
Subclinical Hypothyroidism in Moderate-to-Severe Psoriasis: A Cross-Sectional Study of Prevalence and Clinical Implications

 ,
,
Abstract
1. Introduction
2. Materials and Methods
2.1. Patient Selection
2.2. Data Collection
2.3. Thyroid Function Assessment
2.4. Data Analysis
- Z = 1.96 (for a 95% confidence level)
- p = 0.0424
- E = 0.05 (margin of error)
2.5. Statistical Considerations
3. Results
3.1. Objective 1: Prevalence and Characteristics of Thyroid Dysfunction in Psoriatic Patients
- Type of Hypothyroidism: All 17 patients exhibited subclinical hypothyroidism, representing 100% of the cases within this group. One patient was diagnosed with multinodular goiter, three patients with Hashimoto’s thyroiditis, and the remaining patients with subclinical hypothyroidism.
- Duration of Hypothyroidism: Among those with hypothyroidism, some cases had a documented history dating back to 2014 or earlier, suggesting a chronic progression of thyroid dysfunction over at least a decade in select patients.
- Demographic Profile:
- Mean Age: The mean age of patients with thyroid dysfunction was 57.4 years, with a range of 49.6 to 72.2 years.
- Weight and Height: Patients in this group had a mean weight of 86.7 kg and an average height of 164.7 cm, suggesting that many individuals in this cohort fall within an overweight to mildly obese BMI range.
- Additional Autoimmune Conditions: No other autoimmune diseases were present among patients with thyroid dysfunction, aside from their hypothyroidism.
- Treatment and Follow-Up: All the patients in this subset adhered strictly to the prescribed psoriasis biologic therapy guidelines and did not use combined treatments. On average, these patients attended two follow-up visits per year for monitoring and management.

{kind=link}
{kind=link}
| Patient | Sex | Age | BMI | Smoking Habit | Comorbidities | Year Onset Psoriasis | Year Onset Hypothyroidism | Clinical Onset of Psoriasis |
|---|---|---|---|---|---|---|---|---|
