for the treatment of periodontal diseases. Eur. J. Pharm. Biopharm. 2000, 50, 83–99. [Google Scholar] [CrossRef]
- Paolantonio, M.; D’Angelo, M.; Grassi, R.F.; Perinetti, G.; Piccolomini, R.; Pizzo, G.; Annunziata, M.; D’ARchivio, D.; D’ERcole, S.; Nardi, G.; et al. Clinical and microbiologic effects of subgingival controlled-release delivery of chlorhexidine chip in the treatment of periodontitis: A multicenter study. J. Periodontol 2008, 79, 271–282. [Google Scholar] [CrossRef]
- Qin, Y.; Yuan, M.; Li, L.; Li, W.; Xue, J. Formulation and evaluation of in situ forming PLA implant containing tinidazole for the treatment of periodontitis. J. Biomed. Mater. Res. B Appl. Biomater. 2012, 100, 2197–2202. [Google Scholar] [CrossRef]
- Griffiths, G.S.; Smart, G.J.; Bulman, J.S.; Weiss, G.; Shrowder, J.; Newman, H.N. Comparison of clinical outcomes following treatment of chronic adult periodontitis with subgingival scaling or subgingival scaling plus metronidazole gel. J. Clin. Periodontol 2000, 27, 910–917. [Google Scholar] [CrossRef]
- Davidovich-Pinhas, M. Oleogels: A promising tool for delivery of hydrophobic bioactive molecules. Ther. Deliv. 2016, 7, 1–3. [Google Scholar] [CrossRef] [PubMed]
- Paolantonio, M.; D’Ercole, S.; Pilloni, A.; D’Archivio, D.; Lisanti, L.; Graziani, F.; Femminella, B.; Sammartino, G.; Perillo, L.; Tetè, S.; et al. Clinical, microbiologic, and biochemical effects of subgingival administration of a Xanthan-based chlorhexidine gel in the treatment of periodontitis: A randomized multicenter trial. J. Periodontol 2009, 80, 1479–1492. [Google Scholar] [CrossRef] [PubMed]
- Jain, M.; Dave, D.; Jain, P.; Manohar, B.; Yadav, B.; Shetty, N. Efficacy of xanthan based chlorhexidine gel as an adjunct to scaling and root planing in treatment of the chronic periodontitis. J. Indian Soc. Periodontol. 2013, 17, 439–443. [Google Scholar] [CrossRef] [PubMed]
- Rebaka, V.P.; Rachamalla, A.K.; Batra, S.; Subbiah, N. State of the art and new perspectives in oleogels and applications. In Sustainable Green Chemical Processes and their Allied Applications; Nanotechnology in the Life Sciences; Springer International Publishing: Cham, Switzerland, 2020; pp. 151–182. [Google Scholar]
- Vlachopoulos, A.; Karlioti, G.; Balla, E.; Daniilidis, V.; Kalamas, T.; Stefanidou, M.; Bikiaris, N.D.; Christodoulou, E.; Koumentakou, I.; Karavas, E.; et al. Poly(lactic acid)-based microparticles for drug delivery applications: An overview of recent advances. Pharmaceutics 2022, 14, 359. [Google Scholar] [CrossRef]
- Pagels, R.F.; Prud’homme, R.K. Polymeric nanoparticles and microparticles for the delivery of peptides, biologics, and soluble therapeutics. J. Control. Release 2015, 219, 519–535. [Google Scholar] [CrossRef]
- Iqbal, M.; Zafar, N.; Fessi, H.; Elaissari, A. Double emulsion solvent evaporation techniques used for drug encapsulation. Int. J. Pharm. 2015, 496, 173–190. [Google Scholar] [CrossRef]
- Persson, G.R.; Salvi, G.E.; Heitz-Mayfield, L.J.A.; Lang, N.P. Antimicrobial therapy using a local drug delivery system (Arestin) in the treatment of peri-implantitis. I: Microbiological outcomes. Clin. Oral Implants Res. 2006, 17, 386–393. [Google Scholar] [CrossRef]
- Gopinath, V.; Ramakrishnan, T.; Emmadi, P.; Ambalavanan, N.; Mammen, B.; Vijayalakshmi. Effect of a controlled release device containing minocycline microspheres on the treatment of chronic periodontitis: A comparative study. J. Indian Soc. Periodontol. 2009, 13, 79–84. [Google Scholar] [CrossRef]
- Paquette, D.; Oringer, R.; Lessem, J.; Offenbacher, S.; Genco, R.; Persson, G.R.; Santucci, E.A.; Williams, R.C. Locally delivered minocycline microspheres for the treatment of periodontitis in smokers: Efficacy of minocycline microspheres in smokers. J. Clin. Periodontol. 2003, 30, 787–794. [Google Scholar] [CrossRef]
- Ali, M.; Walboomers, X.F.; Jansen, J.A.; Yang, F. Influence of formulation parameters on encapsulation of doxycycline in PLGA microspheres prepared by double emulsion technique for the treatment of periodontitis. J. Drug Deliv. Sci. Technol. 2019, 52, 263–271. [Google Scholar] [CrossRef]
- Loos, B.G.; Van Dyke, T.E. The role of inflammation and genetics in periodontal disease. Periodontol. 2000 2020, 83, 26–39. [Google Scholar] [CrossRef] [PubMed]
- Sheridan, R.A.; Wang, H.-L.; Eber, R.; Oh, T.-J. Systemic Chemotherapeutic Agents as Adjunctive Periodontal Therapy: A Narrative Review and Suggested Clinical Recommendations. J. Int. Acad. Periodontol. 2015, 17, 123–134. [Google Scholar] [PubMed]
- Stewart, P.S. Antimicrobial Tolerance in Biofilms. Microbiol. Spectr. 2015, 3, 10–1128. [Google Scholar] [CrossRef] [PubMed]
- Oberoi, S.S.; Dhingra, C.; Sharma, G.; Sardana, D. Antibiotics in dental practice: How justified are we. Int. Dent. J. 2015, 65, 4–10. [Google Scholar] [CrossRef]
- Wang, Y.; Li, J.; Tang, M.; Peng, C.; Wang, G.; Wang, J.; Wang, X.; Chang, X.; Guo, J.; Gui, S. Smart stimuli-responsive hydrogels for drug delivery in periodontitis treatment. Biomed. Pharmacother. 2023, 162, 114688. [Google Scholar] [CrossRef]
- Chang, P.-C.; Chao, Y.-C.; Hsiao, M.-H.; Chou, H.-S.; Jheng, Y.-H.; Yu, X.-H.; Lee, N.; Yang, C.; Liu, D. Inhibition of periodontitis induction using a stimuli-responsive hydrogel carrying naringin. J. Periodontol. 2017, 88, 190–196. [Google Scholar] [CrossRef]
- Lin, X.; Lv, J.; Wang, D.; Liu, K. Injectable adhesive carboxymethyl chitosan-based hydrogels with self-mending and antimicrobial features for the potential management of periodontal diseases. RSC Adv. 2023, 13, 11903–11911. [Google Scholar] [CrossRef]
- Ruan, H.; Yu, Y.; Liu, Y.; Ding, X.; Guo, X.; Jiang, Q. Preparation and characteristics of thermoresponsive gel of minocycline hydrochloride and evaluation of its effect on experimental periodontitis models. Drug Deliv. 2016, 23, 525–531. [Google Scholar] [CrossRef]
- Chava, V.K.; Vedula, B.D. Thermo-reversible green tea catechin gel for local application in chronic periodontitis: A 4-week clinical trial. J. Periodontol. 2013, 84, 1290–1296. [Google Scholar] [CrossRef]
- Nasra, M.M.A.; Khiri, H.M.; Hazzah, H.A.; Abdallah, O.Y. Formulation, in-vitro characterization and clinical evaluation of curcumin in-situ gel for treatment of periodontitis. Drug Deliv. 2017, 24, 133–142. [Google Scholar] [CrossRef]