| 1 | M | 75 | 32 | No | Diabetes mellitus, hypertension, dyslipidemia, metabolic syndrome, espondiloartrosis | 1992 | 2001 | Plaque |
| 2 | M | 53 | 26 | No | No | 2019 | 2015 | Plaque |
| 3 | F | 44 | 39 | No | Peripheral psoriasis arthritis, fibromyalgia | 1993 | 2003 | Plaque |
| 4 | F | 49 | 52 | No | Hypertension, peripheral psoriasis arthritis, anxiety–depressive syndrome | 2003 | 2004 | Plaque |
| 5 | F | 50 | 22 | No | Peripheral psoriasis arthritis, anxiety–depressive syndrome | 1984 | 1999 | Plaque |
| 6 | F | 74 | 31 | Yes | Dyslipidemia | 2017 | 2006 | Palmoplantar |
| 7 | F | 50 | 30 | No | Dyslipidemia | 1990 | 1994 | Plaque |
| 8 | F | 53 | 30 | Yes | Dyslipidemia, peripheral psoriasis arthritis, endometriosis | 1984 | 1991 | Palmoplantar |
| 9 | F | 62 | 23 | Yes | No | 2011 | 2012 | Plaque |
| 10 | F | 74 | 41 | Yes | Hypertension, dyslipidemia, metabolic syndrome, peripheral psoriasis arthritis, depression | 2014 | 2001 | Plaque |
| 11 | F | 64 | 33 | Yes | Hypertension, anxiety–depressive syndrome, multiple sclerosis | 2015 | 2017 | Pustulous palmoplantar |
| 12 | F | 61 | 23 | No | Hypertension | 1968 | 1987 | Plaque |
| 13 | F | 72 | 42 | No | Diabetes mellitus, hypertension, dyslipidemia, metabolic syndrome, peripheral psoriasis arthritis, anxiety–depressive syndrome | 2015 | 2024 | Plaque |
| 14 | F | 66 | 27 | No | No | 2000 | 2002 | Palmoplantar |
| 15 | F | 79 | 32 | No | Diabetes mellitus, hypertension, dyslipidemia, metabolic syndrome, heart failure | 2016 | 2014 | Scalp |
| 16 | F | 41 | 26 | No | No | 1993 | 1996 | Plaque |
| 17 | M | 27 | 33 | No | Inflammatory bowel disease | 2009 | 2004 | Scalp |
| Patient | PASI | BSA | DLQI | NRS Pruritus | Number of Therapeutic Lines Used (Systemic and Biological) | Current Treament | Time of Evolution with Treatment (Years) |
|---|---|---|---|---|---|---|---|
| 1 | 8 | 10 | 11 | 5 | Conventional Systemic 4, biological 2 | Ixekizumab | 4.3 |
| 2 | 6 | 8 | 5 | 0 | Conventional Systemic 1, biological 1 | Adalimumab bio | 0.7 |
| 3 | 5 | 5 | 5 | 10 | Conventional Systemic 2, biological 0 | Apremilast | 1.4 |
| 4 | 7 | 18 | 10 | 8 | Conventional Systemic 2, biological 2 | Secukinumab | 4 |
| 5 | 10 | 10 | 12 | 9 | Conventional Systemic 1, biological 1 | Adalimumab bio | 3 |
| 6 | 2 | 4 | 12 | 5 | Conventional Systemic 3, biological 3 | Secukinumab | 4 |
| 7 | 12 | 14 | 8 | 2 | Conventional Systemic 2, biological 2 | Risankizumab | 4 |
| 8 | 4 | 6 | 17 | 10 | Conventional Systemic 1, biological 2 | Secukinumab | 1 |
| 9 | 7 | 9 | 10 | 6 | Conventional Systemic 1, biological 1 | Etanercept | 2 |
| 10 | 17 | 23 | 17 | 7 | Conventional Systemic 1, biological 1 | Adalimumab bio | 7 |
| 11 | 2 | 2 | 2 | 8 | Conventional Systemic 2, biological 2 | Guselkumab | 1 |
| 12 | 6 | 7 | 10 | 0 | Conventional Systemic 1, biological 2 | Tildrakizumab | 0 |
| 13 | 12 | 21 | 13 | 10 | Conventional Systemic 3, biological 2 | Secukinumab | 4 |
| 14 | 3 | 4 | 23 | 10 | Conventional Systemic 3, biological 0 | Apremilast | 0 |
| 15 | 9 | 14 | 22 | 10 | Conventional Systemic 2, biological 1 | Adalimumab bio | 3 |
| 16 | 11 | 16 | 15 | 10 | Conventional Systemic 1, biological 1 | Adalimumab bio | 3 |
| 17 | 5 | 9 | 12 | 8 | Conventional Systemic 1, biological 3 | Risankizumab | 3 |
3.2. Objective 2: Comparison Between Patients with and Without Hypothyroidism
- Demographic Characteristics
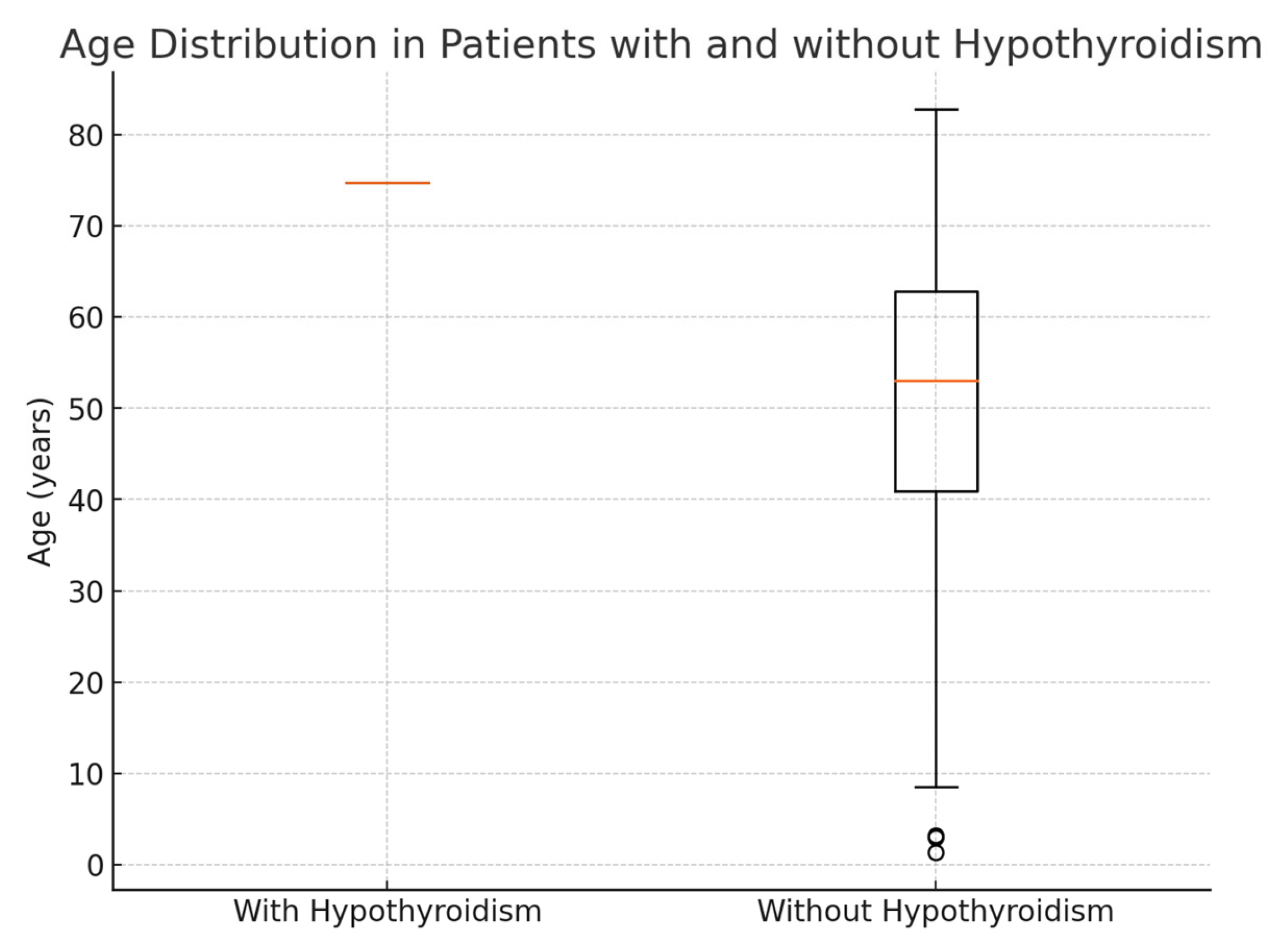
- Age: Patients with hypothyroidism were generally older, with an average age of 74.8 years, compared to an average age of 51.5 years in patients without hypothyroidism. This age difference suggests that thyroid dysfunction in this population may be associated with older age (Figure 1).
- The F:M ratio was 14:17, which meant that 82.35% of the patients with thyroid dysfunction in our study were female.
- Weight and Height: Hypothyroid patients had a mean weight of 92 kg and an average height of 169 cm, whereas those without hypothyroidism averaged 82.8 kg and the same mean height of 169 cm.
- 2.
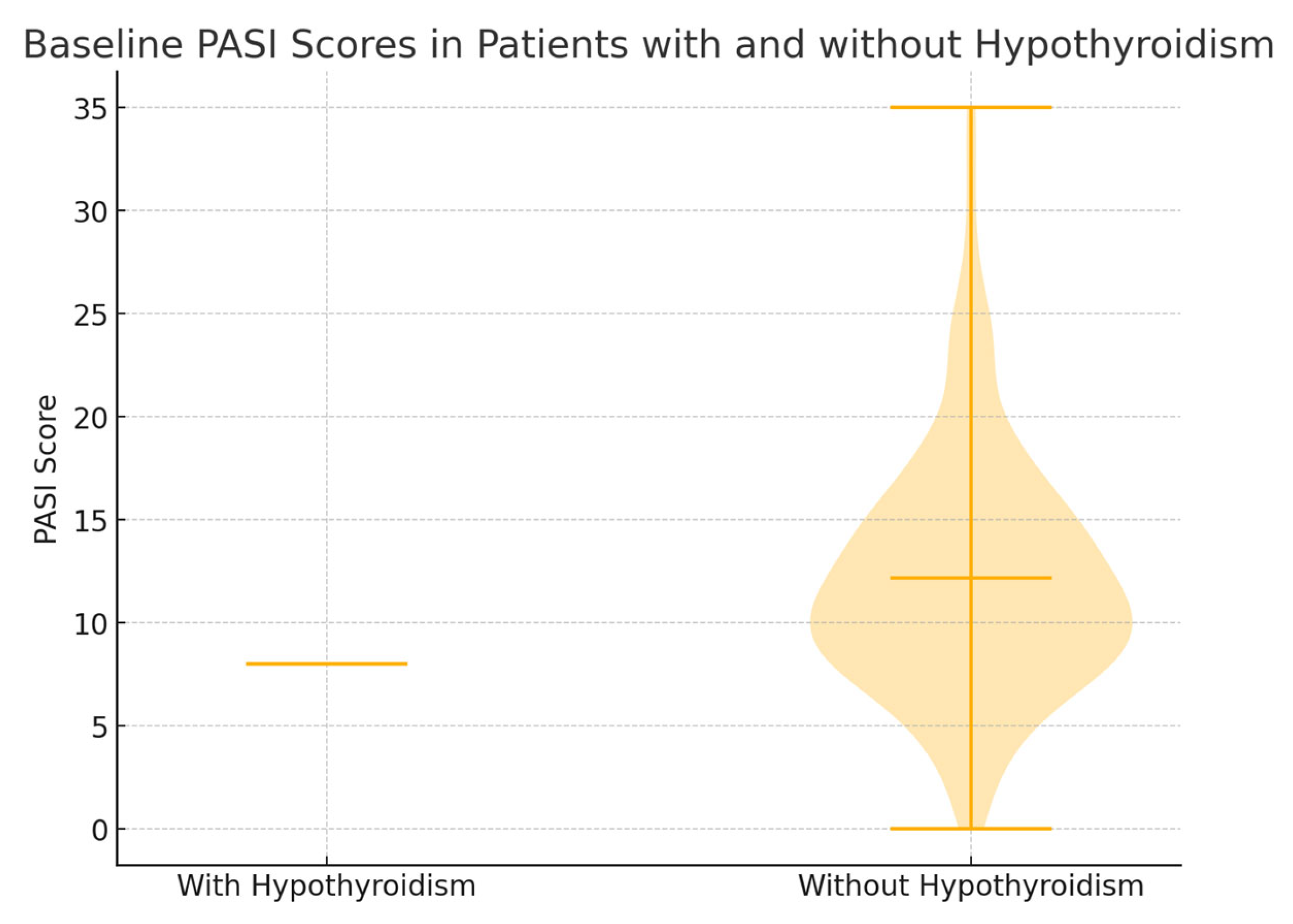
- Psoriasis Severity Parameters (Baseline and Over Time) (Figure 2)