- Cai, G.; Ren, L.; Yu, J.; Jiang, S.; Liu, G.; Wu, S.; Cheng, B.; Li, W.; Xia, J. A microenvironment-responsive, controlled release hydrogel delivering Embelin to promote bone repair of periodontitis via anti-infection and osteo-immune modulation. Adv. Sci. 2024, 11, e2403786. [Google Scholar] [CrossRef] [PubMed]
- Zhang, L.; Wang, Y.; Wang, C.; He, M.; Wan, J.; Wei, Y.; Zhang, J.; Yang, X.; Zhao, Y.; Zhang, Y. Light-activable on-demand release of nano-antibiotic platforms for precise synergy of thermochemotherapy on periodontitis. ACS Appl. Mater. Interfaces 2020, 12, 3354–3362. [Google Scholar] [CrossRef] [PubMed]
- Ji, Q.X.; Chen, X.G.; Zhao, Q.S.; Liu, C.S.; Cheng, X.J.; Wang, L.C. Injectable thermosensitive hydrogel based on chitosan and quaternized chitosan and the biomedical properties. J. Mater. Sci. Mater. Med. 2009, 20, 1603–1610. [Google Scholar] [CrossRef] [PubMed]
- Lin, J.; He, Z.; Liu, F.; Feng, J.; Huang, C.; Sun, X.; Deng, H. Hybrid Hydrogels for Synergistic Periodontal Antibacterial Treatment with Sustained Drug Release and NIR-Responsive Photothermal Effect. Int. J. Nanomed. 2020, 15, 5377–5387. [Google Scholar] [CrossRef]
- Zheng, X.; Dong, Z.; Liang, Z.; Liu, Y.; Yin, X.; Han, M.; Cui, Z.; Mei, X.; Gao, X. Photothermally responsive icariin and carbon nanofiber modified hydrogels for the treatment of periodontitis. Front. Bioeng. Biotechnol. 2023, 11, 1207011. [Google Scholar] [CrossRef]
- Zhao, X.; Yang, Y.; Yu, J.; Ding, R.; Pei, D.; Zhang, Y.; He, G.; Cheng, Y.; Li, A. Injectable hydrogels with high drug loading through B-N coordination and ROS-triggered drug release for efficient treatment of chronic periodontitis in diabetic rats. Biomaterials 2022, 282, 121387. [Google Scholar] [CrossRef]
- Luo, Q.; Yang, Y.; Ho, C.; Li, Z.; Chiu, W.; Li, A.; Dai, Y.; Li, W.; Zhang, X. Dynamic hydrogel-metal-organic framework system promotes bone regeneration in periodontitis through controlled drug delivery. J. Nanobiotechnol. 2024, 22, 287. [Google Scholar] [CrossRef]
- Guo, J.; Sun, H.; Lei, W.; Tang, Y.; Hong, S.; Yang, H.; Tay, F.; Huang, C. MMP-8-responsive polyethylene glycol hydrogel for intraoral drug delivery. J. Dent. Res. 2019, 98, 564–571. [Google Scholar] [CrossRef]
- Kong, L.X.; Peng, Z.; Li, S.-D.; Bartold, P.M. Nanotechnology and its role in the management of periodontal diseases. Periodontol. 2000 2006, 40, 184–196. [Google Scholar] [CrossRef]
- Steinberg, D.; Friedman, M. Sustained-release delivery of antimicrobial drugs for the treatment of periodontal diseases: Fantasy or already reality? Periodontol. 2000 2020, 84, 176–187. [Google Scholar] [CrossRef]
- Sheng, Y.; Chen, Z.; Wu, W.; Lu, Y. Engineered organic nanoparticles to combat biofilms. Drug Discov. Today 2023, 28, 103455. [Google Scholar] [CrossRef] [PubMed]
- Zazo, H.; Colino, C.I.; Lanao, J.M. Current applications of nanoparticles in infectious diseases. J. Control. Release 2016, 224, 86–102. [Google Scholar] [CrossRef] [PubMed]