- Psoriasis Area Severity Index (PASI):
- ○
- Baseline: Patients with hypothyroidism had a lower baseline PASI score (average of 8) compared to patients without hypothyroidism (average of 12.2), suggesting that the latter group had more severe psoriasis at the initial evaluation.
- ○
- Five-Year Follow-Up: PASI scores showed a tendency to decrease in both groups over time, reflecting a positive response to biologic treatment across the cohort.
- Body Surface Area (BSA):
- ○
- Baseline: Patients with hypothyroidism had an average BSA involvement of 10%, while those without hypothyroidism averaged 17.3%, indicating more extensive body surface involvement in the non-hypothyroid group at baseline.
- ○
- Evolution: Over the treatment period, BSA values generally decreased in both groups, demonstrating an improvement in skin involvement with consistent therapy.
- Dermatology Life Quality Index (DLQI): Both groups experienced a reduction in DLQI scores over time, indicating enhanced quality of life with treatment. The initial DLQI values did not significantly differ between the groups, suggesting comparable quality of life impacts from psoriasis regardless of thyroid status.
- Physician’s Global Assessment (PGA) and Pruritus Numerical Rating Scale (NRS): Both scores showed improvements in the severity and pruritus intensity in both groups, with similar initial and follow-up values.
- No statistically significant correlation was observed between Psoriasis Area Severity Index (PASI) or Body Surface Area (BSA) involvement and serum levels of anti-thyroid peroxidase antibodies (anti-TPO) among patients with thyroid dysfunction (Pearson’s r < 0.1, p > 0.05). Likewise, no association was found between the dosage of thyroid hormone replacement therapy (levothyroxine) and psoriasis severity measures (PASI or BSA) in treated patients. These findings suggest that neither autoimmune thyroid antibody levels nor the intensity of hormonal correction correlate with cutaneous disease burden in this cohort.
- 3.