- Yin, I.X.; Zhang, J.; Zhao, I.S.; Mei, M.L.; Li, Q.; Chu, C.H. The antibacterial mechanism of silver nanoparticles and its application in dentistry. Int. J. Nanomed. 2020, 15, 2555–2562. [Google Scholar] [CrossRef] [PubMed]
- Nie, P.; Zhao, Y.; Xu, H. Synthesis, applications, toxicity and toxicity mechanisms of silver nanoparticles: A review. Ecotoxicol. Environ. Saf. 2023, 253, 114636. [Google Scholar] [CrossRef]
- Krishnasamy, N.; Ramadoss, R.; Vemuri, S.; Sujai, G.N.S. Optimizing Desmostachya bipinnata-derived platinum nanoparticles for enhanced antibacterial and biofilm reduction. Microb. Pathog. 2024, 196, 107004. [Google Scholar] [CrossRef]
- Deng, X.; Liang, S.; Cai, X.; Huang, S.; Cheng, Z.; Shi, Y.; Pang, M.; Ma, P.; Lin, J. Yolk-shell structured Au nanostar@metal-organic framework for synergistic chemo-photothermal therapy in the second near-infrared window. Nano Lett. 2019, 19, 6772–6780. [Google Scholar] [CrossRef]
- Dong, Z.; Lin, Y.; Xu, S.; Chang, L.; Zhao, X.; Mei, X.; Gao, X. NIR-triggered tea polyphenol-modified gold nanoparticles-loaded hydrogel treats periodontitis by inhibiting bacteria and inducing bone regeneration. Mater. Des. 2023, 225, 111487. [Google Scholar] [CrossRef]
- Zhao, J.; Wei, Y.; Xiong, J.; Liu, H.; Lv, G.; Zhao, J.; He, H.; Gou, J.; Yin, T.; Tang, X.; et al. A multiple controlled-release hydrophilicity minocycline hydrochloride delivery system for the efficient treatment of periodontitis. Int. J. Pharm. 2023, 636, 122802. [Google Scholar] [CrossRef]
- Pérez-Pacheco, C.G.; Fernandes, N.A.R.; Primo, F.L.; Tedesco, A.C.; Bellile, E.; Retamal-Valdes, B.; Feres, M.; Guimarães-Stabili, M.R.; Rossa, C. Local application of curcumin-loaded nanoparticles as an adjunct to scaling and root planing in periodontitis: Randomized, placebo-controlled, double-blind split-mouth clinical trial. Clin. Oral Investig. 2021, 25, 3217–3227. [Google Scholar] [CrossRef]
- Mahmoud, M.Y.; Steinbach-Rankins, J.M.; Demuth, D.R. Functional assessment of peptide-modified PLGA nanoparticles against oral biofilms in a murine model of periodontitis. J. Control. Release 2019, 297, 3–13. [Google Scholar] [CrossRef]
- Mahmoud, M.Y.; Demuth, D.R.; Steinbach-Rankins, J.M. BAR-encapsulated nanoparticles for the inhibition and disruption of Porphyromonas gingivalis-Streptococcus gordonii biofilms. J Nanobiotechnol. 2018, 16, 69. [Google Scholar] [CrossRef] [PubMed]
- Marek, M.R.J.; Pham, T.-N.; Wang, J.; Cai, Q.; Yap, G.P.A.; Day, E.S.; Rosenthal, J. Isocorrole-loaded polymer nanoparticles for photothermal therapy under 980 nm light excitation. ACS Omega 2022, 7, 36653–36662. [Google Scholar] [CrossRef] [PubMed]
- de Freitas, L.M.; Calixto, G.M.F.; Chorilli, M.; Giusti, J.S.M.; Bagnato, V.S.; Soukos, N.S.; Amiji, M.M.; Fontana, C.R. Polymeric nanoparticle-based photodynamic therapy for chronic periodontitis in vivo. Int. J. Mol. Sci. 2016, 17, 769. [Google Scholar] [CrossRef] [PubMed]
- Mansuri, S.; Kesharwani, P.; Jain, K.; Tekade, R.K.; Jain, N.K. Mucoadhesion: A promising approach in drug delivery system. React. Funct. Polym. 2016, 100, 151–172. [Google Scholar] [CrossRef]
- Fakhri, E.; Eslami, H.; Maroufi, P.; Pakdel, F.; Taghizadeh, S.; Ganbarov, K.; Yousefi, M.; Tanomand, A.; Yousefi, B.; Mahmoudi, S.; et al. Chitosan biomaterials application in dentistry. Int. J. Biol. Macromol. 2020, 162, 956–974. [Google Scholar] [CrossRef]
- Xu, S.; Zhou, Q.; Jiang, Z.; Wang, Y.; Yang, K.; Qiu, X.; Ji, Q. The effect of doxycycline-containing chitosan/carboxymethyl chitosan nanoparticles on NLRP3 inflammasome in periodontal disease. Carbohydr. Polym. 2020, 237, 116163. [Google Scholar] [CrossRef]
- Lu, B.; Lv, X.; Le, Y. Chitosan-modified PLGA nanoparticles for control-released drug delivery. Polymers 2019, 11, 304. [Google Scholar] [CrossRef]
- Liu, D.; Yang, P.; Hu, D.; Liu, F. Minocycline hydrochloride liposome controlled-release gel improves rat experimental periodontitis. Hua Xi Kou Qiang Yi Xue Za Zhi 2013, 31, 592–596. [Google Scholar]
- Hu, F.; Zhou, Z.; Xu, Q.; Fan, C.; Wang, L.; Ren, H.; Xu, S.; Ji, Q.; Chen, X. A novel pH-responsive quaternary ammonium chitosan-liposome nanoparticles for periodontal treatment. Int. J. Biol. Macromol. 2019, 129, 1113–1119. [Google Scholar] [CrossRef]
- Mozafari, M.R.; Javanmard, R.; Raji, M. Tocosome: Novel drug delivery system containing phospholipids and tocopheryl phosphates. Int. J. Pharm. 2017, 528, 381–382. [Google Scholar] [CrossRef]
- Mozafari, M.R.; Alavi, M. Main distinctions between tocosome and nano-liposome as drug delivery systems: A scientific and technical point of view. Micro Nano Bio Asp. 2023, 2, 26–29. [Google Scholar]
- Liu, J.; Liu, H.; Jia, Y.; Tan, Z.; Hou, R.; Lu, J.; Luo, D.; Fu, X.; Wang, L.; Wang, X. Glucose-sensitive delivery of tannic acid by a photo-crosslinked chitosan hydrogel film for antibacterial and anti-inflammatory therapy. J. Biomater. Sci. Polym. Ed. 2022, 33, 1644–1663. [Google Scholar] [CrossRef] [PubMed]
- Roldan, L.; Montoya, C.; Solanki, V.; Cai, K.Q.; Yang, M.; Correa, S.; Orrego, S. A novel injectable piezoelectric hydrogel for periodontal disease treatment. ACS Appl. Mater. Interfaces 2023, 15, 43441–43454. [Google Scholar] [CrossRef] [PubMed]
- Ma, S.; Lu, X.; Yu, X.; Du, Y.; Xu, S.; Li, M.; Peng, C.; Liu, Z.; Deng, J. An injectable multifunctional thermo-sensitive chitosan-based hydrogel for periodontitis therapy. Biomater. Adv. 2022, 142, 213158. [Google Scholar] [CrossRef]
- Conte, R.; Valentino, A.; De Luca, I.; Soares Pontes, G.; Calarco, A.; Cerruti, P. Thermo-responsive hydrogel containing microfluidic chitosan nanoparticles loaded with Opuntia ficus-indica extract for periodontitis treatment. Int. J. Mol. Sci. 2024, 25, 9374. [Google Scholar] [CrossRef]
- Mou, J.; Liu, Z.; Liu, J.; Lu, J.; Zhu, W.; Pei, D. Hydrogel containing minocycline and zinc oxide-loaded serum albumin nanopartical for periodontitis application: Preparation, characterization and evaluation. Drug Deliv. 2019, 26, 179–187. [Google Scholar] [CrossRef]
- Liang, Y.; Wang, B.; Yu, Q.; Wang, W.; Ge, S.; Shao, J. Ebselen optimized the therapeutic effects of silver nanoparticles for periodontal treatment. Int. J. Nanomed. 2023, 18, 8113–8130. [Google Scholar] [CrossRef]