- Treatment Lines
3.3. Objective 3: Prevalence and Characteristics of Thyroid Dysfunction in Psoriatic Patients Receiving Conventional Systemic Therapy
4. Key Differences and Clinical Implications
5. Discussion
6. Conclusions
7. Limitations and Future Directions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Fallahi, P.; Ferrari, S.M.; Ruffilli, I.; Elia, G.; Miccoli, M.; Sedie, A.D.; Riente, L.; Antonelli, A. Increased incidence of autoimmune thyroid disorders in patients with psoriatic arthritis: A longitudinal follow-up study. Immunol. Res. 2017, 65, 681–686. [Google Scholar] [CrossRef] [PubMed]
- Escribano-Serrano, J.; Mancera-Romero, J.; Santos-Sánchez, V.; Payá-Giner, C.; Méndez-Esteban, M.I.; García-Bonilla, A.; Márquez-Ferrando, M.; Hormigo-Pozo, A.; Michán-Doña, A. Prevalencia de hipotiroidismo en Andalucía según el consumo de hormona tiroidea en 2014 [Prevalence of Hypothyroidism in Andalusia, Spain, Determined by Thyroid Hormone Comsumption]. Rev. Esp. Salud Publica 2016, 90, e1–e12. [Google Scholar] [PubMed]
- Ruffilli, I.; Ragusa, F.; Benvenga, S.; Vita, R.; Antonelli, A.; Fallahi, P.; Ferrari, S.M. Psoriasis, Psoriatic Arthritis, and Thyroid Autoimmunity. Front. Endocrinol. 2017, 8, 139. [Google Scholar] [CrossRef] [PubMed]
- Zheng, H.; Li, W.; Liang, J.; Zhang, S. Assessing the relationship between psoriasis and thyroid dysfunction through two sample MR analysis. Arch. Dermatol. Res. 2024, 316, 403. [Google Scholar] [CrossRef] [PubMed]
- Prashant, P.; Garg, R.; Kataria, U.; Vashist, S.; Bansal, P.; Prakash, G.; Dokwal, S.; Bansal, A. Autoimmune Thyroid Disease in Psoriasis Patients: A Case-Control Study. Cureus 2023, 15, e50197. [Google Scholar] [CrossRef] [PubMed]
- Meneghini, V.; Tebar, W.R.; Souza Santos, I.; Silva Janovsky, C.C.P.; de Almeida-Pititto, B.; Lotufo, P.A.; Goulart, A.C.; Bensenor, I.M. Association between psoriasis and thyroid function: Results from the Brazilian Longitudinal Study of Adults Health (ELSA-Brasil). Arch. Endocrinol. Metab. 2023, 67, e000640. [Google Scholar] [CrossRef] [PubMed]
- Yumnam, D.; Kansal, N.K.; Kant, R. Association of Psoriasis With Thyroid Disorders: A Hospital-Based, Cross-Sectional Study. Cureus 2022, 14, e22987. [Google Scholar] [CrossRef] [PubMed]
- Rana, A.; Mahajan, V.K.; Chauhan, P.S.; Mehta, K.S.; Sharma, S.B.; Sharma, A.; Sharma, R. The Association of Thyroid Dysfunction with Chronic Plaque Psoriasis: A Hospital-Based Retrospective Descriptive Observational Study. Indian Dermatol. Online J. 2020, 11, 771–776. [Google Scholar] [CrossRef] [PubMed]
- Alidrisi, H.A.; Al Hamdi, K.; Mansour, A.A. Is There Any Association Between Psoriasis and Hashimoto’s Thyroiditis? Cureus 2019, 11, e4269. [Google Scholar] [CrossRef] [PubMed]
- Mooij, K.R.; Weetman, A.P. Subclinical hypothyroidism in older individuals. Nat. Rev. Endocrinol. 2024, 20, 9–20. [Google Scholar]
- Jansen, S.W.; van der Spoel, E.; van Heemst, D. Incidence and determinants of spontaneous normalization of subclinical hypothyroidism in older adults: Results from the TRUST study. J. Clin. Endocrinol. Metab. 2023, 108, e421–e430. [Google Scholar]
- Vassilatou, E.; Papadavid, E.; Papastamatakis, P.; Alexakos, D.; Koumaki, D.; Katsimbri, P.; Hadjidakis, D.; Dimitriadis, G.; Rigopoulos, D. No association of psoriasis with autoimmune thyroiditis. J. Eur. Acad. Dermatol. Venereol. 2017, 31, 102–106. [Google Scholar] [CrossRef] [PubMed]