- Li, X.; Qi, M.; Li, C.; Dong, B.; Wang, J.; Weir, M.D.; Imazato, S.; Du, L.; Lynch, C.D.; Xu, L.; et al. Novel nanoparticles of cerium-doped zeolitic imidazolate frameworks with dual benefits of antibacterial and anti-inflammatory functions against periodontitis. J. Mater. Chem. B Mater. Biol. Med. 2019, 7, 6955–6971. [Google Scholar] [CrossRef]
- Li, Y.; Xu, C.; Mao, J.; Mao, L.; Li, W.; Liu, Z.; Shin, A.; Wu, J.; Hou, L.; Li, D.; et al. ZIF-8-based nanoparticles for inflammation treatment and oxidative stress reduction in periodontitis. ACS Appl. Mater. Interfaces 2024, 16, 36077–36094. [Google Scholar] [CrossRef]
- Klepac-Ceraj, V.; Patel, N.; Song, X.; Holewa, C.; Patel, C.; Kent, R.; Amiji, M.M.; Soukos, N.S. Photodynamic effects of methylene blue-loaded polymeric nanoparticles on dental plaque bacteria. Lasers Surg. Med. 2011, 43, 600–606. [Google Scholar] [CrossRef]
- Soundarajan, S.; Rajasekar, A. Antibacterial and anti-inflammatory effects of a novel herb-mediated nanocomposite mouthwash in plaque-induced gingivitis: A randomized controlled trial. Dent. Med. Probl. 2023, 60, 445–451. [Google Scholar] [PubMed]
- Lecio, G.; Ribeiro, F.V.; Pimentel, S.P.; Reis, A.A.; da Silva, R.V.C.; Nociti, F., Jr.; Moura, L.; Duek, E.; Casati, M.; Casarin, R.C.V. Novel 20% doxycycline-loaded PLGA nanospheres as adjunctive therapy in chronic periodontitis in type-2 diabetics: Randomized clinical, immune and microbiological trial. Clin. Oral Investig. 2020, 24, 1269–1279. [Google Scholar] [CrossRef] [PubMed]
- Hayashi, J.-I.; Ono, K.; Iwamura, Y.; Sasaki, Y.; Ohno, T.; Goto, R.; Nishida, E.; Yamamoto, G.; Kikuchi, T.; Higuchi, N.; et al. Suppression of subgingival bacteria by antimicrobial photodynamic therapy using transgingival irradiation: A randomized clinical trial. J. Periodontol. 2024, 95, 718–728. [Google Scholar] [CrossRef] [PubMed]
- Qi, Q.M.; Mitragotri, S. Mechanistic study of transdermal delivery of macromolecules assisted by ionic liquids. J. Control. Release 2019, 311–312, 162–169. [Google Scholar] [CrossRef] [PubMed]
- Curreri, A.M.; Mitragotri, S.; Tanner, E.E.L. Recent Advances in Ionic Liquids in Biomedicine. Adv. Sci. 2021, 8, e2004819. [Google Scholar] [CrossRef]
- Tanner, E.E.L.; Ibsen, K.N.; Mitragotri, S. Transdermal insulin delivery using choline-based ionic liquids (CAGE). J. Control. Release 2018, 286, 137–144. [Google Scholar] [CrossRef]
- Yan, C.; Nakajima, M.; Ikeda-Imafuku, M.; Yanagawa, M.; Hayatsu, M.; Fukuta, T.; Shibata, S.; Mitragotri, S.; Tabeta, K. Choline and geranate ionic liquid for subgingival biofilm control. Int. J. Pharm. 2024, 662, 124544. [Google Scholar] [CrossRef]
- Nakajima, M.; Tanner, E.E.L.; Nakajima, N.; Ibsen, K.N.; Mitragotri, S. Topical treatment of periodontitis using an iongel. Biomaterials 2021, 276, 121069. [Google Scholar] [CrossRef]
- Funda, G.; Taschieri, S.; Bruno, G.A.; Grecchi, E.; Paolo, S.; Girolamo, D.; Del Fabbro, M. Nanotechnology scaffolds for alveolar bone regeneration. Materials 2020, 13, 201. [Google Scholar] [CrossRef]
- Hettiaratchi, M.H.; Krishnan, L.; Rouse, T.; Chou, C.; McDevitt, T.C.; Guldberg, R.E. Heparin-mediated delivery of bone morphogenetic protein-2 improves spatial localization of bone regeneration. Sci. Adv. 2020, 6, eaay1240. [Google Scholar] [CrossRef]
- Tan, J.; Zhang, M.; Hai, Z.; Wu, C.; Lin, J.; Kuang, W.; Tang, H.; Huang, Y.; Chen, X.; Liang, G. Sustained release of two bioactive factors from supramolecular hydrogel promotes periodontal bone regeneration. ACS Nano 2019, 13, 5616–5622. [Google Scholar] [CrossRef] [PubMed]
- Lee, B.-S.; Lee, C.-C.; Wang, Y.-P.; Chen, H.-J.; Lai, C.-H.; Hsieh, W.-L.; Chen, Y.W. Controlled-release of tetracycline and lovastatin by poly(D,L-lactide-co-glycolide acid)-chitosan nanoparticles enhances periodontal regeneration in dogs. Int. J. Nanomed. 2016, 11, 285–297. [Google Scholar]
- Ghavimi, M.A.; Bani Shahabadi, A.; Jarolmasjed, S.; Memar, M.Y.; Maleki Dizaj, S.; Sharifi, S. Nanofibrous asymmetric collagen/curcumin membrane containing aspirin-loaded PLGA nanoparticles for guided bone regeneration. Sci. Rep. 2020, 10, 18200. [Google Scholar] [CrossRef] [PubMed]
| Easy Application | Retention | Controlled and Sustained Drug Release | Biodegradability | Biocompatibility | |
|---|---|---|---|---|---|
| Fibers | No | Yes | Yes | Partial | No |
| Requires professional insertion | Structural retention | Sustained drug release over days | Depends on the material | Local tissue irritation | |
| SFs | Partial | Yes | Yes | Yes | Yes |
| Easier insertion, but requires clinical expertise | Mucoadhesive | Initial burst release followed by sustained drug release | Biodegradable polymers | Well-tolerated by periodontal tissues | |
| Gels | Yes | No | Partial | Yes | Yes |
| Injectable formulations | Rapid elimination | Initial burst release followed by sustained drug release | Biodegradable polymers | High biocompatibility | |
| MPs | Yes | No | Yes | Yes | Yes |
| Injectable formulations | Drug washout due to GCF flow | Sustained release with minimal burst risk | Biodegradable polymers | Well-tolerated by periodontal tissues |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nakajima, M.; Yanagawa, M.; Takikawa, H.; Thien, T.T.; Zegarra-Caceres, L.; Yan, C.; Tabeta, K. Advances in Local Drug Delivery for Periodontal Treatment: Present Strategies and Future Directions. Biomolecules 2025, 15, 903. https://doi.org/10.3390/biom15060903
Nakajima M, Yanagawa M, Takikawa H, Thien TT, Zegarra-Caceres L, Yan C, Tabeta K. Advances in Local Drug Delivery for Periodontal Treatment: Present Strategies and Future Directions. Biomolecules. 2025; 15(6):903. https://doi.org/10.3390/biom15060903
Chicago/Turabian StyleNakajima, Mayuka, Mayuko Yanagawa, Honoka Takikawa, Truong Tran Thien, Lorena Zegarra-Caceres, Chunyang Yan, and Koichi Tabeta. 2025. "Advances in Local Drug Delivery for Periodontal Treatment: Present Strategies and Future Directions" Biomolecules 15, no. 6: 903. https://doi.org/10.3390/biom15060903
APA StyleNakajima, M., Yanagawa, M., Takikawa, H., Thien, T. T., Zegarra-Caceres, L., Yan, C., & Tabeta, K. (2025). Advances in Local Drug Delivery for Periodontal Treatment: Present Strategies and Future Directions. Biomolecules, 15(6), 903. https://doi.org/10.3390/biom15060903