- Liu, C.; Papewalis, C.; Domberg, J.; Scherbaum, W.A.; Schott, M. Chemokines, and autoimmune thyroid diseases. Horm. Metab. Res. 2008, 40, 361–368. [Google Scholar] [CrossRef] [PubMed]
- Kurylowicz, A.; Nauman, J. The role of nuclear factor-kappaB in the development of autoimmune diseases: A link between genes and the environment. Acta Biochim. Pol. 2008, 55, 629–647. [Google Scholar] [CrossRef] [PubMed]
- Kadam, D.P.; Suryakar, A.N.; Ankush, R.D.; Kadam, C.Y.; Deshpande, K.H. Role of oxidative stress in various stages of psoriasis. Indian J. Clin. Biochem. 2010, 25, 388–392. [Google Scholar] [CrossRef] [PubMed]
- Du, J.; Ma, C.; Wang, R.; Lin, L.; Gao, L.; Chen, S.; Lu, X. Relationship between Different Psoriasis Types and Thyroid Dysfunction: A Retrospective Analysis. Scanning 2021, 2021, 1834556. [Google Scholar] [CrossRef] [PubMed]
- Borges, A.S.; Valejo Coelho, M.M.; Brasileiro, A. A possible association between psoriasis and thyroid dysfunction. Eur. J. Dermatol. 2018, 28, 715–716. [Google Scholar] [CrossRef] [PubMed]
| Demographic Characteristics (n = 734) | Average/Percentage |
|---|---|
| Age | 42.6 years |
| Gender (Male/Female) | 56%/44% |
| BMI | 29.36 |
| Smoking status | 36% |
| Comorbidities | |
| Hypertension | 27% |
| Dyslipidemia | 19% |
| Diabetes | 12% |
| Psoriatic arthritis | 29% |
| Initial treatment | |
| Methotrexate | 81% |
| Cyclosporine | 6% |
| Acitretin | 4% |
| Phototherapy (NB-UVB) | 9% |
| Time of evolution of psoriasis | 19.6 years |
| Clinical features | |
| PASI | 5.4 |
| BSA | 7.6 |
| IGA | 2.3 |
| NRS pruritus | 4.5 |
| DLQI | 7.8 |
| Clinical features of thyroid dysfunction | |
| Prevalence of hypothyroidism at the time of initiation of systemic therapy | n = 16 (2.18%) |
| Development of hypothyroidism in the observation period after psoriatic treatment | N = 9 (1.25%) |
| Average age of onset of thyroid dysfunction | 51.7 years |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ruiz-Villaverde, R.; Cebolla-Verdugo, M.; Llamas-Segura, C.; Ezomo-Gervilla, P.J.; Molina-Espinosa, J.; Ruiz-Carrascosa, J.C. Subclinical Hypothyroidism in Moderate-to-Severe Psoriasis: A Cross-Sectional Study of Prevalence and Clinical Implications. Diseases 2025, 13, 237. https://doi.org/10.3390/diseases13080237
Ruiz-Villaverde R, Cebolla-Verdugo M, Llamas-Segura C, Ezomo-Gervilla PJ, Molina-Espinosa J, Ruiz-Carrascosa JC. Subclinical Hypothyroidism in Moderate-to-Severe Psoriasis: A Cross-Sectional Study of Prevalence and Clinical Implications. Diseases. 2025; 13(8):237. https://doi.org/10.3390/diseases13080237
Chicago/Turabian StyleRuiz-Villaverde, Ricardo, Marta Cebolla-Verdugo, Carlos Llamas-Segura, Pedro José Ezomo-Gervilla, Jose Molina-Espinosa, and Jose Carlos Ruiz-Carrascosa. 2025. "Subclinical Hypothyroidism in Moderate-to-Severe Psoriasis: A Cross-Sectional Study of Prevalence and Clinical Implications" Diseases 13, no. 8: 237. https://doi.org/10.3390/diseases13080237
APA StyleRuiz-Villaverde, R., Cebolla-Verdugo, M., Llamas-Segura, C., Ezomo-Gervilla, P. J., Molina-Espinosa, J., & Ruiz-Carrascosa, J. C. (2025). Subclinical Hypothyroidism in Moderate-to-Severe Psoriasis: A Cross-Sectional Study of Prevalence and Clinical Implications. Diseases, 13(8), 237. https://doi.org/10.3390/diseases13080237